Proceedings of the 13th International Newborn Brain Conference: Neonatal Neurocritical Care, Seizures, and Continuous EEG monitoring
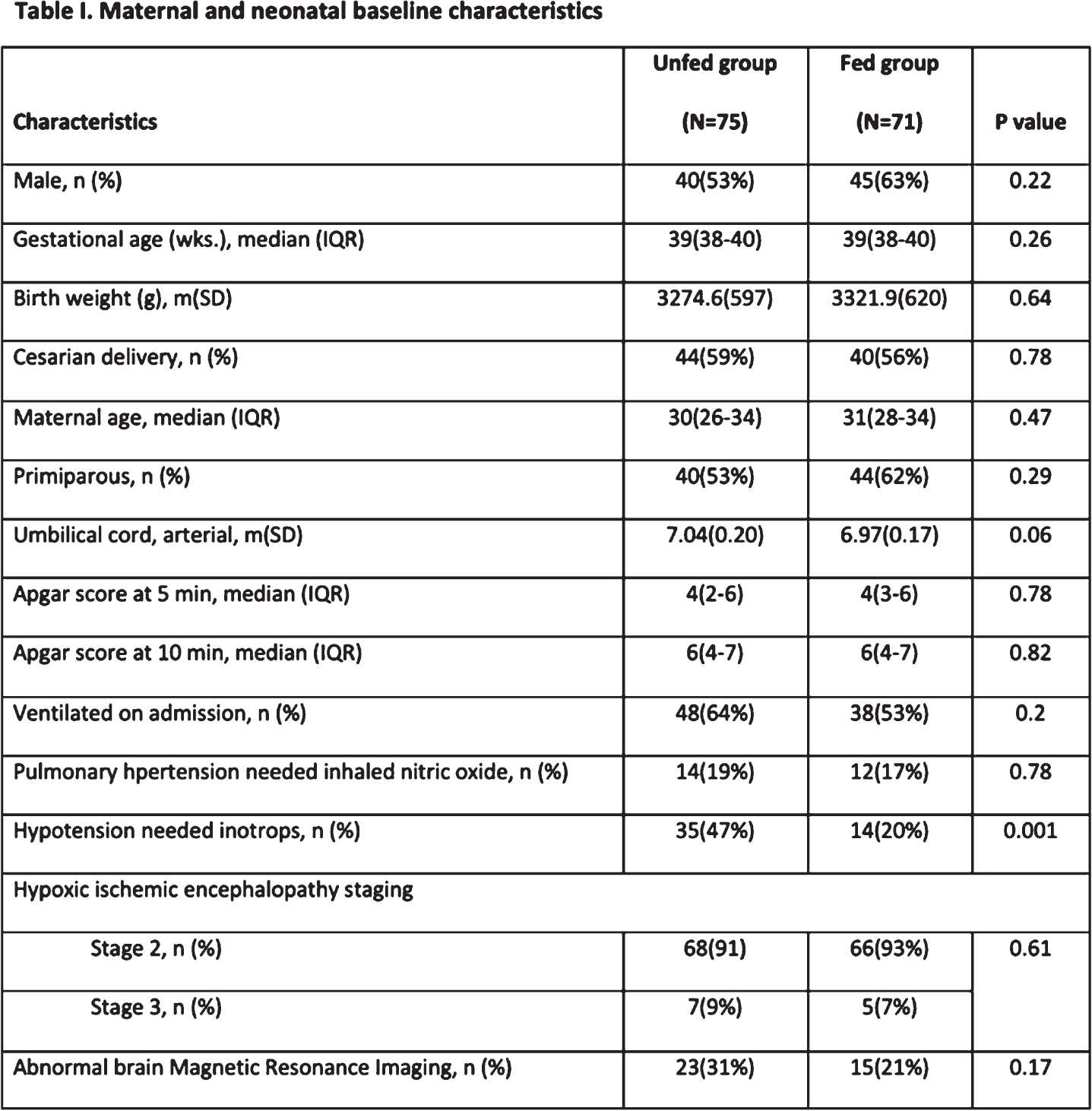
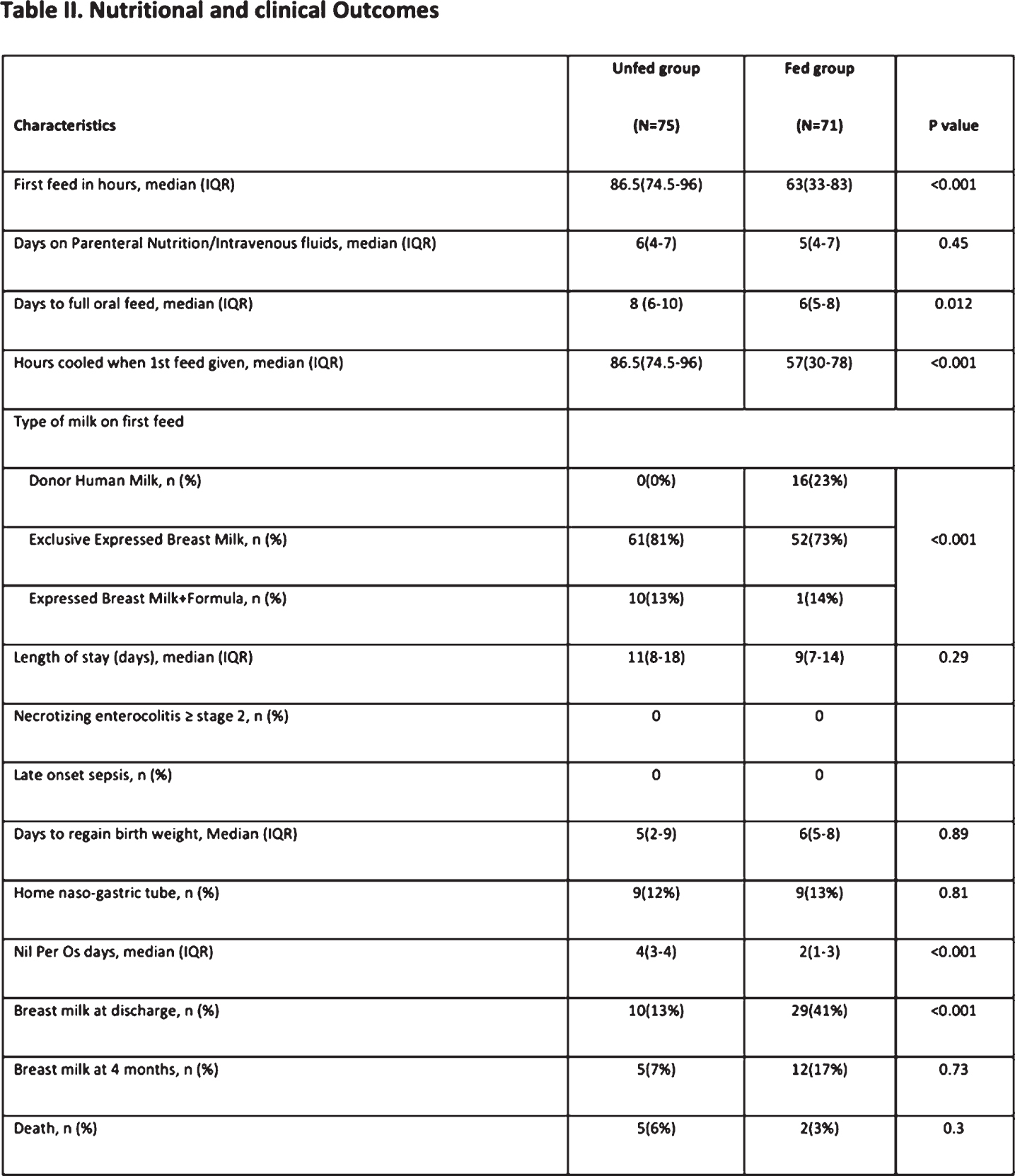
Feeding during therapeutic hypothermia is safe and may improve outcomes in newborns with perinatal asphyxia
Alburaki Wa,b, Scringer-Wilkes Mc, Dawoud Fc, Oliver Nc, Lind Jc, Zein Hc,d, Leijser Lc,d, Esser Mc,d, Mohammad Kc,d
aHorizon Health Network, Saint John, Canada
bDalhousie and Memorial Universities, Saint John, Canada
cAlberta Health Services, Calgary, Canada
dUniversity of Calgary, Calgary, Canada
OBJECTIVE: We assessed the impact of early enteral feeding introduction during therapeutic hypothermia on time to reach full enteral feeding (FEF) and other feeding related outcomes in infants born at =35 weeks gestational age and diagnosed with moderate to severe Hypoxic-Ischemic Encephalopathy.
METHODS: A prospective cohort with historical control study, conducted on infants admitted at the Alberta Children’s Hospital level III NICU in Calgary between January 2013 and December 2018.
Infants were divided into 2 groups: 1) unfed group (UG), which was kept nil per os during the 72 hours of therapeutic Hypothermia (TH), with subsequent introduction of feeding and gradual increase to FEF; 2) fed group (FG), which received feeding at 10 mL/kg/day during TH then increased gradually to FEF. Groups were compared for time to FEF and the type of milk they were being fed on discharge. Other gut related health risks such as NEC and sepsis were examined.
RESULTS: During the study period, 146 infants received therapeutic hypothermia, of whom 75 in the UG and 71 in the FG. The FG compared to the UG received the first feed sooner after TH initiation (median 57 hours vs. 86.5 hours, p<0.001), reached FEF earlier (median 6 days vs. 8 days, p=0.012), was kept NPO for shorter duration (median 2 days vs. 4 days, p<0.001), and had a higher rate of breast milk feeding at discharge (41% vs. 13%, p<0.001). There were no cases of necrotizing enterocolitis or late onset sepsis in either group during the hospital stay.
CONCLUSION: Minimal enteral feeding during therapeutic hypothermia appears to be safe and leads to a shorter time to FEF and higher rates of breast milk feeding at discharge.
Quantitative EEG features of quiet and active sleep in late preterm and full-term newborns
Cubero-Rego La, Ricardo-Garcell J, Harmony Baillet T, Corsi-Cabrera M
aUnidad De Investigación en Neurodesarrollo, Instituto De Neurobiología, Unam, Campus UNAM 3001, 76230 Juriquilla, Qro., Mexico
BACKGROUND: Preterm infants benefit from receiving early neuro habilitation, but it is difficult to decide clinically who really needs the treatment. Magnetic resonance imaging is the most sensitive exam, but it is not always available at term age. The electroencephalogram (EEG) is a more accessible, non-invasive method that, with adequate quantitative analyzes, can provide valuable information on the neonatal brain maturation. Spectral analysis of quiet (QS) and active (AS) sleep (future NREM and REM sleep stages, respectively) offers an objective method for characterizing the evolution of EEG differences between these two stages in newborns during the first month of life, when EEG patterns and brain development are rapidly changing. However, current studies use the same broad bands defined for awake adult humans, that may not be applicable to sleeping neonates.
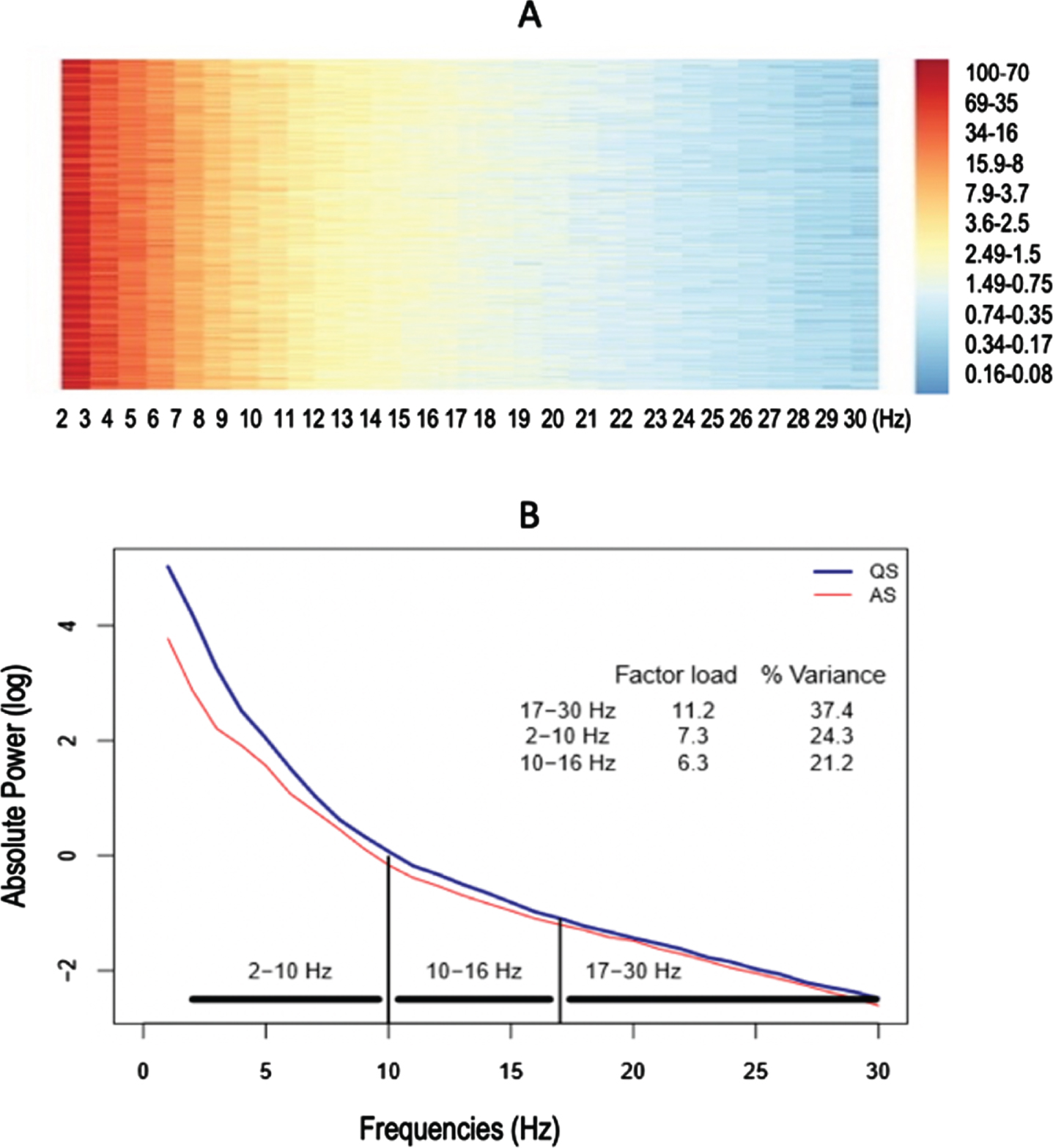
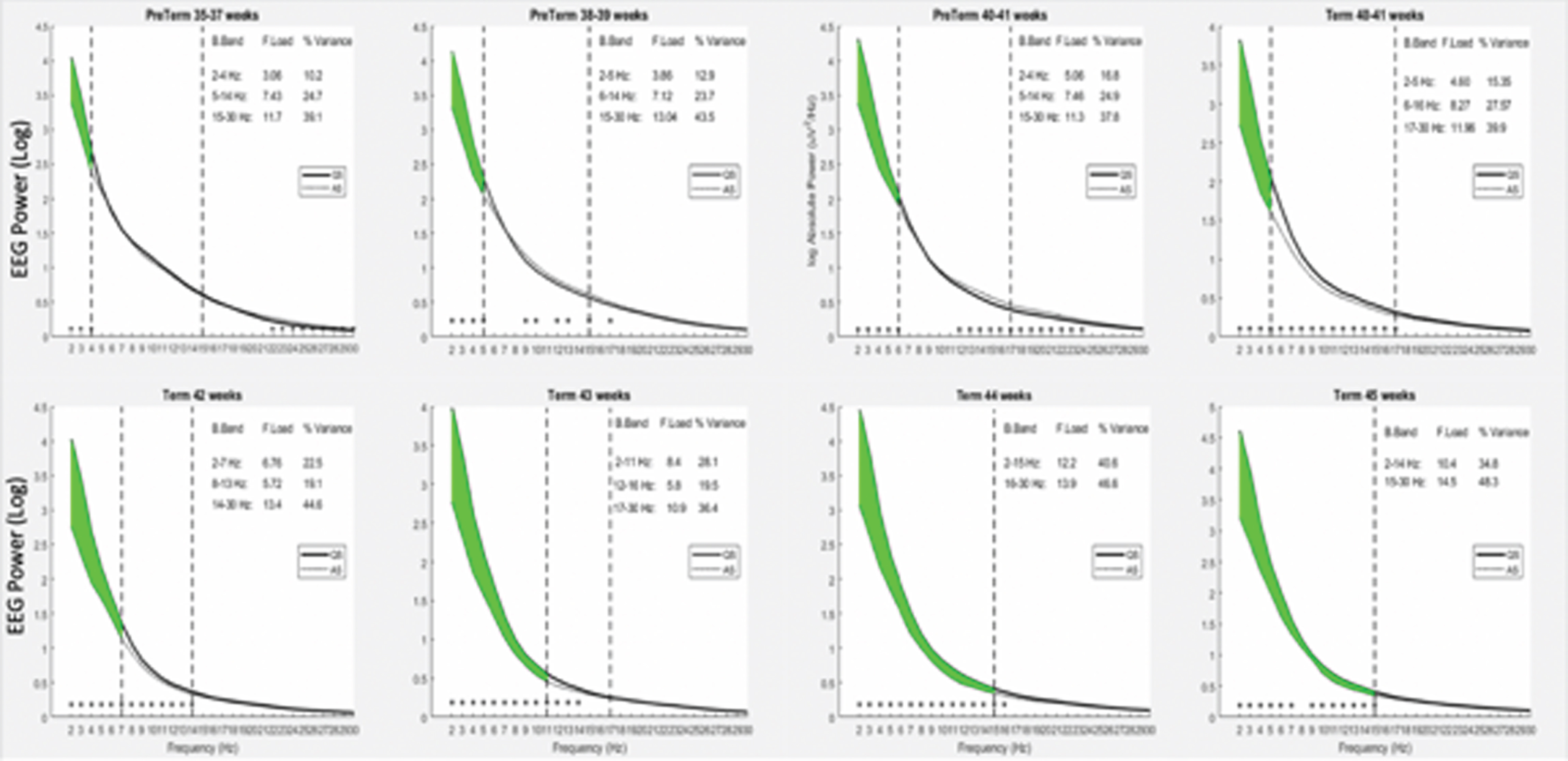
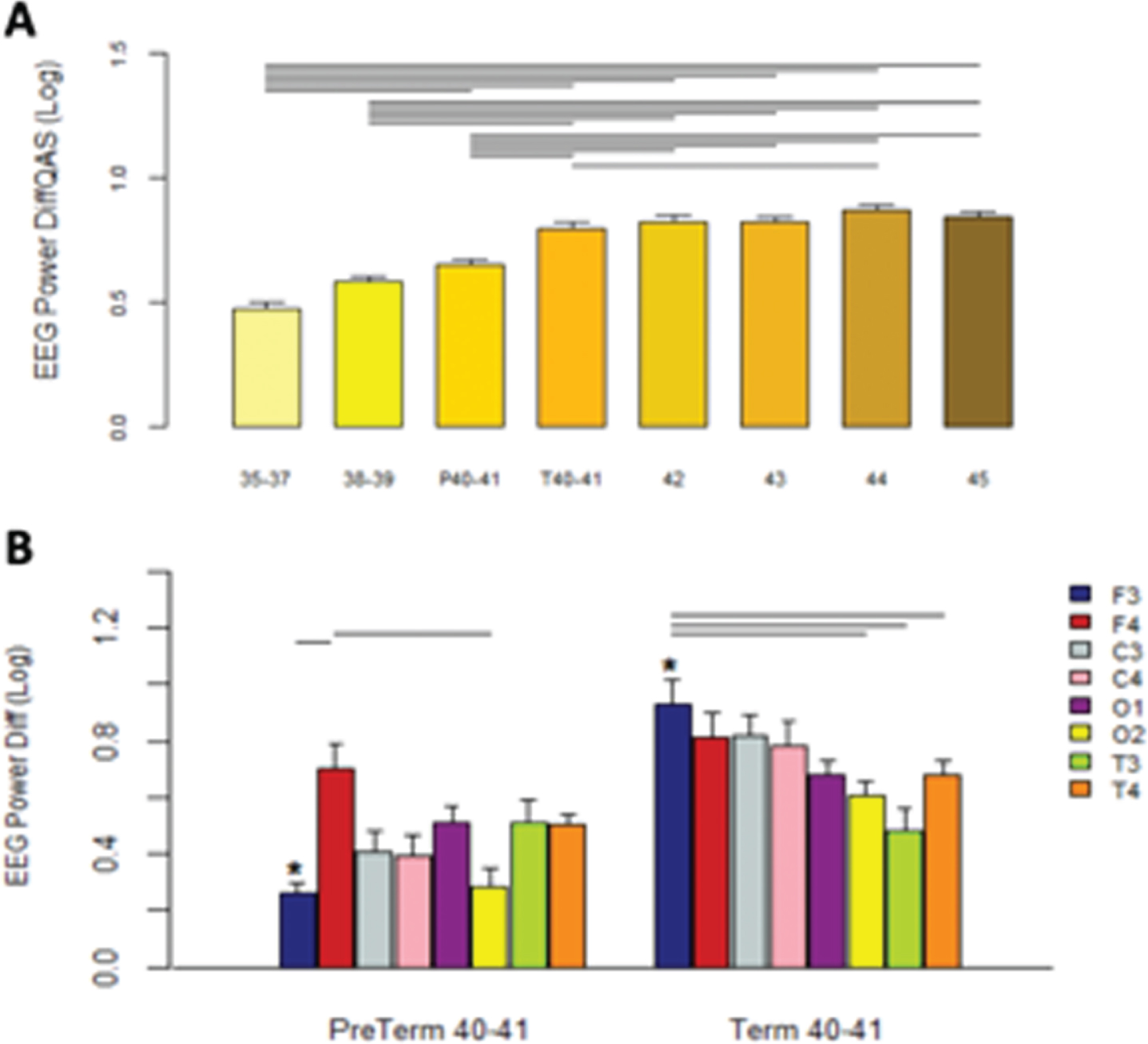
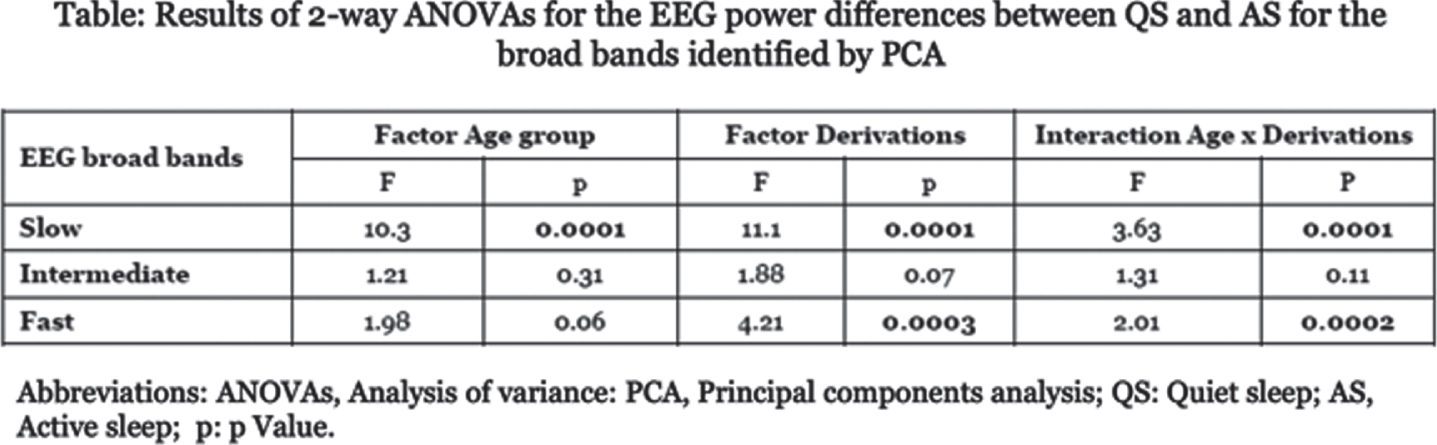
OBJECTIVE: To describe the spectral EEG differentiation in QS and AS in late preterm and in full-term healthy newborns, with the hypothesis that there will be differences in EEG absolute power (AP) between both groups. METHODS. Spontaneous sleep from 96 newborns was studied with polysomnography for 60 minutes. The obtained EEGs were subjected to spectral analysis and principal component analysis (PCA) to extract independent broad bands. The newborns were separated into eight groups (n=12 each): Pret35-37, Pret38-39, Pret40-41, Term40-41, Term42, Term43, Term44 and Term45 weeks PMA at the time of the sleep recordings. Absolute power of QS and AS in the narrow bands (1-Hz bins) and of PCA broad bands were compared, using Student-t tests between QS and AS, and mixed ANOVAs for the difference between QS and AS, with age and EEG derivations as factors.
