
Rehabilitative training system based on a ceiling rail for detecting the intended movement direction of a user
Abstract
BACKGROUND:
Accurate detection of the intended movement direction of a patient plays an important role in the development of a training system for gait rehabilitation and enables to increase the effect of gait rehabilitation training.
OBJECTIVE:
This study investigated the detection of the intended movement of a user to operate a ceiling rail-based rehabilitative training system with accurate timing.
METHODS:
To detect the movement direction intention of a user, two potentiometers were used to measure the movement direction in the anterior, posterior, and left and right directions of the user when operating the driving motor of the rehabilitative training system. A simple test mock-up with two potentiometers was fabricated, and the experiments were conducted to determine the effect of the direction of movement on the measured values of potentiometers. A direction measurement algorithm was developed to control the driving motor of the rail-based gait rehabilitative training system.
RESULTS:
The intended movement direction of the user could be predicted for eight directions by combining the “positive value, 0, negative value” of each measured value of the two potentiometers. Further, the developed algorithm was effectively used to control the driving function to assist the walking, sitting–standing, and climbing up–down the step activities in daily life.
CONCLUSIONS:
The movement intention detection function for users developed in this paper can be used to effectively control a rehabilitative training system for patients with hemiplegia to improve gait movement and posture balance, thereby improving their function of activities of daily living.
1.Introduction
Gait is an action that causes movement from one place to another and promotes forward movement of the center of the body through the movement of multiple joints and the pelvis and the continuous movement of muscles [1], and it is the most basic action in daily activities. In recent years, the aging population in major industrialized countries has been rapidly progressing, and consequently, the number of patients with arthritis, stroke, stroke-induced paralysis, etc. is increasing rapidly; further, it is expected that the number of potential gait disturbance populations with a high probability of experiencing gait disturbances will increase more rapidly with time [2]. Nevertheless, the physical environment in most local communities is centered on people without disabilities. This limits the social participation of people with disabilities, who are limited in their activities due to the loss of their independent mobility, which is a factor that reduces the quality of life [3, 4]. Thus, for them, the problem of mobility is the most fundamental element in preventing social isolation and carrying out activities of daily living, which is a problem that must be handled as a priority [5].
Various studies have been conducted worldwide to develop gait rehabilitative training systems for the effective gait rehabilitation of people with mobility impairments using exoskeleton gait assist systems and treadmills, etc. EKSO Bionics developed EKSO, a lower extremity exoskeleton system using four electric motors for the hip and knee joints that operate only in the sagittal plane to improve the gait ability of patients with spinal cord injury [6]. Lokomat is a gait rehabilitative training system developed by Hocoma, which is a combination of a human wearable gait rehabilitative training system, a body weight support system, and a treadmill, and research is under way to maximize the effect of the rehabilitative training [7]. Studies were also conducted on the development of gait rehabilitation training systems using a treadmill. Hesse investigated the effects of treadmill gait training on patients with hemiplegia [8, 9]. Werner compared the training effects on gait training equipment and treadmill gait in subacute stroke patients [10].
However, the treadmill gait shows a large difference compared to over-ground gait because it is difficult to realize a natural gait motion on a treadmill driven by a motor and performed with a fixed position of a user in a predetermined space. In addition, unlike treadmill gait, gait rehabilitation in daily environment should be performed by determining the gait and the environment of the patient. If the gait motion is performed without sufficient preparation, it is possible to cause a fatal injury to the patient [11]. Many studies have been conducted to compare kinematics to determine the differences in the joint angles for the treadmill and over-ground gaits and kinetics to identify the differences in the force such as joint torque, etc. [12, 13, 14]. In particular, a number of studies have been conducted that compare the effects of treadmill and over-ground gait training, particularly in patients with stroke and incomplete spinal cord injury [15, 16, 17].
Hidler developed a ZeroG rehabilitation training system, which is a gait and balance training system using a ceiling rail [18]. The developed equipment is used in studies on metabolic consumption and muscle usage patterns of stroke-induced hemiplegia patients and incomplete spinal cord injury patients in clinical practices of hospitals in the US [19, 20]. However, the developed equipment has a power cable connected for driving the motor, which leads to limitation in the space of use. Movement intention detection technique plays an important role in patient gait rehabilitation by controlling the driving motor of the gait rehabilitative training system with precise timing. The patient can easily perform the rehabilitation activity as the technique measures the bio-signal related to the movement of the patient and assists the movement at an appropriate timing. Kim developed a gait rehabilitation robot that secures the arm freedom by detecting user intention through the application of precise gait tracking algorithm using variable resistance and stereo camera [21].
Kim developed a ceiling rail-based rehabilitative training system through basic research on the design of the mechanical part of the training system for gait rehabilitation using the battery power supply method free from the power cable, and with the developed system, healthy adults performed activities of daily living related to lower extremities [22, 23]. This paper investigates the detection of the intended movement direction to operate the ceiling rail-based rehabilitative training system with precise timing, and to this end, a simple test mock-up with two potentiometers was fabricated to develop a direction measurement algorithm. This study also aims to confirm whether the direction measurement algorithm developed in this paper can be utilized in the driving motor control of the rail-based gait rehabilitative training system and can assist in the activities of daily living related to lower extremities.
