
Terminology and ontology development for semantic annotation: A use case on sepsis and adverse events
Abstract
Annotations enrich text corpora and provide necessary labels for natural language processing studies. To reason and infer underlying implicit knowledge captured by labels, an ontology is needed to provide a semantically annotated corpus with structured domain knowledge. Utilizing a corpus of adverse event documents annotated for sepsis-related signs and symptoms as a use case, this paper details how a terminology and corresponding ontology were developed. The Annotated Adverse Event NOte TErminology (AAENOTE) represents annotated documents and assists annotators in annotating text. In contrast, the complementary Catheter Infection Indications Ontology (CIIO) is intended for clinician use and captures domain knowledge needed to reason and infer implicit information from data. The approach taken makes ontology development understandable and accessible to domain experts without formal ontology training.
1.Introduction
Many natural language processing (NLP) studies rely on annotated corpora to create models for text classification, information extraction, named entity recognition, question answering, summarization, and text generation. Often, semantic annotation is done to capture domain knowledge within the text. Annotated corpora are frequently generated by annotators based on an annotation guideline, which provides the standard and rules for how to label text using specified terms. This annotation guideline is usually similar to a terminology, unless the corpus was annotated using an ontology. To further enrich an annotated corpus by capturing, reasoning, and inferring the underlying associated domain knowledge, an ontology is needed.
To demonstrate semantic annotation terminology and ontology development, the use case is based on clinician-presented needs for identifying sepsis from adverse events (AEs). Improperly cared for peripheral intravenous catheter (PIVC) medical devices can lead to unwanted and unintentional events that harm patients, such as AEs like phlebitis, bloodstream infections (BSIs), and sepsis. However, PIVCs are poorly documented in clinical records because of routine use among inpatients, and sepsis is also poorly documented outside the intensive care units (ICUs). The lack of explicitly documented concepts makes it challenging to directly detect and annotate PIVC-related phlebitis, BSI, and sepsis for quality surveillance to improve care. Thus, indications for the presence of PIVCs, phlebitis, infections, and sepsis are annotated instead. Those annotations are structurally preserved as a terminology, and the clinical knowledge required to reason about the indications is represented in an ontology. Additional details for the use case are provided in Section 2.
This paper provides a detailed and concrete description of the methodology utilized for ontology development of an annotated corpus based on a use case from the clinical domain. The main contributions presented are:
1. Describing the development process for constructing a terminology that can represent an annotated corpus. Specifically, a terminology for indexing annotated AE documents.
2. Presenting the development process for the terminology’s corresponding ontology, which represents domain knowledge and allows inference of implicit knowledge in a specific domain. The corresponding ontology in the use case represents clinical domain knowledge specifically for annotated catheter-related and infection-related signs in AE documents.
3. Releasing a terminology and ontology that can be applicable to identifying and reasoning about sepsis in an AE corpus.
Based on the presented use case in Section 2 and objective in Section 2.2, an Annotated Adverse Event NOte TErminology (AAENOTE) and corresponding Catheter Infection Indications Ontology (CIIO) were developed. Section 5 details the terminology construction and development process to represent annotated documents, and Section 6 presents the results and evaluations for the AAENOTE. To address shortcomings in the terminology for annotated documents, Section 7 describes the ontology development process for domain knowledge representation of documented content. Additionally, Section 8 presents the results and evaluations for the CIIO. Finally, Section 9 discusses the findings, limitations, representations, accessibility, and utility.
2.Use case background and motivation
2.1.Sepsis from peripheral intravenous catheter-related phlebitis and infection adverse events
As the most commonly used medical device in hospitals, PIVCs are inserted into the peripheral vein to administer intravenous (IV) fluids, IV medications, and blood transfusions [1]. Improper management of PIVCs or the infusions connected to the PIVC can lead to phlebitis, which is either infectious, mechanical, or chemical inflammation of the vein [12,23,47]. Independent of cause, all PIVC phlebitis share many symptoms like redness and swelling near a patient’s infusion insertion site for infectious, mechanical, or chemical phlebitis, making it difficult to distinguish. Furthermore, all PIVC-related phlebitis causes AEs like significant pain, PIVC failure that delays treatment, and compromises future venous access. Infectious phlebitis may lead to BSI due to: 1. migration of bacteria at the insertion site, 2. bacteria migrating through the catheter tract or catheter hub, 3. contaminated infusate, or 4. bacteria from an existing infection in the bloodstream attaching to the catheter [69]. BSIs can potentially cause sepsis and occur when bacteria enter the bloodstream [26]. Staphylococcus aureus (S. aureus) is a lethal bacteria frequently found on skin that commonly causes BSIs [41], defined as a dysregulated host immune response to infection that results in organ failure and a mortality rate of 20% [53]. Approximately 7.6% to 35% of S. aureus BSIs are caused by PIVCs [32].
Even though PIVCs are frequently used, they are routinely not documented in clinical records [1]. Moreover, sepsis is also poorly documented outside the ICUs [49]. This lack of documentation makes it challenging to perform retrospective and real-time systematic quality surveillance of PIVC-related phlebitis or BSIs to identify learning opportunities for improving PIVC care to lower phlebitis-related, BSI-related, and PIVC-related AE incidents. Hence, AE reports or documents, which are customarily used to report PIVC failures, were selected as the clinical text for this project. To capture documented observable patient states and infer underlying knowledge of PIVC-related phlebitis or BSI from clinical text, an ontology that models clinical knowledge representation and reasoning is necessary.
2.2.Use case objective
The use case objective was to develop a model for representing and reasoning about PIVC-related BSIs in the unstructured free-text of AE reports, describe the development process, and discuss the discoveries and limitations. From the research question “is there a connection between BSIs and PIVCs at the hospital?”, competency question requirements for an ontology representing and reasoning about PIVC-related BSIs were identified by clinicians as follows:
1. Does patientA have phlebitis, and was it infectious, chemical, or mechanical phlebitis?
2. Does patientA have an infection?
3. Does patientA have a BSI?
4. How many patients have an infection or BSI?
5. Which patients have sepsis?
6. Does patientB have a catheter?
7. Does patientB have a PIVC?
8. How many catheters does patientB have, where are they, and why does patientB need them?
9. Does patientC have an infection and catheter? If so, was patientC’s infection associated with a catheter?
3.Related work
3.1.Annotation, tagging, and ontologies for natural language processing
Many studies focus on the relationship between annotation, tagging, and ontologies for NLP development. These studies include annotating corpora, NLP extraction, and classification tasks. Below are some studies that have shared their findings, issues, and possible solutions.
Annotated using the Uberon multi-species anatomical ontology [34], the Colorado Richly Annotated Full-Text (CRAFT) Corpus is a resource for NLP development which is also semantically annotated with concepts from eight Open Biomedical Ontologies (OBO) and terminologies [4,6]. However, while annotating with the OBOs, they discovered that the OBOs are not developed for annotation because there are overlapping terms within the different OBOs, context-specific definitions, and semantic ambiguities. Additionally, some OBOs do not follow the OBO Foundry principle of using relations from the OBO Relation Ontology (RO) [57] to link concepts [5]. Therefore, to improve OBOs for semantic annotation of biomedical documents, the researchers proposed desirable ontology implementations such as, but not limited to, integrating overlapping OBOs terms, resolving ontology-specific ambiguities, and expanding relations [5].
A study comparing how anatomy ontologies are used for annotations discovered annotation and ontology issues [61]. Annotations from three public datasets were compared to anatomical terms in the Foundational Model of Anatomy (FMA) [50,51] and Uberon [34] ontologies using the Zooma and Ontology Mapper software tools. Manual and semi-automated preprocessing were done to normalize terms, but there were few matches between the ontologies and annotations, mainly because of strict matching. Additionally, the user-provided annotation labels resulted in mismatches, such as annotating a phrase with multiple ontology terms or using an abbreviation or adjective for an anatomical part instead of the anatomical ontology term. Ontology issues include missing anatomical synonyms used by the annotators and differing anatomical terms in the ontologies because the ontologies are designed for different purposes and made by different design decisions. The study concluded that mapping terms to an ontology requires a large amount of time, effort, and manual curation. Furthermore, an ontology’s design decisions and scope will affect users trying to match annotations to an ontology, and ontologies must be used to understand their potential.
The Unified Medical Language System (UMLS) is a collection of standard biomedical terminology [8], and it has been used to process text by extracting concepts, relations, and knowledge (i.e., link or annotate text with standard terminology) [2]. A software capable of finding and linking biomedical text to terminology concepts in the UMLS Metathesaurus is MetaMap [3]. However, the developers of MetaMap mention that improvement is required for detecting similar names, acronyms, and abbreviations and resolving ambiguities by possibly distinguishing concepts using word sense disambiguation.
In [37], an overview of studies using knowledge bases for entity coreference resolution were discussed. Among those studies was the OntoNotes project, which annotated a multilingual corpus for different levels of semantic structure in the text [25,44,45]. One of the annotation levels includes linking OntoNotes word senses to the Omega ontology [25,46,68]. Near-synonymous word sense pools were created by specialists who grouped sense distinctions from WordNet and dictionaries based on similar definitions. This enables machines to automatically tag senses more accurately and improves inter-annotator agreement due to difficulties determining WordNet distinctions directly in the text [68]. Before each sense pool was linked to a concept in the Omega ontology [42], each sense pool was verified by machine and humans [68].
3.2.Ontology development methods and evaluation
There are many ontology development methods, such as: the Enterprise ontology’s Uschold and King [62], the TOronto Virtual Enterprise (TOVE) ontology’s Grüninger and Fox [20], METHONTOLOGY [14], the On-To-Knowledge Methodology (OTKM) [60], and NeOn [59]. Of those methods, Uschold and King [62] and Grüninger and Fox [20] follow a sequential sequence of phases, whereas METHONTOLOGY [14], OTKM [60], and NeOn [59] are iterative. Whether sequential or iterative, the previously mentioned methods and 2 reviews [10,43] have shown that ontology development typically includes the phases: specification, conceptualization, formalization, implementation, and maintenance. During those phases, the knowledge acquisition, evaluation, and documentation phases also commonly occur either as a separate phase or concurrently with other phases. Appendix A provides a summary of the methods for each phase.
During and between phases, ontology evaluation judges an ontology’s content to a reference, such as requirement specifications, competency questions [20], or the real-world [18,19]. Evaluation includes: (1) verification that the ontology has the correct informal natural language definition and formal ontology language definition, and (2) validation that the ontology represents the world it was created for [18,19]. In theory, there are many criteria for evaluation, but in practice, most studies only use the expressiveness and practical usefulness criteria [11]. Expressiveness is the number of competency questions answerable by the ontology [11,20,38], and practical usefulness is the number of problems an ontology can be applied to [11,38].
3.3.Relevant ontology resources
Table 1
Overview of relevant resources for this study
| Type | Resource | Relevant Concepts or Terms |
| Ontology | Infectious Disease Ontology (IDO) | Sepsis and hospital-acquired infection entities |
| Ontology for General Medical Science (OGMS) | Sign and symptom entities | |
| Vital Sign Ontology (VSO) | Vital sign entities | |
| Foundational Model of Anatomy Ontology (FMA) | Anatomical entities | |
| Biological Spatial Ontology (BSPO) | Anatomical spatial location descriptor entities | |
| Ontology of Adverse Events (OAE) | Adverse event entities | |
| Open Biological and Biomedical Ontology (OBO) Relation Ontology | Relationship object properties | |
| Terminology | National Cancer Institute Thesaurus (NCIT) terminology | Procedure and medical device terms |
| International Classification for Nursing Practice (ICNP) terminology | Terms | |
| Taxonomy | Nursing Interventions Classification (NIC) taxonomy | Terms |
| NANDA International Nursing Diagnoses Classification taxonomy | Terms | |
| Clinical Guideline | 1998 Visual Infusion Phlebitis Scale | Visual infusion phlebitis grading scale |
| 2021 Infusion Therapy Standards of Practice Updates | Updated infusion therapy practice standards |
There lacks an ontology specifically for sepsis-related BSI, infection signs, anatomical locations, medical devices, and procedures. However, pre-existing ontologies can contain relevant concepts. For example, the Infectious Disease Ontology (IDO) [27] has sepsis and hospital-acquired infection entities. Sign and symptom entities are present in the Ontology for General Medical Science (OGMS) [39], and vital sign entities exist in the Vital Sign Ontology (VSO) [17,64]. Anatomical locations can be described using anatomical entities of the Foundational Model of Anatomy Ontology (FMA) [15,51] and anatomical spatial location descriptor entities from the Biological Spatial Ontology (BSPO) [7]. Because AE reports are used, the adverse event entities in the Ontology of Adverse Events (OAE) [21,40] might also be relevant. Furthermore, relationship object properties in the Open Biological and Biomedical Ontology (OBO) Relation Ontology [48,57] could be used to link different entities together to capture more information.
In addition to ontologies, there are also potential relevant terminologies and taxonomies. For example, there are different procedure, medical device, and catheter terms in the National Cancer Institute Thesaurus (NCIT) [35,36]. Potential relevant standardized nursing practice language is found in the International Classification for Nursing Practice (ICNP) terminology [13], Nursing Interventions Classification (NIC) taxonomy [9], and NANDA International Nursing Diagnoses Classification taxonomy [22]. Furthermore, infusion phlebitis-related information can be obtained from the 1998 Visual Infusion Phlebitis Scale [30] and the 2021 Infusion Therapy Standards of Practice Updates [28]. Concepts or terms from these resources can be used to expand the ontology if deemed necessary by ontology users. The relevant ontologies, terminologies, taxonomies, and clinical guidelines can be found in Table 1.
4.Materials
4.1.Synthetic dataset
Documents for annotation are from an AE synthetic dataset. The documents are based on unstructured free-text AE notes within the extracted AE reports from the electronic incident reporting system at St. Olavs hospital, Trondheim University Hospital in Trondheim, Norway, between September 2015 to December 2019 [67]. The synthetic dataset contains 100 AE notes or documents manually created and verified by a nurse to ensure clinical data is anonymized. The Norwegian Regional Committees for Medical and Health Research Ethics (REK) has granted ethical approval to use AEs in this paper (approval no 2018/1201/REKmidt, 26814).
4.2.Annotated synthetic dataset
The synthetic documents were annotated by 8 annotators with clinical backgrounds over 4 annotation sessions [67]. Each annotator annotated 10 documents in session 1 and 20 documents in the remaining 3 sessions (i.e., 70 documents annotated over 4 annotation session). This resulted in 560 annotated synthetic AE documents, as shown in Fig. 1 (i.e., 8 annotators * 70 annotated documents over 4 sessions = 560 total annotated synthetic AE documents). In each annotation session, annotators followed the annotation guideline and used the Brat rapid annotation tool (BRAT) [58] to annotate the documents. Then, documents were evaluated and manually screened to identify ambiguities for revising the annotation guideline. This process was repeated 3 additional times with a new set of documents and a revised annotation guideline.
Fig. 1.
From unannotated documents to an annotated corpus for populating instances in a terminology. 100 synthetic adverse event (AE) unstructured free-text documents were manually generated. Those synthetic documents were annotated by 8 annotators over 4 annotation sessions using revised annotation guidelines. Each annotator annotated 70 documents (i.e, 10 documents in session 1 and 20 documents in the remaining 3 sessions) to produce a total of 560 annotated synthetic AE documents.

4.3.Annotation guideline
An annotation guideline was developed based on the clinical research question: Is there a connection between BSIs and PIVCs at the hospital? Discussions with nurses provided insight into how catheters can be distinguished explicitly by the name or implicitly based on the anatomical insertion site or procedure mentioned. This formed into four domain-specific questions of interest:
1. What are the different signs of infections, specifically for BSIs, sepsis, or infected PIVCs?
2. What are the signs for different types of catheters?
3. Where are the anatomical insertion sites of catheters?
4. What procedures, interventions, and activities can be related to catheter use?
1. Sign: infection signs.
2. Location: anatomical insertion sites.
3. Device: signs of catheter types.
4. Procedure: procedures, interventions, or activities related to catheters.
5. Sensitivity: protected health information.
6. Person: individuals mentioned, such as patient, clinician, or relative.
7. Whole: label representing the span of the whole document and given to indicate if the document contains information about infection, BSI, sepsis, faulty device malfunctioning, catheter, PIVC, or has sensitive protected health information.
All categories except Whole have a hierarchy with more specific subcategories to capture detailed granularity from text (e.g., the Person category has a Patient subcategory). Furthermore, to capture relationships between categories for downstream analysis (e.g., infection sign at a specific location), the following four relationships to link categories were included:
1. Person
2. Procedure
3. Sign
4. Sign, Device, or Procedure
5.Terminology development for annotations
In annotations, categories are known as entities for labeling a span of words or phrases. Whereas in ontologies and terminologies, categories are known as classes. To separate the annotation guideline from the terminology and ontology, the annotation categories and entities are in bold font, and the terminology and ontology classes are in typewriter font.
5.1.Design decision for annotations
The terminology was developed using the bottom-up approach based on the annotation guideline refinement process from 4 iterations. Competency questions were not used to create this terminology. This terminology is meant to assist annotators who want to label text and allow users interested in performing downstream analyses to adjust the granularity of labels. The objective is solely to represent the annotated corpus and provide structure to the terminology used by annotators. Thus, included individuals are based on concrete examples from the annotated corpus. A simplified example of how annotation labels in annotated documents are added to the terminology as individuals is provided in Fig. 2.
Fig. 2.
Using an annotated corpus to populate individuals in a terminology. Each of the 560 documents were translated into an individual, and each label within a document was also translated into an individual. In the simplified example, an annotated document has 2 patient labels, 2 PIVC labels, and 2

Instead of reusing and re-defining existing ontologies, it was easier and simpler to develop a terminology based on what is documented in the data. For instance, although the FMA contains relevant anatomical parts, the ontology was too complex and detailed to be incorporated easily into the terminology to fit the use case’s purpose. Additionally, the purpose was to include only concrete items documented in the terminology and not provide terminology for all existing items. By opting to simplify the terminology, it was easier to build the terminology directly based on the annotation guideline and then modify the terminology to incorporate feedback from discussions with clinicians.
5.2.Convert annotation guideline to terminology
The categories, attributes, and relationships in annotation guidelines described in Section 4.3 correspond to classes, data properties, and object properties in terminologies (Table 2 and Fig. 3).
Table 2
Convert annotation guideline to terminology
| Annotation Guideline | Terminology |
| Entity (category) hierarchies | Class hierarchies |
| Attributes which provide detailed entity information | Data properties |
| Relationships between entities | Object properties |
Fig. 3.
Terminology development. The annotation guideline from the fourth annotation session was converted into a terminology. Annotation categories were converted into ontology classes, relationships into object properties, and attributes into data properties. Then the individuals of documents and labels were added. Additional modifications were incorporated as needed, such as removing ambiguities, re-organizing hierarchies, and adding missing concepts. This resulted in the AAENOTE which models and provides an index of annotated documents.

The terminology was developed from the annotation guideline by translating each hierarchy of entities into a class hierarchy, using attribute information to add data properties, and converting relationships into object properties. During development, the terminology was modified to remove ambiguities by adding new class hierarchies and modifying class names, object properties, and data properties. Specifically, to remove ambiguity between symptoms, infection signs, and device malfunction signs, the Observation class was introduced to encompass them. Additionally, the Sensitive category was revised to the Identifier class and the
Table 3
Annotation Guideline vs Annotated Adverse Event NOte TErminology (AAENOTE). Annotation categories and entities are in bold font and the terminology and ontology classes are in typewriter font
| Annotation Categories | Category Description | Sub-categories | Terminology Classes | Class Description | Subclasses |
| Sign | Infection signs | 29 | Observation | Documented clinical observation including symptoms, infection signs, and device malfunctions | 41 |
| Location | Anatomical insertion sites | 17 | Anatomical location | Anatomical location | 25 |
| Device | Signs of catheter types | 16 | Medical device | Treatment equipment or part | 19 |
| Procedure | Procedures, interventions, or activities related to catheters | 31 | Procedure | Procedure, intervention, or activity for catheter-related versus non-catheter related | 36 |
| Sensitivity | Protected health information | 14 | Identifier | Protected health information | 14 |
| Person | Individuals | 3 | Person | Individual | 3 |
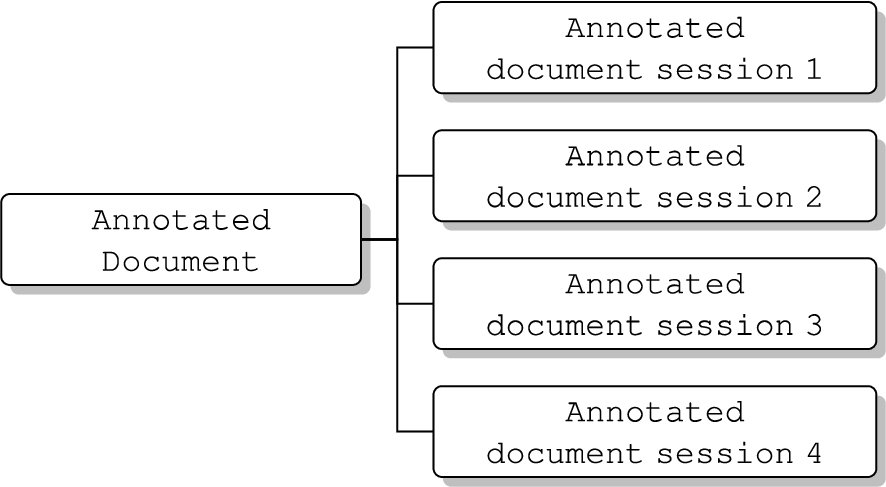
| Whole | Label representing whole text indicating the note contains infection, BSI, sepsis, faulty device malfunctioning, catheter, PIVC, or sensitive information | 0 | Annotated document | Representation of an AE note’s filename, annotation session, annotator, and annotated labels | 4 |
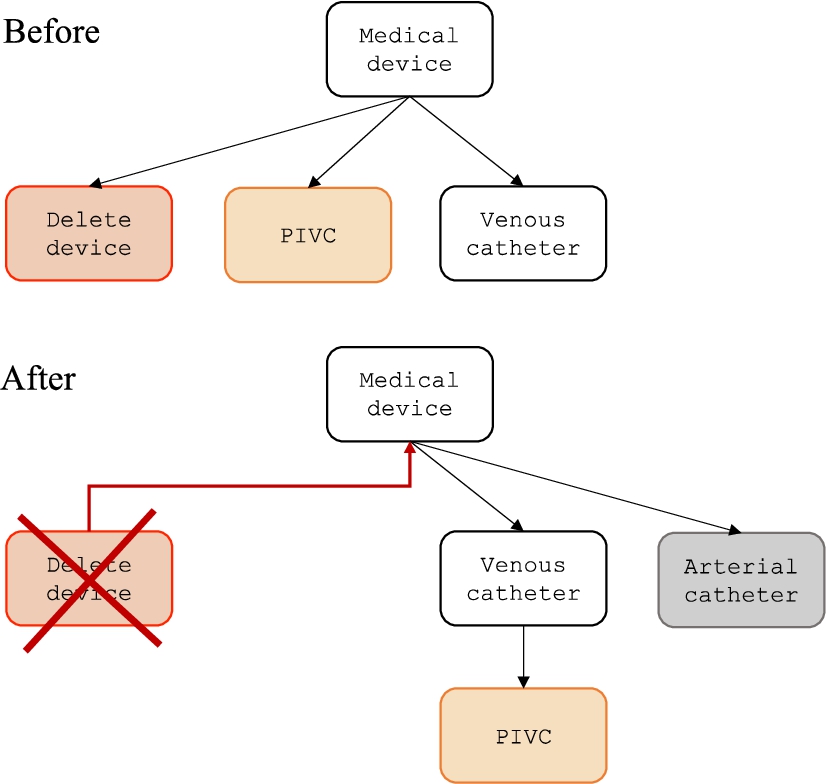
The results from all 4 annotation sessions were included as individuals in the terminology, but the terminology only reflects results based on the last annotation guideline. To accommodate revisions in the annotation guideline, annotation categories that were revised in the guideline are updated in the terminology correspondingly. For instance, removed annotation categories are reflected by changing the granularity of the removed category to a higher level. Annotation categories can also be re-organized to become subclasses of a different class. Moreover, newly added annotation categories are directly added as new classes in the terminology. An example is depicted in Fig. 4.
Fig. 4.
Handling annotation guideline revisions in the terminology. If the Delete device annotation category in red is removed from the annotation guideline, then the Delete device class is removed from the terminology and all individuals of the Delete device terminology class are now part of the superclass Medical device. If the PIVC (peripheral intravenous catheter) annotation category in orange is re-organized to become the sub-category of Venous catheter, then the PIVC class is now a subclass of Venous catheter and the individuals remain as part of the PIVC class. If the Arterial catheter annotation category in gray is added, then the Arterial catheter class is added to the terminology and the corresponding individuals will be added as well.
Although the terminology was not developed to answer competency questions, the competency questions were still used to determine what could be found in annotated documents. To answer competency questions, the annotated documents were imported into the terminology as individuals.
6.Terminology results for annotations
6.1.Annotated Adverse Event NOte TErminology (AAENOTE)
Annotated AE documents and their annotations are modeled by the Annotated Adverse Event NOte TErminology (AAENOTE). To increase accessibility, the terminology is in both English and Norwegian. There are 149 classes, 5 object properties, 27 data properties, and 4470 individuals. The 7 classes which form the main hierarchies are:
1. Observation: Any sign or symptom that can be monitored.
2. Anatomical location: Any anatomical body part, organ, or relative position of the body.
3. Medical device: Any instrument, device, or equipment used for a medical purpose.
4. Procedure: Any procedure, intervention, or activity related to catheters.
5. Identifier: Protected health information that can be used to identify an individual.
6. Person: An individual, such as a patient, clinician, or relative.
7. Annotated document: Annotated adverse event document metadata and labels.
1. Person
2. Procedure
3. Observation
4. Observation, Medical device, or Procedure
5. Annotated document
Fig. 5.