RESULTS: PCA rendered three independent broad bands, distinct from conventional EEG bands. They explained 82.8% of variance and covered the following frequency ranges: 2–10 Hz, 10–16 Hz, and 17–30 Hz. ANOVAs (group × age × derivations) showed significant higher power at 2–10 Hz with greater age, and higher power in QS than AS in all three bands. The higher EEG power in QS than AS began at 2-4 Hz in Pret35-37 and included progressively faster frequencies each week. The planned comparisons between Pret40-41 vs Term40-41 showed that the AP difference at F3 was significantly lower in the preterm group, which showed asymmetries between F3 and F4 derivations, with significantly higher EEG power in F4 than F3 and O2. In the Term40-41 group, the significant AP differences were symmetrical and predominated bilaterally in the frontal and central regions, covering a larger area.
CONCLUSION: These results show that spectral analysis of EEG provides new insights on sleep EEG maturation, improving our understanding of EEG development during the first postnatal month, and can detect functional brain differences between preterm and full-term newborns.
Myers MM (2012) Clin-Neurophysiol 123:1502-1511
Quality Improvement bundled approach reduces the use of inotropes in extremely premature babies
Gurram Venkata Sa, Srivastava Aa, Murthy Pa, Scott Jb, Zein Ha, Leijser La, Ghosh Aa, Momin Sa, Thomas Sa, Mohammad Ka
aSection of Neonatology, Department of Pediatrics, University Of Calgary, Calgary, Canada
bDepartments of Diagnostic Imaging and Clinical Neurosciences, University of Calgary, Calgary, Canada
BACKGROUND: Consensus on the definition and management of hypotension in preterm neonates is lacking.(1–3) Owing to this, there are wide variations in the reported incidence of hypotension in premature infants, especially in the first week from birth.(1,3,4) Inotropes can often cause vasoconstriction, which may alter brain perfusion especially in the absence of established cerebral autoregulation.(5) The use of these drugs is associated with multiple short and long term morbidities.(2,6–12) Studies that targeted blood pressure alone as the criteria for use of inotropes did not show improvement in mortality and morbidity.(12,13) We evaluated the effect of quality improvement (QI) bundle on rate of inotrope use and associated morbidities.
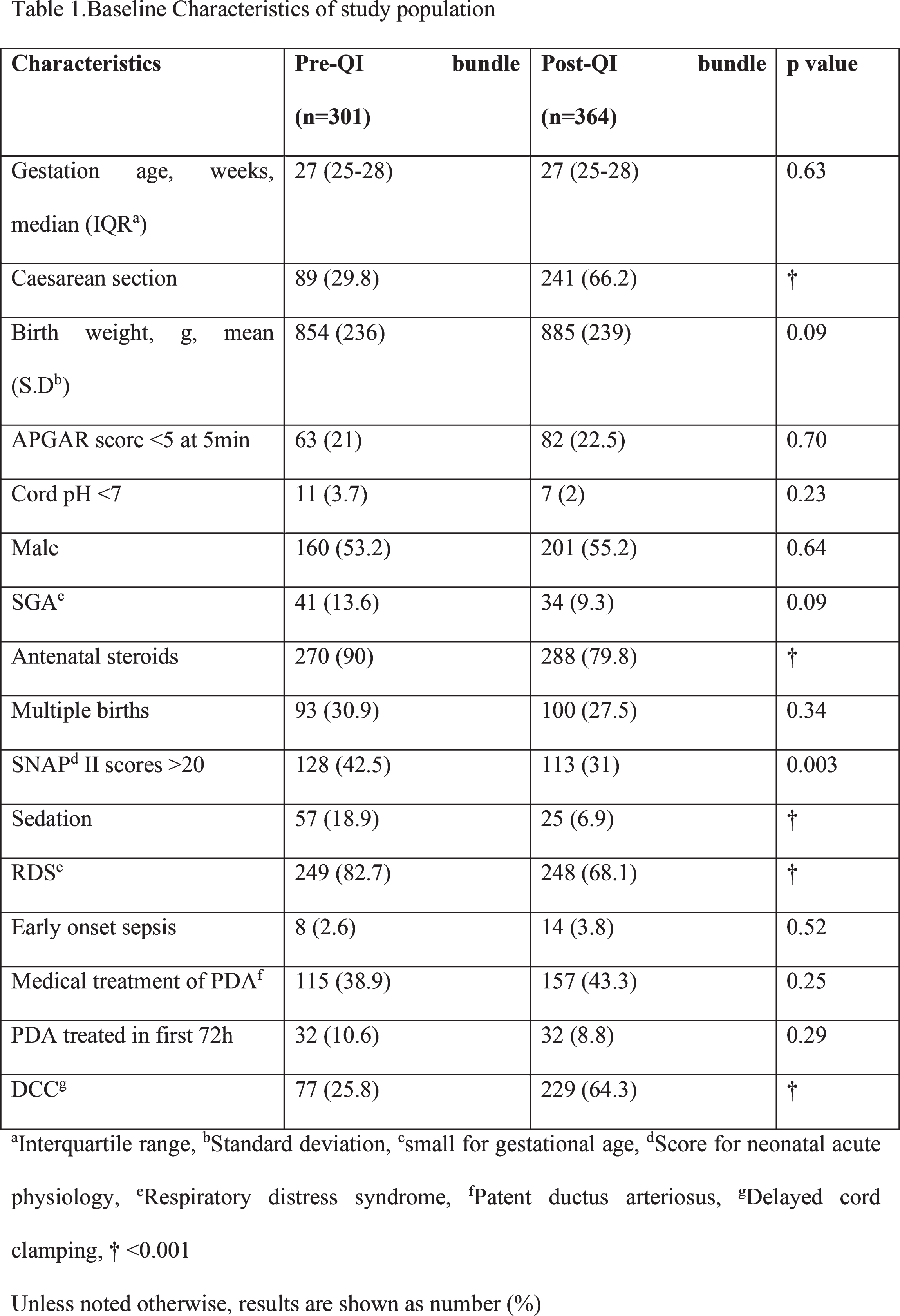
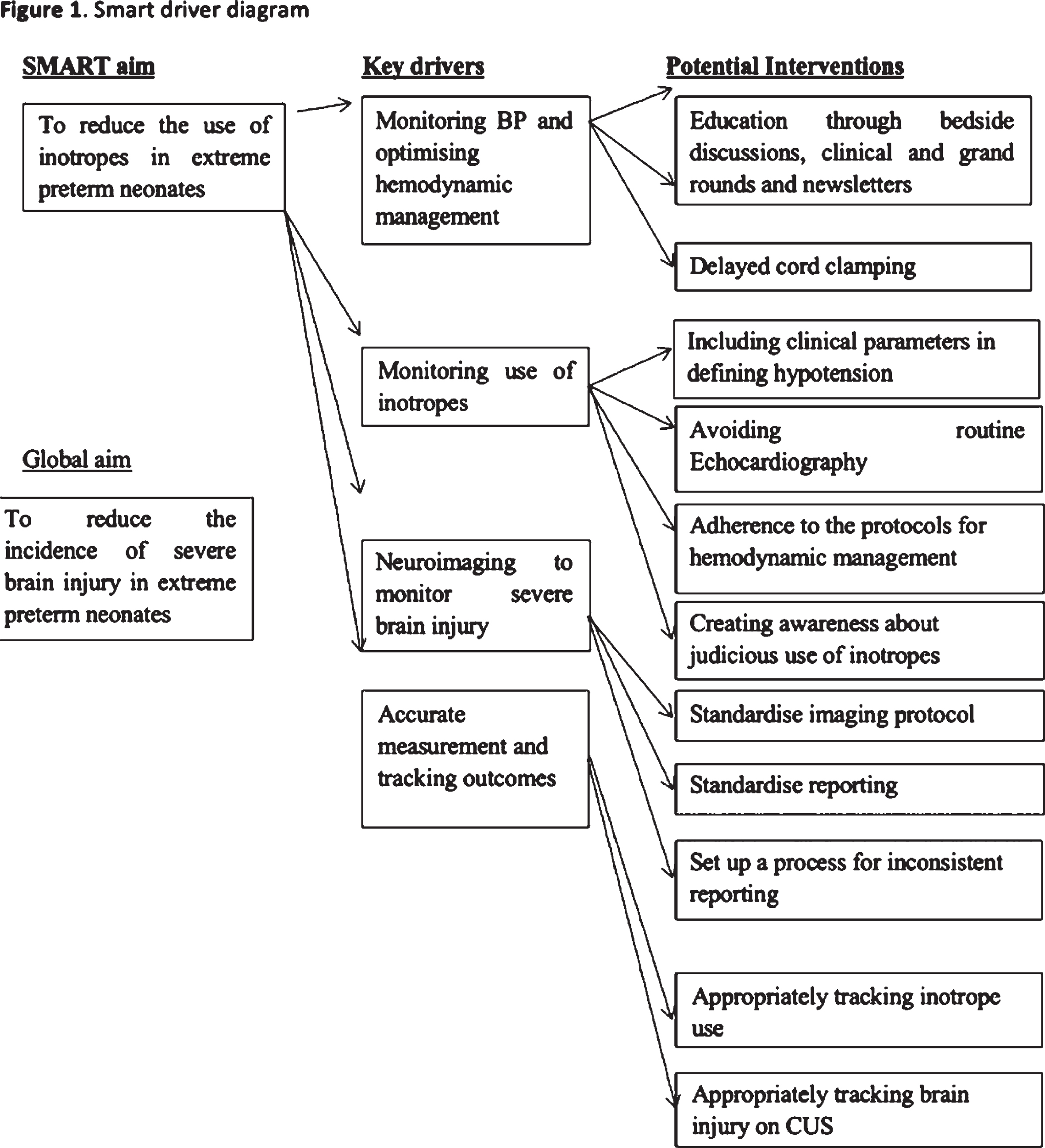
METHODS: Inborn preterm neonates born at <29weeks gestational age (GA) and admitted to level III NICU were included. Neonates with major congenital malformations, congenital heart diseases, antenatal diagnosed genetic defects, and neonates admitted after 72 hours of age were excluded from the study. We implemented a QI bundle (Figure 1) focussing on first 72hours from birth which included delayed cord clamping, avoidance of routine echocardiography, addition of clinical criteria to the definition of hypotension, factoring iatrogenic causes of hypotension (ruling out lung hyperinflation), and standardization of respiratory management. Rate of use of inotropes in the first 72hours of life along with acute brain injury and mortality before and after implementation of the QI bundle were compared. The balancing measure was the rate of ischemic lesions in the form of cPVL. Cranial ultrasound was performed to screen for brain injury and was reported based on an evidence-based reporting system.(14–17) University of Calgary Conjoint Health Research Ethics Board approved the QI project and waived the need for parental consent. (REB14-1466)
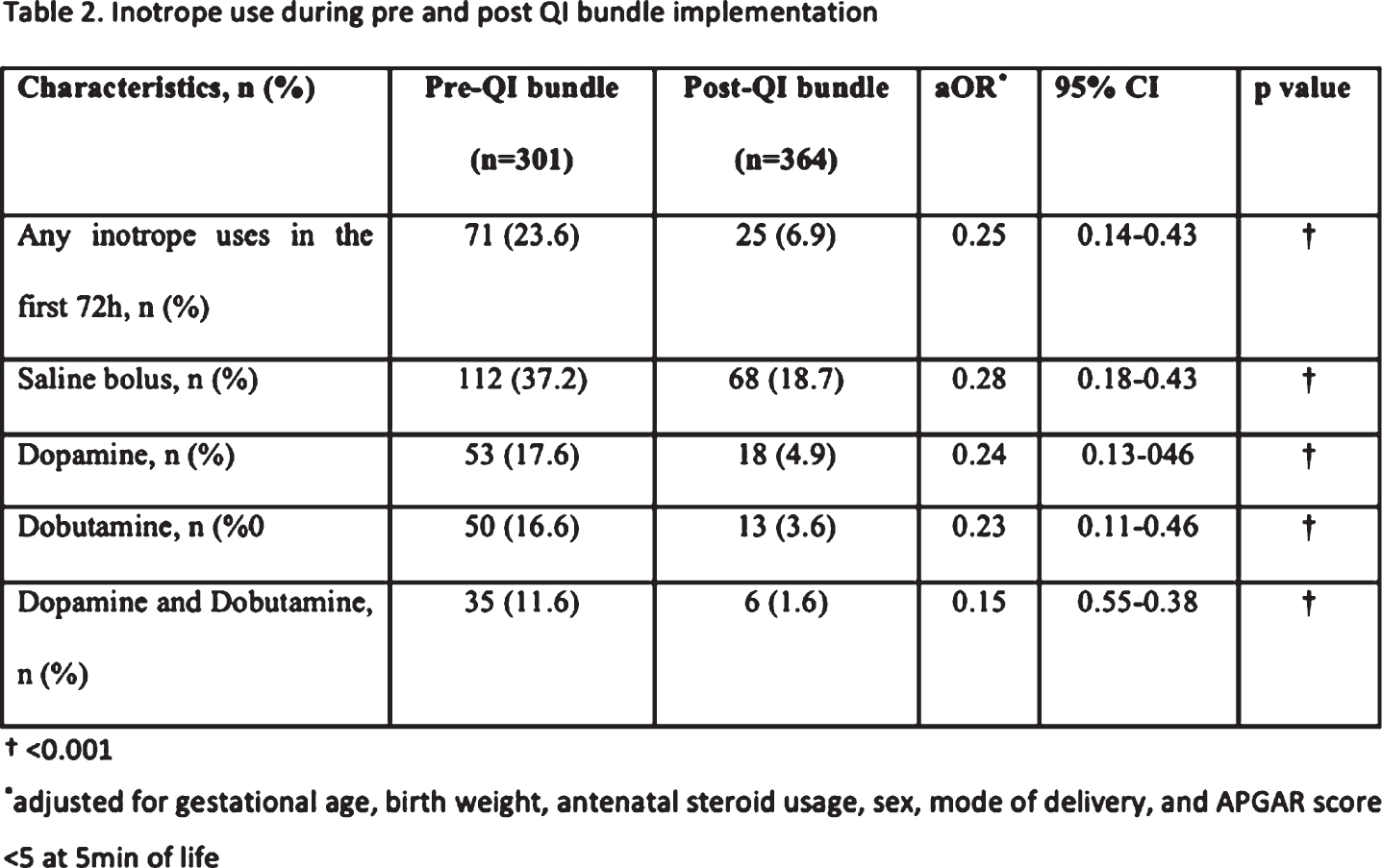
RESULTS: We included 671 neonates (301 before and 364 after the implementation of the bundle) among which 6 neonates were excluded based on the criteria. QI bundle implementation was associated with significant reduction in overall use of inotropes (24% vs 7%, p<0.001), dopamine (18% vs 5%, p<0.001), and dobutamine (17% vs 4%, p<0.001). Rate of acute brain injury decreased significantly: Acute brain injury of any grade (34% vs 20%, p<0.001) and severe brain injury (15% vs 6%, p<0.001). There was no difference in incidence of cPVL (1% vs 1.4%, p=0.66). Associations remained significant after adjusting for confounding factors. The QI bundle implementation was associated with a significant reduction in the use of inotropes when analyzed based on the 6 monthly time intervals (p = 0.006) (Figure 2)
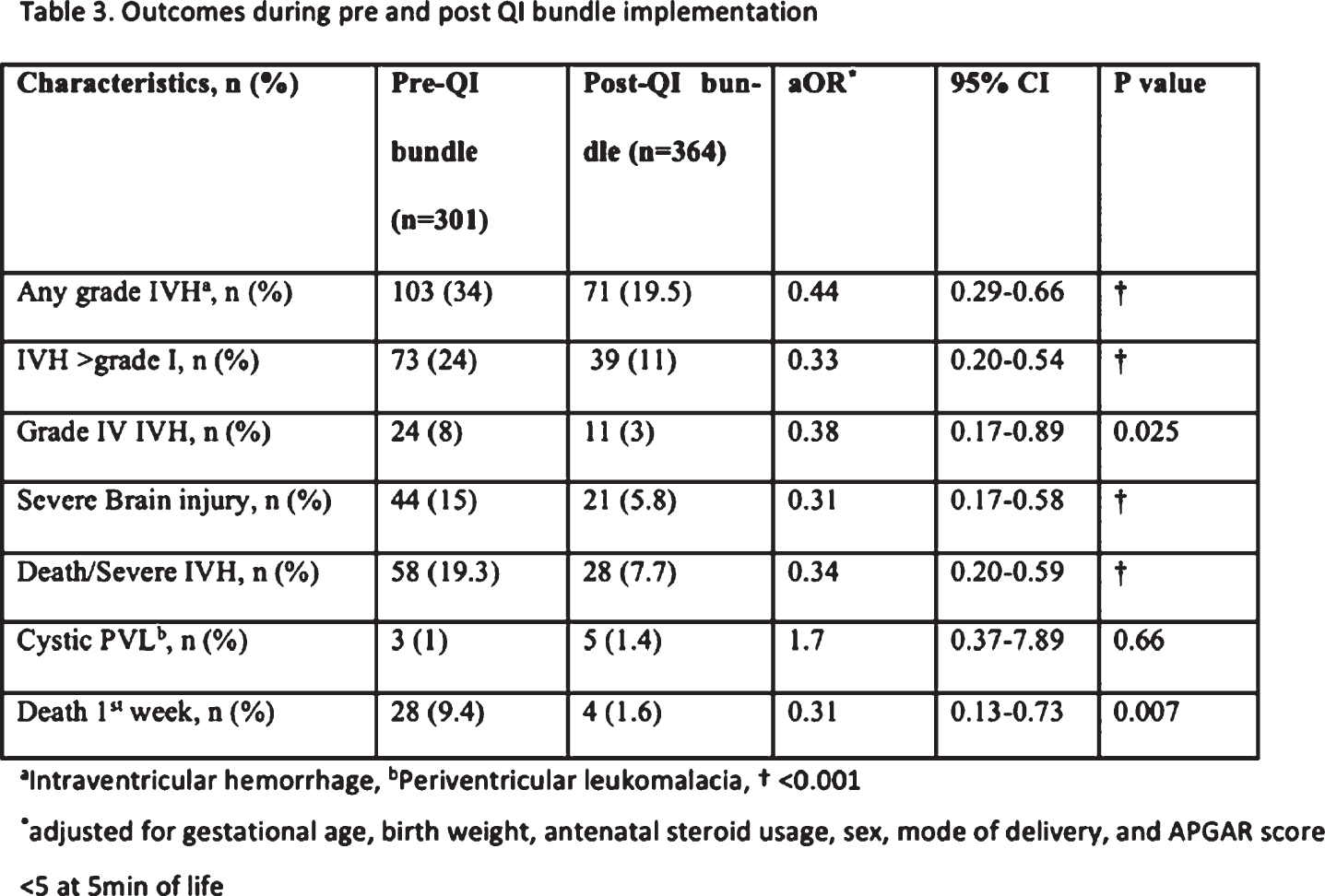
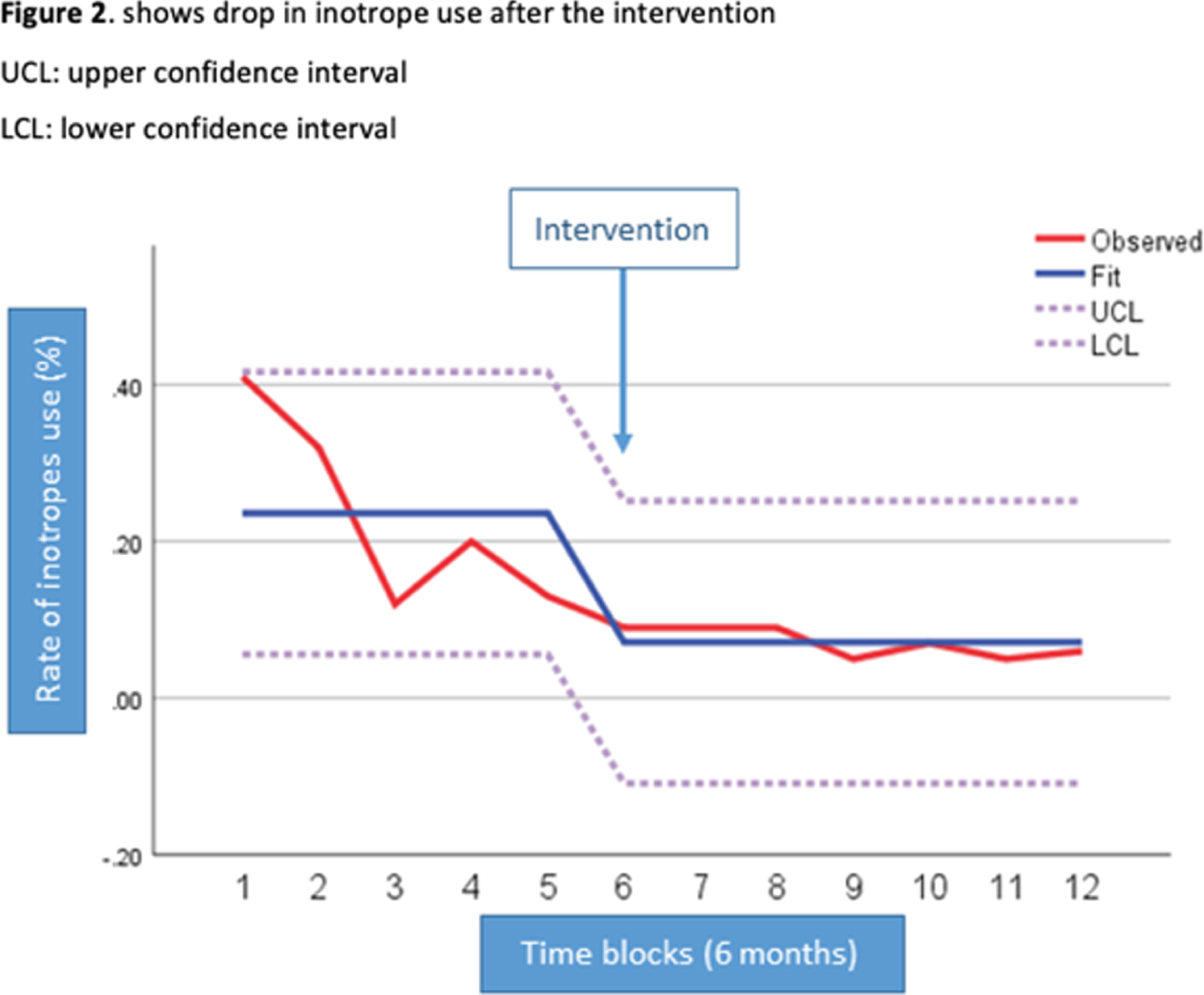
CONCLUSIONS: Our Quality Improvement bundled approach resulted in reduction in inotrope use and associated brain morbidities in premature babies. Follow-up studies evaluating the impact of this initiative on long-term outcomes in survivors are required to complement findings of improved short-term outcomes seen in this study.
