
Assessment of mental health and quality of life among children with congenital heart disease
Abstract
PURPOSE:
The current study aimed to determine the prevalence of specific psychiatric disorders, identify predictors associated with these disorders, and assess the quality of life (QoL) among children with congenital heart disease.
METHODS:
This comparative cross-sectional study was conducted in the National Heart Institute outpatient clinics. It included 204 children with structural congenital heart defects (CHD). In addition to assessing QoL with the Pediatric Quality of Life Inventory scale, the Mini-International Neuropsychiatric Interview for Children and Adolescents was utilized to identify psychiatric disorders in the children studied.
RESULTS:
Children with CHD were at increased risk for mood and anxiety disorders. They were also more susceptible to obsessive-compulsive disorder than the comprative healthy group. In children with CHD, the cyanotic group demonstrated a greater decrease in QoL than the acyanotic group.
CONCLUSION:
Children with CHD have an increased risk of psychiatric disorders and a lower overall QoL score.
1Introduction
Congenital heart defects (CHD) are the most prevalent congenital disorders, affecting 1% of live births in varying degrees [1], ranging from mild (no urgent or possible surgical intervention is required) to severe or complex (typically defined as CHD requiring surgical intervention within the first month to one year of life) [1].
Even though the overall mortality rate has decreased, patients with complex CHD frequently require multiple interventions throughout their lives, and many surgical and medicinal treatments are palliative in nature [2]. Due to improved survival, more adolescents are being diagnosed with CHD, which has increased awareness of non-cardiac comorbidities, such as general mental health [2].
The majority of children and adolescents with CHD are at risk for developing non-cardiac morbidities due to the lifelong effects and complications of the underlying heart disease [3]. Likewise, medical limitations and a series of life-altering events, such as repeated hospitalizations and ongoing medical emergencies, may have a significant adverse effect on the mental health of adolescents and adults [3].
Congenital heart disease increases the likelihood of emotional distress symptoms such as sadness and anxiety in children and adolescents. Emotional distress is well-known to impair quality of life (QoL), psychosocial functioning, and life satisfaction [4].
This study aimed to assess the prevalence of certain psychiatric disorders, identify predictors associated with these disorders, and assess QoL among children with congenital heart diseases.
2Methods
2.1Study design
A comparative cross-sectional study was conducted in the outpatient clinics of the National Heart Institute, Giza, Egypt, in the period from March 2021 to August 2022. The study included 204 children between the age of five and 16 years with structural CHD, as confirmed by echocardiogram. The comparison group included 204 healthy children of matched age and sex who were randomly selected relatives of children with CHD. Children with intellectual disability, comorbid psychiatric or neurological disorders, or other chronic systemic diseases, as well as those with a history of psychotropic drug use, were excluded from the study.
2.2Sample size and sampling technique
The sample size needed for this study was calculated based on the reported prevalence of psychological disorders among children with CHD (18.2%) [5]. An alpha level of 5% and power of 80% determined a minimum required sample size of 187 candidates. Assuming a nonresponse rate of 10%, the final sample size was 204 children with CHD. A systematic random technique was used to select participants.
All participants were evaluated as follows:
1. A self-constructed questionnaire was used for obtaining participants’ demographic data such as age, sex, level of education, and medical history of all patients with CHD (the age of onset of symptoms, diagnosis of CHD, previous cardiac catheterization, and previous cardiac surgery). The Fahmy and El Sherbini questionnaire was used to determine socioeconomic status (SES) [6].
2. The Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), a brief structured diagnostic interview, was used to screen for psychiatric disorders and suicidality in children and adolescents aged six to 17. It was developed in collaboration between psychiatrists/clinicians in the USA and Europe and was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) and International Classification of Diseases, 10th revision (ICD-10) [7]. The Arabic version of the MINI-KID utilized in the present study has been proven to be valid [8].
Each part of MINI-KID included screening and diagnostic questions, with 2-4 screening questions for each disorder using branching tree logic. If the screening questions were answered positively, additional symptom questions for the specific disorder were asked. Each question was formatted in the binary “yes/no” format.
MINI-KID administration takes approximately 30 minutes. The interview is administered to the child along with the parent(s), although it can be administered to adolescents without the presence of a parent. In addition, the test was administered by a psychiatrist with at least five years of experience diagnosing neuropsychiatric disorders in children. The MINI-KID has exhibited inter-rater reliability, test-retest reliability, and validity based on an examination of a sample of children and adolescents [9].
3The Pediatric Quality of Life Inventory (PedsQL)
The PedsQL is a modular approach to measure health-related quality of life (HRQoL) in healthy children and adolescents and those with acute and chronic health conditions. The questionnaire can be filled out by both parents (the Proxy Report) and children and adolescents (the Self-Report). The 23-item PedsQL compromises four Generic Core Scales (eight items for physical functioning and five items for each emotional, social, and school functioning), which were designed to measure the core dimensions of health as delineated by the World Health Organization [10, 11].
