
The Role of Diet in Parkinson’s Disease
Abstract
The aim of this review is to examine the intersection of Parkinson’s disease (PD) with nutrition, to identify best nutritional practices based on current evidence, and to identify gaps in the evidence and suggest future directions. Epidemiological work has linked various dietary patterns and food groups to changes in PD risk; however, fewer studies have evaluated the role of various diets, dietary components, and supplements in the management of established PD. There is substantial interest in exploring the role of diet-related interventions in both symptomatic management and potential disease modification. In this paper, we evaluate the utility of several dietary patterns, including the Mediterranean (MeDi), Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), Alternative Healthy Eating Index (AHEI), vegan/vegetarian, and ketogenic diet in persons with PD. Additionally, we provide an overview of the evidence relating several individual food groups and nutritional supplements to PD risk, symptoms and progression.
INTRODUCTION
Parkinson’s disease (PD) is the second most prevalent neurodegenerative disorder worldwide [1]. The pathogenesis of PD is thought to involve a confluence of intestinal dysbiosis, inflammation, oxidative stress, mitochondrial dysfunction, alpha-synuclein aggregation, and nigrostriatal dopaminergic neuron loss [2]. PD’s cardinal motor features— bradykinesia, rigidity, tremor and postural instability— and non-motor features can interfere with food intake and dietary composition [3]. Motor symptoms can make shopping for, preparing and eating meals, especially in social settings, challenging [3]. Deterioration of smell and taste sensation, depression, apathy, cognitive decline, changes in reward processing, and impulse control disorders can alter appetite and food preferences (e.g., increasing cravings for sweets) [3, 4]. Dysphagia, nausea, delayed gastric emptying, small intestine bacterial overgrowth, and constipation can cause early satiety and impaired levodopa absorption, as can protein-containing foods [3, 5–7]. A recent meta-analysis (n = 5,613) identified a third of persons with PD (PwP) as being at risk of malnutrition [7], which is a risk factor for worse quality of life and health outcomes [3, 8, 9].
Observational studies have linked dietary patterns and individual food groups to PD risk, age of onset, progression, symptom severity, and mortality rates [10–18], yet there is a paucity of randomized controlled trials (RCTs) into nutritional interventions. Nutritional interventions can interact with multiple disease mechanisms simultaneously, offering the potential for disease-modification, while nutritional self-management presents an opportunity for empowerment in PwP. In this paper, we summarize the current evidence on dietary and nutritional supplement strategies in PD and suggest future directions for research.
DIETARY PATTERNS
Mediterranean diets
There is a wide range of Mediterranean (MeDi) diets, overall characterized by a predominantly plant-based diet rich in vegetables, fruits, whole grains, legumes, unsaturated fatty acids (mostly olive oil), nuts/seeds and fish/seafood, with moderate intake of poultry, and wine and low intake of red and processed meat, sweets, sugar-sweetened beverages, refined grains and saturated fatty acids [19]. Between 2020–2023 alone, several observational studies reported inverse associations between MeDi diet adherence and PD risk, age of onset and prodromal PD symptoms [20]. A single-center, cross-sectional Canadian study of 167 participants with PD found a correlation between MeDi diet scores and later disease onset, of up to 8.4 years in men, specifically (p = 0.002) [18]. A US 20-year prospective analysis involving 47,669 individuals [21] reported an inverse association between long-term MeDi diet adherence and prodromal PD features (odds ratio (OR) for 3 + versus 0 features = 0.82 (95% confidence interval (CI): 0.68–1.00)), as did a 3-year study of 1,047 adults in Greece (60–70% lower risk in highest versus lowest quartile for MeDi adherence) [22]. A 30-year study of > 47,000 Swedish women identified a reduced risk of PD among individuals with high versus low adherence to MeDi diets in middle age (hazard ratio (HR) = 0.54 (95% CI: 0.30–0.98)) [14], while the longitudinal Dutch Rotterdam Study of 9,414 adults found a similar potential, although non-significant, association (HR = 0.89 (95% CI: 0.74–1.07)) [13]. The presumed protective properties of MeDi diets against PD may stem from the anti-inflammatory and antioxidant properties of polyphenol phytochemicals and vitamins found in fruits and vegetables, neuroprotective effects of omega-3s found in fish, and/or beneficial effects of high-fiber diets on the gut microbiome [20, 23]. Japanese dietary patterns enriched in vegetables, fruits and fish were similarly associated with reduced PD risk in a case-control study of 249 PwP and 368 controls without neurodegenerative disease [24].
Despite compelling epidemiologic evidence for benefits of MeDi diets in PD, RCTs have been limited. A single-center RCT from Iran involving 80 patients with idiopathic PD reported a modest increase in Montreal Cognitive Assessment and a decrease in Parts I, II and IV Unified Parkinson’s Disease Rating Scale (UPDRS) scores in response to a 10-week Mediterranean diet intervention [11, 12]. In a pilot single-arm study of eight PwP, a 5-week MeDi diet intervention reduced constipation, in association with changes in gut microbiome composition [25].
MIND diet
The MIND diet combines principles from the MeDi and Dietary Approaches to Stop Hypertension diet, originally developed to reduce cognitive decline [26]. The MIND encourages leafy greens, bean and berry consumption and discourages cheese, butter and margarine intake [27]. A longitudinal study of 706 aging American adults found that MIND diet adherence was associated with reduced incidence and slower progression of parkinsonism relative to MeDi diet adherence [28], while a Canadian cross-sectional study found that MIND diet adherence was associated with a higher age at PD onset of up to 17.4 years (p < 0.001) specifically in females [18]. A recent analysis of the Modifiable Variables in Parkinsonism Study identified an approximately two-fold decrease in severity of patient-reported symptoms associated with MIND relative to MeDi diet adherence [27]. However, the effect of the MIND diet on PD symptoms, progression and PD-associated cognitive decline has yet to be evaluated in an interventional study.
Vegetarian and vegan diets
Limited prior epidemiological studies have suggested lower rates of PD in societies mostly following vegetarian and vegan diets [29–31]. A recent UK biobank analysis found an association between a healthful plant-based diet and reduced PD risk (HR = 0.78 (95% CI: 0.61–0.99)), whereas an unhealthy plant-based diet was associated with a higher risk to develop PD (HR = 1.38 (95% CI: 1.08-1.74)) [32]. One recent trial of a 14-day ovo-lacto vegetarian diet in 16 patients with PD demonstrated significant improvements in UPDRS Part III scores [33].
Diet quality as measured by the Alternative Healthy Eating Index
The Alternative Healthy Eating Index (AHEI) is a measure of diet quality adapted from the Healthy Eating Index, which scores foods based on their association with chronic disease risk [34]. A recent analysis of the prospective Nurses’ Health Study and the Health Professionals Follow-Up Study data reported a reduced risk of prodromal PD features over two decades among individuals with higher AHEI scores [21]. In the same cohort, over the 32–34 years of follow-up, 1,251 participants developed PD, of which 942 died. Higher scores on the AHEI were associated with lower rates of all-cause and PD-specific mortality (adjusted HR, highest versus lowest AHEI quartile = 0.69 (95% CI: 0.56–0.85) for prediagnosis scores and 0.57 (95% CI: 0.42–0.78) for postdiagnosis scores) [16]. The association between AHEI scores and mortality was driven primarily by higher intake of whole grains, nuts and legumes, and lower intake of red and processed meats [16]. Additionally, the association was partially explained by higher total flavonoid intake, which was independently linked to reduced mortality in PwP [35].
Ketogenic diet
The KD is a high-fat, low-carbohydrate diet, which, among other mechanisms [36], may circumvent bioenergetic deficits in PD where affected neurons are unable to efficiently utilize glucose for energy production but likely continue to be able to use ketone bodies such as body beta-hydroxybutyrate, generated in response to a high-fat, low-carbohydrate diet [37]. Ketone bodies may enable neurons to feed electrons into the mitochondrial respiratory chain at complex II, bypassing PD-related deficiencies in complex I metabolism [38]. Four recent RCTs have investigated the feasibility, safety and short-term efficacy of KDs in PD [36]. In an 8-week pilot study comparing a KD to a low-fat diet in 38 participants with PD, both groups showed improvement on all four parts of the UPDRS, with the KD group showing greater improvement in Part I scores [39]. However, worsening tremor and/or rigidity was noted in the KD group 1–4 weeks into the diet intervention, leading to two participant withdrawals. In an open-label, non-controlled pilot study of 16 PD participants on a 12-week KD intervention, significant improvements were seen in UPDRS Part I and total Parkinson Anxiety Scale scores [40]. An 8-week study comparing a ketogenic (n = 7) versus high-carbohydrate (n = 7) diet in individuals with PD and mild cognitive impairment reported improvements in lexical access and memory in the ketogenic diet arm [10]. Another study of 68 participants with PD reported improvements in voice quality following three months of a ketogenic diet [41].
