
Proceedings of the 13th International Newborn Brain Conference: Other forms of brain monitoring, such as NIRS, fMRI, biochemical
A retrospective cohort study in neonates with hypoxic ischaemic encephalopathy undergoing therapeutic hypothermia: Using EEG-NIRS wavelet coherence to assess neurovascular coupling
Carkeek Kb, Naulaers Ga, Hermans Tc, Dereymaeker Aa, Cilio Mb
aKU Leuven/UZ Leuven Gasthuisberg, Leuven, Belgium
bUCL/Cliniques Universitaires Saint Luc, Brussels, Belgium
cDepartment of Electrical Engineering (ESAT), STADIUS, KU Leuven , Leuven, Belgium
Hypoxic ischaemic encephalopathy (HIE), an important complication of perinatal asphyxia, remains a major health burden. Neonates are classified using the Sarnat score and neonates >35 weeks with moderate/ severe HIE are treated with therapeutic hypothermia (TH). TH improves survival/ decreases disability however 30-50% of mild HIE cases (not offered TH) develop cognitive impairment. Early biomarkers are vital to redefine HIE and better manage these infants. Cerebral monitoring is essential to establish cerebral activity, categorise encephalopathy stages, diagnose seizures, and monitor treatment. EEG and near infrared spectroscopy (NIRS) may be used concomitantly as monitoring tools (combined cerebral activity and haemodynamics) in order to study neurovascular coupling (NVC). NVC as a biomarker may increase sensitivity and specificity for HIE outcome prediction. Limited research exists on NVC in neonates and in HIE where lower oxygen saturation may exist, physiological patterns may be altered. Easy integration of EEG and NIRS, continuous results over long periods, different clinical settings, favors studies. NVC analysis may identify neonates at risk earlier and reduce neurodevelopmental disabilities.
AIM:
-Study continuous EEG and NIRS data in HIE.
-Measure NVC as biomarker for asphyxia severity
-Identify/establish patterns of outcome prediction
-Study effects of physiological variability and medication on NVC.
METHODOLOGY:
-Single center retrospective cohort study
-UZ Leuven, Belgium: 10-year period 2010 - 2020.
-Establish database and inclusions.
-Inclusion: 72 hours TH, EEG and NIRS, magnetic resonance imaging (MRI) < day 10 of life.
-Demographic and clinical data (REDCap system)
-Statistical analysis using GraphPad Prism.
-MRIs scored blinded (Weeke HIE score). Score = 0 considered normal outcome, 1-2 a mild/moderate and >2 severe HIE. Comparisons between groups were performed.
-EEG and single-channel NIRS computed and wavelet coherence analysis used to describe NVC. Data analysed (blinded to MRI outcome)
-Influence of medication on NVC established
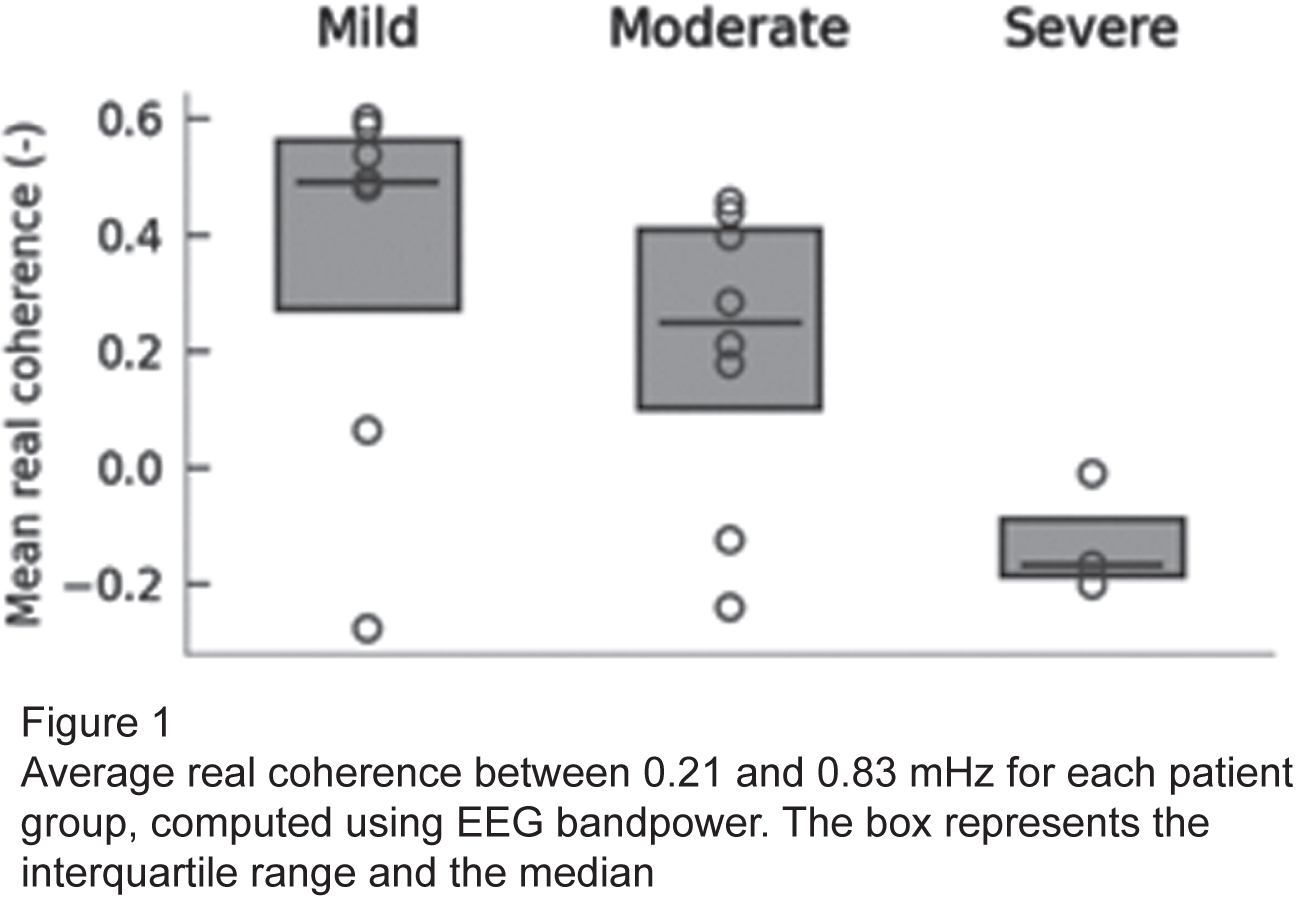
RESULTS: 18/59 neonates admitted for TH met inclusion criteria. Mean gestational age 39 weeks, 55.5% female, 33.3% inborn and 38.9% born via emergency cesarian section. Mean Apgar scores at 1, 5 and 10 minutes were 1.2, 3.1 and 5.4 respectively. Fourteen (77.8%) required intubation at birth and mean Cord pH was 6.95. The average initiation time of TH was 2 hours 21 minutes from birth. Thirteen (72.2%) required inotropic support and all were sedated. Seizures were noted in 33.3% and 9 received Phenobarbital. Overall survival was 94.4% and MRI scores were normal in 38.9% and severe in 16.7%. NVC results showed most coupling occuring between 20-80 minutes after starting TH and increased coupling related to improved outcome. Between 0.21 and 0.83 mHz, real coherence computed using bandpower, was highest (positive) in normal group and lowest (negative) in severe group. (Figure 1)
CONCLUSION: This study validated in a large cohort the measurement of NVC using wavelet coherence analysis.
Bibliography:
[1] Chiang MC, Jong YL, Lin CH Therapeutic hypothermia for neonates with hypoxic ischemic encephalopathy. Pediatr Neonatol.2017 Dec.
[2] M. Douglas-Escobar, M.D. Weiss. Hypoxic–ischemic encephalopathy: a review for the clinician JAMA Pediatr, 169 (2015), pp. 397-403
[3] M.C. Chiang, Q.M. Ashraf, J. Ara, O.P. Mishra, M. Delivoria-Papadopoulos. Mechanism of caspase-3 activation during hypoxia in the cerebral cortex of newborn piglets Neurosci Lett, 421 (2007), pp. 67-71
[4] Chalak LF, Tian F, Adams-Huet B, et al (2017) Novel Wavelet Real Time Analysis of Neurovascular Coupling in Neonatal Encephalopathy. Sci Rep 7:. https://doi.org/10.1038/srep45958
[5] M.V. Johnston, A. Fatemi, M.A. Wilson, F. Northington. Treatment advances in neonatal neuroprotection and neurointensive care. Lancet Neurol, 10 (2011), pp. 372-382
[6] J.H. Skranes, M. Elstad, M. Thoresen, F.M. Cowan, T. Stiris, D.Fugelseth. Hypothermia makes cerebral resistance index a poor prognostic tool in encephalopathic newborns Neonatology, 106 (2014), pp. 17-23
[7] D Hendrikx, A Smits, M Lavanga, O De Wel, L Thewissen, K Jansen, et al. Measurement of Neurovascular Coupling in Neonates. Front Physiol (2019) 10:65. Epub 2019/03/06. doi: 10.3389/fphys.2019.00065. PubMed PMID: 30833901; PubMed Central PMCID: PMCPMC6387909.
[8] TH Schwartz . Neurovascular coupling and epilepsy: hemodynamic markers for localizing and predicting seizure onset. Epilepsy Curr (2007) 7(4):91-4. Epub 2007/08/19. doi: 10.1111/j.1535-7511.2007.00183.x. PubMed PMID: 17694162; PubMed Central PMCID: PMCPMC1941907.
[9] N Roche-Labarbe, F Wallois, E Ponchel, G Kongolo, R Grebe. Coupled oxygenation oscillation measured by NIRS and intermittent cerebral activation on EEG in premature infants. Neuroimage (2007) 36(3):718-27. Epub 2007/05/08. doi: 10.1016/j.neuroimage.2007.04.002. PubMed PMID: 17482837.
[10] A.D. Edwards, P. Brocklehurst, A.J. Gunn, H. Halliday, E. Juszczak, M.Levene, et al. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data. BMJ, 340 (2010), p. c363
[11] S.E. Jacobs, M. Berg, R. Hunt, W.O. Tarnow-Mordi, T.E. Inder, P.G.Davis. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev (1) (2013), p. CD003311
[12] P.D. Gluckman, J.S. Wyatt, D. Azzopardi, R. Ballard, A.D. Edwards, D.M.Ferriero, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet, 365 (2005), pp. 663-670
[13] S. Shankaran, A.R. Laptook, R.A. Ehrenkranz, J.E. Tyson, S.A. McDonald, E.F. Donovan, et al. Whole-body hypothermia for neonates with hypoxic–ischemic encephalopathy. N Engl J Med, 353 (2005), pp. 1574-1584
[14] D.V. Azzopardi, B. Strohm, A.D. Edwards, L. Dyet, H.L. Halliday, E.Juszczak, et al. Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med, 361 (2009), pp. 1349-1358
[15] G. Simbruner, R.A. Mittal, F. Rohlmann, R. Muche, neo.nEURO.network Trial Participants. Systemic hypothermia after neonatal encephalopathy: outcomes of neo.nEURO.network RCT. Pediatrics, 126 (2010), pp. e771-e778
[16] S.E. Jacobs, C.J. Morley, T.E. Inder, M.J. Stewart, K.R. Smith, P.J.McNamara, et al. Whole-body hypothermia for term and near-term newborns with hypoxic–ischemic encephalopathy: a randomized controlled trial
[17] M.A. Tagin, C.G. Woolcott, M.J. Vincer, R.K. Whyte, D.A. Stinson. Hypothermia for neonatal hypoxic ischemic encephalopathy: an updated systematic review and meta-analysis. Arch Pediatr Adolesc Med, 166 (2012), pp. 558-566
[18] Hendrikx D, Thewissen L, Smits A, Naulaers G, Allegaert K, Van Huffel S, Caicedo A. Nonlinear Transfer Entropy to Assess the Neurovascular Coupling in Premature Neonates. Adv Exp Med Biol. 2020;1232:11-17. doi: 10.1007/978-3-030-34461-0_2. PMID: 31893388.
[19] Smits A, Thewissen L, Dereymaeker A, Dempsey E, Caicedo A, Naulaers G. The Use of Hemodynamic and Cerebral Monitoring to Study Pharmacodynamics in Neonates. Curr Pharm Des. 2017;23(38):5955-5963. doi: 10.2174/1381612823666170918124419. PMID: 28925890.
Interaction between Neuronal and Cerebral Metabolic Activity in Neonates with Hypoxic-Ischemic Encephalopathy Undergoing Therapeutic Hypothermia
Chowdhury Ra,b, Mahdi Za, Desnous Ba,c, Marandyuk Ba, Benhmida Ia, Birca Aa,c, Pinchefsky Ea,c,1, Dehaes Ma,d,1
aCHU Sainte-Justine affiliated with University of Montreal, 3175 Cote Sainte-catherine, Canada
bInstitute of Biomedical Engineering, University of Montréal, Montreal, Canada
cDivision of Neurology, Department of Neuroscience, University of Montreal and Sainte-Justine University Hospital Center, Montreal, Canada
dDepartment of Radiology, Radio-oncology and Nuclear Medicine, University of Montreal, Montreal, Canada
1Equal contribution as co-senior author
BACKGROUND AND PURPOSE: The understanding of the interaction between neuronal activity and cerebral metabolic activity in infants with hypoxic-ischemic encephalopathy (HIE) undergoing therapeutic hypothermia (TH) is incomplete. The recovery of electroencephalography (EEG) background after TH is a good prognostic sign [1,2]. The goal of this study is to assess the interaction between neuronal and cerebral metabolic activity and determine early marker of EEG background recovery based on metabolic activity.