3.1Statistical analysis
The Statistical Package for Social Sciences (SPSS) software, version 21 (SPSS Inc., Chicago, Illinois, USA), was used for data analysis. Continuous variables were reported as means±standard deviations and compared using the independent samples t-test based on normality tests. Median and interquartile range were used with nonparametric continuous variables, and the Kruskal-Wallis test was used for comparison between more than two groups. The frequencies and percentages of categorical variables were summarized and compared using chi-square or Fisher exact tests. The P-value was considered significant at < 0.05.
4Results
Table 1 shows the main characteristics of the 408 participants enrolled in this study. There were no statistically significant differences in age, sex, education, residence, weight, height, BMI, or SES between children with CHD and the healthy comparative group.
Table 1
Baseline characteristics among studied groups
| Items | Patients with congenital heart defects (n = 204) | Healthy group (n = 204) | P value |
| Age group | |||
| 5–10 | 106 (52.0%) | 100 (49.0%) | 0.5 |
| 11–18 | 98 (48.0%) | 104 (51.0%) | |
| Sex | |||
| Male | 111 (54.4%) | 99 (48.5%) | 0.2 |
| Female | 93 (45.6%) | 105 (51.5%) | |
| Weight/kg | 30.9±8.3 | 31.9±8.3 | 0.2 |
| Height/cm | 136.2±15.8 | 137.5±15.5 | 0.4 |
| Body Mass Index Z score | –0.06±0.9 | –0.06±1 | 0.2 |
| Level of education | |||
| Primary | 128 (62.7%) | 133 (65.2%) | 0.6 |
| Preparatory | 76 (37.3%) | 71 (34.8%) | |
| Residence | |||
| Urban | 151 (74.0%) | 154 (75.5%) | 0.7 |
| Rural | 53 (26.0%) | 50 (24.5%) | |
| Socioeconomic Status | |||
| Low | 109 (53.4) | 102 (50.0%) | 0.4 |
| Middle | 83 (40.7%) | 94 (46.1%) | |
| High | 12 (5.9%) | 8 (3.9%) |
The cardiac characteristics among the CHD group are illustrated in Table 2.
Table 2
Cardiac characteristics among patient group
| Items | Frequency (%) |
| Acyanotic congenital heart defects group | |
| ASD | 26 (12.7) |
| VSD | 33 (16.2) |
| PDA | 20 (9.8) |
| CoA | 14 (6.9) |
| Others | 40 (19.6) |
| Cyanotic congenital heart defects group | |
| F4 | 27 (13.2) |
| TGA | 18 (8.8) |
| DORV | 17 (8.3) |
| Others | 9 (4.4) |
| Age at diagnosis of heart disease | |
| First year of life | 100 (49.0) |
| 1–5 years | 54 (26.5) |
| >5 years | 50 (24.5) |
| History of previous cardiac surgery | |
| No | 64 (31.4) |
| One time | 85 (41.7) |
| Two times or more | 55 (27.0) |
| History of previous cardiac catheterization | |
| No | 107 (52.5) |
| One time | 57 (27.9) |
| Two times or more | 40 (19.6) |
| Frequency of hospital admission | |
| One time | 110 (53.9) |
| Two times | 76 (37.3) |
| Three times | 18 (8.8) |
ASD: Atrial Septal Defect, VSD: Ventricular Septal Defect, PDA: Patent Ductus Arterious, CoA: Coarctation of Aorta, F4: Fallot tetralogy, TGA: Transposition of Great Arteries, DORV: Double Outlet Right Ventricle.
Regarding psychiatric disorders among the studied children, mood disorders were more prevalent among children with CHD than healthy children (30.4% vs 11.3% respectively). Children with CHD were five times more likely to have anxiety disorders. Also, 18.6%, 18.1%, and 16.2% had social phobia, general anxiety disorder, and separation anxiety, respectively, and 9.3% of children with CHD reported panic attacks. The prevalence of attention-deficit/hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), tic disorders, and anorexia were 12.3%, 8.3%, 6.4%, and 3.9%, respectively, among children with CHD, compared to 5.4%, 2.0%, 1.0%, and 0.5% among the comparison group. There were statistically significant differences between the two groups (Table 3).