Protein-redistribution diets
The timing of macronutrient intake in PD can have important implications for levodopa transport and effectiveness [42]. Ten trials of protein-redistribution diets have been conducted to date [6], which typically involve limiting protein to 0–10 g at breakfast and lunch, with remaining protein intake to occur at dinner. Taken together, these studies reported 32–79% reductions in motor symptoms, 30–107 minute reductions in postprandial motor fluctuations, and reductions in disability scores in PwP on protein-redistribution diets [6, 42]. However, concerns around potential loss of weight and lean body mass on protein-redistribution diets remain [6].
FOOD GROUPS
Dairy
Early prospective studies suggested that high consumption of dairy may increase the risk of PD [43–46]. A prospective analysis of the Nurses’ Health Study (n = 80,736) and the Health Professionals Follow-up Study (n = 48,610) found that this association held only for low-fat dairy foods [17], while in the Rotterdam study, higher intake of yoghurt, fermented milk and butter, respectively, but not milk or cream intake, was associated with higher PD risk [13]. Higher consumption of ice cream, yoghurt and cheese has been associated with faster PD progression [47]. A proposed explanation for the association of PD risk with milk intake relates to the anti-uricemic effect of casein and lactalbumin found in milk, as urate’s antioxidant properties are believed to protect against PD development [48]. Anti-uricemic effects may be mitigated by saturated fats in high-fat dairy products [17]. Alternatively, some have proposed that pesticide contaminants in dairy products may contribute to PD-associated neurodegeneration [17, 49]. Overall, the association of PD risk with specific dairy products is inconclusive.
Alcohol
Evidence regarding the relationship between alcohol intake and PD risk has been mixed. A prospective study of a cohort including 694 incident PD cases found no association between alcohol consumption and PD development overall, though men reporting moderate (5–29.9 g/day) alcohol consumption were at approximately 50% higher risk for PD than those reporting light (0.1–4.9 g/day) consumption (HR = 1.58 (95% CI: 1.07–2.33) for 5–14.9 g/day and HR = 1.52 (95% CI: 1.00–2.33) for 15–29.9 g/day) [50]. However, a linear exposure-response trend was missing [50]. A recent systematic review of 11 prospective studies found a U-shaped association between alcohol intake and PD risk [51], with an overall relative risk for PD comparing any versus no alcohol intake of 0.81 (95% CI: 0.65–0.95). A meta-analysis of 52 observational studies found a negative, dose-dependent association between alcohol intake and PD risk (OR of ever drinking alcohol versus never drinking among PwP = 0.84 (95% CI 0.76–0.92)) [52] However, the authors note that the relationship between alcohol and PD may be confounded by smoking status in many of the studies included in their meta-analysis, and that results may similarly be influenced by survivor, selection and recall bias [52]. Others have suggested that moderate alcohol consumption may be associated with personality features characteristic of a more risk-taking personality, which itself is associated with reduced PD risk [53]. Alternatively, alcohol-mediated increases in levels of plasma antioxidants, such as folic acid, niacin, purine and urate, may help to explain an inverse relationship between alcohol consumption and PD up to a certain threshold [51, 53].
Caffeine
Observational studies have suggested protective effects of caffeinated coffee and tea against PD risk and progression, but benefits of caffeine alone have not borne out in clinical trials involving PwP. In a 2020 meta-analysis, coffee and caffeine were associated with a reduced risk of PD onset among healthy individuals and reduced rates of PD progression among PwP [54]. Regular caffeine intake was also associated with later PD age of onset [55]. Higher plasma caffeine concentrations were linked to PD resistance among pathogenic LRRK2 gene mutation carriers in a metabolomic study [15]. The putative protective effect of caffeine may be mediated by alterations in alpha-synuclein breakdown or gut microbiome composition, or by direct neuroprotective antagonism of adenosine A2A receptors in the brain [56]. However, a RCT in participants with established PD comparing supplementation of caffeine pills (200 mg twice daily, n = 60) to placebo pills (n = 61) was terminated early due to a lack of clinical improvement in parkinsonian symptoms [57]. Additionally, authors noted a slight increase in dyskinesia and decrease in cognitive testing scores [57]. These results could be due to the isolation of caffeine, suggesting other non-caffeine components of coffee and tea may be protective against PD.
PD-specific foods based on patient-reported outcomes
Mischley et al. (2017) investigated effects of various dietary components on Parkinson’s disease progression in a web-based observational cross-sectional study of 1,053 PwP using patient-reported outcomes (PROs) as the primary outcome measure [47]. This study found that fresh vegetables, fresh fruit, nuts and seeds, non-fried fish, olive oil, wine, coconut oil, fresh herbs, and spices were associated with slower rates of PD progression, while canned fruits and vegetables, diet and non-diet soda, fried foods, beef, ice cream, yoghurt, and cheese were associated with faster rates of PD progression.
NUTRITIONAL SUPPLEMENTS
Vitamin D
Several studies have noted high rates of vitamin D deficiency in PD, associated with disease risk, motor severity, cognitive impairment and increased fall risk [58–62]. Vitamin D receptors and vitamin D synthesis enzymes are highly expressed in the substantia nigra, suggesting an important role of vitamin D in the proper functioning of these neurons [63]. A review of the four completed trials of vitamin D supplementation in PD concluded that vitamin D supplementation had no significant effect on PD severity, dyskinesia, activities of daily living or balance [62]. Of note, most studies supplemented vitamin D regardless of baseline vitamin D levels. Furthermore, this finding does not preclude potential genotype-specific benefits of vitamin D supplementation. Suzuki et al. (2013) found that 30 weeks of vitamin D3 supplementation (1200 IU/day) mitigated increases in Hoehn and Yahr stage over a 12-month follow-up period, specifically in PwP with vitamin D receptor FokI genotypes TT and CT [64]. Osteoporosis is more common in PD than age-matched healthy controls while PwP are also at increased risk of falls and fractures with significant implications for morbidity and mortality. Optimized vitamin D and calcium intake are an important part of the management of osteoporosis in PD [65].
Vitamin E and omega-3 fatty acids
Due to their antioxidant and anti-inflammatory properties, vitamin E and omega-3 fatty acid co-supplements have been suggested as potentially beneficial in PD [66]. A 12-week RCT compared supplementation with 1,000 mg omega-3 fatty acid from flaxseed oil and 400 IU vitamin E versus placebo in PD patients [67]. The intervention improved total UPDRS scores, decreased serum high sensitivity C-reactive protein (a marker of systemic inflammation) and increased total antioxidant capacity. A 30-week placebo controlled RCT (n = 40) in PD investigating a formula composed of omega-3 fatty acids, vitamin A, vitamin E and gamma-tocopherol reported significant reductions in UPDRS Part III scores in the treatment group at the 12-month follow-up [68]. Fish oil supplementation was associated with reduced rates of PD progression in Mischley et al.’s observational study (2017) [47].
Vitamins B6, B9, and B12
Homocysteine is an alpha-amino acid intermediary product of methionine metabolism, whose role in PD was recently reviewed [69]. In brief, hyperhomocysteinemia is a common finding in PD, driven by catechol-O-methyltransferase-mediated levodopa metabolism [69]. Hyperhomocysteinemia has been associated with increased risk of cardiovascular [70], and cerebrovascular disease [71], cognitive impairment [72], and cortical structural damage [73]. Vitamins B6, B12, and B9 (folate) are cofactors in downstream pathways responsible for the metabolism of homocysteine, which can become depleted in the context of increased homocysteine generation via levodopa metabolism [69, 72]. Supplementation with vitamins B6 (< 25 mg daily), B12 and folate has been suggested for the prevention and treatment of hyperhomocysteinemia in PD although dedicated RCTs are lacking [69, 74]. Of note, in cases of PD with renal insufficiency, the standard cyanocobalamin B12 supplement should be substituted for methylcobalamin (500–100 ug per day) [69].
