
Understanding the Perseverance of the Muscular Dystrophy Community One-Year into the COVID-19 Pandemic
Abstract
Introduction:
In this study, we examined the long-term social and health impacts of the coronavirus disease 2019 (COVID-19) pandemic on people with muscular dystrophy.
Methods:
We modified our prior COVID-19 Impact Survey to assess impacts from the continuing pandemic using feedback from muscular dystrophy experts, patients, and advocacy group/registry representatives. The survey assessed COVID-19 medical history, and the effects of the pandemic on social aspects, muscle disease, and medical care. We also used the validated 10-item Perceived Stress Scale. The de-identified, electronic survey was distributed to adults with muscular dystrophy via international patient registries and advocacy group websites from February 8, 2021 to March 22, 2021.
Results:
Respondents (n = 1243 : 49% Facioscapulohumeral Muscular Dystrophy (FSHD); 43% Myotonic Dystrophy (DM), and 8% Limb-Girdle Muscular Dystrophy (LGMD)) were mostly women and middle-aged (range 18–90 years). Rates of COVID-19 infections were low at 8% with zero deaths. Reported recovery times were also short with only 9% reporting a recovery period greater than eight weeks, and 7% requiring hospitalization with one individual requiring a ventilator. Major challenges reported during the pandemic included stress management, particularly for those with LGMD (27%), and wearing a mask (24%). The majority reported a slight worsening of their disease state. Respondents reported moderate stress levels (stress score = 16.4; range = 0–39), with higher stress levels reported by women and those under age 30 years. Seventy-percent of participants who had telemedicine visits were satisfied with the encounters; however, most reported a preference for in-person visits.
Conclusions:
People with muscular dystrophy found ways to manage their stress and overcome obstacles during the COVID-19 pandemic. COVID-19 infection rates and medical complications were similar to a general population. Telemedicine visits may have a more permanent role in care.
INTRODUCTION
After two years, the coronavirus disease 2019 (COVID-19) pandemic and the related social guidelines implemented to control its spread, has continued to have an impact on daily living worldwide. The pandemic has limited access to medical care and altered how care is delivered, including an increase in the use of telemedicine visits [1]. In addition, certain populations, such as older adults and those with pre-existing conditions, especially those with cardiac or respiratory diseases, are at higher risk for complications when infected with the coronavirus. Patients with certain muscular dystrophies (MD), such as those with cardio-pulmonary involvement, may be at higher risk for poor outcomes with COVID-19 [2] as well as other impacts on daily living. Given these risks, the Muscular Dystrophy Association has continued to recommend that individuals with MD avoid exposure to COVID-19 by following CDC guidelines, and they now recommend vaccination [3].
In May 2020, we conducted a survey to understand the initial effects of the COVID-19 pandemic and associated social guidelines on people with MD. We found that participants reported challenges with obtaining treatment and essentials, stress management, and social distancing. They also reported moderate stress levels, which were comparable to the general population [4].
This study re-examines the impact of the COVID-19 pandemic and the associated strategies aimed at mitigating the spread on individuals living with MD just over one year into the pandemic. For those who had been infected with COVID-19 we examined their reported experiences. In addition, we sought to better understand their experiences with health care delivery and participation in research one year into the COVID-19 pandemic.
METHODS
We conducted a prospective de-identified electronic survey of people with MD worldwide from, February 8, 2021 to March 22, 2021, before the vaccine became widely available (Addendum 1). The study was approved by the University of Rochester Medical Center Institutional Review Board, and exempted from HIPAA consent requirements, as all surveys were de-identified. Like our prior study [4], participants completed the survey through a weblink connected to a centralized REDCap database [5]. The survey was distributed to individuals with facioscapulohumeral dystrophy (FSHD), myotonic dystrophy (DM), or Limb Girdle Muscular Dystrophy (LGMD) via patient registries and patient advocacy groups. In lieu of a consent, an IRB-approved Information Sheet was sent with the electronic link to the survey. The registries used have approximately a total of 7,000 registrants, which include individuals with muscular dystrophy, their family members, and health care providers; therefore, it is difficult to determine a response rate as the exact number of individuals with MD or caretakers who received the link is unknown. Additionally, to decipher between types of survey respondents, we asked them to identify themselves as either an individual with MD or a caretaker of an individual with MD so that those who do not identify as either would not continue the survey.