Table 3
Distribution of psychiatric disorders among studied groups
| Items | Patients with congenital heart defects (n = 204) | Healthy group (n = 204) | OR (CI 95%) |
| -Mood Disorders | 62 (30.4%) | 23 (11.3%) | 3.4 (2-5.8)* |
| Depression | 50 (24.5%) | 13 (6.4%) | 4.7 (2.5-9.1)* |
| Dysthymia | 21 (10.3%) | 9(4.4%) | 2.5 (1.1-5.6)* |
| Mania | 15 (7.4%) | 5 (2.5%) | 3.1 (1.1-8.9)* |
| -Anxiety disorders | 109 (53.4%) | 36 (17.6%) | 5.3 (3.4-8.4)* |
| Generalized anxiety disorder | 37 (18.1%) | 11 (5.4%) | 3.9 (1.9-7.8)* |
| Panic | 19 (9.3%) | 4 (2.0%) | 5.1 (1.7-15.3)* |
| Separation anxiety | 33 (16.2%) | 7 (3.4%) | 5.4 (2.3-12.5)* |
| Social phobia | 38 (18.6%) | 9 (4.4%) | 4.9 (2.3-10.5)* |
| Specific phobia | 23 (11.3%) | 11 (5.4%) | 2.2 (1.1-4.7)* |
| -Behavioral Disorders (Attention deficit hyperactivity disorder) | 25 (12.3%) | 11 (5.4%) | 2.4 (1.2-5.1)* |
| -Suicide | 18 (8.8%) | 0 (0.0%) | |
| -Obsessive compulsive disorder | 17 (8.3%) | 4 (2.0%) | 4.5 (1.5-13.7)* |
| -Tic disorder | 13 (6.4%) | 2 (1.0%) | 6.9 (1.5-30.7)* |
| -Eating Disorders (Anorexia) | 8 (3.9%) | 1 (0.5) | 8.3 (1.1-16.8)* |
OR: odds ratio, CI: confidence interval. *Confidence interval above 1 which means significant differences (P value < 0.05).
Table 4 shows higher prevalence of mood, behavioral, and anxiety (social phobia) disorders in the cyanotic group compared to acyanotic group. Also, the cyanotic group had a higher prevalence of anorexia than the acyanotic group.
Table 4
Distribution of psychiatric disorders among cyanotic and acyanotic patients
| Items | Cyanotic patients (n = 70) | Acyanotic patients (n = 134) | OR (CI 95%) |
| -Mood Disorders | 36 (51.4%) | 26 (19.4%) | 4.4 (2.3-8.3)* |
| Depression | 29 (41.4%) | 21 (15.7%) | 3.8 (1.9-7.4)* |
| Dysthymia | 12 (17.1%) | 9 (6.7%) | 2.9 (1.1-7.2)* |
| Mania | 13 (18.6%) | 2 (1.5%) | 15 (3.3-28.8)* |
| -Anxiety disorders | 44 (62.9%) | 65 (48.5%) | 1.8 (0.99-3.2) |
| Generalized anxiety disorder | 14 (20.0%) | 23 (17.2%) | 1.2 (0.6-2.5) |
| Panic | 5 (7.1%) | 14 (10.4%) | 0.6 (0.2-1.9) |
| Separation anxiety | 7 (10.0%) | 26 (19.4%) | 0.5 (0.2-1.1) |
| Social phobia | 24 (34.3%) | 14 (10.4%) | 4.4 (2.1-9.3)* |
| Specific phobia | 7 (10.0%) | 16 (11.9%) | 0.8 (0.3-2.1) |
| -Behavioral Disorders (Attention deficit hyperactivity disorder) | 4 (5.7%) | 21 (15.7%) | 0.3 (0.1-0.9)* |
| -Suicide | 10 (14.3%) | 8 (6.0%) | 2.6 (0.99-6.9) |
| -Obsessive compulsive disorder | 7 (10.0%) | 10 (7.5%) | 1.4 (0.5-3.8) |
| -Tic disorder | 4 (5.7%) | 9 (6.7%) | 0.8 (0.2-2.8) |
| -Eating Disorders (Anorexia) | 6 (8.6%) | 2 (1.5) | 6.2 (1.2-31.5)* |
OR: odds ratio, CI: confidence interval. *Confidence interval above 1 which means significant differences (P value < 0.05).
Table 5 illustrates the relationship between psychiatric disorders and sociodemographic and disease status. Mood disorders were more prevalent in females, adolescents in preparatory education, children who were diagnosed with cardiac disease after 5 years of life, those with recurrent hospital admission, and those who had frequent cardiac surgery or catheterization.
