
Exploring the impact of body mass change on fatigue and activity of the muscular system during daily routine
Abstract
BACKGROUND:
Correct body weight is one of the factors that allows you to maintain a properly functioning body. Abnormal body weight can cause muscle tissue remodelling, affecting activity and muscle fatigue. Changes in the muscular system can cause occurrence of functional limitations.
OBJECTIVE:
To determine the effect of weight change on fatigue and activity of the muscular system during daily activities.
METHODS:
The evaluation of musculoskeletal functioning was based on the results of computer simulations conducted in the AnyBody Modeling System. The following activities were analysed: standing, sitting down and getting up from a chair, holding and lifting an object, and walking. The simulations of the activities were carried out using averaged kinematic data, and by changing body mass in the range of 50 kg to 100 kg by increments of 2 kg, to map different nutritional status from excessive thinness to extreme obesity. Identification of loads in the musculoskeletal system was based on solving an inverse dynamics problem and then the estimation of muscle force values using static optimization. The simulation results allowed to determine the value of muscle fatigue and the level of muscle activity.
RESULTS:
For activities (i.e., standing, walking, sitting down and getting up from a chair) it was observed that the value of muscle fatigue increases with increasing body mass. However, for activities that cause more load on the musculoskeletal system, i.e. lifting and holding an object, the highest value of muscle fatigue was observed in underweight individuals.
CONCLUSION:
The change in body weight alters the functioning of the muscular system and thus the ability to perform activities. It was shown that in case of underweight, overweight or obese people, abnormal body weight can be the reason for occurrence of difficulties in performing the activities of lifting and holding a 20 kg object, as well as walking.
1.Introduction
Normal body weight reduces the risk of contracting a number of diseases caused by excess body fat. Both too much and too little body fat can be detrimental to health, so one should strive to maintain body weight within the optimal range. In addition to normal body weight and body fat levels, the level of muscle mass and the state of muscular system (among other strength capabilities) are extremely important for the proper functioning of musculoskeletal system [1].
Unfortunately, these days obesity has already reached epidemic proportions [2]. The prevalence of obesity is increasing at an alarming rate worldwide, having doubled since 1980 [3]. According to WHO statistics from 2016, 50 million girls and 74 million boys worldwide have been identified as obese. In Europe, 52% of the EU population aged
Obesity is also often identified as a detrimental factor that limits the performance of functional tasks [8, 19, 20, 21]. Despite numerous publications, the etiology of mechanical effects of obesity has not yet been well understood. Obesity is characterised by increased body size and weight, which can alter the ability to perform daily activities [19, 20, 22], as well as modify posture and the movement strategies used to perform them successfully [23].
On the other hand, modern times are dominated by the cult of slim figure and physical vigour. Many people, in pursuit of their dream figure, forget that proper body weight ensures healthy functioning of the body. It is worth noting that malnutrition, too little body fat and muscle mass, is also not desirable [24]. In addition, thinness, compared to overweight and obesity, is overlooked in scientific research in terms of causality, health risks and associated pathologies [24, 25]. Underweight, in many cases, is associated with reduced muscle mass and therefore reduced strength capabilities, which can also limit functional tasks [26] and affect the modification of movement strategies to achieve the desired goals.
Expectedly, the motor strategies of daily living activities will differ in people with different levels of BMI. Researchers provide numerous evidence of a strong link between obesity and balance disorders [27]. During daily activities, obese individuals report functional limitations especially in tasks that require flexibility of the trunk and hips [21]. For such a basic activity as walking, research indicates that obese adults have slower gait speed, greater absolute ground reaction forces and altered loading patterns of lower extremity joints compared to normal weight adults [28, 29, 30, 31, 32].
As expected, the research findings indicate that adults with higher BMI tend to experience greater limitations when performing activities of daily living than adults with lower BMI [33]. Erwin et al. [33], conducting a comprehensive review of the literature, also confirmed that there is no measure that can assess the limitations of a given physical activity. Currently, research examining the relationship between body weight and functional tasks has focused primarily on limitations of physical mobility due to body type, while little work has focused on determining the impact of weight change on muscular function. The only non-invasive method of assessing the effects of various factors on functioning of the musculoskeletal system is mathematical modelling of the human motor system [34]. The method of using optimization techniques is successfully applied to investigate clinical problems [34, 35], consequences of post-operative changes [36, 37] and to assess the ergonomics of movement and behaviour of musculoskeletal system under applied loads [38, 39, 40].
The aim of this study was to conduct computational simulations to determine the effect of weight change on fatigue and activity of the muscular system during daily living activities.
2.Materials and methods
The functioning of muscular system while performing basic daily activities was determined based on the results of computer simulations carried out in the AnyBody Modeling System v. 7.4.3 (AnyBody Technology Inc., Aalborg, Denmark). The analysed daily activities consisted of: standing, walking, sitting down and getting up from a chair, holding a 10 kg and 20 kg object, lifting a 10 kg and 20 kg object from a table.