2.System configuration
2.1Overview of the gait rehabilitative training system based on a ceiling rail
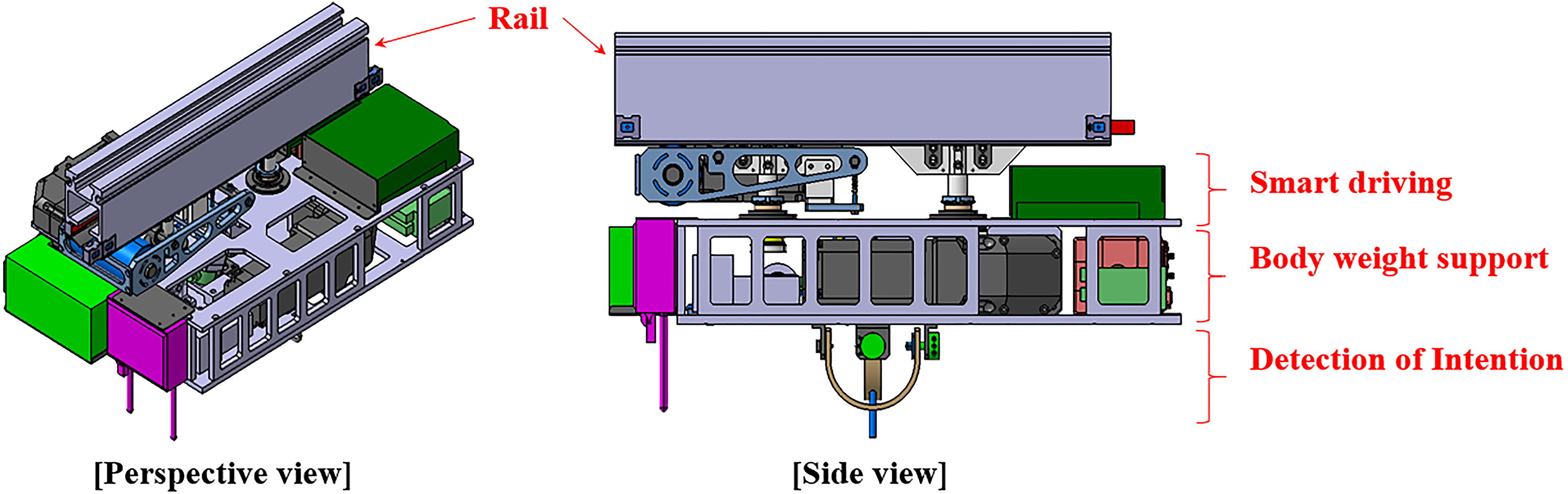
The rail-type rehabilitative training system is a rehabilitation equipment for rail-based gait and postural balance training, and it consists of the rail installed on the indoor ceiling, a trolley that provides the smart driving and weight support functions for rehabilitative training, and a harness that the patient wears. In this rehabilitative training system, a smart driving function helps in posterior-anterior driving, and the body-weight support that controls the weight support level is connected to the patient wearing the harness with a rope [22, 23]. Figure 1 is a 3D design drawing of a gait rehabilitative system that provides smart driving and body weight support. The overall dimensions are 610 mm long, 385 mm wide and 100.5 mm high. Owing to the low indoor ceilings in Korean hospitals, the height was reduced to 100.5 mm, an
Figure 1.
Design concept of the gait rehabilitation system.
2.2Design of the user intention detection function and test mock-up fabrication
The technique of detecting the movement of a patient in advance plays an important role in the main motor control of the rehabilitative training system. In particular, patients with gait disorders with weakened lower extremities function use an exoskeleton robot and a rehabilitative system with body weight support to perform task-oriented training of activities of daily living such as gait motion, sitting-standing motion, and climbing stairs. In this case, motor control of the rehabilitative system that exactly matches the user’s motion can enhance the effect of rehabilitation of the lower extremities of the patient. The ceiling rail-based rehabilitative training system enables customized weight support according to the degree of the gait disorder of the patient, which allows the patient to undergo easier rehabilitation training and prevent secondary risks such as falls. The patient is wired to the ceiling rail-based rehabilitative training system to receive body weight support. It is important to accurately predict the direction of the movement of the user for the patient to receive accurate body weight support from the training system.