Individuals who responded to the first survey, distributed in May 2020, were allowed to complete this survey. Twenty-four percent (n = 297) reported that they completed the initial survey.
Measures
We modified the COVID-19 Impact Survey used in our previous study to assess the impact that the continued pandemic was having on individuals with MD. We implemented feedback provided by muscular dystrophy patients and experts in the field. Specifically, we added questions about genetic confirmation of the participant’s muscular dystrophy, additional COVID-19 questions to assess the severity of infection and its impact on our study population, and additional questions to learn more about experience of telemedicine visits. We also modified the multiple-choice responses on some questions to reflect what we learned from the initial COVID-19 Impact Survey. Participants also completed the Perceived Stress Scale (PSS) as before [4, 6]. The PSS is a 10-item patient reported measure of perceived stress. Each item is scored 0–4 for a total score of 0–40 with higher scores indicating greater stress [8].
Statistical analysis
Data were summarized by responses to each question: frequencies, means, and standard deviations (SD). Associations between discrete or continuous data elements were explored using Pearson correlations [7]. Differences in perceived stress between groups based on clinical diagnosis, gender, age categories (18 to 29 years; 30 to 59 years; older than 60 years), or ambulatory status was performed by ANOVA using Tukey’s method for multiple comparisons, or T-test. Where there were differences by diagnosis, an ANCOVA was performed to adjust for potential demographic differences. Statistical analysis was performed using SPSS (version 26, IBM Corp). For this exploratory survey, all statistical testing was two-sided and a p-value < 0.05 is significant.
RESULTS
Participants
Twelve hundred and forty-three adults with MD residing worldwide responded to the survey (Table 1). Respondents’ mean age was 52.5 years (range 18–90; SD = 14.4) and were more frequently female (58%). Participants were affected by FSHD (50%), DM (43%) and LGMD (8%). The majority (89%) of participants reported genetic confirmation and most individuals reported living with other people, rather than alone. Approximately, one-third reported using a wheelchair for mobility, either part or full-time.
