
Proceedings of the 13th International Newborn Brain Conference: Long-term outcome studies, Developmental care, Palliative care, Ethical dilemmas, and Challenging clinical scenarios
Continuous non-invasive hemodynamic monitoring of neonates undergoing hypothermia
Balog Va, Vatai Ba, Kátai La, Szabó Ma, Jermendy Áa
a1st. Department Of Paediatrics, Semmelweis University, Budapest, Hungary
C. Bührera, B. Metzeb, M. Obladenb
aBasel University and Children’s Hospital, Basel, Switzerland
bDepartment of Neonatology, Charité University Medical Center, Berlin, Germany
INTRODUCTION: Hemodynamic instability is common in asphyxiated neonates undergoing therapeutic hypothermia (TH) for moderate-severe neonatal encephalopathy (NE). Rewarming is a critical period and non-invasive circulatory monitoring may be helpful in guiding cardiovascular supportive therapy. We also hypothesized that cardiac function could provide cues for neurodevelopmental outcome.
AIMS: To provide a comprehensive analysis of cardiac function during TH and rewarming and its relation to neurodevelopmental outcome.
METHODS: In a prospective, observational study, we enrolled 26 neonates with moderate-severe NE, born between 2016 and 2019. A hemodynamic monitor based on electrical velocimetry (ICON, Osypka Medical GmbH, Berlin, Germany) was used. Heart rate (HR), stroke volume (SV), cardiac output (CO) data was recorded continuously throughout TH and rewarming with a minute frequency. Neurological outcome was assessed at 2 years using the BSID II. scale. Good outcome was defined as >70 points on both the psychomotor and mental scale. Time-series analysis was used, and features of cardiac function were described to perform logistic regression modeling for outcome prediction.
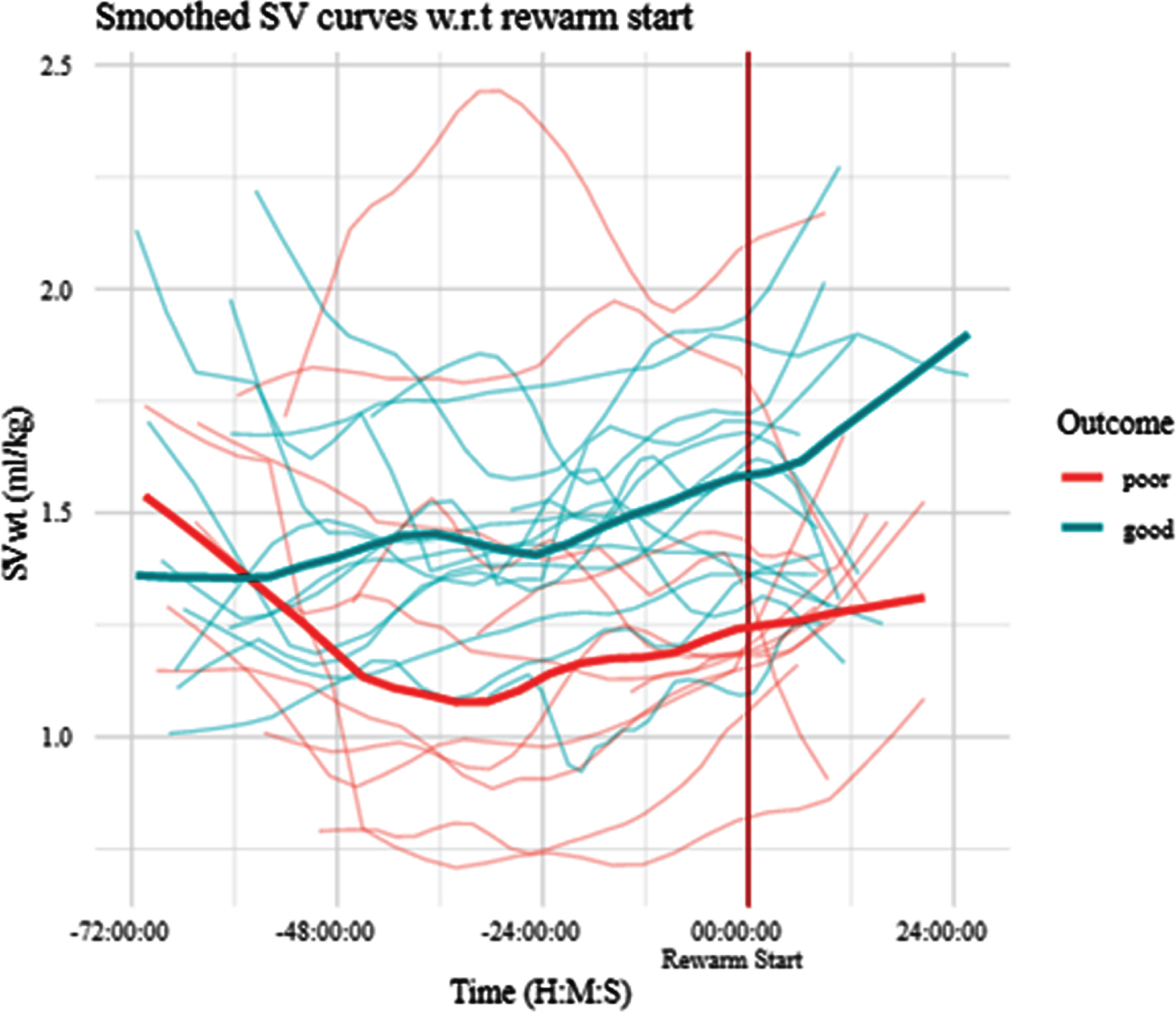
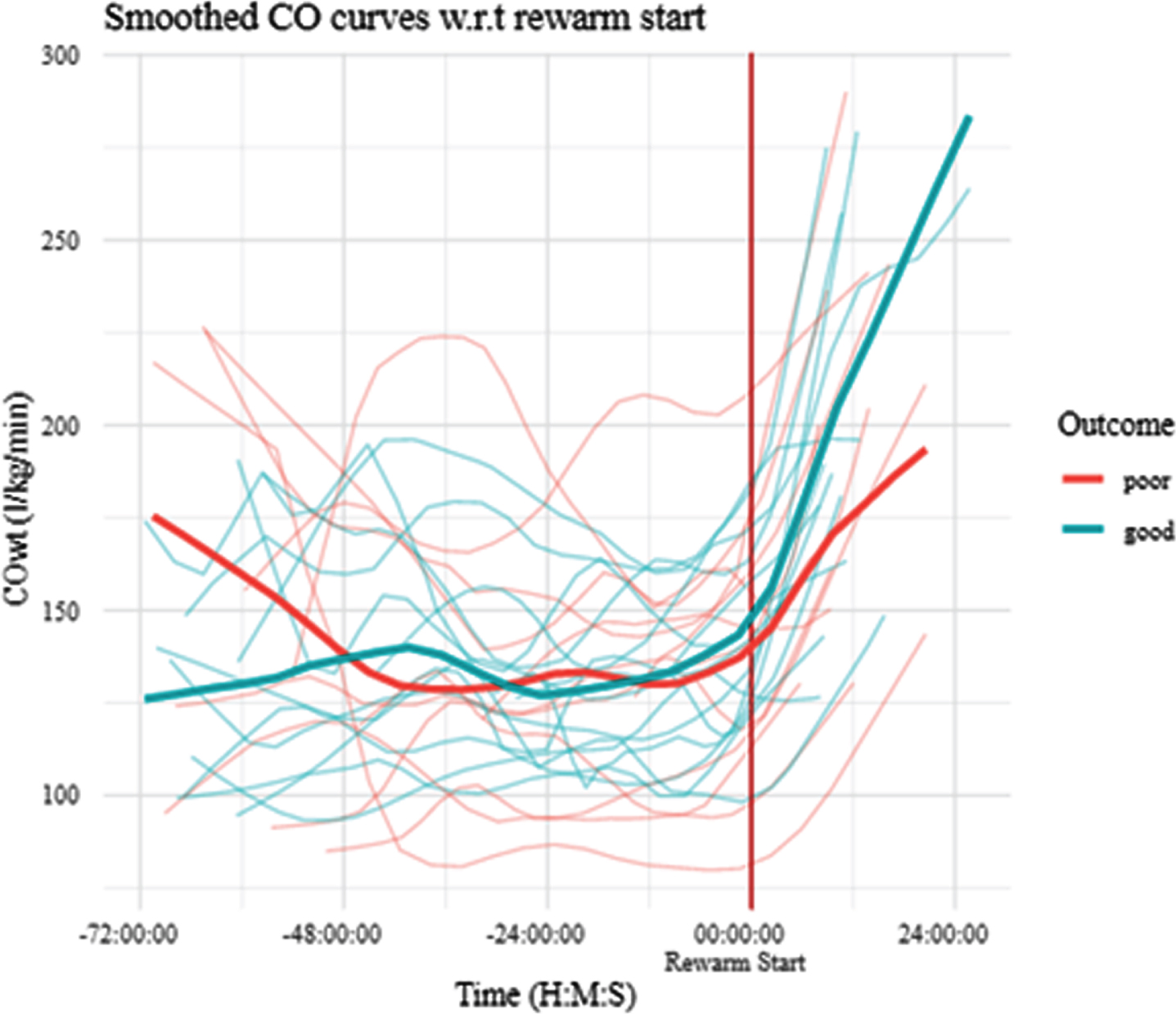
RESULTS: Fourteen (54%) patients had good and twelve (46%) had poor outcome at two years of age. High-frequency data collection started from median [IQR] of 11.8 [7.0; 24.3] hours of life (h) and lasted until 84.0. [81.8; 87.0] h. During TH, the mean HR of the good outcome group was significantly lower than that of the poor outcome group (”HR_TH” feature: 86 ± 13 / min vs. 104 ± 18 / min, p = 0.01). During rewarming HR increased significantly and similarly in both groups (”HR_slope” feature) (Image 1). The SV was unaffected by rewarming and showed a slowly increasing trend (”SV_slope” feature). At the end of TH, SV of the good outcome group was significantly