Annotated Adverse Event NOte TErminology (AAENOTE) representing an annotated document. (a) Example of an annotated document with annotation categories and relationships that link the categories together. (b) Part of the terminology class hierarchies used within the annotation example are shown in the white boxes. The 3 annotated relationships (i.e.,
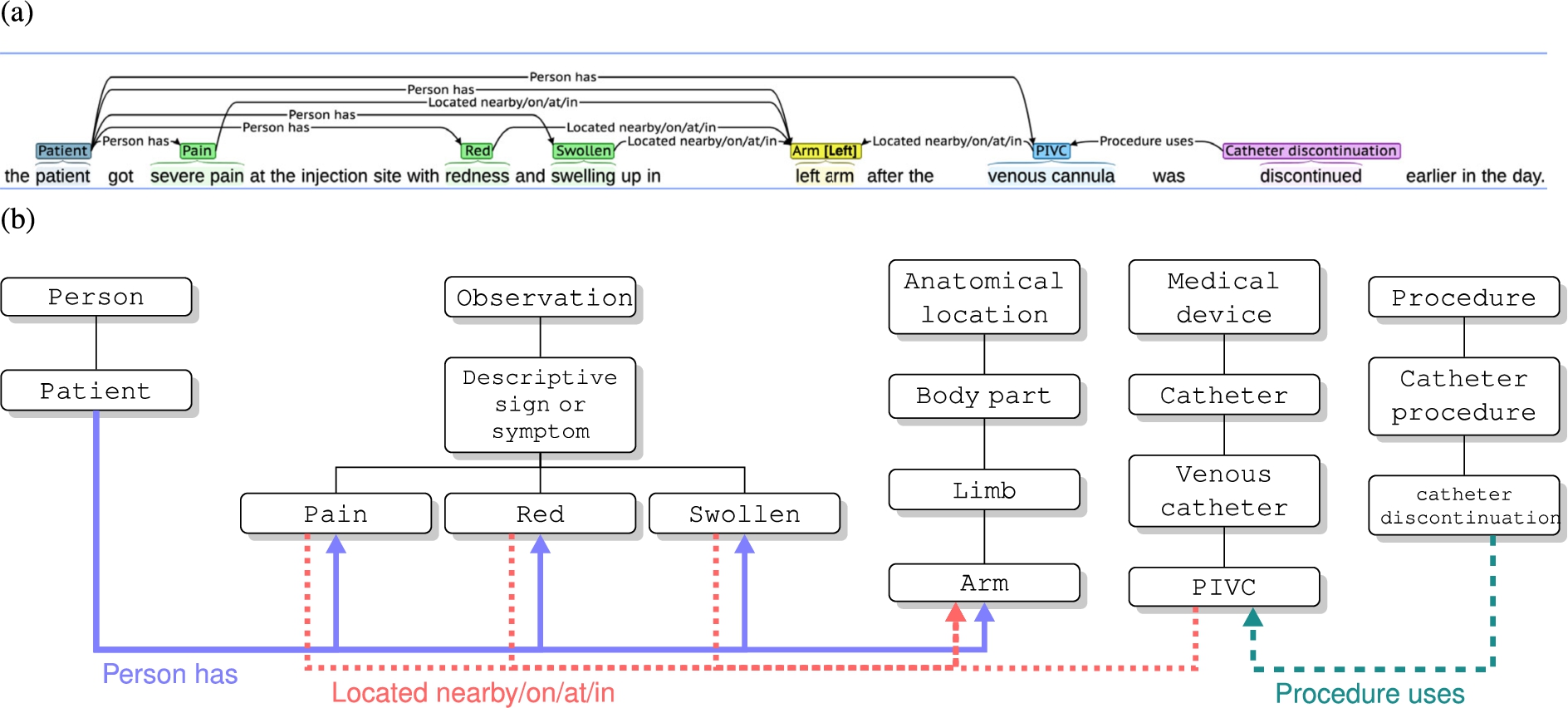
Each annotated AE note or document is an individual of the Annotated document class and can have object properties linking the AE document to individual labels from the other 6 class hierarchies. Additionally, each AE document has data properties for the filename, annotation session, and annotator. The individuals of the other 6 hierarchies can also have object properties and data properties if an annotator provides that information.
6.2.AAENOTE evaluation
The purpose of AAENOTE is to model and provide semantic meaning to annotated AE notes or documents. The terminology was not developed based on competency questions, but it would be interesting to see what competency questions could be answered. Hence, AAENOTE was evaluated using the competency questions as requirements. Competency questions using AAENOTE can only be answered based on explicitly annotated classes or subclasses. Words or phrases that lack annotation are excluded from this terminology. Thus, only the annotation category labels provided by annotators are included as individuals of the corresponding classes.
Knowledge represented by the terminology can either be found explicitly, based on the direct classes and relationships, or be inferred implicitly, based on underlying concrete knowledge and indirect classes and relationships. For example, the competency question “Does patientA have an infection?” can be answered explicitly by finding an individual of the patient class who has an infection (i.e., Patient
SPARQL query results vary depending on the clinician’s interest in knowing how many instances a patient has for one class or a combination of that one class with other classes. For example, to find how many patients explicitly have an infection, the query can be written to find all instances where either: 1. individuals of the patient class have the object property “person has” to an individual of the infection class (i.e., Patient
Table 4
AAENOTE SPARQL query result: patient has infection
| Person | Observation | ||||||||||||||
| Query Result | Instances | # Observations | patient | blood pressure | body temp | c reactive protein | conciousness level | infection | neurological and physiological | observation | pulse | red | respiratory rate | sepsis | swollen |
| 1 | 14 | 1 | ✓ | ✓ | |||||||||||
| 2 | 1 | 1 | ✓ | ✓ | |||||||||||
| 3 | 1 | 2 | ✓ | ✓ | ✓ | ||||||||||
| 4 | 1 | 2 | ✓ | ✓ | ✓ | ||||||||||
| 5 | 1 | 2 | ✓ | ✓ | ✓ | ||||||||||
| 6 | 1 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||
| 7 | 1 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||
| 8 | 1 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||
| 9 | 1 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||
| 10 | 2 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||
| 11 | 1 | 4 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| 12 | 1 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| 13 | 1 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 14 | 1 | 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
Query result 1: Patient
Query result 2–14: Patient
Table 5
AAENOTE SPARQL results for observations located at the skin
| Observations | |||||||
| Query Result | Instances | edema | infection | pain | red | swollen | warm |
| 1 | 1 | ✓ | |||||
| 2 | 3 | ✓ | |||||
| 3 | 3 | ✓ | |||||
| 4 | 2 | ✓ | ✓ | ||||
| 5 | 2 | ✓ | ✓ | ✓ | |||
| 6 | 2 | ✓ | |||||
| 7 | 2 | ✓ | ✓ | ||||
| 8 | 1 | ✓ | |||||
| 9 | 1 | ✓ | ✓ | ||||
| 10 | 1 | ✓ | ✓ | ✓ | |||
Query result 1: Infection
Query result 2–10: Observation
Overall, explicit queries and basic implicit queries in AAENOTE can answer 7 of the 9 competency questions. However, these queries still lack the clinical knowledge needed to include more implicit queries by combining additional observations, anatomical locations, and/or procedures to identify indications. In Appendix B, Table 7 provides the terminology classes and relationships used to form explicit and implicit queries to explicitly and implicitly answer each competency question. Additionally, concrete underlying knowledge used to make inferences is also provided. Results can be found in Appendix B.
7.Ontology development for domain knowledge
7.1.Design decision for domain knowledge
In this use case, the clinicians’ need is to focus on identifying and inferring a patient’s state based on documented observations in AE documents related to PIVCs and BSIs. A patient’s underlying state can be measured by monitoring devices that measure vital signs (e.g., blood pressure, pulse, and respiratory rate) or exhibited by observable signs and symptoms (e.g., pain, fever, chills, and mobility impairment). Those measurable and observable signs and symptoms are then documented by clinicians in the electronic health record (EHR) to record patient conditions and communicate with other clinicians. When an AE incident could have or has happened, clinicians will go through the documentation to recall what occurred and report it in a separate AE document.
To limit the scope of modeling the clinical knowledge ontology, 15 documents were used as examples to form the classes and individuals. Each document was split into sentences to identify catheter and infection indications at the sentence-level and document-level. At the sentence-level, individual sentences were presented to clinicians who determined what observations, anatomical locations, or procedures within the text are needed to determine catheter and infection indication. Only clinician-identified sentences with indications were included as individuals in the ontology. At the document-level, individual sentences from a document were presented together, allowing clinicians to identify indications based on additional information from a more complete documented story. Presenting the document as separate sentences allowed clinicians to identify concepts within a limited example to determine what can and cannot be determined based on limited information. Whereas, allowing a clinician to see the whole document presented more possibilities and helped identify necessary data combinations for indications of catheters and infections.
The focus of the ontology includes catheter indications and the clinicians have identified that it is important to identify infusion phlebitis. Thus, infusion phlebitis was included in the ontology as rules based on the 1998 Visual Infusion Phlebitis Scale [30] mentioned in the 2021 Infusion Therapy Standards of Practice Updates [28]. Furthermore, causality is not within the scope because the exact reason for chemical and mechanical reactions resulting in infection-like signs are more likely found at the body’s cellular or genetic-level in pathophysiology studies [29,55] and unlikely to be documented in AE documents.
Anatomical locations in this ontology were kept simple and similar to the AAENOTE. Clinical guidelines for catheter insertion into anatomical locations are very specific (e.g., a central venous catheter is inserted in the jugular vein until it reaches the superior vena cava [31]) because clinical guidelines provide instructions on how to perform a task properly. However, clinical documentation is more general (e.g., central venous catheter in the chest) because this is common clinical knowledge, and the documentation is written for other clinicians to understand. To match the ontology with available documented data, this ontology relies on general anatomical location terminology. If clinicians deem it necessary, clinical guidelines can be included in a separate ontology focused on identifying catheter locations based on clinical guidelines and the FMA. Inclusion of clinical guidelines to identify specific catheter insertion sites and placement requires anatomical knowledge. For instance, to identify a central venous catheter’s general anatomical location using a clinical guideline and the FMA anatomy ontology, the ontology would need to:
1. Identify the jugular vein insertion site and the superior vena cava placement.
2. Infer that the jugular vein is in the neck and the superior vena cava is present within the superior and middle mediastinum [65], annotated as anatomical location chest.
3. Convert the terms into more general terms that match the available data (i.e., vena cava is in the chest).
7.2.Representing domain knowledge
Discussions with clinicians about example documents and indications formulated the classes, object properties, data properties, and rules within the ontology. Then, the provided indications were sorted and summarized to match the ontology closely. Afterward, indications were verified by clinicians and included in the ontology using SPARQL queries. A list of indications can be found in Appendix C.3.1 to Appendix C.3.7.
8.Ontology results for domain knowledge
8.1.Catheter Infection Indications Ontology (CIIO)
The Catheter Infection Indications Ontology (CIIO) represents clinical knowledge for signs of infections and catheters to identify PIVC-related BSIs and was developed to accompany the AAENOTE. Similar to AAENOTE, this ontology is also in both English and Norwegian. There are 57 classes, 10 object properties, 16 data properties, and 187 individuals. The 7 classes which form the main hierarchies are:
1. Observation: Any sign or symptom that can be monitored.
2. Anatomical location: Any anatomical body part, organ, or relative position of the body.
3. Medical device: Any instrument, device, or equipment used for a medical purpose.
4. Procedure: Any procedure, intervention, or activity related to catheters.
5. Person: An individual.
6. Document: Unstructured free-text report consisting of sentences documented to represent observable patient states.
7. Sentence: A set of words documented to represent observable patient states.
1. Person’s subclass Patient
2. Procedure
3. Observation
4. Observation, Medical device, or Procedure
5. Document or Sentence
6. Procedure’s subclass General IV
7. Procedure’s subclass General IV
8. Procedure’s subclass General IV
9. Observation, Anatomical location, Medical device, Procedure, or Person
10. Anatomical location
Fig. 6.
Catheter Infection Indications Ontology (CIIO) clinical knowledge representation. (a) A sentence from a document used to identify documented clinical knowledge. Annotations are based on terms from the Annotated Adverse Event NOte TErminology (AAENOTE). (b) CIIO has a Sentence class and
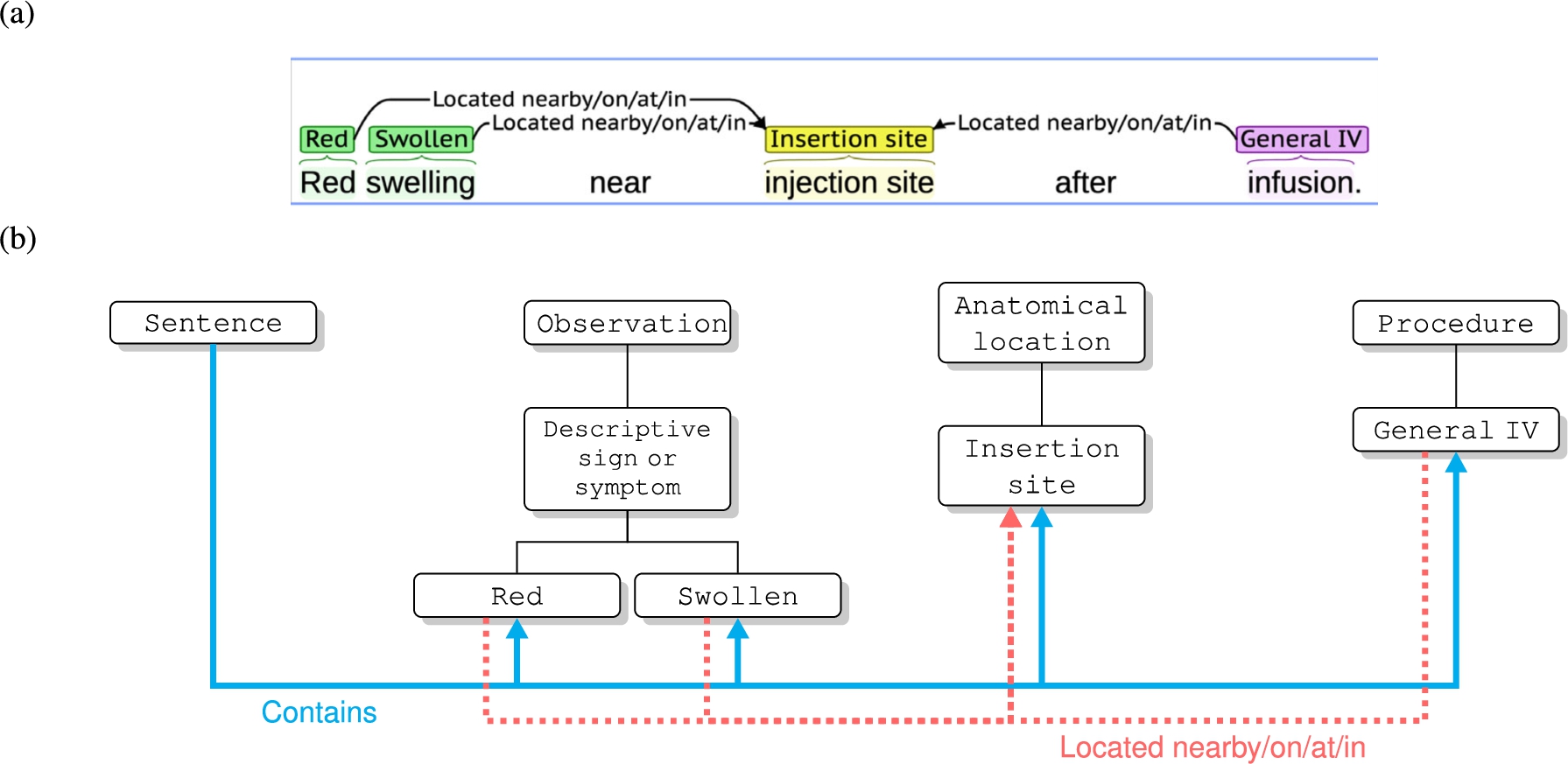
Each sentence documented in the report is an individual of the Sentence class. Sentence class individuals contain Observation, Anatomical location, Medical device, Procedure, or Person individuals present within the text. An individual of the Document class contains the Sentence individuals that form it and the content from those sentences. Similar to AAENOTE, individuals of Observation, Anatomical location, Medical device, Procedure, and Person can also have object properties and data properties.
8.2.CIIO evaluation
Designed to capture and reason about clinical catheter-related and infection-related signs and symptoms documented in an AE report, the CIIO provides the missing clinical domain knowledge for the AAENOTE. CIIO can answer 8 of the 9 competency questions based on assumptions and indications. The assumptions are that 1 AE document represents 1 patient and all sentences within a document are likely to describe concepts within the same event (Appendix C.2). Indications for catheters and infections are provided in (Appendix C.3). Additionally, the ontology classes and relationships used to answer each competency question is detailed in Appendix C.4.
9.Discussion
9.1.Ontology development method comparison
The clinical problem drove this study, and the objective was not to apply an ontology development method. Hence, a specific ontology development method was not applied. However, certain steps taken are similar to the pre-existing methods and this study does include the typical phases of specification, conceptualization, formalization, implementation, maintenance, knowledge acquisition, evaluation, and documentation. An overview of the process is shown in Fig. 7, and similarities to other methods can be found in Appendix A.
Fig. 7.
Development phases for Annotated Adverse Event NOte TErminology (AAENOTE) and Catheter Infection Indications Ontology (CIIO).
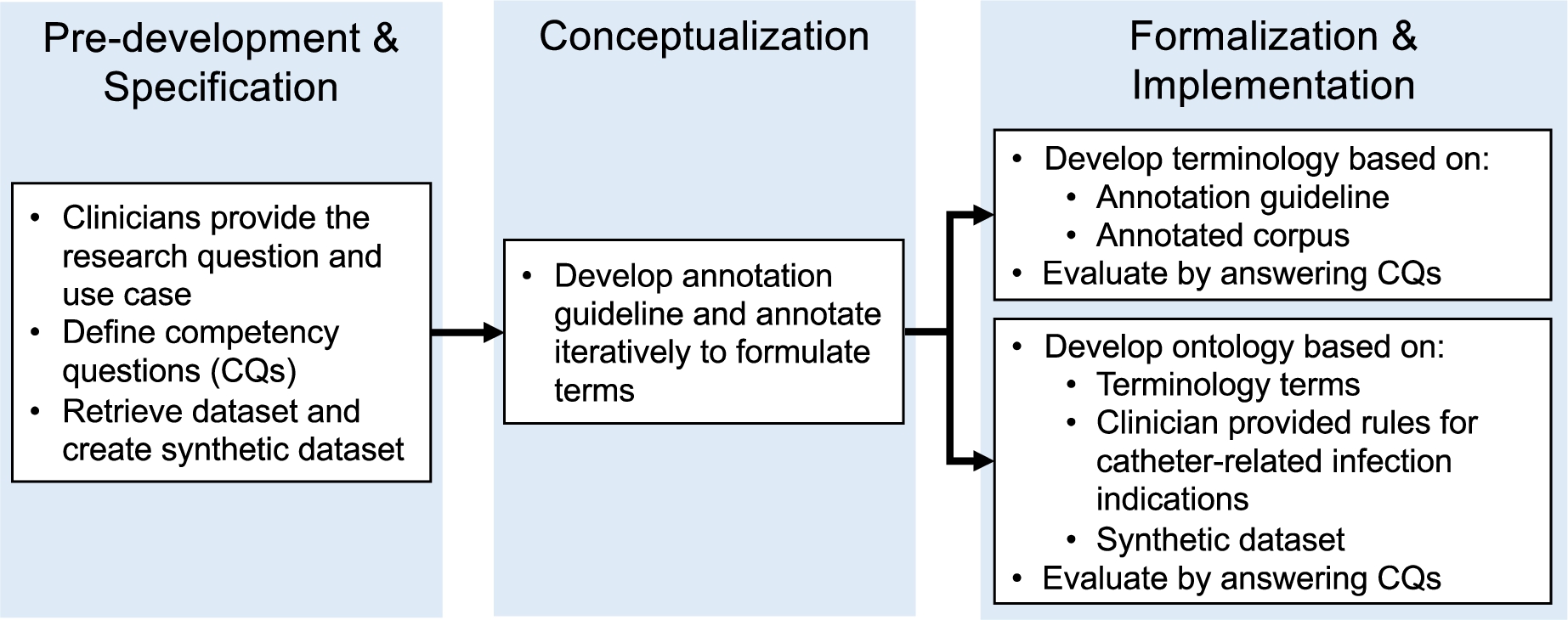
During the pre-development and specification phases of the terminology, clinicians provided the research question and use case. Those were utilized to define the competency questions. Additionally, the AE dataset was retrieved, and an AE synthetic dataset was created. The conceptualization phase was performed by iteratively developing the annotation guideline and annotation sessions. Afterward, the formalization and implementation phases of the terminology were developed iteratively based on the annotation guideline and using instances from the annotated corpus to answer competency questions for evaluation. Knowledge acquisition occurred during all phases with insight, guidance, and feedback from clinicians. Documentation is provided in the annotation guidelines, the annotated corpus, and the evaluation of competency questions. The annotation guidelines document changes in terms over time, and the annotated corpus documents knowledge acquisition from the text. Answers to each competency question are documented using natural language for clinicians and SPARQL queries for computer scientists.
Ontology development is similar to the terminology’s pre-development, specification, and conceptualization phases. However, the formalization and implementation phases differ. The ontology iteratively incorporated clinical knowledge that can be annotated in AE documents using terminology terms to answer competency questions for evaluation. Knowledge acquisition was provided through the annotated corpus, clinician-provided catheter indication rules, and clinician-provided publications containing phlebitis rules. Additionally, clinicians iteratively reviewed and verified documented sentences to match the rules and competency questions. Ontology documentation includes the assumptions (Appendix C.2), rules for catheter and infection indications (Appendix C.3), and how competency questions were answered (Appendix C.4).
Although UMLS includes clinical terminology (i.e., SNOMED CT and ICD-10), the terms are often a combination of different concepts. For example, phlebitis has many options and is combined with different locations, such as “phlebitis of the lower limb vein,” “phlebitis of the portal vein,” and “retainal phlebitis.” Additionally, swollen has many options, such as “foot swelling,” “swollen nose,” and “tongue swelling.” The June 10, 2022 version of SNOMED CT has 361,907 classes.22 It would require extensive time and effort to determine which classes are suitable for our purpose and to maintain a pre-determined class hierarchy. Introducing UMLS terminology would make it difficult for annotators to determine which term to use, introduce ambiguities for the use case, and decrease the precision needed. Furthermore, the UMLS MetaMap is software that finds and links biomedical text to terminology concepts [3]. Unfortunately, that software is for biomedical text and not clinical text. Clinical text differs from biomedical text because it is often ungrammatical and ambiguous, with many shorthand abbreviations and acronyms [33]. Additionally, the MetaMap developers have mentioned that detecting abbreviations and acronyms needs improvements [3].
9.2.AAENOTE scope and limitations
The clinician asks questions about the condition of a physical patient and the patient’s PIVCs, but AAENOTE is about words in the AE document regarding a patient event. The correspondence between clinical condition and document content is represented by CIIO. So, the answer to a question about a patient’s condition will be answered using the document’s annotated text. Understanding a query means translating it from clinical concepts to concepts within the document’s content. Here, the terminology is used to fit and answer questions. SPARQL queries can answer most competency questions, and the results can be used as consistency checks. For example, SPARQL can be used to count and make quantitative queries about the number of catheters and devices. Likewise, qualitative results enabled clinicians to verify if results matched their expectations of clinical events (i.e., the anatomical location of specific catheters) or why the AE was reported (i.e., incorrect medical devices used in a particular procedure).
There are several limitations to the AAENOTE. Although this terminology does not cover sepsis, it does cover events that could lead to sepsis. This terminology lacks the clinical knowledge required to answer several competency questions more in-depth. Moreover, it is not always possible to determine what a patient has because of the document’s content or provided annotations. Most documents do not explicitly mention a patient because these are AE documents, and it is often implied that the adverse event has happened to a patient. Annotators will often not link the patient to all possible observations, anatomical locations, medical devices, or procedures because typically, one AE document refers to one event or patient. Furthermore, referent tracking and resolution are not handled by AAENOTE. Thus, multiple mentions of a label or individual do not indicate whether it is the same item or a different item. For example, given the annotated document in Fig. 2, the terminology cannot determine if the 2 Patient individuals refer to the same patient or not because each label is an individual. Similarly, the same also applies to the 2 PIVC individuals. In this example, a query counting how many patients have a PIVC will answer 2. However, based on the context, both sentences in the document likely refer to the same patient and PIVC and the answer should be 1.
9.3.CIIO scope and limitations
The CIIO is an abstract ontology with instances populated using the terminology. Only parts of the AAENOTE necessary for creating queries with clinician-provided indications were included or extended. This provides flexibility, allows for easier ontology maintenance, and separates the needs of clinicians who use CIIO and annotators who use AAENOTE.
Based on assumptions and indications, competency questions can be answered using SPARQL queries. The queries retrieve documents and translate the content for the user by identifying concepts necessary to answer the competency questions. Thus, the retrieved documents and concepts can provide sufficient information for clinicians to further decipher retrieved answers. For example, the exact reason why a patient needs a catheter cannot be determined by the query unless there is a direct relationship (i.e., Procedure
The lack of detailed documentation inhibits the query’s ability to answer certain questions. This includes why a patient needs a catheter as previously stated, counting catheters within a patient, and where the catheters are located in a patient. Counting the exact number of catheters per document is not possible because multiple sentences within a document could be describing the same catheter or multiple procedures could use the same catheter. The exact anatomical location of catheters per document cannot be determined for several reasons. First, multiple sentences within a document could be describing the same catheter at the same location but with more general terms (i.e., arm instead of hand). Second, the location’s position not being documented makes it difficult to distinguish if a body part is on the same side. Finally, various procedures can be performed at the same location. For example, given an example document, “The patient received IV fluids in elbowA and IV antibiotics in right handB. Right armC showed signs of phlebitis.” Here, handB is part of armC because both are on the right side, but elbowA might or might not be part of armC. Additionally, armC is likely a more general term for handB. Furthermore, an additional anatomical ontology is needed to infer the possible locations based on catheter type.
