
Mediterranean diet and SPA treatment: A healthy association?
Abstract
BACKGROUND:
In 2014, around 1.9 billion adults over the age of 18 were overweight. In the United States and Europe obesity has become a primary public health problem.
Many people who go often to SPAs to perform mud therapy are overweight. The possibility of a dietetic evaluation to follow a dietetic program could be an occasion for both slimming and food education.
OBJECTIVES:
We have look for a possible cooperation between Mediterranean diet and mudpack treatment in losing weight.
METHODS:
A 1 week/2 week follow up intervention with a low calories Mediterranean diet combined or not with mudpack treatment. The main outcome measures are weight, BIA (Body Impedence Assessment), waist-hip ratio, abdominal circumference.
RESULTS AND CONCLUSIONS:
The thermal spas are an opportunity to regain a good state of health, undergoing to traditional mudpack treatments, a balanced and low calories diet, physical activity under strict control of a personal Trainer, and relaxing and draining treatments.
Most overweight and obese patients have lost weight and fat, and this seems to be due not only to low caloric regimen, but also to the mudpack therapy itself. It will be very important to carry out studies with larger statistical relevance in the future.
1Background
1.1Thermal therapies
The thermal spa vacation is to find balance in well-being and beauty. The modern SPA responds to the new concept of health, as a state of complete psychic, physical and social wellness and not just only the absence of illness.
The thermal water of Abano Terme has many therapeutic effects [1, 2], like high-salinity antiseptic action, endocrine action, increasing thyroid activity and stimulating the synthesis of gonadotropins and maturation of ovarian follicles, promoting regularization of the menstrual cycle, stimulation of the immune system, anti-inflammatory action and antifibrotic action.
The mud, characteristic of the Euganean basin, is a complex system consisting of three different components, a solid one (the clay), a mineral one (the salt dissolved in the water) and the biologic one [3, 4]. The beneficial effects of mud, therefore, are not only attributable to the heat and the presence of electrolytes in solution, but mainly depend on what happens during its maturing process: the chemical-physical characteristics of the mud change and community of specific microorganism grow [5–9]. A cyanobacter, the Phormidium sp. ETS-05 [10] produces glycogenic and sulfo-glycolipidic substances, in particular monogalactosildiacyglycerol, with in vitro anti-inflammatory activity equivalent or even superior to traditional anti-inflammatory drugs such as indomethacin and betamethasone [11–13]. In addition, high concentrations of carotenoids, such as beta-carotene, lutein and lycopene, are in the mud, produced by the vegetable felt. In addition, there are high concentrations of C-ficocyanine with a strong antioxidant, antitumor activity, and C-allooxycianine, with antioxidant and anti-inflammatory activities [14]. After 12 mature mud treatment with thermal bath, there is a reduction in the serum concentrations of IL1, transferrin [14] and TNFα [16] and an increased level of IGF1 [15]. In addition, the mudpack therapy affects bone metabolism, especially if associated with physical activity, increasing osteoblastic activity [17].
Recent studies found a significant decrease in leptin and visfatin in patients who underwent two weeks of mud pack [18, 19]. Because of this the mud therapy could also have a role in the treatment of obesity and metabolic syndrome [20].
1.2Overweight and obesity
In 2014, around 1.9 billion adults over the age of 18 were overweight and over 600 million were obese (BMI equal to or greater than 30). The prevalence of obesity in industrialized countries has gradually increased since the first half of the 20th century, becoming in the United States and Europe a primary public health problem. Severe overweight and obesity are one of the major risk factors for the development of many chronic diseases such as respiratory diseases, type 2 diabetes and cardiovascular diseases (arrhythmia, hypertension, heart failure and stroke) [21–23]. There is also an association between overweight and some forms of cancer (colon, breast, endometrial, ovarian and uterine cancer, prostate cancer) [24] as well as psychological problems, such as risk of early death.
The development of overweight and obesity has a multifactorial genesis that includes genetic factors, environmental and behavioral factors, aging and pregnancy, comorbidity with some endocrine or autoimmune disorders, chronic intake of some drugs and a high caloric diet rich in fat [25–27] and sedentary lifestyle [28, 29]. Therefore, nutrition (in terms of quantity and quality of the foods and their modes and times of intake) and physical activity greatly influence the equilibrium of energy balance and are those on which an effective intervention is possible.
The risk of developing one of the aforementioned pathologies is linked to the relative amount of excess weight, the localization of body fat, the importance of weight gain in adulthood and the amount of physical activity. It’s possible to avoid these problems with a relatively modest weight loss (10–15%), especially when combined with an increase in physical exercise.
The anthropometric indexes (BMIs, pliers, waist circumference …) are designed to evaluate in a simple but precise way the amount of body fat and its distribution, so they are an easily applicable method in any clinic because there is no difficulty in execution and no risk for patient.
1.3The mediterranean diet
The Mediterranean Diet is rich in vegetable foods (fruit, cereals, vegetable, legumes, dried fruits, seeds and olives) with olive oil as the main source of added fat, coupled with a moderate consumption of fish and seafood, eggs, cheese and yoghurt, reduced consumption of red meat and moderate alcohol intake.