In this study, two of the most popular models of the whole human body, StandingModel and FullBodyModel (Fig. 1), were used for simulations. These models consist of 69 rigid bodies representing individual body segments, which are connected by kinematic pairs with the number of degrees of freedom corresponding to the mobility of a given joint. The muscular system was modeled with about 1000 linear elements that represented the muscular actons. The kinematic and dynamic data obtained during the experimental studies were used as input data for the development of the models. The test group consisted of 30 adults, with a mean age of 29
Simulations were performed for the averaged kinematic and dynamic values of the entire group. The output data was a person with a height of 1.73 m and a body mass of 62 kg. Simulations of the analysed activities were carried out by changing the body mass from 50 kg to 100 kg by increments of 2 kg (Table 1), which made it possible to determine only the effect of changing mass (from excessive thinness to extreme obesity) on the functioning of musculoskeletal system. The dimensions of the body segments and the maximum values for generating muscle force were determined using the ScalingLengthMassFat scaling method based on weight, body height and body fat percentage [41].
Table 1
Analysed variants of simulated daily activities
| Simulation variants | Height [m] | Body mass [kg] | BMI [kg/m | Nutritional status | Risk of diseases associated with obesity |
|---|---|---|---|---|---|
| 1 | 1.73 | 50 | 16.71 | Underweight | Minimal |
| 2 | 1.73 | 52 | 17.37 | ||
| 3 | 1.73 | 54 | 18.04 | ||
| 4 | 1.73 | 56 | 18.71 | Normal weight | Minimal |
| 5 | 1.73 | 58 | 19.38 | ||
| 6 | 1.73 | 60 | 20.05 | ||
| 7 | 1.73 | 62 | 20.72 | ||
| 8 | 1.73 | 64 | 21.38 | ||
| 9 | 1.73 | 66 | 22.05 | ||
| 10 | 1.73 | 68 | 22.72 | ||
| 11 | 1.73 | 70 | 23.39 | ||
| 12 | 1.73 | 72 | 24.06 | ||
| 13 | 1.73 | 74 | 24.73 | ||
| 14 | 1.73 | 76 | 25.39 | Overweight | Medium |
| 15 | 1.73 | 78 | 26.06 | ||
| 16 | 1.73 | 80 | 26.73 | ||
| 17 | 1.73 | 82 | 27.40 | ||
| 18 | 1.73 | 84 | 28.07 | ||
| 19 | 1.73 | 86 | 28.73 | ||
| 20 | 1.73 | 88 | 29.40 | ||
| 21 | 1.73 | 90 | 30.07 | Obesity | High |
| 22 | 1.73 | 92 | 30.74 | ||
| 23 | 1.73 | 94 | 31.41 | ||
| 24 | 1.73 | 96 | 32.08 | ||
| 25 | 1.73 | 98 | 32.74 | ||
| 26 | 1.73 | 100 | 33.41 |
Figure 1.
Examples of models of analysed daily activities in AnyBody Modeling System.
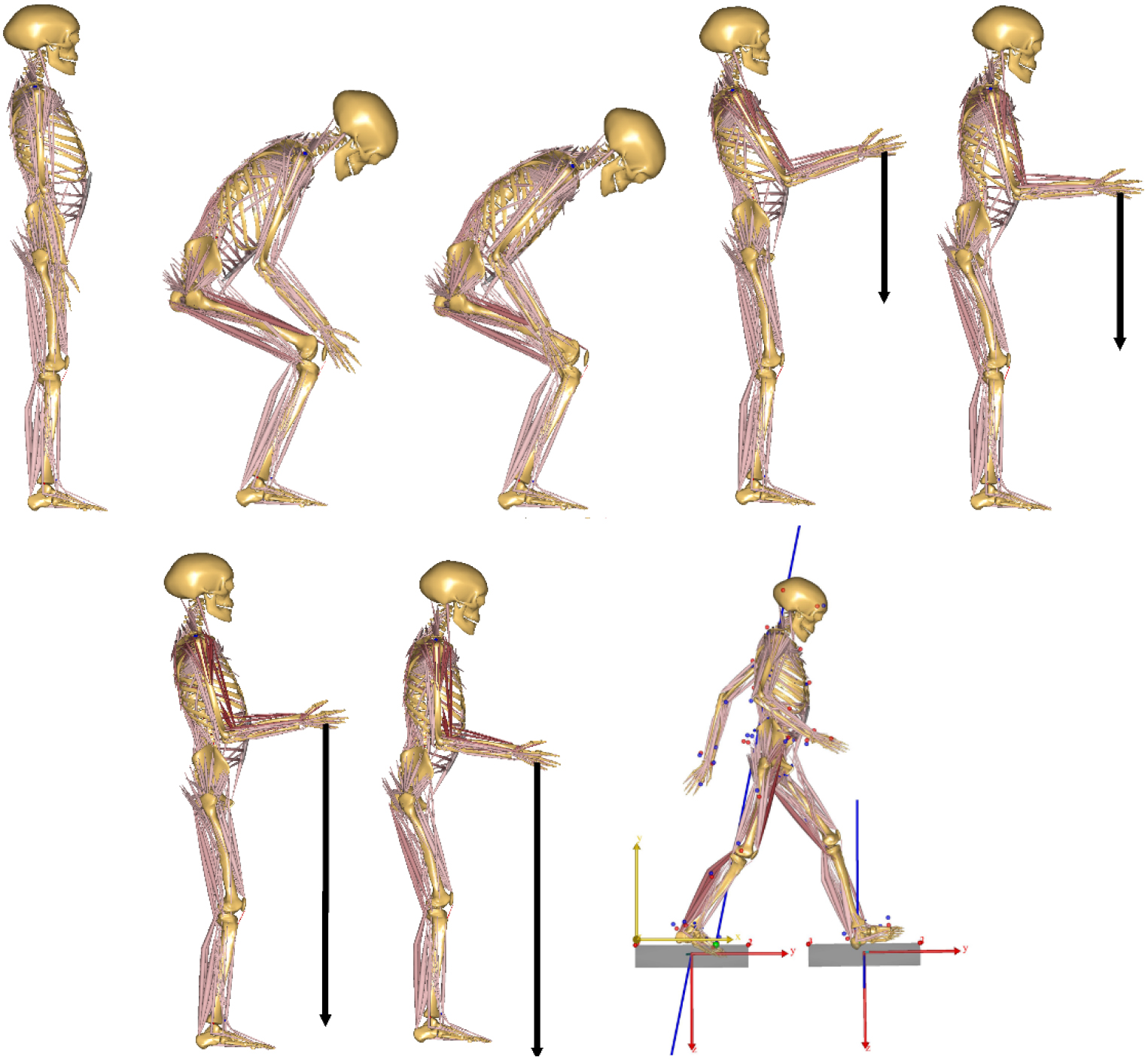
In the process of modifying the StandingModel and GaitFullModel mathematical models and performing simulations, the following assumptions and simplifications were made:
• symmetry of the body structure and performance of all analysed activities except gait was assumed,
• for the activities of sitting down and getting up from a chair and lifting an object from a table, simulations were carried out for a single moment, which, according to the research [39, 40, 42], was considered the most loaded for the lumbar spine:
– sitting down – the last moment before contact with the seat,
– standing up – moment of detachment of the body from the seat,
– lifting an object from the table – moment of detaching the object from the table.