9.4.Purpose of separate terminology and ontology
Even though the ontology uses terms from the terminology, the terminology and ontology are separate. They are separate because of their different purposes and functionalities. Additionally, separation provides downstream analysis flexibility for researchers. It also simplifies evaluation and allows for easier maintenance. Furthermore, separation enables a better understanding of the terminology’s and ontology’s limitations.
The terminology and ontology were developed for different purposes using different methods. AAENOTE is intended to be useful for annotators who are annotating documentation and a way to provide them a structured terminology with varying granularity. In comparison, CIIO is intended to be used by clinicians to clinically reason about a patient state. The design process of AAENOTE is heavily based on the explicit terms used in annotations and not on competency questions. It uses the bottom-up method and the annotation guideline development process to capture semantic annotations. In contrast, the design process of CIIO is based on the competency questions, which focus on patient states. Designed with a top-down method, it is based on concepts naturally used by clinicians to describe patients. Thus, the terminology and ontology have different purposes and functionalities.
Separating the terminology from the ontology enables annotators to annotate concepts with standard terms and clinicians to reason about the annotated concepts. Here, the ontology does not impact the terminology annotators can use. Instead, the ontology provides knowledge for the terminology. Thus, our methods avoid the significant amount of time, effort, and manual curation previously required to map terms to an ontology [61]. Instead, our ontology utilizes concepts in the terminology and is limited by the competency questions, clinical guidelines used, and clinician-provided rules. In downstream analyses, researchers can freely choose to use the terminology to quickly retrieve documents with specific annotations, the ontology to reason and infer clinical knowledge, or both.
The terminology indicates concepts annotated in documents. Using terms from the terminology ensures that the included clinical knowledge within the ontology represents the knowledge documented in the text that can be annotated. As the ontology develops further, it is possible to conceptualize additional terms required to answer the competency questions. Those terms can then be added to the terminology and annotation guideline for additional data curation.
In this paper, separating the terminology made it easier and quicker to evaluate syntax and semantics because the ontology only has 187 instances compared to the terminology’s 4470 instances. Mixing the indexed annotation terminology with a clinical knowledge ontology would be outside the ontology’s scope, decrease ontology reusability, and increase the complexity of ontology maintenance. Additionally, the terminology can cover a broader scope of documents not in the ontology. Finally, using competency questions to evaluate the terminology and ontology separately reveals the distinct limitations of both. The inability to answer competency questions can be due to either the lack of knowledge or lack of necessary content within the data.
9.5.Representing annotated data and revisions
Annotating data provides data meaning, and the corresponding annotation guideline and terminology provide additional structured semantic meaning. Additionally, the terminology can represent knowledge and disambiguate annotation entities and relationships. Each annotation session uses a slightly different annotation guideline that has been revised based on the previous annotation session. Hence, revisions in the annotation guidelines include added, re-organized, and removed categories. Since results from 4 different annotation sessions are included as individuals in the AAENOTE, this indicates the terminology can handle different versions of annotated data while preserving semantic meaning. It is also possible to easily customize the granularity (i.e., superclasses, classes, or subclasses) and extend or retract the terminology based on clinician needs without breaking the terminology.
To alleviate the problem with overlapping terms and ambiguities experienced by [5] and remove mismatches between the annotations and the terminology experienced by [61], all annotators in our study could only use provided annotation labels from the terminology. Using concrete concepts from the annotation guideline based on what can be found in the documentation instead of other pre-existing ontologies lowers the complexity and simplifies the terminology.
9.6.Representing annotated documents the way clinicians view patients
The AAENOTE is a terminology that provides an index of what is annotated in a clinical document. It is not used to design a language’s syntax, grammar, or terms because AAENOTE is a terminology for understanding the language and underlying meanings. Instead, it is the interpreted formalized language that has been translated into basic statements for reasoning. To capture relevant information, the underlying document was represented by annotated labels and relationships for the task of question answering and text understanding instead of solely retrieving information. Hence, the terminology focuses only on items of interest and is blind to items not within the terminology.
The corresponding CIIO is an ontology that models clinical knowledge missing from AAENOTE. It provides the missing clinical knowledge required to reason about the presence of catheters and infections documented in clinical text. Although the data modeled is documented text, it enables clinicians to think about the data as an individual patient because they already do this routinely when documenting patient states.
9.7.Understandability and accessibility for domain experts
The approach in this study made ontology development understandable and accessible for the domain experts without formal ontology training. Furthermore, the employed approach made it possible for clinicians to understand and be part of the design process. In practice, the approach was a necessity to progress in developing the ontology to incorporate clinical knowledge.
9.8.Clinical utility
The collected competency questions and requirements are largely met. Thus, the main objective of developing a terminology and ontology that clinicians and hospital systems can use to get a systematic overview of identifying and reasoning about PIVC-related phlebitis, infection, and sepsis in an AE corpus has been met. Furthermore, our ontology is a step toward automated and continuous quality control that move beyond today’s focus on repeated point prevalence quality controls, like the Peripheral Intravenous Catheter mini Questionnaire (PIVC-miniQ) [24].
The developed ontology is of value for sepsis because of its purpose, clinician involvement during development, and intended use. The ontology focuses on identifying indicators of catheter-related phlebitis or infections that can lead to sepsis by utilizing the clinicians’ documentation and perspectives. Throughout the whole development, clinicians were involved as the users, domain experts, and data annotators. Furthermore, clinical knowledge within the ontology was captured similarly to how clinicians ask questions, document observations, and view documents as patients. The intent is to eventually implement the ontology into a quality surveillance system to automatically detect the presence of PIVC-related phlebitis and BSIs to improve PIVC care and lower sepsis incidents. Thus, only documented content can be included as data, and the ontology must directly correspond to and represent concepts documented within the AE documents from the clinician’s perspective.
10.Future work
For the sepsis-related use case, the synthetic AE dataset used for annotations is a placeholder for the real Norwegian AE dataset and clinical records from the EHR. Future work includes utilizing the current AAENOTE to annotate the real Norwegian AE dataset and clinical records. And to evaluate if clinical knowledge from the CIIO can still be applied and expanded on new data. Additionally, the ontologies could be applied to AE documents at other Norwegian hospitals to assess how similar documentation and knowledge are between different hospitals. The ontologies can be directly translated to other Scandinavian languages (e.g., Swedish and Danish) and applied similarly at other Scandinavian hospitals. The design and representations are largely language-independent and should be easy to transform for English clinical text about adverse events. After all, international literature suggests that the phenomena related to PIVC and devices are language-independent [1]. It would also be possible to provide multi-language querying over multi-language AE documents to enable cross-language repositories [63]. Furthermore, supervised machine learning methods can be employed to identify PIVC-related BSIs and classify patients requiring additional monitoring.
11.Conclusion
The development process resulted in a terminology and an ontology, specifically, the Annotated Adverse Event NOte TErminology (AAENOTE) which models annotated classes in annotated documents and the Catheter Infection Indications Ontology (CIIO) which models clinical knowledge for catheter and infection indications. Although there is a clinical focus here, the methodology for creating a terminology from an annotation guideline for semantically annotated data and a domain knowledge ontology to represent knowledge can be utilized in other domains to provide additional semantic meaning to annotated datasets in other domains.
12.Data availability
The AAENOTE, CIIO, and SPARQL queries for this paper are in the GitHub repository branch “swj” of https://github.com/melissayan/aaenote_and_ciio. Detailed specifications for AAENOTE and CIIO were generated using WIzard for DOCumenting Ontologies (WIDOCO) [16] and are available in English and Norwegian at https://folk.ntnu.no/melissay/ontology/index.html.
Notes
Acknowledgements
The authors would like to acknowledge the eight annotators for producing the annotated clinical adverse event (AE) corpus. Funding was provided by the Computational Sepsis Mining and Modelling project through the Norwegian University of Science and Technology (NTNU) Health Strategic Area. Additionally, ethical approval was granted by the Regional Committees for Medical and Health Research Ethics (REK), approval no. 26814.
Appendices
Appendix A.
Appendix A.Ontology development methods and evaluation similarities
There are various ontology development methods and the steps in this study have some similarities to other methods Table 6.
Table 6
Ontology development methods versus this paper
| Uschold and King [62] | Grüninger and Fox [20] | METHONTOLOGY [14] | On-To-Knowledge [60] | NeOn [59] | This Paper | |
| Pre-development | Feasibility study phase to identify problems. | Initiation phase to specify ontology requirements, intended use, users, and formal language in the form of competency questions and glossary of terms. | Use clinician identified research question to form competency questions. Form terms for annotation, perform data screening and pre-annotation, develop annotation guideline, schedule annotation, implement annotation sessions, and evaluate annotations. | |||
| Specification | Identify ontology purpose, intended use, and users. | Define ontology requirements as competency questions based on a scenario or user provided problem. | Specification phase to produce ontology specifications. | Kickoff phase to document ontology requirements and semi-formal ontology. | Part of pre-development. | Part of pre-development. |
| Conceptualization | Identify terms and relationships of interest. | Define terminology of ontology. | Conceptualization phase to build glossary of terms. | Refinement phase to refine semi-formal ontology and formalize ontology iteratively based on domain expert interviews. | Design phase to produce an informal and formal model to meet requirements. | Annotation and annotation guideline revision phases determine the terms and concepts that are documented in data. |
| Formalization | Codify ontology into formal language. | Specify terminology definitions using first order logic. | Part of conceptualization. | Part of conceptualization. | Implementation phase to implement the formal model into an ontology language. | Codify terminology and ontology in Protégé using OWL. |
| Implementation | Part of formalization. | Represent terminology in a formal language. | Implementation phase to codify ontology into formal ontology. | Part of formalization. | ||
| Management | Apply the ontology and manage it’s evolution and maintenance. | Use the ontology to detect errors or missing knowledge for design phase of the next ontology version. | Terminology can be updated to a new annotation guideline version and its corresponding annotated corpus. Ontology can include new clinical knowledge. |
Table 6
(Continued)
| Uschold and King [62] | Grüninger and Fox [20] | METHONTOLOGY [14] | On-To-Knowledge [60] | NeOn [59] | This Paper | |
| Knowledge Acquisition | Interview experts and/or analyze text. | Knowledge creation, capture, retrieval and access, and use. | Knowledge is introduced by domain experts and ontology practitioners at different development phases. | Knowledge was acquired iteratively with users and domain experts. Discussions with users and domain experts resulted in annotation guideline revisions and discovering the knowledge needed for ontology reasoning and inferences. Annotations by domain expert annotators to capture knowledge from text. | ||
| Evaluation | Adapt what has been done in the knowledge based systems field for ontologies. | Evaluate the ontology by proving completeness theorems to answer competency questions. | Evaluate the ontologies, software environment, and documenation with the requirement specification document during and between each phase. Document how the ontology was evaluated, errors detected, and knowledge sources for evaluation. | Proposed technology-focused (i.e., the development tool’s evaluation of syntax and semantics of the ontology and the evaluation of tools and applications for interoperability and scalability), user-focused (i.e., user satisfaction with the application and comparing the ontology based application to pre-existing ones), and formal evaluation. | Evaluate the ontology using 5 different tasks [54] which includes selecting individual ontology network components for evaluation, selecting the evaluation goal and approach, identifying the reference and evaluation metric, applying the selected evaluation, and presenting the combined results of the individual components. | Ability to answer competency questions and if the ontology is useful from the perspective of the user. |
| Documentation | Document ontology type and purpose | Document ideally all phases, knowledge acquisition, and evaluation. | Document kickoff phase ontology requirements. | Document ontology requirement specifications, ontology description, and evaluation. | Annotation guidelines record changes, annotations document knowledge acquisition, and evaluation documentation answers competency questions in a format understandable to the users and developers. |
Appendix B.
Appendix B.Annotated adverse event NOte TErminology (AAENOTE) hierarchy competency questions (CQs), SPARQL queries, and results
B.1.AAENOTE hierarchy
The AAENOTE classes and their subclasses can be found in the following figures:
Fig. 8.
AAENOTE observation class hierarchy.
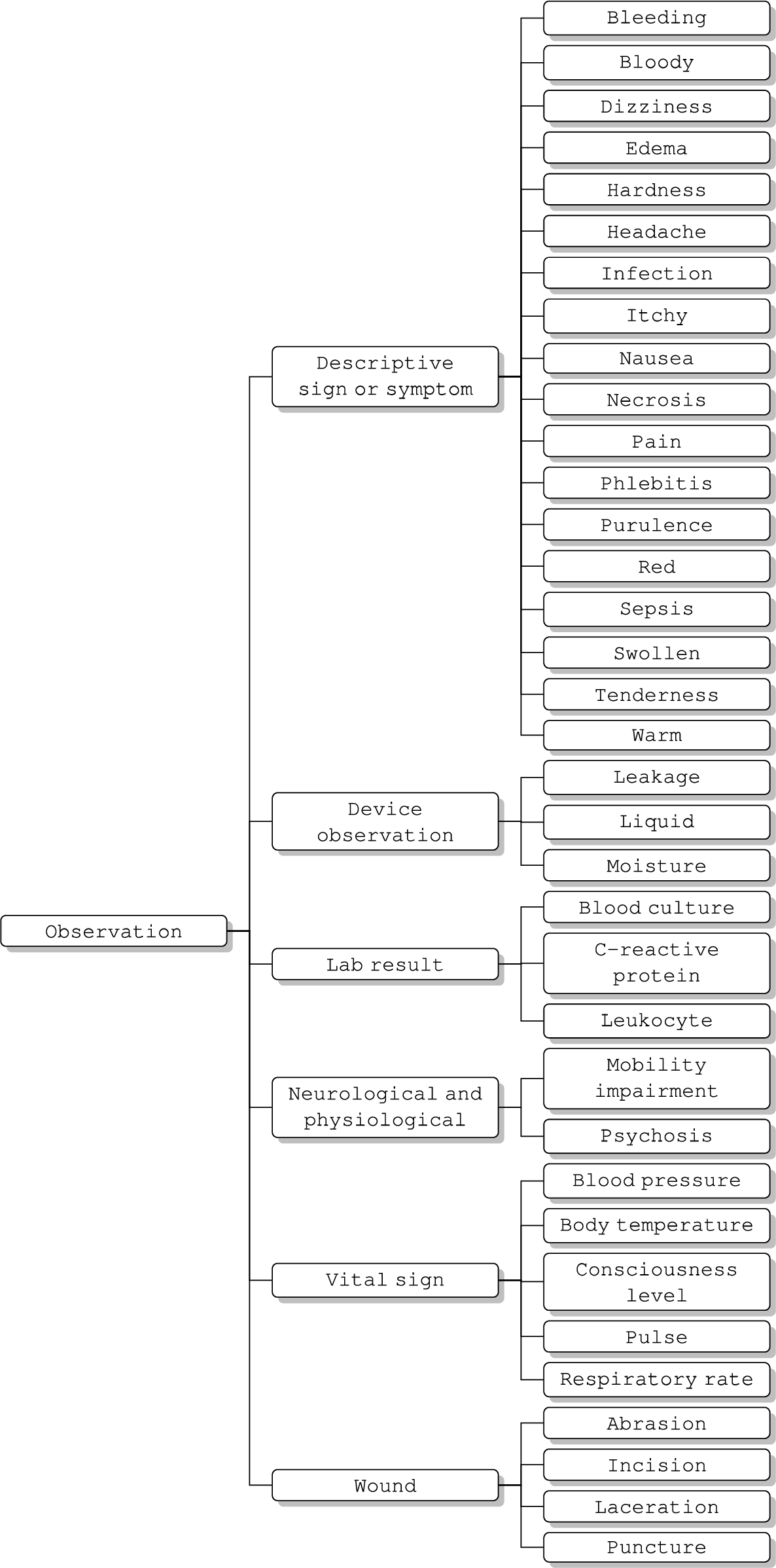
Fig. 9.
AAENOTE anatomical location class hierarchy.
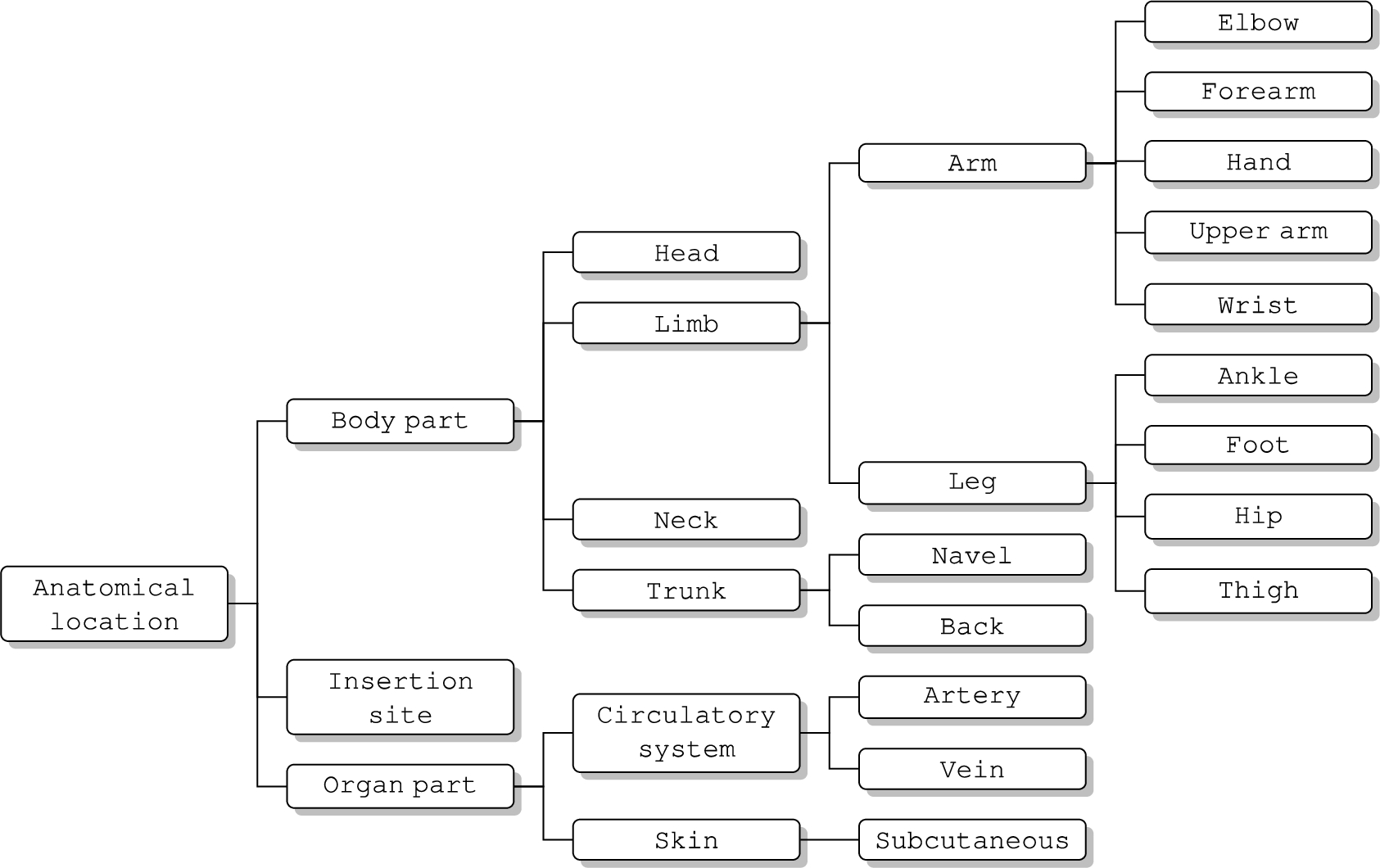
Fig. 10.
AAENOTE medical device class hierarchy.
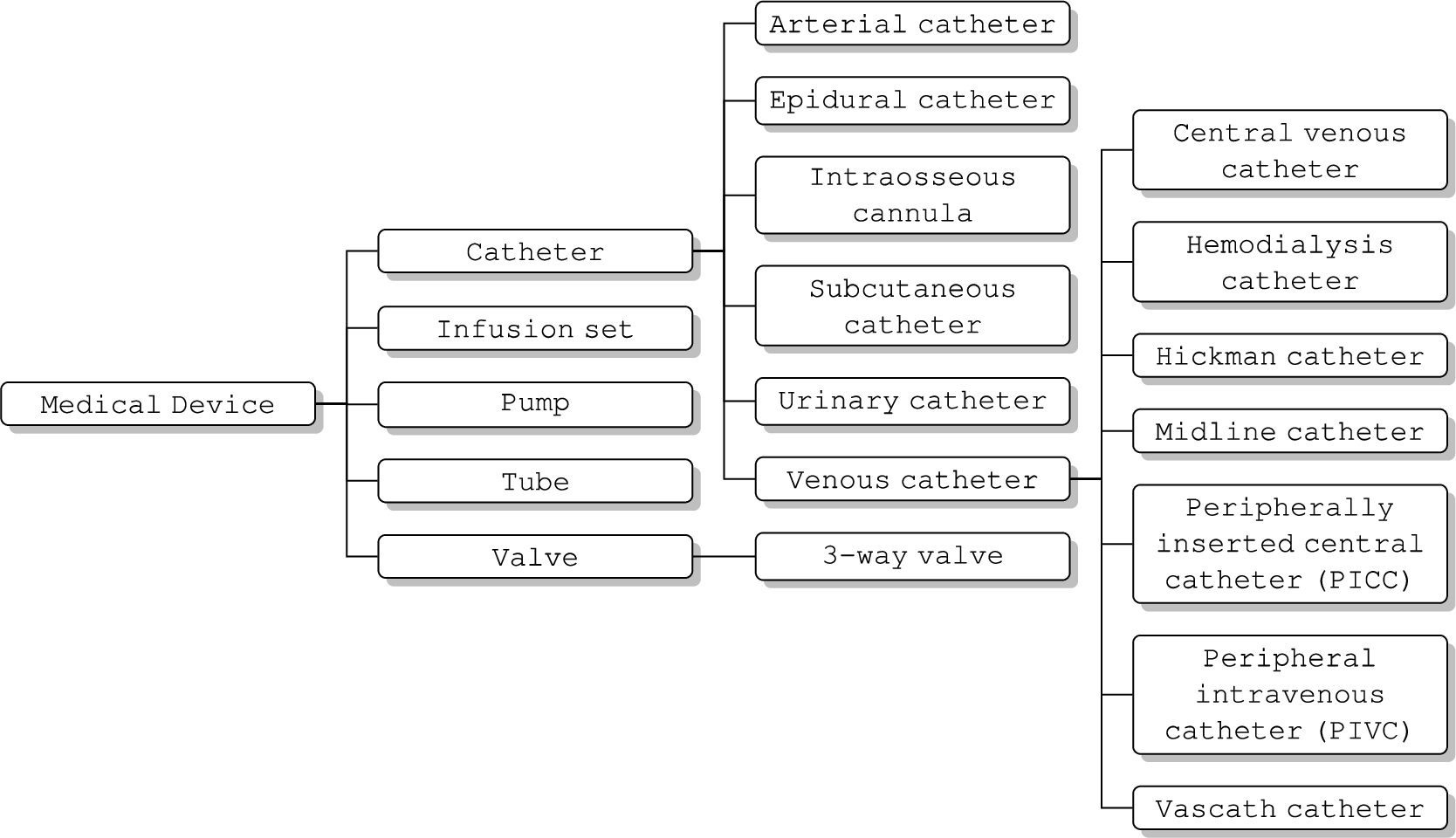
Fig. 11.
AAENOTE procedure class hierarchy.
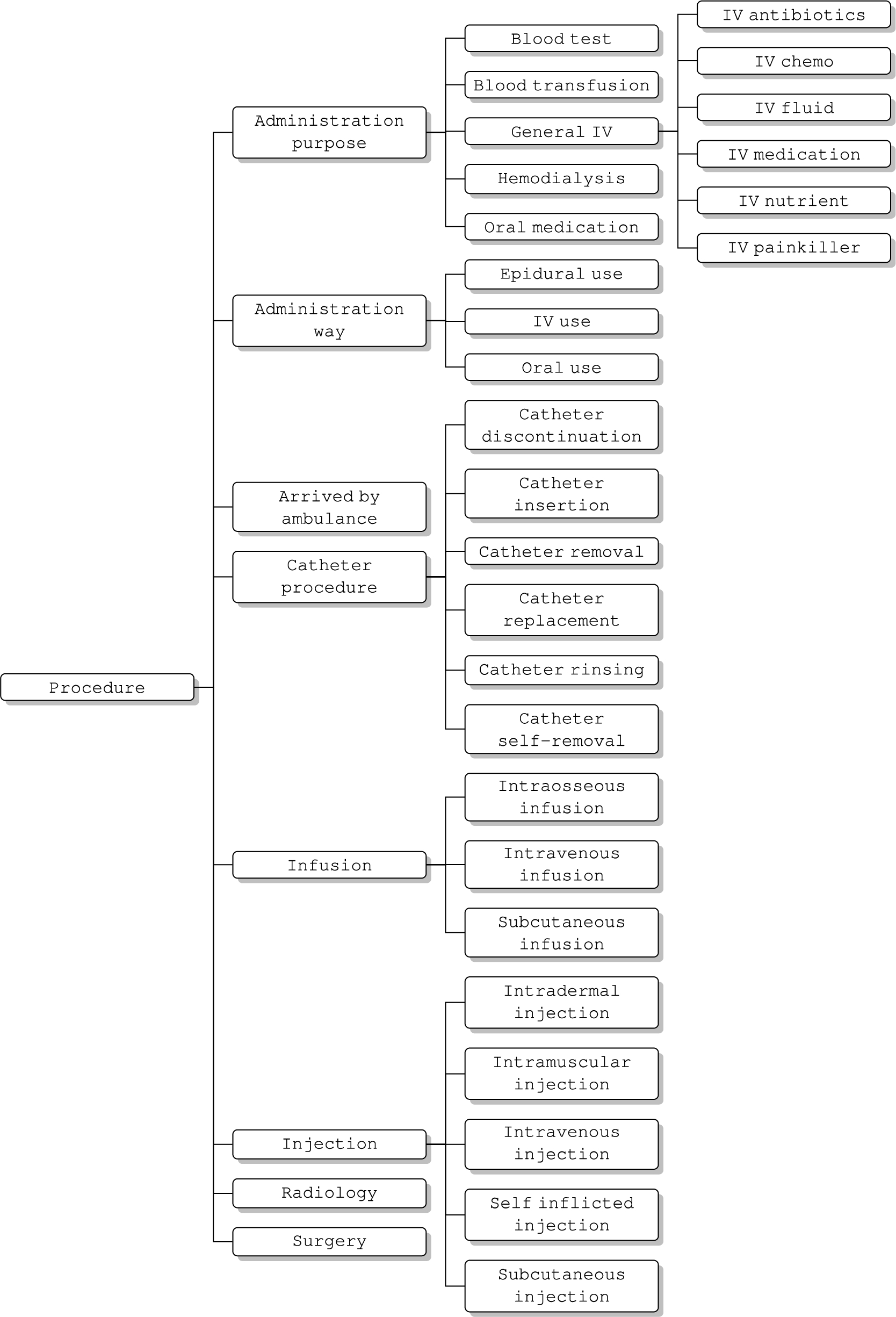
Fig. 12.