Some studies show that adherence to the Mediterranean diet reduces up to 50% the risk of metabolic syndrome and reduces the risk of mortality for up to 20 years [30, 31]. Because of this, the Mediterranean Diet can be an intervention to prevent cardiovascular diseases, to reduce the incidence of type 2 diabetes and peripheral vascular disease, atrial fibrillation rate, metabolic syndrome, as well as to reduce blood pressure, hypertensive risk and carotid atherosclerosis. The World Cancer Research Fund (WCRF) and the American Institute for Cancer Research (AICR) recommend to eat more fruits and vegetables, like in Mediterranean Diet, as part of a healthy diet to prevent various types of cancer [32–35].
2Objective
To look for a possible cooperation between Mediterranean diet and mudpack treatment in losing weight, we have instituted a retrospective study in which we analyze if undergoing both Mediterranean diet and mudpack is effective and if it’s more effective than undergoing just Mediterranean diet.
3Methods
3.1Patients
We enrolled 275 people in this study, from January 2014 to September 2016 (Table 1). 193 people of these were female (70%) and the other 82 was male (30%). Most diet-requiring patients were over 50 years of age, like the medium standard of clients who goes to the Italian spa centers. In particular, patients younger than 30 years represented the 4% of the sample, those between 30 and 39 years were the 9%, those between 40 and 49 years were the 15% and older than 50 were the 72% of the sample (24% of those aged 50 to 59 years, 24% between 60 and 69 years, and 22% between 70 and 79 years). Regarding the origin of patients who have undergone a diet, the 38% of them were from Russian countries (ex USSR), 29% were Italians, 19% were French and 14% from the rest of the world. As for the history, 21 patients (11 females and 10 males) were smokers, 101 women (52%) were menopausal, and 57 (20,6%) suffered of chronic constipation. Considering their pathologies, 129 patients reported evidence of chronical arthritis in one or more districts (46,7 %), although all referred the presence of more or less constant and widespread ‘pains’. Furthermore, 79 patients were on pharmacological treatment (no diuretic) for Hypertension (28,6 %), 37 for Hypercholesterolemia (13,4 %), 4 for Metabolic Syndrome, 16 for Hypothyroidism (5,8 %), 9 for Type I2 Diabetes (3,2 %), 9 for Obstructive Sleep Apnea (3,2 %). The average number of nights spent was 8.6, and 62 % of clients underwent a 6-day treatment cycle, so only 6 days of diet. In fact most of those who required a diet for this limited time was looking for an occasion to detoxify the body more than losing weight (despite a weight loss very often would be needed).
Table 1
Characteristic of the sample
| BMI | |||||||
| Normal | Overweight | Obesity type I | Obesity type II | Obesity tipe III | Total | ||
| Sex | Female | 51 | 87 | 34 | 16 | 5 | 193 |
| Male | 3 | 30 | 36 | 8 | 5 | 82 | |
| Total | 54 | 117 | 70 | 24 | 10 | 275 | |
| Age | 10–29 y | 7 | 2 | 1 | 1 | 0 | 11 |
| 30–39 y | 13 | 5 | 5 | 2 | 0 | 25 | |
| 40–49 y | 8 | 21 | 10 | 2 | 0 | 41 | |
| 50–59 y | 10 | 20 | 24 | 8 | 4 | 66 | |
| 60–69 y | 7 | 39 | 12 | 6 | 3 | 68 | |
| > = 70 aa | 9 | 30 | 18 | 5 | 3 | 64 | |
| Total | 54 | 117 | 70 | 24 | 10 | 275 | |
| Nationality | Italian | 21 | 34 | 17 | 8 | 0 | 80 |
| French | 7 | 30 | 11 | 4 | 0 | 52 | |
| German | 1 | 3 | 0 | 0 | 5 | 9 | |
| Russian language | 24 | 39 | 30 | 8 | 4 | 105 | |
| Switzerland | 0 | 6 | 5 | 1 | 0 | 12 | |
| Rest of the world | 1 | 5 | 7 | 3 | 1 | 17 | |
| Total | 54 | 117 | 70 | 24 | 10 | 275 | |
All participants gave written consent to participate in the study.
3.2Interventions
Spa therapy consisted in 1 or 2 week program performed at the Borile Group Thermal Spa in Abano (Italy). For 200 patients the program included 6, 10 or 14 daily mud-pack applications, thermal bath, and some massage; 75 patients didn’t undergo mud-pack applications.
The mud-pack was applied on the whole body except head and heart areas for 15 minutes at the initial temperature of 45°C. After this application there was a thermal bath in mineral water at the temperature of 36°C for 10 minutes with a light hydromassage.