• lifting an object of 10 kg and 20 kg was modeled by applying to the centre of each hand the vectors of forces acting on the OY axis with values of
• when simulating activities using the StandingModel, due to the limitations of the model, constant contact between the feet and the ground was assumed,
• during the simulation, a possible change in the kinematics of motion due to a change in body weight was not taken into account.
Identification of loads occurring in the musculoskeletal system in the AnyBody was based on solving an inverse dynamics task and then the estimation of muscle force values using static optimization. Adopted optimisation criterion was the criterion of movement control assuming minimisation of the cubic sum of proportion of the muscular force to the maximum force.
Simulations of daily activities were carried out to determine the functioning of the muscular system. The fatigue and muscle activity values of each individual muscle action implemented in AnyBody Modeling System were analysed. Muscle fatigue was expressed by the value of optimization task’s objective function, which should be interpreted as follows: the higher the function value, the higher the muscular fatigue. The ability to perform a given activity was also analysed, which was determined on the basis of the Activity parameter determined for individual muscles – the value of muscle activity. This parameter is defined as the ratio of muscle strength to the maximum force generated by a given muscle (Eq. (1)). The correct value of muscle activity ranges from 0 to 1, where 0 means that the muscle is inactive, while a value of 1 indicates maximum muscle activation. Obtaining a muscle activity value of more than 1 means that the muscular system is overloaded, and therefore unable to perform the activity.
(1)
Interpretation of the results: 0 – inactive muscle, 1 – maximum activation of the muscle,
3.Results
This chapter presents the effects of changing body weight on fatigue and muscle activity values that are the results of static optimization.