AAENOTE identifier class hierarchy.
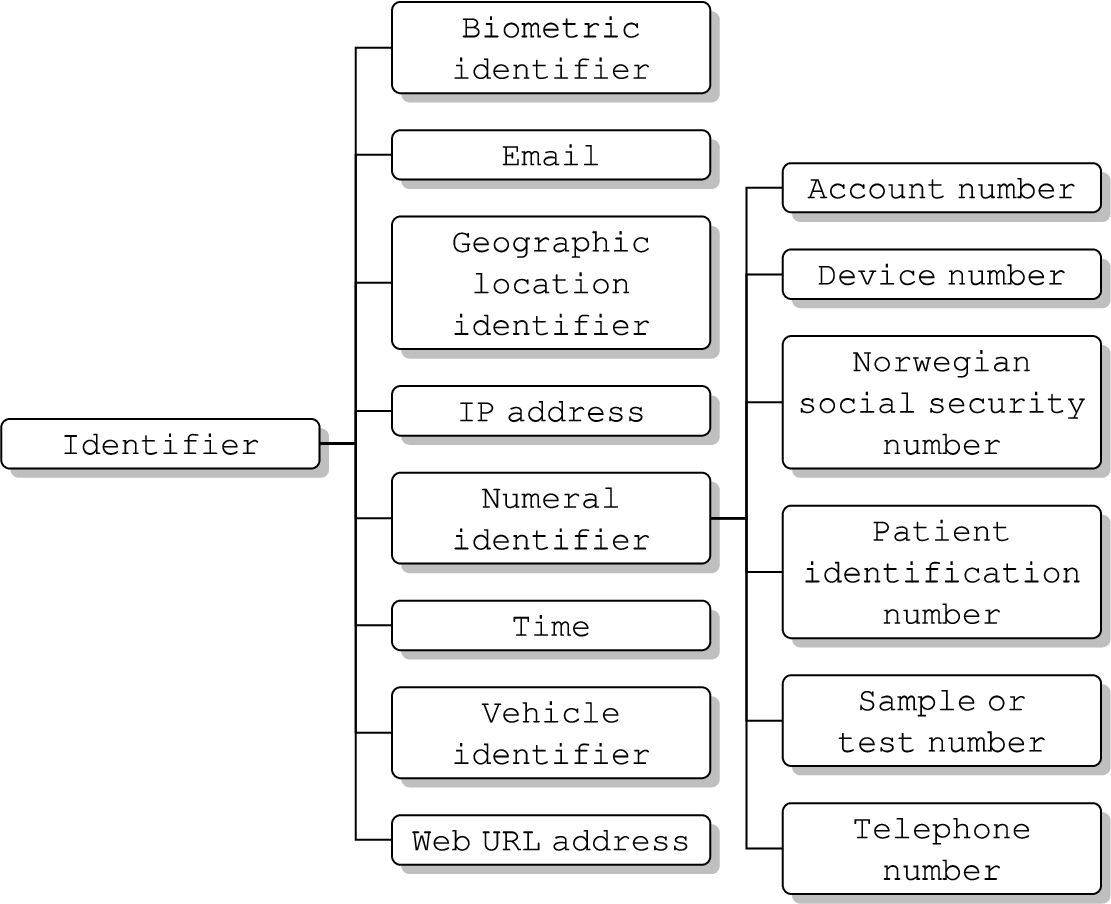
Fig. 13.
AAENOTE person class hierarchy.
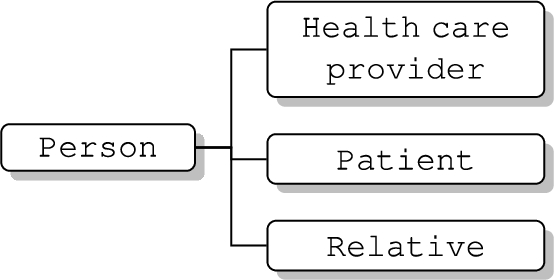
Fig. 14.
AAENOTE annotated document class hierarchy.
B.2.Details about converting annotation guideline to terminology
To further differentiate observations, Descriptive sign or symptom, Vital sign, Neurological and physiological, Wound, Lab result, and Device observation subclasses were introduced. In addition, Insertion site was introduced because some documents document a catheter’s insertion site without mentioning a specific body part. Similarly, Organ parts, such as Skin and Circulatory system, were also introduced because they are documented instead of body part. For Medical device, additional catheters were included (i.e., Intraosseous cannula and Subcutaneous catheter) for specificity. The category for device parts was removed because the terminology only covers catheter and catheter parts; thus, it is a part of a medical device if it is not under a catheter. For Procedure, Administration way was introduced to describe how a substance was administered into the patient, Catheter procedure subclasses all include “catheter” to indicate the action is for catheters only, and different Infusion types were included to differentiate from Injection types.
A hierarchy for certain data properties was introduced to organize the anatomical location descriptors, contents within a document, and document identity. For instance, document identity-related data properties were included for identification, such as annotator ID, filename, and annotation session. Unlike the data property values for body temperature (i.e., hyperthermia, normal, and hypothermia) and severity level (i.e., high, normal, and low), Conciousness level required a separate data property with values of alert, confusion, painfully responsive, unresponsive, and verbally responsive). The “observation is diagnosed by” and “observation said by” data properties were added to distinguish signs from symptoms because signs are what a clinician observes and symptoms are what a patient says.
B.3.AAENOTE competency questions and terminology usage
Table 7
AAENOTE competency questions and terminology usage
| Competency Question | Terminology Classes and Relationships to Find Instances∗ |
| 1. Does patientA have phlebitis, and was it infectious phlebitis, chemical phlebitis, or mechanical phlebitis? |
|
| 2. Does patientA have an infection? |
|
Table 7
(Continued)
| Competency Question | Terminology Classes and Relationships to Find Instances∗ |
| 3. Does patientA have a BSI? | § Cannot determine if there is a BSI without a microbiology laboratory result of a positive blood culture and the cultured bacteria name. |
| 4. How many patients have an infection or BSI? | Same as Competency Question 1 and 2. |
| 5. Which patients have sepsis? |
|
| 6. Does patientB have a catheter? |
|
| 7. Does patientB have a PIVC? |
|
| 8a. How many catheters does patientB have? | Same as Competency Question 6. |
| 8b. Where are the catheters in patientB? |
|
Table 7
(Continued)
| Competency Question | Terminology Classes and Relationships to Find Instances∗ |
| 8c. Why does patientB need the catheter(s)? |
|
| 9a. Does patientC have an infection and catheter? |
|
| 9b. Was patientC’s infection associated with a catheter? | § Cannot determine if an infection is associated with a catheter unless that catheter is tested in the microbiology lab. |
B.4.AAENOTE CQ 1: Does patientA have phlebitis, and was it infectious phlebitis, chemical phlebitis, or mechanical phlebitis?
The patients who have phlebitis are listed in Table 8 using Listing 1. And anatomical locations with phlebitis in Table 9 were queried using Listing 2.
Listing 1:
Patient has phlebitis
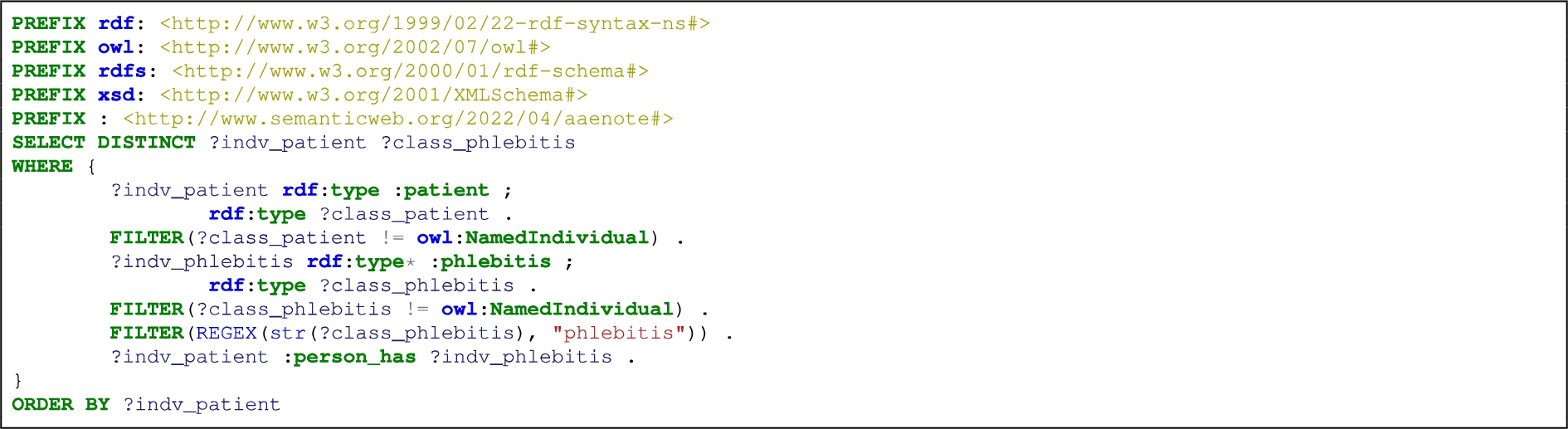
Table 8
AAENOTE SPARQL query result: list patients that have phlebitis
| Query Result | Patient | Phlebitis |
| 1 | patient.T1.2.lo22a.SD_0003 | ✓ |
| 2 | patient.T1.3.do13a.PO_0005 | ✓ |
| 3 | patient.T2.2.do13a.SP_0008 | ✓ |
| 4 | patient.T2.2.lo12a.SD_0003 | ✓ |
| 5 | patient.T2.2.lo22a.PO_0005 | ✓ |
| 6 | patient.T2.3.do23a.PO_0005 | ✓ |
| 7 | patient.T2.3.po24a.SD_0003 | ✓ |
| 8 | patient.T2.4.lo22a.SP_0008 | ✓ |
| 9 | patient.T3.3.po14a.SD_0003 | ✓ |
| 10 | patient.T4.1.po14a.PO_0005 | ✓ |
Query result 1–10: Patient
Listing 2:
List phlebitis located nearby/on/at/in an anatomical location
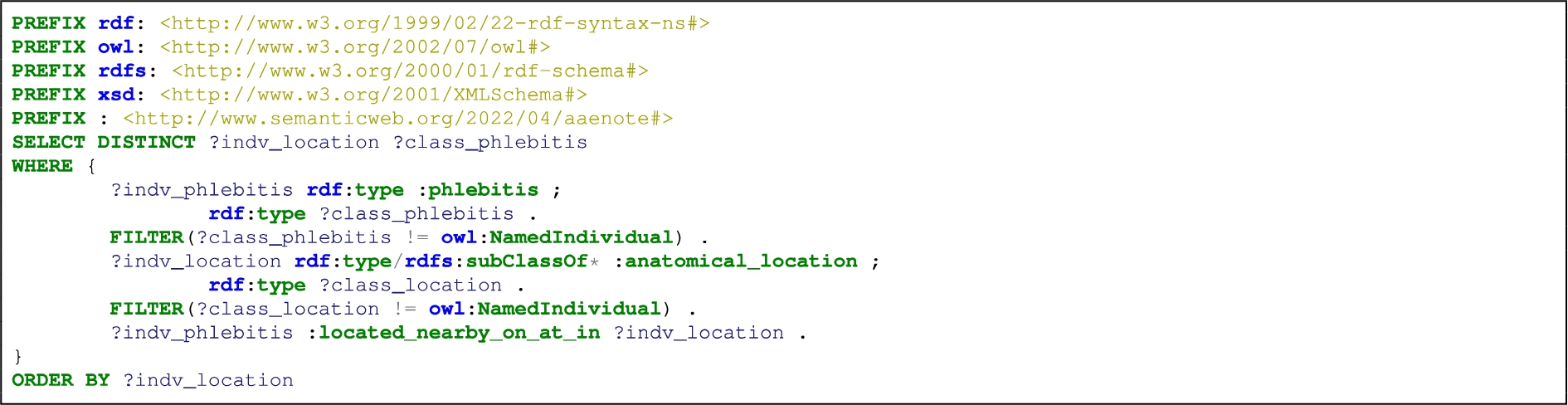
Table 9
AAENOTE SPARQL query result: list phlebitis at an anatomical location
| Query Result | Anatomical Location | Phlebitis |
| 1 | elbow.T1.4.lo22a.DO_0010 | ✓ |
| 2 | elbow.T2.1.do13a.DO_0010 | ✓ |
| 3 | elbow.T2.4.lo12a.DO_0010 | ✓ |
| 4 | elbow.T3.3.so11a.DO_0010 | ✓ |
| 5 | elbow.T3.3.so21a.DO_0010 | ✓ |
| 6 | hand.T3.4.lo12a.SP_0008 | ✓ |
| 7 | hand.T4.3.do13a.PO_0005 | ✓ |
| 8 | hand.T7.2.lo22a.PO_0005 | ✓ |
| 9 | wrist.T4.2.do13a.SP_0008 | ✓ |
| 10 | patient.T4.1.po14a.PO_0005 | ✓ |
Query result 1–10: Listing 2 SPARQL query: Phlebitis
B.5.AAENOTE CQ 2: Does patientA have an infection?
B.5.1.AAENOTE CQ 2 explicit
The patients who have infection are listed in Table 10 using Listing 3. Whereas, patients who have infection and/or other observations are listed in Table 11 using Listing 4.
Listing 3:
List patients who have infection
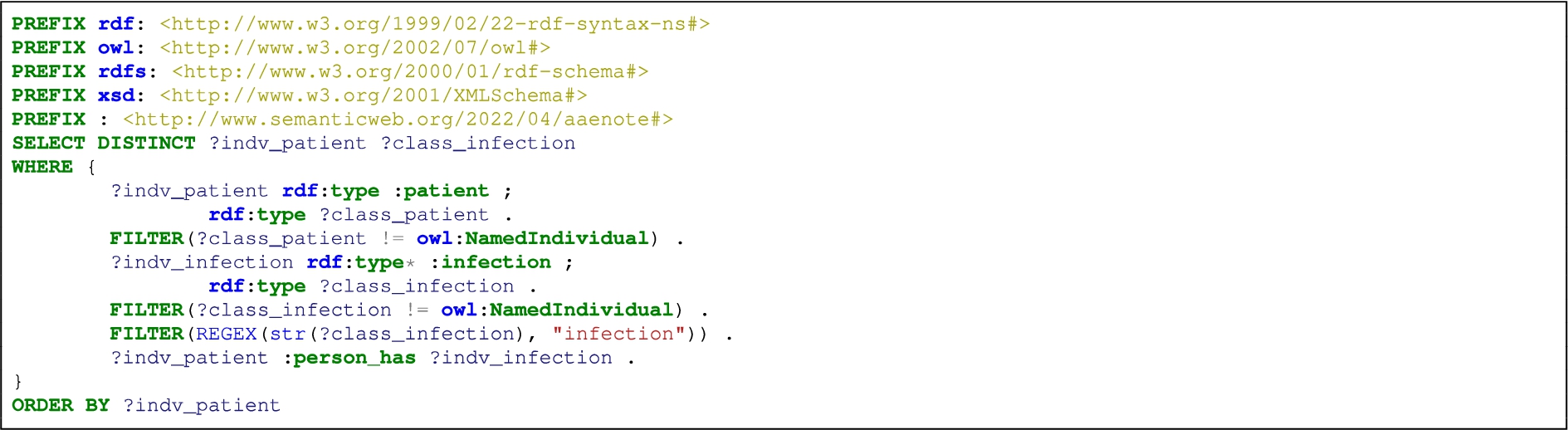
Table 10
AAENOTE SPARQL query result: list patients that have infection
| Query Result | Patient | Infection |
| 1 | patient.T1.2.lo22a.SD_0006 | ✓ |
| 2 | patient.T1.4.lo22a.SP_0002 | ✓ |
| 3 | patient.T10.2.do23a.SP_0007 | ✓ |
| 4 | patient.T12.4.lo12a.SP_0007 | ✓ |
| 5 | patient.T2.2.do23a.SP_0006 | ✓ |
| 6 | patient.T2.2.lo12a.SD_0006 | ✓ |
| 7 | patient.T2.3.do23a.PO_0010 | ✓ |
| 8 | patient.T2.3.po14a.SD_0006 | ✓ |
| 9 | patient.T3.2.do13a.SP_0007 | ✓ |
| 10 | patient.T4.4.lo22a.DO_0008 | ✓ |
| 11 | patient.T4.4.so11a.DP_0010 | ✓ |
| 12 | patient.T5.2.po24a.DO_0008 | ✓ |
| 13 | patient.T5.4.lo22a.SP_0007 | ✓ |
| 14 | patient.T7.3.po24a.SD_0006 | ✓ |
Query result 1–14: Patient
Listing 4:
List patients who have infection and/or other observations
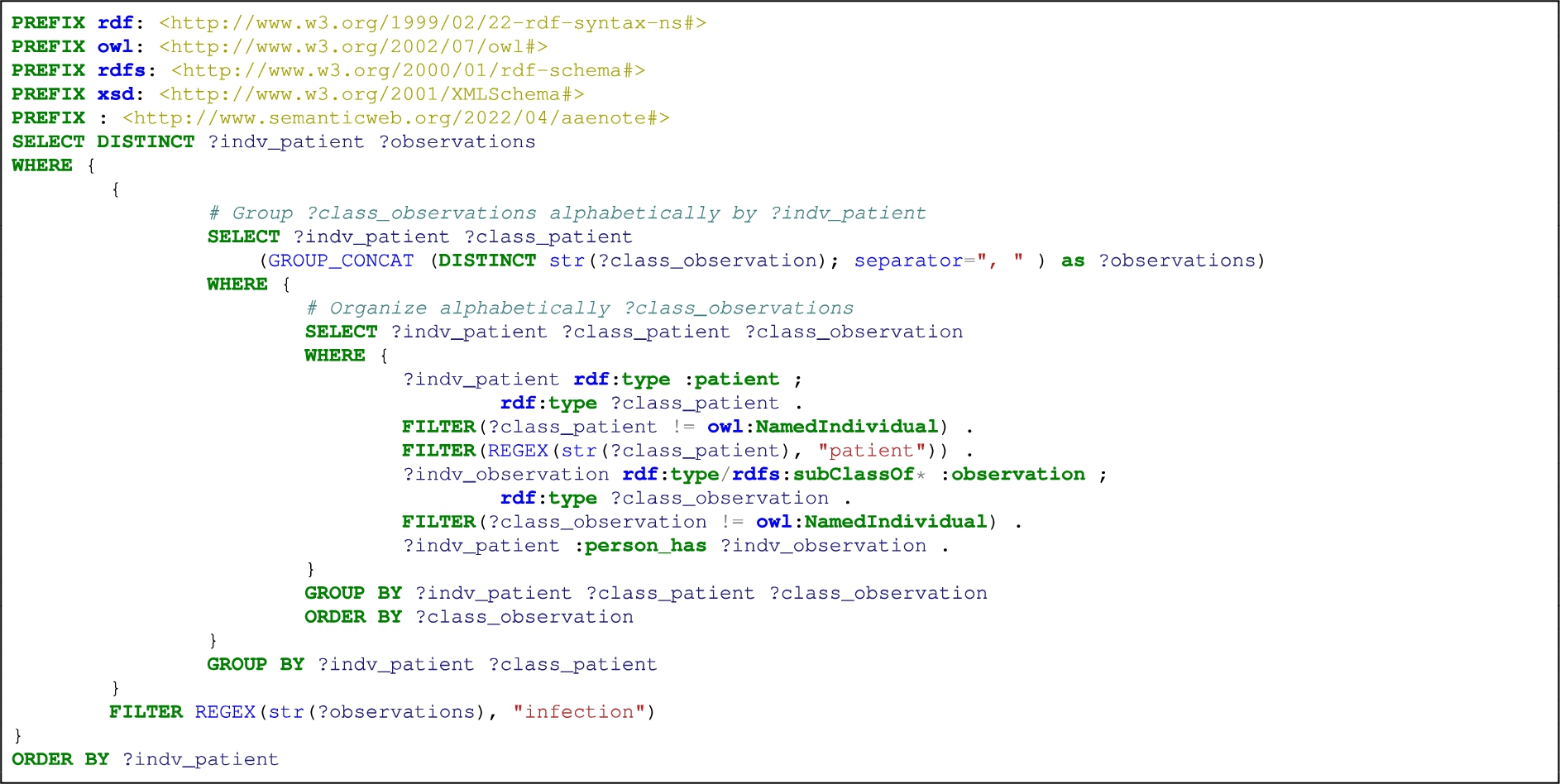
Table 11
AAENOTE SPARQL query result: list patients that have infection and/or another observation
| Person | Observation | ||||||||||||
| Query Result | Patient | blood pressure | body temp | c reactive protein | conciousness level | infection | neurological and physiological | observation | pulse | red | respiratory rate | sepsis | swollen |
| 1 | patient.T1.2.lo22a.SD_0006 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| 2 | patient.T1.4.lo22a.SP_0002 | ✓ | ✓ | ✓ | |||||||||
| 3 | patient.T10.2.do23a.SP_0007 | ✓ | ✓ | ||||||||||
| 4 | patient.T12.4.lo12a.SP_0007 | ✓ | ✓ | ✓ | |||||||||
| 5 | patient.T2.2.do23a.SP_0006 | ✓ | |||||||||||
| 6 | patient.T2.2.lo12a.SD_0006 | ✓ | ✓ | ✓ | |||||||||
| 7 | patient.T2.3.do23a.PO_0010 | ✓ | ✓ | ||||||||||
| 8 | patient.T2.3.po14a.SD_0006 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 9 | patient.T3.2.do13a.SP_0007 | ✓ | ✓ | ✓ | ✓ | ||||||||
| 10 | patient.T4.4.lo22a.DO_0008 | ✓ | ✓ | ✓ | |||||||||
| 11 | patient.T4.4.so11a.DP_0010 | ✓ | ✓ | ||||||||||
| 12 | patient.T5.2.po24a.DO_0008 | ✓ | ✓ | ✓ | |||||||||
| 13 | patient.T5.4.lo22a.SP_0007 | ✓ | ✓ | ✓ | |||||||||
| 14 | patient.T7.3.po24a.SD_0006 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
Query result 1–14: Patient
B.5.2.AAENOTE CQ 2 implicit
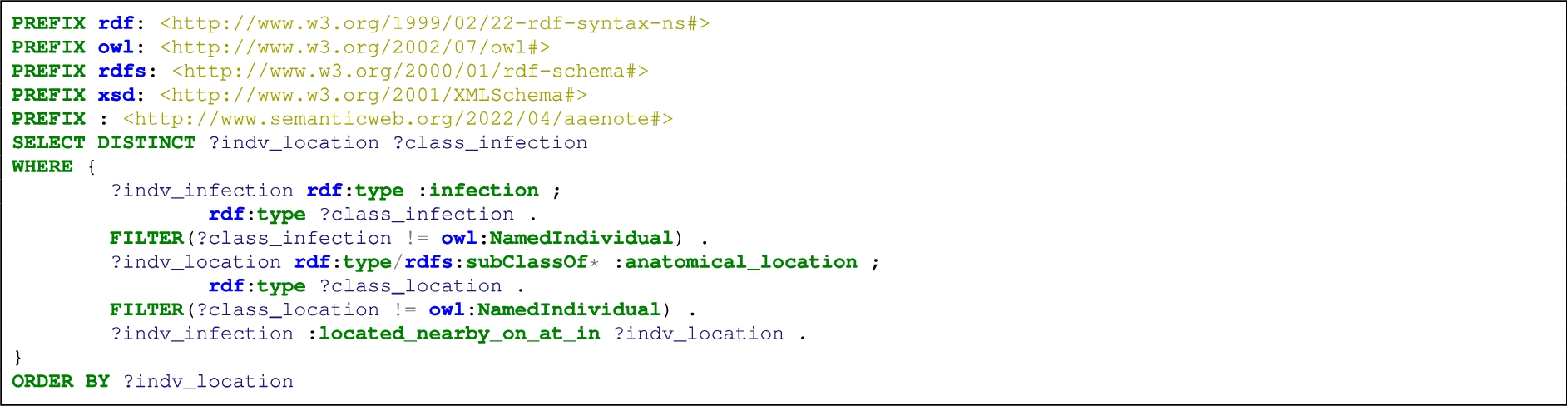
By using anatomical locations it is possible to implicitly identify infection within a patient because the anatomical locations refer to a place on a human and in the context of AE notes anatomical locations commonly refer to a place on a patient. As shown in Table 12, only 1 instance where infection is located at an anatomical location was found using either Listing 5 or Listing 6.