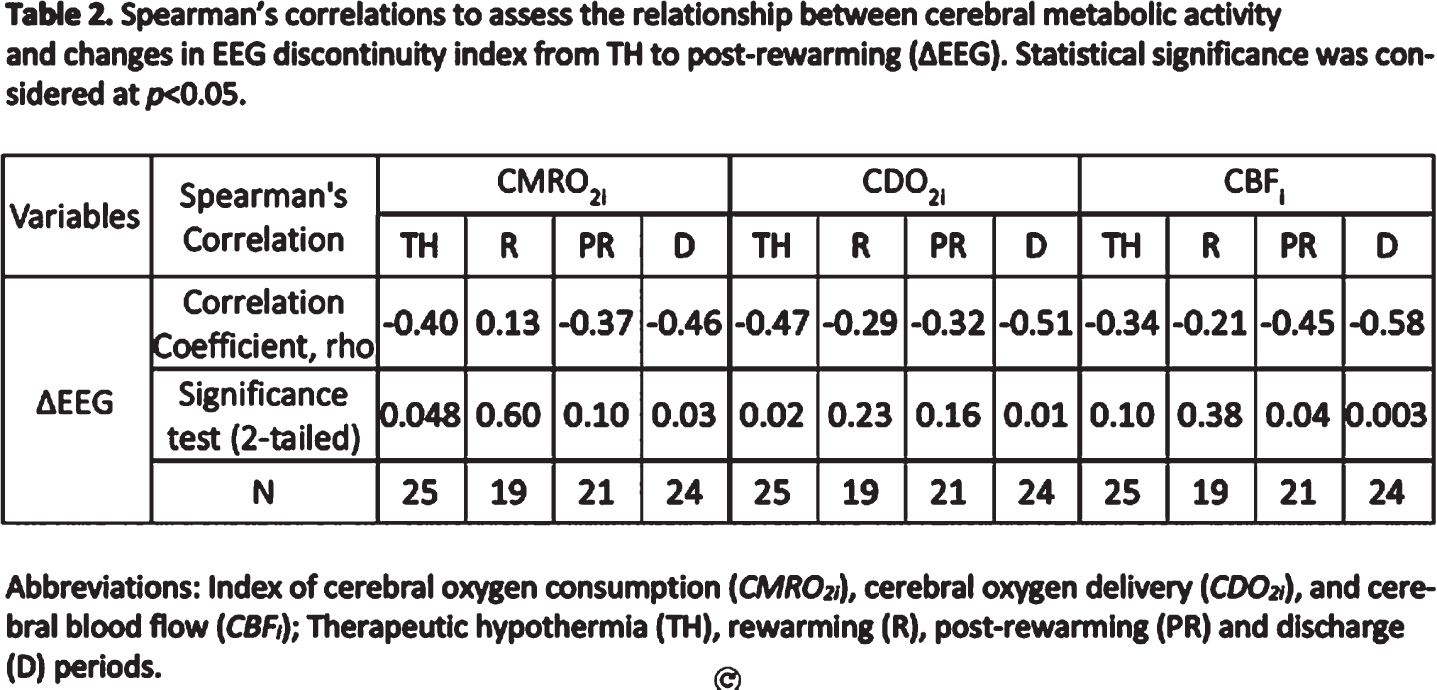
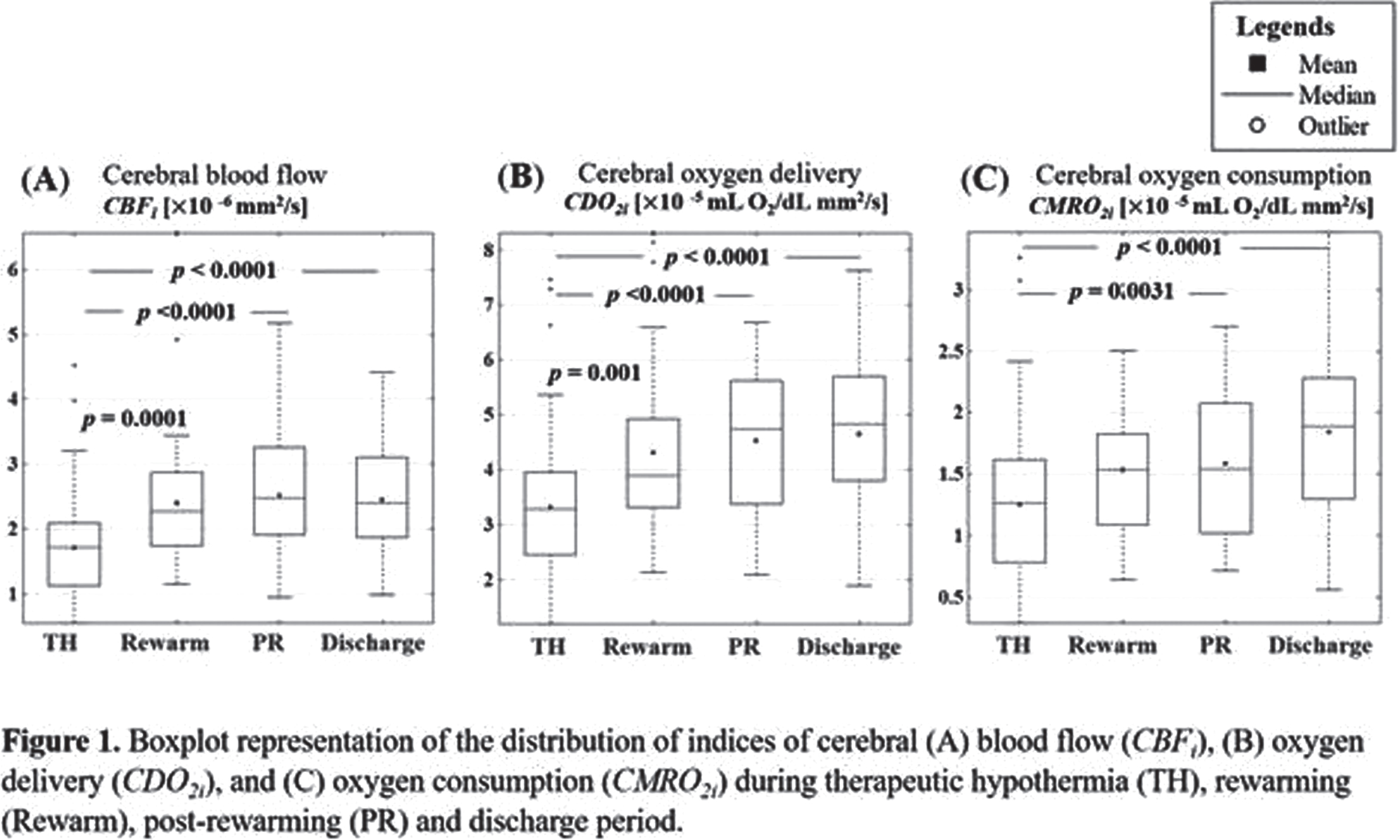
METHODS: HIE neonates who underwent moderate TH (33-34°C for 72h) followed by rewarming (0.5°C/h over 6h) were recruited. Bedside optical monitoring [3] was used to measure indices of cerebral blood flow (CBFi in mm2/s), cerebral oxygen delivery (CDO2i in mL O2 /dL·mm2/s) and cerebral oxygen consumption (CMRO2i in mL O2 /dL·mm2/s) during TH, rewarming, post-rewarming and discharge periods. Quantitative EEG discontinuity index [1,4], represented by the proportion of epochs of low voltage activity <25μV (peak-to-peak) for a duration of 2 seconds, was calculated for 6 hours intervals during TH, rewarming and post-rewarming periods. Changes in cerebral metabolic variables between the monitoring periods were assessed using a general linear mixed model accounting for repeated measures followed by Tukey-Kramer correction. Relationship between cerebral metabolic variables and changes in EEG discontinuity index from TH to post-rewarming (ΔEEG) were assessed using Spearman’s rank-order correlation.
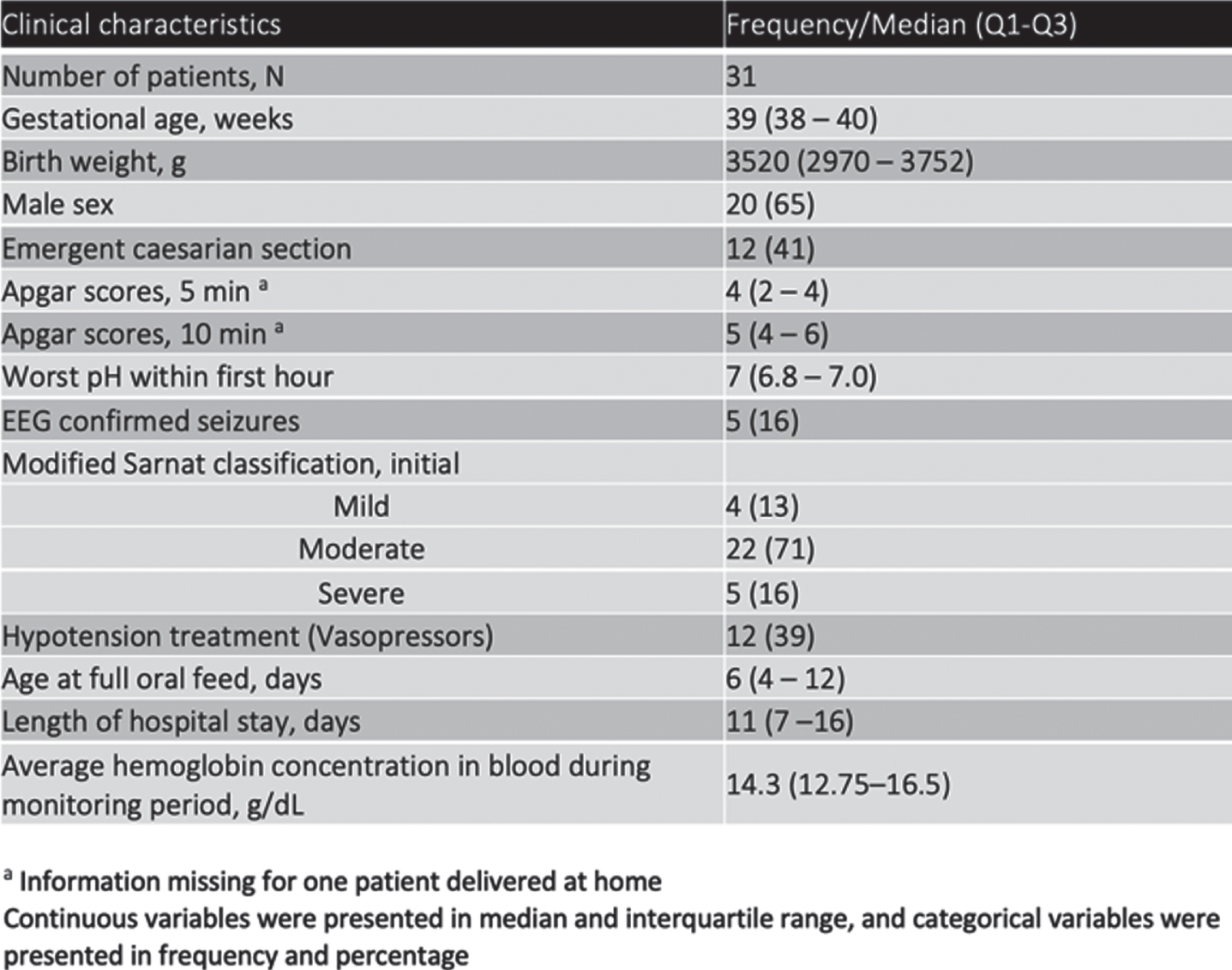
RESULTS: Thirty-one neonates were included (Table 1). We noticed an increase in CBFi and CDO2i during and after rewarming, reflecting an increased cerebral oxygen demand with increased core body temperature (Figure 1). As neonates became normothermic, CBFi, CDO2i and CMRO2i increased, which may indicate a gradual recovery post-therapy. CMRO2i and CDO2i values during TH and discharge showed significant negative correlation with ΔEEG (Table 2). Similarly, CBFi values on post-rewarming and discharge showed significant negative correlation with ΔEEG. Looking more in-depth in these relationships, we noticed that low CMRO2i and CDO2i values during TH were associated with an increase in EEG discontinuity index (>10%) from TH to post-rewarming (Figure 2). On the other hand, high CMRO2i and CDO2i values during TH were associated with a decrease or a small increase in EEG discontinuity index (<10%).
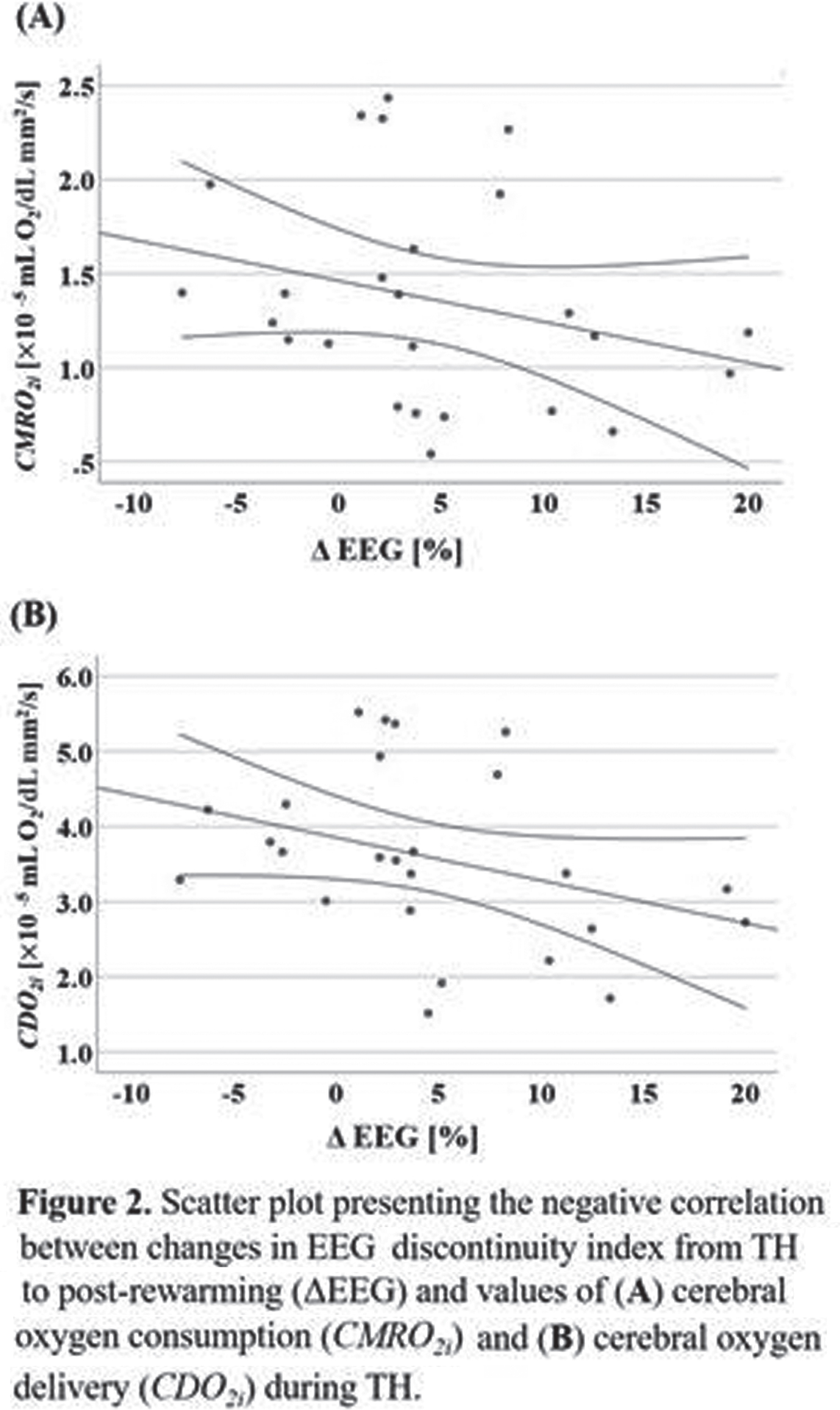
CONCLUSION: CMRO2i and CDO2i values during TH may provide an early indication of whether there will be a favorable EEG evolution following rewarming. A better understanding of the interaction between neuronal and metabolic activity during TH may help optimize duration of rewarming based on individual patient factors. Future work will investigate the association of these interactions with MRI findings post-TH and neurodevelopment outcome at 2 years.
Bibliography:
[1] Birca A et al. Clin Neurophysiol. 2016;127:2087-94.