Seizure severity and treatment response in term and preterm neonates with seizures attributed to intracranial hemorrhage
Herzberg Ea, Machie Mb, Glass Hc, Shellhaas Rd, Wusthoff Ce, Chang Tf, Abend Ng, Chu Ch, Cilio Mi, Bonifacio Sj, Massey Sg, McCulloch Ck, Soul Jl
aDivision of Newborn Medicine, Department of Pediatrics, Massachusetts General Hospital, Boston, United States
bDepartments of Neurology and Pediatrics, University of Texas Southwestern Medical Center, Dallas, United States
cDepartment of Neurology and Weill Institute for Neuroscience, University of California, San Francisco; Department of Pediatrics, Benioff Children’s Hospital, University of California, San Francisco, San Francisco, United States
dDepartment of Pediatrics, University of Michigan, Ann Arbor, United States
eDepartments of Neurology & Pediatrics, Stanford University, Palo Alto, United States
fDepartment of Neurology, Children’s National Hospital, George Washington University School of Medicine, Washington, United States
gDepartments of Neurology and Pediatrics, Children’s Hospital of Philadelphia and Perelman School of Medicine at the University of Pennsylvania, Philadelphia, United States
hDepartment of Neurology, Massachusetts General Hospital, Boston, United States
iDivision of Pediatric Neurology, Department of Pediatrics, Saint-Luc University Hospital, Université Catholique de Louvain, Brussels, Belgium
jDivision of Neonatal and Developmental Medicine, Department of Pediatrics, Stanford University, Palo Alto, United States
kDepartment of Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, United States
lDepartment of Neurology, Boston Children’s Hospital, Boston, United States
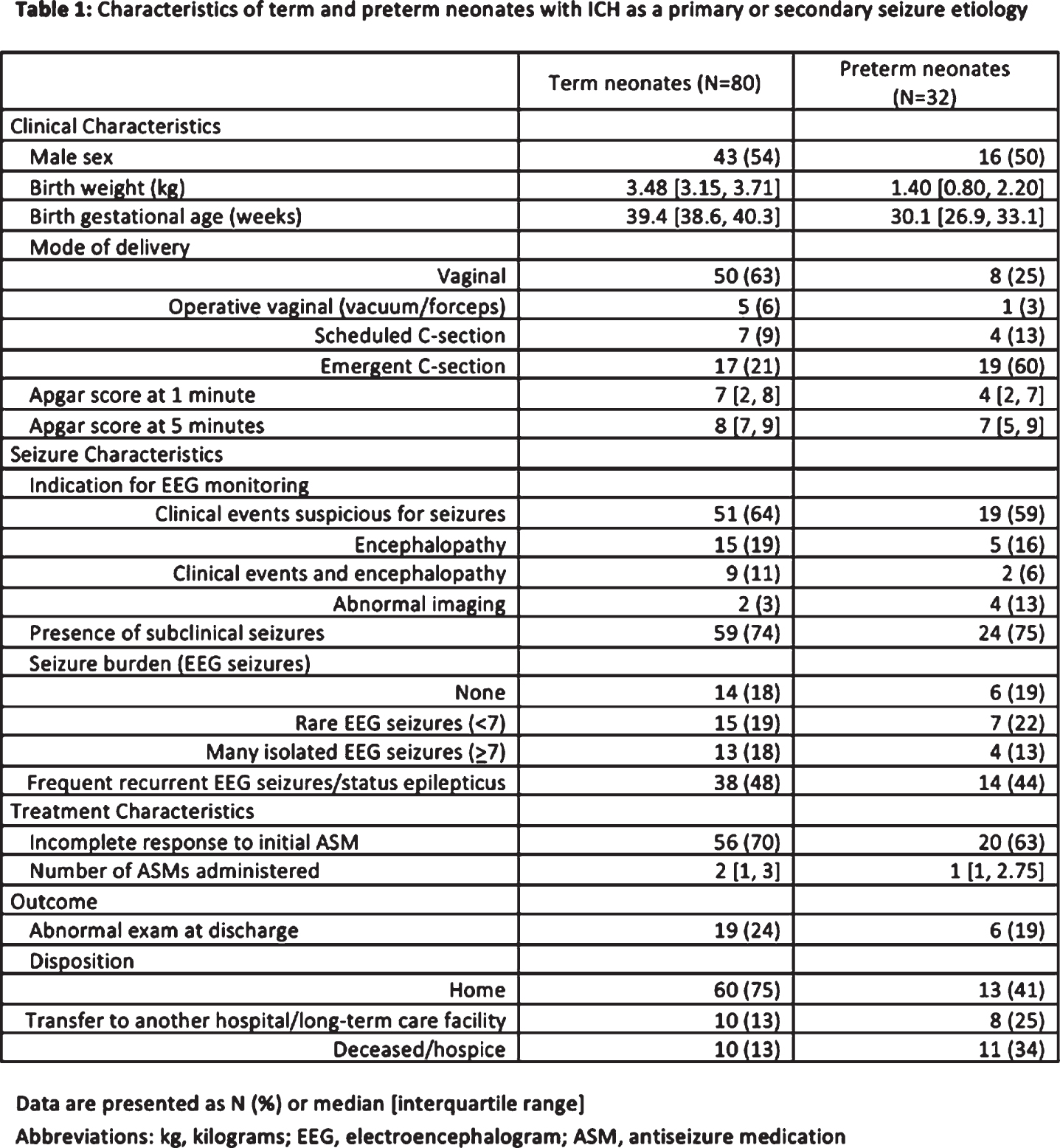
BACKGROUND: Intracranial hemorrhage (ICH) is a common etiology of neonatal seizures; however, types and sites of ICH contributing to seizures have not been studied in detail(1). We aimed to characterize ICH as a seizure etiology in term and preterm neonates and to compare seizure severity and treatment response. We hypothesized that neonates with multi-site ICH or ICH complicating HIE would have higher seizure severity and less response to antiseizure medication (ASM).
STUDY DESIGN/METHODS: We included 112 neonates with seizures attributed to ICH and 201 term neonates with seizures attributed to HIE, from a cohort of consecutive neonates with clinically diagnosed and/or electrographic seizures prospectively enrolled in the multicenter Neonatal Seizure Registry from 1/2013-11/2015. All neonates had continuous video electroencephalogram (cvEEG) monitoring. Data were analyzed using Student’s t-test, Pearson’s Chi-Square, and Fisher’s Exact test.
RESULTS: ICH was a more common seizure etiology in preterm vs. term neonates (27% vs. 10%, p<0.001). The most common sites of ICH were parenchymal hemorrhage (44% in preterm, 46% in term neonates, p=0.84) and intraventricular hemorrhage (IVH), with IVH occurring more frequently in preterm compared with term neonates (53% vs. 30%, p=0.03, Figure 1). Similarly, IVH with periventricular hemorrhagic infarction (PVHI) was more common among preterm (38%) vs. term neonates (9%, p=0.001). More preterm than term neonates had cvEEG monitoring initiated for high-risk clinical scenarios (encephalopathy or abnormal imaging), than for suspected seizures (32% vs. 19%, p=0.26). Most neonates with ICH had subclinical seizures (74%) and an incomplete response to initial ASM (68%) (Table 1). More term neonates with multi-site vs. single site ICH had subclinical seizures (93% vs. 66%, p=0.05, Table 2) and an incomplete response to initial ASM (100% vs. 66%, p=0.02). Status epilepticus was more common in term neonates with HIE and ICH vs. HIE alone (38% vs. 17%, p=0.05, Table 3).
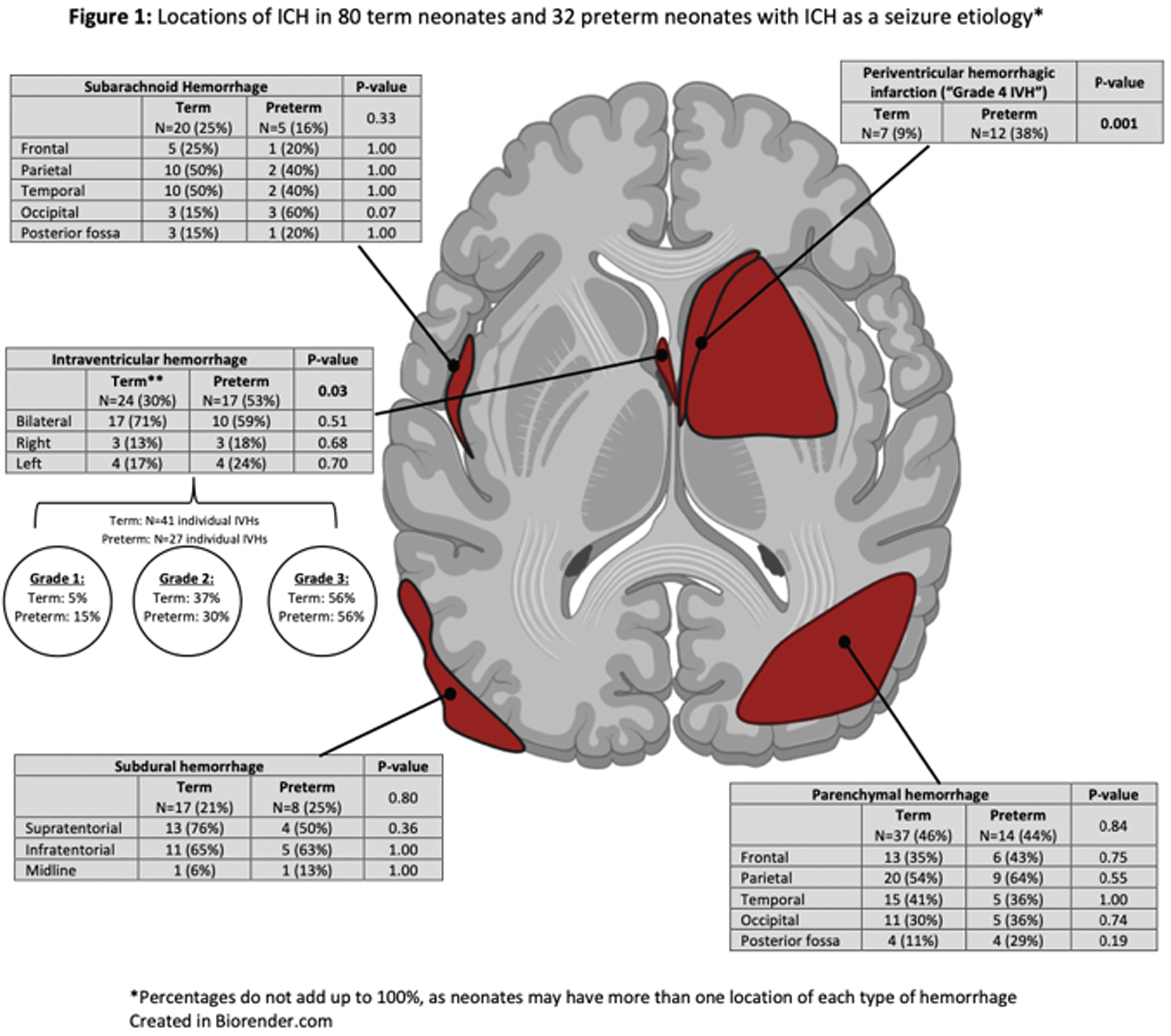
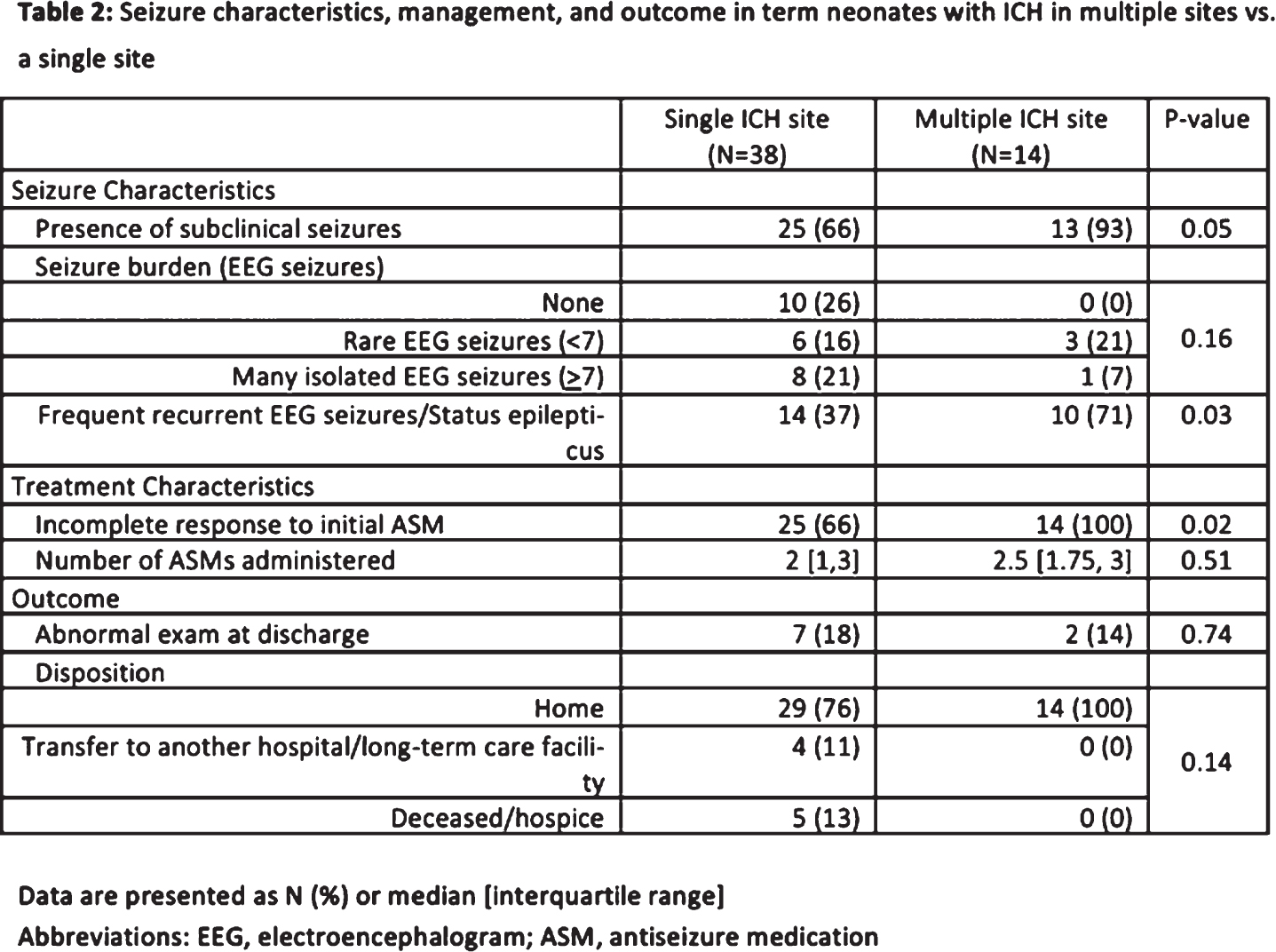
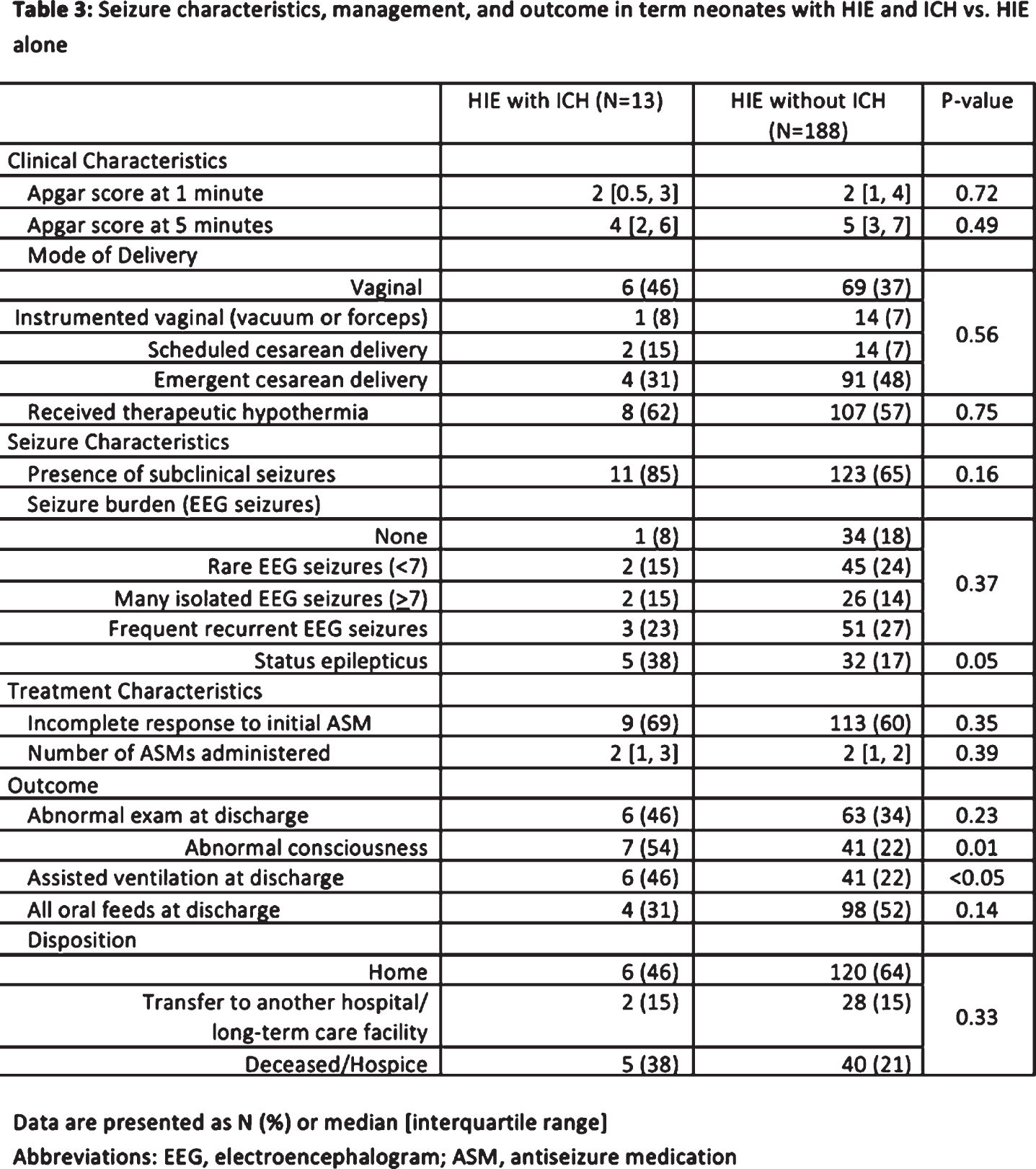
CONCLUSION/IMPACT: Neonates with seizures attributed to ICH most commonly had cerebral parenchymal hemorrhage or IVH. Seizure severity was higher and treatment response was lower among term neonates with complicated ICH, supporting the use of screening cvEEG to detect seizures in neonates with multi-site ICH or HIE with ICH. Secondly, ICH was a more common seizure etiology in preterm than term neonates, largely related to IVH±PVHI. These data support the use of screening cvEEG to detect seizures in preterm infants with ICH, as about one-third of high-risk preterm neonates with encephalopathy/abnormal imaging had EEG-seizures despite a lack of clinically-suspected seizures. Screening cvEEG in these high-risk neonates may increase the odds of successful seizure control(2).
Bibliography:
[1] Glass HC, et al. Contemporary profile of seizures in neonates: a prospective cohort study. J Pediatr. 2016;174:98-103.e1.
[2] Wusthoff CJ, et al. Seizure Control in Neonates Undergoing Screening vs Confirmatory EEG Monitoring. Neurology. 2021;97:e587-e596.
Factors associated with early development of GM/IVH in extremely premature infants
Hildrey Ea, Lee Sa,b, Volpe Ja,b,c, Inder Ta,b, El-Dib Ma,b
aBrigham and Women’s Hospital, Boston, United States
bHarvard Medical School, Boston, United States
cBoston Children’s Hospital, Boston, United States
BACKGROUND: Extremely low GA (ELGA; <28 weeks gestational age) infants are at the highest risk for developing a germinal matrix/intraventricular hemorrhage (GM/IVH) with adverse impact on neurodevelopmental outcome. While an early diagnosis can be achieved using cranial US (cUS) on the first day of life, (Parodi, Govaert et al. Pediatr Res, 2020) recent North American guidelines advocate for cUS screening by 7-10 days of life (Hand, Shellhaas et al. Pediatrics, 2020). In the BWH NICU we adopted a routine screening protocol for cUS in ELGA infants for days of life 1, 3 and 7. The aim of this study was to investigate the incidence of GM/IVH detection on the first day cUS along with factors associated with early versus late GM/IVH.