Therefore, in this paper, we designed a mechanical part to detect the intention of the user’s movement direction. The gait rehabilitative training system in Fig. 1 is connected to the patient’s harness via a rope in the lower part. As the patient moves, the direction of the rope changes, thus enabling accurate measurement of the movement of the patient. Step motor (FASTECH, Korea) and load cell (CASKOREA, Korea) are used as control the length of wire. Figure 2 shows the potentiometer (Copal Electronics, Japan), which can measure two directions of movement – anterior-posterior and medio-lateral – of the wire connected to the patient, wire guide frame jig for the accurate measurement of change in the potentiometer according to the movement direction of the wire. In particular, the u-shaped wire guide frame jig is designed to move the wire smoothly even when moving at 45
3.Method
3.1Simulation method for user movement direction prediction algorithm
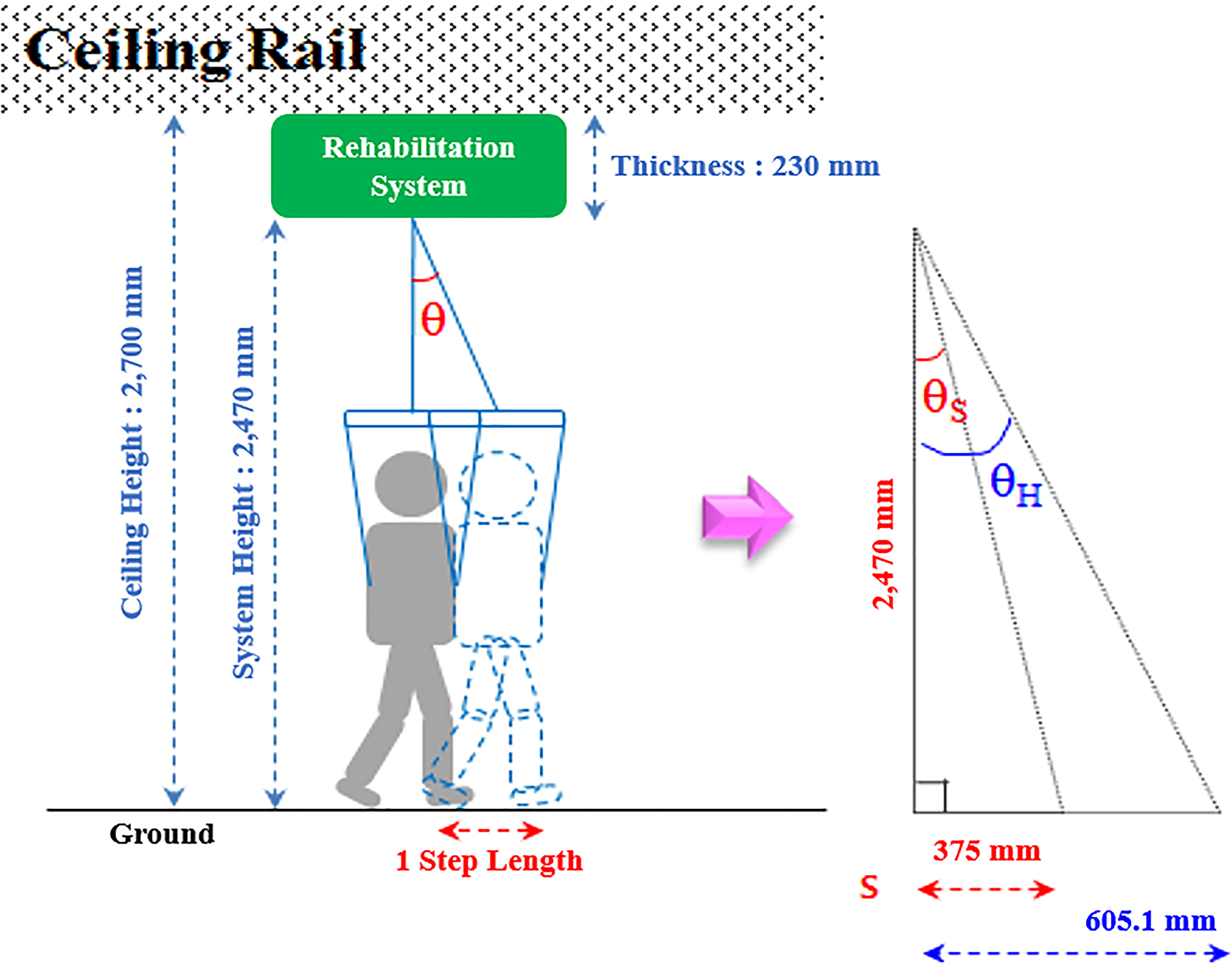
The parameter related to the movement direction of the wire connected to the ceiling rail-based gait rehabilitative training system is the movement angle for each direction of the wire. The movement of wires in each direction based on the movement of the patient creates a certain angle with the direction of gravity. In this regard, we analyzed step lengths of healthy adults, the elderly, and patients with hemiplegia. The examined step length values are shown in Table 1 [24, 25]. The average step lengths of the healthy adults, the elderly, and patients with hemiplegia were 605.1 mm, 590 mm, and 375 nm, respectively. Considering the installation height of the gait rehabilitative training system, as shown in Fig. 3, the movement angles of the wires to the direction of gravity per step of healthy adults, the elderly, and the patients with hemiplegia show wire movement angles of 13.8
Table 1
Comparison of gait stride between the healthy adults, the elderly and stroke patients using a cane [24, 25]
| Subject | Height (mm) | Step length (mm) | Angle ( |
|---|---|---|---|
| Healthy (20 | 2,470 | 605.1 | 13.8 |
| Elderly (60 | 2,470 | 590 | 13.4 |
| Stroke with cane | 2,470 | 375 | 8.6 |
| Test bed | |||
| Simulated elderly | 400 | 100 | 14.0 |
| Simulated stroke step | 400 | 50 | 7.1 |
Figure 2.
Design of motion detection part using two potentiometers.
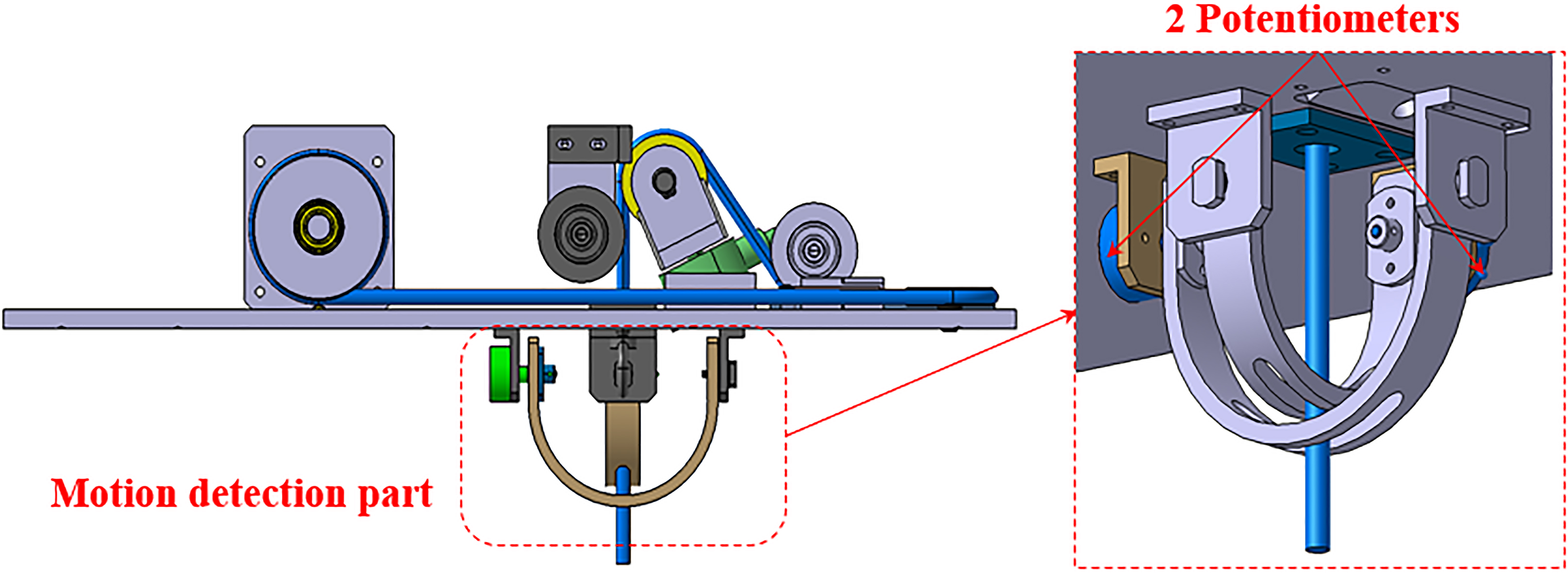
Figure 3.
Wire angle simulation according to the gait motion.