[2] Nash KB et al. Neurology. 2011;76:556-62.
[3] Dehaes M et al. J Cereb Blood Flow Metab. 2014;34:87-94.
[4] Tsuchida TN et al. J Clin Neurophysiol. 2013;30:161-73.
Relationship between cerebral blood flow and oxygen metabolism with neurological status at term-equivalent age in infants born preterm
Cote Corriveau Ga, Beaulieu Oa, Gagnon Ma, Gagnon Ma, Chowdhury Ra, Simard Ma, Dehaes Ma, Luu Ta
aSainte-Justine University Hospital Center, 250 Saint-joseph East Apt 205 Montreal, Canada
BACKGROUND: Infants born at 29-36 weeks’ gestational age (GA) are at risk of neurodevelopmental problems. Early identification of those benefiting the most from specialized follow-up is needed. Non-invasive bedside monitoring techniques could provide better insight into their brain development and lead to new screening strategies. We hypothesize that cerebral blood flow and oxygen metabolism monitored by advanced near infrared spectroscopy (NIRS) are valid biomarkers of cerebral development and correlate with the neuromotor status at term-equivalent age (TEA).
METHODS: Preterm infants (n=150) born 29-36 weeks’ GA and admitted in the neonatal intensive care unit were consecutively recruited in this prospective observational cohort study. We performed advanced NIRS from one week of life to TEA and derived indices of cerebral blood flow (CBFi) and cerebral metabolic rate of oxygen consumption (CMRO2i). Neuromotor examination was completed at TEA. The relationship between changes in advanced NIRS parameters over time and neuromotor status was assessed using logistic regression analysis.
RESULTS: Overall, 80 and 78 participants had valid repeated measures of CBFi and CMRO2i, respectively. At TEA, 71 had an abnormal neuromotor exam. Higher GA was associated with steeper CBFi (β=0.44; P<0.001) and CMRO2i (β=0.44; P<0.001) slopes. Adjusting for GA, neither CBFi (OR 2.09; 95% CI 0.62-7.01) nor CMRO2i (OR 1.14; 95% CI 0.42-3.14) slopes were associated with neuromotor exam at TEA.
CONCLUSIONS: In this population, cerebral NIRS parameters did not correlate with infant neuromotor status at TEA. GA was associated with more rapid increase in cerebral blood flow and oxygen metabolism. These new biomarkers could provide complementary information to neuromotor examination of cerebral development.
Multi-modal monitoring of infants with hypoxic-ischaemic encephalopathy and prediction of short-term outcome
Garvey Aa,b, Walsh Ba,b, Mathieson Sa,b, Moore Mc, O’Toole Ja,b, Livingstone Va,b, Pavel Aa,b, Finn Db, Boylan Ga,b, Murray Da,b, Dempsey Ea,b
aInfant Research Centre, Cork, Ireland
bDepartment of Paediatrics and Child Health, University College Cork, Cork, Ireland
cDepartment of Radiology, Cork University Hospital, Cork, Ireland
BACKGROUND: Despite significant advances in treatment, hypoxic-ischaemic encephalopathy (HIE) still carries a significant risk of brain injury and adverse neurodevelopmental outcome.[1] Early identification of at risk infants is critical to optimise intervention. We aimed to investigate the ability of currently available, bedside monitoring techniques to predict short-term outcome in infants with all grades of HIE.
METHODS: Prospective observational study conducted in a tertiary neonatal intensive care unit, Cork, Ireland. Infants with all grades of HIE had continuous video electroencephalography (EEG), non-invasive cardiac output monitoring (NICOM) and near-infrared spectroscopy (NIRS) commenced within the first 6 hours of admission to the NICU. One-hour epochs of time-synchronised data were selected at 6 and 12 hours of age to assess their ability to predict short-term outcome. All infants had brain magnetic resonance imaging (MRI) within the first 10 days of life and adverse outcome was defined as abnormal MRI (Barkovich score) or death.
RESULTS: Fifty-seven infants were included (27 mild, 24 moderate, 6 severe). Median gestational age was 39.9 weeks (IQR 38.1 – 40.7) and mean birth weight was 3.4 kgs (SD 0.5 kgs). MRIs were performed on day of life 5 (IQR 3-5). NIRS and EEG data was available for 34 infants at 6 hours and 56 infants at 12 hours. 13 infants had NICOM data at 6 hours and 22 infants at 12 hours. 3 infants died. Twenty-one percent of infants with mild, 29% with moderate and 84% with severe HIE had an adverse outcome. At 6 hours, no individual marker significantly predicted short-term outcome. NICOM markers had the highest AUC for adverse outcome at 6 hours; cardiac output 0.76 (95%CI 0.5-1, p=0.1). Stroke volume and heart-rate had the highest AUC for moderate-severe MR injury; (AUC 0.75, 95% CI 0.7-1, p=0.6) and (AUC 0.83, 95% CI 0.6-1, p=0.5) respectively. At 12 hours, qualitative grading of the EEG predicted moderate-severe MR injury (AUC 0.84, 95%CI 0.7-1, p<0.001). Quantitative features of EEG power also significantly predicted adverse outcome. NIRS measurements (cSO2 and FTOE) were not helpful in identifying infants with MRI injury and combining modalities did not improve prediction.
CONCLUSION: Whilst NICOM derived measures at 6 hours were associated with adverse outcome, the best individual predictor of outcome was qualitative and quantitative EEG findings at 12 hours of age.
Bibliography:
1. Jacobs SE, Berg M, Hunt R, Tarnow-Mordi WO, Inder TE, Davis PG. Cooling for newborns with hypoxic ischaemic encephalopathy. The Cochrane database of systematic reviews. 2013(1):CD003311.
Investigating cerebral perfusion to explore the etiology of intraventricular hemorrhage in extremely preterm infants
Keister Fa, Stritzke Ab, Mohammad Ka, Elsayed Ec, Zein Ha, Ghosh Aa, Consoli Aa, Leijser La,b
aUniversity of Calgary, Cumming School of Medicine, Calgary, Canada
bAlberta Health Services, Calgary, Canada
cSaskatchewan Health Authority, Regina, Canada
BACKGROUND: Germinal matrix - Intraventricular hemorrhage (GMH-IVH) occurs in up to 35% of extremely preterm infants born at <29 weeks’ gestation (1). GMH-IVH predominantly develops within the first 72 hours of birth and can be associated with adverse neurodevelopmental outcomes. The risk factors for GMH-IVH are still incompletely understood. A role for changes in cerebral blood flow and perfusion in GMH-IVH development has been suggested (2). The objective of our study was to explore the relationship between cerebral perfusion measured by Near-InfraRed Spectroscopy (NIRS) during the first 72 hours of birth and GMH-IVH development in extremely preterm infants.
METHODOLOGY: A prospective, observational cohort study in extremely preterm infants born at a tertiary Neonatal center in Calgary, Canada. Cerebral perfusion values expressed as cerebral regional oxygen (crSO2) and measured using continuous NIRS monitoring throughout the first 72 hours after birth were collected along with relevant clinical data. Serial cranial ultrasounds (cUS) were conducted at 6, 12, 24, 48, and 72 hours of birth to assess the timing of GMH-IVH development and its progression. An unequal variance and 2-tailed t-test was performed to compare crSO2 values during the 5 time intervals between cUS scans between infants with and without GMH-IVH.
RESULTS: Preliminary results consist of 20 infants (15 females) undergoing NIRS and 5 cUS scans each. Eleven of the 20 infants (55%) developed a GMH-IVH in the first 72 hours. Infants with and without GMH-IVH were comparable for mean (SD) gestational age and birth weight; 25.4 (1.2) weeks and 803 (183) grams and 25.5 (1.3) weeks and 691 (122) grams, respectively. Also, no significant differences in other clinical parameters were found between both groups. There were however significant differences in mean crSO2 values between infants with and without GMH-IVH when comparing values during the time-intervals between the 5 cUS scans (p<0.05 for all time-intervals): Infants with GMH-IVH had higher and more fluctuating mean crSO2 values compared to infants without GMH-IVH (Figure 1).
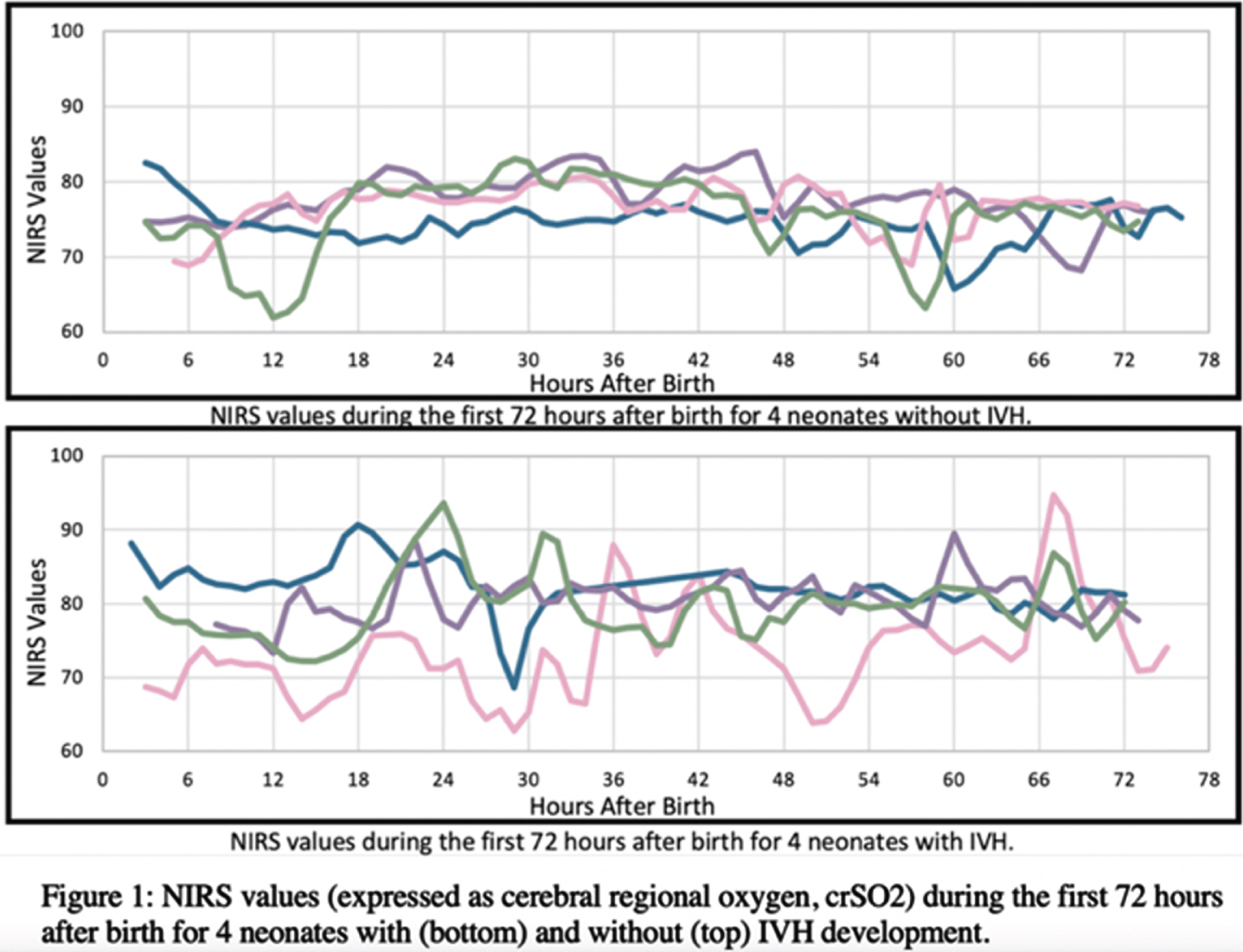
CONCLUSIONS: Infants with GMH-IVH had higher and more fluctuating mean crSO2 values in the first 72 hours after birth compared to infants without GMH-IVH. Results suggest that higher and unstable cerebral perfusion during the first 72 hours may contribute to GMH-IVH development, and therewith possible adverse outcomes, in extremely preterm infants. Further investigation of modifiers of cerebral perfusion is required to prevent GMH-IVH development.
Bibliography:
[1] Özek E, Kersin SG. Intraventricular hemorrhage in preterm babies. Turkish Archives of Pediatrics/Türk Pediatri Arsivi. 2020;55(3):215.
[2] Leijser LM, de Vries LS. Preterm brain injury: Germinal matrix–intraventricular hemorrhage and post-hemorrhagic ventricular dilatation. Handbook of clinical neurology. 2019 Jan 1;162:173-99.