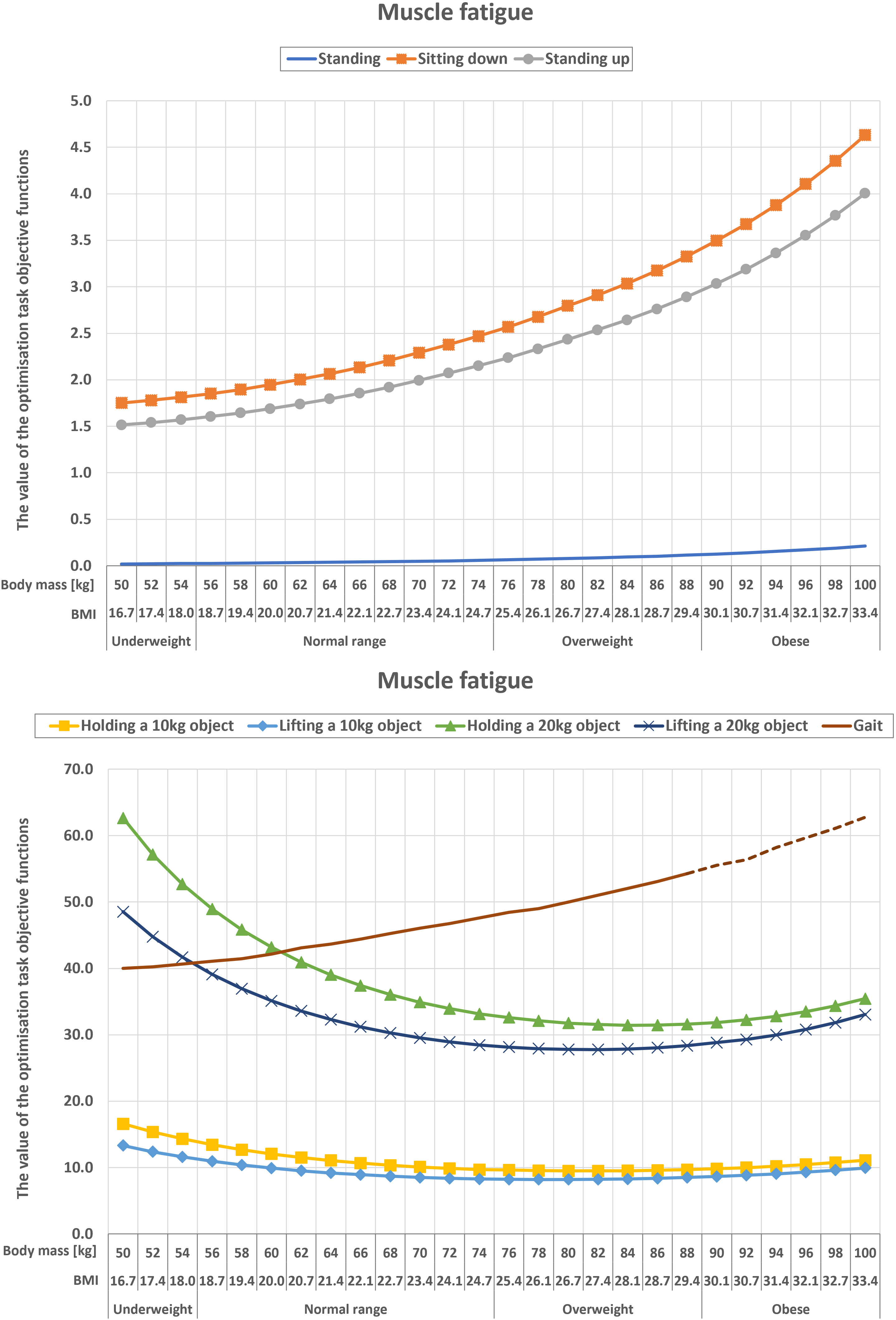
Figure 2 shows the effect of mass change on muscle fatigue recorded during basic daily activities. In the case of gait, graph shows the maximum fatigue value during one cycle. This value was recorded around 50% of the gait cycle. In the case of activities, i.e. standing, sitting and getting up from a chair, and walking, it was observed that the value of muscle fatigue increases with increasing body weight. Comparing the fatigue value for normal body weight (62 kg) and extreme obesity (100 kg), a 1.5-fold (walking) up to a 6-fold (standing) increase was observed. However, for activities that load the musculoskeletal system, i.e. lifting and holding an object, the highest value of muscle fatigue was observed in underweight individuals (body weight: 50–54 kg). Increasing the weight of the lifted object from 10 kg to 20 kg resulted in an average 3.5-fold increase in fatigue values. On the other hand, by analysing individual daily activities, it can be seen that the most demanding daily activities for the muscular system are walking, lifting and holding a 20 kg object.
Figure 2.
Effect of mass change on muscle fatigue during daily activities. In the case of gait, the dashed line indicates the conditions for which the muscular system was overloaded.
The effect of mass change on the ability to perform basic activities of daily living is summarised in Fig. 3. The
Figure 3.
Summary of the ability to perform various daily activities.
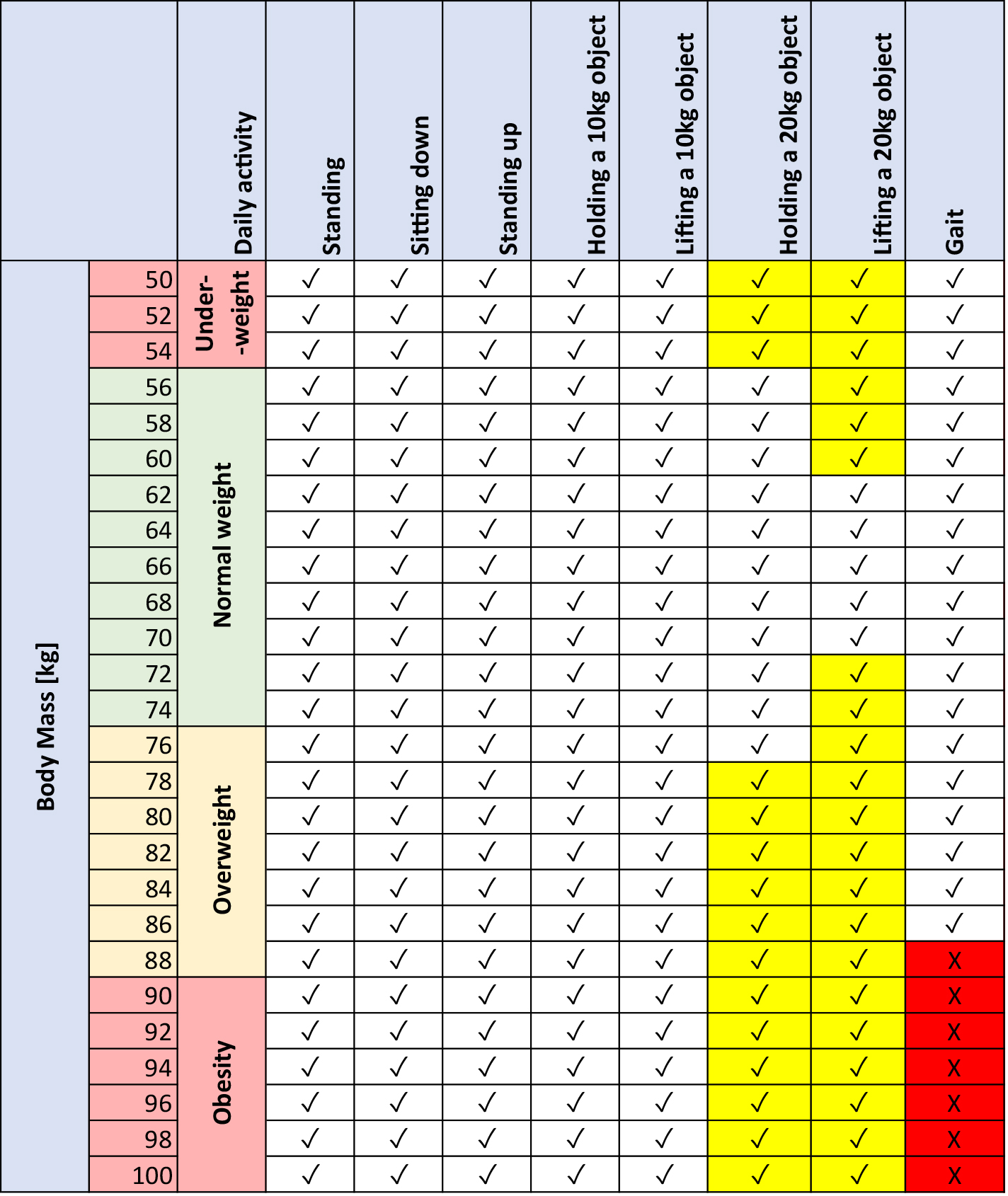
The effect of mass on the ability to perform the activity was noted for holding and lifting a 20 kg object and walking. Performing the activities of holding and lifting a 20 kg object for each variant analysed was possible, but resulted in the generation of maximum muscle force for the following upper limb muscles:
• Musculus brachialis,
• Musculus brachioradialis,
• Musculus biceps brachii caput breve,
• Musculus biceps brachii caput longum.