All the patients in the period of the study were on a 1000–1500 kcal diet (according to their basal metabolism: 1000 Kcal to a baseline metabolism of 1300 kcal/day, 1200 Kcal per metabolism between 1400 and 1800 and 1500 kcal for basal metabolism values above 1800 kcal/die). We chose a Mediterranean diet. We proposed one or two portions of cereal per day (preferring whole grains), two or more portions of vegetables per meal per day, and two portions of fruit per meal per day. The extra virgin olive oil, which is located at the center of the pyramid, was the main source of lipids for both cooking and condiment. We prepared dishes with spices, herbs, garlic and onions, thus reducing salt consumption and thus introducing a good dose of micronutrients and antioxidants in the diet. Weekly fish and seafood (two or more portions), white meat (two portions), eggs (two or four portions), red meat (once a week) was the consumption of proteins of animal origin. The combination of legumes and cereals (a great source of protein and fat) was a great meal.
3.3Data collection
Data collected in the beginning were gender, age, height, nationality, medical history, medications, dietary and physical activity, blood pressure, pulse, tobacco and alcohol consumption, basal metabolism.
3.4Outcome
Patients were assessed at basal time and at the end of the study for clinical parameters: weight, BMI (weight/height2 (Kg/m2)) waist circumference (cm), waist/hip ratio (WHR), BIA.
The weight was always measured with a mechanical balance in the morning before breakfast, two hours after the mudpack treatment.
The BIA for the assessment of the fat percentage was collected in the same moment with the Omron Fat Loss Monitor, that can accurately and easily track body fat percentage and body mass index (BMI). The fat loss monitor can also be set to two separate modes, either normal or athletic depending on client activity level.
We have used Microsoft Excel for the statistical analysis.
4Results
Anthropometric measurements showed that the 42% of the patients was overweight and the 38% was obese with the presence of severe obese (BMI over 40). If we consider BMI, the majority of males was obese (BMI>30), while there was a higher percentage of overweight patients among females (BMI between 25 and 29.9). Considering the values of BMI and the measurement of the waist circumference, as it is shown in Table 2, most of our patients presented a high risk of developing disease, even in the presence of simple overweight.
Table 2
BMI, waist circumference and disease risk in our sample
| BMI (kg/m2) | Men<102 cm | Women<88 cm | Disease risk | Men>102 cm | Women>88 cm | Disease risk | |
| Normal | 18.5–24.9 | 3 | 50 | 0 | 1 | ||
| Overweight | 25.0–29.9 | 17 | 47 | Increased | 12 | 40 | High |
| Obesity I | 30.0–34.9 | 4 | 0 | High | 32 | 34 | Very high |
| Obesity II | 35.0–39.9 | 0 | 0 | Very high | 8 | 16 | Very high |
| Obesity III | >40.0 | 0 | 0 | Extremely high | 5 | 5 | Extremely high |
When evaluating the waist/hip ratio, only in 55% of females there was an increased risk of metabolic complications (WHR> = 0.8), while in the male population the prevalence was higher, equal to 78% (WHR> = 0.9).
If we consider the fat percentage measured with BIA together with the BMI and WHR, the 83% of our patients was obese.
In general, these patients did not show a particular propensity to physical activity (also at home they had a sedentary life), preferring massage treatments, where no effort is required. During the dietetic visit, however, physical activity was always proposed, with the awareness of how important this is to maintain the results achieved.
At the follow up in the end of the staying, the first thing that we evaluated was the weight loss and the fat mass percentage.
As it is shown in Table 3, the reduction in body weight and in the fat mass percentage measured through BIA increased with the increase of diet days.
Table 3
Relation between the number of day of diet and the weight loss and the BIA
| Diet days | Weight loss (Kg) | Δ BIA |
| < = 5 days | 1,4 | 0 |
| 6–8 days | 1,71 | 0,81 |
| 10 days | 2,3 | 0,89 |
| 14 days | 2,4 | 1,2 |
Then we looked for if there was a relation between the weight loss and also the fat mass reduction and the initial BMI.
In Table 4, the average weight loss values according to BMI is shown in the first line, and the decrease in body fat percentage measured with BIA, is shown in the second line. We can see how customers with a higher BMI on the first evaluation had on average lost more weight and more fat. In particular, like it is shown in Fig. 1, there seems to be a linear correlation between the BMI of the first day of treatment and the weight loss in the end.
Fig.1
Relation between weight loss and BMI.