Perioperative neuromonitoring of neonatal hydrocephalus in Uganda
Rajaram Aa,b, Kemigisha Me, Vadset Ta,b, Seruwu Me, Vyas Ra,b, Magombe Je, Hsiao Ca,b, Nsubuga Be, Tatz Ja,b, Natukwatsa De, Playter Ka,b, Wabukoma Me, Peterson Mf, Nalule Ee, Woglom Ma,b, Lippman Ra,b, Wandukwa Je, Queally Jd, Mulondo Re, Schiff Sf, Grant Pa,b,c, Sutin Ja,b, Mbabazi Ee, Warf Bg, Lin Pa,b
aDivision of Newborn Medicine, Boston Children’s Hospital, Boston, USA
bFetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children’s Hospital, Boston, USA
cDepartment of Radiology, Boston Children’s Hospital, Boston, USA
dDepartment of Psychiatry, Boston Children’s Hospital, Boston, USA
eCURE Children’s Hospital of Uganda, Mbale, Uganda
fCenter for Neural Engineering, Pennsylvania State University, State College, USA
gDepartment of Neurosurgery, Boston Children’s Hospital, Boston, USA
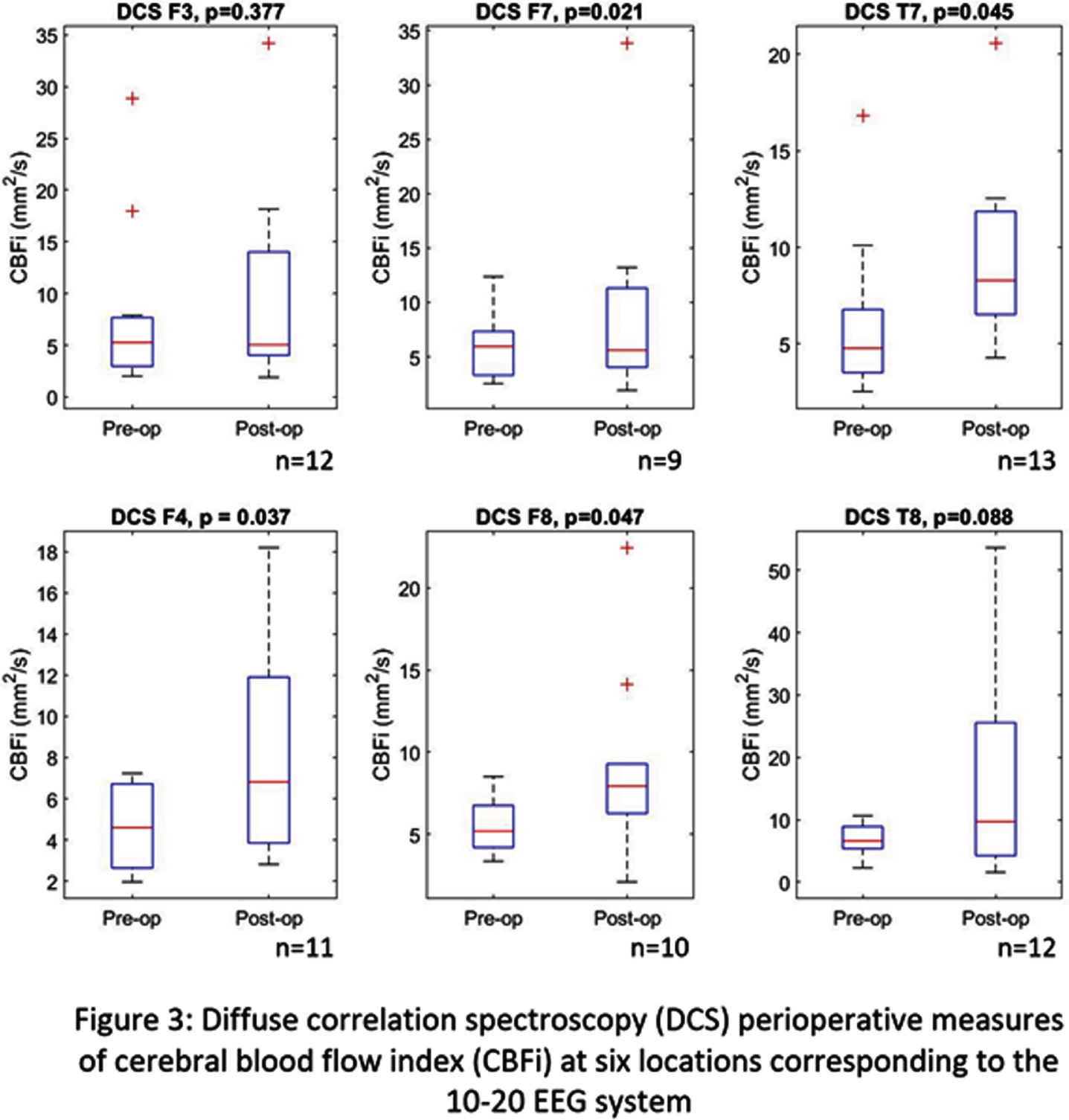
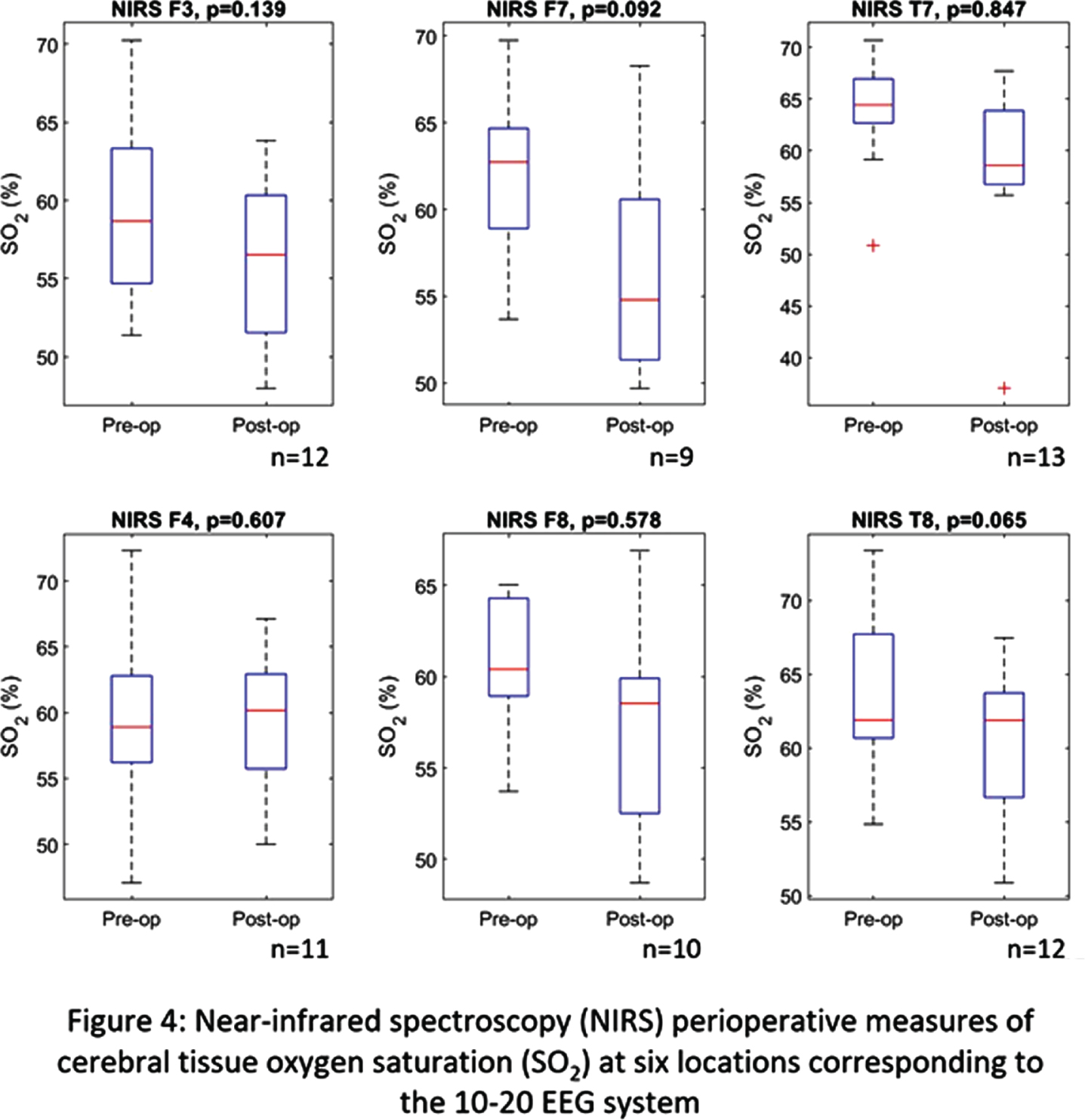
MOTIVATION: Neonatal hydrocephalus, defined by an excessive build-up of cerebrospinal fluid (CSF) in the brain’s ventricles, can lead to an increased intracranial pressure and compression of brain tissue, resulting in significant long-term injury or death. Sub-Saharan Africa sees 100,000 cases of post-infectious hydrocephalus (PIH) annually [1]. Ventriculoperitoneal shunts (VPS) are traditionally implemented to alleviate CSF build-up but utilize a permanent fixture requiring life-long maintenance while experiencing a two-year failure rate of 40% [2]. Endoscopic third ventriculostomy combined with choroid plexus cauterization (ETV/CPC) is an effective, low-resource alternative to VPS to improve CSF drainage while minimizing its production. ETV/CPC requires less post-operative care and has a lower rate of infection [3], but treatment failure remains a significant problem. CT and ultrasound (US) imaging are essential to diagnose PIH but are limited in routine monitoring and predicting outcome. Biomedical optics offer a non-invasive, and cost-effective approach to bedside monitoring of cerebral physiology. Near-infrared (NIRS) and diffuse correlation spectroscopy (DCS) can quantify cerebral tissue oxygen saturation (SO2) and cerebral blood flow (CBFi), which have shown to provide an early indication of brain development/injury in premature infants and those with post-hemorrhagic hydrocephalus [4,5].
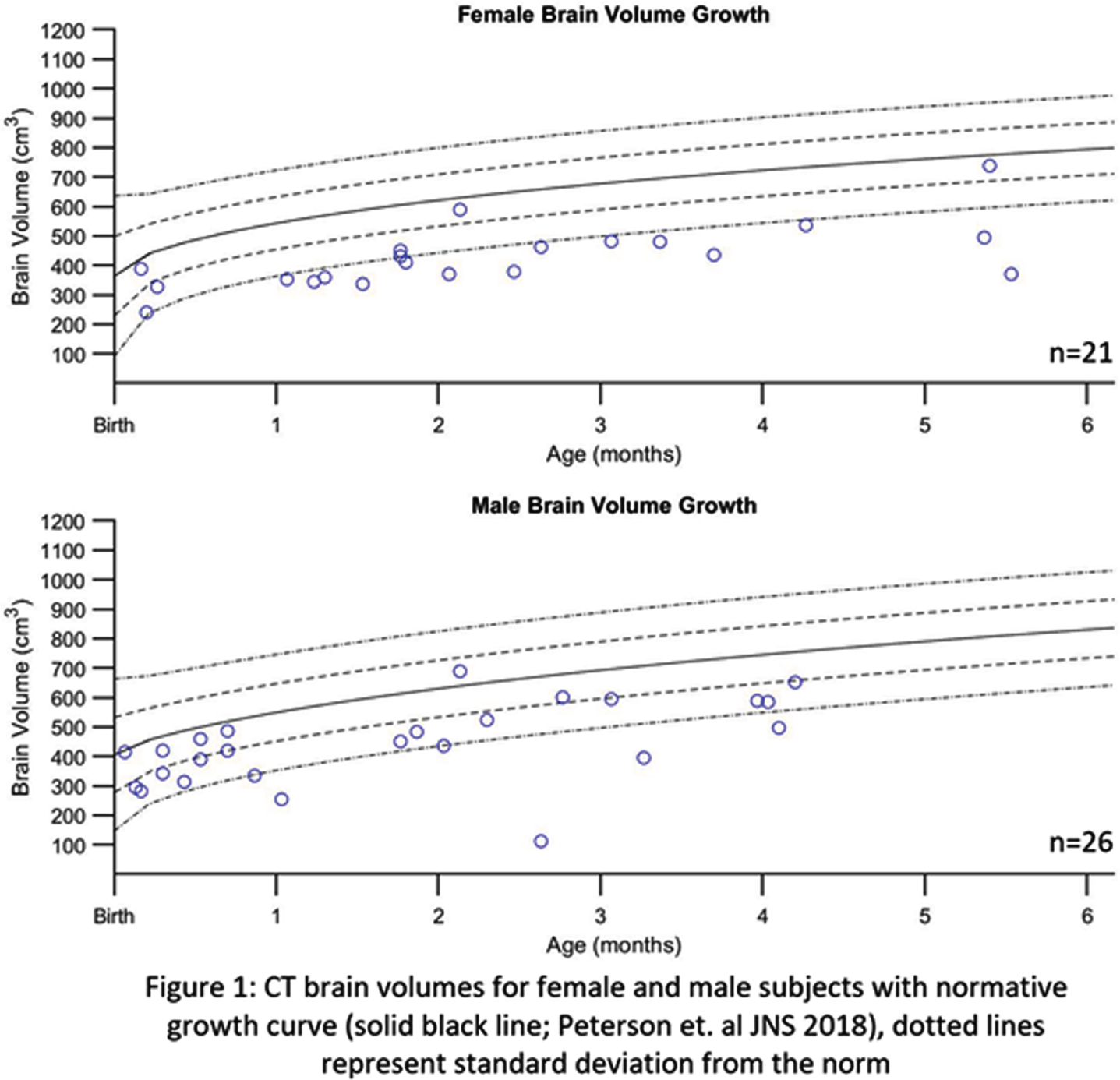
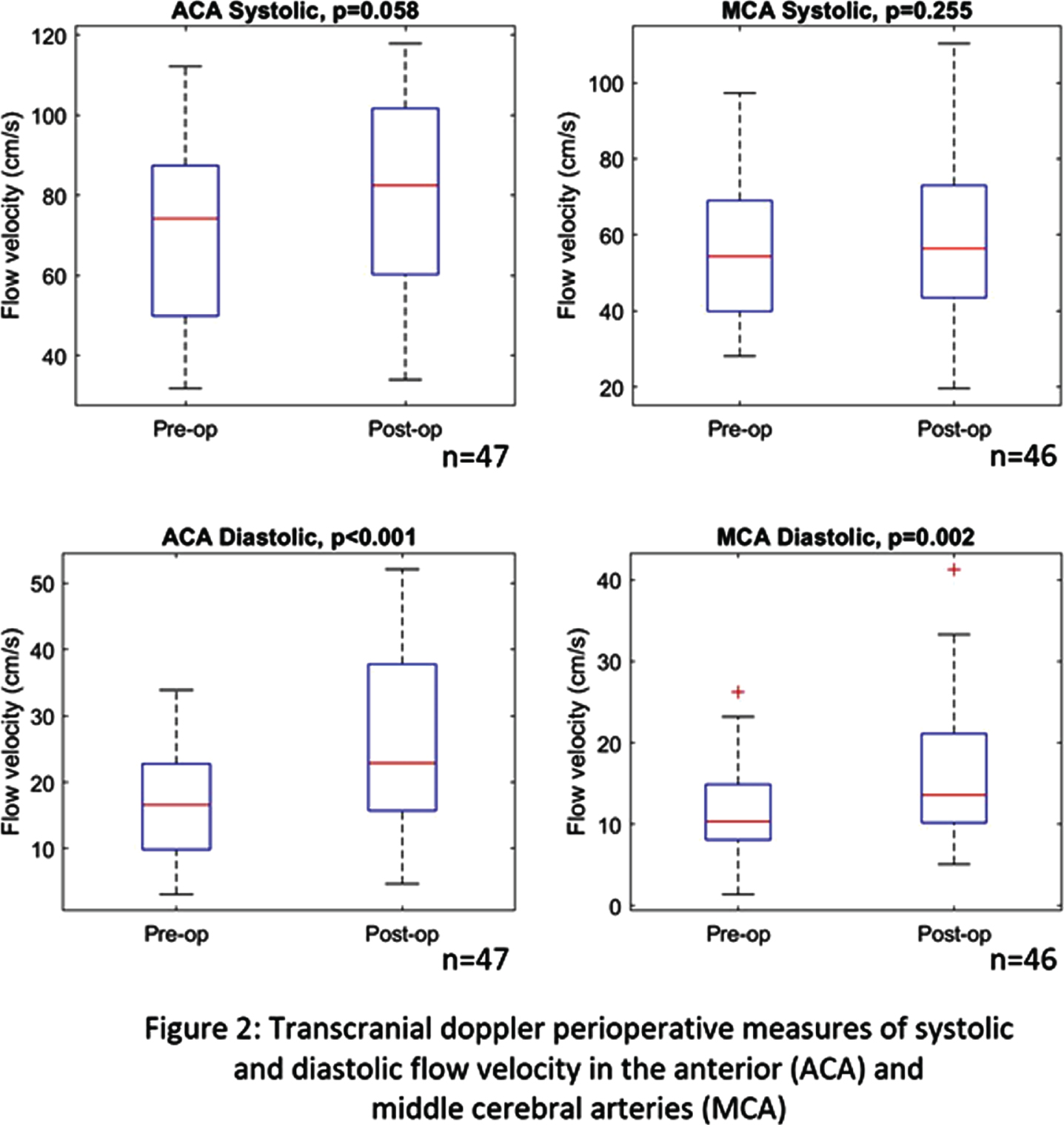
METHODOLOGY: This work investigates perioperative monitoring of ETV/CPC at CURE Children’s Hospital of Uganda (CCHU), a neurosurgical center with likely the highest volume of PIH in the world. Infants at CCHU scheduled for surgical intervention were recruited. Following consent, pre-operative measurements of transcranial doppler (LOGIQ V5, GE) characterized systolic and diastolic flow velocity in the anterior (ACA) and middle cerebral arteries (MCA) and NIRS/DCS (MetaOx, ISS) quantified SO2 and CBFi at six frontal/temporal locations. TCD and NIRS/DCS monitoring were repeated post-operatively within two days of surgery.
