Experimental study on the effectiveness of Motivational Counseling (CM) in the nutritional field
Abstract
The project has evaluated the effectiveness of interventions for nutritional counseling through the use of techniques of motivational counseling, aimed at increasing motivation to change unhealthy lifestyles. The study was carried out almost experimentally with three nutritional outpatients, that enrolled subjects to be submitted to nutritional counseling using techniques of motivational counseling representing the “experimental group” and one outpatient which recruited subjects submitted only to traditional Nutritional Counseling representing the “control group”. The trial, conducted between September 2009 to December 2011, was structured in 5 stages: Visit, First Control, Second, Third and Fourth Control. Aspects investigated were: 1) Willingness to change, 2) Motivational factors, 3) Body Mass Index and 4) Lifestyles and physical activity. The work of NO was considered effective if it had obtained following results: not gaining weight for normal weight people, a reduction of at least 5% for overweight in the period that went from the first visit to the fourth control. This definition allowed us to distinguish outcomes in “Success” and “Failures”. For the four motivational factors analyzed in the “Pilot” and “Controls”, it was found that the Inner Fracture and the Temptation decreased, while the Self-efficacy and Importance increased. The increase of scores recorded in the evaluation of the Availability to change has increased the effectiveness of treatment. From the analysis of results for the Willingness to change and the four motivational factors, it was observed that the increase of average scores recorded also an increase of the effectiveness of the treatment.
1Introduction
To maintain a healthy lifestyle and to reduce the excess weight, are not sufficient neither the knowledge of correct alimentation rules nor the simple diet or regular physical activity; the personal motivation has got a fundamental role to modify habits and unhealthy lifestyle. Communication is the essential tool used by health operators who have as objective the promotion of correct behavior and editing risk behaviors both for the individual subjects and for the community in general. In health care, in some moments of the interview, use of counseling skills can be particularly effective: welcoming users, active listening of their needs, in their education in health behaviors, helping the person to accept and maintain a healthy lifestyle, in support to subjects in the course of disease (from acceptance to compliance to treatment). Define the counseling is not easy because there are several theoretical models and schools of thought. A possible general definition is that counseling is a process that relates a professional (counselor) to another person (subject) who feels the need to be supported in the management of a problem or a decision. The counseling is designed as a professional intervention, based on communication and relationship skills, which includes a call for a single, a couple, a family to be joined in the recognition of the necessary information to face a problem, in the search for concrete resources to be used to cope with changes in the assessment of not simple and sometimes conflicting choices. The counselor doesn’t offer advice, doesn’t indicate solutions, neither develops psychotherapeutic paths: the specific quality of his work is to support the person who asks for help in the search for hypotheses, of possible ways of changing situations that have become difficult and a source of discomfort. Objective of the intervention is to enable the capacity and resources customer to reorganize the information held and undertake a process of change towards goals that sees possible and achievable. The customer self-efficacy and empowerment are the conditions on which it is based a counseling intervention, supporting the customer in the search for new behaviors through a decision-making which is author and manager [13]. Most of studies and evaluation tools of motivation for change used in clinical work and research has been developed in the field of substance use in general, in particular alcoholism. These instruments refer more or less directly to the concept of Availability to Change as shown by Prochaska and Di Clemente in their well-known model of stages of change (Fig. 1) [12] The evaluation of the Availability to Change occurs most simply through of the allocation of the subject in a prevalent stadium and more articulately through the creation of a profile that describes the “weight” of the typical components of various stages in the problem representation. In this way you get an assessment of the presence of problem awareness (the reasons for change) the desire / decision to change (the commitment to change) and the concrete implemented of behavioral changes (actions to change). Knowing that some specific “factors” that significantly affect the movement along stages, and among these in particular were identified as two factors [11], the Inner Fracture and the Self-efficacy, that changed over time affect the Availability to Change, constituting dynamic elements very relevant in outpatients. The term Inner Fracture [10] shows the painful perception of a contradiction between what a person is and what would be (or could, or should), in relation to personal self-image, their system of values and resulting goals and aspirations; the comparison between the objective to be pursued and perception of their current condition is considered an important motivating element [7]. Behavior and conflicting conditions with its self- image (ideal) are perceived as “threats” that must somehow be reduced [18] with a behavior modification and / or its representation. Evaluation of Inner Fracture can be made by considering both concerns, dissatisfactions of the current situation (the need for change) and the value and importance that the change has respect their personal goals (desire to change). The importance of the sense of self-efficacy [3] in change processes is supported by a very extensive scientific literature; the confidence of a person in his own ability to achieve and maintain a specific objective is considered a predictor factor very important in the field of problems related to the drugs use [14]. The evaluation of the Self-efficacy is mostly performed through an estimation of their ability to cope with high-risk situations; are mainly used tools that explore predetermined situations [1, 4] or with semi-structured interviews [9]. From these ratings we get an estimate of the capacity perceived by the subject (the confidence in the change). The integration of the motivation to change description in a “three-factor model” thus appears with clear clinical utility, early exposed; it is also helpful to have tools, easy administration, which will enrich the assessment of Availability to Change (Awareness, Commitment, Shares) with simultaneous consideration of the Inner Fracture (Need and Desire) and of Self-efficacy (Confidence). The Italian research in the evaluation field of the motivation for change have been developed for 15 years from a questionnaire, called MAC, it can provide a synchronous evaluation of the three factors, validated in the version for heroin [15] and for tobacco smoke [6]. The experiences of use of previous versions of the MAC led to a later version of the questionnaire, called MAC2, validated in the form for use of alcohol [16, 17].
The study had 2 objectives:
1) Building a model of individual folder for subjects who access to nutritional outpatients.
2) Evaluate the effectiveness of the interventions of nutritional counseling of AN of SIAN of 4 Local Health Units (ASL) Piemontesi (ASL TO4, TO5 ASL, ASL and ASL AT NO).
The expected results were:
1) Evaluate the effectiveness of nutritional counseling through dashboard of indicators defined “ad hoc” in the individual folder (dropout rate; weight loss at 3, 6 and 12 months; behavioral change - food, physical activity, both).
2) Measure the motivational stage of the subject to achieve the most suitable and effective nutritional intervention.
2Materials and methods
The project, funded by Regione Piemonte, has evaluated the effectiveness of interventions for nutritional counseling through the use of techniques of motivational counseling (CM), aimed at increasing motivation to change unhealthy lifestyles. The study has been made of almost experimental with 3 nutritional outpatients (AN) that enrolled subjects for a nutritional counseling using traditional techniques of motivational counseling (Experimental treatment - Intervention - CM) representing the “Pilot group” (GS - Cases) and outpatients which recruited subjects submitted only to traditional nutritional advice (Standard treatment - CN) representing the “Check group” (GC - Controls). Each subject was followed over time: an initial enrollment visit and four subsequent visits. The trial, conducted between September 2009 to December 2011, was divided into five stages based on the organization of the NC in AN (Fig. 2):
• STAGE 1 - t0: Visit (Vs);
• STAGE 2 - t1: First Check (Check 1) After 1 month from visit;
• STAGE 3 - t2: Second Check (Check 2) After 2 months from visit;
• STAGE 4 - t3: Third Check (Check 3) After 4 months from visit;
• STAGE 5 - t4: Fourth Check (Check 4) After 6 months from visit.