Table 5
Relationship between some psychiatric disorders and sociodemographic and disease status
| Mood Disorders | Anxiety disorders | Behavioral disorders | ||||
| Yes | No | Yes | No | Yes | No | |
| Age group | ||||||
| 5–10 | 16 (25.8)* | 90 (63.4) | 52 (47.7) | 54 (56.8) | 16 (64.0) | 90 (50.3) |
| 11–18 | 46 (74.2) | 52 (36.6) | 57 (52.3) | 41 (43.2) | 9 (36.0) | 89 (49.7) |
| Sex | ||||||
| Male | 22 (35.5)* | 89(62.7) | 52 (47.7)* | 59 (62.1) | 14 (56.0) | 97 (54.2) |
| Female | 40 (64.5) | 53 (37.3) | 57 (52.3) | 36 (37.9) | 11 (44.0) | 82 (45.8) |
| Level of education | ||||||
| Primary | 24 (38.7)* | 104 (73.2) | 64 (58.7) | 64 (67.4) | 20 (80.0) | 108 (60.3) |
| Preparatory | 38 (61.3) | 38 (26.8) | 45 (41.3) | 31 (32.6) | 5 (20.0) | 71 (39.7) |
| Residence | ||||||
| Urban | 16 (25.8) | 37 (26.1) | 77 (70.6) | 74 (77.9) | 17 (68.0) | 134 (74.9) |
| Rural | 46 (74.2) | 105 (73.9) | 32 (29.4) | 21 (22.1) | 8 (32.0) | 45 (25.1) |
| Socioeconomic Status | ||||||
| Low | 26 (41.9) | 83 (58.5) | 56 (51.4) | 53 (55.8) | 13 (52.0) | 96 (53.6) |
| Middle | 33 (53.2) | 50 (35.2) | 47 (43.1) | 36 (37.9) | 12 (48.0) | 71 (39.7) |
| High | 3 (4.8) | 9 96.3) | 6 (5.5) | 6 (6.3) | 0 (0.0) | 12 (6.7) |
| Age at diagnosis of heart disease | ||||||
| At 1st year of life | 25 (40.3)* | 75 (52.8) | 55 (50.5) | 45 (47.4) | 19 (76.0)* | 81 (45.3) |
| 1–5 years | 9 (14.5) | 45 (31.7) | 22 (20.2) | 32 (33.7) | 6 (24.0) | 48 (26.8) |
| >5 years | 28 (45.2) | 22 (15.5) | 32 (29.4) | 18 (18.9) | 0 (0.0) | 50 (27.9) |
| Hospital admission | ||||||
| Single admission | 14 (22.6)* | 96 (67.6) | 43 (39.4)* | 67 (70.5) | 17 (68.0) | 93 (52.0) |
| Multiple admissions | 48 (77.4) | 46 (32.4) | 66 (60.6) | 28 (29.5) | 8 (32.0) | 86 (48.0) |
| Cardiac surgery | ||||||
| No | 6 (9.7)* | 58 (40.8) | 32 (29.4)* | 32 (33.7) | 15 (60.0)* | 49 (27.4) |
| One time | 24 (38.7) | 61 (43.0) | 37 (33.9) | 48 (50.5) | 6 (24.0) | 79 (44.1) |
| Two times or more | 32 (51.6) | 23 (16.2) | 40 (36.7) | 15 (15.8) | 4 (16.0) | 51 (28.5) |
| History of catheterization | ||||||
| No | 19 (30.6)* | 88 (62.0) | 46 (42.2)* | 61 (64.2) | 14 (56.0) | 93 (52.0) |
| One time | 15 (24.2) | 42 (29.6) | 33 (30.3) | 24 (25.3) | 7 (28.0) | 50 (27.9) |
| Two times or more | 28 (45.2) | 12 (8.5) | 30 (27.5) | 10 (10.5) | 4 (16.0) | 36 (20.1) |
*Significant differences between groups (P value < 0.05).
Behavioral disorders were more prevalent among children who were diagnosed with cardiac disease in their first year of life and those who were not exposed to cardiac surgery.
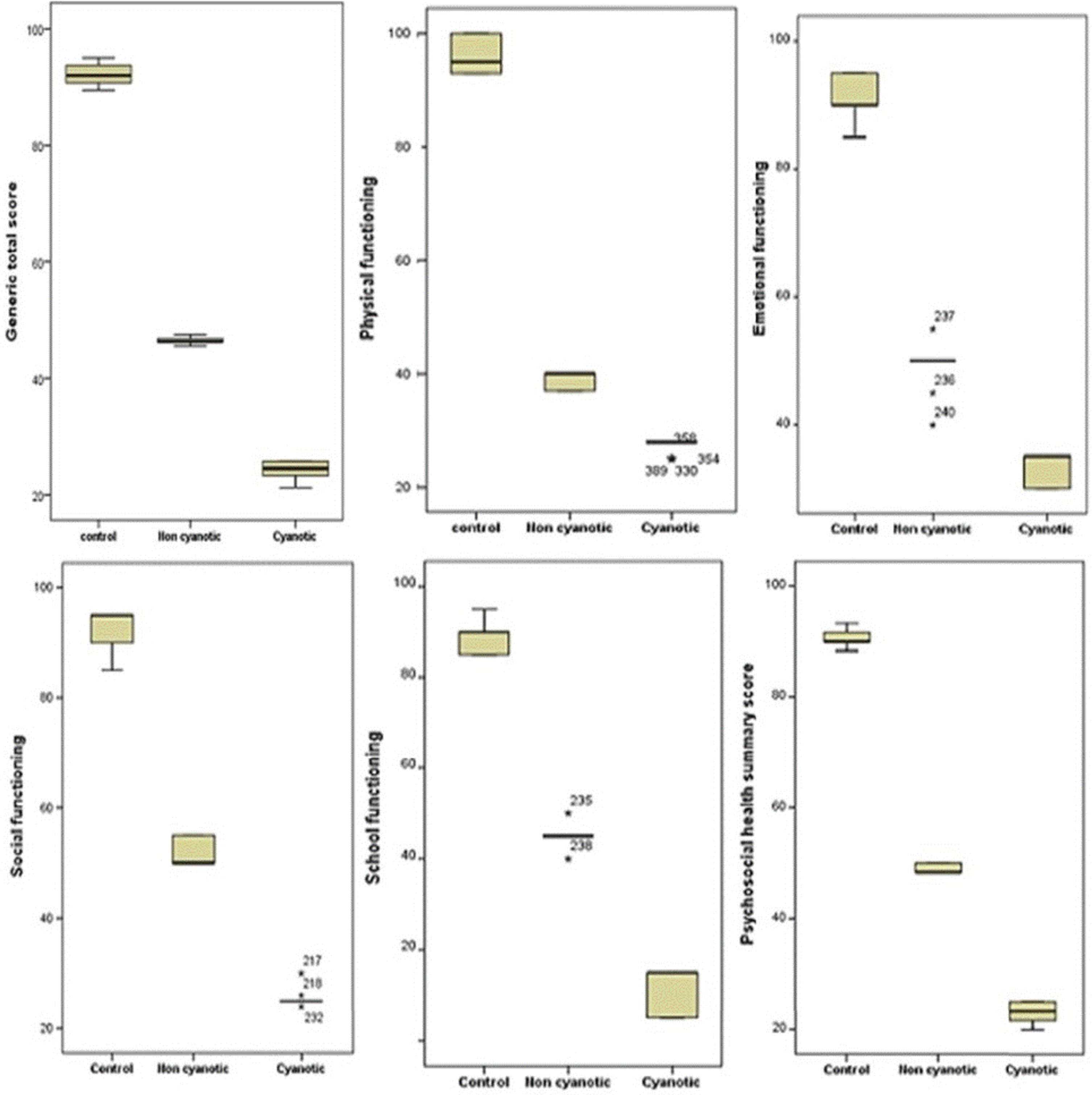
A more marked reduction of QoL occurred in cyanotic children than acyanotic children in comparison to the healthy comparative group (Table 6, Fig. 1).
Table 6
Pediatric Quality of Life Inventory 4.0 generic core scales among studied children