Vitamin B1
The role of vitamin B1 (thiamine) supplementation in PD remains relatively unexplored, although a recent study has suggested an association between thiamine deficiency and mild cognitive impairment in PD [75].
Vitamin C
There is no association between vitamin C intake and PD risk on meta-analysis [76]. However, vitamin C enhances levodopa absorption, and may confer benefit in elderly individuals with PD in whom drug bioavailability is often limited [77].
Citicoline
Citicoline (cytidine-diphosphocholine (CDP-Cho)) is an endogenous compound involved in the biosynthesis of acetylcholine, whose neuroprotective properties have been suggested by several animal and human studies [78]. A systematic review of 355 patients across seven heterogenous, small and mostly older studies found that citicoline supplementation was associated with motor and cognitive improvements in PD, facilitating a reduction in levodopa dose by up to 50% [78].
Fiber, prebiotics, and probiotics
Emerging evidence for a role of gut dysbiosis in PD has led to increasing interest in microbial-based therapies, such as probiotics. A 2023 meta-analysis of 11 RCTs reported high quality evidence for a beneficial effect of probiotics on UPDRS Part III, Non-Motor Symptoms Questionnaire, and two depression scale scores [79]. Although significant improvement in gastrointestinal motility was shown in the probiotic group compared to the placebo group, constipation symptoms and Bristol Stool Scale scores did not differ between the two groups in this meta-analysis [79]. However, two RCTs to date have provided Class I evidence in support of the use of multi-strain probiotics to treat constipation in PwP [80, 81]. In [81], the multi-strain probiotic was combined with prebiotic fiber in a fermented milk preparation. Beyond symptomatic benefits, dietary fiber may alleviate the PD-associated decrease in butyrate-synthesizing bacteria in the gut, which is thought, among other mechanisms, to reduce inflammation [82]. Two recent studies demonstrated that dietary fiber could increase butyrate production in PD participants’ stools in vitro [82, 83].
Mucuna pruriens
Mucuna pruriens is a levodopa-containing leguminous plant which grows in tropical climates, and may be considered as an alternative therapy to synthetic levodopa/carbidopa in low-resource settings [84]. A double-blind crossover study by [85] in eight patients with PD reported a faster onset of effect and longer “on” time duration with Mucuna pruriens preparation versus a standard 200/50 mg levodopa/carbidopa preparations. A double-blind, randomized, controlled crossover study with 18 PD patients, [86] found that single-dose Mucuna pruriens produced a similar motor response with a noninferior safety profile to levodopa/benserazide. A second double-blind, randomized, controlled crossover study from the same group in 14 patients with PD motor fluctuations and dyskinesias corroborated the findings of similar symptomatic control between daily Mucuna pruriens and levodopa/carbidopa over 16 weeks [87]. However, the high rate of gastrointestinal side effects and shortening “on” time in the Mucuna pruriens arm of this trial led to a 50% dropout rate [87]. Authors recommend that patients appropriately managed on synthetic levodopa/carbidopa in high-resource settings be advised against self-medicating with Mucuna pruriens due to the poor tolerability profile.
DISCUSSION AND FUTURE PERSPECTIVES
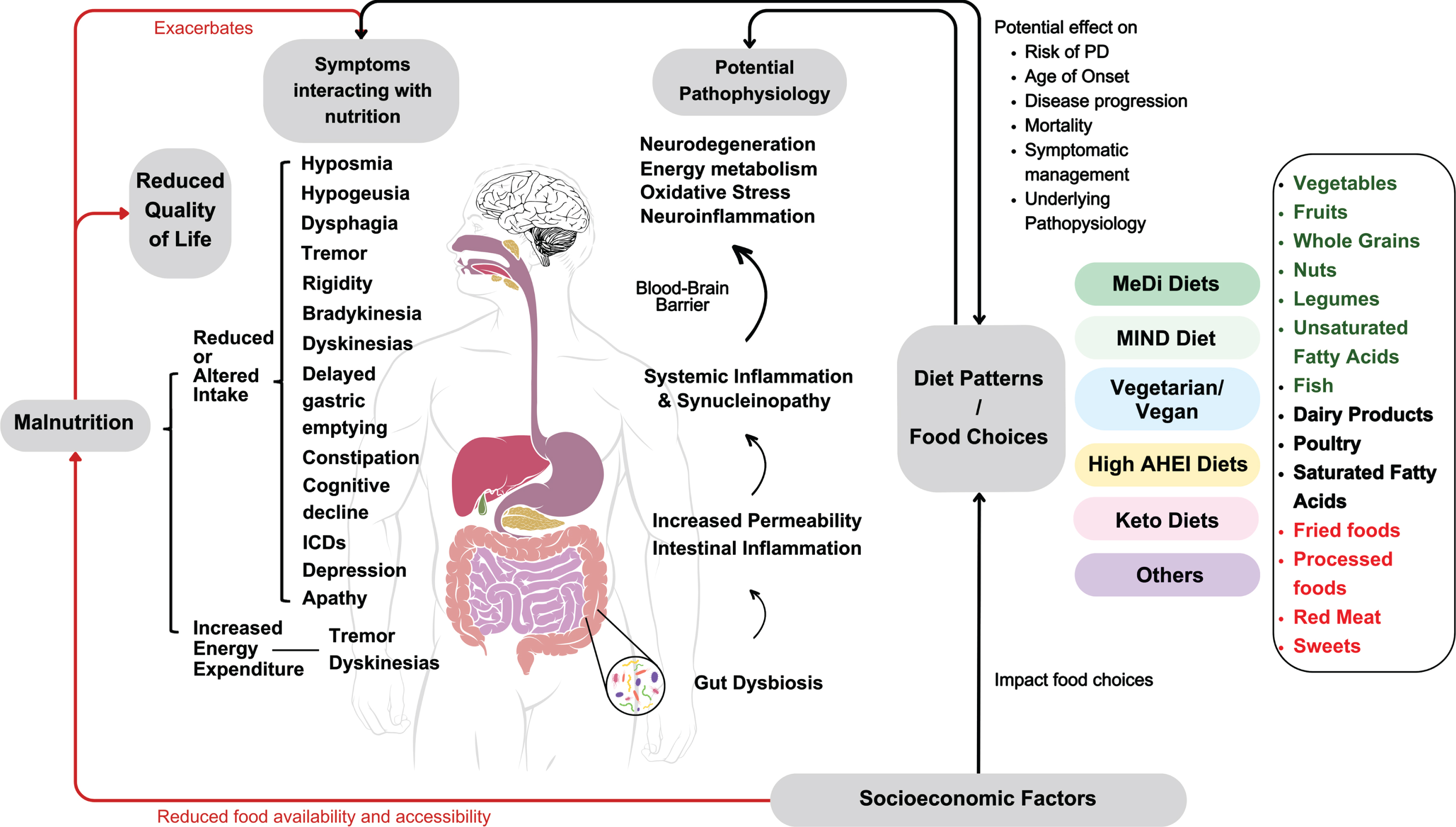
The role of nutrition in PD is of interest among clinicians, researchers and PwP alike, given strong epidemiological evidence implicating dietary patterns and malnutrition in the disease process [20]. However, few high-quality randomized controlled dietary intervention trials have been conducted in PD to date [20]. Randomized controlled nutrition intervention trials are challenging to conduct due to a variety of reasons including variability in baseline dietary factors and nutrient status [88], the necessity for substantial behavioral changes on the part of the participant and their household members, the risk of high attrition rates and suboptimal adherence, blinding and treatment standardization [89]. Reliable and convenient capture of dietary intake presents a further challenge as does variability in nutrient content in a given food, although the advent of biomarkers of food intake, or biomarkers of food intake (BFIs, e.g. of specific flavonoids) may prove to be an increasingly valuable tool in these regards [90]. In PD, added complications include long follow-up times required to ascertain a disease modifying effect, and the lack of reliable biomarkers to both identify patients with early disease who may optimally benefit from such interventions and to track interventional outcomes [20]. While consensus recommendations around a particular diet have yet to be developed for PD as a result, this paper sought to provide a comprehensive review of evidence in the field, and we will conclude with suggestions for future directions. Figure 1 illustrates the complex relationships between dietary patterns and food choices, socioeconomic factors, quality of life, PD-related malnutrition, symptoms and disease pathophysiology, highlighted in this review.
Fig. 1
Summary of the complex interactions of dietary patterns and food choices with socioeconomic factors, PD-related malnutrition, disease pathophysiology, symptoms and quality of life.