To “visit” were recruited by health operators (OSS) of AN eligible subjects, within 6 months was followed by subsequent checks. Health operators of ASL of SIAN for the “Pilot group” were trained on the CM and on the use and interpretation of certain tools to assess subjects recruited motivation to change to healthy eating habits and regular physical activity (Test 3 At EMME: MAC2-AL and EMME 3 AF: MAC2-AF); therefore they have completed the nutrition counseling using traditional techniques of CM (Experimental treatment - Intervention - CM). While caregivers of SIAN ASL the “control group” have completed only nutritional counseling Traditional (Standard treatment - CN). The study was almost experimental (without random assignment of subjects in the2 groups):
| Before | Action | After | |
| Pilot group (ASL TO5, ASL AL, ASL TO4) | |||
| O | X | O | |
| Check group (ASL NO) | |||
| O | O | ||
O = Tracking of weight, height, BMI calculation, eating habits, physical activity, motivation to change.
X = Motivational Counseling (CM).
In STAGE 1 - Visit: health operators of AN of SIAN of 4 ASL given before the Visit test Emme3 AL (VMC-AL) and AL Emme3 (VMC-AF), during the Visit the subject individual Folder, after Visit test Emme3 AL (MAC 2R-AL) and AL Emme3 (MAC 2R-AF).
In STAGE 2 - First Control (Check 1): health operators of AN of SIAN of 4 ASL given during the Control 1 the subject individual Folder, after 1 Control Questionnaire CLICO.paziente.
In STAGE 3 - Second Control (Check 2): health operator of AN of SIAN of 4 ASL given during the Control 2 the subject individual folder, after two controls test Emme3 AL (MAC 2R-AL), AL Emme3 (MAC-2 R AF) and finally the Questionnaire CLICO.paziente.
In STAGE 4 - Third control (Check 3): health operators of AN of SIAN of 4 ASL given during 3 Control subject individual folder, after 3 Control Questionnaire CLICO.paziente.
In STAGE 5 - Fourth Control (Check 4): health operators of AN of SIAN of 4 ASL given during Knob 4 subject individual folder, after 4 Control test Emme3 AL (MAC 2R-AL), AL Emme3 (MAC-2 R AF) and finally the Questionnaire CLICO.paziente.
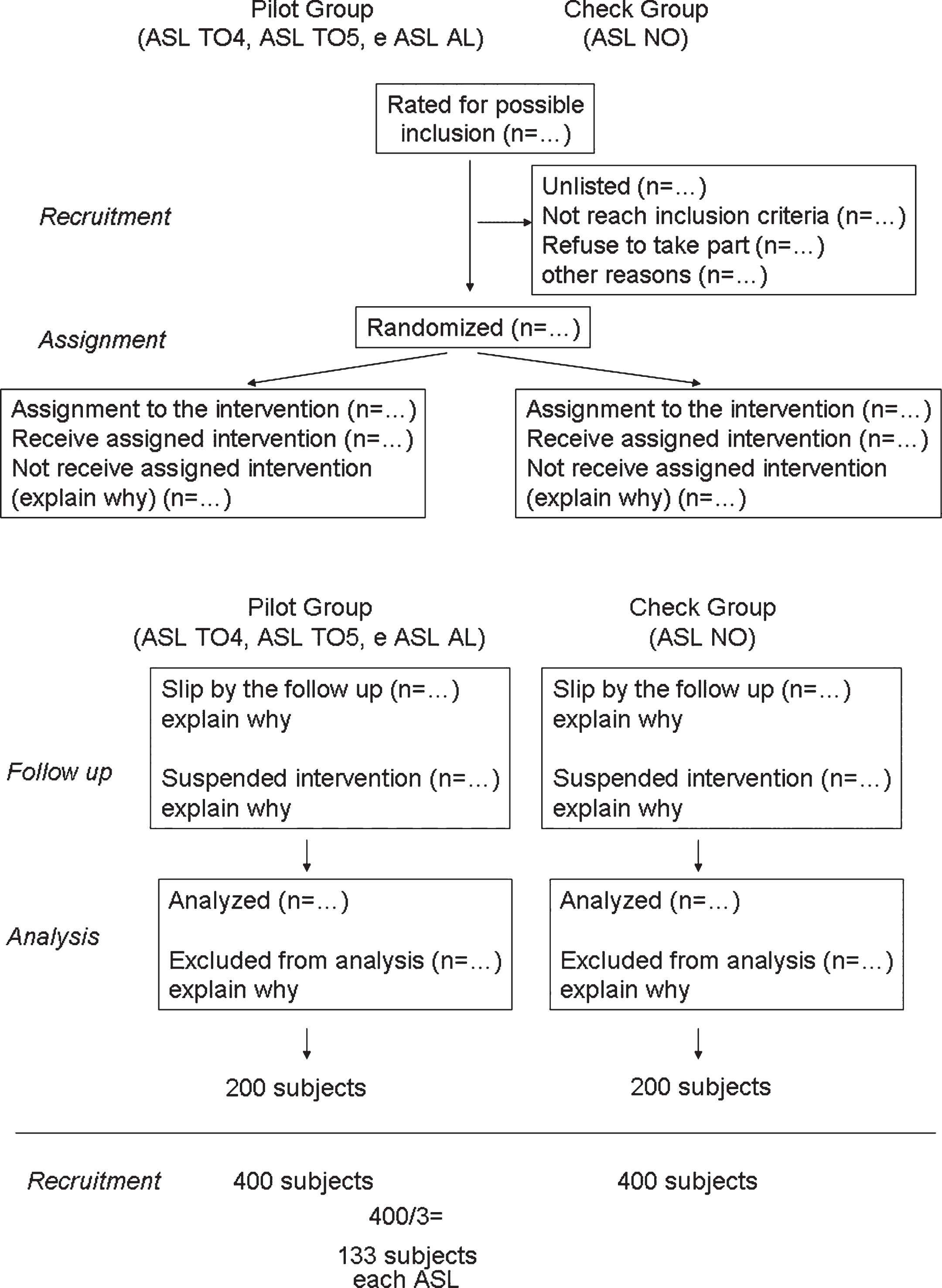
The study design was structured by following the suggestions in the CONSORT statement (AIRAS, 2013) (Fig. 3).
Subjects of AN, for join the research, they had to meet following inclusion criteria:
✓ lack of eating disorders and severe psychiatric diseases that alter the relationship with reality;
✓ age of majority;
✓ preserved cognitive abilities to understand and answer to Test Emme3;
✓ chance to continue the path in the outpatient for at least 6 months.