| Items | Healthy children | Acyanotic | Cyanotic | P value |
| (n = 204) | (n = 134) | (n = 70) | ||
| Generic total score | ||||
| Median (Q3-Q1) | 92 (93.75-90.75) | 46.25 (46.7-46.2) | 24.5 (25.7-23.2) | <0.01* |
| Physical functioning | ||||
| Median (Q3-Q1) | 95 (100-93) | 40 (40-37) | 28 (28-28) | <0.01* |
| Emotional functioning | ||||
| Median (Q3-Q1) | 90 (95-90) | 50 (50-50) | 35 (35-30) | <0.01* |
| Social functioning | ||||
| Median (Q3-Q1) | 95 (95-90) | 50 (55-50) | 25 (25-25) | <0.01* |
| School functioning | ||||
| Median (Q3-Q1) | 85 (90-85) | 45 (45-45) | 15 (15-5) | <0.01* |
| Psychosocial health summary | ||||
| Median (Q3-Q1) | 90 (91.7-90) | 48.3 (50-48.3) | 23.3 (25-21.7) | <0.01* |
*Significant differences between groups (P value < 0.05).
Fig. 1
Pediatric Quality of Life Inventory 4.0 generic core scales among studied children.
5Discussion
Children with chronic illnesses are more likely to exhibit emotional, behavioral, and psychiatric symptoms, which may be due to frequent hospitalization and physical limitations imposed by the illness itself [12].
In the present study, 24.5% of children with CHD met the diagnostic criteria for major depressive disorder. This finding is consistent with the findings reported by Gupta et al. [13]; in contrast, Awaad and Darahim [14] and Muller et al. [15] reported a lower prevalence among their studied groups (18.3% and 8.6%, respectively). Nousi et al. [16] has explained that the development of depression in children with CHD may be due to higher frequency of operations and the presence of postoperative scars that alter body image, as well as the delay in physical development. A higher prevalence of depression in the present study may be attributable to the timing of the study, which was done during the COVID-19 pandemic.
Preparatory education and recurrent hospital admission were considered risk factors for developing depressive symptoms in the studied children with CHD. Awaad and Darahim [14] found that children with low literacy and those with CHD who had symptoms were at higher risk for depression.
The present investigation of other mood disorders revealed that 10.3% of children with CHD had dysthymia and 7.4% had mania; this is supported by previous research [17, 18], which has indicated that adolescents with CHD are at an increased risk for psychological comorbidities.
The prevalence of suicidal thoughts was recorded in the studied children with CHD more often than in the healthy comparative group. This is in agreement with Ferro et al. [19], who reported that adolescents and young adults with chronic illness had more likelihood of suicidal thoughts and behaviors and suggested that chronic illness increases the risk for the development of psychiatric disorders, which thereby increases the risk for suicidal behavior.