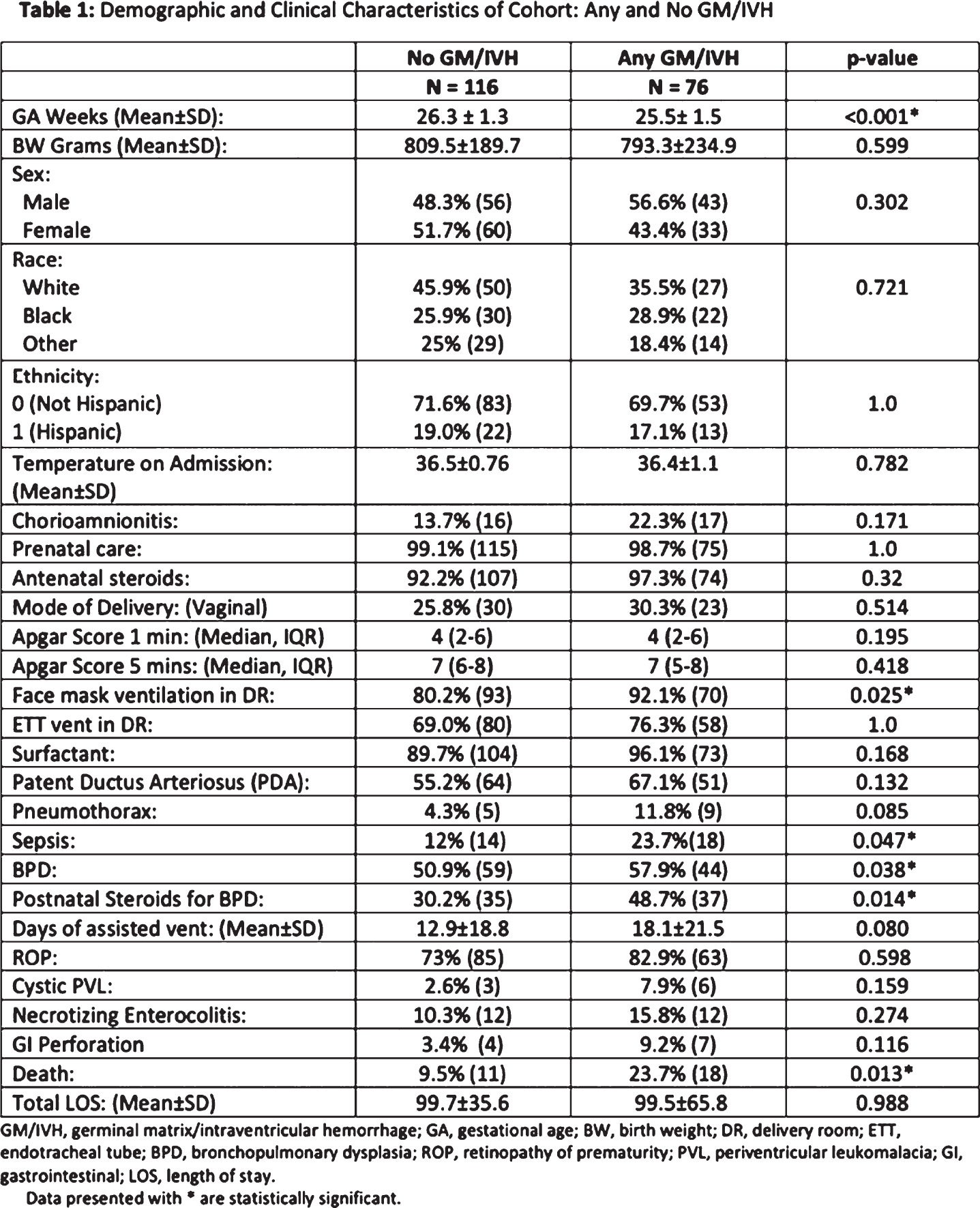
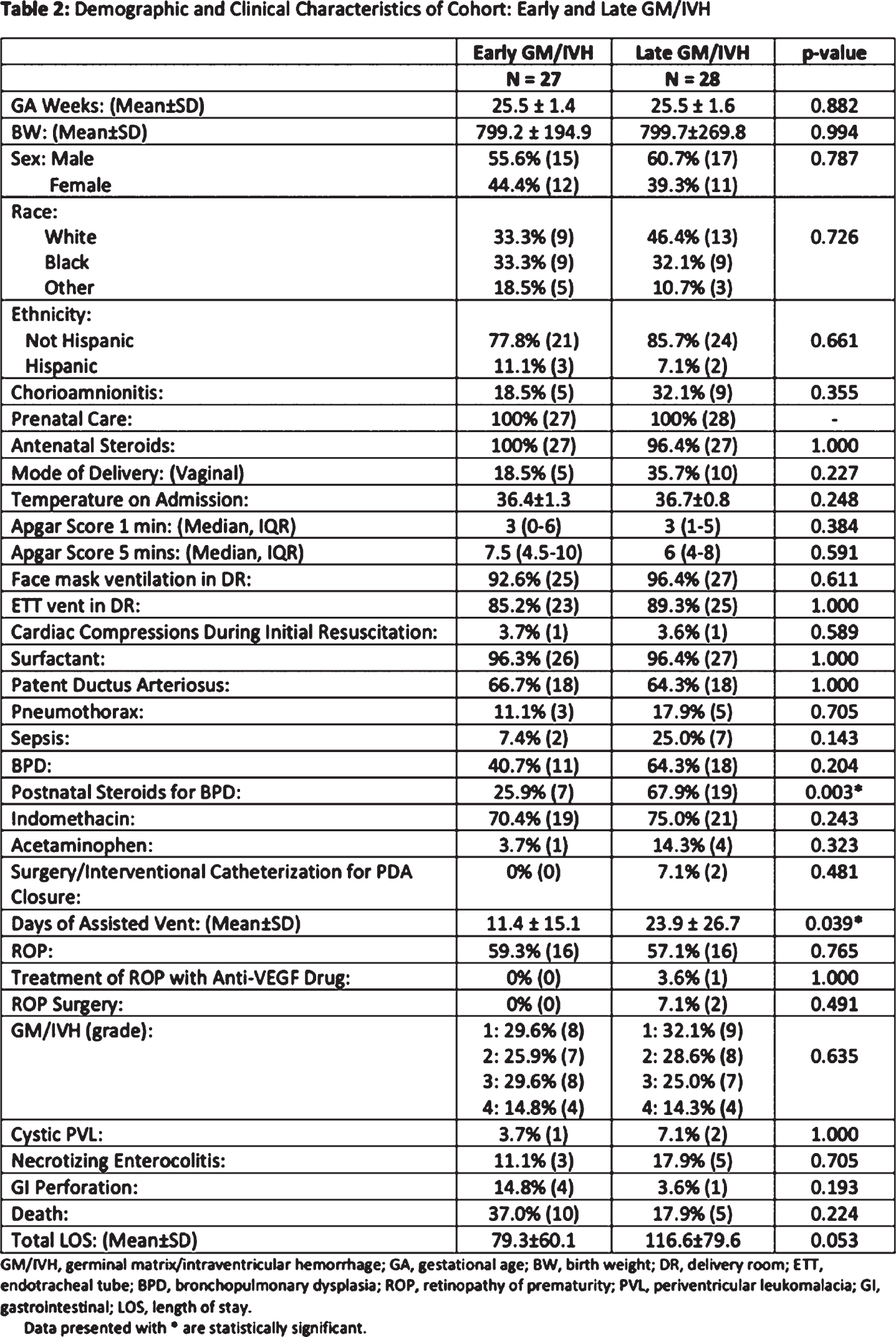
DESIGN/METHODS: Retrospective review of center data collected as part of VON Network and chart review were used. All infants (n=192) born between 23-27 weeks GA during a 5-year period (Jan 2015-Dec 2019) had their charts and cUS reports reviewed, except for those who did not receive a cUS (n=17). Infants were classified into any, or no, GM/IVH. Moreover, infants with GM/IVH who received Day 1 and Day 3 cUS were classified as early GM/IVH versus late GM/IVH. Mann Whitney U and Fisher’s exact test were performed for statistical significance.
RESULTS: During the study period, of all 192 infants, 116 (60%) had no GM/IVH and 76 (40%) had any grade of GM/IVH (24 Grade 1, 23 Grade 2, 20 Grade 3, 9 PVHI). Of those with any degree of GM/IVH, early cUS was available in 55 (72.4%). In this group, Day 1 and Day 3 cUS were completed at 19.4±8.2 and 69.3±31.3 hours respectively. Of the 55 infants who received cUS in the first day of life, 27 were diagnosed with GM/IVH (49.1%). Of those 27 infants, 17 (63%) were diagnosed with the highest GM/IVH grade at the first cUS. When compared to infants with no GM/IVH, infants who had any GM/IVH were more likely to be of lower GA, require PPV in the DR, have sepsis, BPD, postnatal steroids for BPD, and higher rates of death. When compared to infants with late GM/IVH, those with early GM/IVH did not differ on any perinatal factors but were more likely to have adverse respiratory comorbidity (postnatal steroids for BPD and greater days of assisted ventilation).
CONCLUSION(S): First day cUS allows for detection of GM/IVH in ELGA neonates in almost 50% of infants with GM/IVH. Early detection may inform subsequent clinical management, or discussion with family regarding neurodevelopmental prognosis. More information is needed to evaluate the differential effect of early GM/IVH on later neurodevelopmental outcomes.
Evolution of regional management for neonatal hypoxic ischaemic encephalopathy (HIE): Review against the British Association of Perinatal Medicine (BAPM) framework for practice
Jefferies Ka,b, Adams Ea
aOxford University Hospitals NHS Trust, Oxford, United Kingdom
bPrincess Anne Hospital, Southampton, United Kingdom
BACKGROUND AND PURPOSE: Neonatal HIE occurs in approximately 1-3.5/1000 UK births(1,2,3). Therapeutic hypothermia (TH) initiated within 6 hours of birth, lowering core temperature to 33-34°C for 72 hours, successfully reduces rates of death and disability at 18 months in infants with moderate to severe HIE(4). In 2020, BAPM published the new “Therapeutic hypothermia for Neonatal Encephalopathy framework for practice”. Accordingly, we aimed to establish whether the following key recommendations were being met across our neonatal network:
• TH for mild HIE is not recommended outside clinical trials
• All infants meeting criteria A but with normal initial neurological examinations should have serial assessments within the first 6 hours
• Special Care (SCUs) and Local Neonatal Units (LNUs) should be able to instigate TH and use amplitude integrated electroencephalogram (aEEG) to confirm treatment eligibility
• To initiate TH and reach core target temperature within 6 hours
• Infants receiving TH should undergo MRI between day 5-15 (preferably day 5-7) and a standardised neurodevelopmental assessment at 2-years.
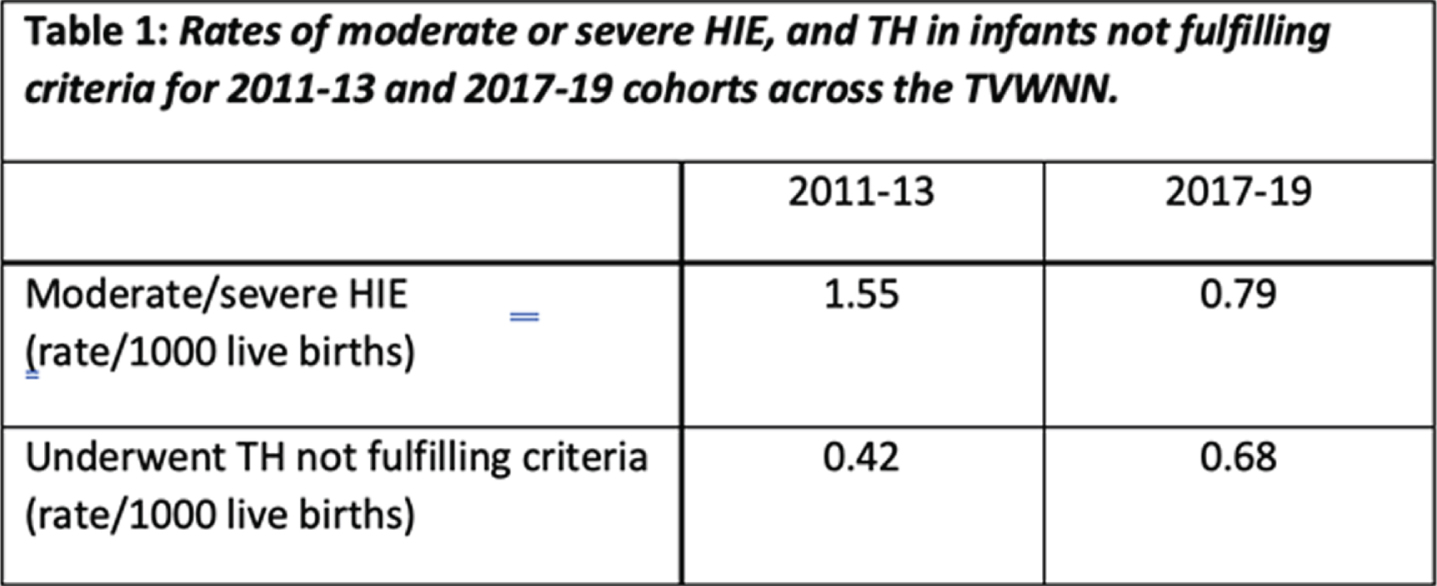
METHODOLOGY: This retrospective audit conducted across the Thames Valley and Wessex Neonatal Network (TVWNN) included 3 NICUs and 10 SCUs/LNUs. The network analyst identified cases using Badgernet. Search terms included: “moderate or severe HIE diagnosis”, or “active therapeutic hypothermia”, or “met any A criteria”. Data were compared between two cohorts 2011-2013 and 2017-2019.
RESULTS: For infants meeting criteria A, serial neurological assessments were completed appropriately in 67.9%. Documentation was enhanced in sites using the network assessment form, introduced between the two cohorts. 4% of infants who met criteria A but didn’t undergo TH were diagnosed with moderate-severe HIE on follow up. For infants who completed TH: aEEG was commenced pre-transfer (if delivered in a SCU/LNU) or in NICU in 76.3%. Only half of the SCU/LNUs could instigate TH and aEEG prior to NICU transfer for ongoing care . Core temperature <34°C within 6 hours was achieved in 73.3% (median 232, IQR 145-170 minutes) and was more often delayed in SCU/LNUs. MRI was performed between day 5-7 in 48% and day 5-15 in 77.4% (median 6, IQR 5-9days). At follow up, 8.3% had died, 56% had 2-year follow up data available and 67% of these infants had normal neurodevelopment.
CONCLUSION/IMPACT: Moderate-severe HIE rates have fallen. However, mild HIE cases receiving TH has risen. Despite increasing recognition that adverse neurodevelopmental outcomes also impact this group(5,6), the BAPM framework advises TH for mild HIE should be reserved for clinical trials. Widespread use of the network assessment form to document neurological assessments, as well as increasing accessibility to aEEG and cooling equipment across the network could improve identification of infants eligible for TH and minimise delays initiating and reaching core target temperature.
Functional connectivity alternations before and during neonatal seizure
Khazaei Ma, Raeisi Ka, Croce Pb, Tamburro Gb, Zappasodi Fc, Comani Sb
aDepartment of Neuroscience Imaging and Clinical Sciences, University “G. d’Annunzio” of Chieti–Pescara, Chieti, Italy
bBehavioral Imaging and Neural Dynamics Center, University “G. d’Annunzio” of Chieti–Pescara, Chieti, Italy
cInstitute for Advanced Biomedical Technologies (ITAB), University “G. d’Annunzio” of Chieti–Pescara, Chieti, Italy
BACKGROUND AND PURPOSE: Seizures are the most common clinical presentation of neurological conditions in neonates and could potentially have an adverse effect on neurodevelopment. So far, assessing the dynamic behavior of functional networks before and during seizures has been poorly investigated1, although it can help achieve insights into neurological well-being. This study aims to assess how functional networks, extracted with different functional connectivity methods and EEG montages, change after seizure onset.
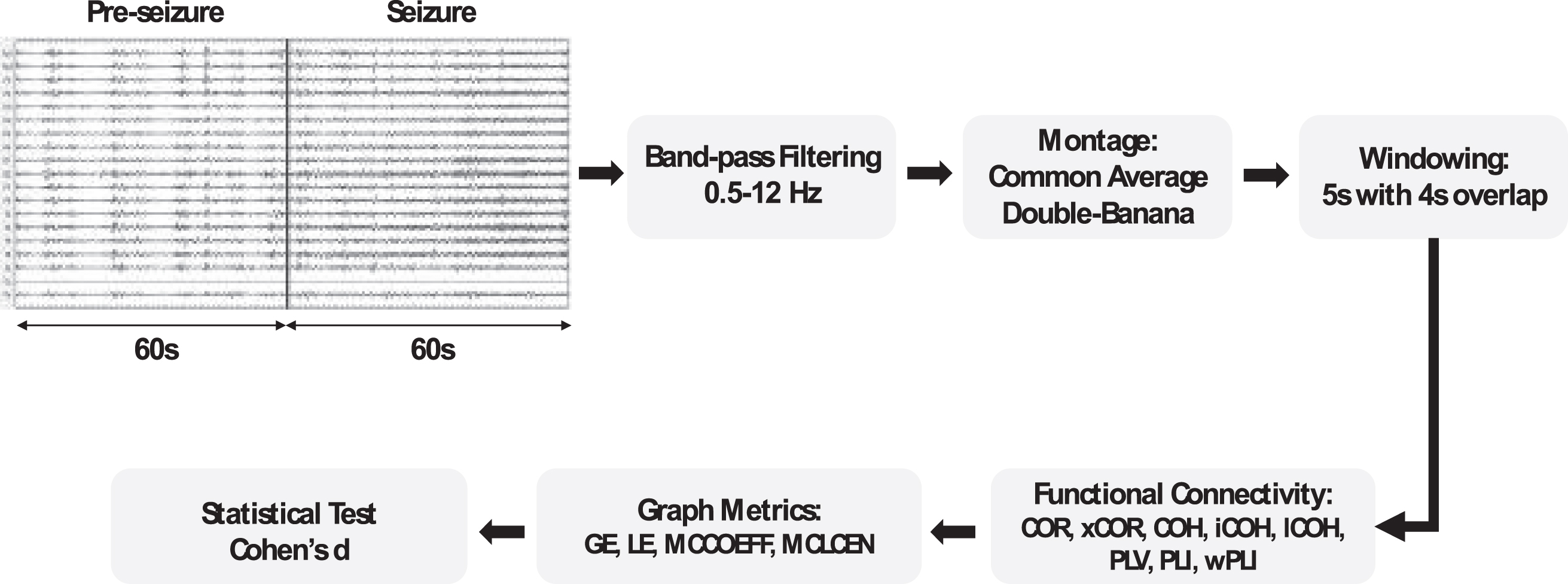
MATERIALS AND METHODS: EEG recordings belonging to a public dataset2 and recorded using 19 electrodes and 256 Hz sampling frequency were used. Two-minute EEG segments containing one-minute pre-seizure and one-minute seizure were selected, resulting in 50 segments from 23 term neonates. Data were band-pass filtered between 0.5-12 Hz. Functional connectivity matrices (FCMs) were calculated using cross-correlation, correlation, coherence, the imaginary part of coherence, lagged coherence, phase-locking value, phase-lag index, and weighted phase-lag index for common average and double-banana EEG montages2. The dynamics of the functional networks were assessed by graph-theory-based metrics (i.e., global efficiency, local efficiency, mean clustering coefficient, and mean closeness centrality) (Fig. 1). A t-test permitted to check the differences between the derived metrics. Cohen’s d was calculated to quantify significant differences.
Figure 1 –
The pipeline of the analysis of functional connectivity matrices using graph metrics )for pre-seizure and seizure parts of the EEG segments. COR: correlation; xCOR: cross-correlation; COH: coherence; iCOH: imaginary part of coherence; lCOH: lagged coherence; PLV: phase-locking value; PLI: phase-lag index; wPLI: weighted phase-lag index; GE: global efficiency; LE: local efficiency; MCCOEFF: mean clustering coefficient; MCLCEN: and mean closeness centrality.
RESULTS: The statistical tests indicated that graph metrics derived from different FCMs for pre-seizure and seizure segments significantly differed for both EEG montages (p < 0.001), with global efficiency having the largest variations between pre-seizure and seizure segments for both montages and all functional networks, and mean clustering coefficient having the smallest differences (Fig. 2). For both montages, coherence maps showed the largest Cohen’s d indicating that they can best differentiate between seizure and non-seizure segments. Conversely, graphs constructed based on the phase-lag index had the lowest performance (Fig. 2).
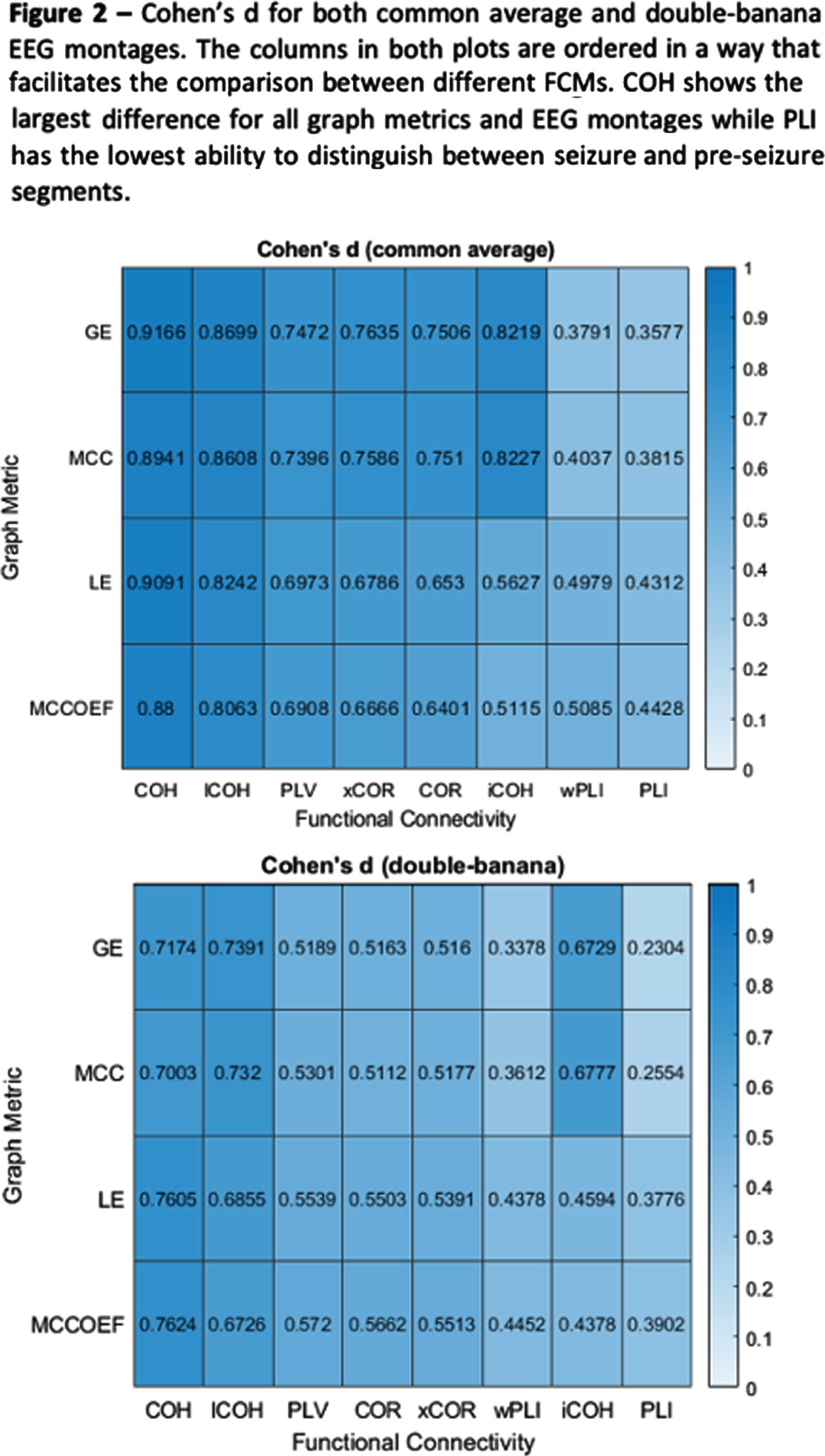
CONCLUSION: Our results confirm that metrics based on graph theory and calculated from different FCMs can typify the different dynamics occurring in functional networks before and during seizures. Graph metrics calculated on functional connectivity maps based on coherence and common average montage were the most effective in capturing the functional changes occurring in the neonatal EEG due to the onset of neonatal seizures. This result might suggest that synchronization between different brain regions increases during seizure and that it depends on the oscillation frequency.