Activities of the AN were considered effective if we obtained following results: for normal weight not gain weight, to overweight and obese reduction of at least 5% in the period between the first visit to the fourth control (6 months, a minimum of 5 and a maximum of 8). This definition allowed us to distinguish results of treatments in “Success” and “Failure”. Frequency distributions were made on key sociodemographic variables and lifestyles of subjects and analysis of variance to assess differences in the scores of BMI between GS and GC in different times of the study. Subjects were recruited from the AN of SIAN of 4 ASL among those who have booked nutritional counseling for the first time and who have responded to the requirements of inclusion. They excluded those people who called for a single appointment to have a pattern of diet or nutrition counseling. Eligible subjects were recruited by health operators of AN in the following periods:
– AN ASL NO during the period between 22 March 2010 to the end of March 2011;
– AN TO5 of ASL, ASL AL, ASL TO4 in the period between May 2010 to the end of March 2011.
2.1Survey tools
At each meeting they detected information through various tools. Issues were investigated: 1) Availability for change, 2) Motivational factors, 3) BMI and 4) eating habits and physical activity. We built “ad hoc” model of electronic personal folder (CI) divided into 7 sections to collect subject information and evaluate the effectiveness of CN interventions. The Emme3 AL / AF is a set of tools for evaluation of motivation to change to healthy eating habits and regular physical activity. It was divided into two sets of tools, Emme3 AL (diet) and Emme3 AF (physical activity). For research it has been used:
• The set of centesimal scale VMC (which can be “AL” or “AF”). It was divided into six questions that can be answered on analog centesimal scale and evaluated factors: Inner Fracture, Self Effectiveness, Availability of change, stabilization of change, Temptation, Importance.

• The questionnaire MAC2 R (which can be “AL” or “AF”). It was divided into 18 sentences to which one replied on 7 levels Likert scale (0 to 6) aims to assess 9 factors (2 items for factor): Precontemplation, Contemplation, Determination, Action, Maintenance, self Effectiveness, Temptation, Inner Fracture, Importance.

Tools provided an evaluation of the presence in the subject of following issues:
• Precontemplation (P). Subjects with prevailing Precontemplation issues are not willing or do not consider it appropriate to implement significant changes in their lifestyle (eating habits / physical activity): they do not pay attention to the behavior in question and for them is not a problem. They not usually occur spontaneously to request a therapeutic intervention and possible contacts are due to send by medical doctor or specialized doctor.
• Contemplation (C). Subjects with prevailing Contemplation issues are basically undecided; They may require a consultation and try to implement some changes, but have not yet “develop” a real decision to change unhealthy behavior.
• Determination (D). Subjects with prevailing Determination issues are close to the “decision threshold”, they are “ready” to implement the change; they seek and expect to receive concrete information and advice to implement the desired pitch.
• Action (A). Subjects with prevailing action issues have changed recently (no more than six months), their behavior is not healthy and they still feel committed to consolidate introduced changes (eating habits / active lifestyle).
• Maintenance (M). Subjects with prevailing Maintenance issues introduced some time (at least six months), the health behavior and they are making efforts to consolidate this choice.
• Self Effectiveness (AE). Subjects who score high in the scale of Self-efficacy have confidence in their ability to achieve or sustain introduced healthy behavior. They think that this goal is within their reach and that they can reach it with the personal and environmental resources available.
• Temptation (TE). Subjects who score high on this scale feel a strong attraction or pleasure towards unhealthy behavior (sedentary life, pleasures of food). The temptation measure the attraction it exerts instead the weakness in front of the object.
• Inner Fracture (FI). Subjects who score high on this scale declare themselves unhappy about the considered behavior. They concerned about the state of things and they fear possible repercussions on their quality of life.
• Importance (I). Subjects with high scores on this scale give much value to correct behavior and thinks this is considered essential to their well-being. The importance attached to the desired result is considered a decisive factor in both phases before, in the early stages and after the change.
• Willingness to change (DC). It’s a significant construct in stages before the change and indicates the favorable attitude to change and the likelihood of action in that direction.
• Stabilization (ST). It’s a significant construct in phases that follow the change. It indicates the degree of acquisition and rooting of the new condition.
As all evaluation questionnaires also Emme3 AL/AF needed several precautions given to ensure the reliability of results. We had to ensure sufficient privacy to subjects who were asked to complete the questionnaire, providing a comfortable, quiet and free of distractions. The Emme3 AL/AF was designed to be completed independently from the subject after a brief description of its features. In case that a subject needed help, support was provided through reading sentences together with the person and it was determined the correct interpretation, possibly providing simple explanations. They were provided by health operators of the AN of SIAN, in these cases, indications neutral and essential as possible, to avoid significantly affect the literal meaning of sentences. At the end of the administration we checked, that there have been no omissions. This final check was carried out in the presence of the subject, in order to be able to enter any missing data otherwise no longer recoverable. With these tools, we wanted to evaluate in terms of effectiveness measuring certain parameters are changed after the intervention of CM compared to CN.
2.2Statistical analysis
We carried out distributions of relative frequency and indicators of central tendency on the main socio-demographic and lifestyles variables in subjects enrolled. To evaluate differences in BMI scores in GS and GC in different times of the study we used variance analysis. With “post hoc” Bonferroni test we evaluated both GS and GC between which times of the study differences in the reduction of BMI were statistically significant. Various items that make up the motivational scale in the two groups indicated in summary rate were calculated and differences between t0 and t4 scores. Differences obtained were subjected to the t-test to assess if there was a statistically significant difference between two groups. With the t-test we evaluated some changes of motivational profile as a function of “Success” or “Failures” in weight loss in both GS and GC. Statistical analysis were performed with the SAS System 9.2 software, modules and Base Stat.