Where dietary patterns are concerned, the strongest evidence supports adherence to mostly plant-based, MIND and MeDi-style diets in PD, whereas the potential role of ketogenic diets is still unclear. While RCT data is limited, MIND and MeDi diets are believed to be generally safe and beneficial for overall health, and their adherence predicts reduced risk of prodromal and manifest PD [22, 28], older age of onset [18], reduced disease severity [11, 12], progression [28], and self-reported symptom burden in PD [27]. Higher scores on the related AHEI are strongly associated with lower mortality in PD [16]. Preliminary, short-term evidence suggests potential benefits of ketogenic diets in PD [10, 37, 39, 40], the safety and feasibility of these high-fat low-carbohydrate diets have yet to be adequately studied in PD, though. In practical terms, KD may be challenging to follow due to its restrictions on grains, sweets, and fruits. Therefore, ketone supplements and precursors, such as medium-chain triglyceride supplements, may be used to promote ketosis without rigorous limitations on carbohydrates. Intermittent fasting has been proposed as an alternative strategy to target bioenergetic deficits in PD; however, no interventional trials have yet been published to examine their safety, feasibility or efficacy to date [91]. Regardless of the dietary pattern followed, protein-redistribution diets may help to minimize motor fluctuations, though the safety of these diets with respect to weight maintenance and lean muscle mass preservation is an active area of investigation [6, 42].
Evidence for the effects of particular food groups on PD incidence, progression and symptomatology is similarly mixed, with the majority of work involving longitudinal observational studies. Such studies often report differences in PD incidence over several decades based on stratification according to dietary factors at baseline. One limitation in the interpretation of these studies is thus the possibility that participants’ dietary composition may have changed substantially over the follow-up period from their baseline state, which would reduce the strength of associations. Once PD is manifest, adherence to a healthy diet such as the AHEI is associated with reduced mortality during follow-up and a diet based on PROs is associated with slower disease progression, respectively [16, 47]. Several epidemiological studies have linked higher dairy consumption to an increased risk of PD, though it remains unclear whether this applies to all dairy products or specific groups only [17, 43–47]. Findings regarding the relationship of alcohol with PD risk are inconclusive, where the consumption of some alcohol compared to abstinence is potentially beneficial, and the moderate consumption of wine is frequently part of the MeDi [47, 52]; however, the possibility of reverse causation cannot be excluded, as reduced alcohol/drug consumption may represent a feature of a more risk-averse personality type associated with PD [92]. There are differences between food groups included in different MeDi diets and the role of items such as poultry, or potatoes remains to be further explored. In addition to applying existing dietary rating instruments originally developed for other conditions to PD cohorts, data-driven approaches should identify dietary patterns associated with better PD outcomes.
Limited RCTs suggest that dietary supplementation with vitamin E and omega-3 fatty acids may reduce the risk of PD, while citicoline may reduce motor and cognitive symptoms. Vitamin C, B6, B12 and folate supplementation may be of benefit in patients who are on levodopa [42, 76, 78, 93] although there is a paucity of RCTs. There is insufficient evidence for the potential role of vitamin D and B1 [62, 75]. Future studies into vitamin supplementation should take baseline levels into consideration and target those with baseline deficiencies in a move towards personalized medicine.
There are potential safety concerns regarding the use of Mucuna pruriens as an adjuvant therapy [87] but in low-resource settings, Mucuna pruriens might be a valuable alternative to levodopa.
Table 1
Summary of current evidence for nutritional interventions in Parkinson’s Disease
| Dietary pattern, component, or supplement | Description | Observational studies | Interventional studies |
| Mediterranean diet | Encourage: vegetables, fruits, nuts and seeds, fish/seafood, olive oil, wine (modest intake), whole grains, legumes, modest intake of poultry, seeds/nuts, wine | Mediterranean diets have been associated with reduced PD incidence, age of onset (particularly in men) and prodromal features [13, 14, 18, 21, 22] | Evidence from one RCT and one pilot study suggests that Mediterranean diets may improve cognition, relieve constipation and reduce PD symptom severity [11, 12] |
| Discourage: red/processed meat, fried food, sweets, soda [19] | |||
| MIND diet | Encourage: green leafy vegetables, nuts and seeds, seafood, berries, olive oil, wine, whole grains, poultry, legumes | The MIND diet is associated with reduced incidence, delayed age of onset (particularly in women) and slower progression of PD [18, 27, 28] | |
| Discourage: red meat, butter, fried food, soda, refined grains, sweets and pastries [26] | |||
| Vegan/Vegetarian diet | Reduced incidence of PD seen in vegan/vegetarian cultures [29, 32, 101] | One RCT showed improvements in motor symptoms following a 2-week ovo-lacto vegetarian diet intervention [33] | |
| AHEI | Encourage: Omega-3s, unsaturated fatty acids, vegetables, nuts and seeds, fruit, poultry, soy, up to 2 alcoholic drinks/day for men, 1 drink/day for women | Associated with reduced risk of developing PD prodromal features in the general population, and reduced all-cause mortality among PwP [16, 21, 102, 103] | |
| Discourage: red meat, processed meat, sugar sweetened beverages, fruit juices, trans fats, sodium [34] | |||
| Ketogenic diet | Encourage: High fat intake, low carbohydrate intake, vegetables, nuts and seeds, seafood, olive oil, coconut oil, egg, poultry, full-fat dairy | A total of four RCTs have demonstrated reductions in non-motor symptom severity and anxiety, and improvements in cognition and voice quality [10, 39–41] | |
| Discourage: soda, refined grains, sweets and pastries, pasta | |||
| Protein-redistribution diets | Reduced daytime and increased dinner time intake of protein while maintaining unchanged total protein intake | 10 RCTs have collectively shown that protein redistribution may help to minimize motor fluctuations, though more work is needed to evaluate the effects on muscle mass and body weight [6, 42] | |
| Dairy | Dairy intake may confer increased risk of PD [17, 43–46, 49] | ||
| Alcohol | Moderate alcohol consumption may be associated with reduced risk of PD [51, 52] | ||
| Caffeine | Coffee and caffeine intake are associated with reduced risk of PD onset among healthy individuals and reduced rates of progression among PwP [15, 55] | An RCT showed no benefits of caffeine pills relative to placebo, with potential adverse effects on cognition and dyskinesias [57] | |
| PRO-PD diet | Encourage: fresh vegetables, fresh fruit, nuts and seeds, non-fried fish, olive oil, wine, coconut oil, fresh herbs, and spices | Encouraged dietary components were associated with reduced rates of PD progression based on patient-reported outcomes in a large cross-sectional study [47] | |
| Discourage: canned fruits and vegetables, diet and non-diet soda, fried foods, beef, ice cream, yoghurt, and cheese [47] | |||
| Vitamin D | Several studies have noted high rates of vitamin D deficiency in PD, associated with disease risk, motor severity, cognitive impairment and increased fall risk [58–62] | Clinical trials have failed to demonstrate a benefit for vitamin D supplementation in the overall population of PwP [62]. Vitamin D3 supplementation may confer benefit in individuals with Fokl genotypes TT and CT [64] | |
| Vitamin E and omega-3 fatty acids | Omega-3 fatty acids: ALA (plants), DHA (fish) and EPA (fish) | Fish oil supplementation has been associated with reduced rates of PD progression using patient-reported outcomes [47, 93] | RCTs have shown reduced rates of progression of PD symptoms, decreased serum markers of inflammation and increased antioxidant capacity in response to supplementation with vitamin E and omega-3s [67, 68] |
| B Vitamins | Vitamin B1 (thiamine), vitamin B6, vitamin B9 (folate), vitamin B12 | Vitamin B1 deficiency may be associated with cognitive impairment in PD[75]. Supplementation with vitamin B6, B9 and B12 may be considered as a strategy to prevent hyperhomocysteinemia [69, 74] | |
| Vitamin C | Vitamin C enhances levodopa absorption and may be recommended in patients for whom drug availability is limited [77] | ||
| Citicoline | Citicoline supplementation might reduce motor and cognitive symptoms in PD and enable reductions in levodopa dose but studies are small, older and heterogenous [78] | ||
| Probiotics and prebiotics | Meta-analysis of 11 RCTs suggests improvements in motor and nonmotor symptoms and depression with use of a probiotic [27]. Prebiotics have been found to alleviate constipation symptoms in PD [81] | ||
| Mucuna pruriens | Mucuna pruriens may provide comparable symptomatic relief to levodopa in PD, though tolerability remains a barrier to widespread adoption [84–87] |
Two RCTs have established multi-strain probiotics as useful therapies for the treatment of PD-associated constipation [80, 81] and emerging evidence from a 2023 meta-analysis suggests that probiotics may reduce depression, motor and non-motor symptoms in PwP [79]. However, findings must be interpreted in light of significant heterogeneity in the bacterial strains, dosages, treatment durations and methods of administration between included trials. Most current probiotics consist of Bifidobacteria and Lactobacillus strains [94], which are elevated in PwP [95]. It is unclear whether single- or multi-strain probiotics offer greater benefits [96], and how the mode of delivery (ex. tablets, capsules, powdered sachets, yoghurts, and fermented milk drinks) affects bacterial stability, viability and subsequent colonization in the gut [97] and how concurrent diet might influence probiotic efficacy. Six trials of probiotics targeting depression, anxiety, gut health, constipation, and disease severity in PD are currently registered as active in on clinicaltrials.gov (NCT04871464; NCT05576818; NCT05146921; NCT04293159; NCT03968133; NCT05568498). The results of these trials will provide critical information regarding the indications for probiotic supplementation and their efficacy in PD.