Listing 5:
List infection located nearby/on/at/in an anatomical location
Listing 6:
List infection and other observations located nearby/on/at/in an anatomical location
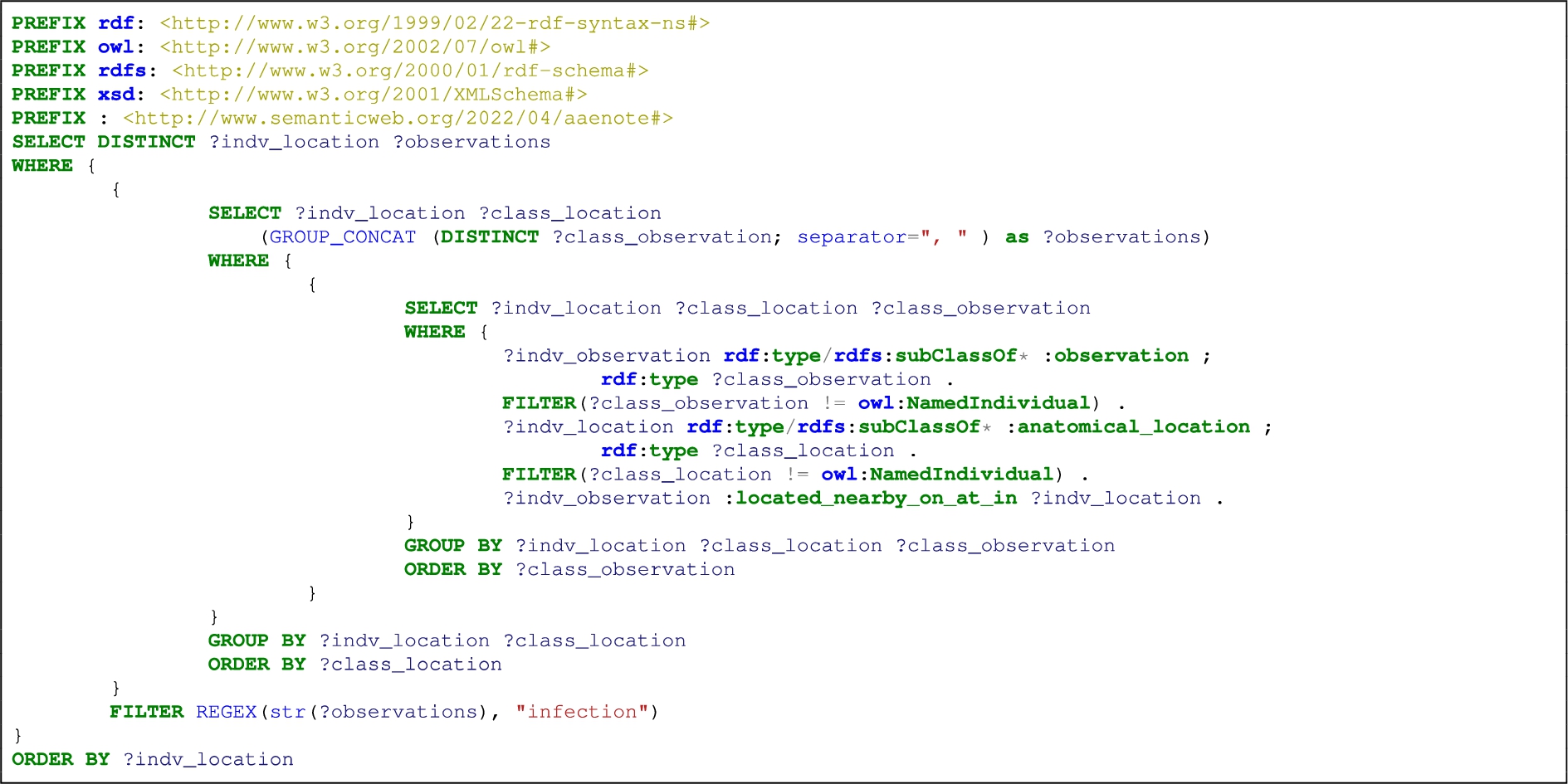
Table 12
AAENOTE SPARQL query result: list infections and/or observations at an anatomical location
| Query Result | Anatomical Location | Infection |
| 1 | skin.T4.2.po14a.SL_0006 | ✓ |
B.6.AAENOTE CQ 3: Does patientA have a BSI?
Cannot determine if there is a BSI without a microbiology laboratory result of a positive blood culture and the cultured bacteria name.
B.7.AAENOTE CQ 4: How many patients have an infection or BSI?
Explicitly, Table 4 shows the number of patients with infection and the number of patients with infection and/or other observations (Listing 7). Implicitly, there was only 1 anatomical location that had infection (Appendix B.5.2), so the results are not shown for the query in Listing 8. If there was clinical knowledge, it could provide the insight required to determine if combinations of observations at certain anatomical locations are indications of an infection (Listing 9 and Table 13). As previously stated in Appendix B.6, BSI cannot be determined because this requires microbiology laboratory blood test results.
Listing 7:
Count the number of patients with infection and number patients with infection and other observations
Listing 8:
Count the number of anatomical locations where infection and other observations are located nearby/on/at/in that anatomical location
Listing 9:
Count the number of anatomical locations with the same observations located nearby/on/at/in that anatomical location
Table 13
AAENOTE SPARQL results for anatomical location with combinations of observations
| Anatomical Location | Observation | |||||||||||||||
| Query Result | Instances | arm | elbow | hand | skin | body temp | edema | infection | mobility impairment | pain | phlebitis | purulence | red | swollen | warm | wound |
| 1 | 12 | ✓ | ✓ | |||||||||||||
| 2 | 7 | ✓ | ✓ | |||||||||||||
| 3 | 6 | ✓ | ✓ | ✓ | ||||||||||||
| 4 | 4 | ✓ | ✓ | ✓ | ||||||||||||
| 5 | 3 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 6 | 2 | ✓ | ✓ | ✓ | ||||||||||||
| 7 | 2 | ✓ | ✓ | |||||||||||||
| 8 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 9 | 1 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 10 | 1 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| 11 | 1 | ✓ | ✓ | |||||||||||||
| 12 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 13 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 14 | 1 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 15 | 7 | ✓ | ✓ | |||||||||||||
| 16 | 7 | ✓ | ✓ | |||||||||||||
| 17 | 7 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 18 | 6 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 19 | 5 | ✓ | ✓ | ✓ | ||||||||||||
| 20 | 4 | ✓ | ✓ | |||||||||||||
| 21 | 3 | ✓ | ✓ | |||||||||||||
| 22 | 2 | ✓ | ✓ | ✓ | ||||||||||||
| 23 | 1 | ✓ | ✓ | |||||||||||||
| 24 | 1 | ✓ | ✓ | |||||||||||||
| 25 | 4 | ✓ | ✓ | |||||||||||||
| 26 | 3 | ✓ | ✓ | |||||||||||||
| 27 | 2 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 28 | 1 | ✓ | ✓ | |||||||||||||
| 29 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 30 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 31 | 3 | ✓ | ✓ | |||||||||||||
| 32 | 3 | ✓ | ✓ | |||||||||||||
| 33 | 2 | ✓ | ✓ | ✓ | ||||||||||||
| 34 | 2 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 35 | 2 | ✓ | ✓ | |||||||||||||
| 36 | 2 | ✓ | ✓ | ✓ | ||||||||||||
| 37 | 1 | ✓ | ✓ | |||||||||||||
| 38 | 1 | ✓ | ✓ | |||||||||||||
| 39 | 1 | ✓ | ✓ | ✓ | ||||||||||||
| 40 | 1 | ✓ | ✓ | ✓ | ✓ | |||||||||||
Query result 1–40: Observation(s)
B.8.AAENOTE CQ 5: Which patients have sepsis?
Explicitly, 5 patients have sepsis (Table 14, Listing 10) and 3 of the 5 patients with sepsis have sepsis and another observation (Table 15, Listing 11). Additional clinical knowledge is needed to determine if other observations combined without the sepsis class are indications of sepsis.
Listing 10:
List patients who have sepsis
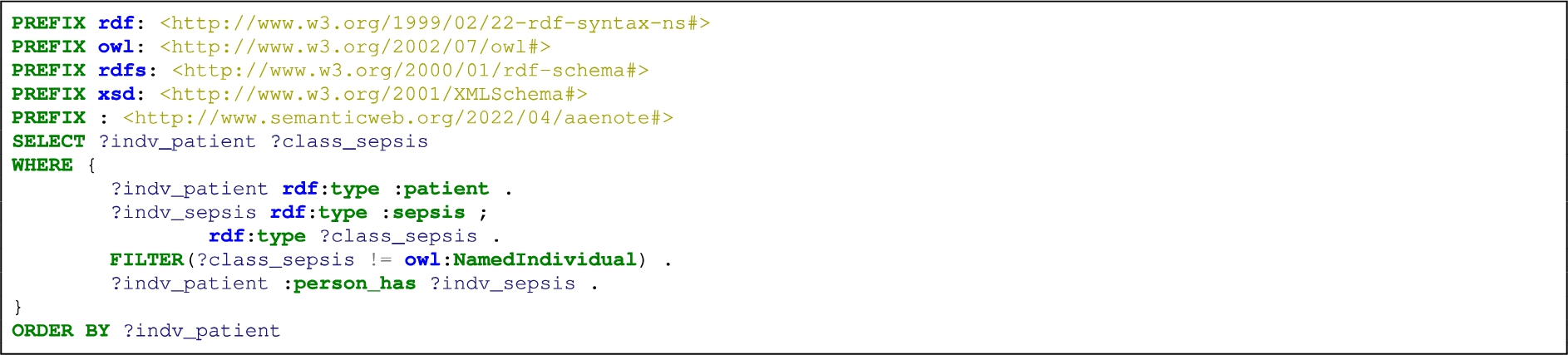
Table 14
AAENOTE SPARQL query result: list patients that have sepsis
| Query Result | Patient | Sepsis |
| 1 | patient.T1.2.do13a.SP_0006 | ✓ |
| 2 | patient.T1.4.lo12a.SP_0006 | ✓ |
| 3 | patient.T6.3.lo22a.DP_0010 | ✓ |
| 4 | patient.T7.2.po24a.SL_0004 | ✓ |
| 5 | patient.T7.3.po24a.SD_0006 | ✓ |
Query result 1–5: Patient
Listing 11:
List patients that have sepsis and/or other observations
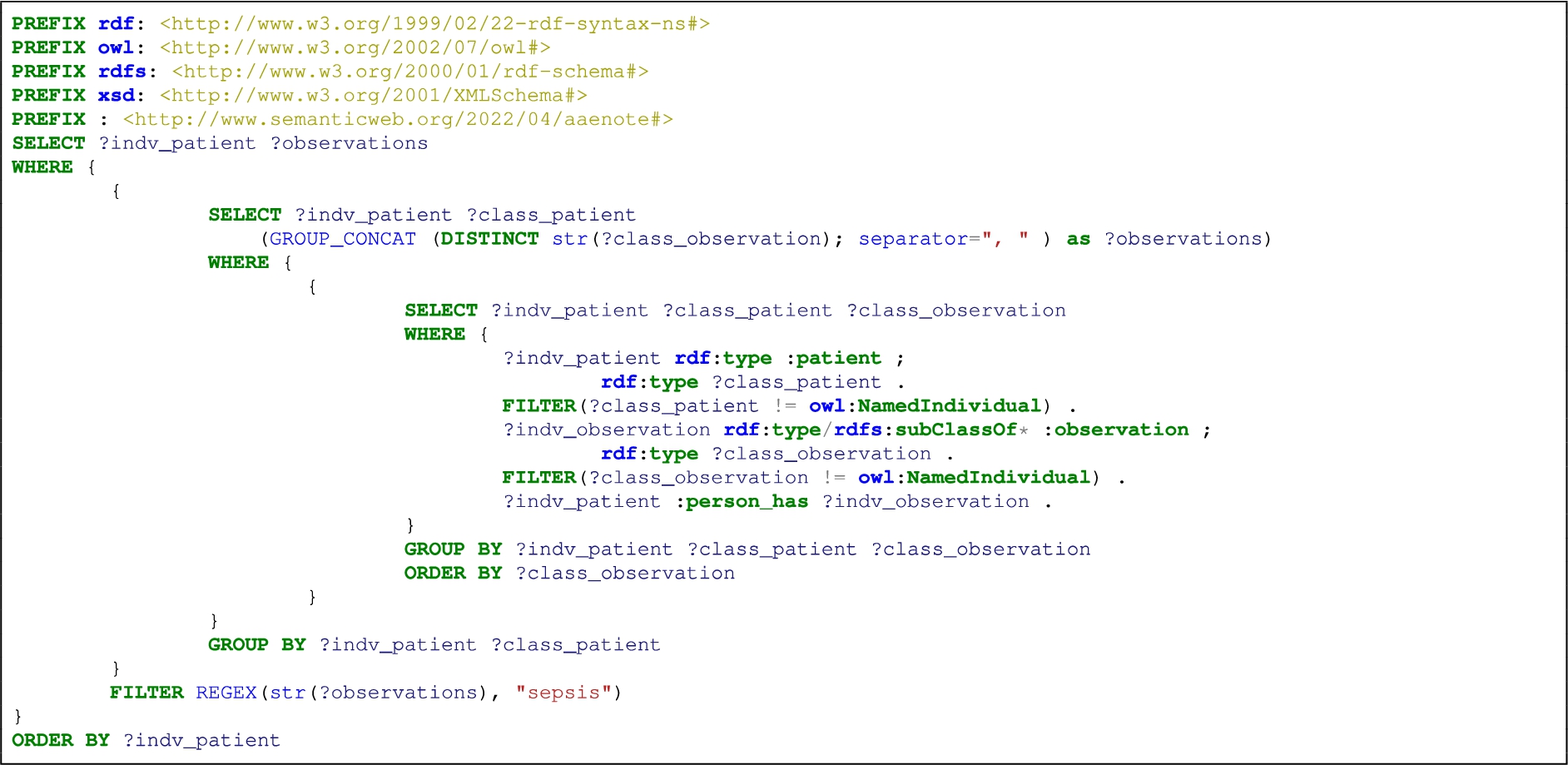
Table 15
AAENOTE SPARQL query result: list patients that have sepsis and/or another observation
| Person | Observation | |||||||||
| Query Result | Patient | blood pressure | body temp | c reactive protein | infection | pulse | red | respiratory rate | sepsis | swollen |
| 1 | patient.T1.2.do13a.SP_0006 | ✓ | ||||||||
| 2 | patient.T1.4.lo12a.SP_0006 | ✓ | ||||||||
| 3 | patient.T6.3.lo22a.DP_0010 | ✓ | ✓ | |||||||
| 4 | patient.T7.2.po24a.SL_0004 | ✓ | ✓ | ✓ | ✓ | |||||
| 5 | patient.T7.3.po24a.SD_0006 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
Query result 1–5: Patient
B.9.AAENOTE CQ 6: Does patientB have a catheter?
The patient and the type of catheter a patient has can be found explicitly using Listing 12. A subset of the results are in Table 16, where each patient individual is listed with a type of catheter and how many catheters of that specific type are present. Thus, the same patient can be listed multiple times as seen in Table 16’s Query Result 28–30 where the same patient is listed 3 times because the patient has 3 catheters of different types. Implicitly, an anatomical location with a catheter indicates a person has a catheter (Listing 13, Table 17). Additional clinical knowledge is needed to determine if other observations combined indicate a catheter is present.
Listing 12:
List patients that have a catheter, the catheter’s type, and the number of that catheter type
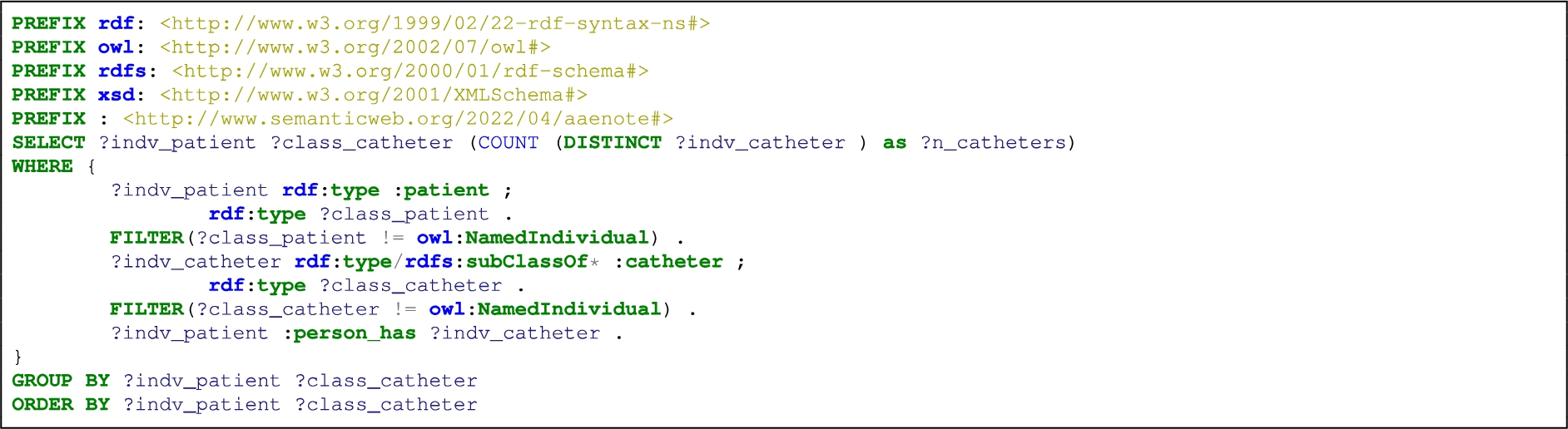
Table 16
AAENOTE SPARQL query result: list of patients with a catheter
| Person | Catheter | ||||||||||
| Query Result | Number of specific catheters | Patient | catheter | central venous catheter | epidural catheter | hickman catheter | hemodialysis catheter | peripheral intravenous catheter | urinary catheter | vas catheter | venous catheter |
| 1 | 1 | patient.T1.1.lo12a.LO_0007 | ✓ | ||||||||
| 2 | 1 | patient.T1.1.lo22a.LO_0007 | ✓ | ||||||||
| 3 | 1 | patient.T1.1.lo22a.LO_0009 | ✓ | ||||||||
| 4 | 1 | patient.T1.2.do13a.LO_0001 | ✓ | ||||||||
| 5 | 1 | patient.T1.2.do13a.SP_0001 | ✓ | ||||||||
| 6 | 1 | patient.T1.2.do13a.SP_0005 | ✓ | ||||||||
| 7 | 1 | patient.T1.2.do13a.SP_0006 | ✓ | ||||||||
| 8 | 1 | patient.T1.2.do13a.SP_0010 | ✓ | ||||||||
| 9 | 1 | patient.T1.2.lo12a.PO_0005 | ✓ | ||||||||
| 10 | 1 | patient.T1.2.lo12a.SD_0007 | ✓ | ||||||||
| 11 | 1 | patient.T1.2.lo22a.SD_0002 | ✓ | ||||||||
| 12 | 1 | patient.T1.2.lo22a.SD_0007 | ✓ | ||||||||
| 13 | 1 | patient.T1.2.po24a.DO_0001 | ✓ | ||||||||
| ... | |||||||||||
| 22 | 1 | patient.T1.4.lo12a.SP_0003 | ✓ | ||||||||
| 23 | 1 | patient.T1.4.lo22a.DO_0003 | ✓ | ||||||||
| 24 | 1 | patient.T1.4.lo22a.SP_0005 | ✓ | ||||||||
| 25 | 1 | patient.T1.4.lo22a.SP_0006 | ✓ | ||||||||
| 26 | 1 | patient.T1.4.lo22a.SP_0010 | ✓ | ||||||||
| 27 | 1 | patient.T1.4.po24a.LD_0004 | ✓ | ||||||||
| 28 | 1 | patient.T1.4.po24a.LD_0009 | ✓ | ||||||||
| 29 | 1 | patient.T1.4.po24a.LD_0009 | ✓ | ||||||||
| 30 | 1 | patient.T1.4.po24a.LD_0009 | ✓ | ||||||||
| ... | |||||||||||
| 93 | 1 | patient.T3.4.so11a.LO_0003 | ✓ | ||||||||
| 94 | 1 | patient.T3.4.so21a.LO_0004 | ✓ | ||||||||
| 95 | 2 | patient.T4.1.lo22a.LO_0003 | ✓ | ||||||||
| ... | |||||||||||
| 138 | 1 | patient.T9.2.so11a.LD_0003 | ✓ | ||||||||
| 139 | 1 | patient.T9.3.po24a.SD_0005 | ✓ | ||||||||
Query result 1–139: Patient
Query result 28–30, same patient but different catheters.
Query result 95, the patient has 2 PIVCs.
Listing 13:
List the anatomical location and the type of catheter located nearby/on/at/in there
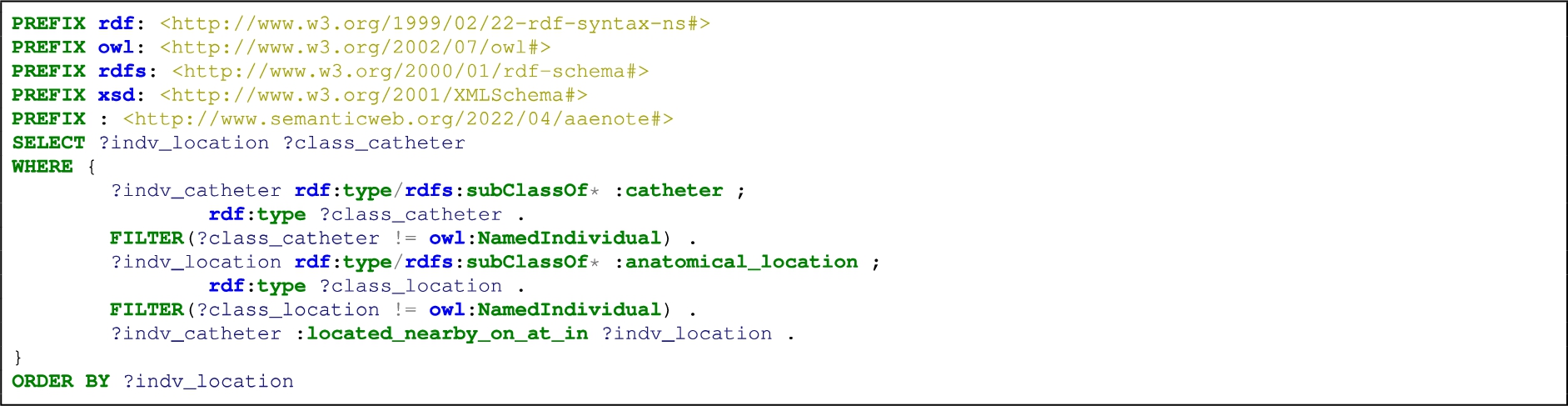
Table 17
AAENOTE SPARQL query result: list anatomical locations with catheters
| Anatomical Location | Catheter | |||
| Query Result | Individuals under class | catheter | venous catheter | peripheral intravenous catheter |
| 1 | arm.T14.3.po24a.SD_0002 | ✓ | ||
| 2 | arm.T2.3.po24a.LO_0002 | ✓ | ||
| 3 | arm.T2.3.po24a.SD_0001 | ✓ | ||
| 4 | arm.T3.3.po24a.LO_0005 | ✓ | ||
| 5 | arm.T5.3.po24a.LO_0004 | ✓ | ||
| 6 | arm.T5.3.po24a.SD_0003 | ✓ | ||
| 7 | arm.T5.3.so11a.DO_0002 | ✓ | ||
| 8 | arm.T5.4.lo12a.DO_0003 | ✓ | ||
| 9 | arm.T5.4.lo22a.DO_0003 | ✓ | ||
| … | ||||
| 14 | arm.T9.4.lo12a.DO_0003 | ✓ | ||
| 15 | body_part.T8.3.po14a.LO_0004 | ✓ | ||
| 16 | elbow.T2.2.lo12a.SD_0001 | ✓ | ||
| … | ||||
| 69 | hand.T9.2.so21a.LD_0003 | ✓ | ||
| 70 | navel.T5.3.so11a.LP_0010 | ✓ | ||
| 71 | navel.T5.4.do23a.LP_0010 | ✓ | ||
| 72 | skin.T11.3.po24a.LO_0001 | ✓ | ||
| 73 | skin.T5.2.do23a.LO_0005 | ✓ | ||
| 74 | subcutaneous.T12.2.do23a.LO_0004 | ✓ | ||
| 75 | wrist.T2.2.do13a.LO_0005 | ✓ | ||
| 76 | wrist.T3.2.do23a.LO_0005 | ✓ | ||
| 77 | wrist.T3.4.so11a.LO_0005 | ✓ | ||
| 78 | wrist.T7.3.po14a.LO_0005 | ✓ | ||
Query result 1–78: Catheter
B.10.AAENOTE CQ 7: Does patientB have a PIVC?
This competency question (CQ) can be answered similarily to Appendix B.9. Explicitly using Listing 14 (Table 18) and implicitly using Listing 15 (Table 19). Likewise, additional clinical knowledge is needed to determine if other observations combined indicate a PIVC is present.