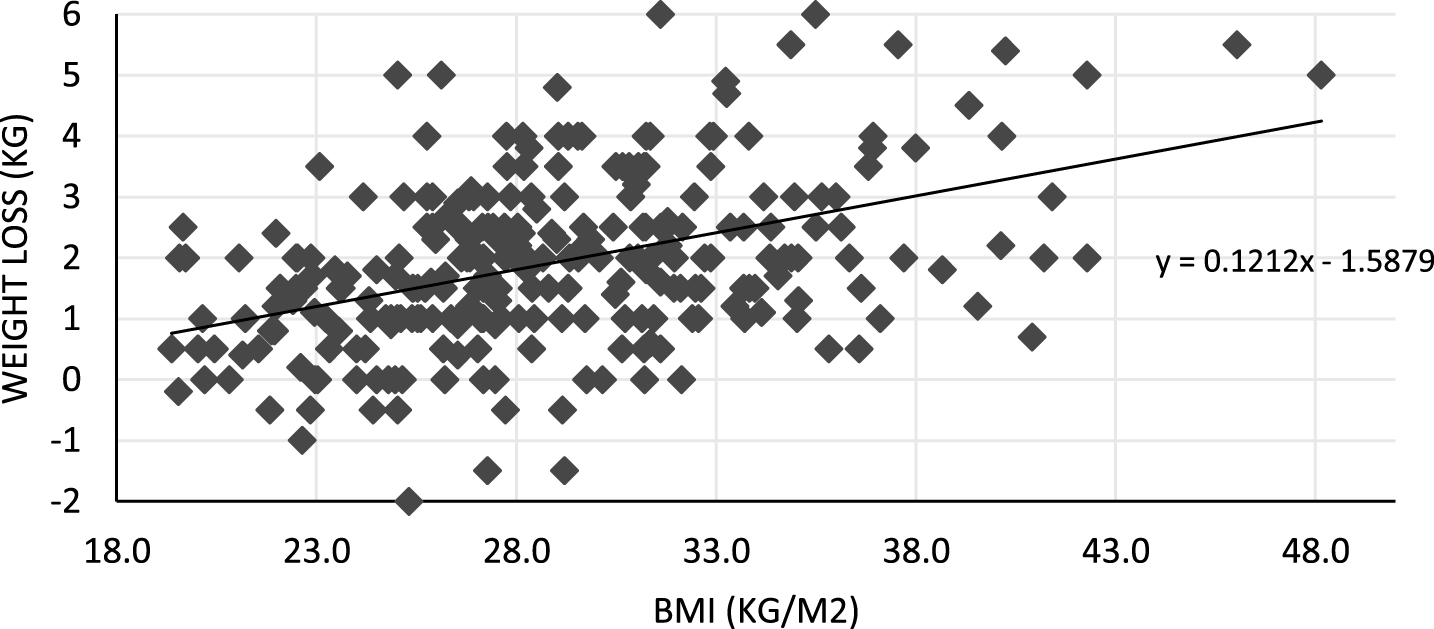
Table 4
Relation between BMI and average weight loss and average BIA decrease
| Normal weight | Overweight | Obesity I | Obesity II | Obesity III | |
| Weight loss (kg) | 1 | 1,85 | 2,2 | 2,8 | 3,48 |
| Δ BIA | 0,77 | 0,80 | 0,82 | 1,40 | 1,60 |
It is possible that subjects with a higher BMI had a greater adherence to the diet, because they were more motivated to lose weight, or because most of these subjects had a very high baseline metabolism and so they lost easily weight with a calorie restriction.
Then we have considered whether mudpack could have some effect on weight loss, and/or on fat mass reduction. We have considered the two groups: 201 patients who underwent mudpack together with diet and 74 patients who underwent only diet.
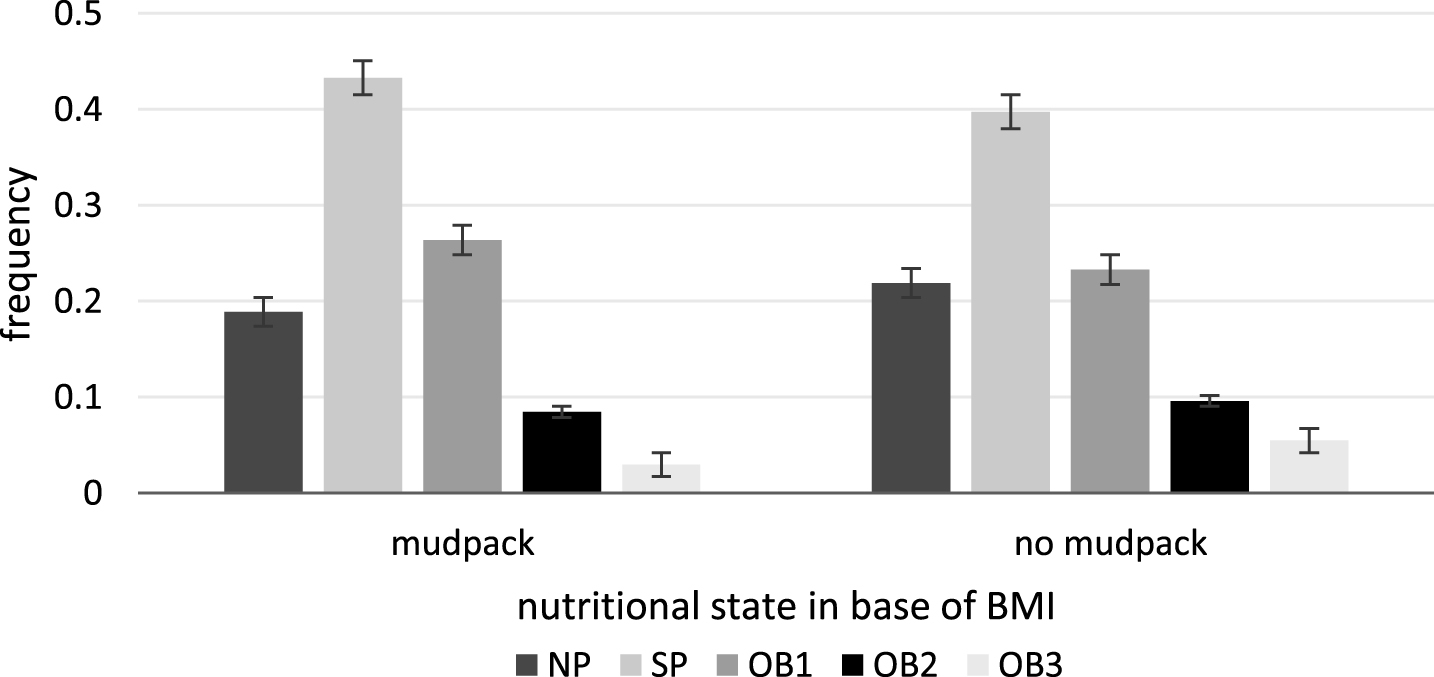
The Fig. 2 shows the distribution of the two samples (mudpack and diet; no mudpack and diet) with respect to BMI. The two samples have a similar distribution. The Pearson’s Chi Squared-Test, which resulted in a p-value equal to 0,81, confirmed the homogeneity of the two groups, with respect to their distribution, and their independence.