The present work reported that 18.1% and 16.2% of the children with CHD had general and separation anxiety disorder, respectively; this was supported by Oliver et al., who found that 18.1% and 16.2% of children with CHD had general and separation anxiety disorders, respectively. An additional study by Oliver et al. [20] reported that children aged 7-16 years with CHD had significantly higher levels of health anxiety. Similarly, Fbgbrbşan et al. [21] reported that children with cyanotic CHD between the ages of six and 10 were 13.5 times more likely to exhibit anxious behavior than the healthy control group.
Female gender and an increase in the frequency of admission were considered risk factors for anxiety disorders. Similarly, Areias et al. [22] found that female gender and complex forms of CHD were associated with higher levels of anxiety and depression in hospitalized patients. This result may be due to the fact that females are more emotionally sensitive and exhibit more internalizing disorders, such as depression and anxiety, than boys [23]. In contrast, boys tend to conceal their mental health issues and have a higher prevalence of externalizing disorders, such as antisocial personality disorder and dependence [23].
The increased prevalence of anxiety, panic disorders, and social and specific phobias in children with congenital heart disease could be explained by the fact that they had fewer opportunities to develop appropriate social skills due to higher rates of medically-related school absences [24].
In the present study, 8.3% of the studied children with CHD had OCD and repeated hospitalization was associated with increased risk for the development of OCD. This result is supported by the findings of Geyer et al. [25], who found that patients with coronary heart disease had significantly different obsessive-compulsive thoughts than healthy controls. In addition, it was observed that females with CHD were at a higher risk for OCD than males, which may be explained by the hypothesized role of ovarian hormones in the pathogenesis of OCD, placing females at a higher risk during and after menarche [26].
The studied children with CHD presented with more tic disorders than healthy controls. This may be explained by comorbid symptoms of anxiety, OCD, and depression; tic disorders are frequently comorbid with other psychiatric symptoms, such as ADHD, OCD, depression, and anxiety disorders [27].
Increased risk of ADHD was noticed in the children with CHD (12.3% compared to 7.4% of the healthy controls). This is consistent with Fbgbrbşan et al. [21] and Gonzalez et al. [5], who found that 11.6% and 5.1%, respectively, of their studied children with CHD had ADHD. Moreover, Yamada et al. [28] reported that the prevalence of ADHD was 29% among children aged 7-15 years undergoing any open-heart surgery.
The cause of behavioral disorders in children with CHD is still unclear; Rollins et al. [29] suggested that ADHD-related behavior in children with CHD may be due to altered brain white matter microstructure caused by a prolonged type of hypoxia and cyanosis.
In the present work, the cyanotic group had a higher frequency of mood disorders, anxiety disorders, social phobia, ADHD, and anorexia compared to the acyanotic group. This finding aligns with Cohen et al. [30], who reported that adolescents with severe/cyanotic heart disease exhibited higher levels of depression and lower self-esteem than adolescents with moderate to mild heart disease and age-matched healthy controls. Previous studies have also concluded that children with complex CHD who underwent surgery had worse psychosocial adjustment [31, 32].
Psychiatric disorders in the cyanotic group may be explained by early physiological risk factors, such as brain immaturity in utero, perioperative hemodynamic changes, and systemic inflammation. These events may negatively impact neurobiological development, changing how children respond to stressors in the long run and raising the likelihood of psychiatric morbidities [33, 34].
In the present work, all scores of QoL dimensions, including physical, emotional, social, and school functioning, were reduced in children with CHD compared to controls. This finding concurs with previous reports that have studied the quality of life in children with CHD [35, 36]. In contrast, Sertçelik et al. [37] found that school and family sub-dimensions of total QoL scores were unaffected in children with CHD. This discrepancy may be due to differences in the environment of the studied sample.
Reduction in total QoL score was observed more often in the cyanotic group. Sertçelik et al. [36] and Tahirovic et al. [37] have also reported that QoL perception was poorer in children with cyanotic CHD compared with acyanotic groups.
6Conclusion and recommendation
Children with CHD have an increased risk of various psychiatric disorders and an overall reduction of QoL. Regular psychiatric follow-up and cooperation between pediatric cardiology and psychiatric physicians is essential for early intervention. Programs are needed to enhance exercise function and capacity, support the self-confidence of patients and their families to take part in age-appropriate activities, encourage proper nutrition, and provide education that fulfills the needs of those children even with recurrent school absence.
7Limitations of the study
The significant limitation of this study was that it was conducted during the COVID-19 pandemic, which may have increased the prevalence of psychological disorders in the studied children. Also, a relatively small cohort was used; further research with a large number of participants is needed.
8Strengths of the study
The study was done in a low-income country (Egypt) and included multiple psychiatric disorders in addition to the QoL assessment among children who had not previously complained of this problem. Also, the cyanotic group was included in the comparison, which has not been previously studied.
Acknowledgments
The authors are grateful to the patients and families who participated in this work.
Conflict of interest
The authors have no conflicts of interest to declare.
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical approval
Written informed consent was completed by each participant’s parents. The study protocol was approved by Al-Azhar University local Ethics Committee, Faculty of Medicine for Girls. The council number is 202101012 and all procedures were in accordance with the Helsinki Delcaration.