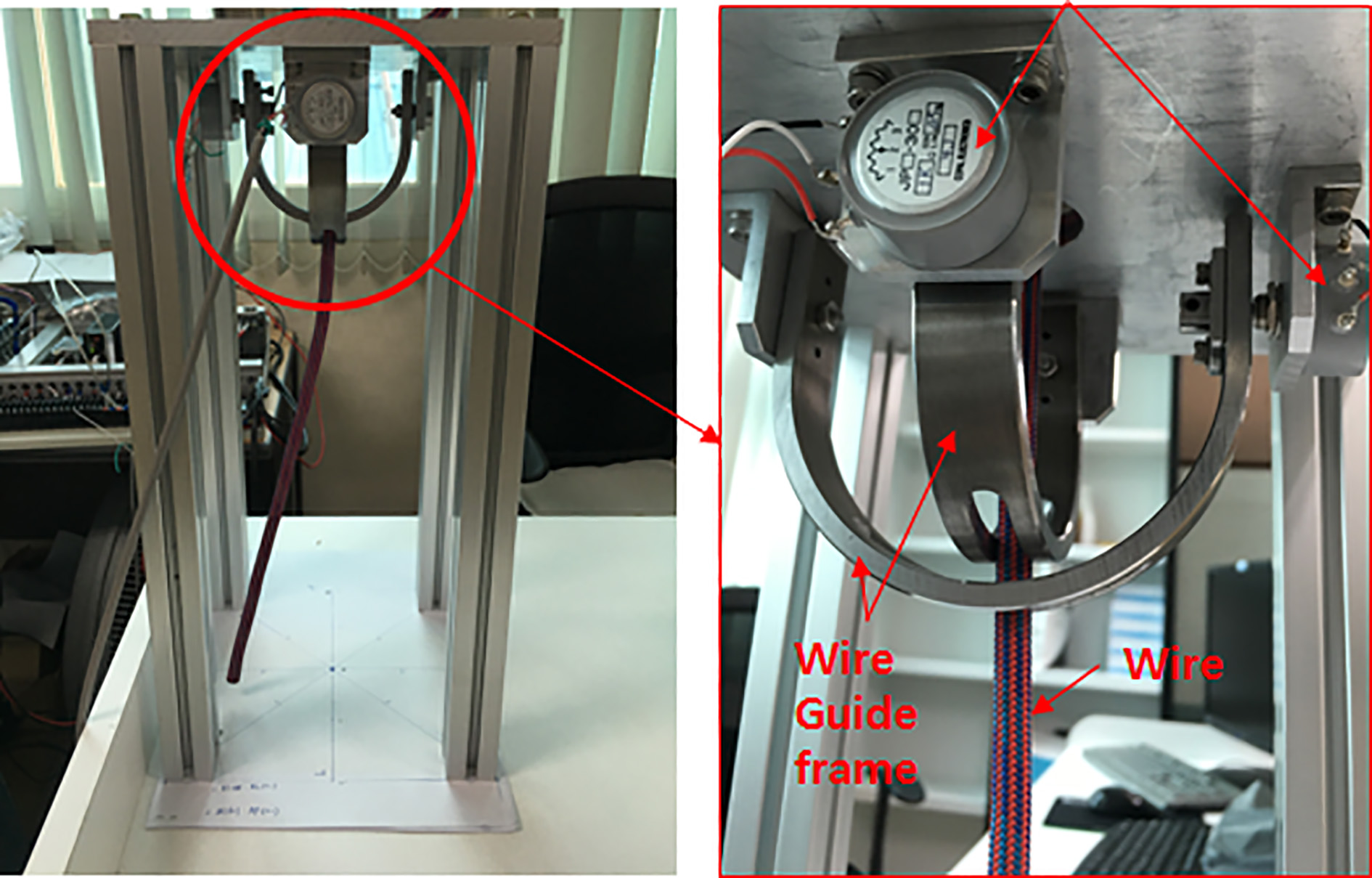
Based on these analyses, to test the similar angles to the gravitational direction according to the movement of healthy adults, the elderly, and patients with hemiplegia, a test mock up (dimensions: 400 mm, height; 100 mm each, width and length) was fabricated as shown in Fig. 4. The intended movement detection mechanism installed in this mock-up showed similar movement for healthy adults and the elderly with the wire angle to the gravity direction changing to 14
Figure 4.
Test mock-up using two potentiometers.
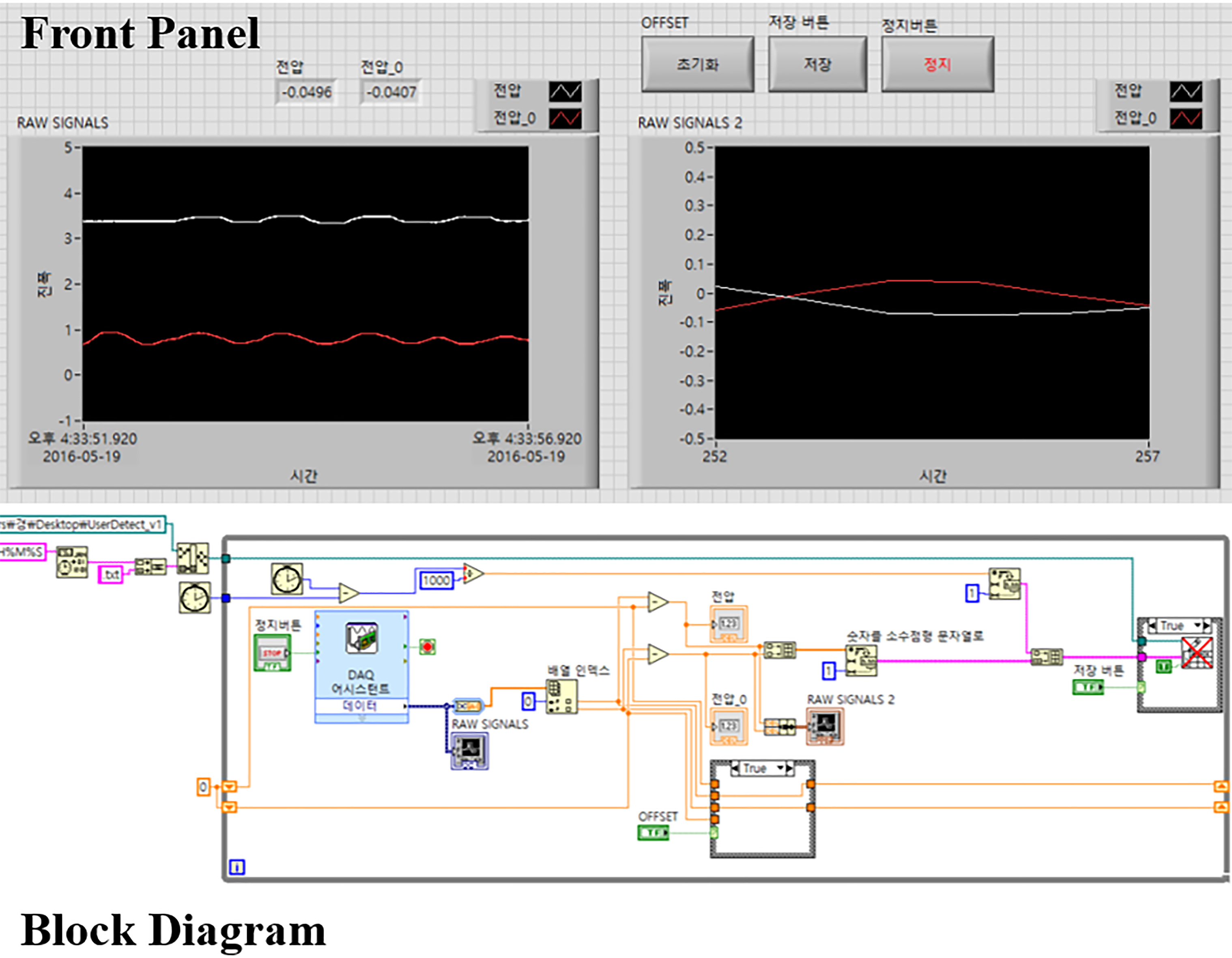
In order to verify the function of the developed user intention detection in Fig. 4, a test mock-up was fabricated as shown in Table 1. The values of the two potentiometers as the wire direction of the test mock-up changed were collected using a LabVIEW program. Figure 5 shows the front panel of the LabVIEW program and the program source for the block diagram.