Nutritional interventions are of great interest to PwP, as they provide an opportunity for self-management and empowerment, are generally low-risk, and can be beneficial for the treatment and prevention of a wide range of health conditions [98]. However, several barriers to dietary modification in PD need to be addressed: cultural considerations may require adjustment of MeDi-style diets [99], financial constraints can limit access to healthy foods, sex-specific effects of different dietary regimens need to be further investigated, and individualization of dietary regimens is often required to suit the requirements of patients and their care partners/families [98]. Physicians receive limited nutrition education in medical school curricula [100], and dietitians are rarely members of a PwP’s team.
CONCLUSION
PD intersects with nutrition on numerous levels, including pathophysiological mechanisms, motor and non-motor symptoms, medication interactions, disease course, quality of life and socio-economic determinants of health. Observational studies of Mediterranean-type dietary patterns suggest benefits for the risk to develop parkinsonism or PD, age of onset of PD, progression and survival, but RCTs of dietary patterns are urgently needed. The symptomatic management of nutrition-related complications in PD including the significant risk of malnutrition, requires an interdisciplinary team and evidence-supported strategies such as protein-redistribution diets. Nutritional guidelines in PD, training in nutrition for medical students [100] and physicians and access to dietitians trained in PD are necessary steps to integrate nutritional strategies into routine PD care while empowering PwP with a generally low-risk but potentially crucial self-management tool.
ACKNOWLEDGMENTS
The authors thank the following for their support: SAC is supported by the Marg Meikle Professorship in Parkinson’s Research (Pacific Parkinson’s Research Institute (PPRI)). KNT is funded by the Canada Graduate Scholarships Master’s (CGS-M) program. JSTL is supported by a Parkinson Canada Graduate Student Award. YNW and JSTL are supported by grants from the Weston Family Foundation. AC is supported by a grant from the Jack and Darlene Poole Foundation.
FUNDING
No external funding was received for this study.
CONFLICT OF INTEREST
The authors report no conflicts of interest in relation to the content of this manuscript. SAC has received grant funding from the Weston Family Foundation and the Pacific Parkinson’s Research Institute to study nutritional interventions in Parkinson’s disease.
REFERENCES
[1] | GBD 2016 Parkinson’s Disease Collaborators ((2018) ) Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016, Lancet Neurol 17: , 939–953. |
[2] | Dong-Chen X , Yong C , Yang X , Chen-Yu S , Li-Hua P ((2023) ) Signaling pathways in Parkinson’s disease: Molecular mechanisms and therapeutic interventions. Signal Transduct Target Ther 8: , 73. |
[3] | Fereshtehnejad S-M , Ghazi L , Shafieesabet M , Shahidi GA , Delbari A , Lökk J ((2014) ) Motor, psychiatric and fatigue features associated with nutritional status and its effects on quality of life in Parkinson’s disease patients, PLoS One 9: , e91153. |
[4] | Palavra NC , Lubomski M , Flood VM , Davis RL , Sue CM ((2021) ) Increased added sugar consumption is common in Parkinson’s disease. Front Nutr 8: , 628845. |
[5] | Simon N , Gantcheva R , Bruguerolle B , Viallet F ((2004) ) The effects of a normal protein diet on levodopa plasma kinetics in advanced Parkinson’s disease. Parkinsonism Relat Disord 10: , 137–142. |
[6] | Rusch C , Flanagan R , Suh H , Subramanian I ((2023) ) To restrict or not to restrict? Practical considerations for optimizing dietary protein interactions on levodopa absorption in Parkinson’s disease. NPJ Parkinsons Dis 9: , 98. |
[7] | Kacprzyk KW , Milewska M , Zarnowska A , Panczyk M , Rokicka G , Szostak-Wegierek D ((2022) ) Prevalence of malnutrition in patients with Parkinson’s disease: A systematic review. Nutrients 14: , 5194. |
[8] | Sheard JM , Ash S , Mellick GD , Silburn PA , Kerr GK ((2013) ) Markers of disease severity are associated with malnutrition in Parkinson’s disease, PLoS One 8: , e57986. |
[9] | Sheard JM , Ash S , Mellick GD , Silburn PA , Kerr GK ((2014) ) Improved nutritional status is related to improved quality of life in Parkinson’s disease. BMC Neurol 14: , 212. |
[10] | Krikorian R , Shidler MD , Summer SS , Sullivan PG , Duker AP , Isaacson RS , Espay AJ ((2019) ) Nutritional ketosis for mild cognitive impairment in Parkinson’s disease: A controlled pilot trial. Clin Park Relat Disord 1: , 41–47. |
[11] | Paknahad Z , Sheklabadi E , Derakhshan Y , Bagherniya M , Chitsaz A ((2020) ) The effect of the Mediterranean diet on cognitive function in patients with Parkinson’s disease: A randomized clinical controlled trial. Complement Ther Med 50: , 102366. |
[12] | Paknahad Z , Sheklabadi E , Moravejolahkami AR , Chitsaz A , Hassanzadeh A ((2022) ) The effects of Mediterranean diet on severity of disease and serum Total Antioxidant Capacity (TAC) in patients with Parkinson’s disease: A single center, randomized controlled trial. Nutr Neurosci 25: , 313–320. |
[13] | Strikwerda AJ , Dommershuijsen LJ , Ikram MK , Voortman T ((2021) ) Diet quality and risk of Parkinson’s disease: The Rotterdam Study. Nutrients 13: , 3970. |
[14] | Yin W , Löf M , Pedersen NL , Sandin S , Fang F ((2021) ) Mediterranean dietary pattern at middle age and risk of Parkinson’s disease: A Swedish cohort study. Mov Disord 36: , 255–260. |
[15] | Crotty GF , Maciuca R , Macklin EA , Wang J , Montalban M , Davis SS , Alkabsh JI , Bakshi R , Chen X , Ascherio A , Astarita G , Huntwork-Rodriguez S , Schwarzschild MA ((2020) ) Association of caffeine and related analytes with resistance to Parkinson disease among LRRK2 mutation carriers: A metabolomic study, Neurology 95: , e3428–e3437. |
[16] | Zhang X , Molsberry SA , Schwarzschild MA , Ascherio A , Gao X ((2022) ) Association of diet and physical activity with all-cause mortality among adults with Parkinson disease, JAMA Netw Open 5: , e2227738. |
[17] | Hughes KC , Gao X , Kim IY , Wang M , Weisskopf MG , Schwarzschild MA , Ascherio A ((2017) ) Intake of dairy foods and risk of Parkinson disease. Neurology 89: , 46–52. |
[18] | Metcalfe-Roach A , Yu AC , Golz E , Cirstea M , Sundvick K , Kliger D , Foulger LH , Mackenzie M , Finlay BB , Appel-Cresswell S ((2021) ) MIND and Mediterranean diets associated with later onset of Parkinson’s disease. Mov Disord 36: , 977–984. |
[19] | Hutchins-Wiese HL , Bales CW , Porter Starr KN ((2022) ) Mediterranean diet scoring systems: Understanding the evolution and applications for Mediterranean and non-Mediterranean countries. Br J Nutr 128: , 1371–1392. |