Listing 14:
List patients that have a PIVC and number of PIVCs
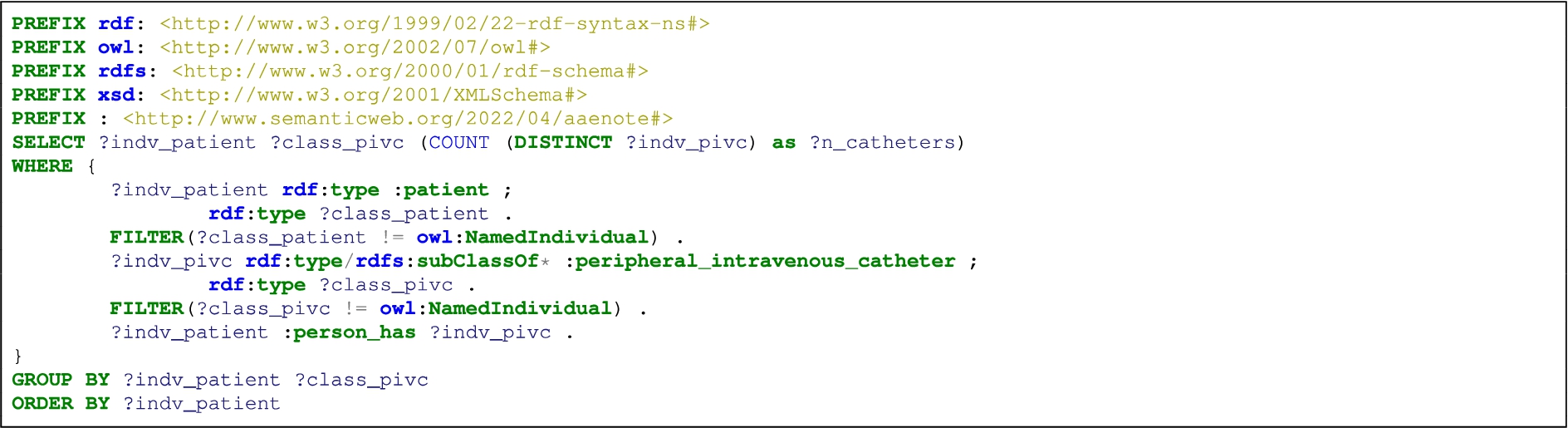
Table 18
AAENOTE SPARQL query result: list patients that have a PIVC
| Query Result | Number of PIVCs | Patient | peripheral intravenous catheter |
| 1 | 1 | patient.T1.1.lo12a.LO_0007 | ✓ |
| 2 | 1 | patient.T1.1.lo22a.LO_0007 | ✓ |
| 3 | 1 | patient.T1.2.do13a.LO_0001 | ✓ |
| 4 | 1 | patient.T1.2.do13a.SP_0005 | ✓ |
| 5 | 1 | patient.T1.2.do13a.SP_0006 | ✓ |
| … | |||
| 31 | 1 | patient.T2.1.lo22a.LO_0001 | ✓ |
| 32 | 2 | patient.T2.1.lo22a.LO_0003 | ✓ |
| 33 | 1 | patient.T2.2.do23a.LO_0001 | ✓ |
| … | |||
| 91 | 1 | patient.T8.4.lo22a.SP_0010 | ✓ |
| 92 | 1 | patient.T9.2.so11a.LD_0003 | ✓ |
| 93 | 1 | patient.T9.3.po24a.SD_0005 | ✓ |
Query result 1–93: Patient
Listing 15:
List anatomical locations with a PIVC
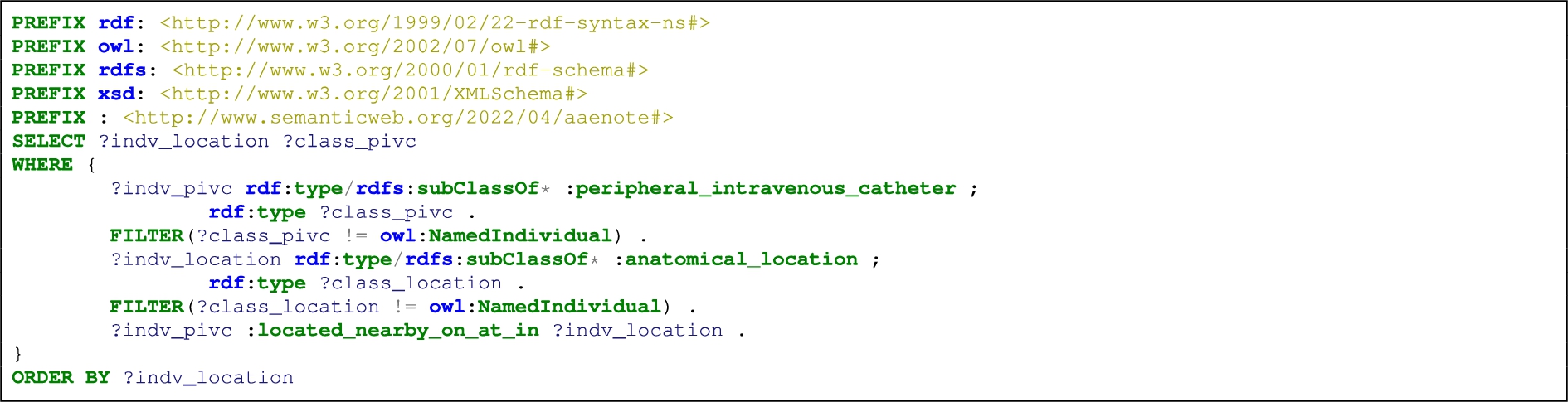
Table 19
AAENOTE SPARQL query result: list anatomical locations with a PIVC
| Anatomical Location | Catheter | |
| Query Result | Individuals under class | peripheral intravenous catheter |
| 1 | arm.T14.3.po24a.SD_0002 | ✓ |
| 2 | arm.T2.3.po24a.LO_0002 | ✓ |
| 3 | arm.T2.3.po24a.SD_0001 | ✓ |
| 4 | arm.T3.3.po24a.LO_0005 | ✓ |
| 5 | arm.T5.3.po24a.LO_0004 | ✓ |
| … | ||
| 14 | body_part.T8.3.po14a.LO_0004 | ✓ |
| 15 | elbow.T2.2.lo12a.SD_0001 | ✓ |
| 16 | elbow.T2.2.lo22a.SD_0001 | ✓ |
| … | ||
| 67 | hand.T7.2.lo22a.PO_0005 | ✓ |
| 68 | hand.T9.2.so21a.LD_0003 | ✓ |
| 69 | skin.T11.3.po24a.LO_0001 | ✓ |
| 70 | skin.T5.2.do23a.LO_0005 | ✓ |
| 71 | subcutaneous.T12.2.do23a.LO_0004 | ✓ |
| 72 | wrist.T2.2.do13a.LO_0005 | ✓ |
| 73 | wrist.T3.2.do23a.LO_0005 | ✓ |
| 74 | wrist.T3.4.so11a.LO_0005 | ✓ |
| 75 | wrist.T7.3.po14a.LO_0005 | ✓ |
Query result 1–75: PIVC
B.11.AAENOTE CQ 8a: How many catheters does patientB have?
Listing 16 is used to explicitly query the number and types of catheters a patient has as shown in Table 20. Sometimes there is a direct relationship between a person and multiple catheters such as in Query Result 28, 30, 45, and 52 of Table 20. Whereas, typically there is only one direct relationship between one catheter and an anatomical location when using the implicit query Listing 17 (Table 21). Similarly to Appendix B.7 where with clinical knowledge it could be possible to identify infection indications based on a combination of observations at a certain anatomical location, it could also be possible to determine if combinations of observations at certain anatomical locations are indications of a catheter.
Listing 16:
Count the number of catheters a patient has and provide the types of catheters
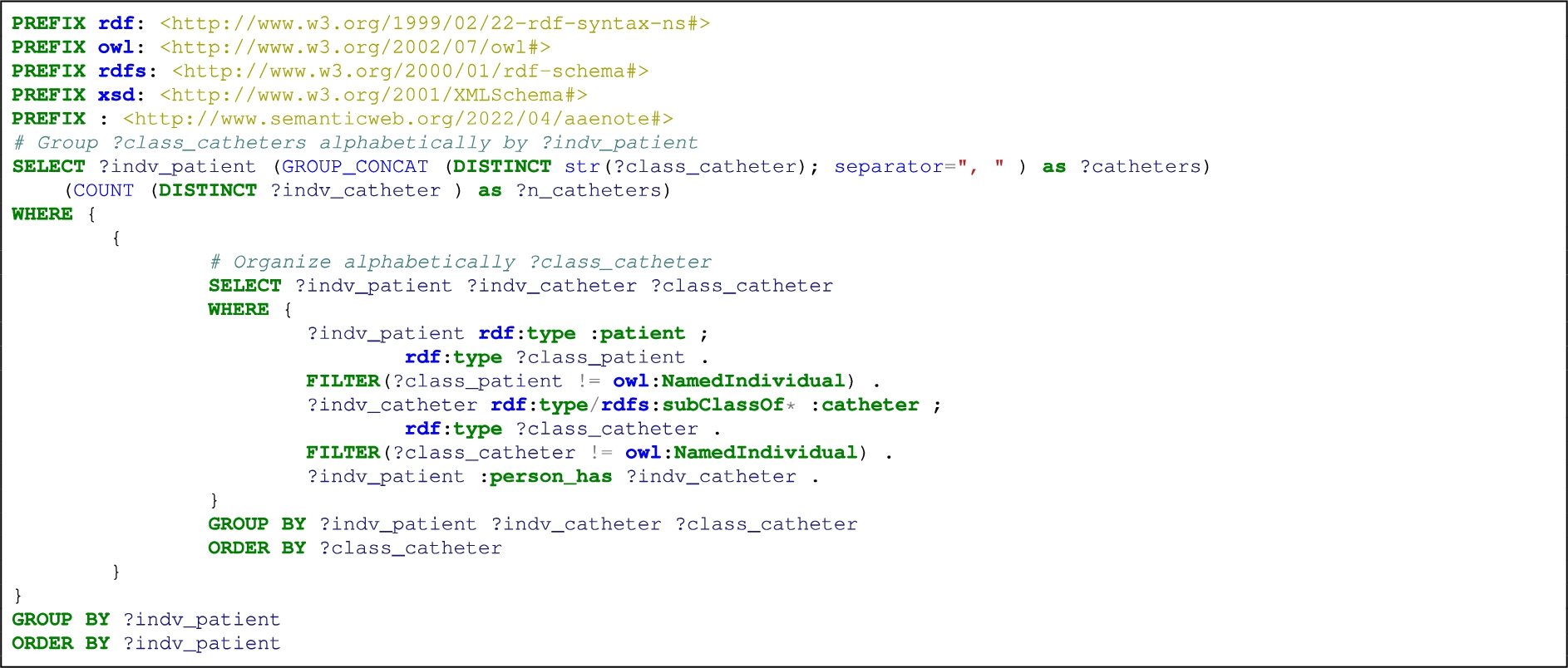
Table 20
AAENOTE SPARQL query result: list how many catheters and type of catheter a patient has
| Person | Catheter | ||||||||||
| Query Results | Number of catheters | Patient | catheter | central venous catheter | epidural catheter | hickman catheter | hemodialysis catheter | peripheral intravenous catheter | urinary catheter | vas catheter | venous catheter |
| 1 | 1 | patient.T1.1.lo12a.LO_0007 | ✓ | ||||||||
| 2 | 1 | patient.T1.1.lo22a.LO_0007 | ✓ | ||||||||
| 3 | 1 | patient.T1.1.lo22a.LO_0009 | ✓ | ||||||||
| 4 | 1 | patient.T1.2.do13a.LO_0001 | ✓ | ||||||||
| 5 | 1 | patient.T1.2.do13a.SP_0001 | ✓ | ||||||||
| 6 | 1 | patient.T1.2.do13a.SP_0005 | ✓ | ||||||||
| 7 | 1 | patient.T1.2.do13a.SP_0006 | ✓ | ||||||||
| 8 | 1 | patient.T1.2.do13a.SP_0010 | ✓ | ||||||||
| 9 | 1 | patient.T1.2.lo12a.PO_0005 | ✓ | ||||||||
| 10 | 1 | patient.T1.2.lo12a.SD_0007 | ✓ | ||||||||
| 11 | 1 | patient.T1.2.lo22a.SD_0002 | ✓ | ||||||||
| 12 | 1 | patient.T1.2.lo22a.SD_0007 | ✓ | ||||||||
| 13 | 1 | patient.T1.2.po24a.DO_0001 | ✓ | ||||||||
| … | |||||||||||
| 26 | 1 | patient.T1.4.lo22a.SP_0010 | ✓ | ||||||||
| 27 | 1 | patient.T1.4.po24a.LD_0004 | ✓ | ||||||||
| 28 | 4 | patient.T1.4.po24a.LD_0009 | ✓ | ✓ | ✓ | ✓ | |||||
| 29 | 1 | patient.T1.4.po24a.SO_0009 | ✓ | ||||||||
| 30 | 2 | patient.T1.4.so11a.DP_0002 | ✓ | ✓ | |||||||
| … | |||||||||||
| 45 | 2 | patient.T2.1.lo22a.LO_0003 | ✓ | ||||||||
| 46 | 1 | patient.T2.2.do13a.SP_0003 | ✓ | ||||||||
| 47 | 1 | patient.T2.2.do23a.LO_0001 | ✓ | ||||||||
| 48 | 1 | patient.T2.2.do23a.LO_0007 | ✓ | ||||||||
| 49 | 1 | patient.T2.2.do23a.SP_0006 | ✓ | ||||||||
| 50 | 1 | patient.T2.2.lo22a.PO_0005 | ✓ | ||||||||
| 51 | 1 | patient.T2.2.po14a.DO_0002 | ✓ | ||||||||
| 52 | 3 | patient.T2.2.so11a.LD_0009 | ✓ | ✓ | ✓ | ||||||
| 53 | 1 | patient.T2.2.so11a.PO_0005 | ✓ | ||||||||
| … | |||||||||||
| 70 | 1 | patient.T3.2.do23a.SP_0003 | ✓ | ||||||||
| 71 | 1 | patient.T3.2.po14a.DO_0001 | ✓ | ||||||||
| 72 | 1 | patient.T3.2.po14a.DO_0003 | ✓ | ||||||||
| 73 | 1 | patient.T3.2.so11a.LD_0003 | ✓ | ||||||||
| 74 | 1 | patient.T3.2.so11a.LD_0004 | ✓ | ||||||||
| 75 | 1 | patient.T3.3.do13a.SL_0002 | ✓ | ||||||||
| … | |||||||||||
| 131 | 1 | patient.T9.2.so11a.LD_0003 | ✓ | ||||||||
| 132 | 1 | patient.T9.3.po24a.SD_0005 | ✓ | ||||||||
Query result 1–132: Patient
Listing 17:
Count the number of catheters located nearby/on/at/in an anatomical location and provide the types of catheters
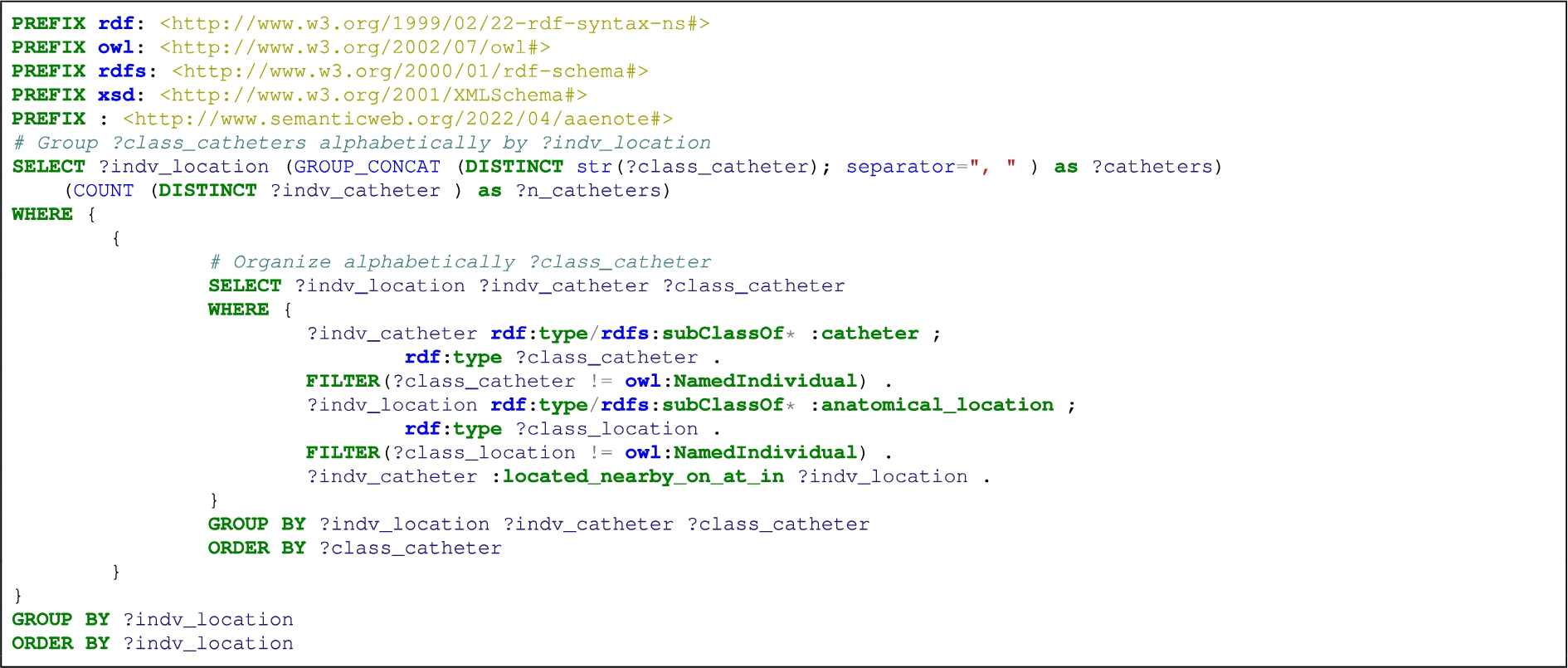
Table 21
AAENOTE SPARQL query result: list how many catheters and type of catheter an anatomical location has
| Anatomical Location | Catheter | ||||
| Query Results | Number of catheters | Individuals under class | catheter | peripheral intravenous catheter | venous catheter |
| 1 | 1 | arm.T14.3.po24a.SD_0002 | ✓ | ||
| 2 | 1 | arm.T2.3.po24a.LO_0002 | ✓ | ||
| 3 | 1 | arm.T2.3.po24a.SD_0001 | ✓ | ||
| 4 | 1 | arm.T3.3.po24a.LO_0005 | ✓ | ||
| 5 | 1 | arm.T5.3.po24a.LO_0004 | ✓ | ||
| 6 | 1 | arm.T5.3.po24a.SD_0003 | ✓ | ||
| 7 | 1 | arm.T5.3.so11a.DO_0002 | ✓ | ||
| 8 | 1 | arm.T5.4.lo12a.DO_0003 | ✓ | ||
| 9 | 1 | arm.T5.4.lo22a.DO_0003 | ✓ | ||
| … | |||||
| 14 | 1 | arm.T9.4.lo12a.DO_0003 | ✓ | ||
| 15 | 1 | body_part.T8.3.po14a.LO_0004 | ✓ | ||
| 16 | 1 | elbow.T2.2.lo12a.SD_0001 | ✓ | ||
| … | |||||
| 67 | 1 | hand.T6.3.do23a.PO_0005 | ✓ | ||
| 68 | 1 | hand.T7.2.lo22a.PO_0005 | ✓ | ||
| 69 | 1 | hand.T9.2.so21a.LD_0003 | ✓ | ||
| 70 | 1 | navel.T5.3.so11a.LP_0010 | ✓ | ||
| 71 | 1 | navel.T5.4.do23a.LP_0010 | ✓ | ||
| 72 | 1 | skin.T11.3.po24a.LO_0001 | ✓ | ||
| 73 | 1 | skin.T5.2.do23a.LO_0005 | ✓ | ||
| 74 | 1 | subcutaneous.T12.2.do23a.LO_0004 | ✓ | ||
| 75 | 1 | wrist.T2.2.do13a.LO_0005 | ✓ | ||
| 76 | 1 | wrist.T3.2.do23a.LO_0005 | ✓ | ||
| 77 | 1 | wrist.T3.4.so11a.LO_0005 | ✓ | ||
| 78 | 1 | wrist.T7.3.po14a.LO_0005 | ✓ | ||
Query result 1–78: Catheter
B.12.AAENOTE CQ 8b: Where are the catheters in patientB?
Explicitly Listing 18 and Table 22. Implicitly, it is the same as Appendix B.9’s Listing 13 and Table 17 where catheter located at an anatomical location indicates a person has the catheter. Here also, additional clinical knowledge is needed to determine if other observations combined indicate a catheter is present.
Listing 18:
List patients that have an anatomical location, a catheter, and the patient’s catheter is located nearby/on/at/in the patient’s anatomical location
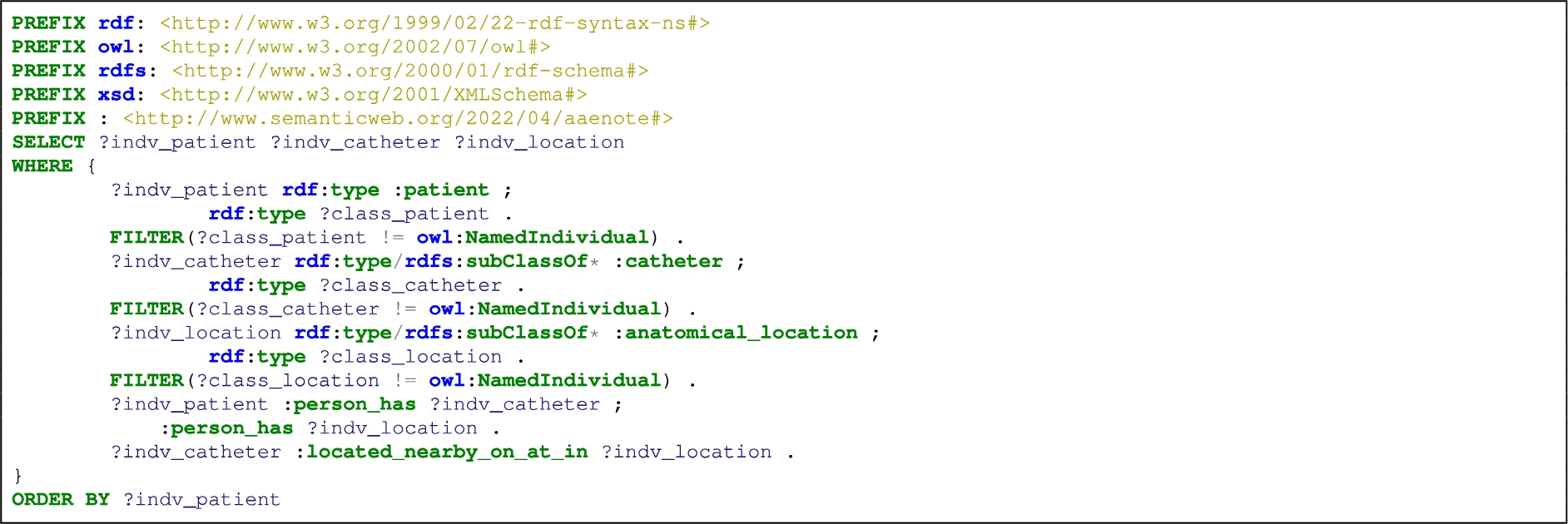
Table 22
AAENOTE SPARQL query result: patient has an anatomical location, patient has a catheter, and that catheter is at the patient’s anatomical location
| Query Result | Patient | Catheter | Anatomical Location |
| 1 | patient.T1.4.lo22a.DO_0003 | venous_catheter.T6.4.lo22a.DO_0003 | arm.T5.4.lo22a.DO_0003 |
| 2 | patient.T4.2.lo22a.SD_0003 | peripheral_intravenous_catheter.T5.2.lo22a.SD_0003 | hand.T6.2.lo22a.SD_0003 |
Query result 1–2: Patient Ⓧ
B.13.AAENOTE CQ 8c: Why does patientB need the catheter(s)?