Figure 5.
LabVIEW program for data acquisition.
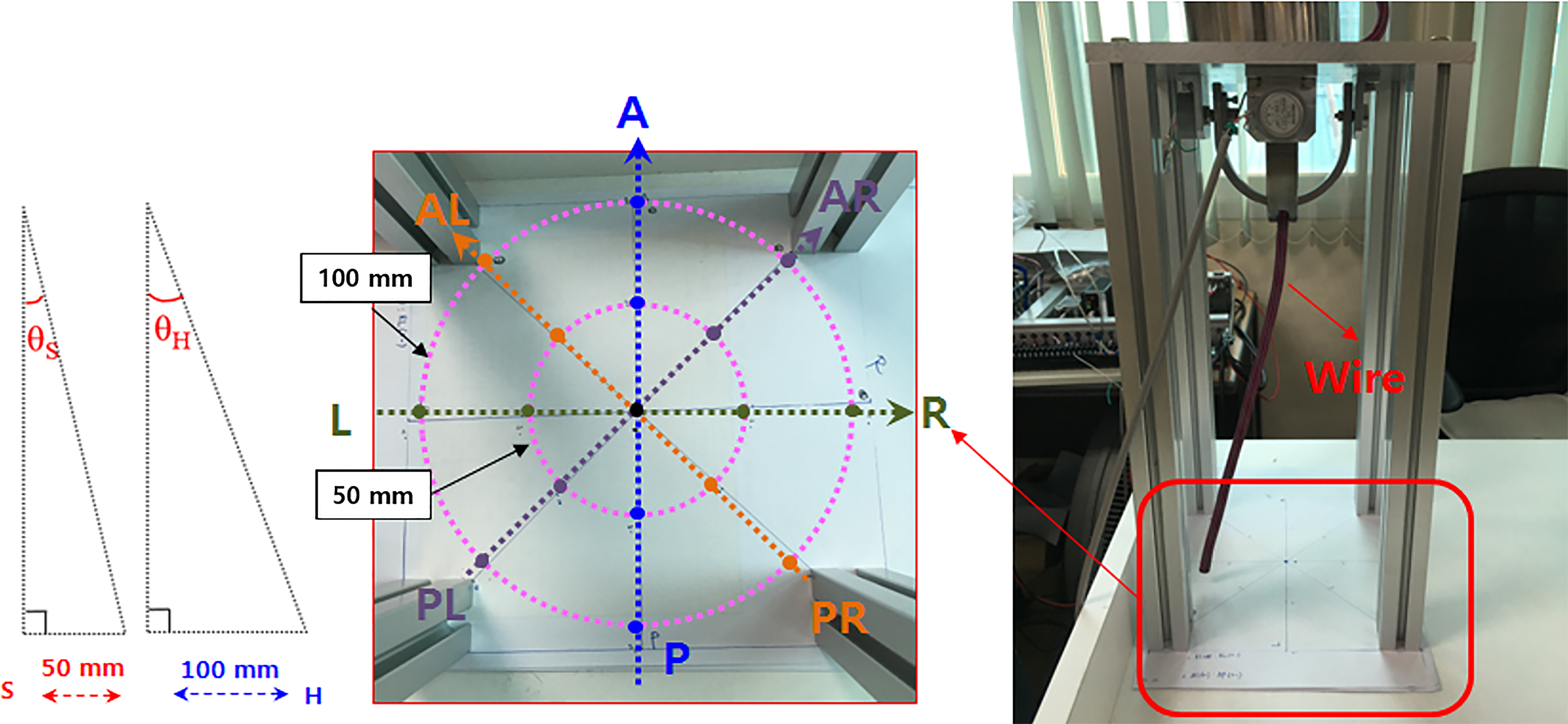
For accurate wire movement detection, at the bottom of the test mock up, as shown in Fig. 6, the imaginary lines that mark the exact points at 50 mm and 100 mm were checked according to the eight directions: anterior (Anterior, A), posterior (Posterior, P), right (Right, R), left (Left, L), anterior-left (Anterior-left, AL), anterior-right (Anterior-right, AR), posterior-left (PL), and posterior-right (PR). For the movement direction prediction algorithm, values of two potentiometers were measured when the wire connected to the test mock up performed pendular movements of 50 mm and 100 mm in the four directions (AP, LR, AL-PR, and AR-PL).
Figure 6.
Virtual line for accurate movement of the wire.
4.Results and discussion
When the wires of the test mock-up were moved in eight directions, the values of the two potentiometers of anterior-posterior (
Figure 7.
Results of two potentiometers according to eight directions.