[20] | Rees J , Ryan J , Laws M , Devine A (2023) A comprehensive examination of the evidence for whole of diet patterns in Parkinson’s disease: A scoping review. Nutr Neurosci, doi:10.1080/1028415X.2023.2233727. |
[21] | Molsberry S , Bjornevik K , Hughes KC , Healy B , Schwarzschild M , Ascherio A ((2020) ) Diet pattern and prodromal features of Parkinson disease, Neurology 95: , e2095–e2108. |
[22] | Maraki MI , Yannakoulia M , Xiromerisiou G , Stefanis L , Charisis S , Giagkou N , Kosmidis MH , Dardiotis E , Hadjigeorgiou GM , Sakka P , Scarmeas N , Stamelou M ((2023) ) Mediterranean diet is associated with a lower probability of prodromal Parkinson’s disease and risk for Parkinson’s disease/dementia with Lewy bodies: A longitudinal study. Eur J Neurol 30: , 934–942. |
[23] | Ghosh TS , Rampelli S , Jeffery IB , Santoro A , Neto M , Capri M , Giampieri E , Jennings A , Candela M , Turroni S , Zoetendal EG , Hermes GDA , Elodie C , Meunier N , Brugere CM , Pujos-Guillot E , Berendsen AM , De Groot LCPGM , Feskins EJM , Kaluza J , Pietruszka B , Bielak MJ , Comte B , Maijo-Ferre M , Nicoletti C , De Vos WM , Fairweather-Tait S , Cassidy A , Brigidi P , Franceschi C , O’Toole PW ((2020) ) Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: The NU-AGE 1-year dietary intervention across five European countries. Gut 69: , 1218–1228. |
[24] | Okubo H , Miyake Y , Sasaki S , Murakami K , Tanaka K , Fukushima W , Kiyohara C , Tsuboi Y , Yamada T , Oeda T , Shimada H , Kawamura N , Sakae N , Fukuyama H , Hirota Y , Nagai M Fukuoka Kinki Parkinson’s Disease Study Group ((2012) ) Dietary patterns and risk of Parkinson’s disease: A case-control study in Japan. Eur J Neurol 19: , 681–688. |
[25] | Rusch C , Beke M , Tucciarone L , Nieves C Jr , Ukhanova M , Tagliamonte MS , Mai V , Suh JH , Wang Y , Chiu S , Patel B , Ramirez-Zamora A , Langkamp-Henken B ((2021) ) Mediterranean diet adherence in people with Parkinson’s disease reduces constipation symptoms and changes fecal microbiota after a 5-week single-arm pilot study. Front Neurol 12: , 794640. |
[26] | Morris MC , Tangney CC , Wang Y , Sacks FM , Bennett DA , Aggarwal NT ((2015) ) MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement 11: , 1007–1014. |
[27] | Fox DJ , Park SJ , Mischley LK ((2022) ) Comparison of associations between MIND and Mediterranean diet scores with patient-reported outcomes in Parkinson’s disease. Nutrients 14: , 5185. |
[28] | Agarwal P , Wang Y , Buchman AS , Holland TM , Bennett DA , Morris MC ((2018) ) MIND diet associated with reduced incidence and delayed progression of ParkinsonismA in old age. J Nutr Health Aging 22: , 1211–1215. |
[29] | McCarty MF ((2001) ) Does a vegan diet reduce risk for Parkinson’s disease? , Med Hypotheses 57: , 318–323. |
[30] | Williams U , Bandmann O , Walker R ((2018) ) Parkinson’s disease in Sub-Saharan Africa: A review of epidemiology, genetics and access to care. J Mov Disord 11: , 53–64. |
[31] | Ma C-L , Su L , Xie J-J , Long J-X , Wu P , Gu L ((2014) ) The prevalence and incidence of Parkinson’s disease in China: A systematic review and meta-analysis. J Neural Transm 121: , 123–134. |
[32] | Tresserra-Rimbau A , Thompson AS , Bondonno N , Jennings A , Kühn T , Cassidy A ((2023) ) Plant-based dietary patterns and Parkinson’s disease: A prospective analysis of the UK Biobank. Mov Disord 38: , 1994–2004. |
[33] | Hegelmaier T , Lebbing M , Duscha A , Tomaske L , Tönges L , Holm JB , Bjørn Nielsen H , Gatermann SG , Przuntek H , Haghikia A ((2020) ) Interventional influence of the intestinal microbiome through dietary intervention and bowel cleansing might improve motor symptoms in Parkinson’s disease. Cells 9: , 376. |
[34] | Chiuve SE , Fung TT , Rimm EB , Hu FB , McCullough ML , Wang M , Stampfer MJ , Willett WC ((2012) ) Alternative dietary indices both strongly predict risk of chronic disease. J Nutr 142: , 1009–1018. |
[35] | Zhang X , Molsberry SA , Yeh T-S , Cassidy A , Schwarzschild MA , Ascherio A , Gao X ((2022) ) Intake of flavonoids and flavonoid-rich foods and mortality risk among individuals with Parkinson disease: A prospective cohort study, Neurology 98: , e1064–e1076. |
[36] | Grammatikopoulou MG , Tousinas G , Balodimou C , Anastasilakis DA , Gkiouras K , Dardiotis E , Evangeliou AE , Bogdanos DP , Goulis DG ((2022) ) Ketogenic therapy for Parkinson’s disease: A systematic review and synthesis without meta-analysis of animal and human trials. Maturitas 163: , 46–61. |
[37] | Bohnen JLB , Albin RL , Bohnen NI ((2023) ) Ketogenic interventions in mild cognitive impairment, Alzheimer’s disease, and Parkinson’s disease: A systematic review and critical appraisal. Front Neurol 14: , 1123290. |
[38] | Norwitz NG , Hu MT , Clarke K ((2019) ) The mechanisms by which the ketone body D-β-hydroxybutyrate may improve the multiple cellular pathologies of Parkinson’s disease. Front Nutr 6: , 63. |
[39] | Phillips MCL , Murtagh DKJ , Gilbertson LJ , Asztely FJS , Lynch CDP ((2018) ) Low-fat versus ketogenic diet in Parkinson’s disease: A pilot randomized controlled trial. Mov Disord 33: , 1306–1314. |
[40] | Tidman MM , White D , White T ((2022) ) Effects of an low carbohydrate/healthy fat/ketogenic diet on biomarkers of health and symptoms, anxiety and depression in Parkinson’s disease: A pilot study. Neurodegener Dis Manag 12: , 57–66. |
[41] | Koyuncu H , Fidan V , Toktas H , Binay O , Celik H ((2021) ) Effect of ketogenic diet versus regular diet on voice quality of patients with Parkinson’s disease. Acta Neurol Belg 121: , 1729–1732. |
[42] | Boelens Keun JT , Arnoldussen IA , Vriend C , van de Rest O ((2021) ) Dietary approaches to improve efficacy and control side effects of levodopa therapy in Parkinson’s disease: A systematic review. Adv Nutr 12: , 2265–2287. |
[43] | Chen H , Zhang SM , Hernan MA , Willett WC , Ascherio A ((2002) ) Diet and Parkinson’s disease: A potential role of dairy products in men. Ann Neurol 52: , 793–801. |
[44] | Park M , Ross GW , Petrovitch H , White LR , Masaki KH , Nelson JS , Tanner CM , Curb JD , Blanchette PL , Abbott RD ((2005) ) Consumption of milk and calcium in midlife and the future risk of Parkinson disease. Neurology 64: , 1047–1051. |
[45] | Chen H , O’Reilly E , McCullough ML , Rodriguez C , Schwarzschild MA , Calle EE , Thun MJ , Ascherio A ((2007) ) Consumption of dairy products and risk of Parkinson’s disease. Am J Epidemiol 165: , 998–1006. |
[46] | Kyrozis A , Ghika A , Stathopoulos P , Vassilopoulos D , Trichopoulos D , Trichopoulou A ((2013) ) Dietary and lifestyle variables in relation to incidence of Parkinson’s disease in Greece. Eur J Epidemiol 28: , 67–77. |
[47] | Mischley LK , Lau RC , Bennett RD ((2017) ) Role of diet and nutritional supplements in Parkinson’s disease progression. Oxid Med Cell Longev 2017: , 6405278. |
[48] | Cortese M , Riise T , Engeland A , Ascherio A , Bjørnevik K ((2018) ) Urate and the risk of Parkinson’s disease in men and women. Parkinsonism Relat Disord 52: , 76–82. |