3Outcome
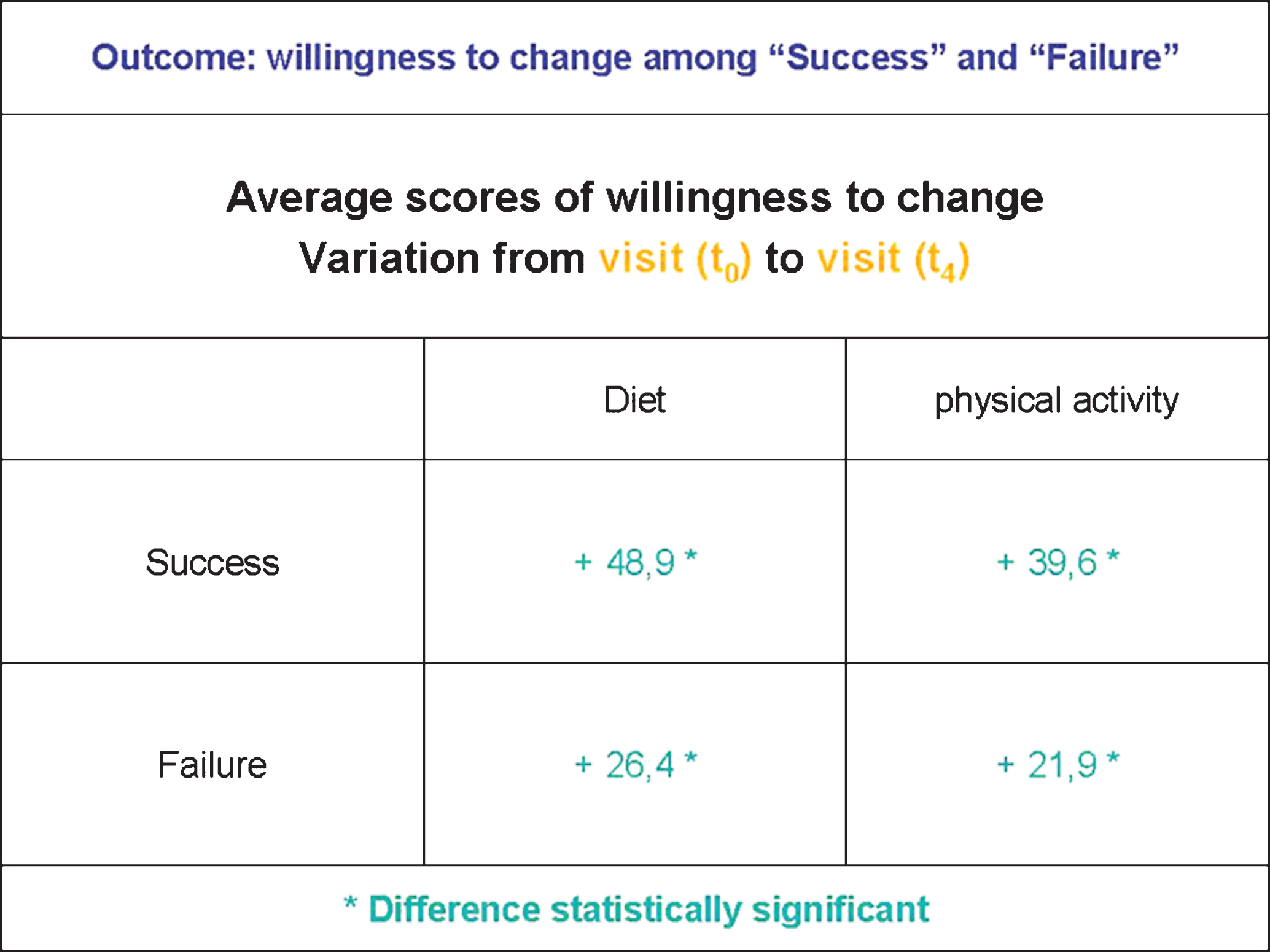
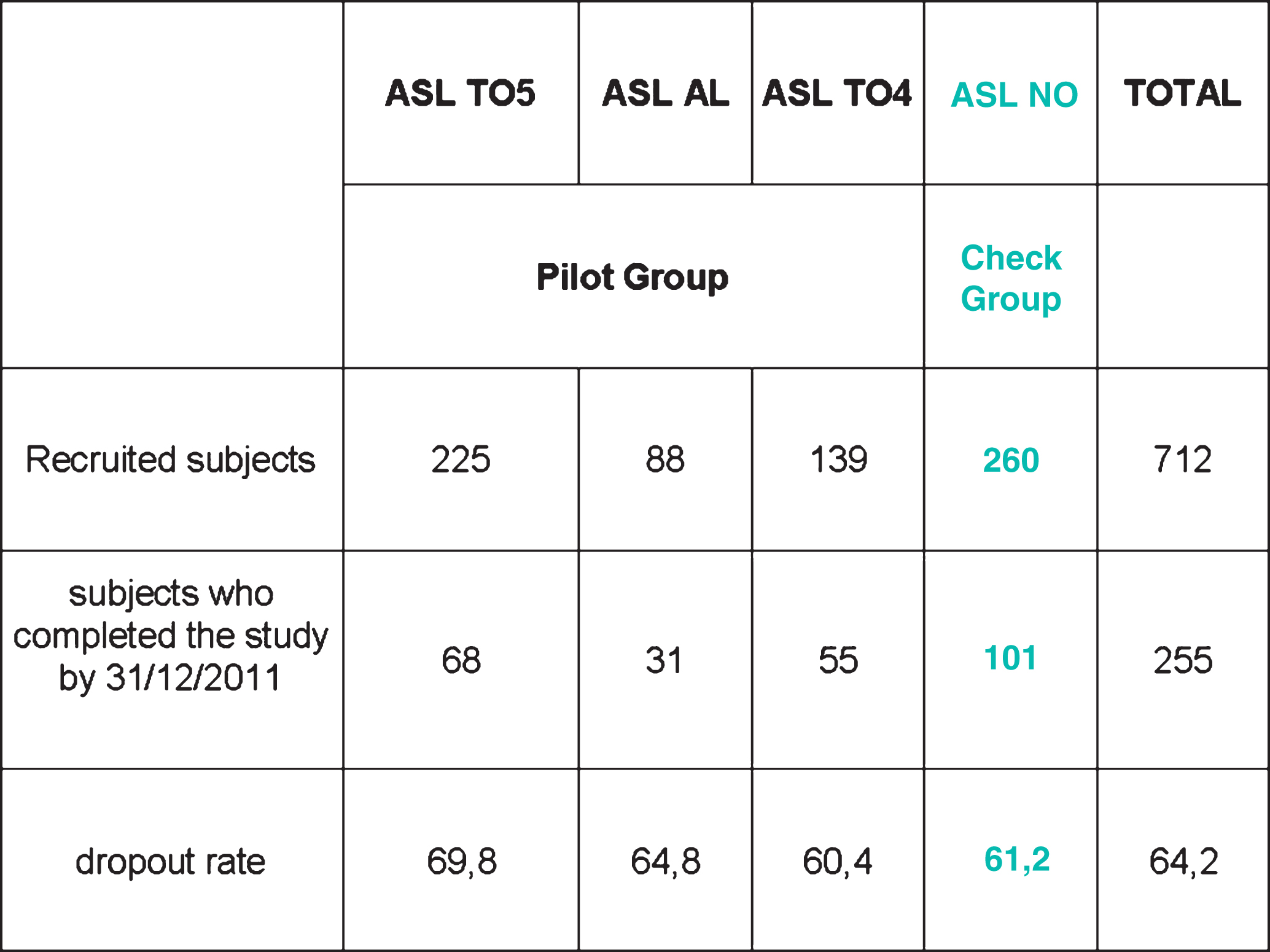
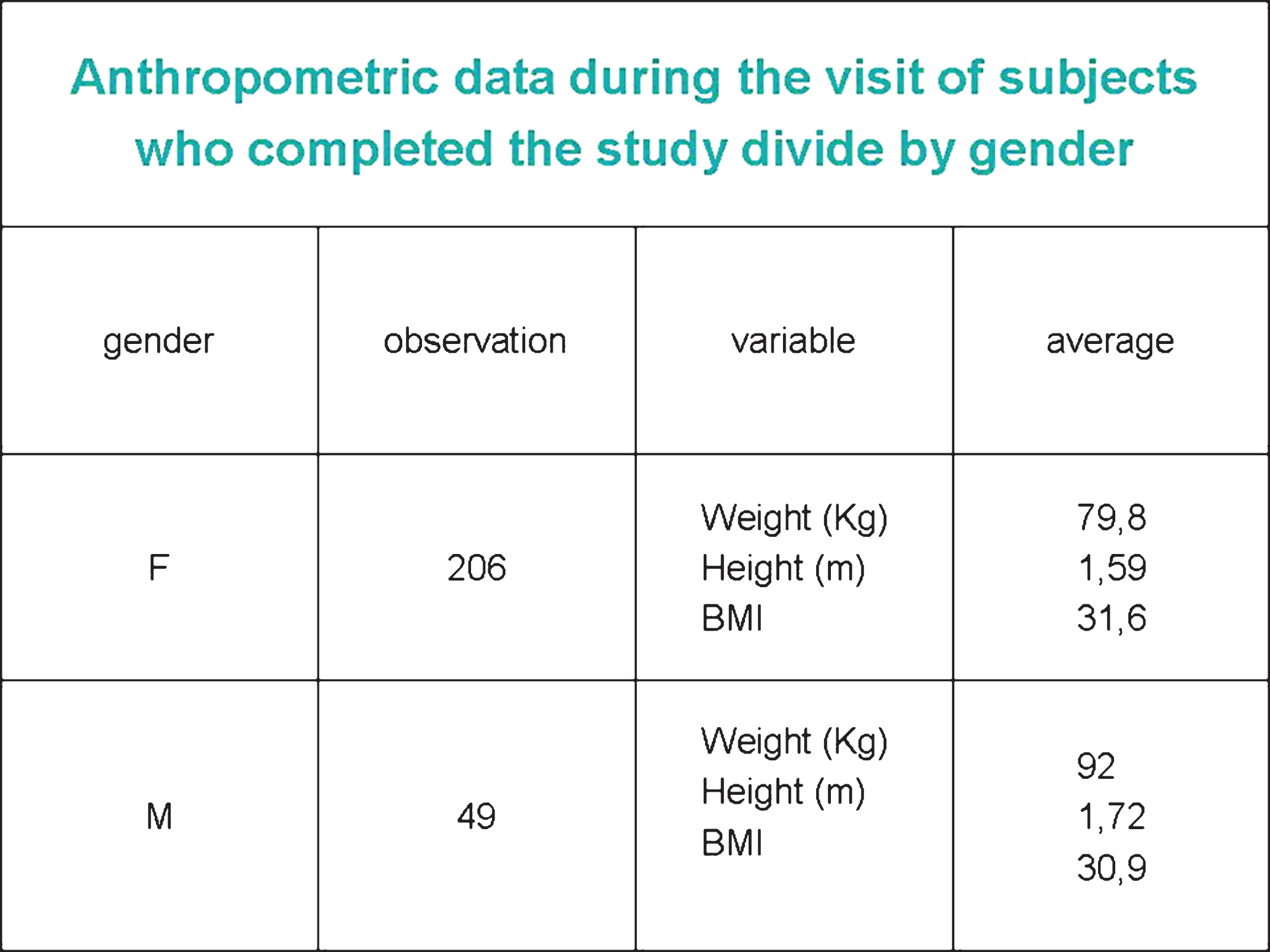
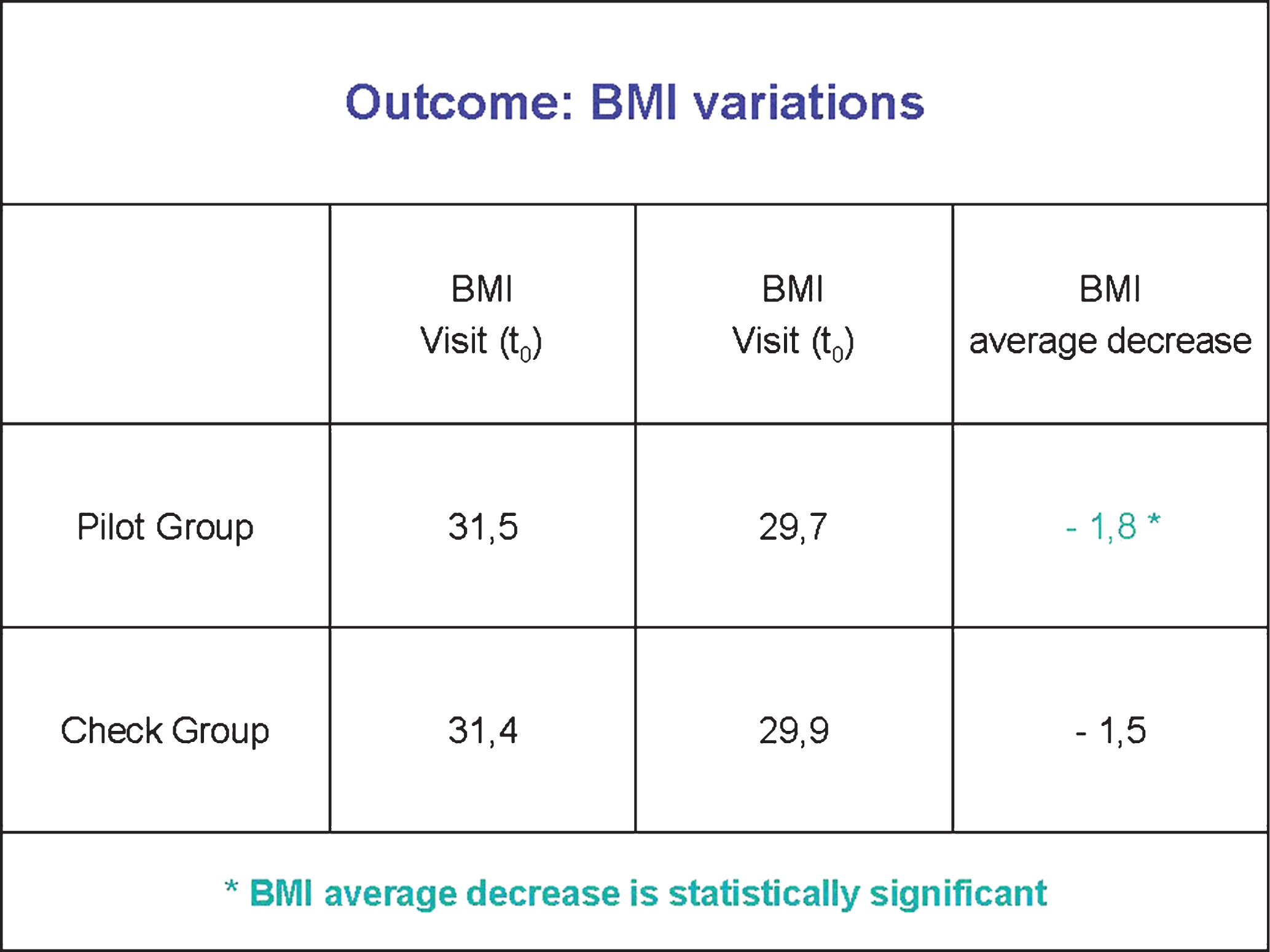
They were enrolled 712 subjects distributed over the 4 AN of participants ASL (452 in the GS and 260 in the GC). The dropout rate was 64.2% with no significant differences between the 4 AN. Only 255 subjects (154 “cases” and 101 “controls”) completed the course at 31 December 2011 (Chart I). For all variables collected at the first visit, there were no appreciable differences between the 2 groups. The average age of participants was 47.5 (SD 12.6), 81% were women. At the first visit, the women weighed an average of 80 kg (DS 14) with BMI 31.6 (DS 5.4), men 92 kg (DS 15) with BMI 30.9 (DS 4.3) (Chart II). The 87.4% consumed breakfast (among these, 38.1% in an inadequate way from a caloric point of view). 45% and 54.5% have consumed two or more servings a day respectively of vegetables and fruit. The more frequent eating habit was “snacking” (41.2%), followed by “not balanced choice of food” (38.4%). 43.8% they did not perform any type of physical activity and 29.5% have played for less than 30 minutes a day. The comparison of the change in BMI between subjects treated with CM and subjects treated with CN has been a major achievement in the evaluation of the effectiveness of CM in 154 subjects exposed to treatment with CM, the BMI rose from an average of 31.5 at the visit (t0) to a mean value of 29.7 to fourth check (t4), the decrease of 1.8 points of BMI is statistically significant already at t3 compared to t0. In 101 subjects exposed to treatment with CN BMI rose from an average of 31.4 to visit (t0) to an average of 29.9 in the fourth control (t4), a decrease of 1.5 points of BMI it’s not statistically significant (Chart III). In the analysis compared to the availability to change both for eating habits and for physical activity were not statistically significant differences between GS and GC for both power and for physical activity, average scores of Availability to the change were higher in the “Success” (48, 9 for diet, 39.6 for physical activity) than the “Failures” (26.4 for diet, 21.9 for physical activity), these differences were statistically significant (p < 0.05). Within each groups, however, were not statistically significant differences between subjects exposed to treatment with the CM and subjects exposed to treatment with the CN (Chart IV). Four motivational factors analyzed in the “Cases” and “Control” (Importance, Inner Fracture, Temptation and Self-efficacy), both for the diet and for the