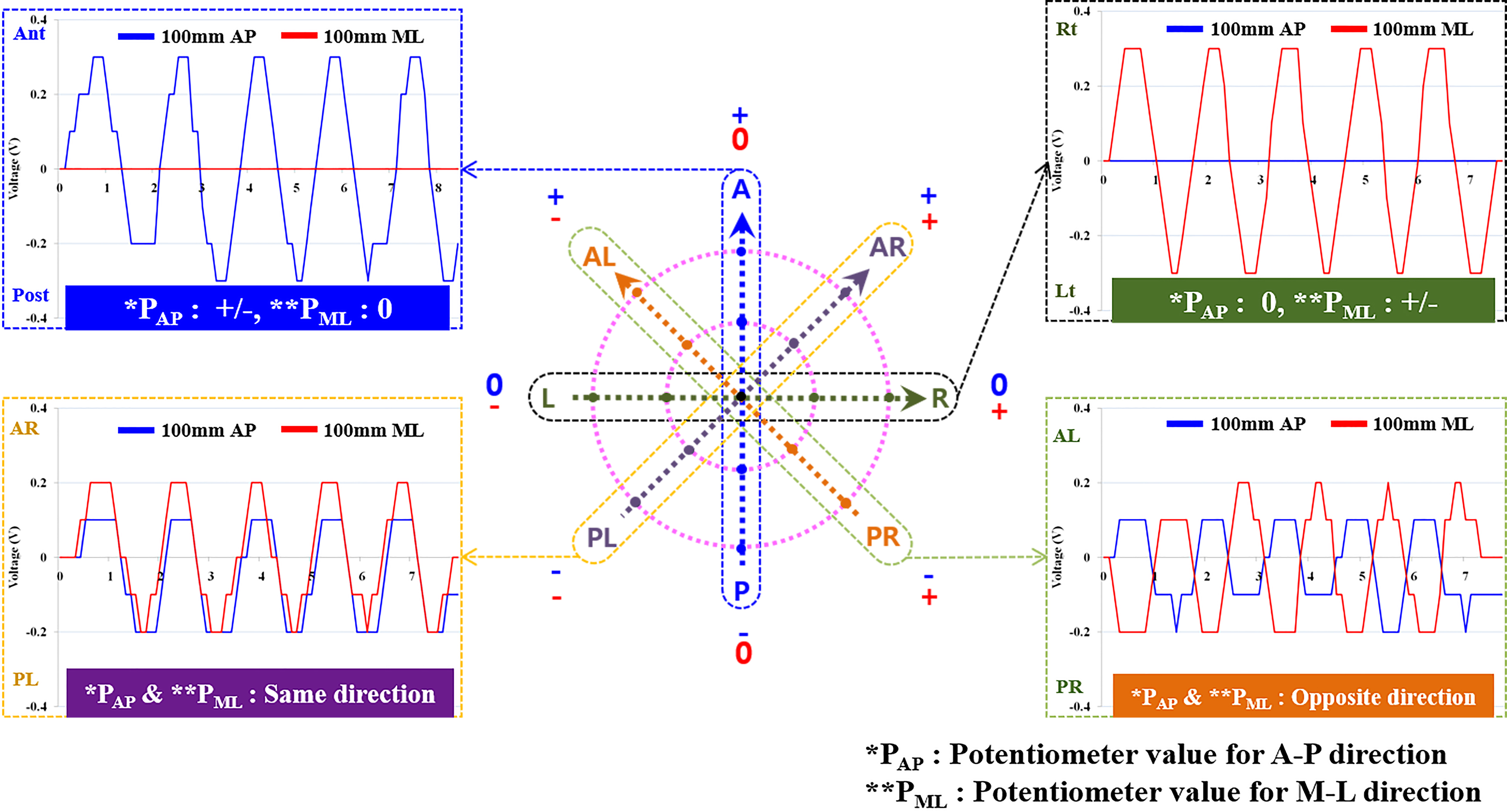
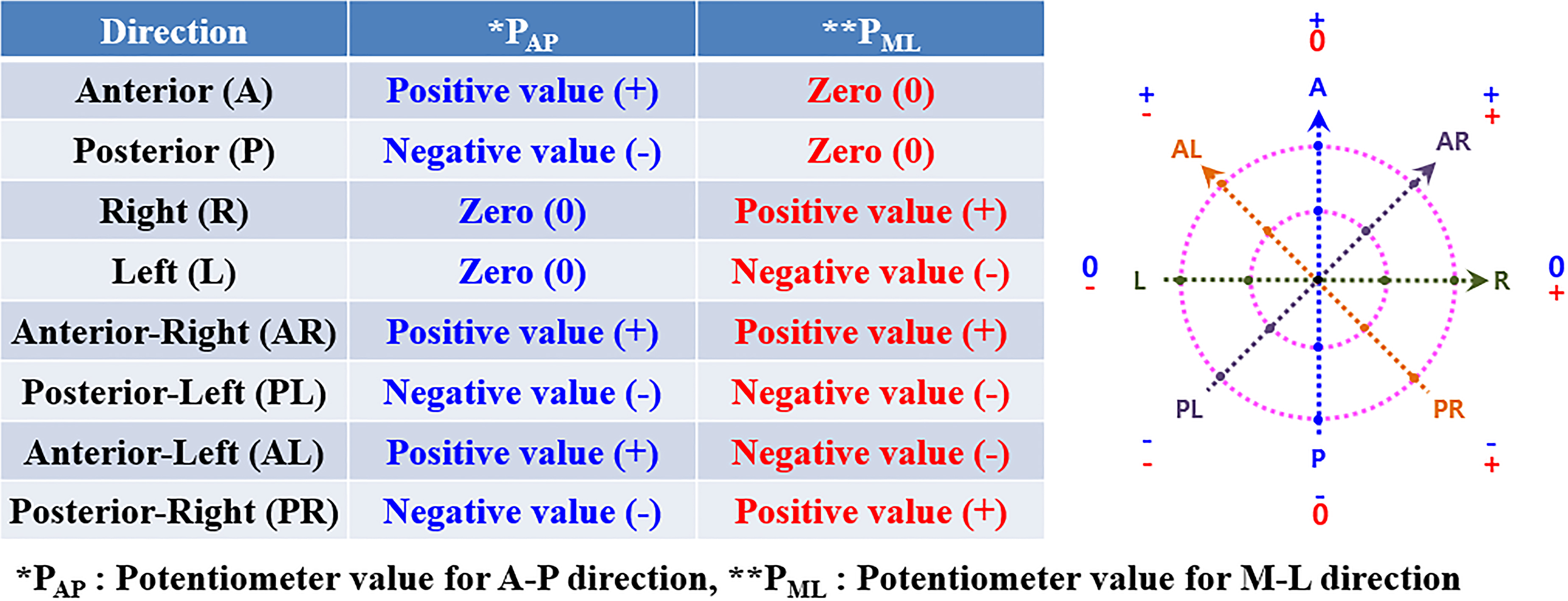
Using the results of the two potentiometers with the wire’s movement in eight directions, an algorithm to predict the user’s intention of the movement direction was developed, as shown in Fig. 8. For easier understanding, the right eight directions in Fig. 8 are shown using two potentiometer values. On the other hand, the amplitudes of the angle measurement of the potentiometer for distinguishing 50 mm and 100 mm tended to be inconsistent, but the combination of (
Figure 8.