Table 1
Patient demographics
| FSHD (n = 613) | DM (n = 531) | LGMD (n = 99) | Total (n = 1243) | |
| Gender | ||||
| Male | 45% | 39% | 38% | 42% |
| Female | 54% | 61% | 60% | 58% |
| Age | ||||
| 18–30 | 6% | 5% | 20% | 7% |
| 31–59 | 52% | 64% | 71% | 59% |
| 60+ | 42% | 31% | 9% | 35% |
| Race | ||||
| White | 92% | 95% | 87% | 93% |
| Black | 0% | 1% | 1% | 0% |
| Asian | 3% | 1% | 9% | 3% |
| American Indian/Alaskan Native | 1% | 1% | 1% | 1% |
| More than one race | 3% | 2% | 0% | 2% |
| Unknown | 1% | 1% | 2% | 1% |
| Ethnicity | ||||
| Hispanic/Latino | 5% | 4% | 7% | 5% |
| Not Hispanic/Latino | 92% | 92% | 89% | 92% |
| Not reported | 3% | 4% | 4% | 3% |
| Location | ||||
| US | 65% | 70% | 55% | 66% |
| Canada | 4% | 4% | 4% | 4% |
| Europe and UK | 22% | 19% | 23% | 21% |
| Other/Not reported | 9% | 6% | 18% | 9% |
COVID-19
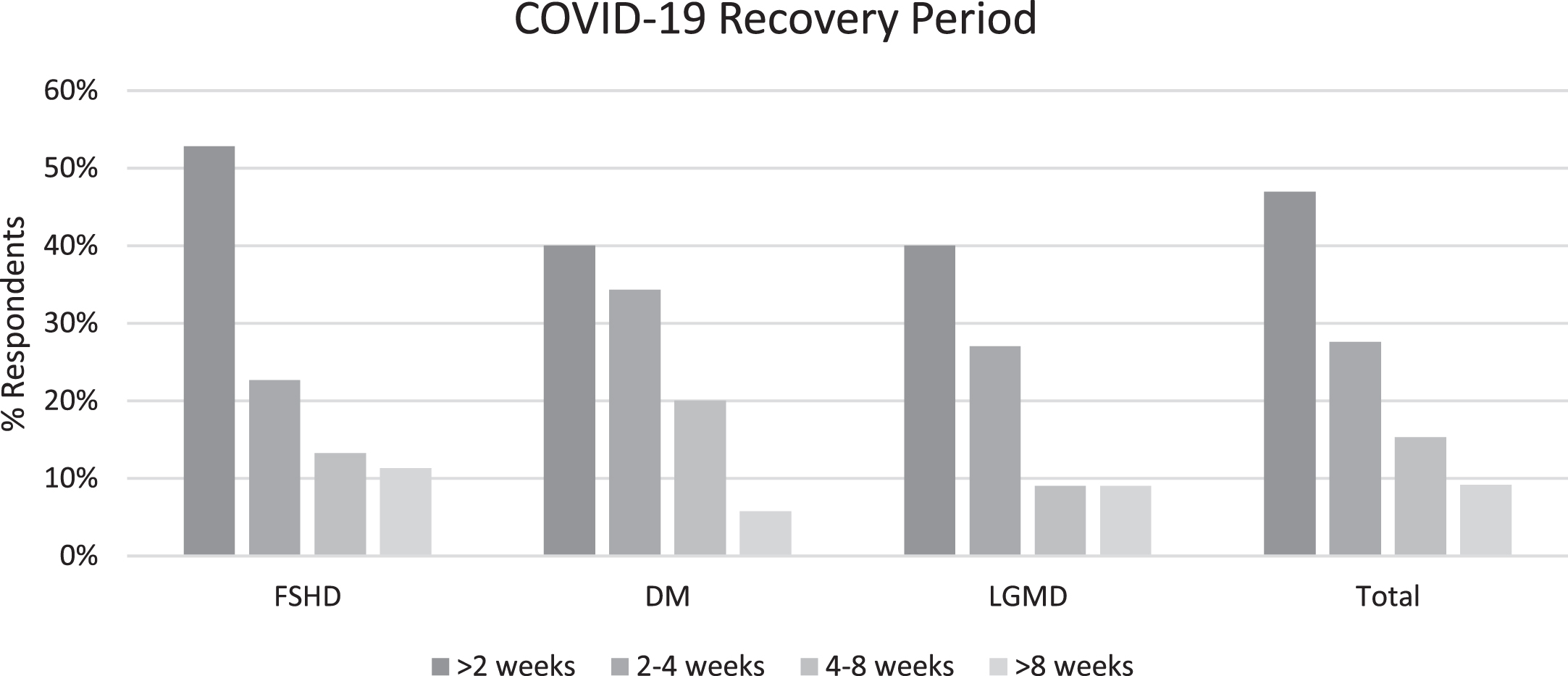
Approximately one year into the pandemic 98 (7.9%; 95% Confidence Interval (CI): 6–10%) individuals with MD (DM = 34%; FSHD = 56%; LGMD = 10%) reported having COVID-19 at one point. Their average age was 48.3 years (range 20–74; SD = 13.1), majority were Caucasian (93%) and non-Hispanic (89%), and followed the distribution of sex in the overall sample. The majority of the individuals who had COVID-19 (68%) were living in the US; 20% were living in the European Union. Figure 1 summarizes the common COVID-19 symptoms experienced by those with MD, with fatigue being the most common symptom (80%) among all the muscle diseases. Eight individuals were hospitalized with two individuals requiring care in the intensive care unit and one requiring ventilator support. The majority (68%; 95% CI 60–78%) of individuals reported that they were not medically impacted (i.e., required hospitalization, on a ventilator, in the intensive care unit) by COVID-19, and 47% (95% CI: 39–57%) reported a recovery of less than two weeks (Fig. 2). However, 24 (24% (95% CI: 16–32%) individuals took more than a month to recover (no longer having symptoms) (Fig. 2). Recovery time was not significantly different between age groups (F(2,94) = 2.1; p = 0.13) or diagnoses (F(2,94) = 2.16, p = 0.81).
Fig. 1
Symptoms experienced and reported by individuals with MD.