Fig.2
Samples’ (mudpack, no mudpack) distribution relative to BMI.
It’s very remarkable, as it can be seen from Figs 3 and 4, that overweight and obese subjects, if they have undergone diet and mudpack therapy, seem to have lost more weight and achieved a greater reduction in the fat mass than those who have done only diet. So we tested, with a T-Student test, whether the average weight loss of the first group (mud pack and diet) was lower than the one of the second group (diet only). Data led us to reject (with α= 0,05) the null hypothesis in favor of the alternative one (p = 0,0377), thus implying a weight loss of the first group significantly higher with respect to the second group. The same test has been performed by considering only patients having BMI> = 25. With α= 0,05 the conclusion was again a weight loss for the first group higher than the second (p = 0.0303).
Fig.3
Weight loss in patients who underwent diet and mudpack versus only diet.
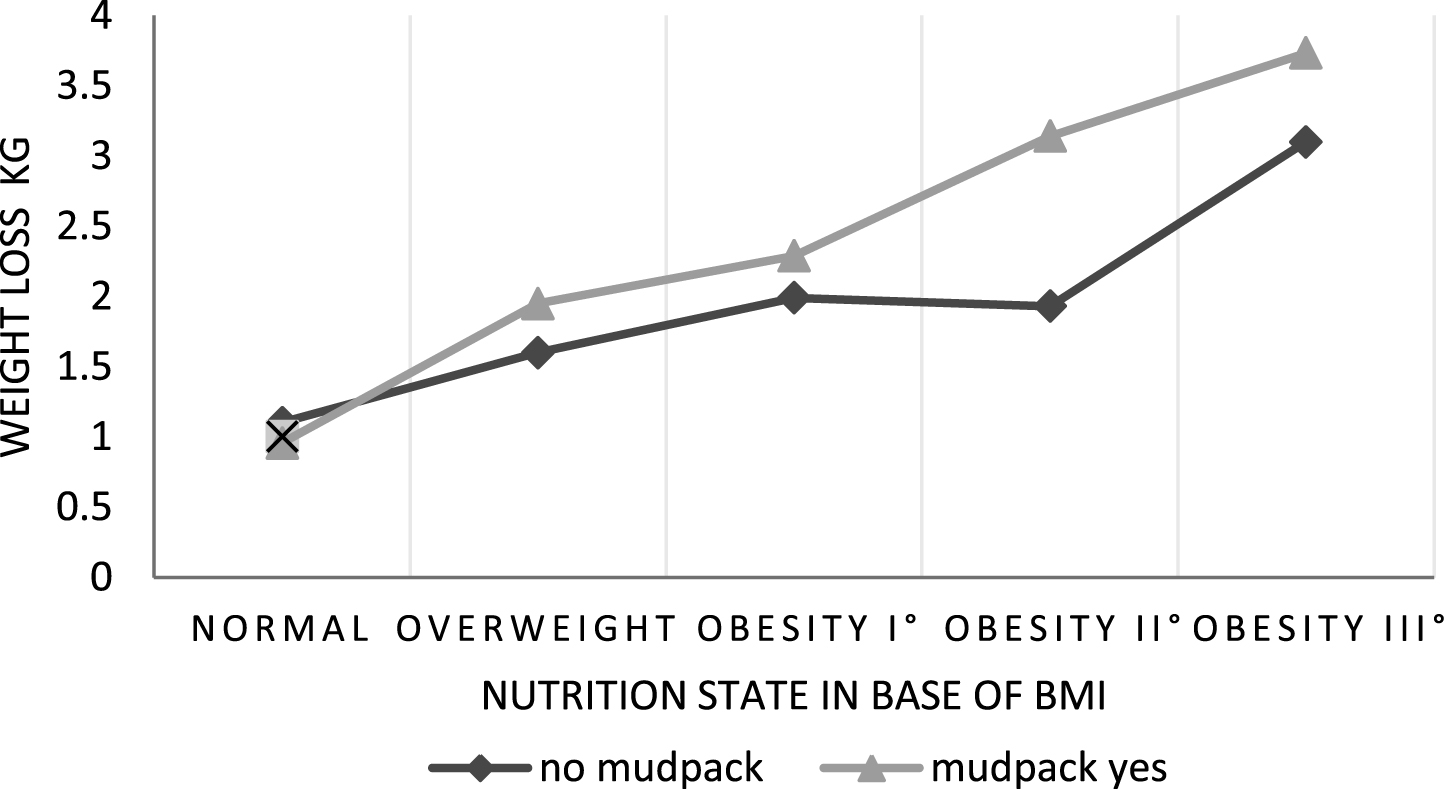
Fig.4
Reduction of BIA in patients who underwent diet and mudpack versus only diet.