[49] | Abbott RD , Ross GW , Petrovitch H , Masaki KH , Launer LJ , Nelson JS , White LR , Tanner CM ((2016) ) Midlife milk consumption and substantia nigra neuron density at death. Neurology 86: , 512–519. |
[50] | Peters S , Gallo V , Vineis P , Middleton LT , Forsgren L , Sacerdote C , Sieri S , Kyrozis A , Chirlaque M-D , Zamora-Ros R , Hansson O , Petersson J , Katzke V , Kühn T , Mokoroa O , Masala G , Ardanaz E , Panico S , Bergmann MM , Key TJ , Weiderpass E , Ferrari P , Vermeulen R ((2020) ) Alcohol consumption and risk of Parkinson’s disease: Data from a large prospective European cohort. Mov Disord 35: , 1258–1263. |
[51] | Shao C , Wang X , Wang P , Tang H , He J , Wu N ((2021) ) Parkinson’s disease risk and alcohol intake: A systematic review and dose-response meta-analysis of prospective studies. Front Nutr 8: , 709846. |
[52] | Mitchell E , Chohan H , Bestwick JP , Noyce AJ ((2022) ) Alcohol and Parkinson’s disease: A systematic review and meta-analysis. J Parkinsons Dis 12: , 2369–2381. |
[53] | Liu R , Guo X , Park Y , Wang J , Huang X , Hollenbeck A , Blair A , Chen H ((2013) ) Alcohol consumption, types of alcohol, and Parkinson’s disease, PLoS One 8: , e66452. |
[54] | Hong CT , Chan L , Bai C-H ((2020) ) The effect of caffeine on the risk and progression of Parkinson’s disease: A meta-analysis. Nutrients 12: , 1860. |
[55] | Gabbert C , König IR , Lüth T , Kolms B , Kasten M , Vollstedt E-J , Balck A , Grünewald A , Klein C , Trinh J ((2022) ) Coffee, smoking and aspirin are associated with age at onset in idiopathic Parkinson’s disease. J Neurol 269: , 4195–4203. |
[56] | Ren X , Chen J-F ((2020) ) Caffeine and Parkinson’s disease: Multiple benefits and emerging mechanisms. Front Neurosci 14: , 602697. |
[57] | Postuma RB , Anang J , Pelletier A , Joseph L , Moscovich M , Grimes D , Furtado S , Munhoz RP , Appel-Cresswell S , Moro A , Borys A , Hobson D , Lang AE ((2017) ) Caffeine as symptomatic treatment for Parkinson disease (Cafe-PD): A randomized trial. Neurology 89: , 1795–1803. |
[58] | Zhou Z , Zhou R , Zhang Z , Li K ((2019) ) The association between vitamin D status, vitamin D supplementation, sunlight exposure, and Parkinson’s disease: A systematic review and meta-analysis. Med Sci Monit 25: , 666–674. |
[59] | Lawton M , Baig F , Toulson G , Morovat A , Evetts SG , Ben-Shlomo Y , Hu MT ((2020) ) Blood biomarkers with Parkinson’s disease clusters and prognosis: The oxford discovery cohort. Mov Disord 35: , 279–287. |
[60] | Wu H , Khuram Raza H , Li Z , Li Z , Zu J , Xu C , Yang D , Cui G ((2022) ) Correlation between serum 25(OH)D and cognitive impairment in Parkinson’s disease. J Clin Neurosci 100: , 192–195. |
[61] | Zhang H-J , Zhang J-R , Mao C-J , Li K , Wang F , Chen J , Liu C-F ((2019) ) Relationship between 25-Hydroxyvitamin D, bone density, and Parkinson’s disease symptoms. Acta Neurol Scand 140: , 274–280. |
[62] | Barichella M , Garrì F , Caronni S , Bolliri C , Zocchi L , Macchione MC , Ferri V , Calandrella D , Pezzoli G ((2022) ) Vitamin Dstatus and Parkinson’s disease. Brain Sci 12: , 790. |
[63] | Eyles DW , Smith S , Kinobe R , Hewison M , McGrath JJ ((2005) ) Distribution of the vitamin D receptor and 1 alpha-hydroxylase in human brain. J Chem Neuroanat 29: , 21–30. |
[64] | Suzuki M , Yoshioka M , Hashimoto M , Murakami M , Noya M , Takahashi D , Urashima M ((2013) ) Randomized, double-blind, placebo-controlled trial of vitamin D supplementation in Parkinson disease. Am J Clin Nutr 97: , 1004–1013. |
[65] | Henderson EJ , Lyell V , Bhimjiyani A , Amin J , Kobylecki C , Gregson CL ((2019) ) Management of fracture risk in Parkinson’s: A revised algorithm and focused review of treatments. Parkinsonism Relat Disord 64: , 181–187. |
[66] | Tamtaji OR , Taghizadeh M , Aghadavod E , Mafi A , Dadgostar E , Daneshvar Kakhaki R , Abolhassani J , Asemi Z ((2019) ) The effects of omega-3 fatty acids and vitamin E co-supplementation on gene expression related to inflammation, insulin and lipid in patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled trial. Clin Neurol Neurosurg 176: , 116–121. |
[67] | Taghizadeh M , Tamtaji OR , Dadgostar E , Daneshvar Kakhaki R , Bahmani F , Abolhassani J , Aarabi MH , Kouchaki E , Memarzadeh MR , Asemi Z ((2017) ) The effects of omega-3 fatty acids and vitamin E co-supplementation on clinical and metabolic status in patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled trial. Neurochem Int 108: , 183–189. |
[68] | Pantzaris M , Loukaides G , Paraskevis D , Kostaki E-G , Patrikios I ((2021) ) Neuroaspis PLP10TM, a nutritional formula rich in omega-3 and omega-6 fatty acids with antioxidant vitamins including gamma-tocopherol in early Parkinson’s disease: A randomized, double-blind, placebo-controlled trial. Clin Neurol Neurosurg 210: , 106954. |
[69] | Ahlskog JE ((2023) ) Levodopa, homocysteine and Parkinson’s disease: What’s the problem? Parkinsonism Relat Disord 109: , 105357. |
[70] | Rogers JD , Sanchez-Saffon A , Frol AB , Diaz-Arrastia R ((2003) ) Elevated plasma homocysteine levels in patients treated with levodopa: Association with vascular disease. Arch Neurol 60: , 59–64. |
[71] | Smith AD , Refsum H ((2021) ) Homocysteine - from disease biomarker to disease prevention. J Intern Med 290: , 826–854. |
[72] | Periñan MT , Macías-García D , JesúsS , Martín-Rodríguez JF , Muñoz-Delgado L , Jimenez-Jaraba MV , Buiza-Rueda D , Bonilla-Toribio M , Adarmes-Gómez AD , Gómez-Garre P , Mir P ((2023) ) Homocysteinelevels, genetic background, and cognitive impairment in Parkinson’sdisease. J Neurol 270: , 477–485. |
[73] | Sampedro F , Martínez-Horta S , Horta-Barba A , Grothe MJ , Labrador-Espinosa MA , Jesús S , Adarmes-Gómez A , Carrillo F , Puig-Davi A , Lora FR , Barbera MA , Pastor P , Arroyo SE , Vila BS , Foraster AC , Martínez JR , Padilla FC , Morlans MP , Aramburu IG , Ceberio JI , Vara JH , de Febregues-Boixar O , de Deus Fonticoba T , Ávila A , Martínez-Castrillo JC , Bejr-Kasem H , Campolongo A , Pascual-Sedano B COPPADIS Study Group Martínez-Martín P , Santos-García D , Mir P , Kulisevsky J ((2022) ) Increased homocysteine levels correlate with corticalstructural damage in Parkinson’s disease., J Neurol Sci 434: , 120148. |
[74] | Anamnart C , Kitjarak R ((2021) ) Effects of vitamin B12, folate, and entacapone on homocysteine levels in levodopa-treated Parkinson’s disease patients: A randomized controlled study. J Clin Neurosci 88: , 226–231. |
[75] | Håglin L , Domellöf M , Bäckman L , Forsgren L ((2020) ) Low plasma thiamine and phosphate in male patients with Parkinson’s disease is associated with mild cognitive impairment. Clin Nutr ESPEN 37: , 93–99. |