Prediction algorithm for the movement intention of the patient using the results of two potentiometers.
The driving motor control test of the gait rehabilitative training system based on the ceiling rail was directly performed using the user movement direction prediction algorithm developed in this paper. As a result, the trolley of the gait rehabilitative training system moved to the anterior direction when the wire moved in A, AL, and AR directions, and the trolley moved to the posterior direction when the wire moved in the P, PL, and PR directions. When the wire moved to only the left and right, we checked that the trolley did not move from its place to prevent possible falls.
This movement direction prediction algorithm can be used for rehabilitation training that performs activities related to actual lower extremity movements in daily living. As shown in Fig. 9, it was confirmed that the trolley of the gait rehabilitative training system moved along with the user using the driving motor according to the user’s movement direction. When the user performs dynamic movement training such as gait movement, the user moves in the anterior direction. In accordance with the user’s gait speed, the trolley served as a movement aid in the user’s posterior side and performed body weight support functions.
Figure 9.
Apparatus of the gait and sitting motion using the motion detection function of the rehabilitation training system.
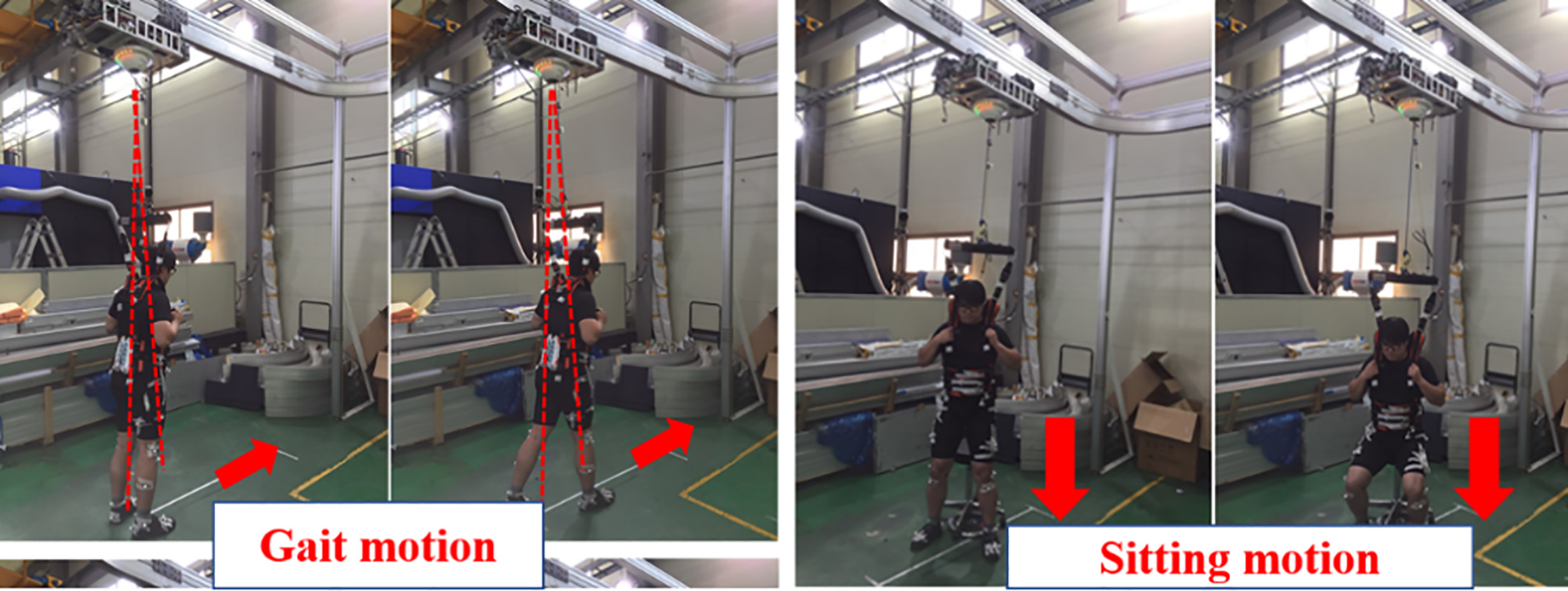
Furthermore, the sitting-standing motion was performed at one place where the chair is located; however, the user’s center of gravity moves back and forth slightly according to the sitting-standing motion. At this time, the trolley will move slightly in the A and P directions for safe body weight support as the angle of the wire changes. In this way, the safety of this system was confirmed during the movement test in healthy adults before experimenting with elderly people and hemiplegia patients. In future research, we plan to test the algorithm for predicting user’s movement direction in elderly, and patients with hemiplegia.
5.Conclusion
This paper investigated the user’s movement intention detection to operate the ceiling rail-based rehabilitative training system with precise timing. A simple test mock up with two potentiometers was fabricated, and the experiments were conducted to determine the change in measured values of the potentiometers based on the movement direction; eight directions including anterior, posterior, left and right movements, were considered. We were able to predict the user movement intention for eight directions according to the combination of “positive value, 0, and negative value” using the measured values of the two potentiometers.
The direction measurement algorithm developed in this paper was used to control the driving motor of the rail-based gait rehabilitative training system, and it was confirmed that it was effectively used to control the driving function to assist the gait, sitting-standing, and climbing up-down stairs motions in daily life. The user’s movement intention detect function developed in this paper is expected to be effectively used to control the training system for rehabilitation of patients with hemiplegia to improve their gait motion and posture balance, which will help enhance their quality of life.