Funds and grants
None received.
References
[1] | Liu Y , Chen S , Zühlke L , et al. Global birth prevalence of congenital heart defects 1970-2017: updated systematic review and meta-analysis of 260 studies. Int J Epidemiol. (2019) ;48: (2):455–463. doi: 10.1093/ije/dyz009 |
[2] | Stout KK , Daniels CJ , Aboulhosn JA , et al. AHA/ACC guideline for the management of adults with congenital heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation. (2019) ;139: (14):e831–e832. doi: 10.1161/CIR.0000000000000603 |
[3] | DeMaso DR , Calderon J , Taylor GA , et al. Psychiatric Disorders in Adolescents With Single Ventricle Congenital Heart Disease. Pediatrics. (2017) ;139: (3):e20162241.. doi: 10.1542/peds.2016-2241 |
[4] | Knowles RL , Day T , Wade A , et al. Patient-reported quality of life outcomes for children with serious congenital heart defects. Arch Dis Child. (2014) ;99: (5):413–419. doi: 10.1136/archdischild-2013-305130 |
[5] | Gonzalez VJ , Kimbro RI , Cutitta KE , et al. Mental Health Disorders in Children with Congenital Heart Disease. Pediatrics. (2021) ;147: (2):e20201693.. doi: 10.1542/peds.2020-1693 |
[6] | Fahmy SI , El Sherbini AF . Determining Simple Parameters for Social Classification for Health Research. Bulletin of the High Institute of Public Health. (1983) ;8: , 95–107. |
[7] | Sheehan DV , Lecrubier Y , Sheehan KH , et al. The Mini-International Neuropsychiatric Interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) ;59: (Suppl 20):22–33;quiz 34-57. |
[8] | Ghanem MH , Ibrahim M , El Behairy AA , El Merghany H . Mini International Neuropsychiatric Interview for children/ adolescents (MINI Kid): Arabic version. 1st ed. Cairo: Department of Neuopsychiatry, Faculty of Medicine, Ain Shams University; 1999. |
[9] | Sheehan DV , Sheehan KH , Shytle RD , et al. Reliability and validity of the mini international neuropsychiatric interview for children and adolescents (MINI-KID). J Clin Psychiatry. (2010) ;71: (3):313–26. doi: 10.4088/JCP.09m05305whi |
[10] | Abdul-Rasoul M , AlOtaibi F , AlMahdi M , AlKandari H . Reliability and validity of the Arabic version of the PedsQL TM 40 generic ore scales and PedsQL TM 3.0 diabetes module. Journal of Diabetes Mellitus. (2012) ;2: (3):301–307. doi: 10.4236/jdm.2012.23047 |
[11] | Varni JW , Seid M , Kurtin PS . Peds QLTM 4.0: reliability and validity of the pediatric quality of life inventory version 4.0 generic core scales in healthy and patient populations.. Med Care. (2001) ;39: (8):800–12. doi: 10.1097/00005650-200108000-00006 |
[12] | Werninger I , Ehrler M , Wehrle FM , et al. Social and Behavioral Difficulties in 10-Year-Old Children With Congenital Heart Disease: Prevalence and Risk Factors. Front Pediatr. (2020) ;8: :604918. doi: 10.3389/fped.2020.604918 |
[13] | Gupta S , Giuffre RM , Crawford S , Waters J . Covert fears, anxiety and depression in congenital heart disease. Cardiol Young. (1998) ;8: (4):491–499. doi: 10.1017/S1047951100007162 |
[14] | Awaad MI , Darahim KE . Depression and anxiety in adolescents with congenital heart disease. European Psychiatry. (2015) ;30: (Suppl 1):610. doi: 10.1016/S0924-9338(15)31916-7 |
[15] | Muller J , Hess J , Hager A . Minor symptoms of depression in patients with congenital heart diseases have a larger impact on quality of life than limited exercise capacity. Int J Cardiol. (2012) ;154: (3):265–269. doi: 10.1016/j.ijcard.2010.09.029 |
[16] | Nousi D , Christou A . Factors affecting the quality of life in children with congenital heart disease. Health Science Journal. (2010) ;4: (2), 94–100. |
[17] | Udholm S , Nyboe C , Dantoft TM , Jørgensen T , Rask CU , Hjortdal VE . Small atrial septal defects are associated with psychiatric diagnoses, emotional distress, and lower educational levels. Congenit Heart Dis. (2019) ;14: (5):803–810. doi: 10.1111/chd.12808 |
[18] | Morel P , Santacroce SJ . Illness uncertainty and posttraumatic stress in young adults with congenital heart disease. J Cardiovasc Nurs. (2018) ;33: (4):356–362. doi: 10.1097/JCN.0000000000000471 |
[19] | Ferro MA , Rhodes AE , Kimber M , et al. Suicidal Behaviour Among Adolescents and Young Adults with Self-Reported Chronic Illness. Can J Psychiatry. (2017) ;62: (12):845–853. doi: 10.1177/0706743717727242 |