[76] | Niu F , Xie W , Zhang W , Kawuki J , Yu X (2023) Vitamin C, vitamin E, β-carotene and risk of Parkinson’s disease: A systematic review and dose-response metaanalysis of observational studies. Nutr Neurosci, doi: 10.1080/1028415X.2023.2192561. |
[77] | Nagayama H , Hamamoto M , Ueda M , Nito C , Yamaguchi H , Katayama Y ((2004) ) The effect of ascorbic acid on the pharmacokinetics of levodopa in elderly patients with Parkinson disease. Clin Neuropharmacol 27: , 270–273. |
[78] | Que D-LS , Jamora RDG ((2021) ) Citicoline as adjuvant therapy in Parkinson’s disease: A systematic review, Clin Ther 43: , e19–e31. |
[79] | Park JM , Lee SC , Ham C , Kim YW ((2023) ) Effect of probiotic supplementation on gastrointestinal motility, inflammation, motor, non-motor symptoms and mental health in Parkinson’s disease: A meta-analysis of randomized controlled trials. Gut Pathog 15: , 9. |
[80] | Tan AH , Lim S-Y , Chong KK , Manap AMAA , Hor JW , Lim JL , Low SC , Chong CW , Mahadeva S , Lang AE ((2021) ) Probiotics for constipation in Parkinson disease: A randomized placebo-controlled study, Neurology 96: , e772–e782. |
[81] | Barichella M , Pacchetti C , Bolliri C , Cassani E , Iorio L , Pusani C , Pinelli G , Privitera G , Cesari I , Faierman SA , Caccialanza R , Pezzoli G , Cereda E ((2016) ) Probiotics and prebiotic fiber for constipation associated with Parkinson disease: An RCT. Neurology 87: , 1274–1280. |
[82] | Baert F , Matthys C , Maselyne J , Van Poucke C , Van Coillie E , Bergmans B , Vlaemynck G ((2021) ) Parkinson’s disease patients’ short chain fatty acids production capacity after fecal fiber fermentation, NPJ Parkinsons Dis 7: , 72. |
[83] | Hall DA , Voigt RM , Cantu-Jungles TM , Hamaker B , Engen PA , Shaikh M , Raeisi S , Green SJ , Naqib A , Forsyth CB , Chen T , Manfready R , Ouyang B , Rasmussen HE , Sedghi S , Goetz CG , Keshavarzian A ((2023) ) An open label, non-randomized study assessing a prebiotic fiber intervention in a small cohort of Parkinson’s disease participants. Nat Commun 14: , 926. |
[84] | Fothergill-Misbah N , Maroo H , Cham M , Pezzoli G , Walker R , Cilia R ((2020) ) Could Mucuna pruriens be the answer to Parkinson’s disease management in sub-Saharan Africa and other low-income countries worldwide? Parkinsonism Relat Disord 73: , 3–7. |
[85] | Katzenschlager R , Evans A , Manson A , Patsalos PN , Ratnaraj N , Watt H , Timmermann L , Van der Giessen R , Lees AJ ((2004) ) Mucuna pruriens in Parkinson’s disease: A double blind clinical and pharmacological study. J Neurol Neurosurg Psychiatry 75: , 1672–1677. |
[86] | Cilia R , Laguna J , Cassani E , Cereda E , Pozzi NG , Isaias IU , Contin M , Barichella M , Pezzoli G ((2017) ) Mucuna pruriens in Parkinson disease: A double-blind, randomized, controlled, crossover study. Neurology 89: , 432–438. |
[87] | Cilia R , Laguna J , Cassani E , Cereda E , Raspini B , Barichella M , Pezzoli G ((2018) ) Daily intake of Mucuna pruriens in advanced Parkinson’s disease: A 16-week, noninferiority, randomized, crossover, pilot study. Parkinsonism Relat Disord 49: , 60–66. |
[88] | Weaver CM , Miller JW ((2017) ) Challenges in conducting clinical nutrition research. Nutr Rev 75: , 491–499. |
[89] | Mirmiran P , Bahadoran Z , Gaeini Z ((2021) ) Common limitations and challenges of dietary clinical trials for translation into clinical practices, Int J Endocrinol Metab 19: , e108170. |
[90] | Dragsted LO , Gao Q , Scalbert A , Vergères G , Kolehmainen M , Manach C , Brennan L , Afman LA , Wishart DS , Andres Lacueva C , Garcia-Aloy M , Verhagen H , Feskens EJM , Praticò G ((2018) ) Validation of biomarkers of food intake-critical assessment of candidate biomarkers. Genes Nutr 13: , 14. |
[91] | Neth BJ , Bauer BA , Benarroch EE , Savica R ((2021) ) The role of intermittent fasting in Parkinson’s disease. Front Neurol 12: , 682184. |
[92] | Evans AH , Lawrence AD , Potts J , MacGregor L , Katzenschlager R , Shaw K , Zijlmans J , Lees AJ ((2006) ) Relationship between impulsive sensation seeking traits, smoking, alcohol and caffeine intake, and Parkinson’s disease. J Neurol Neurosurg Psychiatry 77: , 317–321. |
[93] | Mischley LK , Farahnik J , Mantay L , Punzi J , Szampruch K , Ferguson T , Fox DJ ((2023) ) Parkinson symptom severity and use of nutraceuticals. Nutrients 15: , 802. |
[94] | Hong C-T , Chen J-H , Huang T-W ((2022) ) Probiotics treatment for Parkinson disease: A systematic review and meta-analysis of clinical trials. Aging 14: , 7014–7025. |
[95] | Romano S , Savva GM , Bedarf JR , Charles IG , Hildebrand F , Narbad A ((2021) ) Meta-analysis of the Parkinson’s disease gut microbiome suggests alterations linked to intestinal inflammation. NPJ Parkinsons Dis 7: , 27. |
[96] | Ouwehand AC , Invernici MM , Furlaneto FAC , Messora MR ((2018) ) Effectiveness of multistrain versus single-strain probiotics: Current status and recommendations for the future. , Proceedings from the 9th Probiotics, Prebiotics and New Foods, Nutraceuticals and Botanicals for Nutrition&Human and Microbiota Health Meeting, held in Rome, Italy from September 10 to 12, 2017, J Clin Gastroenterol 52 Suppl 1: , S35–S40. |
[97] | Cunningham M , Vinderola G , Charalampopoulos D , Lebeer S , Sanders ME , Grimaldi R ((2021) ) Applying probiotics and prebiotics in new delivery formats - is the clinical evidence transferable? Trends Food Sci Technol 112: , 495–506. |
[98] | Willett W , Rockström J , Loken B , Springmann M , Lang T , Vermeulen S , Garnett T , Tilman D , DeClerck F , Wood A , Jonell M , Clark M , Gordon LJ , Fanzo J , Hawkes C , Zurayk R , Rivera JA , De Vries W , Majele Sibanda L , Afshin A , Chaudhary A , Herrero M , Agustina R , Branca F , Lartey A , Fan S , Crona B , Fox E , Bignet V , Troell M , Lindahl T , Singh S , Cornell SE , Srinath Reddy K , Narain S , Nishtar S , Murray CJL ((2019) ) Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 393: , 447–492. |
[99] | Sauerbier A , Schrag A , Martinez-Martin P , Hall LJ , Parry M , Mischley LK , Zis P , Chaudhuri KR ((2018) ) Dietary variations in a multiethnic Parkinson’s disease cohort and possible influences on nonmotor aspects: A cross-sectional multicentre study. Parkinsons Dis 2018: , 7274085. |
[100] | Crowley J , Ball L , Hiddink GJ ((2019) ) Nutrition in medical education: A systematic review, Lancet Planet Health 3: , e379–e389. |
[101] | McCarty MF , Lerner A ((2021) ) Perspective: Low risk of Parkinson’s disease in quasi-vegan cultures may reflect GCN2-mediated upregulation of parkin. Adv Nutr 12: , 355–362. |
[102] | Gao X , Chen H , Fung TT , Logroscino G , Schwarzschild MA , Hu FB , Ascherio A ((2007) ) Prospective study of dietary pattern and risk of Parkinson disease. Am J Clin Nutr 86: , 1486–1494. |
[103] | Sääksjärvi K , Knekt P , Lundqvist A , Männistö S , Heliövaara M , Rissanen H , Järvinen R ((2013) ) A cohort study on diet and the risk of Parkinson’s disease: The role of food groups and diet quality. Br J Nutr 109: , 329–337. |