In case of holding an object, the need to generate maximum muscle force was observed when the person reached a body mass corresponding to overweight, while the lifting movement required the use of maximum muscle force already at normal body mass (72 kg). It should also be noted that for these two activities, the need to use maximum muscle force was also observed in underweight individuals.
During gait, problems with movement were observed after exceeding 88 kg of body mass (onset of obesity). The increased mass affected the overload of the following lower limb muscles:
• Gastrocnemius medialis,
• Muscuslus tibialis anterior,
• Musculus rectus femoris.
4.Discussion
The main scientific observations of our study are as follows:
1) an increase in body mass (and BMI values) leads to increased muscle fatigue for activities of daily living performed without additional external load (i.e., for standing, sitting down and getting up from a chair, and walking);
2) the appearance of additional external load required to be transferred by the musculoskeletal system (activities of lifting and holding an object) leads to an increase in muscle fatigue for underweight and normal weight individuals (with a normal BMI range), the lowest muscle fatigue was recorded for those with BMI values indicating overweight;
3) overweight, obesity and underweight can lead to muscle fatigue when performing activities of daily living; in extreme cases, people with abnormal body mass may have difficulties with performing simple movements.
The following are possible explanations and interpretations of the obtained results, also referring to the results of scientific works by other authors.
Effect of body mass on muscle quality and strength capabilities
Obesity affects muscle function, particularly muscle strength and muscle fatigue. Some studies have shown that higher BMI was associated with greater muscle mass and even with an increased absolute force and power production capacity [1, 17]. However, when these parameters were normalised to body mass, it appeared that overweight and obesity were associated with a reduction in strength capacity and muscle quality (i.e., expression of muscle function per unit of muscle mass) [1, 17]. Valenzuela et al. [18] showed a very high prevalence (75–92%) of poor muscle quality among obese individuals of various ages (18–75). And the poor muscle quality was mainly due to poor specific strength (not power). The probability of poor muscle quality increases with age, BMI, and is dependent on sex [18]. Despite treating obesity and muscular impairment as independent factors for morbidity and mortality, combining them together increases the risk of functional limitations and mortality [18, 43]. Inadequate muscle strength, especially in the lower extremities, can impair motor function during daily activities, as well as reducing the ability to work [44, 45]. The consequences of reduced muscle strength in the lower extremities are particularly significant in the elderly population, in whom muscle weakness reduces quality of life [16].
It seems to be extremely important for the proper functioning of the muscular system during daily activities to maintain body mass within the recommended ranges depending on weight and height. Implementing tailored interventions (e.g., strengthening appropriate muscle groups [46, 47], implementing a diet) to reduce the incidence of poor quality muscles with reduced strength capabilities can be important in both overweight, obese and underweight individuals.
Body mass status and functional limitations of activities of daily living
The simulation results indicate that the activity of lifting and holding an additional external heavy-weight load can lead to the generation of maximum upper limb muscle forces in underweight, overweight, and obese individuals, which may generate problems with the performance of the activity. It should be noted that the activity of lifting and holding an object have been rated as among the most spine-loading activities of daily living [39, 40]. The results of Corbeil et al. [48] suggest that an overweight obese worker has a significant additional impact on the strain on the musculoskeletal structures of the back, putting obese workers at greater risk of developing spinal conditions. On the other hand, underweight individuals with poor muscular strength capabilities may find it difficult to perform a simple functional task [26], and any additional weight will lead to overload of the musculoskeletal system and may involve modifications of movement strategies. It seems that in case of lifting activities, increased body mass (not excessively!), which will be associated with increased strength capabilities, can be used positively, also as part of the strategy of the applied lifting technique.