physical activity, it showed that the Inner Fracture and Temptation decreased while Self-efficacy and importance increased (with the exception of the importance of diet in the “Controls” which decreased). Differences in these scores did not significantly statistically differ between “cases” and “controls”, therefore was not possible to say that the CM was more effective than CN changing the statement of four Motivational factors.
4Discussion
By the analysis of the results obtained from the processing of various items contained in the survey instruments (Individual Folder subject, and TEST EMME3 AF and AF) has revealed that of the total number of enrolled subjects research participants (712 subjects enrolled) at the outpatients of SIAN only 36% (255 subjects recruited) concluded the study, of them 154 have been subjected to traditional nutritional counseling using techniques of motivational counseling (experimental treatment - Intervention - CM) representing the “experimental group”(GS - Case) and 101 subjects underwent only the traditional nutritional advice (standard treatment - CN) representing the “Control Group” (GC - Controls). The Churn (Drop-out rate) was 64%, higher than that reported in the scientific literature [8]. The low number of people recruited and, therefore, of those who have completed the study decreased the statistical power of the obtained results. In the research we calculated the BMI average values separately for “Cases” and “Controls” in all stages of the study in which this parameter was measured (t0, t1, t2, t3, t4). In the 154 “cases” the BMI increased from an average value of 31.5 during the visit (t0) at an average value of 29.7 in the fourth control (t4). The decrease of 1.8 points of BMI recorded in “Cases” was statistically significant already at t3 than the t0. In the 101 “controls” the BMI increased from an average value of 31.4 to visit (t0) to an average value of 29.9 in the fourth control (t4). The decrease of 1.5 points of BMI recorded in “Controls” is not statistically significant. Both in “Cases” and “Controls” there was an average decrease of BMI between t0 and t4, the average decrease in “Case” (1.8 points of BMI) was higher than the “Controls” (1,5 points of BMI); so it would appear that the CM has been more effective than CN. However, our data not allowed to say that the difference of the average reduction in BMI between “Cases” and “Controls” was statistically significant, so it was not possible to state that the CM was more effective than CN in reducing BMI. Even a recent systematic review and meta-analysis of randomized and controlled study [2], which evaluated in overweight or obese adults how much the actions of Motivational Counseling could affect on their behavioral changes compared to weight control; it suggested that motivational counseling appears to increase the weight loss in overweight and obese subjects. In this systematic review the motivational counseling was associated with a greater reduction in BMI than controls, there was a significant reduction in body weight in subjects belonged to the group exposed to motivational counseling intervention than the subjects belonged to the control group. In our research were also analyzed the Availability to change and the four Motivational Factors: Importance, Inner Fracture, Temptation and Self-efficacy, which significantly influence the movement along the various stages of change (precontemplation, contemplation, preparation, action and maintenance), and among these in particular have been identified by Miller and Rollnick [11] two factors, the Inner Fracture and the Self-efficacy, that changed over time affect the Availability to change, creating dynamic elements very relevant in the clinic. From the overall analysis of the results concerning the Availability to change and the four motivational factors (Importance, Inner Fracture, Temptation and Self-efficacy), it was observed that the increase of the average scores recorded in the assessment of the availability to change, it seemed to increase parallel the effectiveness of treatment. So it can be concluded that who lost weight, during a treatment, has seen change some motivational parameters:
– Increased the availability to change (and therefore to treatment), the Self-efficacy (defined as a person’s confidence in their ability to achieve and maintain a specific target, is considered a predictor also very important in the field of the problems related to ‘use of sostanze [4, 14]), and Importance (understood as the degree of values and objectives investment);
– And decreased the Inner Fracture (understood as the painful perception of a contradiction between what a person is and what he wants) and susceptibility to Temptations. Also in our research we analyzed the Availability to change depending on Outcome of treatment, the sample of subjects recruited who completed the study was divided into 2 groups: “Success” and “Failures”; a subject is included in the group of “Successes” if in the period between the first visit to the fourth control Visit (6 months: minimum 5 and maximum 8 months) has seen;
– its weight reduced by at least 5% (for overweight and obese);
– its weight has not increased (for normal weight).