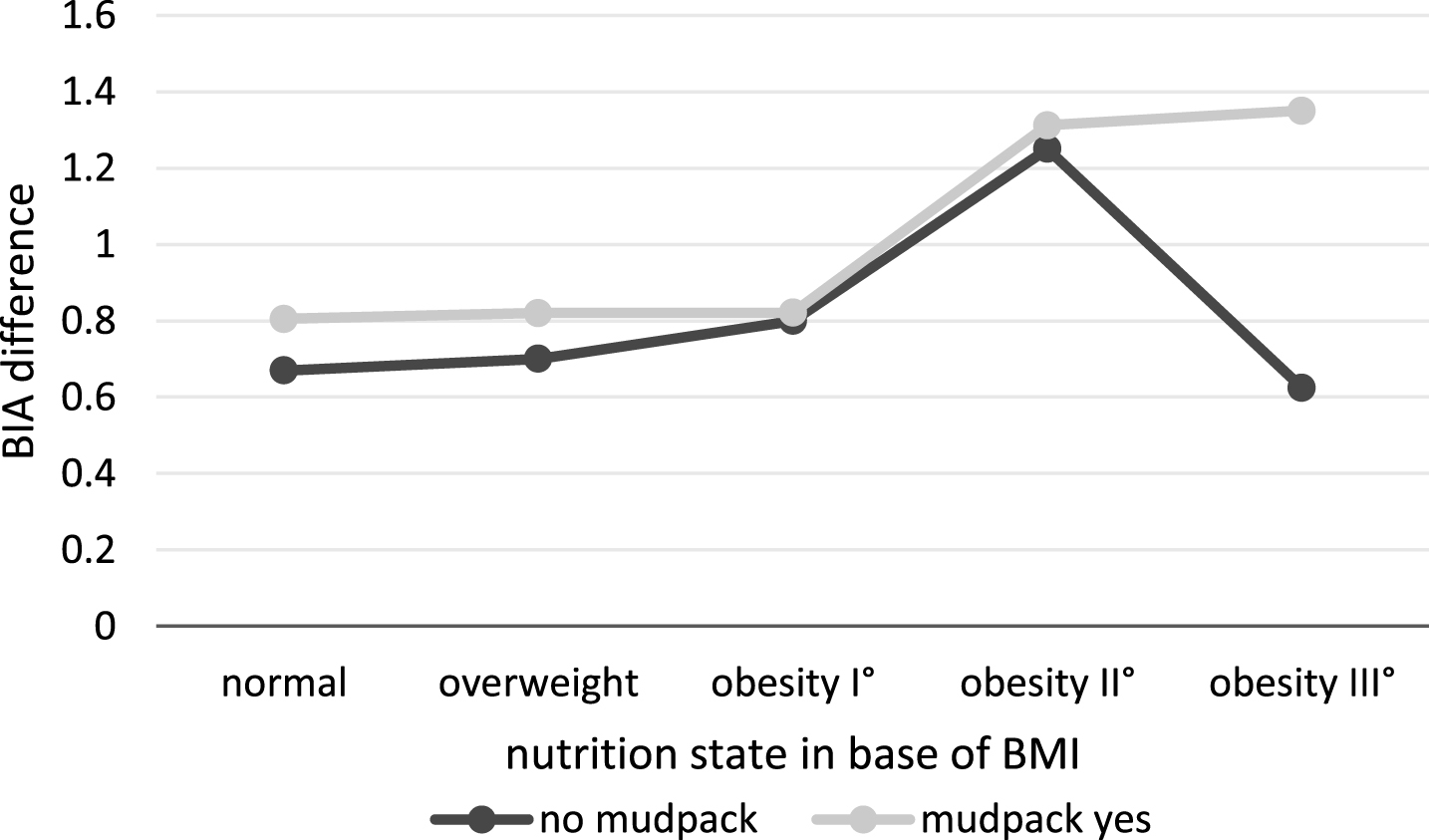
We have also tested if there is a significant difference in the BIA assess relative to the two groups. Even if the difference of BIA assess (from the beginning to the end of treatments) of the first group is higher than the one of the second, we couldn’t conclude that they are significantly different. We think this is possibly due to the short duration of the treatment.