The results of the simulation obtained in this work indicate that obese people may also have problems with independent walking due to significant overloading of the muscles of the lower limbs. Kim et al. [29] have reported that individuals with a high BMI (
Limitation of this work and directions of futher research
In this study, it was decided to conduct computer simulations based on the unchanged, averaged kinematics of the performed movement, which represents a certain simplification. Literature data indicate that obese individuals may or may not have changed their strategies for performing basic activities of daily living. The most common movement analysed in the literature is gait, while information on the impact of obesity on movement kinematics is inconclusive. Kim et al. [29] detected no group differences in the COM motion or lower extremity kinetics and kinematics during gait, while Peggy et al. [50] showed some significant differences in temporal-spatial, joint motion and joint moment data between the obese and the non-obese participants. Therefore, the use of unchanged kinematics seems to be an acceptable simplification.
In further work, the plan is to conduct a series of experimental studies involving analysis of the kinematics of basic daily activities in subjects with different BMIs to verify the impact of the adopted simplifications on the simulation results and to develop scaling methods that allow the representation of different body shapes.
5.Conclusion
Both overweight and obesity, as well as underweight, can be dangerous to health, and our modeling studies also show that it can have an impact on the functioning of the muscular system in daily life. Based on the model studies carried out and the results obtained, the following conclusions were formulated:
• Being underweight, overweight or obese can lead to problems with performing basic everyday activities, due to the overloading of the muscular system (excessive muscle fatigue).
• With an abnormal BMI, lifting a 20 kg object and holding it can become a major challenge. Performing the activities resulted in the generation of maximum muscle force for the several upper limb muscles (musculus brachialis, musculus brachioradialis, musculus biceps brachii caput breve, musculus biceps brachii caput longum).
• Severely overweight and obese people may be unable to walk independently. The increased mass affected the overload of some of the lower limb muscles (gastrocnemius medialis, muscuslus tibialis anterior, musculus rectus femoris).
• A body mass that is too low can result in a person not having the enough muscle strength to perform a lifting action.
• Increased body weight requires the body to engage more muscles to perform the simplest daily activities.
Author contributions
Conceptualization: HZ, RM; Formal analysis and investigation: HZ, RM, KNL; Writing – original draft preparation: HZ, KNL; Writing – review and editing: RM; Resources: HZ, KNL; Supervision: RM.
Ethical approval
The experimental study was carried out with the approval of the bioethics committee issued by the Academy of Physical Education in Katowice (resolution number: 1/2020).
Funding
This research was funded by the National Science Centre Poland, project: “Mathematical model of prediction of health consequences in musculoskeletal system as a result of sedentary lifestyle” (grant number: 2019/35/O/ST8/02719).
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
References
[1] | Tallis J, James RS, Seebacher F. The effects of obesity on skeletal muscle contractile function. J Exp Biol. (2018) ; 221. doi: 10.1242/JEB.163840. |
[2] | World Obesity Federation. World Obesity Atlas. (2022) . |
[3] | Afshin A, Forouzanfar N, Reitsma M, Sur P, Estep K, Lee A, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. (2017) ; 377: : 13-27. doi: 10.1056/NEJMOA1614362. |
[4] | World Health Organization. Who European Regional Obesity Report. (2022) . |
[5] | Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, Wright CM, et al. The hormone resistin links obesity to diabetes. Nature. (2001) ; 409: : 307-12. doi: 10.1038/35053000. |
[6] | Manson JE, Colditz GA, Stampfer MJ, Willett WC, Rosner B, Monson RR, et al. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med. (1990) ; 322: : 882-9. doi: 10.1056/NEJM199003293221303. |
[7] | Manicardi V, Camellini L, Bellodi G, Coscelli C, Ferrannini E. Evidence for an association of high blood pressure and hyperinsulinemia in obese man. J Clin Endocrinol Metab. (1986) ; 62: : 1302-4. doi: 10.1210/JCEM-62-6-1302. |
[8] | Larsson B, Svärdsudd K, Welin L, Wilhelmsen L, Björntorp P, Tibblin G. Abdominal adipose tissue distribution, obesity, and risk of cardiovascular disease and death: 13 year follow up of participants in the study of men born in 1913. Br Med J (Clin Res Ed). (1984) ; 288: : 1401. doi: 10.1136/BMJ.288.6428.1401. |