RESULTS AND SIGNIFICANCE: ETV/CPC was performed on 47 infants. Pre-operative CT images were segmented to quantify brain tissue volume and compared to a normative brain volume growth curve [6] (Figure 1); subjects consistently failed to meet the normative curve, indicating the severity of their initial condition. Perioperatively, a statistically significant difference was found for TCD’s diastolic flow (Figure 2) and CBFi at four of the six measured locations (Figure 3). No significant change was noted for SO2 measures (Figure 4). Optical measurements with significant motion or failing to adequately interrogate brain tissue (due to large subdural collections) were excluded from analysis. Future work seeks to correlate these findings to treatment failure and clinical outcome. Bedside neuromonitoring of cerebral physiology could provide an early indication of treatment efficacy and has potential to alter patient management and improve outcomes associated with PIH in low-resource, high-volume settings.
References:
[1] Warf, J.Neurosurg Ped, 2011
[2] Kulkarni, J.Neurosurg Ped, 2013
[3] Di Rocco, Child Nerv Sys, 2006
[4] Lin, Sci Rep, 2016
[5] Rajaram, Brain Sci, 2020
[6] Peterson, JNS, 2018
NIRS in preterm infants before and after red blood cells transfusion
Sharafutdinova Da, Ionov O, Balashova E, Kirtbaya A, Golubtsova Y, Ryndin A, Zubkov V, Degtyarev D
aNational Medical Research Center For Obstetrics, Gynecology And Perinatology Named Academician V.i. Kulakov Of The Mini, Moscow, Russian Federation
bSechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenov University), Moscow, Russian Federation
PURPOSE: To determine the difference between cerebral and regional tissue oxygenation measured by near-infrared spectroscopy (NIRS) before and after red blood cells transfusion in extremely and very low birth weight infants.
MATERIALS OR METHODOLOGY: The NIRS prospective study enrolled extremely and very low birth weight infants from neonatal intensive care unit (N=55). Oximetry indicators Me (q1-q3): cerebral tissue oxygenation (CrSO2), splanchnic tissue oxygenation (SrSO2), renal tissue oxygenation (RrSO2), SCOR = SrSO2/CrSO2, Cerebral Fractional Tissue Oxygen Extraction (C-FTOE) = (SpO2 – CrSO2) / SpO2, Renal Fractional Tissue Oxygen Extraction (R-FTOE) = (SpO2 – RrSO2) / SpO2, Splanchnic Fractional Tissue Oxygen Extraction (S-FTOE) = (SpO2 – SrSO2) / SpO2 were continuously monitored using a neonatal sensor before, during and after red blood cells transfusion. Red blood cells transfused based on restrictive strategy. Absolute indication for red blood cells transfusion was Ht level less than 20%.
RESULTS: median gestational age was 28/2 weeks (25/0-32/6) and median birth weight 1205 g (680-1440). Pre-transfusion Hb was 8.1 g/dl (range 7.4-8.6), Ht was 25% (range 19-30). Pre-transfusion CrSO2, SrSO2, RrSO2 correlated with pre-transfusion Hb and Ht level. The pre-transfusion to post-transfusion CrSO2, SrSO2, RrSO2 changes correlated with pre-transfusion Hb level (r = 0.512, p=0.0012). CrSO2 increased from 63 (60-72)% to 74 (72-84)% post transfusion (p < 0.001), RrSO2 increased from 54 (46-58)% to 65 (62-66)% post transfusion (p < 0.001), SrSO2 increased from 46 (38-58)% to 60 (58-64)% post transfusion (p < 0.001), SCOR increased from 0.76 to 0.86 post transfusion (p < 0.001). Also C-FTOE, S-FTOE were decreased significantly after red blood cells transfusion. SCOR≤0.76, C-FTOE ≥0.35, CrSO2≤60%, SrSO2≤38% and RrSO2≤46% were identified as a cut-point for infants with increasing severity of anemia and were the additional indications for red blood cells transfusion.
CONCLUSIONS: These results suggest that cerebral and regional tissue oxygenation may be suitable as a guide to the need for blood transfusions.
Continuous assessment of cerebral autoregulation in extremely low gestational age newborns using diffuse correlation spectroscopy and signal cross-correlation
Sunwoo Ja, Martin Aa, Zavriyev Aa, Kaya Ka, Munster Cb, Steele Tb, Cuddyer Db, Sheldon Yb, Inder Tb, Herzberg Ec, Franceschini Ma, El-Dib Mb
aAthinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Harvard Medical School, Boston, USA
bDepartment of Pediatric Newborn Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, USA
cDivision of Neonatology and Newborn Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, USA
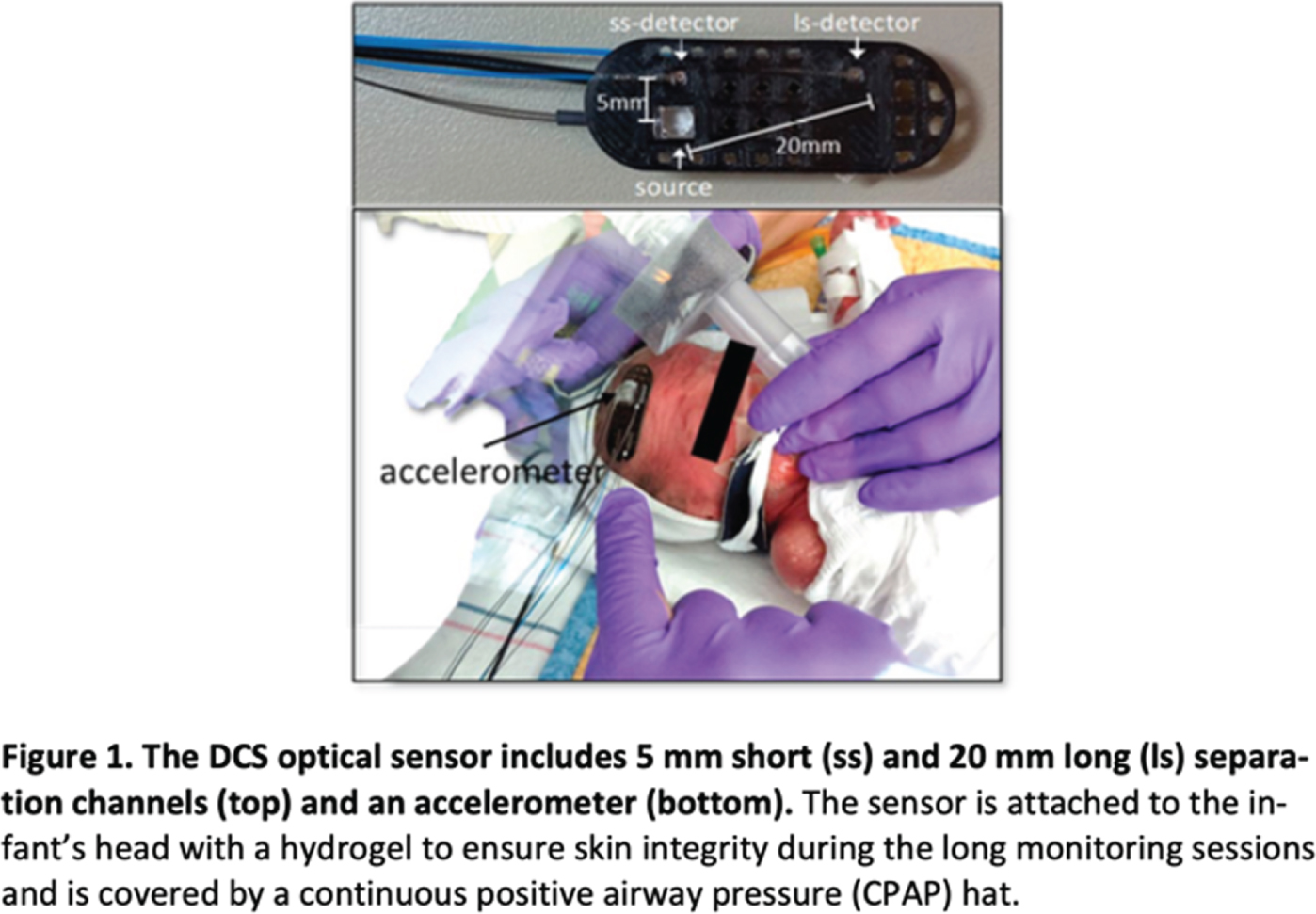
BACKGROUND/AIMS: Extremely low gestational age (ELGA, <29 weeks GA) newborns have limited cerebral autoregulation and frequent pressure-passive fluctuations in cerebral blood flow which predispose them to germinal matrix and intraventricular hemorrhage (GM-IVH). Previous studies have shown that the loss of cerebral autoregulation in preterm infants was associated with brain injury and IVH; however, most of these studies relied on signal cross-correlation using continuous-wave-near-infrared spectroscopy (cerebral oximetry) and invasive blood pressure (BP) measurements. Challenges exist because cerebral oximetry does not provide the best marker of blood flow, and arterial BP monitoring is not used on all ELGA infants at risk for IVH. Therefore, we propose a novel methodology for quantifying the loss of cerebral autoregulation, using cross-correlation between cerebral blood flow and scalp blood flow (as a surrogate measure of systemic flow) both obtained by diffuse correlation spectroscopy (DCS). In addition, we evaluated the association of this assessment with development of GM-IVH.
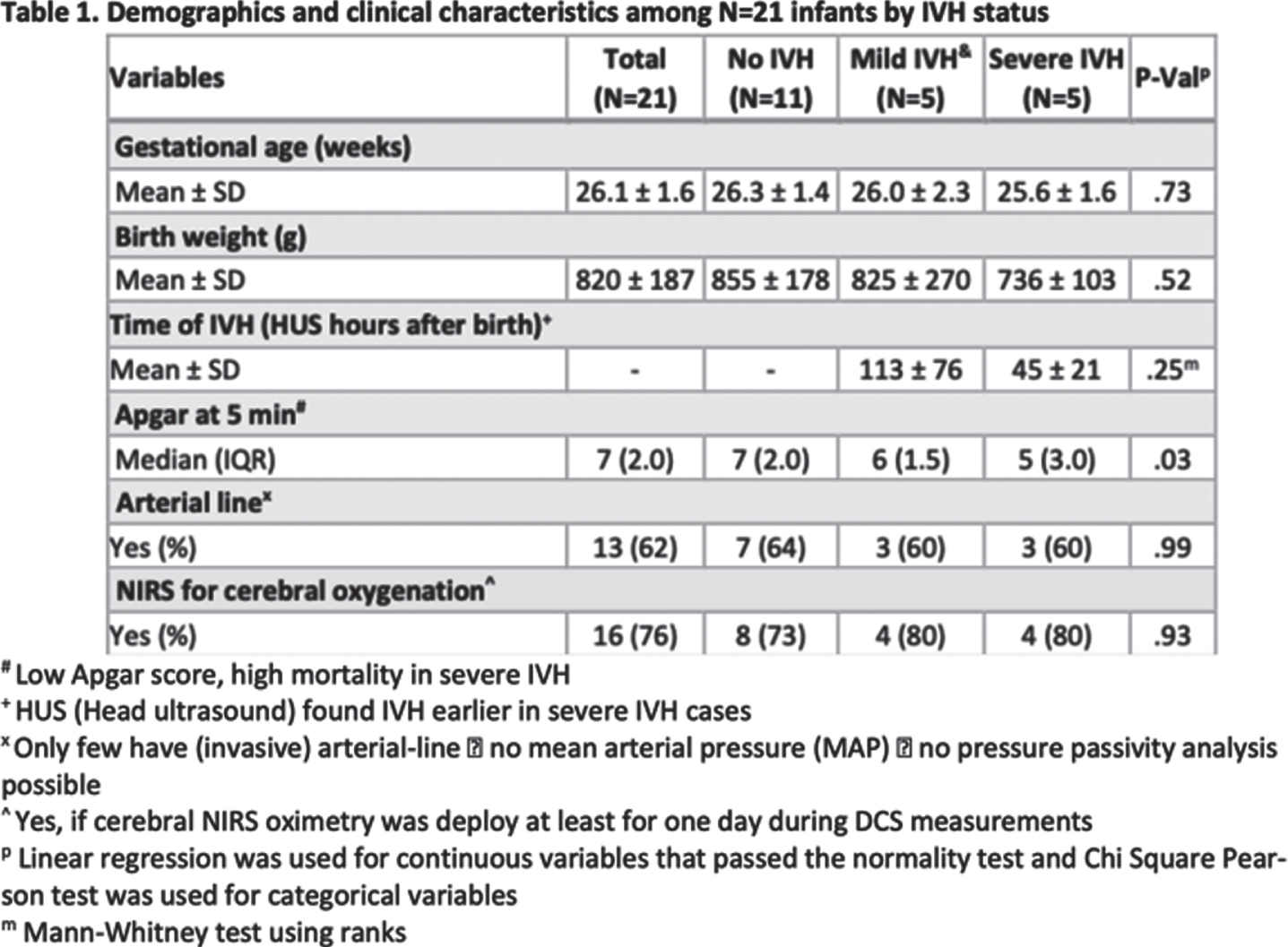
DESIGN/METHODS: This report represents pilot data analysis from an ongoing study evaluating the utility of DCS monitoring in the first few days of life in ELGA infants. The optical sensor for DCS has long separation (20mm) and short separation (5mm) detectors to monitor cerebral blood flow and scalp blood flow, respectively (Figure 1). Other data collected simultaneously include systemic pulse oximetry, EKG, and when available cerebral oximetry and arterial BP. Head ultrasounds (HUS) were done on days 1, 3, and 7 according to the clinical protocol. Infants were classified as no-IVH, mild-IVH (GMH or Grade II), and severe-IVH groups (Grade III or IV).