Listing 19:
List patients that have a catheter and the procedures which use that catheter
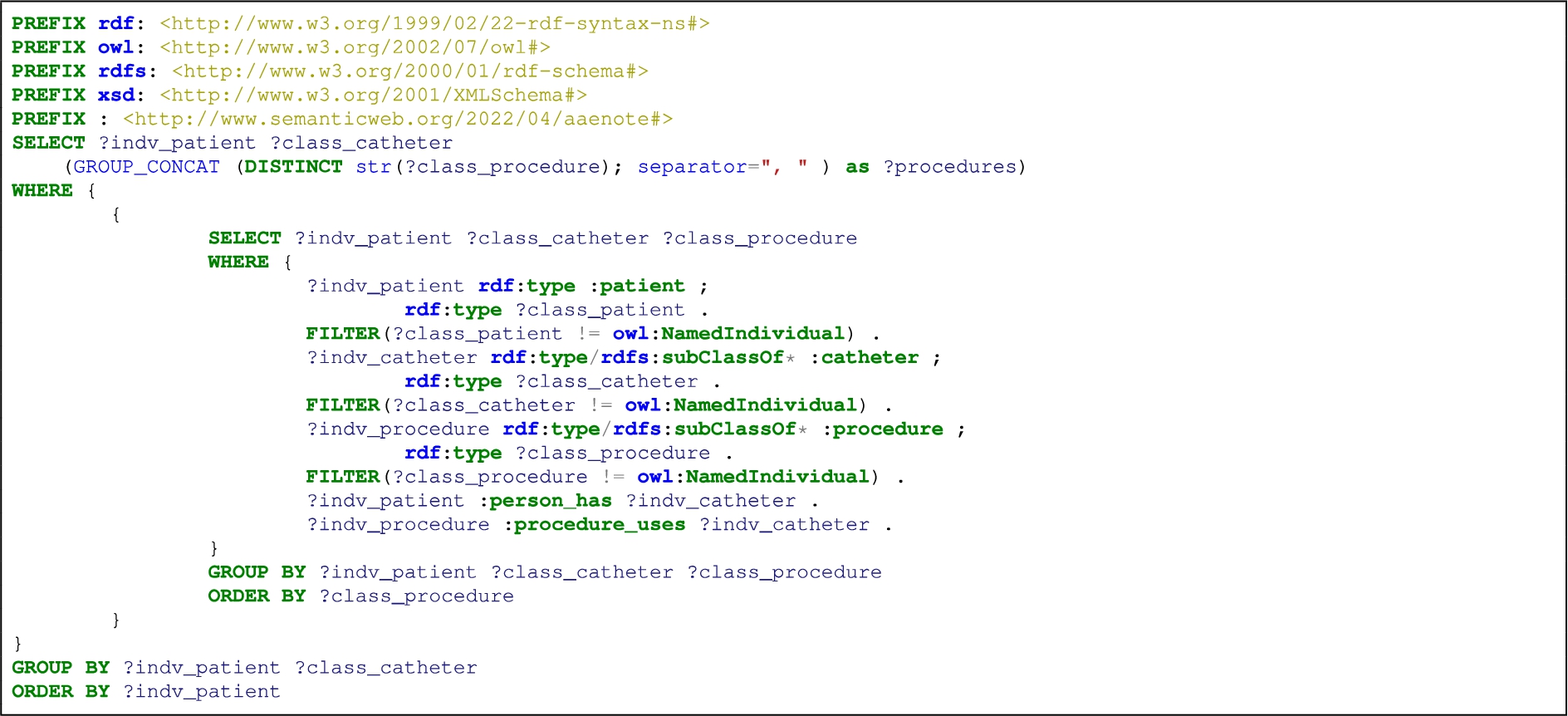
Table 23
AAENOTE SPARQL query result: list patients that have a catheter which was used for a procedure
| Person | Catheter | Procedure | |||||||||||||||
| Query Results | Patient | central venous catheter | epidural catheter | peripheral intravenous catheter | venous catheter | urinary catheter | administration purpose | catheter discontinue use | catheter rinse | catheter self removal | general iv | iv antibiotics | iv chemo | iv fluid | iv medication | iv nutrient | subcutaneous injection |
| 1 | patient.T1.1.lo12a.LO_0007 | ✓ | ✓ | ||||||||||||||
| 2 | patient.T1.1.lo22a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||||
| 3 | patient.T1.2.do13a.LO_0001 | ✓ | ✓ | ||||||||||||||
| 4 | patient.T1.4.lo12a.DO_0003 | ✓ | ✓ | ||||||||||||||
| 5 | patient.T1.4.lo12a.SP_0003 | ✓ | ✓ | ||||||||||||||
| 6 | patient.T1.4.lo22a.DO_0003 | ✓ | ✓ | ||||||||||||||
| 7 | patient.T1.4.lo22a.SP_0010 | ✓ | ✓ | ✓ | |||||||||||||
| 8 | patient.T1.4.so11a.DP_0002 | ✓ | ✓ | ||||||||||||||
| 9 | patient.T1.4.so11a.DP_0002 | ✓ | ✓ | ||||||||||||||
| 10 | patient.T1.4.so11a.LO_0001 | ✓ | ✓ | ||||||||||||||
| 11 | patient.T11.1.lo22a.LO_0004 | ✓ | ✓ | ||||||||||||||
| 12 | patient.T12.4.so11a.LO_0003 | ✓ | ✓ | ||||||||||||||
| 13 | patient.T2.2.do23a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||||
| 14 | patient.T2.3.so11a.LP_0007 | ✓ | ✓ | ||||||||||||||
| 15 | patient.T2.3.so21a.LP_0004 | ✓ | ✓ | ||||||||||||||
| 16 | patient.T2.4.lo22a.DO_0001 | ✓ | ✓ | ||||||||||||||
| 17 | patient.T2.4.so11a.DP_0001 | ✓ | ✓ | ||||||||||||||
| 18 | patient.T2.4.so11a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||||
| 19 | patient.T3.2.so11a.LD_0003 | ✓ | ✓ | ||||||||||||||
| 20 | patient.T3.4.po24a.SO_0002 | ✓ | ✓ | ||||||||||||||
| 21 | patient.T3.4.so11a.LO_0003 | ✓ | ✓ | ||||||||||||||
| 22 | patient.T4.3.po14a.SD_0005 | ✓ | ✓ | ||||||||||||||
| 23 | patient.T4.3.so11a.LP_0004 | ✓ | ✓ | ||||||||||||||
| 24 | patient.T5.3.po24a.LO_0003 | ✓ | ✓ | ✓ | |||||||||||||
| 25 | patient.T5.4.lo12a.SP_0010 | ✓ | ✓ | ||||||||||||||
| 26 | patient.T6.1.lo22a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||||
| 27 | patient.T6.3.lo22a.DP_0001 | ✓ | ✓ | ||||||||||||||
| 28 | patient.T7.2.do23a.LO_0004 | ✓ | ✓ | ||||||||||||||
| 29 | patient.T7.3.po24a.SD_0007 | ✓ | ✓ | ||||||||||||||
| 30 | patient.T7.4.so11a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||||
| 31 | patient.T8.4.lo22a.SP_0010 | ✓ | ✓ | ||||||||||||||
| 32 | patient.T9.3.po24a.SD_0005 | ✓ | ✓ | ||||||||||||||
Query result 1–32: Patient
Listing 20:
List patients that have a catheter, a procedure, and the patient’s procedure uses the patient’s catheter
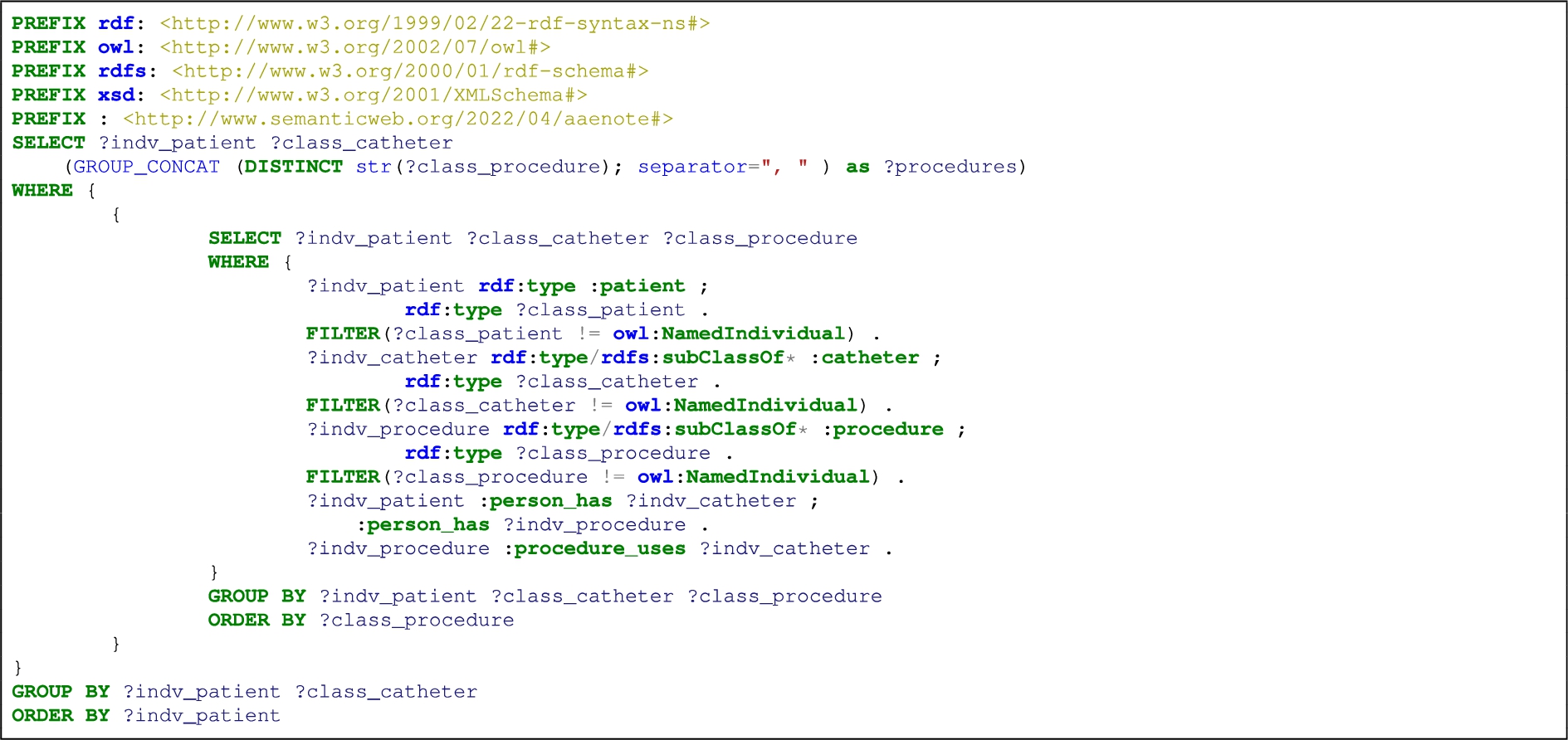
Table 24
AAENOTE SPARQL query result: list patients that have a catheter, have a procedure, and where the catheter was used for that procedure
| Person | Catheter | Procedure | |||
| Query Result | Patient | peripheral intravenous catheter | iv antibiotics | iv fluid | iv medication |
| 1 | patient.T1.1.lo22a.LO_0007 | ✓ | ✓ | ✓ | |
| 2 | patient.T1.4.lo22a.SP_0010 | ✓ | ✓ | ✓ | |
| 3 | patient.T2.2.do23a.LO_0007 | ✓ | ✓ | ✓ | |
| 4 | patient.T6.1.lo22a.LO_0007 | ✓ | ✓ | ✓ | |
Query result 1–14: Patient Ⓧ
Listing 21:
List patients that have a catheter and a procedure, and all catheters and all procedures the patient has
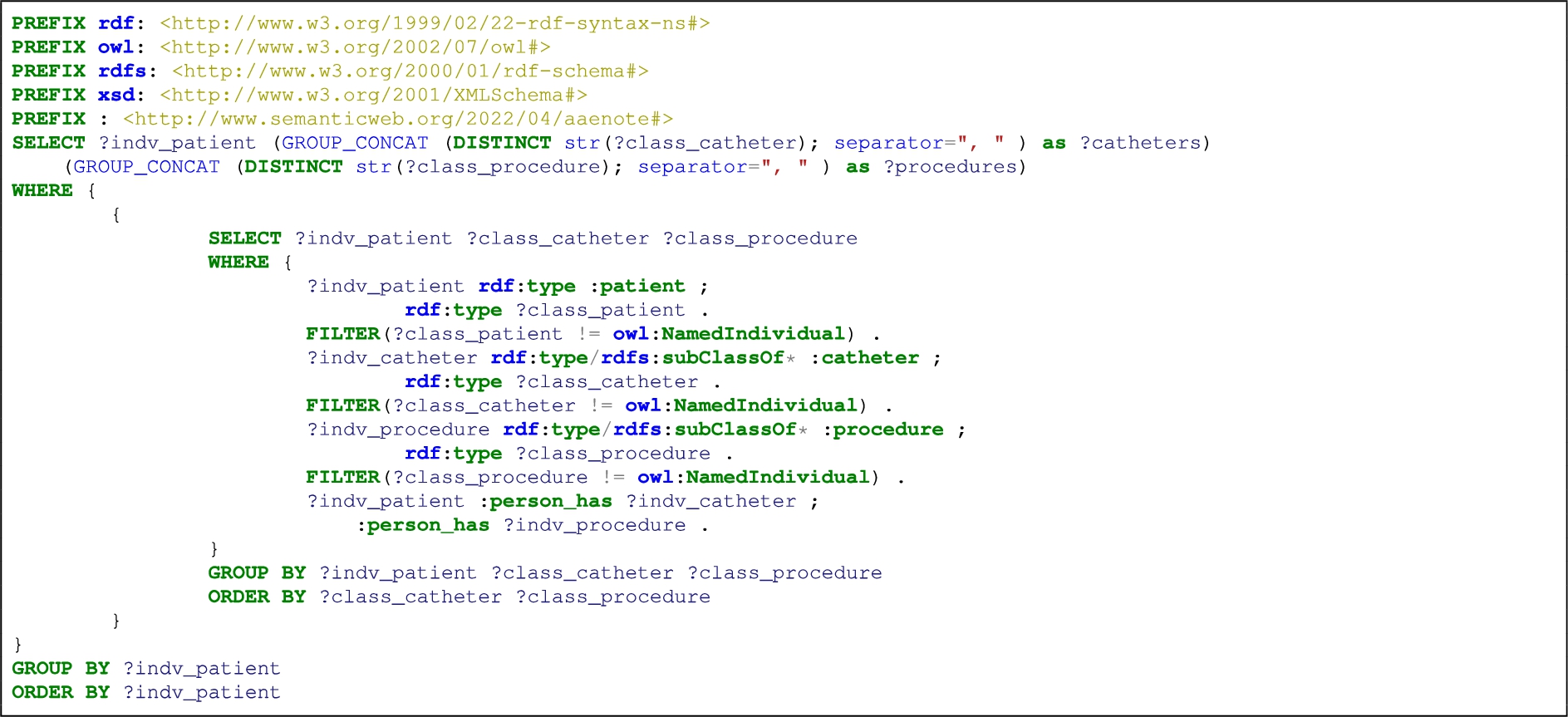
Table 25
AAENOTE SPARQL query result: list patients that have a catheter and a procedure
| Person | Catheter | Procedure | |||||||||||||
| Query Result | Patient | catheter | central venous catheter | hemodialysis catheter | peripheral intravenous catheter | urinary catheter | administration purpose | blood test | general iv | iv antibiotics | iv chemo | iv fluid | iv medication | procedure | surgery |
| 1 | patient.T1.1.lo22a.LO_0007 | ✓ | ✓ | ||||||||||||
| 2 | patient.T1.1.lo22a.LO_0009 | ✓ | ✓ | ||||||||||||
| 3 | patient.T1.2.do13a.SP_0001 | ✓ | ✓ | ||||||||||||
| 4 | patient.T1.2.do13a.SP_0010 | ✓ | ✓ | ✓ | |||||||||||
| 5 | patient.T1.2.lo22a.SD_0002 | ✓ | ✓ | ✓ | |||||||||||
| 6 | patient.T1.4.do13a.LP_0004 | ✓ | ✓ | ||||||||||||
| 7 | patient.T1.4.lo22a.SP_0006 | ✓ | ✓ | ||||||||||||
| 8 | patient.T1.4.lo22a.SP_0010 | ✓ | ✓ | ✓ | ✓ | ||||||||||
| 9 | patient.T12.2.lo22a.SD_0002 | ✓ | ✓ | ||||||||||||
| 10 | patient.T15.3.po24a.SD_0002 | ✓ | ✓ | ||||||||||||
| 11 | patient.T2.1.lo22a.LO_0001 | ✓ | ✓ | ||||||||||||
| 12 | patient.T2.2.do13a.SP_0003 | ✓ | ✓ | ||||||||||||
| 13 | patient.T2.2.do23a.LO_0001 | ✓ | ✓ | ||||||||||||
| 14 | patient.T2.2.do23a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||
| 15 | patient.T2.2.lo22a.PO_0005 | ✓ | ✓ | ||||||||||||
| 16 | patient.T2.3.do23a.PO_0005 | ✓ | ✓ | ||||||||||||
| 17 | patient.T3.2.do13a.LO_0007 | ✓ | ✓ | ||||||||||||
| 18 | patient.T3.2.do23a.SP_0003 | ✓ | ✓ | ||||||||||||
| 19 | patient.T3.3.lo22a.SO_0008 | ✓ | ✓ | ||||||||||||
| 20 | patient.T3.3.po14a.SD_0002 | ✓ | ✓ | ||||||||||||
| 21 | patient.T3.4.lo22a.SP_0003 | ✓ | ✓ | ||||||||||||
| 22 | patient.T4.2.po24a.DO_0002 | ✓ | ✓ | ||||||||||||
| 23 | patient.T5.2.do13a.LO_0003 | ✓ | ✓ | ||||||||||||
| 24 | patient.T5.3.po24a.LO_0001 | ✓ | ✓ | ||||||||||||
| 25 | patient.T6.1.lo22a.LO_0007 | ✓ | ✓ | ✓ | |||||||||||
| 26 | patient.T6.2.do13a.LO_0004 | ✓ | ✓ | ||||||||||||
| 27 | patient.T6.4.do13a.LP_0002 | ✓ | ✓ | ||||||||||||
| 28 | patient.T6.4.do23a.LP_0004 | ✓ | ✓ | ||||||||||||
| 29 | patient.T8.4.lo22a.SP_0010 | ✓ | ✓ | ||||||||||||
Query result 1–29: Patient Ⓧ
B.14.AAENOTE CQ 9a: Does patientC have an infection and catheter?
Listing 22:
List patients that have an infection and a catheter
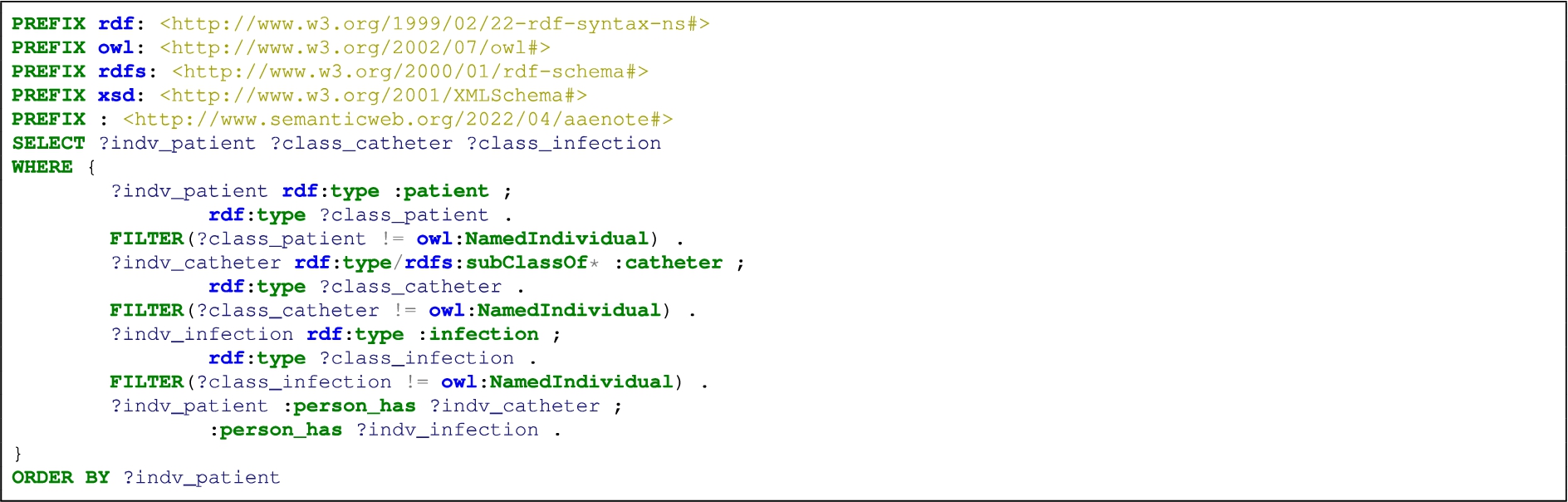
Table 26
AAENOTE SPARQL query result: list patients that have a infection and a catheter
| Query Result | Patient | peripheral intravenous catheter | infection |
| 1 | patient.T2.2.do23a.SP_0006 | ✓ | ✓ |
Query result 1: Patient Ⓧ
B.15.AAENOTE CQ 9b: Was patientC’s infection associated with a catheter?
Cannot determine if a patient’s infection is associated with a catheter unless that catheter is tested in the microbiology lab.
Appendix C.
Appendix C.Catheter infection indications ontology (CIIO) hierarchy, assumptions, indications, and competency questions
C.1.CIIO hierarchy
The CIIO classes and their subclasses can be found in the following figures:
Fig. 15.
CIIO observation class hierarchy.
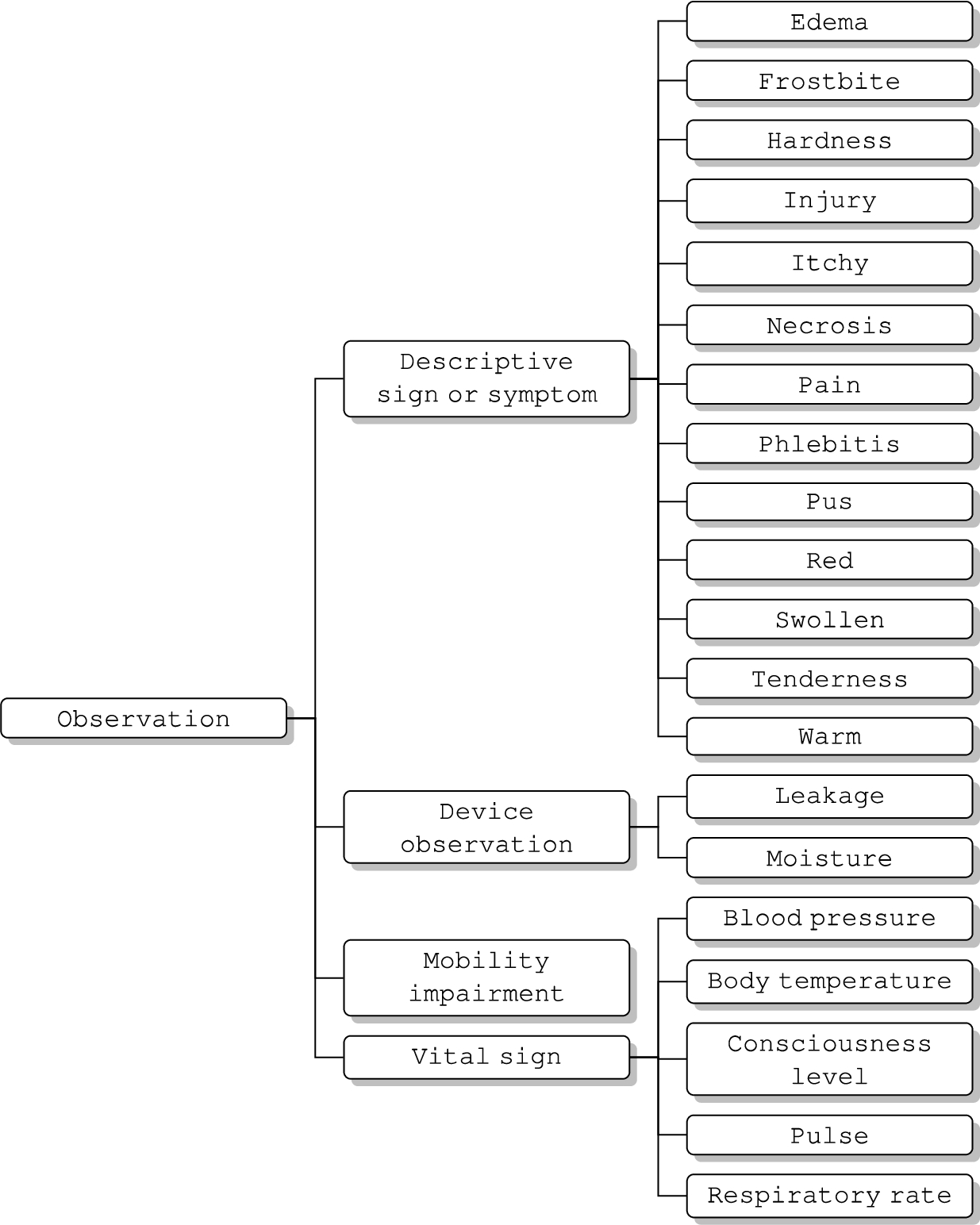
Fig. 16.
CIIO anatomical location class hierarchy.
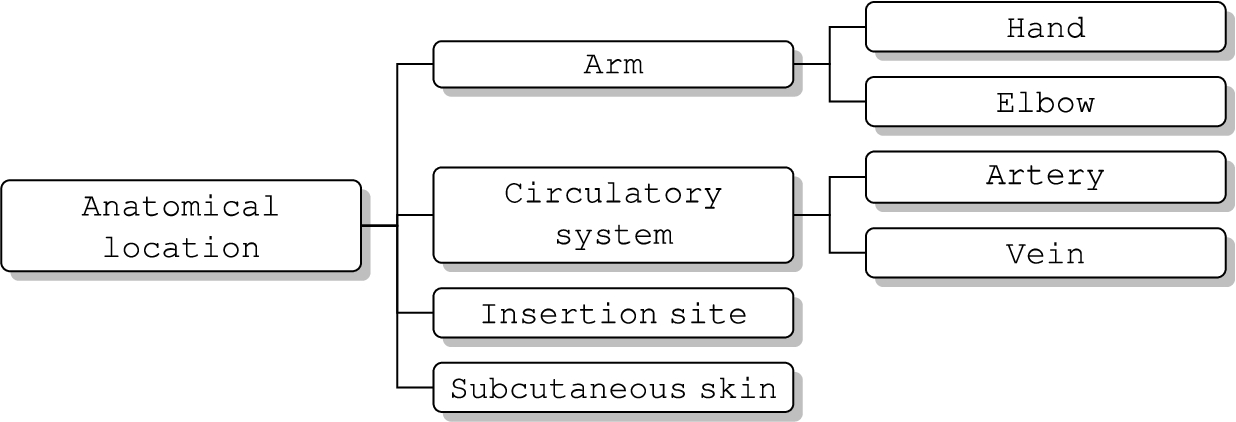
Fig. 17.
CIIO medical device class hierarchy.

Fig. 18.
CIIO procedure class hierarchy.