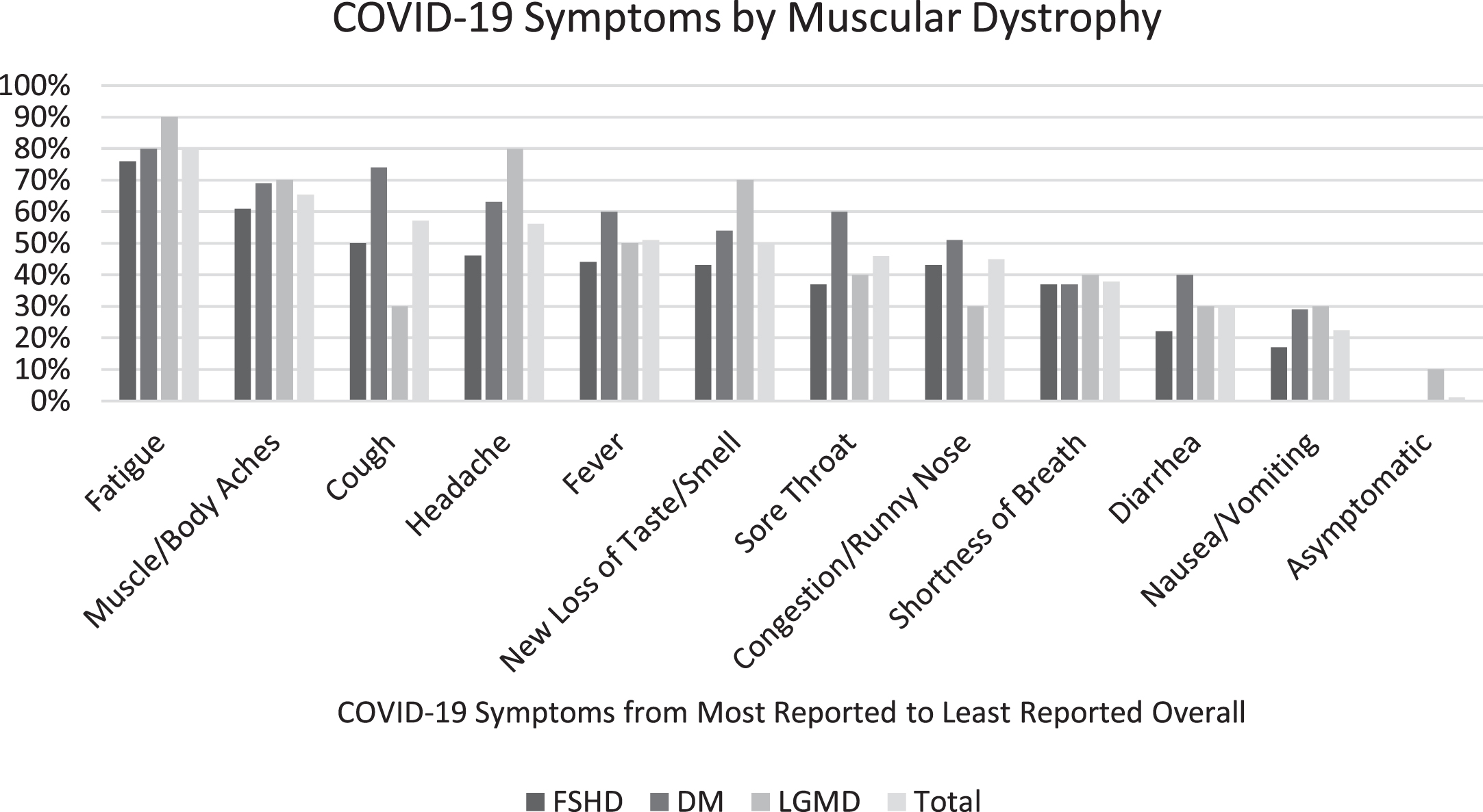
Fig. 2
Reported recovery times after being infected with COVID-19.
3.3Strategies and Challenges during COVID-19 Pandemic
Social distancing (96%), wearing masks in public (95%), and avoiding crowds larger than ten people (85%), were reported by the majority of participants as social strategies in their geographic area. Challenges most frequently reported during the COVID-19 pandemic were obtaining treatment (42%), managing stress (45%), and social distancing (41%). Other challenges reported by participants included social isolation, lack of access to exercise (the most-cited was swimming), and lack of access to mental health services.