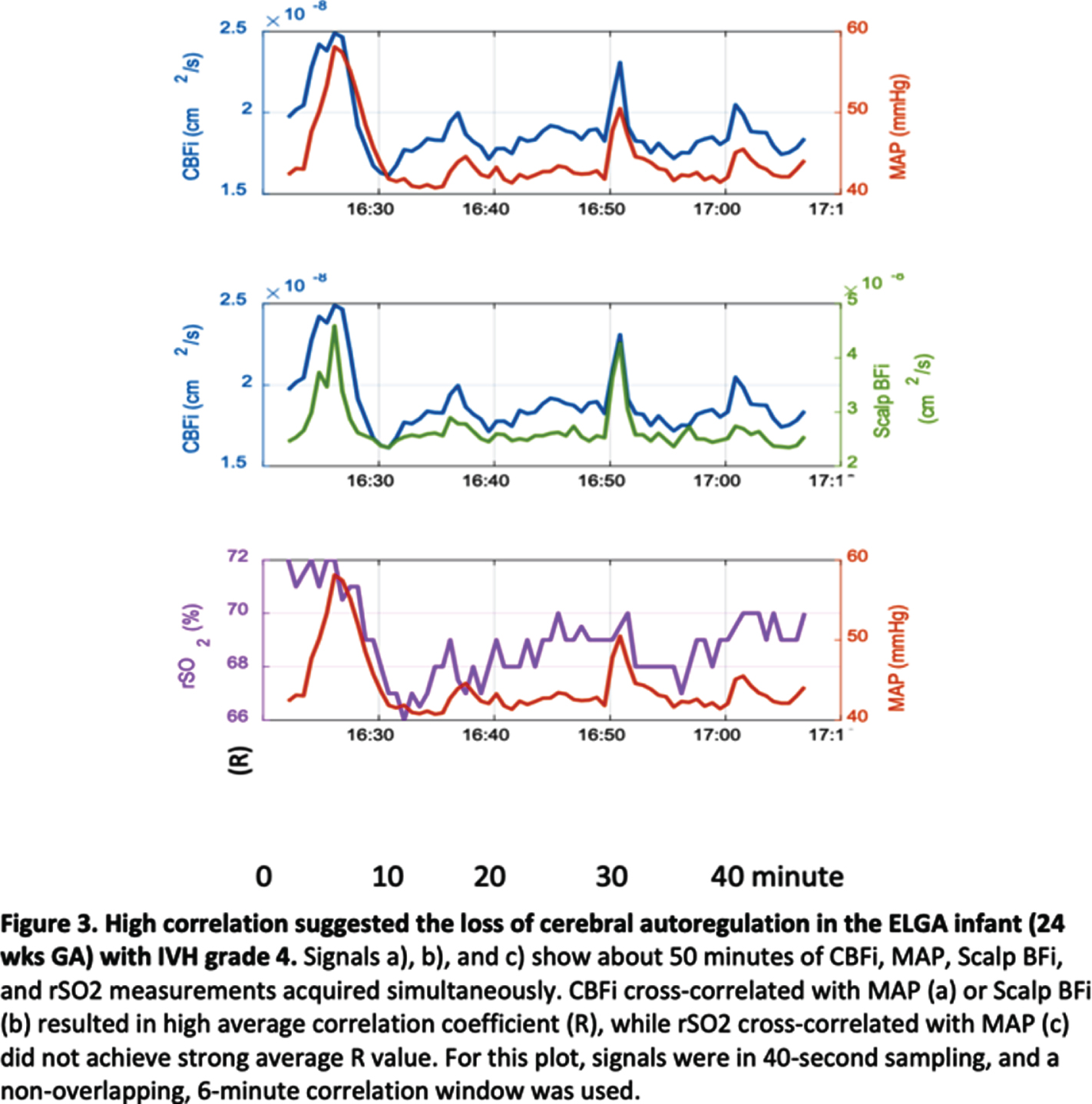
RESULTS: We analyzed 21 ELGA infants, monitored for 6-24 hours between day 2-5 of life, and found a significantly higher chance of dysregulated cerebral blood flow in the severe-IVH group (Table 1; P=.046, Figure 2). The signal example in Figure 3 is a 24-weeks GA infant diagnosed with IVH grade IV at the first HUS, indicating strong pressure passiveness (Figure3-a, average R=.69) and the loss of cerebral autoregulation (Figure3-b). For the same period, cross-correlation of cerebral oximetry measurement (Figure3-c) did not lead to the same conclusion. Using the lagged correlation between scalp blood flow and cerebral blood flow as a biomarker of cerebral autoregulation as illustrated in Figure 3-b, we found that severe-IVH group showed the highest correlation, indicating loss of cerebral autoregulation.
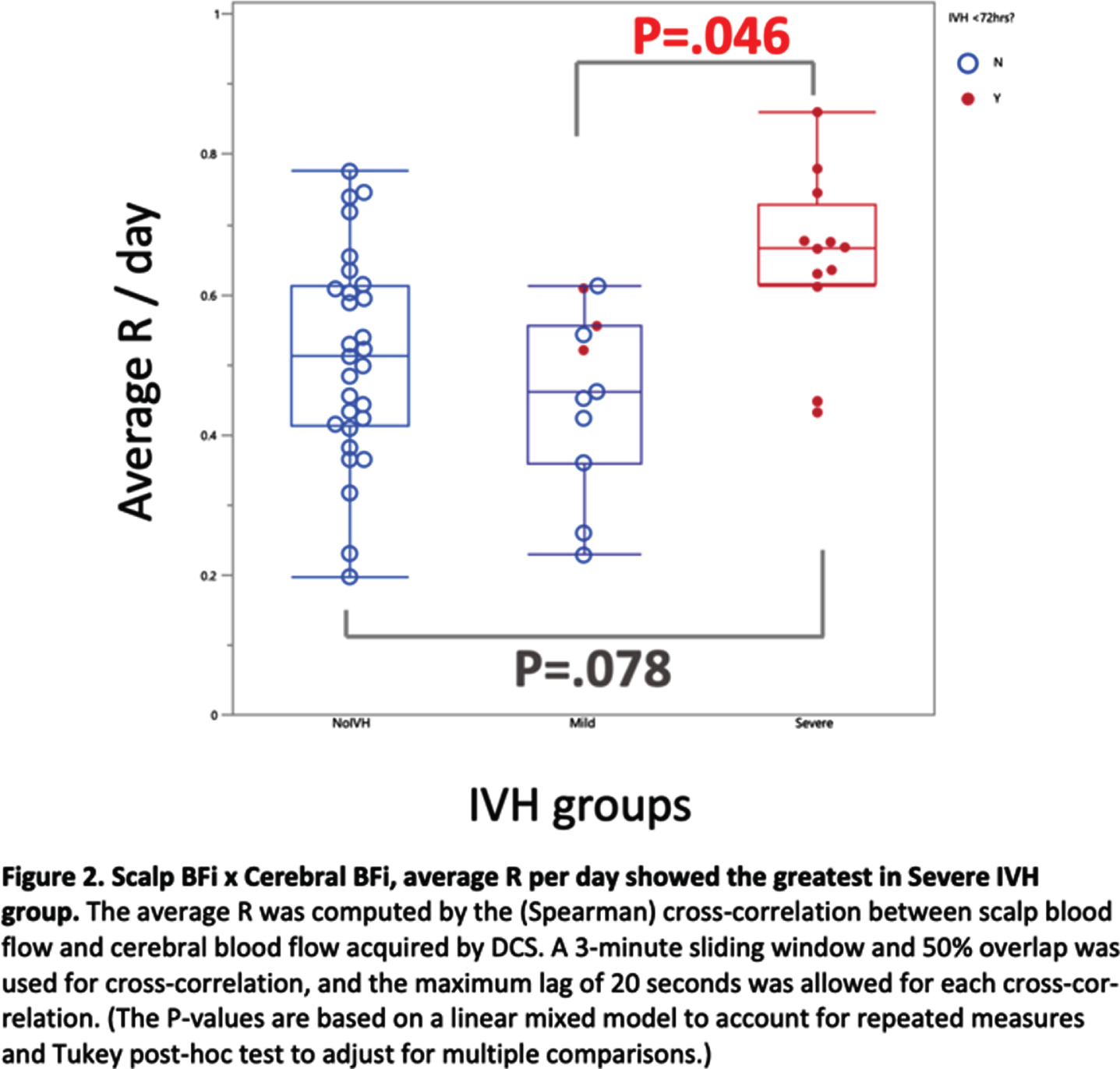
CONCLUSION: Signal cross-correlation between cerebral blood flow and scalp blood flow using DCS could provide a novel noninvasive methodology for assessing cerebral autoregulation in ELGA infants and pressure passivity demonstrated using this methodology is associated with higher grade IVH.
ACKNOWLEDGEMENT: The authors would like to thank Zachary Starkweather for building DCS sensors, Dr. Felipe Orihuela-Espina for helpful discussion, Elizabeth Singh and Sarah Lee for their support, and Yujing Huang for the DCS graphical-user-interface.
Non-invasive arterial and microvascular cerebral blood flow: Comparison of transcranial doppler ultrasound and diffuse correlation spectroscopy measurements in infants with intraventricular hemorrhage and hydrocephalus
Vadset Ta,b, Sims Ja,b, Freeman Sa,b, Zampolli La,b, Vyas Ra,b, Hsiao Ca,b, Hay Sc, Warf Bd, Grant Pa,b,e, Sutin Ja,b, Lin Pa,b
aDivision of Newborn Medicine, Boston Children’s Hospital, Boston, United States
bFetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children’s Hospital, Boston, United States
cDepartment of Pediatrics, Beth Israel Deaconess Medical Center, Boston, United States
dDepartment of Neurosurgery, Boston Children’s Hospital, Boston, United States
eDepartment of Radiology, Boston Children’s Hospital, Boston, United States
BACKGROUND: Transcranial Doppler Ultrasound (TCD) is a common bedside tool that measures cerebral blood flow velocity (CBFV) in the assessment of the progression of IVH and hydrocephalus in infants. Diffuse coherence spectroscopy (DCS)(1) is an emerging optical technology that enables regional microvascular blood flow measured non-invasively at the bedside. Few studies have reported a moderate agreement between the values from the two modalities in a small number of preterm infants but without intraventricular hemorrhage (IVH) or hydrocephalus(2, 3). In this study, we compared clinical TCD results of CBFV in the anterior cerebral artery (ACA) from clinical head ultrasound exams with DCS measurements of microvascular cerebral blood flow (CBF) in a larger cohort of NICU infants whose TCD assessments are clinically indicated for suspicion of or confirmed IVH or hydrocephalus.
DESIGN/METHODS: This is a subgroup analysis of a prospective, observational study of monitoring cerebral blood flow and metabolism in infants with intraventricular hemorrhage and post-hemorrhagic hydrocephalus (NCT02601339). Regional CBF and tissue oxygenation (ctSO2) at the frontal location were measured by a Frequency Domain Near-Infrared and Diffuse Correlation Spectroscopies (FDNIRS-DCS) system on the same day of the clinical TCD exam. DCS-CBF and ctSO2 were compared with the mean, systolic and diastolic CBFV as well as with the TCD resistive index (RI).
RESULTS: Seventeen patients with 29 measurements were included in this analysis (F/M:9/8; GA:31.6 (5.89) wks; PMA: 37.5 (8.2) wks). We observed a moderate correlation between DCS-CBF and systolic (r=0.58 and 0.68 respectively, P<0.0001) and mean CBFV (r=0.46 and 0.63 respectively, P<0.001) with and without compression but no association with diastolic flow (r=-0.06 and 0.33 respectively, P=0.77 and 0.086)(Figure 1). Resistive index correlated positively with DCS-CBF (r=0.368, P=0.05) and negatively with ctSO2 (r=-0.41, P=0.026, Figure 2).
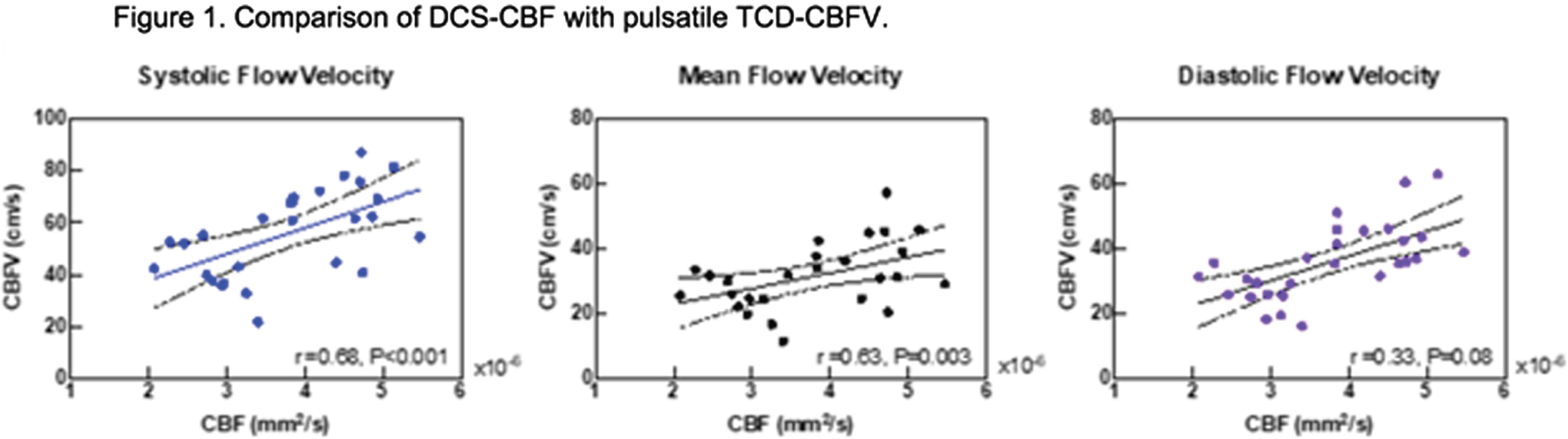
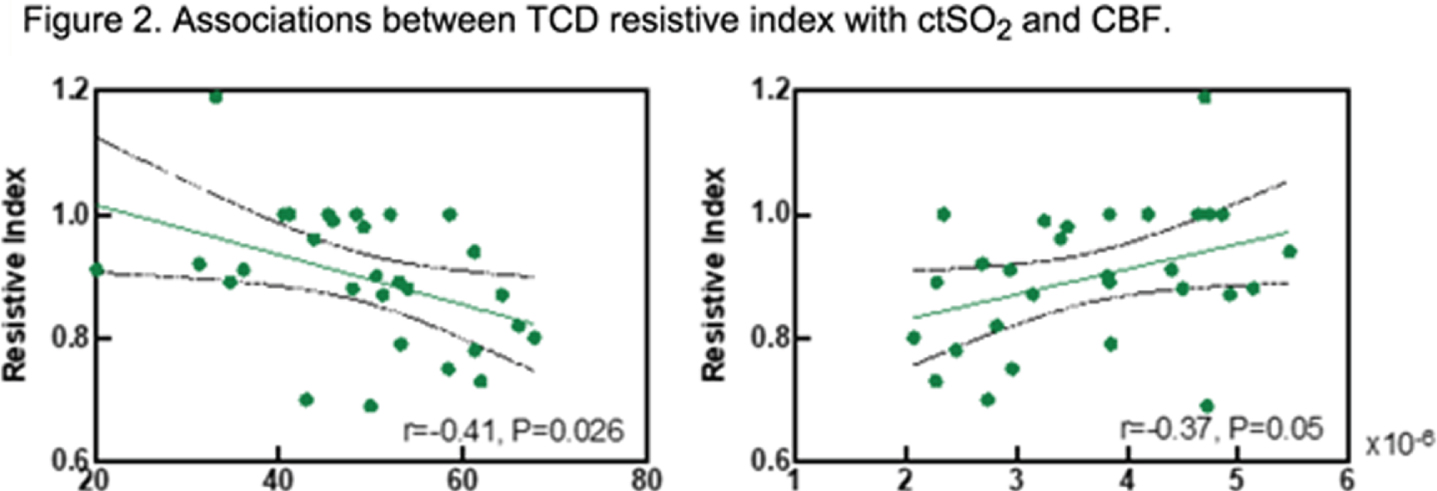
CONCLUSION: TCD measures flow velocity in large arteries, while DCS measures microvascular flow in the pial and parenchymal vascular beds. The pulsatile components of blood flow waveforms are related to different components of vascular regulation, with the systolic component related to cardiac output and proximal arterial resistance and the diastolic component determined by distal resistance from downstream tissue beds. The differences in correspondence between DCS measurements and the pulsatile components of TCD may reflect the differences in the tissue compartments that they measure. DCS and TCD are complementary but not identical measurements of CBF. Future work will explore the association between the pulsatile DCS-CBF with those of TCD-CBFV.