[9] | Song YM, Sung J, Smith GD, Ebrahim S. Body mass index and ischemic and hemorrhagic stroke: A prospective study in Korean men. Stroke. (2004) ; 35: : 831-6. doi: 10.1161/01.STR.0000119386.22691.1C. |
[10] | Maffiuletti NA, Jubeau M, Agosti F, Col A, Sartorio A. Quadriceps muscle function characteristics in severely obese and nonobese adolescents. Eur J Appl Physiol. (2008) ; 103: : 481-4. doi: 10.1007/S00421-008-0737-3. |
[11] | Blimkie CJR, Sale DG, Bar-Or O. Voluntary strength, evoked twitch contractile properties and motor unit activation of knee extensors in obese and non-obese adolescent males. Eur J Appl Physiol Occup Physiol. (1990) ; 61: : 313-8. doi: 10.1007/BF00357619. |
[12] | Maffiuletti NA, Jubeau M, Munzinger U, Bizzini M, Agosti F, De Col A, et al. Differences in quadriceps muscle strength and fatigue between lean and obese subjects. Eur J Appl Physiol. (2007) ; 101: : 51-9. doi: 10.1007/S00421-007-0471-2. |
[13] | Hulens M, Vansant G, Lysens R, Claessens AL, Muls E, Brumagne S. Study of differences in peripheral muscle strength of lean versus obese women: An allometric approach. Int J Obes Relat Metab Disord. (2001) ; 25: : 676-81. doi: 10.1038/SJ.IJO.0801560. |
[14] | Zoico E, Di Francesco V, Guralnik JM, Mazzali G, Bortolani A, Guariento S, et al. Physical disability and muscular strength in relation to obesity and different body composition indexes in a sample of healthy elderly women. Int J Obes Relat Metab Disord. (2004) ; 28: : 234-41. doi: 10.1038/SJ.IJO.0802552. |
[15] | Rolland Y, Lauwers-Cances V, Pahor M, Fillaux J, Grandjean H, Vellas B. Muscle strength in obese elderly women: Effect of recreational physical activity in a cross-sectional study. Am J Clin Nutr. (2004) ; 79: : 552-7. doi: 10.1093/AJCN/79.4.552. |
[16] | Tomlinson DJ, Erskine RM, Morse CI, Winwood K, Onambélé-Pearson G. The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology. (2016) ; 17: : 467-83. doi: 10.1007/S10522-015-9626-4. |
[17] | Cava E, Yeat NC, Mittendorfer B. Preserving healthy muscle during weight loss. Adv Nutr. (2017) ; 8: : 511-9. doi: 10.3945/AN.116.014506. |
[18] | Valenzuela PL, Maffiuletti NA, Tringali G, De Col A, Sartorio A. Obesity-associated poor muscle quality: prevalence and association with age, sex, and body mass index. BMC Musculoskelet Disord. (2020) ; 21. doi: 10.1186/S12891-020-03228-Y. |
[19] | Backholer K, Wong E, Freak-Poli R, Walls HL, Peeters A. Increasing body weight and risk of limitations in activities of daily living: A systematic review and meta-analysis. Obes Rev. (2012) ; 13: : 456-68. doi: 10.1111/j.1467-789X.2011.00970.x. |
[20] | Gilleard W. Functional task limitations in obese adults. Curr Obes Rep. (2012) ; 1: : 174-80. doi: 10.1007/s13679-012-0019-6. |
[21] | Capodaglio P, Castelnuovo G, Brunani A, Vismara L, Villa V, Maria Capodaglio E. Functional limitations and occupational issues in obesity: A review. Int J Occup Saf Ergon. (2010) ; 16: : 507-23. doi: 10.1080/10803548.2010.11076863. |
[22] | Houston DK, Ding J, Nicklas BJ, Harris TB, Lee JS, Nevitt MC, et al. The association between weight history and physical performance in the Health, Aging and Body Composition study. Int J Obes. (2007) ; 31: : 1680-7. doi: 10.1038/sj.ijo.0803652. |
[23] | Gilleard W, Smith T. Effect of obesity on posture and hip joint moments during a standing task, and trunk forward flexion motion. Int J Obes. (2007) ; 31: : 267-71. doi: 10.1038/sj.ijo.0803430. |
[24] | Golubnitschaja O, Liskova A, Koklesova L, Samec M, Biringer K, Büsselberg D, et al. Caution, “normal” BMI: Health risks associated with potentially masked individual underweight-EPMA Position Paper 2021. EPMA J. (2021) ; 12: : 243-64. doi: 10.1007/S13167-021-00251-4. |
[25] | Lazzeri G, Rossi S, Kelly C, Vereecken C, Ahluwalia N, Giacchi MV. Trends in thinness prevalence among adolescents in ten European countries and the USA (1998–2006): A cross-sectional survey. Public Health Nutr. (2014) ; 17: : 2207-15. doi: 10.1017/S1368980013002541. |
[26] | An R, Shi Y. Body weight status and onset of functional limitations in U.S. middle-aged and older adults. Disabil Health J. (2015) ; 8: : 336-44. doi: 10.1016/j.dhjo.2015.02.003. |
[27] | Del Porto HC, Pechak CM, Smith DR, Reed-Jones RJ. Biomechanical effects of obesity on balance. Int J Exerc Sci. (2012) ; 5: : 301-20. |
[28] | Kim D, Lewis CL, Gill SV. Effects of obesity and foot arch height on gait mechanics: A cross-sectional study. PLoS One. (2021) ; 16. doi: 10.1371/JOURNAL.PONE.0260398. |
[29] | Kim HK, Lu SH, Lu TW, Chou LS. Contribution of lower extremity muscles to center of mass acceleration during walking: Effect of body weight. J Biomech (2023) ; 146: : 111398. doi: 10.1016/J.JBIOMECH.2022.111398. |
[30] | Browning RC. Locomotion mechanics in obese adults and children. Curr Obes Rep. (2012) ; 1: : 152-9. doi: 10.1007/S13679-012-0021-Z/FIGURES/1. |