ACKNOWLEDGMENT: This project receives funding from the European Union’s Horizon 2020 Framework Programme under grant agreement No.813843.
References:
[1] Abbas AK, Azemi G, Ravanshadi S, Omidvarnia A (2021) An EEG-based methodology for the estimation of functional brain connectivity networks: Application to the analysis of newborn EEG seizure. Biomedical Signal Processing and Control 63:102229 doi:10.1016/j.bspc.2020.102229.
[2] Stevenson NJ, Tapani K, Lauronen L, Vanhatalo S (2019) A dataset of neonatal EEG recordings with seizure annotations. Sci Data 6(1):190039 doi:10.1038/sdata.2019.39
Persistent pulmonary hypertension in term newborns with neonatal encephalopathy treated with therapeutic hypothermia and impact on brain injury score
Kilmartin Ka, Al Balushi Aa, Barbosa Vargas Sa, Maluomi Ja, Wintermark Pa
aMontreal Children’s Hospital, Mcgill University Health Centre, Montréal, Canada
BACKGROUND: Birth asphyxia causing neonatal encephalopathy (NE) is associated with significant mortality and morbidity, even when these neonates are treated with therapeutic hypothermia (TH). These neonates often present with multi-organ failure, including hypoxic respiratory failure and persistent pulmonary hypertension (PPHN).
OBJECTIVE: To investigate the effect of PPHN on outcome in neonates with NE treated with TH.
METHODS: This single-center retrospective study included all near-term and term neonates with NE treated with TH between 2011 and 2020. PPHN was defined as a pre- and post-ductal saturation difference of more than 10% leading to the use of inhaled nitric oxide. Adverse outcome was defined as mortality and/or brain injury on MRI.
RESULTS: 384 newborns with NE were treated with TH. Among them, 24% had PPHN. Those with and without PPHN had similar gestational age, birth weight, and sex. Neonates with PPHN had higher fraction of inspired oxygen requirement in the first 4 days of life (P <0.001), were more often intubated (87% vs. 58%, P <0.001), and were more often treated for associated hypotension (73% vs. 44%, P < 0.001). They had significantly lower PaO2 levels during the first 2 days of life (P < 0.001), significantly higher PaO2 levels on days 3 and 4 of life (P <0.001), and had significantly more variations of PaO2 during the first 4 days of life (P < 0.001). They died more often (22% vs. 12%, P = 0.009) and more often developed brain injury (47% vs. 37%, P = 0.02) than those without PPHN.
CONCLUSION: PPHN occurred frequently in neonates with NE treated with TH. PPHN was associated with a higher incidence of adverse outcome. It remains important to avoid hyperoxemia and limit variations of PaO2 in these neonates during the first 4 days of life to potentially limit the incidence of adverse outcome.
EEG background response to rewarming and neurodevelopmental outcomes in neonatal HIE: a prospective study
Mahdi Za, Marandyuk Ba, Chowdhury Ra, Gallagher Aa, Birca Aa, Pinchefksy Ea, Dehaes Ma
aCHU Sainte-Justine, Montreal, Canada
Neonatal hypoxic-ischemic encephalopathy (HIE) is associated with high mortality and long-term neurodevelopmental disability in survivors. Therapeutic hypothermia (TH) is now standard of care for infants with moderate-severe HIE as it provides effective neuroprotection by improving survival rates and reducing severe neurodevelopmental disability (1). Rewarming at the end of TH represents a transient phase of increased neurological vulnerability with previous studies reporting rebound seizures and impaired cerebral activity during gradual rewarming (2,3). The aim of the present study was to examine whether EEG background changes during rewarming phase are associated with neurodevelopmental outcomes.
Forty-nine neonates with HIE who received TH and had EEG recordings available were enrolled prospectively between June 2017 and September 2021. Quantitative EEG discontinuity index, represented by proportion of epochs of low voltage activity <15μV for a duration of 2-seconds, was calculated at 6-hour intervals during TH, rewarming and post-rewarming periods. The Alberta Infant Motor Scale (AIMS) evaluation at 4-month or death before 4 months was used to categorize our cohort into favourable and adverse outcome groups at 4 months of age. An AIMS score < the 5th percentile rank was defined as significantly delayed or “high risk” for adverse outcome. Cognitive, language, and motor development were assessed with the Bayley-III performed at age 2 years. Wilcoxon signed-rank test and Spearman rank-order statistics were conducted to examine significant EEG background changes from baseline (i.e. during TH) to end of rewarming and post-rewarming across our two groups, and assess their correlations with Bayley-III scores, respectively.
Out of the 49 patients included in the study (male 63%), 11 (22%) were at high risk of motor delay based on the 4-month AIMS assessment (<5th percentile) and three died by 4-month of age (6%). Seventeen patients (35%) had Bayley-III data available at follow-up. Infants with adverse outcome at 4 months (39%) had a significant increase in EEG discontinuity index from TH to rewarming (p=0.02), and from TH to post-rewarming (p<0.01) (Fig.1). None of these changes were significant in infants with favourable 4-month outcome. Spearman correlation showed significant associations between increasing EEG discontinuity index from TH to rewarming and decreasing cognitive (r=-0.602, p=0.01) (Fig.2A), language (r=-0.564, p=0.02) (Fig.2B) and motor (r=-0.607, p=0.01) (Fig.2C) composite scores on Bayley-III.
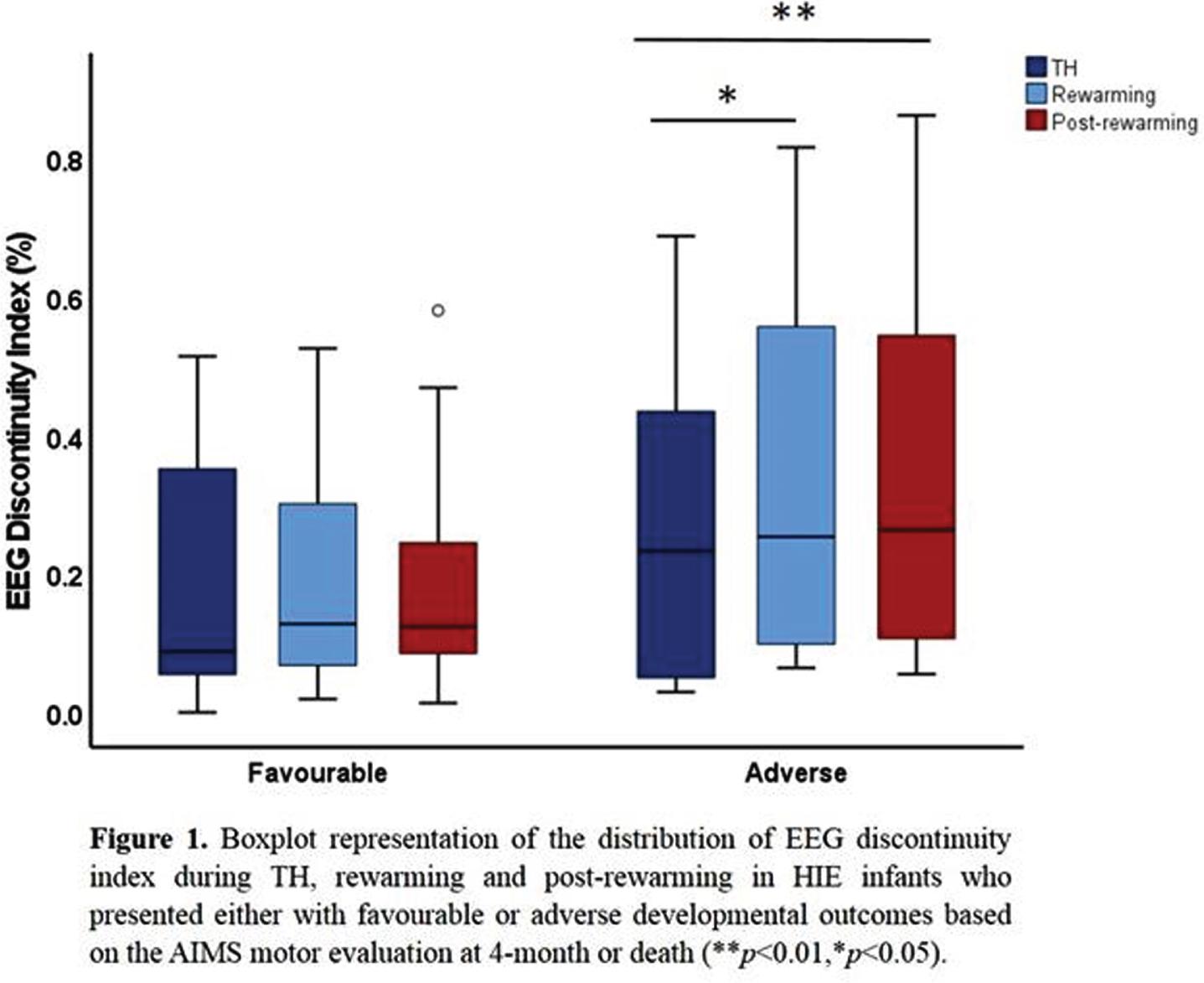
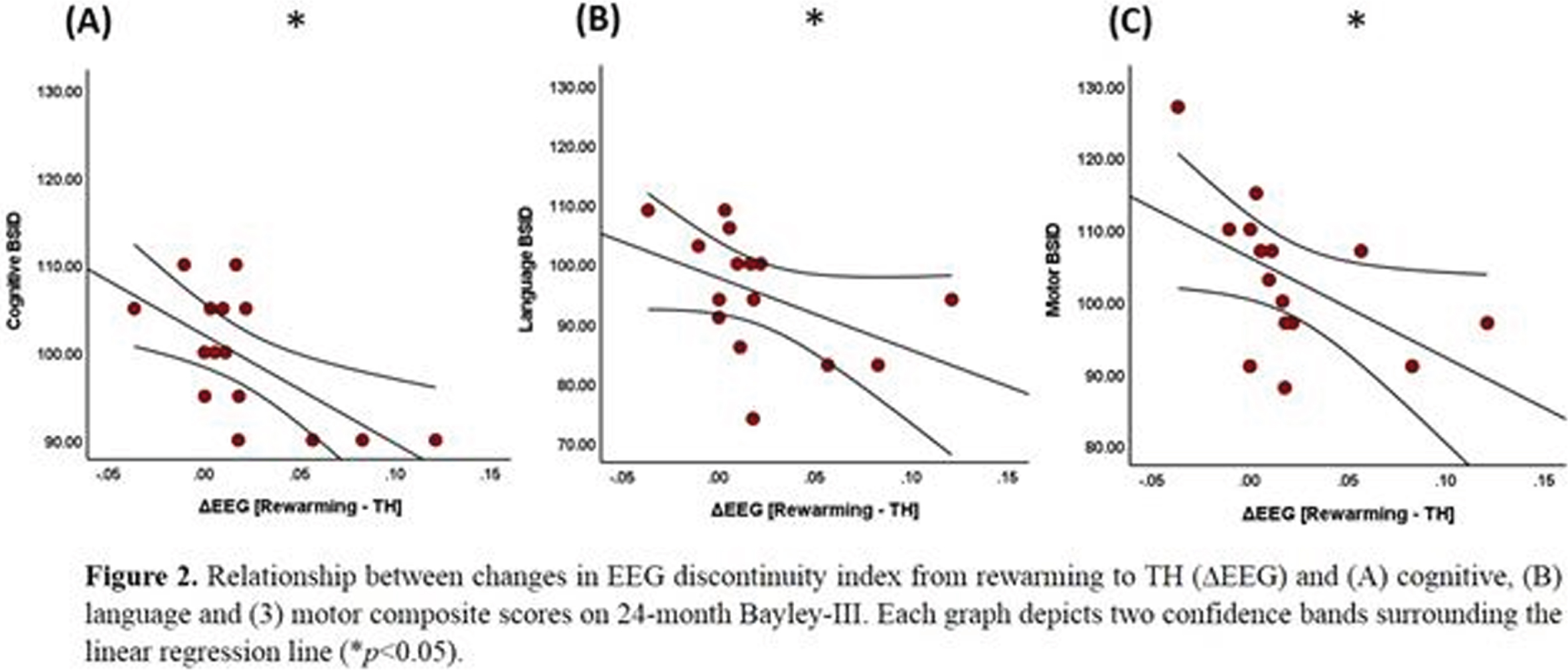
In HIE neonates with adverse early outcomes, EEG background showed significant increase in discontinuity index during rewarming, but remained unchanged in neonates with early favourable outcome. Increasing EEG discontinuity during rewarming correlated with decreasing cognitive, language and motor scores at age 2 years. These preliminary results suggest that EEG background evolves during rewarming and might serve as a predictor of neurodevelopmental outcome.
1. Shankaran S et al., Cochrane Library. 2012;366:2085-2092.
2. Birca A, et al., Clinl Neurophysiol. 2016;127:2087-94.
3. Battin M et al., Pediatrics. 2004;114:1369.
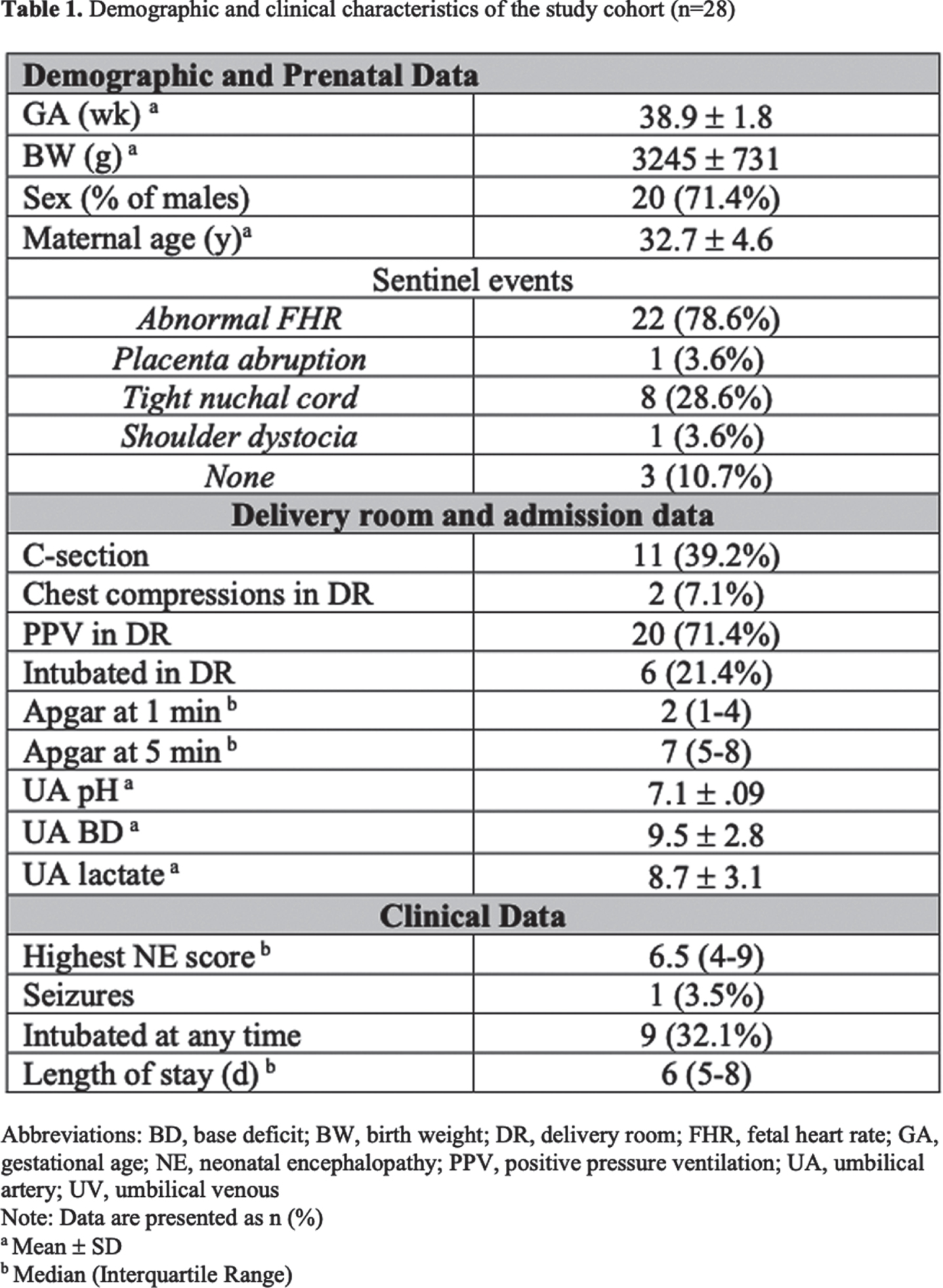
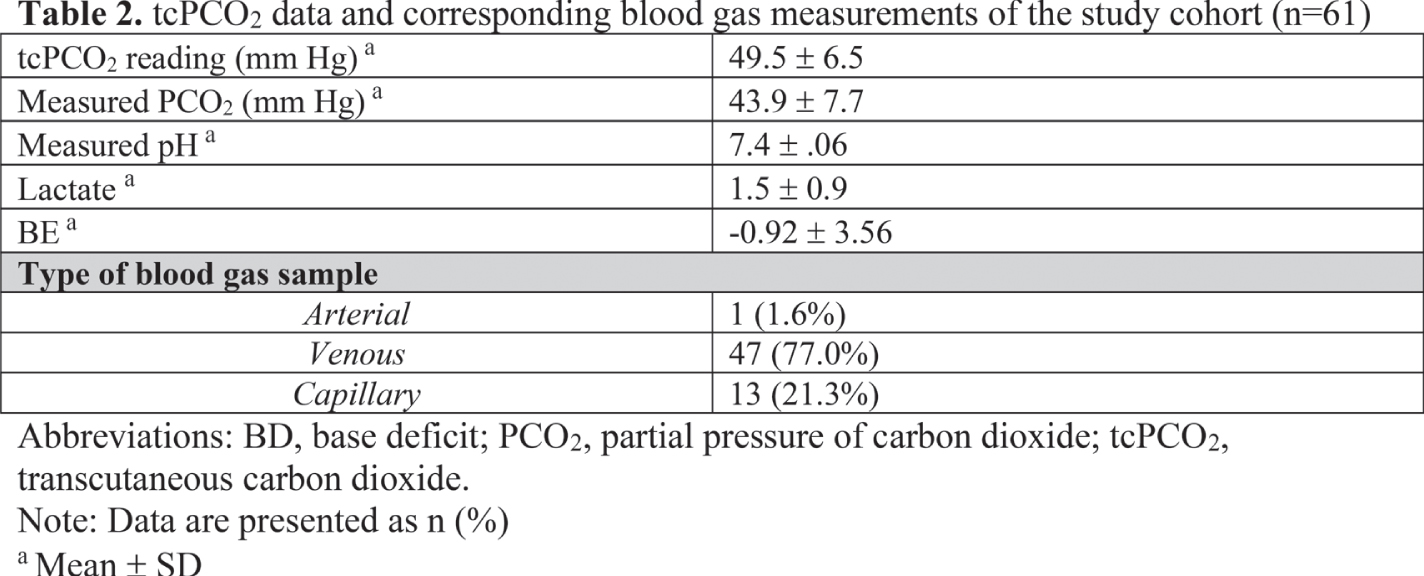
Transcutaneous carbon dioxide monitoring in neonates receiving therapeutic hypothermia for neonatal encephalopathy
Munster Ca, Lee Sa, Szakmar Ea,b, Sunwoo Jc, Elshibiny Ha, Franceschini Mc, Robinson Ja, Christou Ha, Inder Ta, El-Dib Ma
aDepartment of Pediatric Newborn Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, United States
b1st Department of Pediatrics, Semmelweis University, Budapest, Hungary
cAthinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Harvard Medical School, Charlestown, United States
BACKGROUND AND PURPOSE : Hypocarbia is associated with brain injury and adverse neurodevelopmental outcome in infants who receive therapeutic hypothermia (TH) for neonatal encephalopathy (NE) [1,2]. Transcutaneous measurement of CO2 (tcPCO2) is a noninvasive method to continuously monitor PCO2 levels. However, the accuracy of the PCO2 readings from this transcutaneous monitoring method has not been evaluated in neonates undergoing TH. Thus, the aim of this study was to assess the reliability of tcPCO2 readings in infants undergoing TH by evaluating the agreement between PCO2 determined via blood gas analysis and tcPCO2.
METHODOLOGY: This analysis is from an ongoing prospective study conducted at Brigham and Women’s Hospital to test the feasibility and reliability of tcPCO2 in term infants receiving TH for NE. We included infants enrolled between October 2019 and September 2021. tcPCO2 was monitored using the SenTec Digital Monitor. Since the TCOM probe warms the skin underneath, we used measured PCO2 values that were not corrected for hypothermia. PCO2 values were obtained from blood gas analysis of venous, arterial and capillary samples. For statistical analysis, paired-samples t-test was used to compare the means of PCO2 and tcPCO2. Pearson correlation test was performed to calculate the correlation coefficient, and Bland-Altman plot was used to analyze the agreement between PCO2 and tcPCO2.