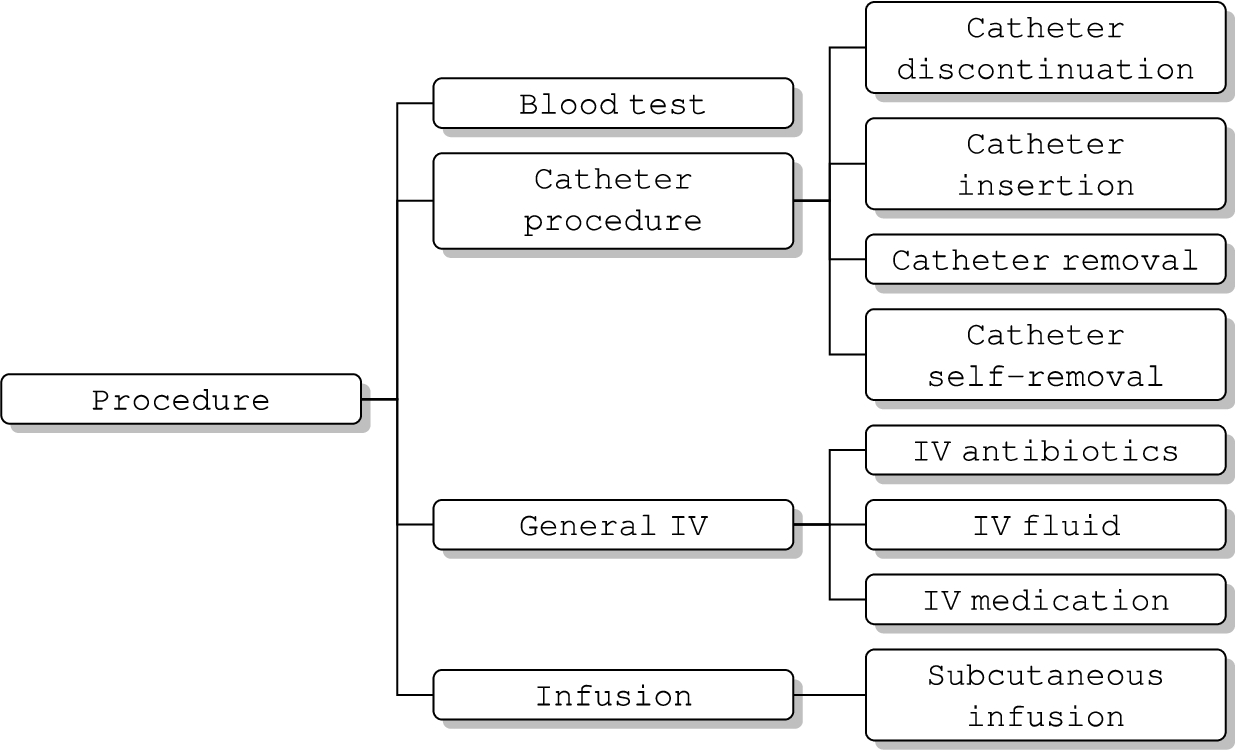
Fig. 19.
CIIO person class hierarchy.

Fig. 20.
CIIO document class hierarchy.

Fig. 21.
CIIO sentence class hierarchy.

C.2.CIIO assumptions
To address the competency questions (CQs) which ask about patients and not documents and alleviate the problem of patients being implicitly mentioned, 1 AE document represents 1 patient. In the actual electronic incident reporting system database, if the reported AE is related to a patient, there will be a patient ID. This allows users to know if the AE is about 1 patient, more than 1 patient, or no patients. Additionally, concepts that are documented within different sentences of the same document are likely describing concepts that occurred in the same event for the same patient. Furthermore, concepts documented in the same sentence that are linked together by a relationship are directly related. Certain relationships can provide the reason for why a concept was or is needed (i.e., procedureA
C.3.Catheter and infection indications
C.3.1.Catheter indications
1. A patient has a specific catheter documented.
2. Any IV usage or infusion indicates some type of catheter is used. IV usage includes general IV, IV medication, IV fluid, and IV antibiotics. Infusion includes infusion, intraosseous infusion, intravenous infusion, and subcutaneous infusion. Based on the type of IV usage or infusion alone, it is not enough to determine what type of catheter was used.
3. Catheter procedures indicate that a catheter is or was present because they require a catheter. Catheter procedures include catheter insertion, catheter discontinued use, catheter removal, catheter replacement, and catheter self-removal.
4. Infusion phlebitis indication indicates that some type of catheter is used.
C.3.2.Peripheral intravenous catheter (PIVC) indications
1. PIVCs are rarely documented, so any PIVC explicitly documented indicates a PIVC was used or in use.
2. Leaking IV or an infusion at the arm, elbow, or hand indicates a PIVC is used. IV includes general IV, IV medication, IV fluid, and IV antibiotics. Infusion includes infusion, intraosseous infusion, intravenous infusion, and subcutaneous infusion. Central venous catheters (CVCs) are deep, so there should not have leakage on the skin. PIVC leakage typically occurs because the catheter dressing is not properly secured or the PIVC is placed near a movable joint (i.e., elbow) and becomes dislodged.
C.3.3.Epidural indication
1. Epidural usage will explicitly be documented.
2. A epidural catheter is the only catheter located nearby/on/at/in the back (i.e., spinal cord).
C.3.4.Infusion phlebitis
As previously stated, infusion phlebitis can be mechanical, chemical, or infectious [23]. Regardless of cause, it is documented similarly and can either be a catheter-related infection or complication.
1. Early stage of infusion phlebitis is indicated by an insertion site or infusion with 2 of the following signs: (i) pain or tenderness, (ii) red, (iii) swollen or edema, or (iv) warm.
2. Medium stage of infusion phlebitis is indicated by (1) a vein with pain and (2) an insertion site or infusion with 2 signs: (i) red, (ii) swollen or edema, or (iii) warm.
3. Advanced stage of infusion phlebitis is indicated by (1) a vein with pain and hardness and (2) an insertion site or infusion with 2 signs: (i) red, (ii) swollen or edema, or (iii) warm.
C.3.5.Infection
1. Pus at an insertion site indicates an infection. Because pus present is a sure sign of infection.
C.3.6.Bloodstream infection (BSI)
1. A bloodstream infection is indicated by a blood test with a positive test result and/or the name of the cultured bacteria.
C.3.7.Sepsis
1. Infection combined with mobility impairment, high body temperature, and frostbite indicates sepsis.
2. Meeting the Quick Sequential Organ Failure Assessment Score (qSOFA) [56] sepsis criteria is indicated if there is an infection indication and at least 2 of the following: (1) high respiratory rate, (2) low blood pressure, or (3) a consciousness level that is either confusion, verbally responsive, painfully responsive, or unresponsive.
3. Sepsis is indicated if there is an infection indication and the National Early Warning Score 2 (NEWS2) [52] criteria for clinical deterioration is met by a combination of (1) high respiratory rate, (2) low blood pressure, (3) high pulse, (4) low body temperature or high body temperature, and (5) consciousness level = confusion, verbally responsive, painfully responsive, or unresponsive.
C.4.CIIO competency questions and ontology usage
SPARQL queries for answering the CIIO competency questions are available on GitHub at https://github.com/melissayan/aaenote_and_ciio/wiki/Ontology-SPARQL-Queries.
Table 27
CIIO competency questions and ontology usage
| Competency Question | Ontology Classes and Relationships to Find Instances |
| 1. Does patientA have phlebitis, and was it infectious phlebitis, chemical phlebitis, or mechanical phlebitis? |
|
| 2. Does patientA have an infection? |
|
| 3. Does patientA have a BSI? |
|
| 4. How many patients have an infection or BSI? | Same as Competency Question 1 and 2. |
Table 27
(Continued)
| Competency Question | Ontology Classes and Relationships to Find Instances |
| 5. Which patients have sepsis? |
|
Table 27
(Continued)
| Competency Question | Ontology Classes and Relationships to Find Instances |
| 6. Does patientB have a catheter? |
|
Table 27
(Continued)
| Competency Question | Ontology Classes and Relationships to Find Instances |
| 7. Does patientB have a PIVC? |
|
| 8a. How many catheters does patientB have? |
|
| 8b. Where are the catheters in patientB? |
|
Table 27
(Continued)
| Competency Question | Ontology Classes and Relationships to Find Instances |
| 8c. Why does patientB need the catheter(s)? |
|
| 9a. Does patientC have an infection and catheter? |
|
| 9b. Was patientC’s infection associated with a catheter? | § Cannot determine if an infection is associated with a catheter unless that catheter is tested in the microbiology lab. |
References
[1] | E. Alexandrou, G. Ray-Barruel, P.J. Carr, S.A. Frost, S. Inwood, N.S. Higgins, F. Lin, L. Alberto, L.A. Mermel and C.M. Rickard, Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes Worldwide, Journal of Hospital Medicine 13(5) (2018). doi:10.12788/jhm.3039. |
[2] | L. Amos, D. Anderson, S. Brody, A. Ripple and B.L. Humphreys, UMLS users and uses: A current overview, Journal of the American Medical Informatics Association ((2020) ). doi:10.1093/jamia/ocaa084. |
[3] | A.R. Aronson, Effective mapping of biomedical text to the UMLS Metathesaurus: The MetaMap program, Proceedings. AMIA Symposium (2001), 17–21. |
[4] | M. Bada, M. Eckert, M. Palmer and L. Hunter, An overview of the CRAFT concept annotation guidelines, in: Proceedings of the Fourth Linguistic Annotation Workshop, LAW 2010, Uppsala, Sweden, July 15–16, 2010, Association for Computational Linguistics, (2010) , pp. 207–211. |
[5] | M. Bada and L. Hunter, Desiderata for ontologies to be used in semantic annotation of biomedical documents, Journal of Biomedical Informatics 44: (1) ((2011) ), 94–101. doi:10.1016/j.jbi.2010.10.002. |
[6] | M. Bada, N. Vasilevsky, W.A. Baumgartner, M. Haendel and L.E. Hunter, Gold-standard ontology-based anatomical annotation in the CRAFT Corpus, Database 2017 (2017). doi:10.1093/database/bax087. |
[7] | Biological Spatial Ontology, 2020. http://obofoundry.org/ontology/bspo. |
[8] | O. Bodenreider, The Unified Medical Language System (UMLS): Integrating biomedical terminology, Nucleic Acids Research 32(Database issue) (2004), D267–70. doi:10.1093/nar/gkh061. |
[9] | H.K. Butcher, G.M. Bulechek, J.M. Dochterman and C.M. Wagner, Nursing Interventions Classification (NIC), Elsevier, (2018) . ISBN 9780323497701. |
[10] | O. Corcho, M. Fernández-López and A. Gómez-Pérez, Methodologies, tools and languages for building ontologies. Where is their meeting point?, Data & Knowledge Engineering 46: (1) ((2003) ), 41–64. doi:10.1016/S0169-023X(02)00195-7. |
[11] | A. Degbelo, A snapshot of ontology evaluation criteria and strategies, in: Proceedings of the 13th International Conference on Semantic Systems, SEMANTiCS 2017, Amsterdam, the Netherlands, September 11–14, 2017, ACM, (2017) . ISBN 9781450352963. doi:10.1145/3132218.3132219. |
[12] | C. Dendle, R.L. Stuart and D. Egerton-Warburton, Think before you insert an intravenous catheter, The Medical journal of Australia 199: (10) ((2013) ), 655. doi:10.5694/mja13.10733. |
[13] | eHealth & International Classification for Nursing Practice (ICNP™), 2021. https://www.icn.ch/what-we-do/projects/ehealth-icnptm. |
[14] | M. Fernández-López, A. Gómez-Pérez and N. Juristo, METHONTOLOGY: From ontological art towards ontological engineering, in: Proceedings of the Ontological Engineering AAAI-97, 24–26 March 1997, Spring Symposium Series, AAAI Press, Stanford, CA, USA, (1997) . |
[15] | Foundational Model of Anatomy, 2008. http://si.washington.edu/projects/fma. |
[16] | D. Garijo, WIDOCO: A wizard for documenting ontologies, in: Proceedings, Part II, The Semantic Web – ISWC 2017 – 16th International Semantic Web Conference, Vienna, Austria, October 21–25, 2017, Springer, (2017) , pp. 94–102. doi:10.1007/978-3-319-68204-4_9. |
[17] | A. Goldfain, B. Smith, S. Arabandi, M. Brochhausen and W.R. Hogan, Vital sign ontology, in: Proceedings of the Workshop on Bio-Ontologies, Intelligent Systems in Molecular Biology (ISMB), Vienna, Austria, July 17–19, 2011, (2011) . |
[18] | A. Gómez-Pérez, Towards a framework to verify knowledge sharing technology, Expert Systems with Applications 11: (4) ((1996) ), 519–529. doi:10.1016/S0957-4174(96)00067-X. |
[19] | A. Gómez-Pérez, Ontology evaluation, in: Handbook on Ontologies, S. Staab and R. Studer, eds, Springer, Berlin Heidelberg, Berlin, Heidelberg, (2004) , pp. 251–273. ISBN 9783540247500. doi:10.1007/978-3-540-24750-0_13. |
[20] | M. Grüninger and M.S. Fox, Methodology for the design and evaluation of ontologies, in: Proceedings of the Workshop on Basic Ontological Issues in Knowledge Sharing, International Joint Conference on Artificial Intelligence (IJCAI-95), Montreal, Canada, (1995) , ISSN 1045-0823. |
[21] | Y. He, S. Sarntivijai, Y. Lin, Z. Xiang, A. Guo, S. Zhang, D. Jagannathan, L. Toldo, C. Tao and B. Smith, OAE: The ontology of adverse events, Journal of Biomedical Semantics 5: ((2014) ), 29. doi:10.1186/2041-1480-5-29. |
[22] | T. Heather Herdman, S. Kamitsuru and C.T. Lopes, NANDA International Nursing Diagnoses: Definitions & Classification, 2021–2023, Thieme Medical Publishers, Incorporated, (2021) . ISBN 9781684204540. |
[23] | R. Higginson and A. Parry, Phlebitis: Treatment, care and prevention, Nursing Times 107: (36) ((2011) ), 18–21. |
[24] | L.H. Høvik, K.H. Gjeilo, S. Lydersen, C.M. Rickard, B. Røtvold, J.K. Damås, E. Solligård and L.T. Gustad, Monitoring quality of care for peripheral intravenous catheters; feasibility and reliability of the peripheral intravenous catheters mini questionnaire (PIVC-miniQ), BMC Health Services Research 19: (1) ((2019) ), 636. doi:10.1186/s12913-019-4497-z. |
[25] | E. Hovy, M. Marcus, M. Palmer, L. Ramshaw and R. Weischedel, in: OntoNotes: The 90% Solution, in: Human Language Technology Conference of the North American Chapter of the Association of Computational Linguistics, Proceedings, New York, New York, USA, June 4–9, 2006, Association for Computational Linguistics, (2006) , pp. 57–60. |
[26] | L.E. Huerta and T.W. Rice, Pathologic difference between sepsis and bloodstream infections, The Journal of Applied Laboratory Medicine 3: (4) ((2019) ), 654–663. doi:10.1373/jalm.2018.026245. |
[27] | Infectious Disease Ontology, 2017, https://bioportal.bioontology.org/ontologies/IDO. |
[28] | Infusion Nurses Society, 2021 Infusion Therapy Standards of Practice Updates, Journal of Infusion Nursing 44(4) (2021), 189–190. doi:10.1097/NAN.0000000000000396. |
[29] | K.N. Iskander, M.F. Osuchowski, D.J. Stearns-Kurosawa, S. Kurosawa, D. Stepien, C. Valentine and D.G. Remick, Sepsis: Multiple abnormalities, heterogeneous responses, and evolving understanding, Physiological Reviews 93: (3) ((2013) ), 1247–1288. doi:10.1152/physrev.00037.2012. |
[30] | A. Jackson, Infection control – a battle in vein: Infusion phlebitis, Nursing Times 94: (4) ((1998) ), 68–71. |
[31] | J. Kolikof, K. Peterson and A.M. Baker, Central venous catheter, in: StatPearls, StatPearls Publishing, Treasure, Island (FL), (2021) . |
[32] | L.A. Mermel, Short-term peripheral venous catheter-related bloodstream infections: A systematic review, Clinical Infectious Diseases 65: (10) ((2017) ), 1757–1762. doi:10.1093/cid/cix562. |
[33] | S.M. Meystre, G.K. Savova, K.C. Kipper-Schuler and J.F. Hurdle, Extracting information from textual documents in the electronic health record: A review of recent research, Yearbook of Medical Informatics (2008), 128–144. doi:10.1055/s-0038-1638592. |
[34] | C.J. Mungall, C. Torniai, G.V. Gkoutos, S.E. Lewis and M.A. Haendel, Uberon, an integrative multi-species anatomy ontology, Genome Biology 13: (1) ((2012) ), R5. doi:10.1186/gb-2012-13-1-r5. |
[35] | National Cancer Institute Thesaurus. https://bioportal.bioontology.org/ontologies/NCIT. |
[36] | NCI Thesaurus, https://ncithesaurus.nci.nih.gov/ncitbrowser/. |
[37] | V. Ng, Machine learning for entity coreference resolution: A retrospective look at two decades of research, in: Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, February 4-9, 2017, ISSN, Vol. 31: , AAAI Press, San Francisco, California, USA, (2017) , pp. 4877–4884. doi:10.1609/aaai.v31i1.11149. |
[38] | N.F. Noy and C.D. Hafner, The state of the art in ontology design: A survey and comparative review, AI Magazine 18: (3) ((1997) ), 53–53. doi:10.1609/aimag.v18i3.1306. |
[39] | Ontology for General Medical Science, 2021, http://www.obofoundry.org/ontology/ogms. |
[40] | Ontology of Adverse Events, 2021. http://www.obofoundry.org/ontology/oae. |
[41] | J. Paulsen, A. Mehl, Å. Askim, E. Solligård, B.O. Åsvold and J.K. Damås, Epidemiology and outcome of Staphylococcus aureus bloodstream infection and sepsis in a Norwegian county 1996–2011: An observational study, BMC Infectious Diseases 15: ((2015) ), 116. doi:10.1186/s12879-015-0849-4. |
[42] | A. Philpot, E. Hovy and P. Pantel, The omega ontology, in: Proceedings of OntoLex 2005 – Ontologies and Lexical Resources, Jeju Island, Korea, October 15, 2005, (2005) . |
[43] | H.S. Pinto and J.P. Martins, Ontologies: How can they be built?, Knowledge and information systems 6: (4) ((2004) ), 441–464. doi:10.1007/s10115-003-0138-1. |
[44] | S. Pradhan, A. Moschitti, N. Xue, O. Uryupina and Y. Zhang, CoNLL-2012 shared task: Modeling multilingual unrestricted coreference in OntoNotes, in: Joint Conference on Empirical Methods in Natural Language Processing and Computational Natural Language Learning – Proceedings of the Shared Task: Modeling Multilingual Unrestricted Coreference in OntoNotes, EMNLP-CoNLL 2012, Jeju Island, Korea, July 13, 2012, Association for Computational Linguistics, (2012) , pp. 1–40. |
[45] | S. Pradhan, L. Ramshaw, M. Marcus, M. Palmer, R. Weischedel and N. Xue, CoNLL-2011 shared task: Modeling unrestricted coreference in OntoNotes, in: Proceedings of the Fifteenth Conference on Computational Natural Language Learning: Shared Task, CoNLL 2011, Portland, Oregon, USA, June 23–24, 2011, Association for Computational Linguistics, (2011) , pp. 1–27. |
[46] | S.S. Pradhan, E. Hovy, M. Marcus, M. Palmer, L. Ramshaw and R. Weischedel, OntoNotes: A unified relational semantic representation, in: Proceedings of the First IEEE International Conference on Semantic Computing (ICSC 2007), Irvine, California, USA, September 17–19, 2007, (2007) , pp. 517–526. doi:10.1109/ICSC.2007.83. |
[47] | G. Ray-Barruel, D.F. Polit, J.E. Murfield and C.M. Rickard, Infusion phlebitis assessment measures: A systematic review, Journal of Evaluation in Clinical Practice 20: (2) ((2014) ), 191–202. doi:10.1111/jep.12107. |
[48] | Relation Ontology, 2021. http://obofoundry.org/ontology/ro. |
[49] | J.M. Rohde, A.J. Odden, C. Bonham, L. Kuhn, P.N. Malani, L.M. Chen, S.A. Flanders and T.J. Iwashyna, The epidemiology of acute organ system dysfunction from severe sepsis outside of the intensive care unit, Journal of Hospital Medicine 8: (5) ((2013) ), 243–247. doi:10.1002/jhm.2012. |
[50] | C. Rosse and J.L.V. Mejino, The foundational model of anatomy ontology, in: Anatomy Ontologies for Bioinformatics: Principles and Practice, A. Burger, D. Davidson and R. Baldock, eds, Springer, London, London, (2008) , pp. 59–117. ISBN 9781846288852. doi:10.1007/978-1-84628-885-2_4. |
[51] | C. Rosse and J.L.V. Mejino Jr., A reference ontology for biomedical informatics: The foundational model of anatomy, Journal of Biomedical Informatics 36: (6) ((2003) ), 478–500. doi:10.1016/j.jbi.2003.11.007. |
[52] | Royal College of Physicians, National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party, Technical Report, Royal College of Physicians, 2017. |
[53] | K.E. Rudd, N. Kissoon, D. Limmathurotsakul, S. Bory, B. Mutahunga, C.W. Seymour, D.C. Angus and T.E. West, The global burden of sepsis: Barriers and potential solutions, Critical Care 22: (1) ((2018) ), 232. doi:10.1186/s13054-018-2157-z. |
[54] | M. Sabou and M. Fernandez, Ontology (network) evaluation, in: Ontology Engineering in a Networked World, M.C. Suárez-Figueroa, A. Gómez-Pérez, E. Motta and A. Gangemi, eds, Springer, Berlin Heidelberg, Berlin, Heidelberg, (2012) , pp. 193–212. ISBN 9783642247941. doi:10.1007/978-3-642-24794-1_9. |
[55] | R. Salomão, B.L. Ferreira, M.C. Salomão, S.S. Santos, L.C.P. Azevedo and M.K.C. Brunialti, Sepsis: Evolving concepts and challenges, Brazilian Journal of Medical and Biological Research 52: (4) ((2019) ), e8595. doi:10.1590/1414-431X20198595. |
[56] | C.W. Seymour, V.X. Liu, T.J. Iwashyna, F.M. Brunkhorst, T.D. Rea, A. Scherag, G. Rubenfeld, J.M. Kahn, M. Shankar-Hari, M. Singer, C.S. Deutschman, G.J. Escobar and D.C. Angus, Assessment of clinical criteria for sepsis: For the third international consensus definitions for sepsis and septic shock (sepsis-3), JAMA 315: (8) ((2016) ), 762–774. doi:10.1001/jama.2016.0288. |
[57] | B. Smith, W. Ceusters, B. Klagges, J. Köhler, A. Kumar, J. Lomax, C. Mungall, F. Neuhaus, A.L. Rector and C. Rosse, Relations in biomedical ontologies, Genome Biology 6: (5) ((2005) ), R46. doi:10.1186/gb-2005-6-5-r46. |
[58] | P. Stenetorp, S. Pyysalo, G. Topić, T. Ohta, S. Ananiadou and J. Tsujii, BRAT: A web-based tool for NLP-assisted text annotation, in: EACL 2012, 13th Conference of the European Chapter of the Association for Computational Linguistics, Avignon, France, April 23–27, 2012, (2012) , pp. 102–107. |
[59] | M.C. Suárez-Figueroa, A. Gómez-Pérez and M. Fernández-López, The NeOn methodology for ontology engineering, in: Ontology Engineering in a Networked World, M.C. Suárez-Figueroa, A. Gómez-Pérez, E. Motta and A. Gangemi, eds, Springer, Berlin Heidelberg, Berlin, Heidelberg, (2012) , pp. 9–34. ISBN 9783642247941. doi:10.1007/978-3-642-24794-1_2. |
[60] | Y. Sure, S. Staab and R. Studer, On-to-knowledge methodology (OTKM), in: Handbook on Ontologies, S. Staab and R. Studer, eds, Springer, Berlin Heidelberg, Berlin, Heidelberg, (2004) , pp. 117–132. ISBN 9783540247500. doi:10.1007/978-3-540-24750-0_6. |
[61] | R.S. Travillian, T. Adamusiak, T. Burdett, M. Gruenberger, J. Hancock, A.-M. Mallon, J. Malone, P. Schofield and H. Parkinson, Anatomy ontologies and potential users: Bridging the gap, Journal of Biomedical Semantics 2: (Suppl 4) ((2011) ), S3. doi:10.1186/2041-1480-2-S4-S3. |
[62] | M. Uschold and M. King, Towards a methodology for building ontologies, in: Workshop on Basic Ontological Issues in Knowledge Sharing, Held in Conjuction with IJCAI-95, Artificial Intelligence Applications Institute, Montreal, Canada, Edinburgh, (1995) , pp. 1–13. |
[63] | M. Villegas, A. Intxaurrondo, A. Gonzalez-Agirre, M. Marimon and M. Krallinger, The MeSpEN resource for English-Spanish medical machine translation and terminologies: Census of parallel corpora, glossaries and term translations, in: Proceedings of the LREC 2018 Workshop “MultilingualBIO: Multilingual Biomedical Text Processing”, European Language Resources Association (ELRA), (2018) . |
[64] | Vital Sign Ontology, 2012. https://bioportal.bioontology.org/ontologies/VSO. |
[65] | H.J. White and M.P. Soos, Anatomy, thorax, superior vena cava, in: StatPearls, StatPearls Publishing, Treasure, Island (FL), (2021) . |
[66] | M.Y. Yan, L.H. Høvik, L.T. Gustad and Ø. Nytrø, Understanding and reasoning about early signs of sepsis: From annotation guideline to ontology, in: IEEE International Conference on Bioinformatics and Biomedicine, BIBM 2021, Houston, TX, USA, December 9–12, 2021, IEEE, (2021) , pp. 1906–1911. doi:10.1109/BIBM52615.2021.9669311. |
[67] | M.Y. Yan, L.H. Høvik, A. Pedersen, L.T. Gustad and Ø. Nytrø, Preliminary processing and analysis of an adverse event dataset for detecting sepsis-related events, in: IEEE International Conference on Bioinformatics and Biomedicine, BIBM 2021, Houston, TX, USA, December 9–12, 2021, IEEE, (2021) , pp. 1605–1610. doi:10.1109/BIBM52615.2021.9669410. |
[68] | L.-C. Yu, C.-H. Wu, A. Philpot and E. Hovy, OntoNotes: Sense pool verification using Google N-Gram and statistical tests, in: Proceedings of the OntoLex Workshop at the 6th International Semantic Web Conference (ISWC 2007), (2007) . |
[69] | L. Zhang, S. Cao, N. Marsh, G. Ray-Barruel, J. Flynn, E. Larsen and C.M. Rickard, Infection risks associated with peripheral vascular catheters, Journal of Infection Prevention 17: (5) ((2016) ), 207–213. doi:10.1177/1757177416655472. |