[31] | Ko SU, Stenholm S, Ferrucci L. Characteristic gait patterns in older adults with obesity-results from the Baltimore Longitudinal Study of Aging. J Biomech. (2010) ; 43: : 1104-10. doi: 10.1016/J.JBIOMECH.2009.12.004. |
[32] | DeVita P, Hortobágyi T. Obesity is not associated with increased knee joint torque and power during level walking. J Biomech. (2003) ; 36: : 1355-62. doi: 10.1016/S0021-9290(03)00119-2. |
[33] | Ervin CM, Whalley D, von Huth Smith L, Crawford R, Dine J, Fehnel SE. Development of the impact of weight on daily activities questionnaire: A patient-reported outcome measure. Clin Obes. (2020) ; 10. doi: 10.1111/COB.12387. |
[34] | Michnik R, Jurkojć J, Pauk J. Identification of muscles forces during gait of children with foot disabilities. Mechanika. (2009) ; 80: : 48-51. doi: 10.5755/J01.MECH.80.6.15505. |
[35] | Marra MA, Vanheule V, Fluit R, Koopman BHFJM, Rasmussen J, Verdonschot N, et al. A subject-specific musculoskeletal modeling framework to predict in vivo mechanics of total knee arthroplasty. J Biomech Eng. (2015) ; 137. doi: 10.1115/1.4029258. |
[36] | Dreischarf M, Albiol L, Zander T, Arshad R, Graichen F, Bergmann G, et al. In vivo implant forces acting on a vertebral body replacement during upper body flexion. J Biomech. (2015) ; 48: : 560-5. doi: 10.1016/J.JBIOMECH.2015.01.007. |
[37] | Rajaee MA, Arjmand N, Shirazi-Adl A, Plamondon A, Schmidt H. Comparative evaluation of six quantitative lifting tools to estimate spine loads during static activities. Appl Ergon. (2015) ; 48: : 22-32. doi: 10.1016/J.APERGO.2014.11.002. |
[38] | Zadoń H, Nowakowska-Lipiec K, Michnik R. A sitting or standing position – which one exerts more loads on the musculoskeletal system of the lumbar spine? Comparative tests based on the methods of mathematical modelling. Acta Bioeng Biomech. (2021) ; 23: : 1-17. doi: 10.37190/ABB-01762-2020-01. |
[39] | Zadoń H, Michnik R, Nowakowska K, Myśliwiec A. Assessment of Loads Exerted on the Lumbar Segment of the Vertebral Column in Everyday-Life Activities – Application of Methods of Mathematical Modelling. Adv. Intell. Syst. Comput. vol. 1011, Springer Verlag; 2019: ; 554-65. doi: 10.1007/978-3-030-23762-2_49. |
[40] | Nowakowska K, Michnik R, Myśliwiec A, Zadoń H. Identification of loads occurring in the lumbar spine section during the action of lifting objects. Eng. Mech. 2018. 24th Int. Conf. May 14–17, 2018, Svratka, Czech Repub. (2018) ; pp. 617-20. doi: 10.21495/91-8-617. |
[41] | Rasmussen J, de Zee M, Damsgaard M, Christensen ST, Marek C, Siebertz K. A General Method for Scaling Musculo-Skeletal Models. Int Symp Comput Simul. (2005) . |
[42] | Nowakowska K, Gzik M, Michnik R, Myśliwiec A, Jurkojć J, Suchoń S, et al. The loads acting on lumbar spine during sitting down and standing up. Adv Intell Syst Comput. (2017) ; 526: : 169-76. doi: 10.1007/978-3-319-47154-9_20/FIGURES/3. |
[43] | da Silva Alexandre T, Scholes S, Ferreira Santos JL, de Oliveira Duarte YA, de Oliveira C. Dynapenic abdominal obesity increases mortality risk among english and brazilian older adults: A 10-year follow-up of the ELSA and SABE studies. J Nutr Heal Aging. (2018) ; 22: : 138-44. doi: 10.1007/s12603-017-0966-4. |
[44] | Hills AP, Hennig EM, Byrne NM, Steele JR. The biomechanics of adiposity – Structural and functional limitations of obesity and implications for movement. Obes Rev. (2002) ; 3: : 35-43. doi: 10.1046/j.1467-789X.2002.00054.x. |
[45] | Maffiuletti NA, Ratel S, Sartorio A, Martin V. The impact of obesity on in vivo human skeletal muscle function. Curr Obes Rep. (2013) ; 2: : 251-60. doi: 10.1007/s13679-013-0066-7. |
[46] | Nowakowska K, Michnik R, Myśliwiec A, Chrzan M. Impact of strengthening of the erector spinae muscle on the values of loads of the muskuloskeletal system in the lumbar spine section. Eng. Mech. 2017, 23rd Int. Conf. May 15–18, Svratka, Czech Republic. 2017; pp. 718-21. |
[47] | Nowakowska-Lipiec K, Michnik R, Linek P, Myśliwiec A, Jochymczyk-Woźniak K, Gzik M. A numerical study to determine the effect of strengthening and weakening of the transversus abdominis muscle on lumbar spine loads. Comput Methods Biomech Biomed Engin. (2020) ; 1-10. doi: 10.1080/10255842.2020.1795840. |
[48] | Corbeil P, Plamondon A, Handrigan G, Vallée-Marcotte J, Laurendeau S, Ten Have J, et al. Biomechanical analysis of manual material handling movement in healthy weight and obese workers. Appl Ergon. (2019) ; 74: : 124-33. doi: 10.1016/j.apergo.2018.08.018. |
[49] | Amiri P, Hubley-Kozey CL, Landry SC, Stanish WD, Astephen Wilson JL. Obesity is associated with prolonged activity of the quadriceps and gastrocnemii during gait. J Electromyogr Kinesiol. (2015) ; 25: : 951-8. doi: 10.1016/j.jelekin.2015.10.007. |
[50] | Lai PPK, Leung AKL, Li ANM, Zhang M. Three-dimensional gait analysis of obese adults. Clin Biomech. (2008) ; 23: : S2-6. doi: 10.1016/j.clinbiomech.2008.02.004. |