RESULTS: To date, we have collected 61 PCO2 data points from 28 enrolled infants. Demographic and clinical characteristics of infants are shown in Table 1. Table 2 shows the blood gas results and the corresponding tcPCO2 readings. There was no significant difference between PCO2 from blood gas analyses and tcPCO2 (51.0 ± 8.7 vs. 49.5 ± 6.5 respectively, p=0.2). There was a modest correlation between PCO2 and tcPCO2 (r=0.36, p = 0.004, Figure 1). The difference between PCO2 and tcPCO2 was < 10 mm Hg in 72% of samples. Figure 2 shows the differences between tcPCO2 and PCO2; the Bland-Altman plot gave a bias of -1.45 ± 8.78 mm Hg with limits of agreement between -18.66 and 15.76 mm Hg.
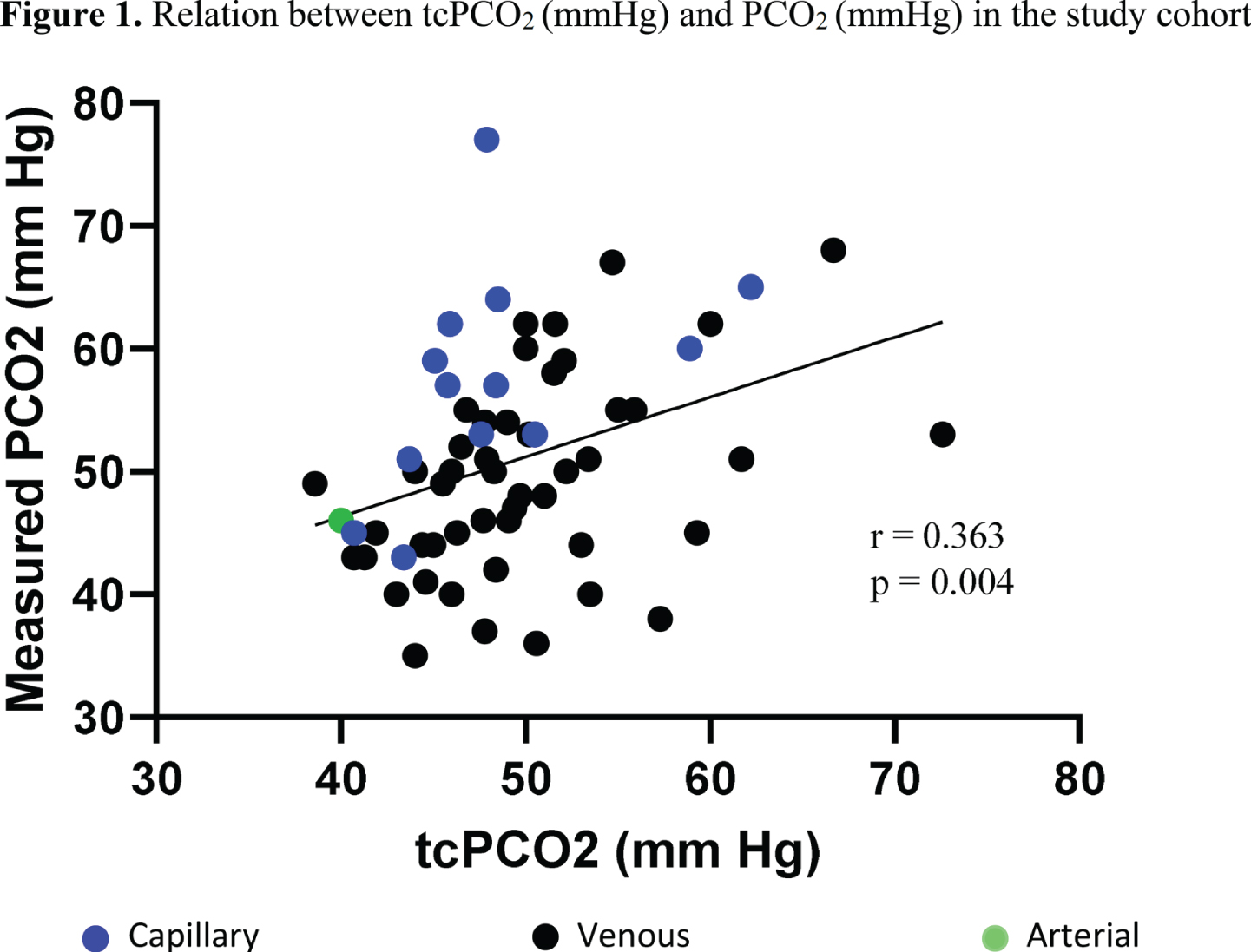
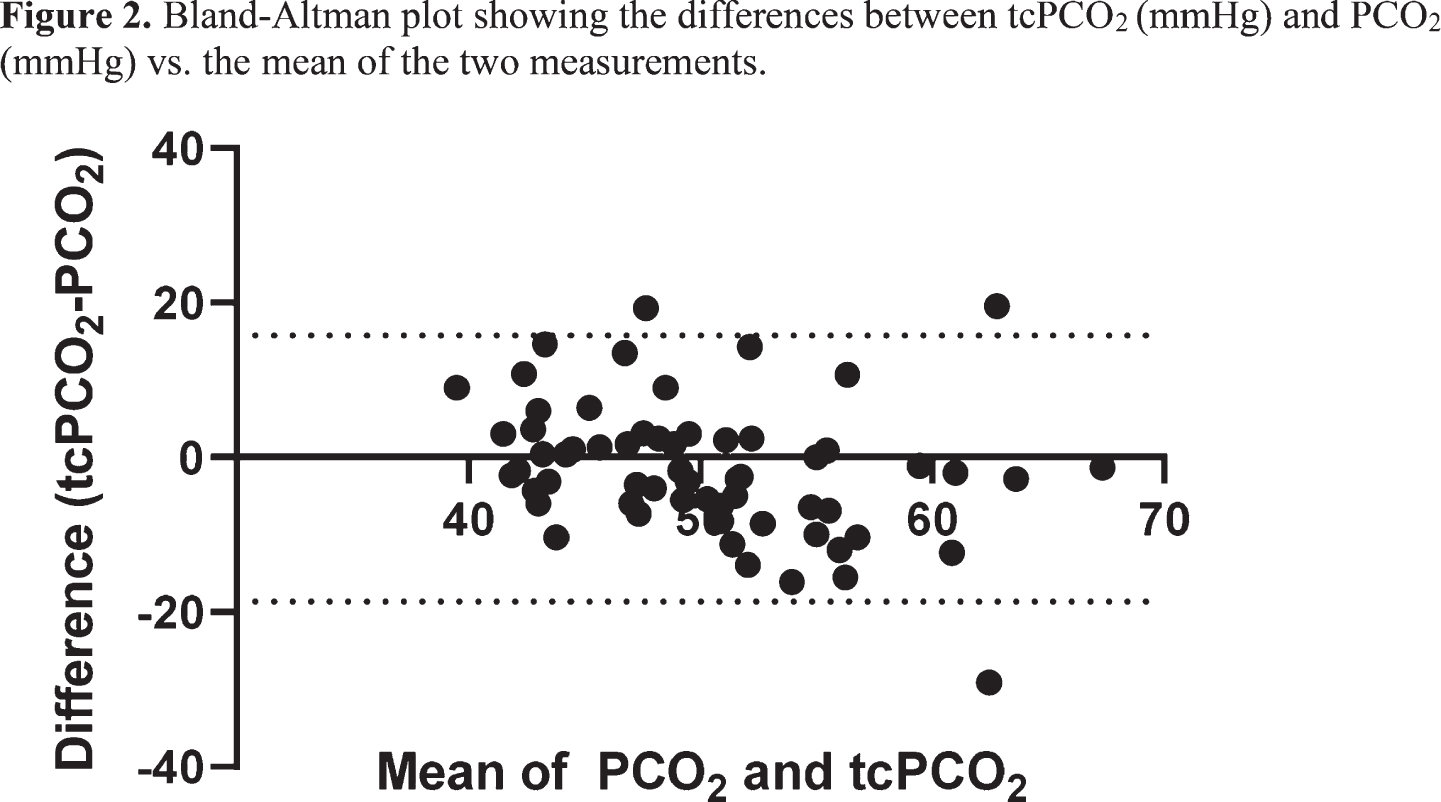
CONCLUSION: This study supports the feasibility and possible utility of using tcPCO2 measurements in term infants receiving TH for NE. We will collect additional data points and will continue to investigate factors associated with better correlation between PCO2 and tcPCO2.
References:
1. Pappas A et al. Hypocarbia and adverse outcome in neonatal hypoxic-ischemic encephalopathy. The Journal of pediatrics 2011, 158(5): 752-758 e751.
2. Lingappan K et al. Relationship between PCO2 and unfavorable outcome in infants with moderate-to-severe hypoxic ischemic encephalopathy. Pediatr Res 2016, 80(2): 204-208.
Recovery speed of aEEG background activity after perinatal hypoxic ischemic encephalopathy predicts development of postneonatal epilepsy
Nyman Ja, Mikkonen Kb, Metsäranta Mc, Toiviainen-Salo Sd, Vanhatalo Sa,e, Lauronen La, Nevalainen Pa,e
aEpilepsia Helsinki, Clinical Neurophysiology, HUS Diagnostic Center, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
bEpilepsia Helsinki, Division of Child neurology, Children’s Hospital and Pediatric Research Center, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
cDepartment of Neonatology, Children’s Hospital, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
dDepartment of Pediatric Radiology, HUS Medical Imaging Center, Radiology, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
eBABA center, Children’s Hospital and Pediatric Research Center, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
BACKGROUND AND PURPOSE: Although perinatal hypoxic ischemic encephalopathy (HIE) is a well-known risk factor for later epilepsy, there is currently a shortage of means to predict at individual level, which of the affected neonates will develop epilepsy. We evaluated the accuracy of neonatal amplitude-integrated electroencephalography (aEEG) brain monitoring for predicting development of postneonatal epilepsy after perinatal HIE. We hypothesized that aEEG background, reflecting the degree of brain injury, would be a more accurate predictor of later epilepsy than neonatal seizures.
MATERIALS AND METHODOLOGY: We studied a population-based cohort of 85 consequent neonates with moderate-to-severe HIE that had aEEG brain monitoring started before 12 hours postnatal age. We marked electrographic seizures and scored each hour of the aEEG background as inactive (score 4), burst-suppression (score 3), or continuous without (score 2) or with sleep cycling (score 1). These aEEG findings were compared to outcome at age four years. The outcome groups were: deceased, epilepsy (with or without CP), CP without epilepsy, and favorable outcome meaning no CP or epilepsy diagnosis.
RESULTS: Out of the 80 infants with follow-up information available six developed epilepsy. They had all had severe HIE. All epilepsy diagnoses were made by age one year and no new diagnoses were made between one and four years of age. The total seizure burden (p = 0.003, Kruskal-Wallis test) and maximum hourly seizure burden (p = 0.007, Kruskal-Wallis test) were both significantly associated with outcome so that the deceased neonates and those who developed epilepsy had a higher total seizure burden and maximum hourly seizure burden than those with a favorable outcome. The aEEG background recovery speed also significantly differed between the outcome groups (p < 0.001, Kaplan-Meier Log Rank test) so that the deceased neonates and those who developed epilepsy had significantly slower background recovery than those neonates who developed CP without epilepsy or those with a favorable outcome. At individual level the most accurate (97% i.e. two false predictions) predictors for later epilepsy amongst the survivors were aEEG background score 4 at 24 hours (sensitivity 67%, PPV 100% i.e. two false negatives and no false positives) and aEEG background score 3 or 4 at 48 hours (sensitivity 100%, PPV 75% i.e. two false positives and no false negatives).
CONCLUSIONS: aEEG background provides accurate prediction for development of epilepsy after perinatal HIE. Although neonatal seizures were associated with later epilepsy, they were not as accurate predictors at individual level as the aEEG background.
Hypocapnia in early hours of life is associated with brain injury in moderate- severe neonatal encephalopathy
Szakmar Ea, Munster Ca, Shibiny Ha, Jermendy Ab, Inder Ta, El-Dib Ma
aDepartment of Pediatric Newborn Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, United States
b1st Department of Pediatrics, Semmelweis University, Budapest, Hungary
BACKGROUND AND PURPOSE: Increasing evidence supports that there is an association between hypocapnia and neurological impairment in infants with moderate- severe neonatal encephalopathy (NE). As therapeutic hypothermia (TH) has clearly proven to be safe, many centers including ours started to provide TH for mild cases. While hypocapnia could still be encountered in those with mild NE, whether hypocapnia is associated with brain injury in this population is unknown. The aim of this study was to evaluate the association between hypocapnia within the first 24 hours and brain injury assessed by post-rewarming MRI in infants receiving TH stratified by the stage of NE.
METHODOLOGY: This retrospective cohort study included infants who received TH between June 2015 and May 2019 in Brigham and Women’s Hospital. The pattern of the brain injury on post-rewarming MRI was evaluated according to the novel grading system developed by Weeke et al. Arterial, capillary, and venous temperature corrected PCO2 values within the first 24 hours of life were analyzed via multiple ways. Quasi-Poisson regression modelling was performed to explore the association between the PCO2 variables and the total score of brain injury. The regression models were adjusted for 5-minutes Apgar score and first postnatal pH and stratified according to the stage of NE.
RESULTS: 188 infants were included in the study with 47.9 % of mild and 52.1% of moderate- severe stage of NE. Fifty per cent of the infants had at least one PCO2 value = 35 mmHg within 24 hours of life in the full cohort. Infants with moderate- severe NE spent more time in hypocapnia (median 2.3 [0.0; 6.3] vs. 0.0 [ 0.0; 2.7] hours, p=0.004) and presented with more severe brain injury compared to mild cases (median 2 [1; 6] vs. 1 [0; 3] total score of brain injury, p=0.001). The increase in total MRI score was 6% (Incidence Rate Ratio: 1.06; 95% CI 1.00- 1.11) for each extra hour spent in hypocapnic range in infants with moderate-severe NE after adjusting for Apgar 5’and postnatal pH. In the group of infants with mild NE, the hours spent in hypocapnia had no effect on developing brain injury (Figure 1).
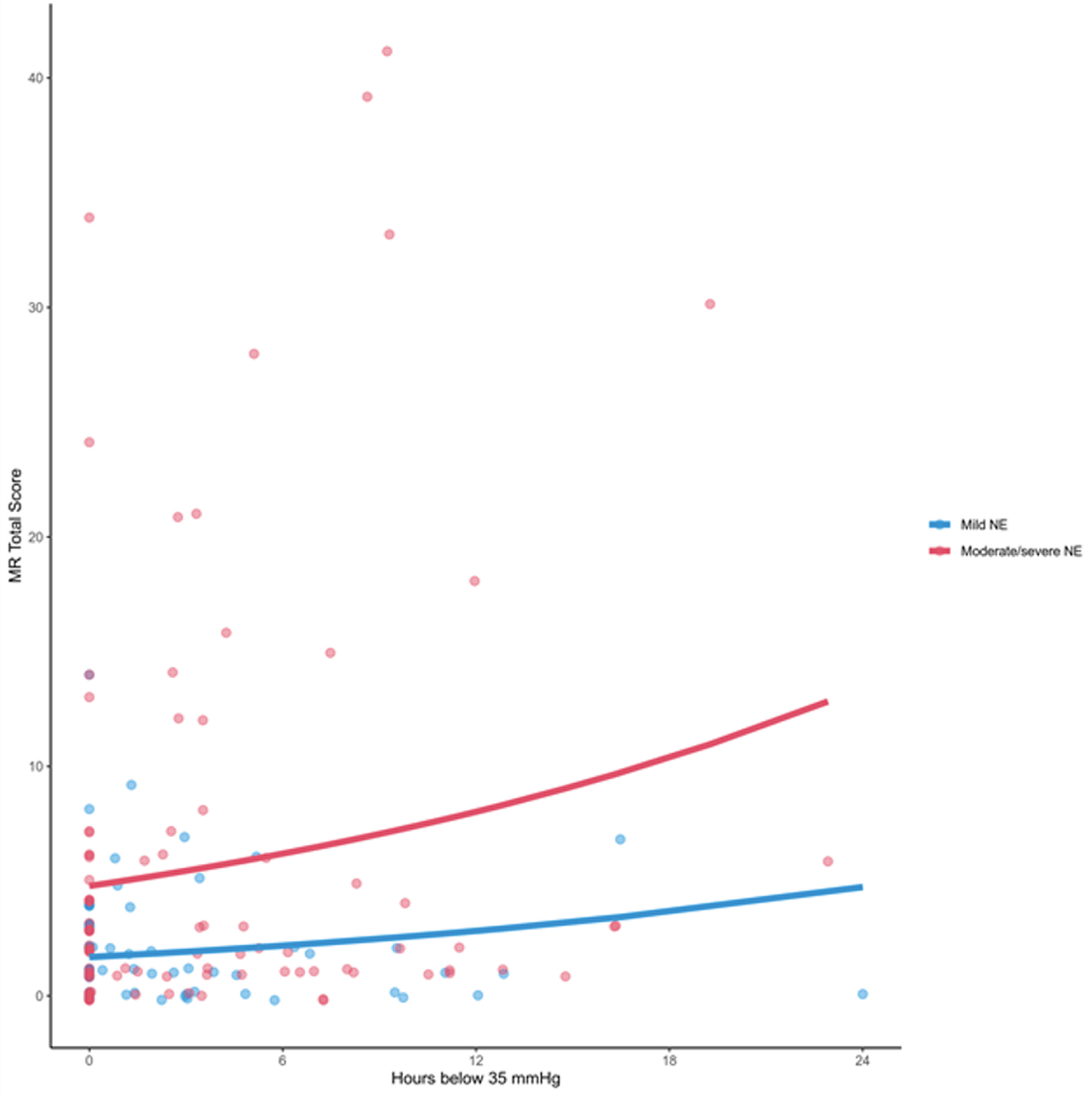
CONCLUSION: Hours spent below PCO2 of 35 mmHg was an independent predictor of increasing total injury score on post-rewarming brain MRI in infants with moderate and severe NE. In contrast, there was no association between hypocapnia and hypoxic-ischemic injury in mild NE. Our results emphasize that careful CO2 monitoring is very valuable in infants with moderate- severe NE. However, prospective randomized trial of controlled normocapnia is warranted to test whether hypocapnia is a biomarker or a modifiable risk factor of brain injury.
Adjustment of the dose of fentanyl used for sedation/analgesia in the ventilated neonates by using the sleep/wake cycles pattern on aEEG
Toma Aa,b
aLife Memorial Hospital, Calea Grivitei 365, Sector 1, Romania
bUniversity Titu Maiorescu. Faculty of Medicine, Bucharest, Romana
BACKGROUND AND PURPOSE: Sedation/analgesia is needed for the ventilated neonates, but there are short and long-term effects of the drugs used that could impact on the course of the disease or the outcome of the patient. Our study aimed to describe a method of adjusting the level of the sedatiion by using the aEEG, in order to decrease the impact of sedation/analgesia on the developing brain.
MATERIALS AND METHODOLOGY: 20 ventilated term and preterm neonates (gestational age 34-38 weeks) were sedated using fentanyl continuous drip, starting at a dose of 0,5 micrograms/kg/minute. All the patients wer monitored with aEEG. The level of pain control was monitored by using NIPS (Neonatal Infant Pain Profile) with a score < 5 was considered to reflect a good pain control. The dose of fentanyl was decreased until the appearance of the sleep/wake cycles on aEEG and then decreased gradually when extubation was anticipated. The study cohort was compared with paired hystoric controls with the same respirratory pathology, gestational age that recieved fentanyl at a fixed dose 0.5 micorgrams/kg/hour, that was modified only according to the pain score. There were not included in the study patients with perinatal asphyxia. There were compared between the two groups the pain control (NIPS - Neonatal/Infant Pain Scale) scores, duration of ventilation, extubation failure due to depressed respiratory drive. duration of stay in hospital, neurologic examination at discharge and neurologic exam at 1 year corrected age.
RESULTS: The dose of fentanyl used for sedation/analgesia was lower in the aEEG monitored group (mean 0.3 micrograms/kg/hour) than in the control group (mean 0.5 micrograms/kg/hour) (p < 0.02). There was no difference in pain control expressed by NIPS score between the two groups (p - n..s.). The mean duration of ventilation was lower in the aEEG monitored group (63.6 hours) compared with the control group (72.4 hours) (p< 0.001). The duration of stay in hospital was also significantly lower for the a EEG monitored group ( mean 7.5 days) compared with a mean of 9 days in the control group (p<0.03). The neurologic examination at discharge showed a decreased axial tone (7/20 versus 3/20 and ocular fixation (8/20 versus 2/20) in the control group compared with the aEEG monitored group. The examination at 1 year did not show differences between the two groups.
CONCLUSIONS: The adjustement of the dose of fentanyl by using aEEG in the ventilated neonates resulted in a decreased duration of ventilation and stay in the hospital and a better axial tone and ocular fixation at discharge compared with the use of a standard dose.
Four years’ experience of a tele-neuromonitoring approach in Brazil: a broader focus on neonates at risk for brain injury
Variane Ga,b,c,d, Rodrigues Da,e, Llaguno Na,e, Pietrobom Ra,b, Netto Aa, Magalhães Ma,b,d
aProtecting Brains & Saving Futures Organization, São Paulo, Brazil
bDivision of Neonatology, Department of Pediatrics, Irmandade da Santa Casa de Misericórdia de São Paulo, São Paulo, Brazil
cFaculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo, Brazil
dDivision of Neonatology, Grupo Santa Joana, São Paulo, Brazil
ePediatric Nursing Department, Escola Paulista de Enfermagem, Universidade Federal de São Paulo, São Paulo, Brazil
BACKGROUND: The elevated rate of impaired neurological outcomes in high-risk newborns is a challenge. Amplitude-integrated electroencephalography (aEEG) is a non-invasive and simplified technique for continuous neuromonitoring at the bedside, allowing brain function assessment in the Neonatal Intensive Care Units (NICU). Newer equipment can associate aEEG with raw EEG traces and video imaging (video aEEG/EEG), leading to better accuracy of seizures detection. Telemedicine is a growing field that can reduce distances between different places, increase access and reach of specific techniques, and decrease structural costs. Protecting Brains and Saving Futures (PBSF) is a Brazilian project that works with a telemedicine system to train and implement neurocritical care in hospitals assisted by a remote monitoring center.
PURPOSE: To evaluate the applicability and describe findings of a tele-neurocritical care model using remote video aEEG/EEG in Brazil.
METHODOLOGY: All monitored infants with three-channel video aEEG/EEG from July/2017 to September/2021 were included in this study. Electroencephalographic information was collected using a central hub at the bedside and all information was uploaded to a cloud database. Two experienced readers remotely accessed all exams using a monitoring center entitled Center of Surveillance and Intelligence (CSI). Indication of brain monitoring, aEEG predominant background activity, sleep-wake cycle (SWC), and seizures were evaluated. Longitudinal training and standard clinical protocols were implemented to homogenize care. Statistical analysis was descriptive, and data was presented according to absolute and relative frequency.