The higher average weight loss could be justified both by metabolic activation determined by mudpack therapy documented in clinical trials and by the particular action that mudpack therapy appears to have on lipid metabolism [20]. In particular, the effect of a mudpack cycle on leptin levels should be relevant. Leptin is the hormone of satiety, and therefore associating mudpack with a low calorie diet may be of help to the patient. The reduction also of serum TNF-α levels following a mudpack cycle is well documented. This is very important, to reduce insulin resistance, another factor that could positively influence the effect of a diet in the obesity, especially if affected by type II diabetes mellitus.
5Conclusions
The thermal spa can certainly be a good opportunity to regain physical and mental well-being, combining the mudpack with thermal bath, a balanced diet, physical activity and relaxing and draining treatments.
We choose the Mediterranean Diet for giving a food education, rather than a greater effectiveness in slimming than the other type of diet. In fact in order to keep the results achieved for a long time, it is essential that the proposed food regime is pleasing, easy-to-use and cook and with ubiquitous products.
Most overweight and obese patients have lost weight and fat, and this seems to be due not only to low caloric diet, but also to thermal mudpack itself. It will be very important to carry out studies with greater statistical value in the future, with a greater number of controls, and especially by performing blood dosages of certain parameters such as blood glucose, cholesterol, triglycerides, leptin, TNF-α. To follow up these patients would also be important for knowing their long-term outcome.
References
[1] | Nappi G . Medicina e clinica termale. Selecta Medica, Pavia, (2001) . |
[2] | Solimene U , Bruttomesso G . Medicina termale. Il moderno approccio scientifico ad una forma di cura molto antica. Red ediz Milano, (2010) . |
[3] | Galzigna L , Moretto C , Lalli A . Physical and biochemical changes of thermal mud after maturation. Biomed & Pharmacother. (1996) ;50: :306–8. |
[4] | Tolomio C , Ceschi-Berrini C , De Apollonia F , Galzigna L , Masiero L , Moro L , Moschin E . Diatoms in the thermal mud of Abano Terme, Italy (Maturation period). Algological Studies. (2002) ;105: :11–27. |
[5] | Tolomio C , De Appolonia F , Moro I , Ceschi Berrini C . Thermophilic microalgae growth on different substrates and at different temperatures in experimental tanks in Abano Terme (Italy). Algological Studie. (2004) ;111: :145–57. |
[6] | Bellometti S , Galzigna L . Serum levels of a prostaglandin and a leukotriene after thermal mud pack therapy. Journal of Investigative Medicine. (1998) ;46: (4):140–5. |
[7] | Bellometti S , Galzigna L . Function of the hypothalamic adrenal axis in patients with fibromyalgia syndrome undergoing mud-pack treatment. International Journal Clin Pharm Res. (1999) ;19: (1):27–33. |
[8] | Bruno A , Rossi C , Marcolongo G , Di Lena A , Venzo A , Berrie CP , Corda D . Selective in vivo anti-inflammatory action of the galactolipid monogalactosyldiacylglycerol. EJP. (2005) ;524: :159–68. |
[9] | Marcolongo G , De Appolonia F , Venzo A , Berrei CP , Carofiglio T , Ceschi Berrini C . Diacylglycerolipids isolated from a thermophile cyanobacterium from Euganean hot spring. Nat Prod Res. (2006) ;20: (8):766–74. |
[10] | Ceschi-Berrini C , De Apolonnia F , Dalla Valle L , Komarer J , Andreoli C . Morphological and molecular characterization of a thermophilic cyanobacterium (Oscillatoriales) from the Euganean Thermal Springs (Padua, Italy). Algological Studies. (2004) ;113: :73–85. |
[11] | Lalli A , Andreoli C , Ceschi Berrini C , De Apollonia F , Marcolongo G . Antiinflammatory acrive principles in Euganean Thermal MUD. (2004) . Brevetto n°05100038.8. |
[12] | Bruno A , Rossi C , Marcolongo G , Di Lena A , Venzo A , Berrie CP , Corda D Selective in vivo anti-inflammatory action of the galactolipid monogalactosyldiacylglycerol, EJP. (2005) ;524: :159–68. |
[13] | Ulivi V , Lenti M , Gentili C , Marcolongo G , Cancedda R , De Scalzi Cancedda F . Anti-inflammatory activity of monogalactosyldiacylglycerol in human articular cartilage in vitro: Activation of an anti-inflammatory cyclooxygenase-2 (COX-2) pathway. Arthritis Res. (2001) ;13: :R92. |
[14] | Eriksen NT . Production of Phycocyanin-1 pigment with application in biology, biotechnology, foods and medicine. Appl Microbiol Biotechnol. (2008) ;1: :1–14. |