The “Successes” were obtained in 45.5% of the recruited subjects sample who completed the study, in particular, they were higher in the “Cases” (46.7%) compared to the “Controls” (43.6%). Both the Food and the Physical Activity the average scores of Availability to the change were higher in the “Successes” than the “Failures”. These differences were statistically significant. So it can be said that with the increase of scores recorded in the assessment of the availability to change has increased the effectiveness of treatment. In other words, major was the motivation to change, major results were obtained in terms of weight reduction. There were no statistically significant differences between “cases” and “controls”, therefore it was not possible to say that the CM was more effective than the traditional treatment in increasing average scores of Availability to change between t0 and t4 for both “Success “for the” Failures”. Finally, in our research we analyzed the variation of the four motivational factors (Importance, Inner Fracture, Temptation and Self-efficacy) versus Outcome of treatment (“Success” and “Failures”). Most of the motivational factors for both the Food and the Physical Activity have varied considerably between “Successes” and “Failures”; But the differences between the two groups (“Success” and “Failures”) were statistically significant only in the context of Food, in particular:
– increased the Importance of Food in the “Success”;
– decreased the Inner Fracture of Food in the “Success”;
– decreased the Temptation in the Food “Success”;
– increased the Self-efficacy in Food in the “successes”.
Between “Cases” and “Controls” did not reveal never statistically significant differences in average values of four motivational factors for both Food and Physical Activity. So it can be said that, when you start up a treatment aimed to control and weight loss, you need to apply specific strategies involving these elements, as they play an essential role in making change to correct lifestyles. The considerations that have emerged from the analysis of the results concerning the Availability to change and Motivational Factors, with related effects on the lifestyles of the recruited subjects who completed the study, are also suggested by recent scientific research [7], which shows that the motivational Counseling supplied as an independent component in addition to a behavioral program of weight loss can increase weight loss and probably exerts its beneficial effects by enhancing the commitment to the treatment of the subject and to adopt the behavioral recommendations. Our research was the expression of the needs shared by professionals of SIAN piemontese (italian) to work together to improve the quality, appropriateness and effectiveness of the dietetic- nutritional advice interventions as well as promoting a rational therapeutic approach and careful about the ratio cost / benefits; these requirements have led to a common journey made together and which ended with the results of that research.
References
[1] | Annis HM , Sklar SM , Turner NE . The Drug Taking Confidence Questionnaire (DTCQ): User’s Guide Addiction Research Foundation, Toronto, 1997. |
[2] | Armstrong MJ , Mottershead TA , Ronksley PE , Sigal RJ , Campbell TS , Hemmelgarn BR . Motivational interviewing to improve weight loss in overweight and/or obese patients: A systematic review and meta-analysis of randomized controlled trials. Obesity Reviews. (2011) ;2: (9):709–723. |
[3] | Bandura A . Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. (1977) ;84: :191–215. |
[4] | DiClemente CC , Carbonari JP , Montgomery RPG , Hughes S.O. . The alcohol abstinence self-efficacy scale. J Stud Alcohol. (1994) ;55: :141–148. |
[5] | DiLillo V , West DS . Motivational interviewing for weight loss. The Psychiatric Clinics North America. (2011) ;34: (4):861–869. |
[6] | Guelfi GP , Spiller V , Scaglia M . La valutazione della motivazione al cambiamento nel tabagismo: Il questionario MAC/T. Atti del Convegno: “A fuoco il fumo”, 1° Congresso Nazionale sul Tabagismo. Padova (1999) ;30. |
[7] | Kanfer FH . Self regulation and behavior In: Hechhausen H., Gollwitzer PM, Weinert FE (eds) Jenseits des Rubikon, Heildelberg, Springer-Verlag. (1987) , pp. 286–299. |
[8] | Melin I , Reynisdottir S , Berglund L , Zamfir M , Karlström B . Conservative treatment of obesity in an academic obesity unit. Long-term outcome and drop-out. Eating and Weight Disorders. (2006) ;11: (1):22–30. |
[9] | Miller KJ , McCrady BS , Abrams DB , Labouvie EW . Taking an individualized approach to the assessment of self efficacy and the prediction of alcoholic relapse. J Psychopathol Behav. (1994) ;16: :11–20. |
[10] | Miller WR . Motivational interviewing with problem drinkers. Behav Psychoth. (1983) ;11: :147–72. |
[11] | Miller WR , Rollnick S.. Il colloquio motivazionale. Centro Studi Erickson, Trento, (2004) . |
[12] | Prochaska JO , DiClemente CC . Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research and Practice 19: :276–88. |
[13] | REGIONE PIEMONTE Sanitá. Pubblicazioni. L’attivitá ambulatoriale di nutrizione e le abilitá di counselling. Linee di indirizzo, (2011) . |
[14] | Rollnick S , Heather N . The Application of bandura’s self efficacy theory to abstinence oriented alcoholim treatment. Addict Behav. (1982) ;7: :243–250. |
[15] | Spiller V , Guelfi GP . La valutazione della motivazione al cambiamento: Il questionario MAC/E (Assessing Motivation for Change in Heroin Addicts: The MAC/E Questionnaire). Bollettino delle Farmacodipendenze e Alcoolismo (Italian Journal on Drug Addiction and Alcoholism). (1988) ;21: :7–16. |
[16] | Spiller V , Scaglia M , Meneghini S , Vanzo A . Assessing motivation for change toward healthy nutrition and regular physical activity. Validation of two set of instruments. Mediterranean Journal of Nutrition and Metabolism. (2009) ;2: :41–47. |
[17] | Spiller V , Zavan V , Guelfi GP . Assessing motivation for change in subjects with alcohol problems: The MAC2-A questionnaire. Alcohol Alcoholism. (2006) ;41: :616–623. |
[18] | Steele CM . The psychology of self-affirmation: Sustaining the integrity of the self. In: Berkowitz L (ed) Advances in Experimental Social Psychology. Academic Press, New York. pp. (1988) 261–302. |
Figures and Tables
Fig.1
Prochaska Stages of Change Model (REGIONE PIEMONTE. Sanità. Pubblicazioni. L’attività ambulatoriale di nutrizione e le abilità di counselling. Linee di indirizzo, 2013).