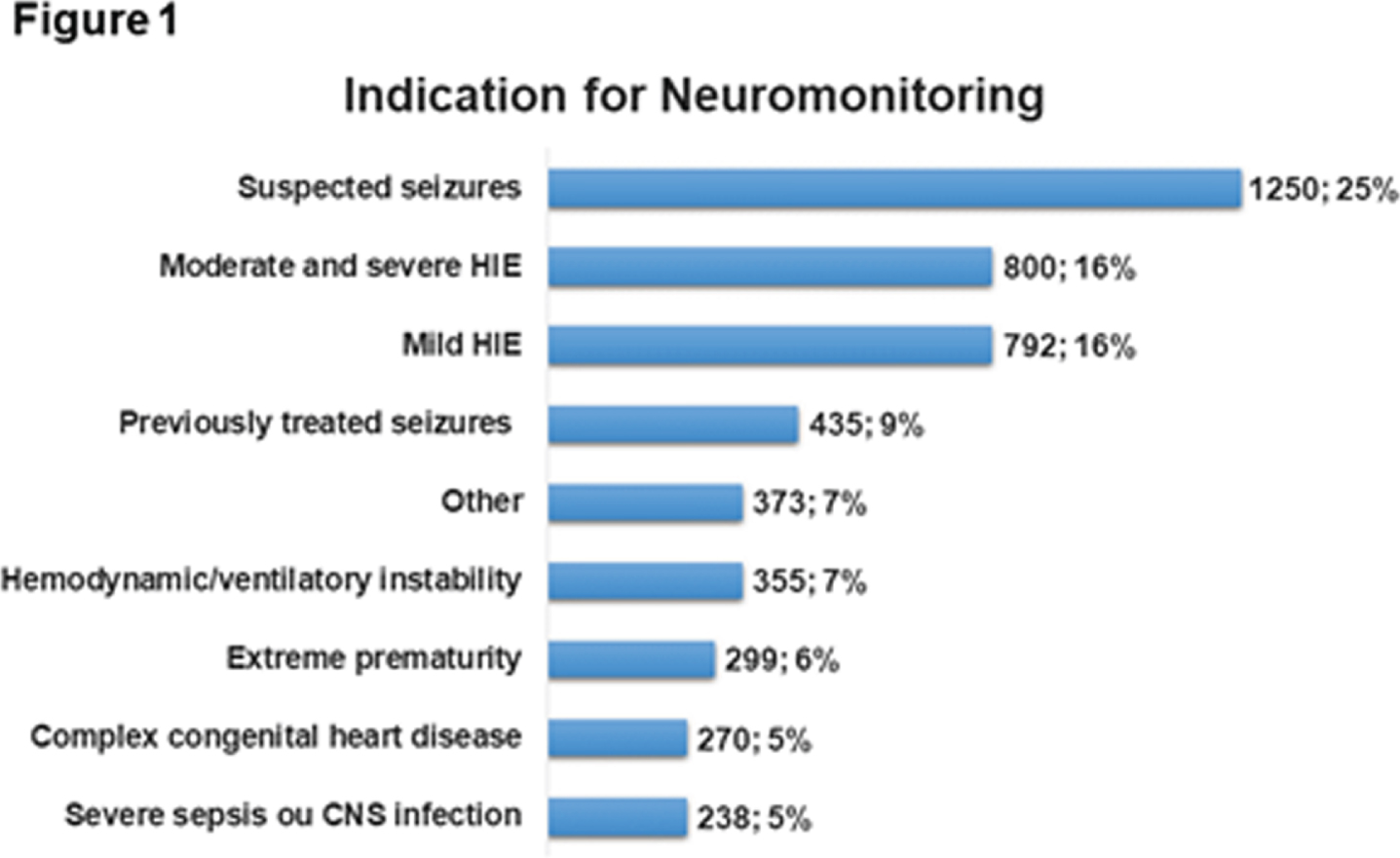
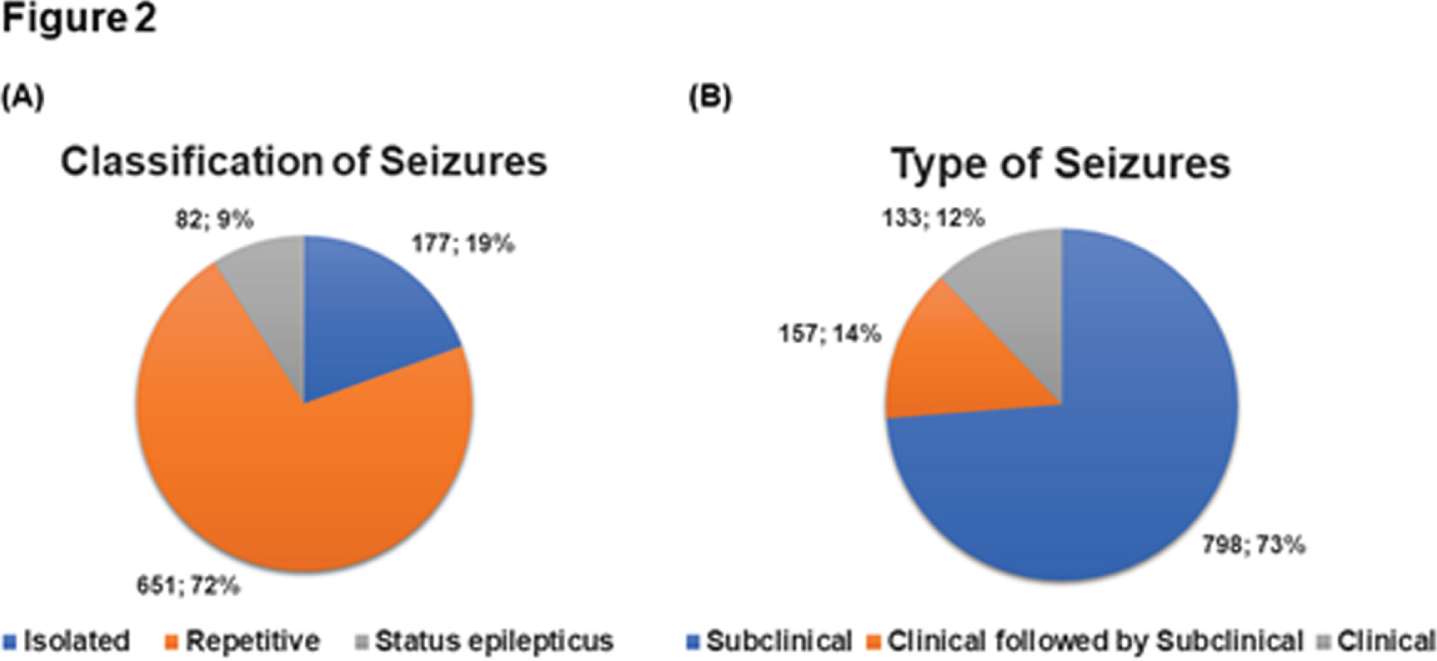
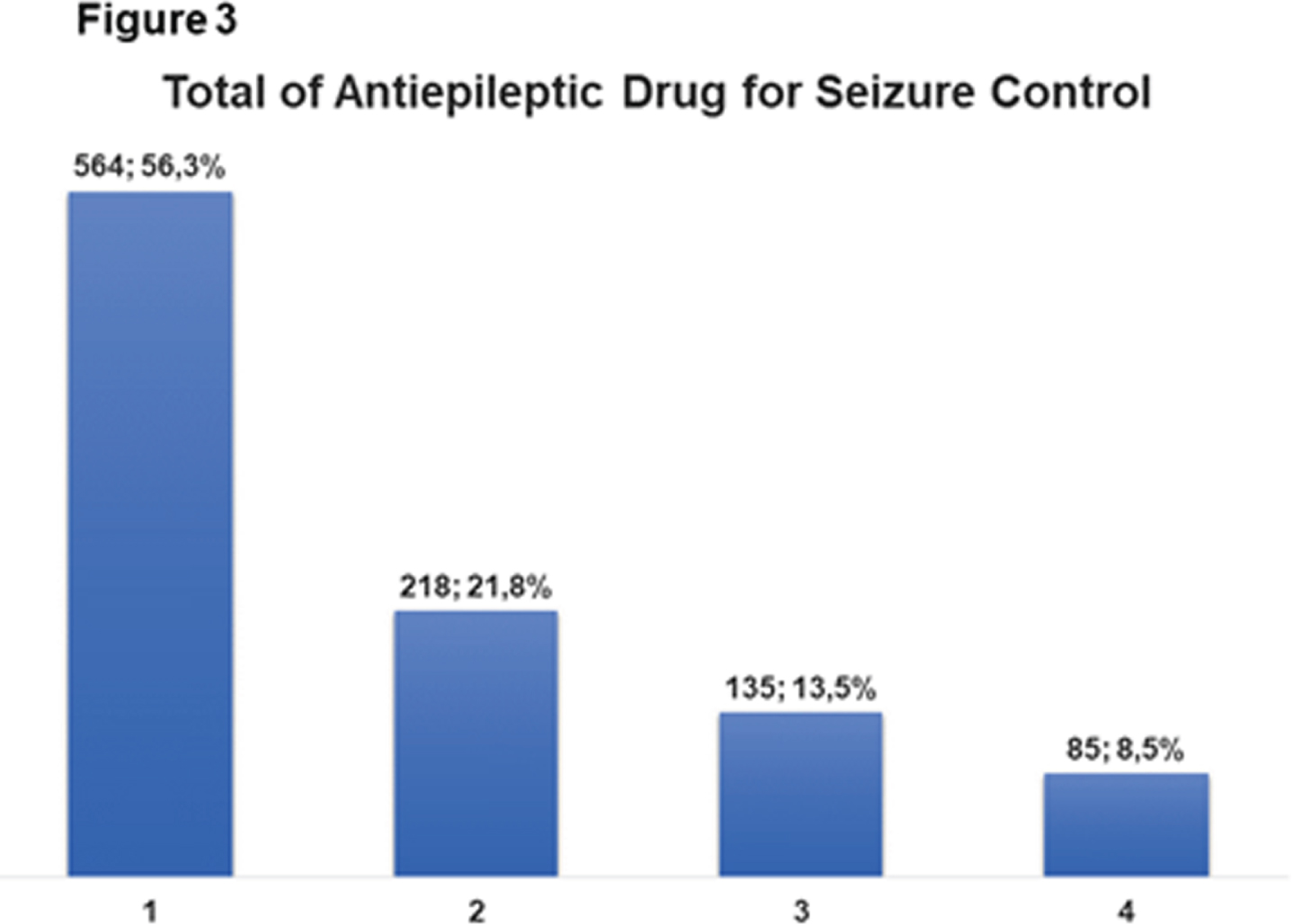
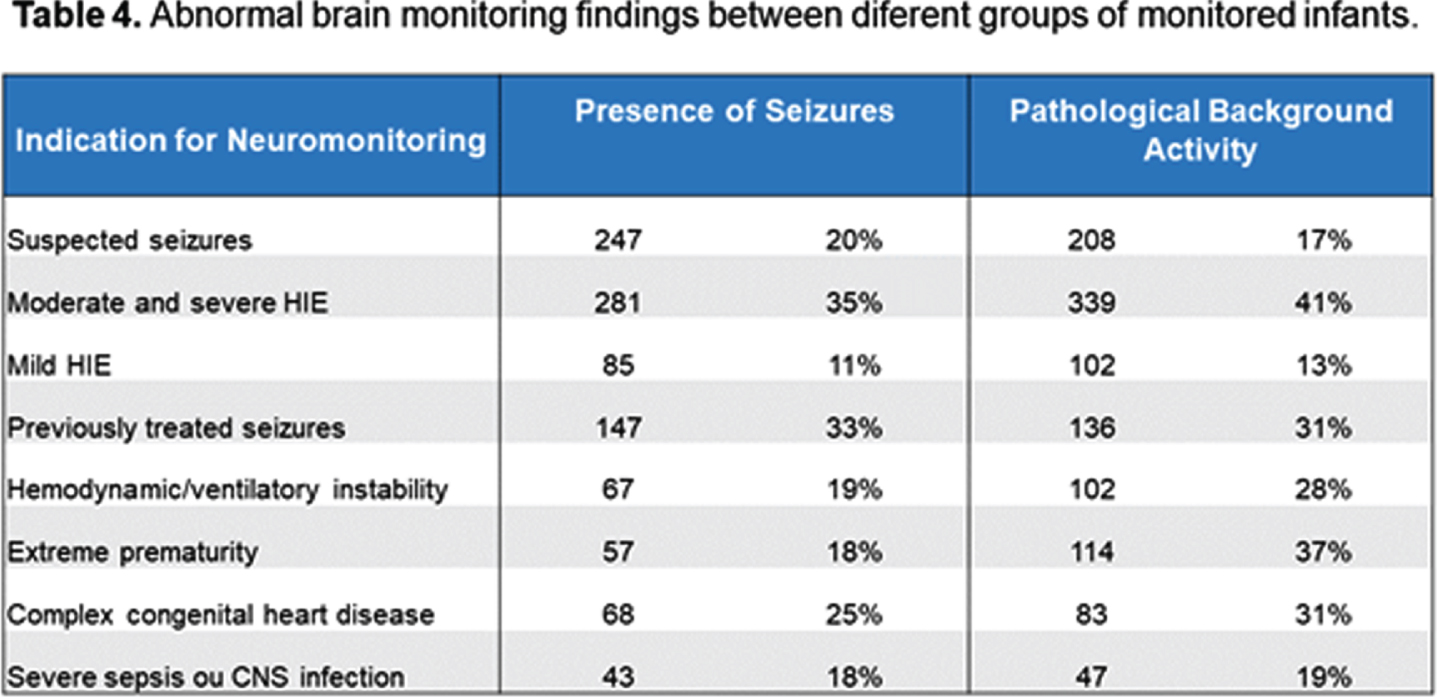
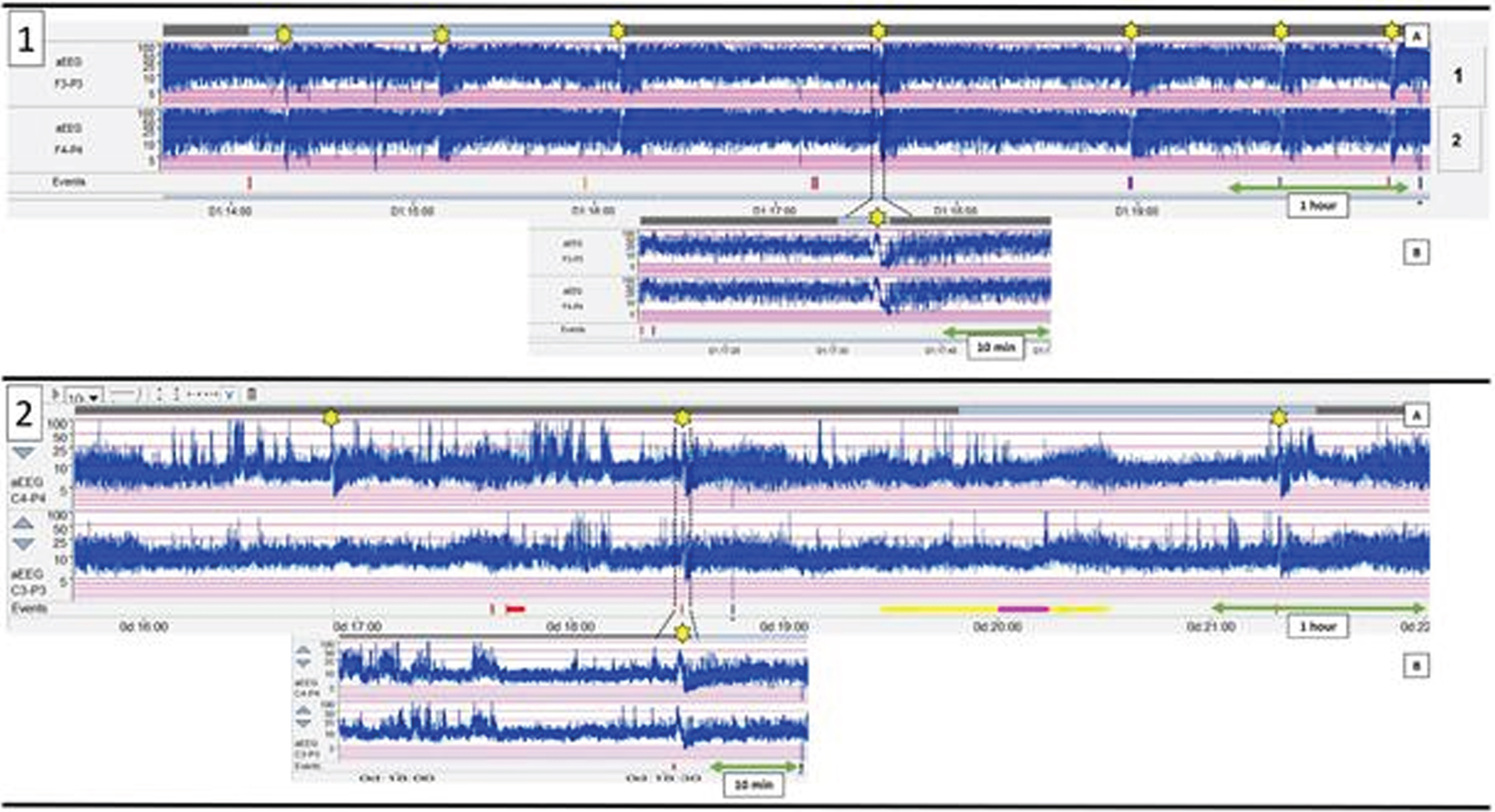
RESULTS: This tele-neuromonitoring approach was implemented in 39 hospitals across all regions of Brazil. A total of 323,114 hours of recording were analyzed. 5025 newborns were monitored with video aEEG/EEG, 2833(57,2%) were male and 3398(69,5%) were born by C-section. Most common indications were suspected seizures (1250;25%), moderate and severe hypoxic-ischemic encephalopathy (HIE) (800;16%), mild HIE (792;16%), previously treated seizures (435;9%), and hemodynamic/ventilatory instability (355;7%) (Figure 1). Pathological background activity, classified as burst suppression, low voltage, and flat trace, was found in 1210(24%) infants, and SWC was absent in 2488(49,5%). 1062(21,1%) infants presented seizures, being 651(72%) repetitive and 798(73%) subclinical(Figures 2 – A and B). 564(56,3%) required only one drug for seizures control(Figure 3), and phenobarbital was the first-line drug of choice. Abnormal brain monitoring findings differed between groups of monitored infants(Table 4). There were 53,852 interactions between CSI remote team and the bedside medical staff for clinical support in real-time.
CONCLUSION: A tele-neuromonitoring solution was successfully implemented in a large number of centers in Brazil with the assistance of experienced readers. Pathological background activity and seizures were frequent in the studied group. This approach is feasible and may be particularly useful in resource-limited countries, where neurocritical programs are scarce.
Bibliography:
1. Alderliesten T, et al. Pediatric Research(2016).
2. Mastrangelo M, et al. Seizure(2013).
3. Hall RW, et al. Ethn. Dis.(2010).
Decreased heart rate entropy is strongly associated with seizures in HIE infants
Vesoulis Za, El Ters Na, Zempel Jb, Fairchild Kc
aWashington University, Department of Pediatrics, St. Louis, United States
bWashington University, Department of Neurology, St. Louis, United States
cUniversity of Virginia, Department of Pediatrics, Charlottesville, United States
BACKGROUND AND PURPOSE: Automated seizure detection algorithms have significant issues with false positive and negative detection. The use of supplemental, non-EEG data may provide a valuable secondary source of information to improve the accuracy of seizure detection. Heart rate variability (HRV) has previously been used to predict outcomes after HIE, finding that infants with better outcomes have greater variability (a sign of autonomic health). Seizures may acutely disrupt autonomic function which can be quantitatively detected as changes in HRV. Entropy is one such HRV metric which quantifies the degree of irregularity of fluctuations over the course of time. We hypothesize that measures of HRV may improve seizure detection, since acute seizures often reduce heart rate variability.
MATERIALS: Infants with moderate or severe HIE and gestational age =35 weeks undergoing therapeutic hypothermia treatment were enrolled in a prospective EEG monitoring study. All infants underwent conventional EEG-video study for 96h after birth (72h TH + 24h rewarming). EEGs were reviewed for seizures by a single expert; timing of all seizure events was recorded. Infants were divided into two groups, those with seizures and those who never had seizures. All infants had high-resolution (200 Hz), time-synchronized ECG data. For seizure infants, the segment of the ECG recording bounded by the start and stop of each seizure was isolated. For non-seizure infants, 10-minute segments of ECG recording were extracted from points of the recording time-matched to infants in the seizure group. All extracted ECG segments were imported into Kubios HRV for analysis. Automated artifact and ectopic beat detection and correction was employed. HRV metrics evaluated included mean HR, standard deviation of NN intervals (SDNN), standard deviation of HR, and sample entropy (SampEn).
RESULTS: A total of 23 infants were included (15 without seizures, 8 with seizures) with mean GA of 36.8 weeks, 43% female, mean cord pH of 7.02, and median one- and five-minute Apgar scores of 2 and 5. A total of 23 seizure events were noted for the 8 infants with seizures with a median length of 305 seconds, occurring at a median postnatal age of 39.7 hours. There was a marked difference in mean HR between seizure and control periods (115 vs 103 bpm, p=0.02) but not SDNN or standard deviation of the HR. SampEn was significantly lower for seizure periods (1.12 vs 1.33, p=0.01).
CONCLUSION: During seizure events, infants have an elevated heart rate and decreased entropy (measured as SampEn) compared to similar time periods in infants who never had seizures. These quantitative measures could be added to automated seizure detection algorithms to increase accuracy, decrease time to seizure detection and treatment, and improve patient outcomes.
Early recognition of unique amplitude-integrated EEG patterns and clinical semiology of neonatal seizures caused by SCN2A, KCNQ2 and KCNQ3 mutations
Pijpers J, Ping Yee B, Weeke La, Vein A, Smit L, Vilan A, Jacobs E, de Vries L, Steggerda S, Appendino J, Peeters C
aErasmus MC, Rotterdam, Netherlands
BACKGROUND AND PURPOSE: Early recognition of neonatal seizures secondary to pathogenic variants in potassium or sodium channel coding genes is crucial, as these seizures are often resistant to commonly used anti-seizure medications (ASM), but respond well to sodium channel blockers. Recently, a distinctive ictal amplitude-integrated electroencephalogram (aEEG) pattern was described in newborns with KCNQ2 mutations. In this descriptive study of neonatal seizures caused by SCN2A and KCNQ3 pathogenic variants, we report a similar (a)EEG pattern.
METHODOLOGY: International multicentre descriptive study, reporting clinical characteristics, aEEG and conventional EEG findings of 9 newborns with seizures secondary to pathogenic variants in SCN2A and KCNQ3 genes.