3.4Impact on Muscular Dystrophy
More than half of the individuals reported that they felt that their muscle disease was slightly worse, while over one-quarter of participants reported no change in their muscle disease in the prior six months. One-fifth reported that local pandemic-related policies contributed to the change in their muscle disease, and cited not being able to go to physical therapy, gyms, leave their home, or receive medical care as factors affecting their muscle disease. Of those individuals who reported exercising (n = 716), 54% reported that their exercise had decreased over the prior three months (20% reported an increase in exercise and 32% reported no change).
In regard to pain, almost three-quarters of individuals reported pain with a mean pain level 52 on a 100-point scale. A higher percentage of individuals with FSHD (79%) reported pain, followed by DM (68%) and LGMD (53%). Of those that reported pain, more than half of them reported their pain had worsened over the prior three months, 35% reported no change in their pain, and a small percentage of participants (6%) reported improvement in their pain.
Perceived Stress
The mean PSS score was 16.4 (range 0–39; sd = 7.5) indicating moderate stress (low = 0–13; moderate = 14–26; and high = 27–39) [8]. Individuals with FSHD (mean PSS = 16.21) and DM (mean PSS = 16.23) had similar stress scores, but those with LGMD (mean PSS = 18.70) reported significantly higher stress scores (F(2,1240) = 4.50, p = 0.007). The significant difference in stress scores between the various MDs was eliminated when we adjusted for sex and age (F(2,1232) = 2.2, p = 0.12). We also found that women and individuals younger than 30 years of age also reported statistically significant higher levels of stress. Stress scores were positively correlated with pain and inability to manage stress (ρ= 0.27; p < 0.0001 and r = 0.48; p < 0.0001, respectively). Individuals who reported engaging in exercise had significantly less stress than their counterparts who did not report exercise (F(1,1230) = 24.2; p < 0.001). Many participants (86%) reported that they have been able to manage their stress and have done so most frequently by maintaining a routine, faith, and connecting with family and friends. Additionally, those who reported that they were able to manage their stress had lower reported pain levels (F(1,858) = 19.9; p < 0.001).
Impact on Access to Healthcare and Participation in Research
Most of the survey respondents (91%) reported residing in countries with advanced medical care, which indicated they had access to similar levels of careTable 1). Half of the survey respondents reported canceled or rescheduled health care visits. The majority of these visits were primary care, followed by neurology and therapy (i.e. physical or occupational therapy). Sixty-one percent of participants reported they had participated in a telemedicine appointment via telephone calls or video conferencing platforms. Participants were asked to rate their satisfaction with their telemedicine experience on a 0 (not satisfied) to 10 (completely satisfied) scale. The reported mean satisfaction rating was 7.2, with 76.5% stating they would like the option to continue telemedicine visits. More than half who participated in telemedicine visits reported that the visits would be better if the technology were easier to access and use. Other commonly-cited reasons that would make them more likely to participate in telemedicine visits were mobility issues that make it difficult to get to in-person appointments, having reliable audio/visual in the technology, and increased access to non-local healthcare providers. The majority of individuals (64.4%) who experienced both in-person and telemedicine health care appointments preferred in-person visits.
Ten percent of survey respondents reported participating in research studies during COVID-19 and more than half reported that their study was not affected by the pandemic. Only 31% of research participants reported delayed study visits, 20% reported canceled study visits, and 22% reported modified study procedures. Despite these challenges, two-thirds of survey respondents who participated in research during COVID-19 reported that they would be more likely or definitely likely to continue to participate in research; 20.2% reported their likelihood of continuing to participate in research remains unchanged.
DISCUSSION
The day-to-day lives of individuals with MD continued to be affected by the pandemic, and by the associated guidelines to mitigate the spread of COVID-19, as we entered Year Two. At that later time point, more individuals had been infected with COVID-19, which enabled us to better examine their experiences with the virus. Throughout the pandemic, clinicians were concerned about individuals with MD as they can have impaired cardio-pulmonary function which has been reported to increase the risk of morbidity and mortality associated with COVID-19 [2, 9]. Although we are not able to capture the mortality associated with COVID-19 using the current survey, we noted that individuals who completed the survey on behalf of a family member either did not indicate if the person with MD died from COVID-19, or they did not complete the survey because the person was deceased. Nevertheless, the reported hospitalizations, medical acuity and reported recovery from the virus does not suggest that respondents with MD who had COVID-19 suffered more frequently from serious complications as a result of the virus. Even for those who were considered to be at greater risk of mortality and morbidity [2, 10], the majority reported that they were not medically impacted (i.e., did not require hospitalization or did not lose care) and had a recovery period of less than two weeks. There were minimal hospitalizations reported, and only one respondent reported requiring respiratory support.