[20] | Oliver AM , Wright KD , Kakadekar A , et al. Health anxiety and associated constructs in children and adolescents with congenital heart disease: A CHAMPS cohort study. J Health Psychol. (2020) ;25: (10-11):1355–1365. doi: 10.1177/1359105318755263 |
[21] | Fbgbrbşan A , Al-Akel F , Cerghit-Paler A , et al. Psychological Distress in Children with Surgically CorrectedCongenital Heart Disease. Pediatr Perinatol Child Health. (2020) ;4: (2):42–51. doi: 10.26502/jppch.74050040 |
[22] | Areias MEG , Pinto CI , Vieira PF , et al. Long term psychosocial outcomes of congenital heart disease (CHD) in adolescents and young adults. Transl Pediatr. (2013) ;2: (3):90–98. doi: 10.3978/j.issn.2224-4336.2013.06.02 |
[23] | Van Droogenbroeck F , Spruyt B , Keppens G . Gender differences in mental health problems among adolescents and the role of social support: results from the Belgian health interview surveys 2008 and 2013. BMC Psychiatry. (2018) ;18: (1):6. doi: 10.1186/s12888-018-1591-4 |
[24] | Emerson ND , Distelberg B , Morrell HER , Williams-Reade J , Tapanes D , Montgomery S . Quality of Life and School Absenteeism in Children With Chronic Illnes. J Sch Nurs. (2016) ;32: (4):258–266. doi: 10.1177/1059840515615401 |
[25] | Geyer S , Hessel A , Kempa A , et al. [Psychological symptoms and body image in patients after surgery of congenital heart disease]. Psychother Psychosom Med Psychol. (2006) ;56: (11):425–31. doi: 10.1055/s-2006-951809 |
[26] | Mathes BM , Morabito DM , Schmidt NP . Epidemiological and Clinical Gender Differences in OCD. Curr Psychiatry Rep. (2019) ;21: (5):36. doi: 10.1007/s11920-019-1015-2 |
[27] | Ueda K , Black KJ . A Comprehensive Review of Tic Disorders in Children. J Clin Med. (2021) ;10: (11):2479. doi: 10.3390/jcm10112479 |
[28] | Yamada DC , Porter AA , Conway JL , et al. Early repair of congenital heart disease associated with increased rate of attention deficit hyperactivity disorder symptoms. Can J Cardiol. (2013) ;29: (12):1623–1628. doi: 10.1016/j.cjca.2013.07.007 |
[29] | Rollins CK , Watson CG , Asaro LA , et al. White matter microstructure and cognition in adolescents with congenital heart disease. J Pediatr. (2014) ;165: (5):936–44. doi: 10.1016/j.jpeds.2014.07.028 |
[30] | Cohen M , Mansoor D , Langut H , Lorber A . Quality of life, depressed mood, and self-esteem in adolescents with heart disease. Psychosoma Med. (2007) ;69: (4):313–8. doi: 10.1097/PSY.0b013e318051542c |
[31] | Hülser K , Dubowy K-O , Knobl H , Meyer H , Schölmerich . Developmental outcome and psychosocial adjustment in children after surgery for congenital heart disease during infancy. Journal of Reproductive and Infant Psychology. (2007) ;25: (2):139–51. doi: 10.1080/02646830701292308 |
[32] | Spijkerboer AW , Utens EMWJ , De Koning WB , Bogers AJJC , Helbing WA , Verhulst FC . Health-related Quality of Life in children and adolescents after invasive treatment for congenital heart disease. Qual Life Res. (2006) ;15: (4):663–73. doi: 10.1007/s11136-005-3692-z |
[33] | Licht DJ , Shera DM , Clancy RR , et al. Brain maturation is delayed in infants with complex congenital heart defects. Journal Thorac Cardiovasc Surg. (2009) ;137: (3):529–536. doi: 10.1016/j.jtcvs.2008.10.025 |
[34] | Mahle WT , Matthews E , Kanter KR , et al. Inflammatory response after neonatal cardiac surgery and its relationship to clinical outcomes. Ann Thorac Surg. (2014) ;97: (3):950–956. doi: 10.1016/j.athoracsur.2013.10.069 |
[35] | Mahmoud SE , Ismail SS , Hassan SE . Quality of life among Children with Congenital Heart Diseases. Egyptian Journal of Health Care. (2020) ;11: (2):85–97. doi: 10.21608/ejhc.2020.88541 |
[36] | Sertçcelik T , Alkan F , Sapmaz SY , et al. Life quality of childrenwith congenital heart diseases. Turk Pediatri Arsivi. (2018) ;53: (2):78–86. doi: 10.5152/2018.6428 |
[37] | Tahirović E , Begić H , Nurkić M , Tahirović H , Varni JW . Does the severity of congenital heart defects affectdisease-specific health-related quality of life in children inBosnia and Herzegovina? Eur J Pediatr. (2010) ;169: (3):349–53. doi: 10.1007/s00431-009-1060-7 |