RESULTS: Seizures started in the first postnatal week. Seizure semiology typically included tonic posturing with apnea and desaturation. The aEEG showed a characteristic sequence of brief onset with a decrease, followed by a quick rise, and then postictal amplitude attenuation. This pattern correlated with bilateral suppression in the conventional EEG at onset, followed by rhythmic discharges ending in several seconds of post-ictal amplitude attenuation. Interictally, aEEG and conventional EEG activity showed wide degree of findings, ranging from normal to severe encephalopathy. The majority of patients became seizure free upon initiation of a sodium channel blocker.
CONCLUSION: Neonatal seizures caused by SCN2A and KCNQ3 mutations can be recognized by a characteristic ictal aEEG pattern and clinical semiology previously reported only in KCNQ2-associated epilepsy, extending these unique features to other channelopathies. Awareness of this pattern facilitates the prompt initiation of targeted therapy with sodium channel blockers before genetic test results are available.
Experience in the treatment of hypoxic ischaemic encephalopathy with therapeutic hypothermia in a third level neonatal intensive care unit in Argentina
Nieves Ma
aGarrahan Hospital, Buenos Aires, Argentina
BACKGROUND AND AIMS: Therapeutic hypothermia reduces the risk of death or disability in children with moderate severe hypoxic ischemic encephalopathy (HIE). Our objective is to describe the experience of treatment with total body hypothermia in HIE at a third level NICU in South America and assess its safety.
METHODS: Retrospective descriptive study performed at the Garrahan Hospital in Buenos Aires, Argentina. All patients who required hypothermia between 2013 - december 2020 were analyzed. Maternal history, demographic, physical exam, laboratory, imaging studies, cerebral function monitoring (CFM), complications during treatment and clinical evolution and discharge condition were evaluated.
RESULTS: 175 patients were included. 98% of the patients were transferred. The median gestational age was 39 weeks (IQR36-41) with a birth weight of 3400g (3008-3750). Vaginal delivery in 48,6% cases, sentinel event was 40% the prolonged expulsion period. 19,6% of patients were admitted after six hours of life. At admission 66,3% were classified as moderate according to Sarnat – Sarnat scale. Time of life at the start of treatment was 5 hours (4-6). Cord pH was 6,89 (IQR 6,8 - 6,96). 71% of patients required invasive mechanical ventilation at admission. 53,7% of patients had hemodynamic dysfunction, 12% iNO and 1 patient required ECMO. In the neurological area, 50% of patients had clinical seizures. CFM abnormal pattern 41% on entry. 70% required anticonvulsive medication during neonatal period. Normalization of CFM median at 24hs with a range of 24-72. 3% had minor cold-secondary skin lesions. Brain MRI was pathologic in 54%. Mortality was 11,4%. In 1% of patient’s adequacy of therapeutic effort was decided during hospitalization.
CONCLUSIONS: Therapeutic hypothermia is a standard of care for the treatment of patients with HIE. Our results are similar to other series around the world. No significant complications have been reported regarding this treatment. In no case had the therapeutic been suspended.
A post-pandemic playbook: How the COVID-19 pandemic exposed deficiencies in neonatal neurology care
Rosati Ja, Duncan Aa, Nguyen Ja
aUniversity Of Rochester, Rochester, United States
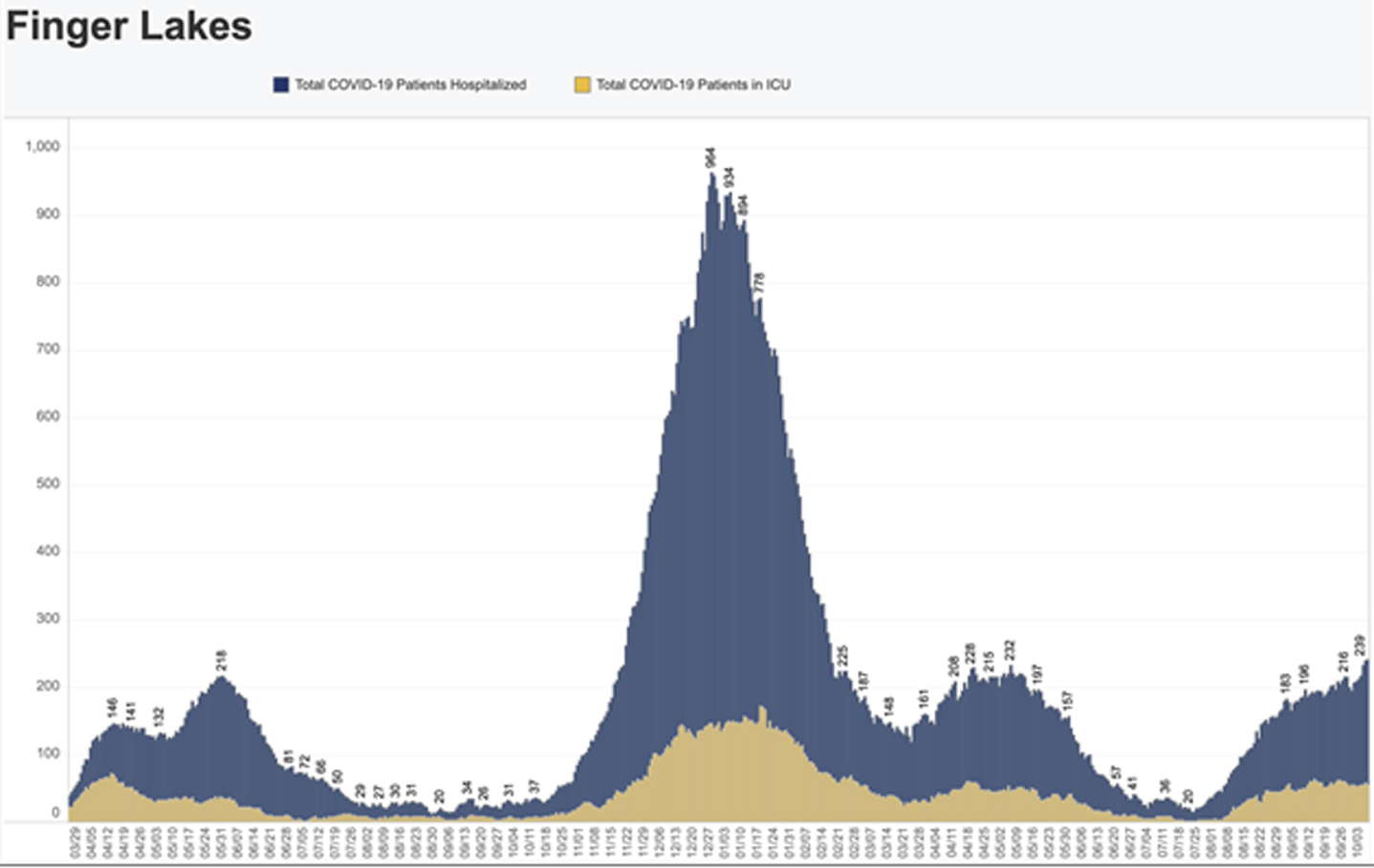
BACKGROUND: The COVID-19 Pandemic caused an unanticipated and radical change in healthcare delivery. Resources and personnel were shifted to meet the needs of a growing population of critically ill COVID patients. While COVID-19 related care burdened the medical system as a whole, care for non-COVID-19 related conditions remained necessary. While the NICU remained relatively spared by the direct effects of COVID-19, indirect effects occurred. While concerns existed in NICU preparedness in low and middle-income countries (Klingenberg et al, 2021), few studies have looked at the effects in higher income countries. The aim of our study was to determine whether there were delays in care in neonatal hypoxic ischemic encephalopathy, which has a time sensitive protocol.
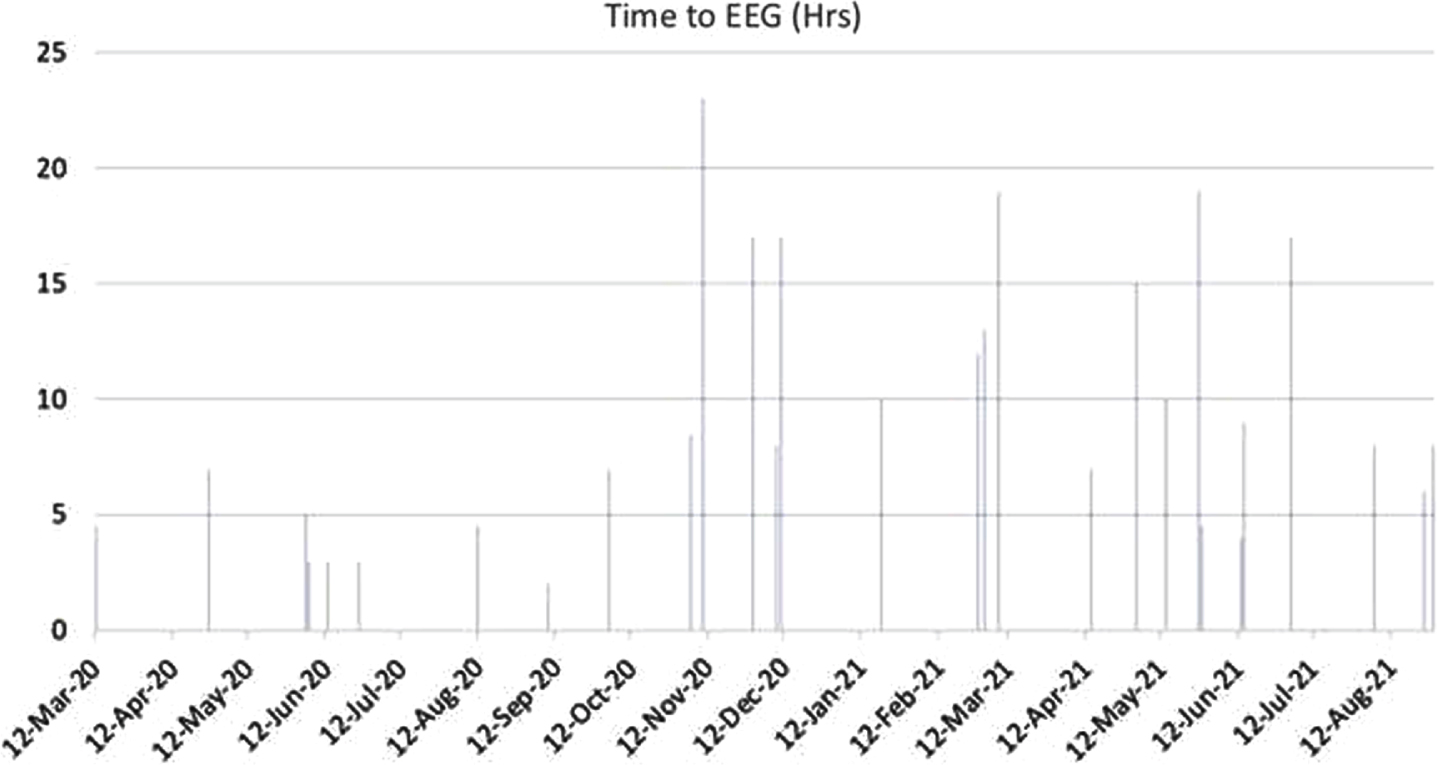
METHODS: At a tertiary care academic center between March 2020-September 2021, 30 neonates diagnosed with neonatal encephalopathy underwent therapeutic hypothermia (TH). Adherence to institutional TH protocol was defined as continuous EEG (cEEG) within 6 hours of TH initiation with repeat at 12-24 hours of normothermia. Time to cEEG placement was evaluated.
RESULTS: In this cohort, time to cEEG appeared to positively correlate with overall COVID-19 hospitalization rates in the region. During Summer 2020 (June-September), time to cEEG consistently was below 6 hours, with an average of 3.4 hours. When COVID-19 cases increased in Fall 2020 to Spring 2021 (November-March), time to cEEG drastically increased to an average of 14.2 hours.
CONCLUSIONS/IMPACT: This data shows an increase in the average time to initiation of cEEG in TH was significantly different between these two time periods of the COVID-19 Pandemic (p=0.0044). There were multiple factors involved in these delays. In consultation of the Epilepsy Department, several factors were identified as barriers to timely initiation of cEEG during times of high hospital census: 1) need to wait for results of COVID-19 testing on patients before EEG hook up as per protocol, 2) EEG technologists required full personal protective equipment during procedures which took time to put on and take off, and the technologist were out of contact to respond to further requests for EEGs during that time, 3) decreased availability of technologists due to quarantine or illness, and 4) decreased available EEG equipment due to lack of replacement parts due to global supply chain issues. While not all of these factors can be controlled, a theme of communication difficulties causing delays emerged. A dedicated Neonatal Neurology team of providers and nurses has the possibility to assist with implementing specific protocols. This team could improve efficiencies of care delivery and provide a pathway for the next set of systemic challenges in our health care system.
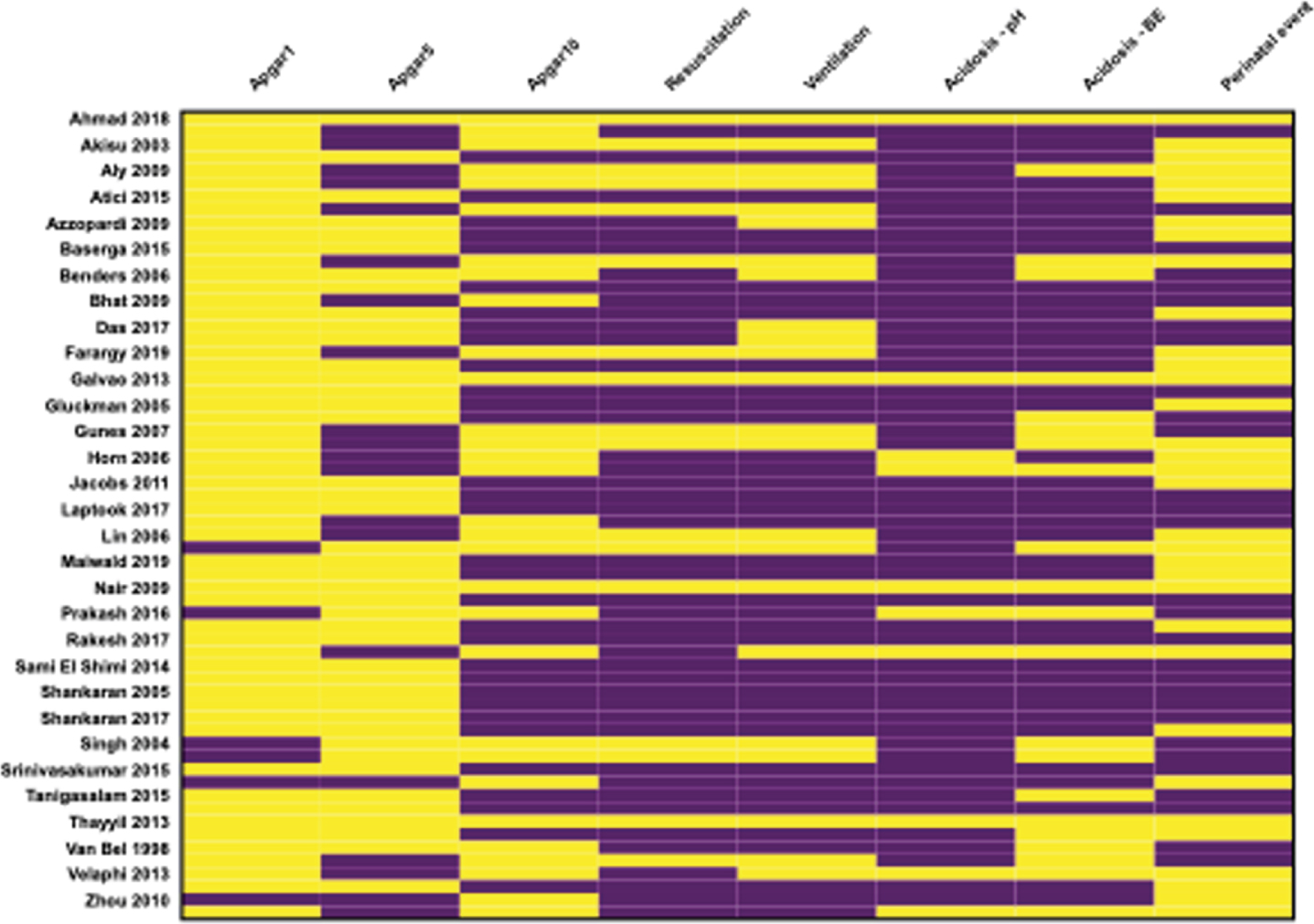
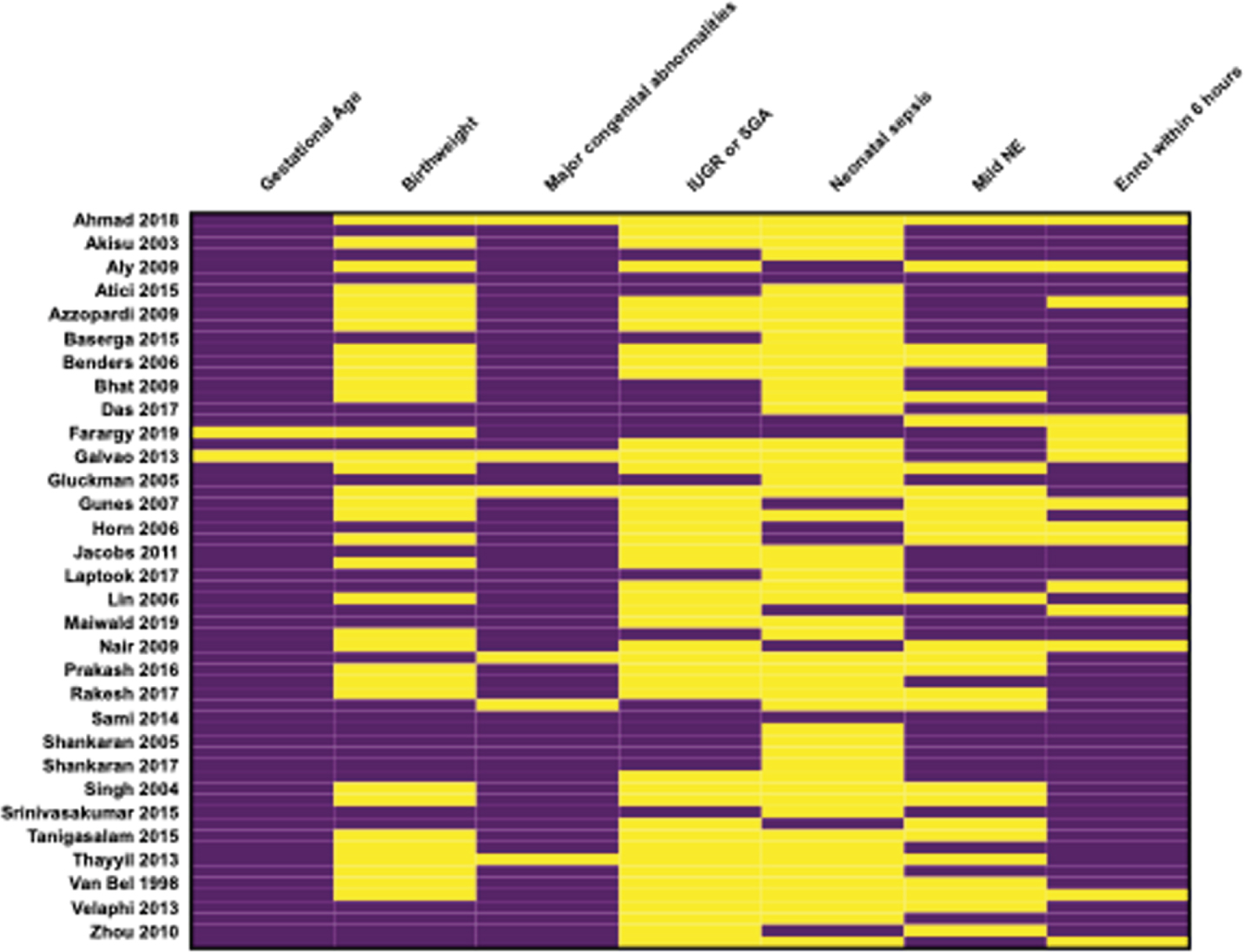
Terminology and participant criteria in trials for neonatal encephalopathy: a systematic review
Hurley Ta, Quirke Fb, Branagan Aa, Finucane Eb, King Ga, Devane Db, Molloy Ea
aTrinity College Dublin, Dublin, Ireland bNational University of Ireland, Galway, Galway, Ireland
BACKGROUND: Appropriate terminology and definitions of neonatal encephalopathy (NE), hypoxic ischaemic encephalopathy (HIE), and perinatal asphyxia (PA) have been debated for the past 20 years. Many, including the American Academy of Pediatrics, have advocated for NE to be used as it does not assume an aetiology, however this is not universally accepted. Moreover, there is no generally accepted case definition criteria for NE/HIE/PA. Instead, the criteria used in trials of therapeutic hypothermia (TH) are frequently employed. However, variation in inclusion and exclusion criteria lead to variation in participants recruited and the severity of NE/HIE. This may explain differences in mortality in control groups between trials. Consistent terminology and case definition criteria would clarify the clinical entity, standardise participant criteria in future trials, and provide greater generalisability of trial results. We completed a systematic review to examine the terminology, definitions, and case participant criteria used in trials of NE/HIE.
METHODOLOGY: A comprehensive search was run in December 2019 in the databases Embase, MEDLINE, CENTRAL, CDSR, the WHO for randomized controlled trials (RCTs) of interventions for the treatment of NE/HIE/PA. Any definition or criteria for NE or HIE were eligible. Follow up studies of original trials were excluded. Outcomes for this study were a description of the terminology, definitions, and participant inclusion/exclusion criteria. 2 reviewers independently screened the results of the literature search, and 2 reviewers independently extracted the data. The qualitative results were synthesised in a narrative summary.
RESULTS: The literature search identified 4375 results, of which 62 were included in the qualitative synthesis. HIE was the most frequently used descriptive term (53/62), next PA (32/62), and NE was least frequent (15/62). Several studies used different terms interchangeably. Inclusion criteria were divided into perinatal asphyxia, of which Apgar scores (58/62) and evidence of acidosis (53/62) were the most frequently used. However, there was significant variation between timing and cut-off values in Apgar score, and cut-off score in pH or base excess. Evidence of neurologic dysfunction most frequently required reduced level of consciousness (LOC) (51/62), reduced tone (50/62), and abnormal reflexes (48/62) but seizures were less frequently required (38/62). The threshold age for exclusion varied frequently between studies and as did the exclusion of participants with mild NE/HIE (35/62).
CONCLUSION: This review identified variation in terminology used, major points of agreement between studies in the inclusion and exclusion criteria for trial participants, and major points of variance between studies. These results will inform a consensus process for developing a definition and case definition of NE/HIE.