We also found that race and ethnicity were not high-risk factors in our study population as has been reported in the general population [11]. However, this may be due to the small numbers in our sample as only 6.7% reported being non-Caucasian and 4.7% reported as Hispanic/Latino.
The social strategies employed to reduce the spread of COVID-19, challenges due to the pandemic and social distancing, and research participation reported by participants at the second time point were similar to our findings at the beginning of the pandemic [4].
Despite our concern that individuals with MD would report higher stress levels due to physical limitations, possible reduction of caregiving and medical treatment, and higher risk for poor outcomes if infected with COVID-19, participants reported moderate stress levels early in the pandemic. Moderate stress levels were also reported at this later time point. Similar to the previous findings, women and those under the age of 30 years reported higher levels of stress. This finding continues to be consistent with reports in the general public where young adults (ages 18 to 24) experienced several pandemic-related consequences, such as changes in their college education status, loss of income, and poor mental health [12, 13].
Managing stress continued to be one of the biggest challenges reported by individuals with MD. However, similarly to our earlier findings, 86% of study participants report they have been able to manage their stress. Interestingly, study participants reported different stress management techniques than those previously reported even when the most frequently-cited challenges were the same at each of the two time points. At the year one time point, participants reported maintaining a routine, faith, and connecting with family and friends versus sleep/rest and exercise as reported earlier in the pandemic [4]. The time point of this survey was after vaccines were developed, approved and administered to essential workers and older adults. This resulted in some relaxation of social guidelines and allowed many to visit with family and friends safely, which may have helped individuals manage their stress levels [13].
Individuals who reported higher levels of pain reported higher stress scores, and individuals who reported that they were able to manage their stress reported lower stress scores and lower pain levels. Additionally, those who reported exercising had significantly lower levels of stress. While these associations do not indicate a causal relationship; it still may be important for health care providers to consider pain and stress management and exercise recommendations as they care for patients with MD.
Medical care became more accessible with more individuals reporting participating in telemedicine visits (57%) than at the beginning of the pandemic (40%) [4]. Care also improved with fewer reports of visits canceled or rescheduled. The satisfaction rate with telemedicine visits was consistent with our findings from the first study [4]. However, at the year one time point, more individuals showed a preference for telemedicine visits than in the beginning of the pandemic and more individuals expressed interest in telemedicine visits being an option after the pandemic. This may be attributed to an increased level of comfort with the telemedicine technology and patients realizing the potential benefits of telehealth. Those who reported completing both surveys also reported that they were more likely to participate in research studies. While the pandemic did effect research studies though delayed or canceled visits, it did not appear to have an influence on future participation in research endeavors.
There are several limitations to this study. We did not have a control group to compare our findings to and, therefore, compared our findings to reports of the general population in the literature. The participants in this study likely learned about and accessed the survey though participation in a patient registry, which may have resulted in a biased sample. This method may have also reduced access to the survey for those who do not speak English, as the survey was only provided in English, and for those without access to technology. We did not ask participants about their medical history, which may have put them at a greater or lesser risk of COVID-19 complications, and may have biased our results, if healthier and/or less affected individuals completed our survey.
CONCLUSION
Our survey allowed us to understand the impact of the ongoing COVID-19 pandemic and social guidelines on individuals with muscular dystrophy one year into the pandemic. The participants in this study have shown a resiliency, finding coping mechanisms to manage their stress and overcome obstacles presented by the pandemic, while faring well with infection risks similar to the general population. We have been able to better understand their respective muscle diseases in a unique environment to help us continue to provide high-level care as the pandemic continues. Understanding the impact on social and medical aspects of care can guide future interventions for the muscular dystrophy community. This may present an opportunity to rethink the previously predicted risks for those with muscular dystrophy. More of the general population is vaccinated and boosted, and the COVID-19 variants are not as severe; therefore, the risk of getting COVID-19, or having severe complications from COVID-19 infection, appears to be much lower than at the beginning of the pandemic. This may allow individuals with muscular dystrophy to feel more comfortable going back to in-person care appointments, doing physical exercise or physical therapy, and socializing in-person, all of which may improve their physical and mental health.