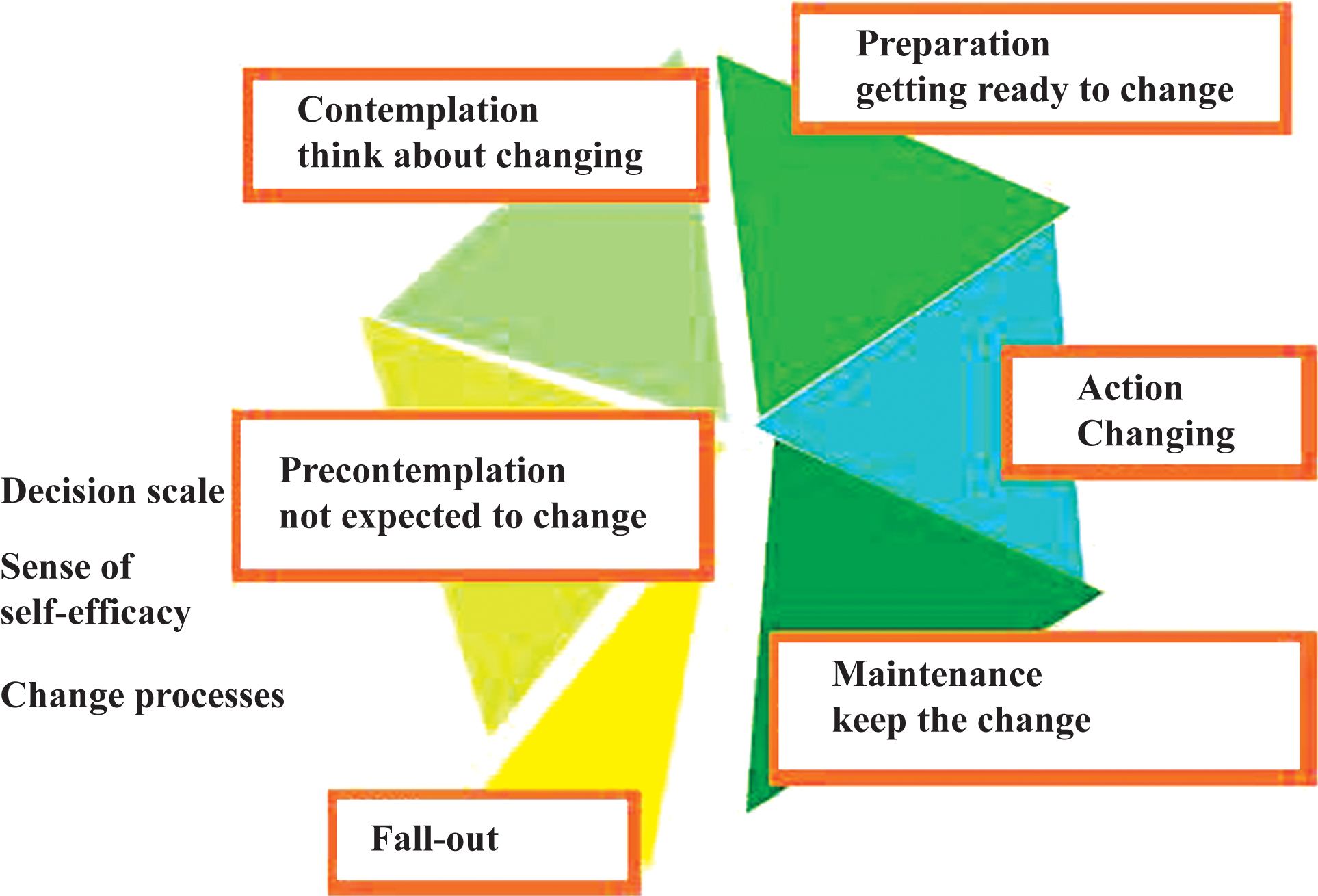
Fig.2
Study design.
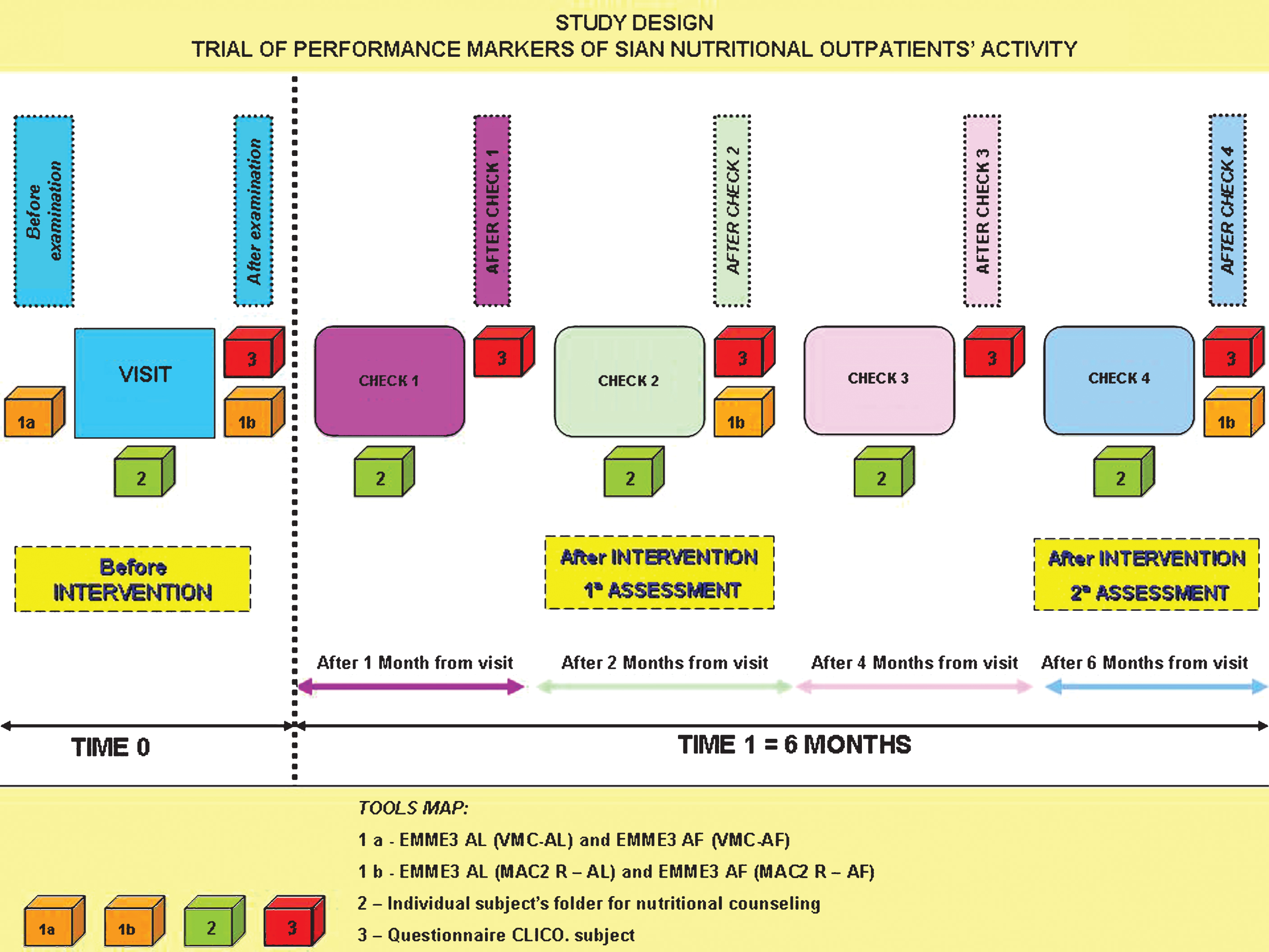
Fig.3
Flow chart of the sequence of stages in a randomized trial (recruitment, intervention assignment, follow-up and data analysis) according to the CONSORT (Consolidated Standards and Reporting Trials) used to structure the study design of research project (AIRAS, 2013).
ChartI
Sample size.
ChartII
Anthropometric data during the visit of subjects who completed the study divide by gender.
ChartIII
BMI variations among “Pilot” subjects and “Check” subjects.
ChartIV
Willingness to change among “Success” and “Failure”.