[15] | Bellometti S , Galzigna L . Serum levels of a prostaglandin and a leukotriene after thermal mudpack therapy. Journal of Investigative Medicine. (1998) ;46: (4):140–5. |
[16] | Bellometti S , Cecchettin M , Galzigna L . Mud pack therapy in osteoarthrosis. Changes in serum levels of chondrocyte markers. Clinica Chimica Acta. (1997) ;101–6. |
[17] | Bellometti S , Bertè F , Richelmi P , Tassoni T , Galzigna L . Bone remodelling in osteoarthrosic subjects undergoing a physical exercise program. Clinica Chimica Acta. (2002) ;97–104. |
[18] | Fioravanti A , Cantarini L , Bacarelli MR , de Lalla A , Ceccatelli L , Blardi P . Effects of spa therapy on serum leptin and adiponectin levels in patients with knee osteoarthritis. Rheumatol Int. (2011) ;31: (7):879–82. |
[19] | Fioravanti A , Giannitti C , Cheleschi S , Simpatico A , Pascarelli NA , Galeazzi M . Circulating levels of adiponectin, resistin, and visfatin after mud-bath therapy in patients with bilateral knee osteoarthritis. Int J Biometeorol. (2015) ;59: (11):1691–700. |
[20] | Fioravanti A , Adamczyk P , Pascarelli NA , Giannitti C , Urso R , Tolodziecki M , Ponikowska I . Clinical and biochemical effects of a 3-week program of diet combined with spa therapy in obese and diabetic patients. A pilot open study. Int J Biometeorol. (2015) ;59: (7):783–9. |
[21] | Ford ES , Li C , Zhao G . Prevalence and correlates of metabolic syndrome based on a harmonious definition among adults in the US. J Diabetes. (2010) ;2: :180–93. |
[22] | Alexopoulos N , Katritsis D , Raggi P . Visceral adipose tissue as a source of inflammation and promoter of atherosclerosis. Atherosclerosis. (2014) ;233: :104–12. |
[23] | Phillips CM , Tierney AC , Perez-Martinez P , Defoort C , Blaak EE , Gjelstad IM , Lopez-Miranda J , Kiec-Klimczak M , Malczewska-Malec M , Drevon CA , Hall W , Lovegrove JA , Karlstrom B . Obesity and body fat classification in the metabolic syndrome: Impact on cardiometabolic risk metabotype. Obesity. (2013) ;21: :E154–61. |
[24] | Arnold M , Pandeya N , Byrnes G , Renehan AG , Stevens GA , Ezzati M , Ferlay J , Miranda JJ , Romieu I , Dikshit R , Forman D , Isabelle Soerjomataram I . Global burden of cancer attributable to high body-mass index in 2012: A population-based study. Lancet Oncol. (2015) ;16: (1):36–46. |
[25] | Astrup A . Low fat diets and energy balance: How does the evidence stand in 2002?. Proceedings of the Nutrition Society ((2002) ;61: (2):299–309. |
[26] | Bell EA . Energy density of foods affects energy intake in normal weight women. AJCN. (1998) ;67: :412–20. |
[27] | Stubbs RJ , et al. Covert manipulation of dietary fat and energy density: Effect on substrate flux and food intake in men eating ad libitum. AJCN. (1995) ;62: :316–29. |
[28] | Di Pietro L . Physical activity in the prevention of obesity: Current evidence and research issues. ACSM. (1999) ;31: :S542–6. |
[29] | Fogelholm M , Kukkonen N , Harjula K , Does physical activity prevent weight gain: A systematic review, Obesity Reviews. (2000) ;1: :95–111. |
[30] | Esposito K , Marfella R , Ciotola M , Di Palo C , Giugliano F , Giugliano G , D’Armiento M , D’Andrea F , Giugliano D . Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA. (2004) ;292: :1440–292. doi:10.1001/jama.292.12.1440 |
[31] | Panagiotakos BD , Polychronopoulos E . The role of Mediterranean diet in the epidemiology of metabolic syndrome; converting epidemiology to clinical practice Lipids Health Dis. (2005) ;4: :7. |
[32] | Oh KJ , Lee DS , Kim WK , Han BS , Lee SC , Bae KH . Metabolic Adaptation in Obesity and Type II Diabetes: Myokines, Adipokines and Hepatokines. Int J Mol Sci. 18: (1) (2016) ) pii: E8. doi:10.3390/ijms18010008 |
[33] | Castelló A , Pollán M , Buijsse B , Ruiz A , Casas AM , Baena-Cañada JM , Lope V , Antolín S , Ramos M , Muñoz M , Lluch A , de Juan-Ferré A , Jara C , Jimeno MA , Rosado P , Díaz E , Guillem V , Carrasco E , Pérez-Gómez B , Vioque J , Boeing H , Martín M . Spanish Mediterranean diet and other dietary patterns and breast cancer risk: Case-control EpiGEICAM study. Br J Cancer. (2014) ;111: (7):1454–62. |
[34] | La Vecchia C . Association between Mediterranean dietary patterns and cancer risk. Nutr Rev. (2009) ;67: (Suppl 1):S126–9. |
[35] | Pelucchi C , Bosetti C , Rossi M , Negri E , La Vecchia C . Selected aspects of Mediterranean diet and cancer risk. Nutr Cancer. (2009) ;61: (6):756–66. |