ABBREVIATIONS
Facioscapulohumeral Muscular Dystrophy – FSHD
Limb-Girdle Muscular Dystrophy- LGMD
Muscular Dystrophy- MD
Myotonic Dystrophy- DM
Perceived Stress Scale- PSS
Standard deviation- SD
ETHICAL PUBLICATION STATEMENT
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
DISCLOSURES
KE serves as a consultant or on advisory boards, and has received consulting fees from Ionis, Biogen, Acceleron, Fulcrum, Avidity, and Dyne Therapeutics.
NJ reports grants from NINDS (R01NS104010), grants from NCATS (R21TR003184), grants from CDC (DD19-002), grants from FDA (R01FD006071), grants from Muscular Dystrophy Association, grants from Myotonic Dystrophy Foundation, grants from Coalition to Cure Calpain-3, grants and personal fees from Dyne, grants and personal fees from AveXis, grants and personal fees from Vertex Pharma, grants and personal fees from Fulcrum Therapeutics, grants and personal fees from ML Bio, grants and personal fees from Sarepta, grants and personal fees from Acceleron, grants from AMO Pharma, outside the submitted work; In addition, NJ has a patent CMTHI with royalties paid, and a patent CCMDHI issued.
RT serves on advisory boards for Fulcrum Therapeutics, Roche and miRecule Biotech and is consultant for Dyne therapeutics, Arrowhead Pharma, and MT Pharma.
JS received grant support from NIH, FSHD Society, Muscular Dystrophy Association, Friends of FSH Research, and FSHD Canada. JS served as a consultant or on the advisory boards for Acceleron, Fulcrum, Dyne, Strongbridge, Sarepta, Avidity, and Genzyme.
LL, ND, KH, MW, DP, and JC report no disclosures
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JND-220794.
REFERENCES
[1] | Ohannessian R , Duong TA , Odone A . Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action, JMIR Public Health Surveill.(2020) ;6: , e18810. |
[2] | Dhont S , Callens R , Stevens D , et al. Myotonic dystrophy type 1 as a major risk factor for severe COVID-19? Acta Neurol Belg (2021) ;121: , 1761–5. |
[3] | COVID-19 Resources Accessed August 17 2021 https://www.mda.org/covid19. |
[4] | Eichinger K , Lewis L , Dilek N , et al. A patient-focused survey to assess the effects of the COVID-19 pandemic and social guidelines on people with muscular dystrophy, Muscle Nerve (2021) ;64: , 321–7. |
[5] | Harris PA , Taylor R , Thielke R , Payne J , Gonzalez N , Conde JG . ,Research electronic data capture (REDCap): A metadata-drivenmethodology and workflow process for providing translationalresearch informatics support, J Biomed Inform (2009) ;42: (2), 377–81. |
[6] | Cohen S , Kamarck T , Mermelstein R . A global measure of perceived stress, J Health Soc Behav (1983) ;24: , 385–96. |
[7] | Hinkle DE , Wiersma W , Jurs SG . Applied Statistics for the Behavioral Sciences. 5th ed. Houghton Mifflin: Boston, (2003) . |
[8] | Cohen S . Perceived Stress Scale. Mind Garden. http://www.mindgarden.com/documents/PerceivedStressScale.pdf.Accessed April 7, 2020 . |
[9] | Phelps M , Christensen DM , Gerds T , et al. Cardiovascular comorbidities as predictors for severe COVID-19 infection or death, Eur Heart J Qual Care Clin Outcomes (2021) ;7: , 172–80. |
[10] | Mueller AL , McNamara MS , Sinclair DA . Why does COVID-19 disproportionately affect older people? Aging (Albany NY) (2020) 12: , 9959–81. |
[11] | Magesh S , John D , Li WT , et al. Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status: A Systematic-Review and Meta-analysis, JAMA Network Open (2134) ;4: , e2134147–e2134147. |
[12] | Hamel L , Salganicoff A . Is There a Widening Gender Gap in Coronavirus Stress. https://www.kff.org/coronaviruspolicy-watch/is-there-widening-gender-gap-in-coronavirus-stress. Accessed August 17, 2021. |
[13] | Mental Health https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm.Accessed August 17, 2021. |