However, the potentiometer sensor used in this paper was not accurate enough to directly distinguish the difference in the angle to the gravity direction coming from the difference in step length between patients with hemiplegia and healthy adults. In future research, we plan to use high-precision angle sensors such as encoders that can distinguish the angle change of wires according to the movement of the hemiplegia patients.
Acknowledgments
This study was supported by a grant of the Translational Research Center for Rehabilitation Robots, Korea National Rehabilitation Center, Ministry of Health & Welfare, Korea (no. NRCTR-EX16005), and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (no. 2018R1D1A3B07049251).
Conflict of interest
None to report.
References
[1] | Perry J, Thorofare S, Jon D. Gait Analysis: Normal and pathological function. Journal of Pediatric Orthopaedics. (1992) ; 12: (6): 815. |
[2] | U.S. Department of Health and Human Services. Vital and Health Statistics 2. Centers for Disease Control and Prevention and Nation Center for Health Statistics. (2010) ; 152. |
[3] | HelpAge. Global AgeWatch index 2014. |
[4] | Chae SY, An NY. A study of the psychosocial impact on use of assistive technology devices of spinal cord Injury patients. Journal of Special Education & Rehabilitation Science. (2012) ; 51: (2): 179-196. |
[5] | Lee DY, Rhee KM, Lee DY, Lee SC, Lee SW, Lim MJ, Kim KM. A study on the conceptual design of cars accessible for persons with disabilities. The Journal of Special Education: Theory and Practice. (2004) ; 5: (3): 139-159. |
[6] | Kolakowsky-Hayner SA, et al. Safety and Feasibility of using the EksoTM bionic exoskeleton to aid ambulation after spinal cord injury. Journal of Spine. (2013) ; S4: : 3. doi: 10.4172/2165-7939.S4-003. |
[7] | Colombo G, et al. Treadmill training ofparaplegic patients using a robotic orthosis. Journal of Rehabilitation Research & Development, (2000) ; 37: : 693-700. |
[8] | Hesse S, Bertellt C, Schaffrin A, Malezic M, Mauritz KH. Restoration of gait in nonambulatory hemiparetic patients by treadmill training with partial body-weight support. Arch Phys Med Rehabil. (1994) ; 75: : 1087-1093. |
[9] | Hesse S, Bertelt C, Jahnke MT, Schaffrin A, Baake P, Malezic M, Mauritz KH. Treadmill training with partial body weight support compared with phyiotherapy in nonambulatory hemiparetic patients. Stroke. (1995) ; 26: : 976-981. |
[10] | Werner C, Frankenberg SV, Treig T, Konrad M, Hesse S. Treadmill Training with partial body weight support and an electromechanical gait trainer for restoration of gait in subacute stroke patients a randomized crossover study. Stroke. (2002) ; 33: : 2895-2901. |
[11] | Jung JY, Park HS, Lee DY, Jang IH, Lee DW, Lee HG. Organization of Sensor system and user’s intent detection algorithm for rehabilitation robot. Journal of Institute of Control. Robotics and Systems. (2010) ; 16: (10): 933-938. |
[12] | Alton F, Baldey L, Caplan S, Morrissey MC. A kinematic comparison of overground and treadmill walking. Clinical Biomechanics. (1998) ; 13: (6): 434-440. |
[13] | Riley PO, Paolini G, Croce UD, Paylo KW, Kerrigan DC. A kinematic and kinetic comparison of overground and treadmill walking in healthy subjects. Gait & Posture. (2007) ; 26: : 17-24. |
[14] | Lee SJ, Hidler J. Biomechanics of overground vs. treadmill walking in healthy individuals. J Appl Physiol. (2008) ; 104: : 747-755. |
[15] | Hesse S, Konrad M, Uhlenbrock D. Treadmill walking with partial body weight support versus floor walking in hemiparetic subjects. Arch Phys Med Rehabil. (1999) ; 80: (4): 421-427. |
[16] | Dobkin B, Apple D, Barbeau H, Basso M, Behrman A, Degorge D, Ditunno J, Dudley G, Elashoff R, Fugate L, Harkema S, Saulino M, Scott M. Weight-supported treadmill vs over-ground training for walking after acute incomplete SCI. Neurology. (2006) ; 66: (4): 484-493. |
[17] | Miller EW, Quinn ME, Seddon PG. Body weight support treadmill and overground ambulation training for two patients with chronic disability secondary to stroke. Phys Ther. (2002) ; 82: : 53-61. |
[18] | Hidler J, Brennan D, Black I, Nichols D, Brady K, Nef T, Zero G. Overground gait and balance training system. Journal of Rehabilitation Research & Development. (2011) ; 48: (4): 287-298. |
[19] | Fenuta AM, Hicks AL. Muscle activation during body weight-supported locomotion while the ZeroG. Journal of Rehabilitation Research & Development. (2014) ; 51: (1): 51-58. |
[20] | Fenuta AM, Hicks AL. Metabolic demand and muscle activation during different forms of bodyweight supported locomotion in men with incomplete SCI. BioMed Research International. (2014) ; 2014: : 632765. doi: 10.1155/2014/632765.. |
[21] | Park MJ, Kim JY. Development of intelligent walking assistive robot using stereo cameras. Trans Korean Soc Mech Eng A. (2014) ; 38: (8): 837-848. |
[22] | Kim K, Song WK, Chong WS, Yu CH. Structural analysis of a rehabilitative training system based on a ceiling rail for safety of hemiplegia patients. Technology and Health Care. (2018) ; 26: (S1): 259-268. |
[23] | Song SM, Heo M, Yu CH, Kim K, Kwon TK. Analysis of planter pressure and muscular strength of daily activities with change of weight support. International Journal of Precision Engineering and Manufacturing. (2018) ; 19: (8): 1219-1224. |
[24] | Oberg T, Karsznia A, Oberg K. Basic gait parameter: Reference data for normal subjects, 10–79 years of age. J of Rehabilitation Research and Development. (1993) ; 30: (2): 210-223. |
[25] | Chen CL, Chen HC, Wong MK, Tang FT, Chen RS. Temporal stride and force analysis of cane-assisted gait in people with hemiplegic stroke. Arch Phys Med Rehabil. (2000) ; 81: : 43-48. |