References:
[1] P.-Y. Lin et al., J Vis Exp Jove, e4379 (2013).
[2] E. M. Buckley et al., Opt Express. 17, 12571 (2009).
[3] N. Roche-Labarbe et al., Hum Brain Mapp. 31, 341–352 (2010).
Non-invasive respiratory support is associated with increased incidence of occult cerebral hypoxia
Noroozi Ma, Whitehead Ha, Vesoulis Za, Liao Sa
aWashington University, Department of Pediatrics, St. Louis, United States
BACKGROUND AND PURPOSE: Impaired cerebral oxygen delivery is a known risk factor for preterm brain injury including intraventricular hemorrhage, white matter injury, and cerebellar hemorrhage. Monitoring of cerebral oxygenation with near-infrared spectroscopy (NIRS) may offer more information on “hidden” cerebral hypoxia not otherwise apparent We hypothesized that less invasive respiratory modes may provide inadequate cerebral oxygen delivery not apparent on convention pulse oximetry.
MATERIALS: Preterm infants born before 32 weeks gestation were enrolled in a prospective, longitudinal NIRS monitoring study. After recruitment, infants underwent daily cerebral NIRS and pulse oximetry monitoring (ForeSight Elite, Edwards Lifesciences, Irvine, CA) for 2 weeks, every other day monitoring for 2 weeks, and then weekly monitoring under 35 weeks corrected age. The goal monitoring time was at least 4-6 hours but was held in cases of patient instability or parent/medical team request. Data was captured at 0.5 Hz. Annotation was made of the mode of respiratory support at the time of recording as well as the average fraction of inspired oxygen (FiO2). Modes were classified as invasive (conventional and high-frequency), non-invasive positive pressure ventilation (NIPPV), high flow nasal cannula (HFNC, >=2 LPM), low-flow nasal cannula (LFNC, <2LPM), or room air. Each recording underwent simple error correct to remove outliers and missing values by replacement with NaN. The mean cerebral saturation (c-sat) and mean systemic saturation (SpO2) were calculated for each recording. The proportion of recorded cSat samples below critical hypoxia threshold (<67%, following SafeBoosC-III guidelines) and the proportion SpO2 samples below critical desaturation threshold (<85%) were calculated. Kruskall-Wallis test was used for non-parametric multiple group comparison.
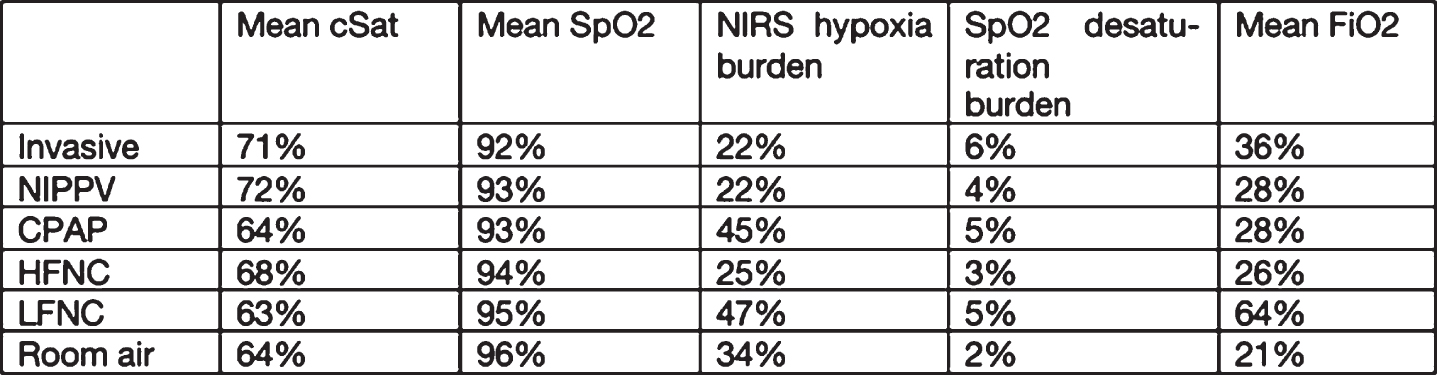
RESULTS: 134 infants were included with a mean gestational age of 25.9 weeks, 48% female, a mean birthweight of 897 grams, and 13% died during NICU hospitalization (Table 1). From these infants, 442 recordings were made with a mean length of 9.3 hours. Invasive ventilation was the most common mode during recording (46%), with NIPPV and room air next most common (Table 2). Mean SpO2 values were similar across respiratory support types and within target range (mean 92-96%. Mean cSat values were greater for invasive and NIPPV (71-72%) compared to other modes, most of which had mean cSat values below critical threshold. Cerebral hypoxia burden was significantly lower in the invasive and NIPPV groups compared to less supported groups (p<0.01). SpO2 desaturation burden was not different between groups (3-6% of recording). Although invasive support was associated with greater FiO2, this difference was not significant.
CONCLUSION: Cerebral NIRS identifies significant occult cerebral hypoxemia, not apparent on pulse oximetry. More invasive modes of support were associated with an approximately 50% reduction in cerebral hypoxia burden. Careful selection of respiratory in conjunction with monitoring should be bused to avoid cerebral hypoxemia.
Table 1.
Sample descriptives
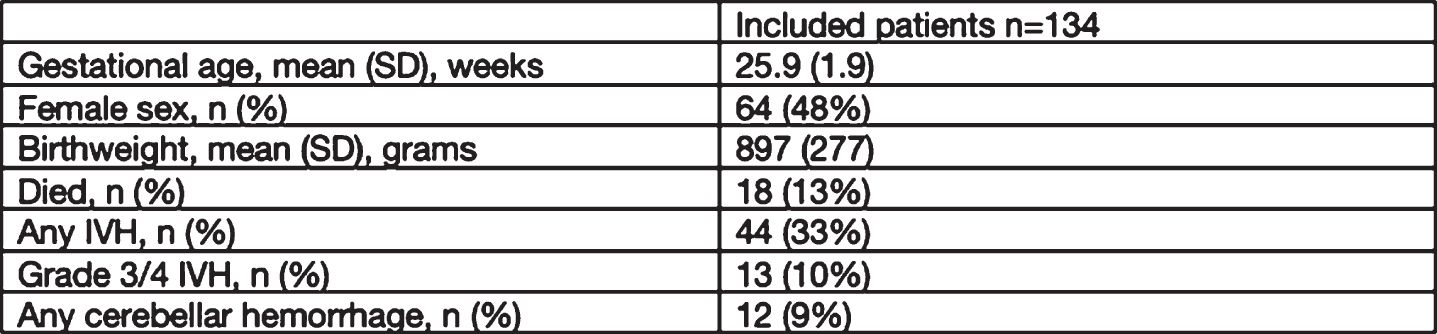 |
Table 2.
Recording descriptives
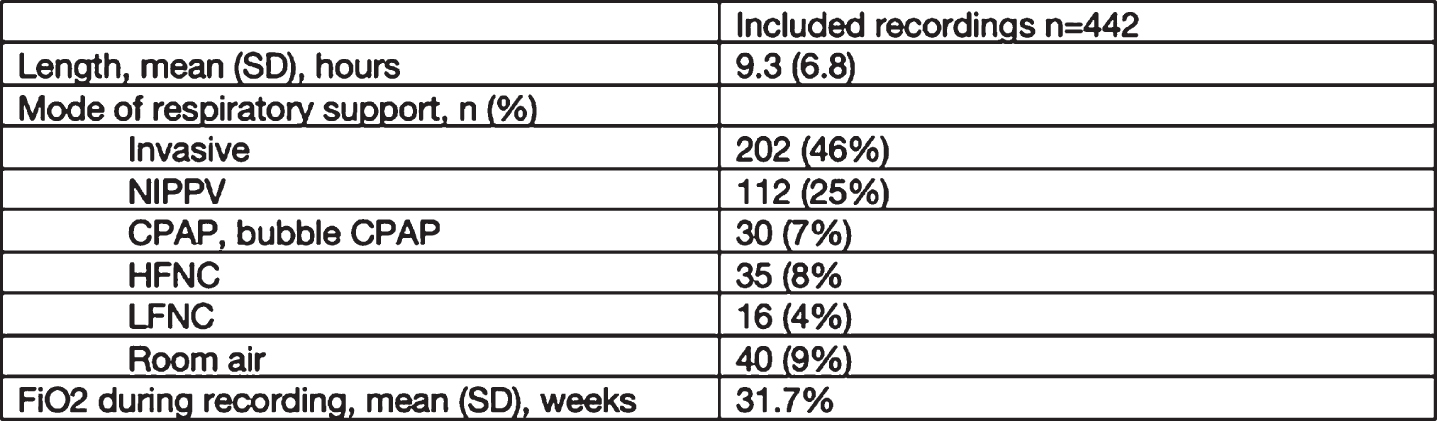 |
Table 3.
Saturation characteristics
 |
Precision of cerebral tissue oxygenation and blood flow measured by frequency-domain near-infrared and diffuse correlation spectroscopies in NICU neonates
Vyas Ra,b, Feldman Ha,d, Yen Fb, Hsiao Ca,b, Rajaram Aa,b, Vadset Ta,b, Hay Sf, Warf Be, Grant Pa,b,c, Sutin Ja,b, Lin Pa,b
aDivision of Newborn Medicine, Boston Children’s Hospital, Boston, USA
bFetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children’s Hospital, Boston, USA
cDepartment of Radiology, Boston Children’s Hospital, Boston, USA
dInstitutional Centers for Clinical and Translational Research, Boston Children’s Hospital, Boston, USA
eDepartment of Neurosurgery, Boston Children’s Hospital, Boston, USA
fDepartment of Neonatology, Beth Israel Deaconess Medical Center, Boston, USA
BACKGROUND: Absolute measurement of cerebral tissue oxygenation (ctSO) and blood flow (CBF) is necessary for development of clinically useful thresholds. Previous studies investigated precision of near-infrared and diffuse correlation spectroscopies in cross-sectional studies of stable neonates. We first report precision of ctSO and CBF measured longitudinally in a heterogenous NICU population.
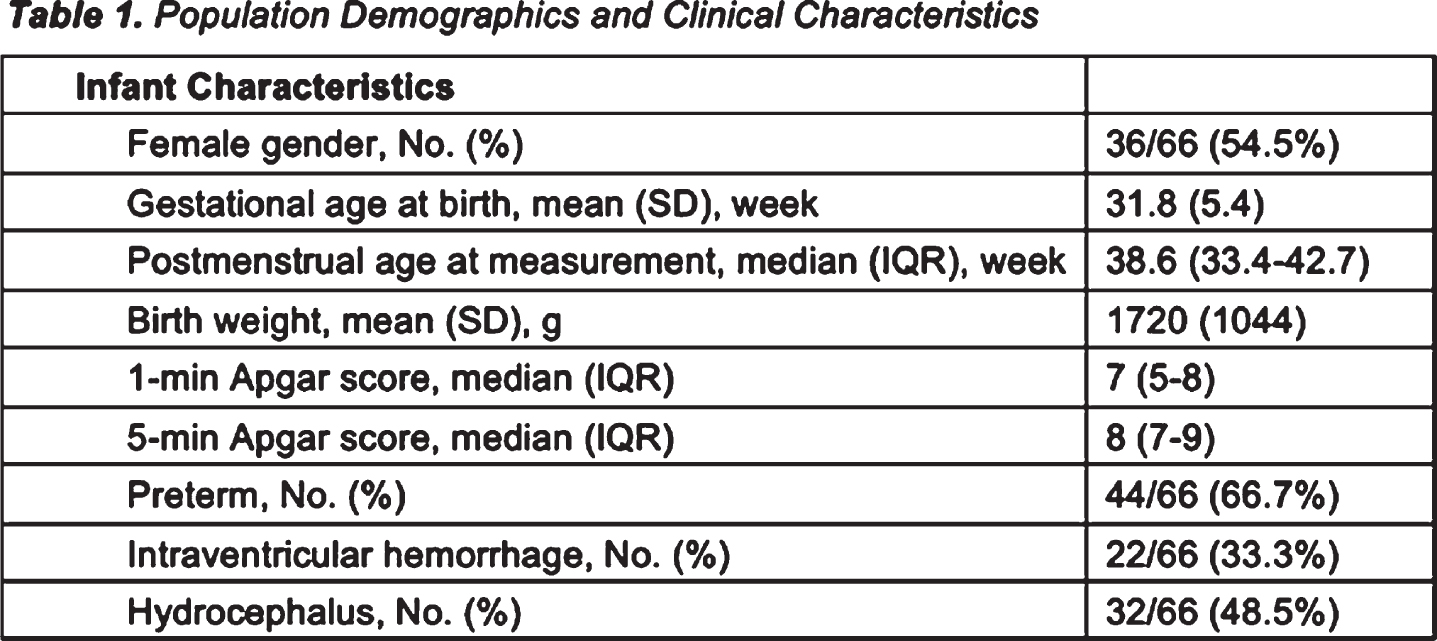
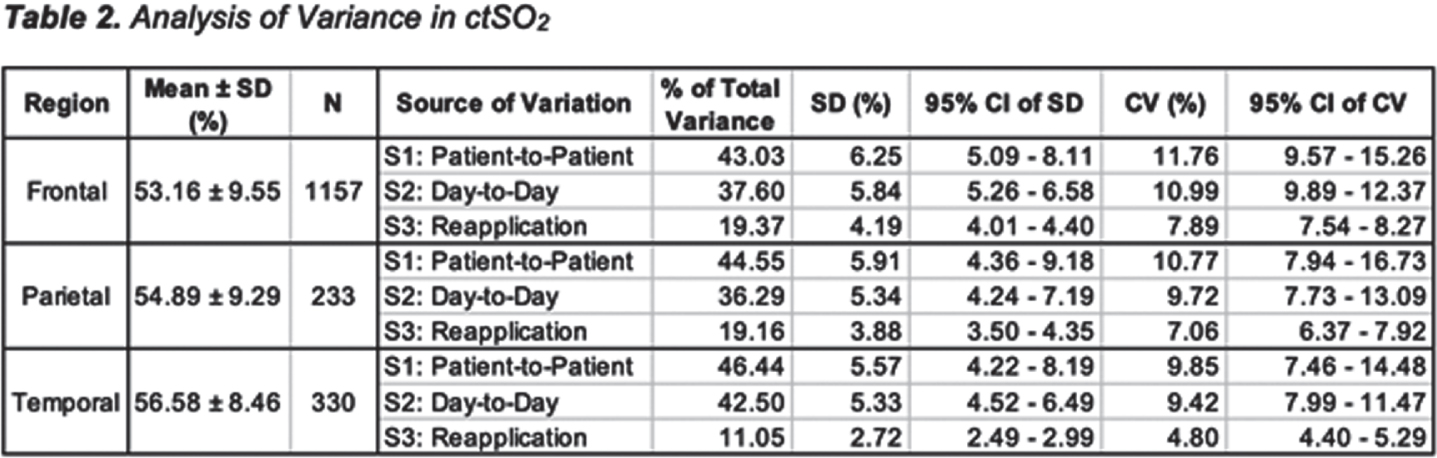
METHODS: This is a secondary analysis of a prospective, observational study (NCT0601339). Sixty-six infants from NICUs at Boston Children’s Hospital and Beth Israel Deaconess Medical Center were included in this analysis (Table 1). Bedside measurements ctSO2 and CBF were performed longitudinally during the NICU stay by frequency domain near-infrared and diffuse correlation spectroscopies (FDNIRS-DCS)[1]. During each session, up to six locations were measured: frontal (F), parietal (P) and temporal (T) on both left and right sides. For each location, three or more 30s recordings were obtained. A linear mixed-effects model was applied to estimate measurement precision and to quantify the variability in ctSO and CBF at each location from three main sources: patient-to-patient (S1), day-to-day (S2) for each patient, and reapplications (S3) on each location during a measurement session for a given patient. The percentage of total variance, standard deviation (SD) and coefficient of variation (CV) were computed for each source. Precision was defined as the SD of measurements from reapplication at each location.
RESULTS: A total of 250 measurements were included in the analysis. Most of the variance was attributed to differences between patients (S1) and longitudinal changes within a given patient (S2) for all locations in both ctSO and CBF (Table 2-3, combined variance of S1 and S2 was 80.7%-88.9% in ctSO; 68.0%-80.3% in CBF). Variance from reapplication contributed the least to the total variance of the model which led to the precision of 4.2, 3.9 and 2.7% for ctSO and 1.0, 0.9 and 1.0 μm2/s for CBF in F, P and T respectively.
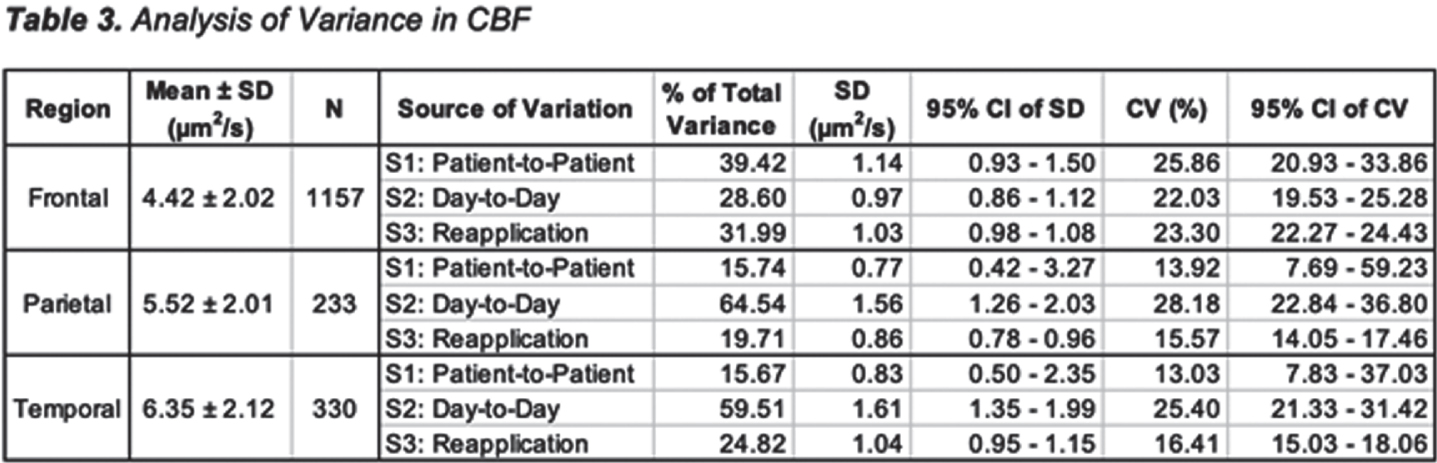
CONCLUSION: We found the precision of FDNIRS-measured ctSO in a larger heterogenous cohort of NICU infants is comparable to values reported from other types of NIRS systems in smaller sample sizes[3,4]. ctSO precision was within the clinically meaningful threshold of 5% proposed for neonatology[2]. We also found less reapplication variation at the T location compared to F and P. The higher variation of CBF with reapplication may suggest that DCS-measured CBF is more sensitive to tissue inhomogeneity than NIRS-measured ctSO. Despite the greater reapplication variance, the predominant source of CBF variance was physiological. Nevertheless, our data suggests that clinically meaningful effect sizes for CBF should take into account the natural variation from reapplication of the sensor.
Bibliography:
[1] Lin P-Y et al., Scientific Reports. 2016;6(1):25903
[2] Greisen G et al. Neurophotonics. 2016;3(3):031407
[3] Andresen B et al. Pediatr Res. 2019;86(4):515-521
[4] Avian A et al. Neurophotonics. 2021;8(4):045001
Evaluation of diffuse correlation spectroscopy to continuously monitor cerebral blood flow in premature infants
Zimmermann Ba, Iennaco Ma, Lee Sb, Inder Tb, El-Dib Mb
a149 Medical Inc., Boston, United States
bBrigham and Women’s Hospital, Department of Pediatric Newborn Medicine, Boston, United States
BACKGROUND: Cerebral blood flow (CBF) is an important physiological parameter for assessing brain health. In premature infants, CBF instabilities and immature cerebrovascular reactivity put infants at significant risk for brain in- jury including intraventricular hemorrhage (IVH). Yet there is no method for continuously, non-invasively monitoring CBF. A few techniques provide a glimpse of cerebral hemodynamics but are inadequate in sig- nificant ways. The characteristics of these techniques are outlined in Table 1.To fill this unmet need we built a novel device, a Near Infrared Doppler Spectroscope (NIRDS) that uses dif-fuse correlation spectroscopy (DCS) to continuously and non-invasively record CBF. DCS uses near-infrared light to measure microvascular blood flow in the cerebral cortex by quantifying the temporal intensity fluc- tuations of the speckle field produced by moving red blood cells.This feasibility study aims to demonstrate that NIRDS is a safe and effective method to measure CBF of premature infants in the NICU.
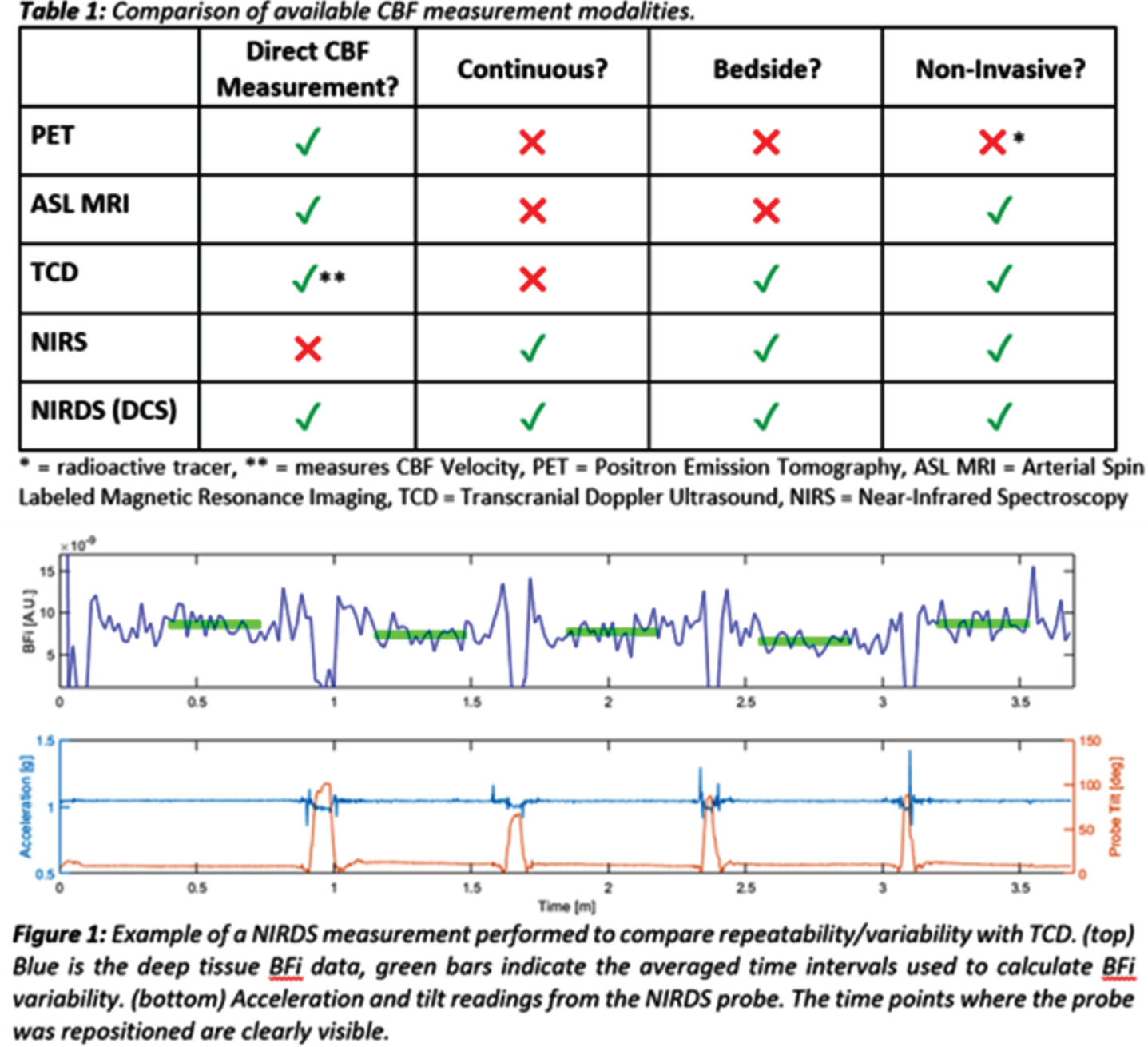
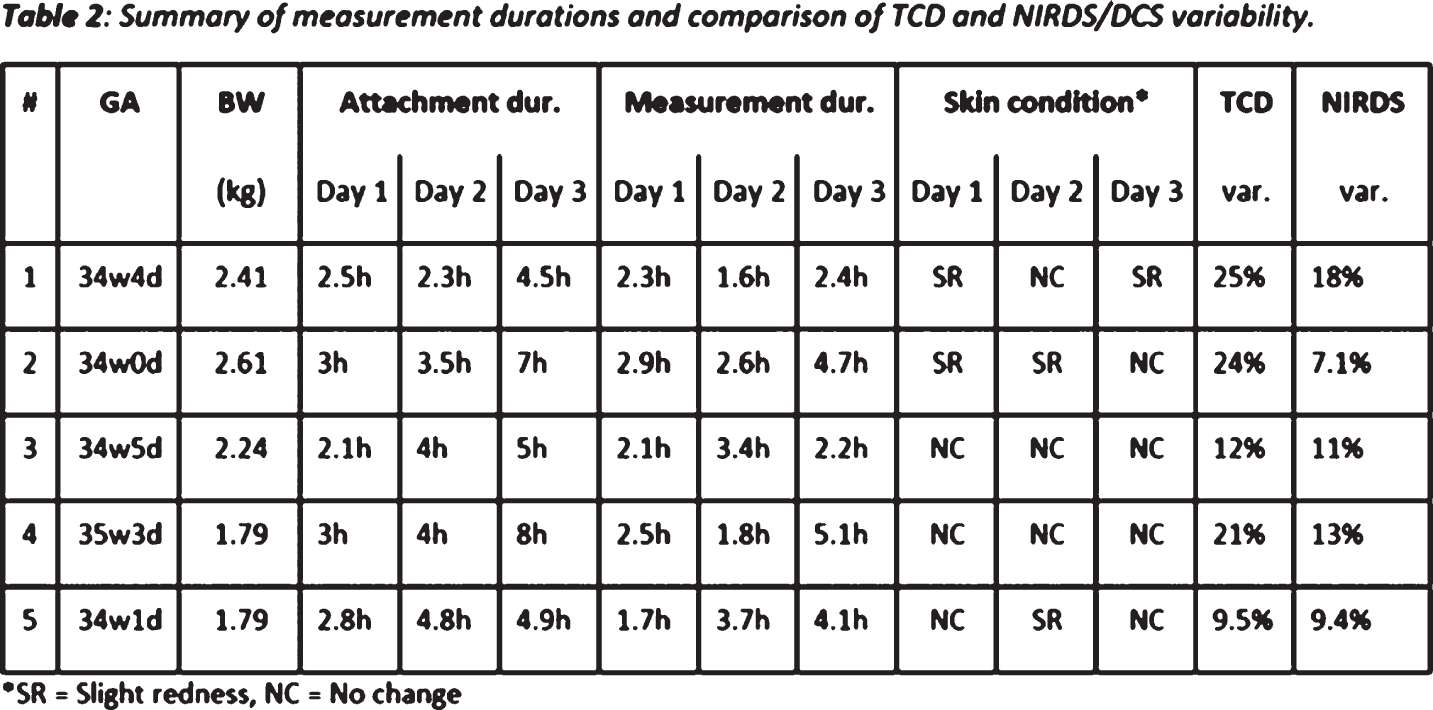
METHODOLOGY: Five premature infants (≤ 48h age, gestational age ranging from 34 to 35.5 weeks, birth weight ranging from 1785 to 2608 grams) from the Brigham and Women’s Hospital NICU were enrolled. On the first day of measurement, the probe was attached for 2-3 hours, then for up to 8 hours on the second and third day. After each measurement, the skin under the probe was evaluated for adverse effects.To compare repeatability of our method with that of transcranial doppler (TCD), five independent, serial TCD readings of the pericallosal artery and five 20 seconds long NIRDS measurements were obtained on each infant’s third day of life (see example measurement in Figure 1). The coefficient of variation over all readings of the time-averaged TCD mean velocity was compared to that of the NIRDS blood flow index (BFi).
RESULTS: Table 2 lists the measurement durations, skin condition and variability of both NIRDS and TCD in the study cohort. There were no adverse events, with only minimal skin redness observed in 5 of the 15 measure- ments. NIRDS showed slightly less variability than TCD, with a consistently lower coefficient of variation. Overall, blood flow data were of good quality, and motion artifacts corresponded to infants movement de- tected by accelerometer. High quality data continued to be obtained in subject 4 while receiving photo- therapy and subject 5 while on continuous positive airway pressure (CPAP).
CONCLUSION: NIRDS is feasible and reliable for the continuous monitoring of CBF in premature infants during their first three days of life. Future work will test this technology in extremely low gestational age infants (<29 wk GA) and will investigate the correlation between CBF fluctuations and incidence and severity of IVH. Using this method to monitor CBF has the potential to guide individualized therapies at the bedside and improve neu- rodevelopmental outcomes.