higher compared to the poor outcome group (”SV_TH” feature 1.55 ± 0.23 mL/kg vs 1.29 ± 0.30 mL/kg, p= 0.035) (Image 2). In line with this, CO was similar at the end of TH in both groups (134 ± 36 mL/kg/min vs 136 ± 27 mL/kg/min, and a significant 25 % increase in CO was observed during rewarming (Image 3). Based on multiple regression modeling, of all features,” HR TH” was independetly associated neurological outcome (p=0.023).
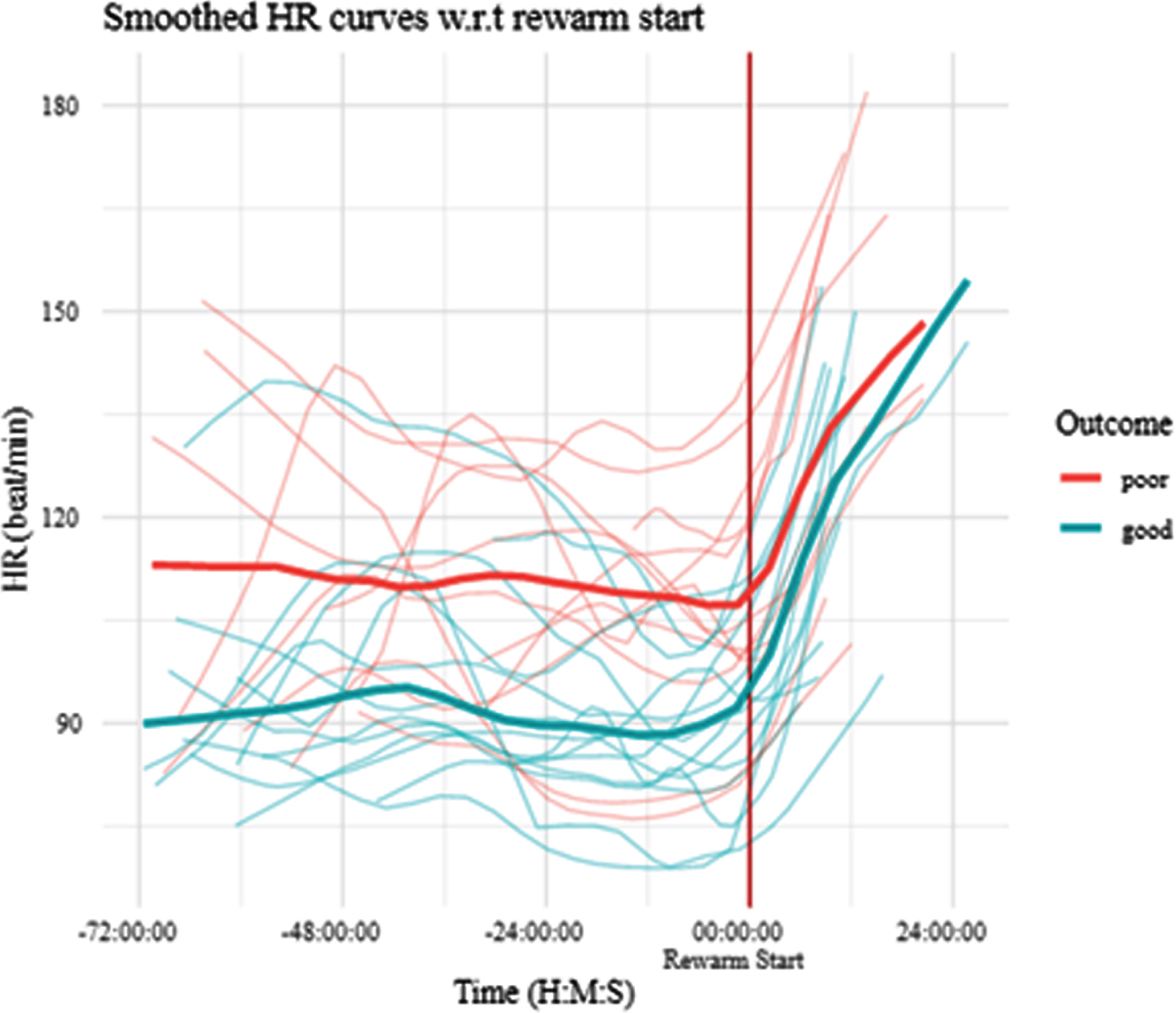
CONCLUSION: Based on continuous hemodynamic monitoring, patients with poor outcome compensate the lower SV with higher HR to achieve similar CO to patients with good outcome during TH. Heart rate during TH is an independent predictor of outcome.
HIElights of Hope: Engaging families and providers in the storytelling process
Bansal Sa, Pilon Ba
aDuke University, Durham, United States,
bHope for HIE, West Bloomfield, United States
BACKGROUND AND PURPOSE: Families of children with hypoxic ischemic encephalopathy (HIE) often express the desire to hear the stories of others who have endured similar struggles as them. Since the range of potential outcomes of HIE is wide, hearing a breadth of diverse stories can help parents cope with uncertainty, consider different possibilities, and conceptualize what the future might look like. Yet, the HIE family stories that do exist are scattered across different platforms. Storytelling is a powerful tool that bridges the divide that separates HIE families and providers, offers a window into the parent experience, and empowers families in their respective healing processes. By highlighting the narratives of families impacted by HIE and providers who treat HIE patients in a centralized location, the book aims to (a) spread awareness about HIE, (b) connect families to peer support, and (c) foster empathy and collaboration in family-provider interactions. A secondary aim is to explore how leveraging principles of narrative medicine and giving book participants a platform to voice their stories can help them cope with their unique circumstances.
METHODOLOGY: Families of infants with HIE and providers representing various specialties were recruited to share their stories for the book through their affiliation with Hope for HIE, a parent-support organization, from May-August of 2021. Families and providers completed semi-structured interviews over Zoom with the first author (SB), where they shared their experiences related to HIE. The interviews were recorded, transcribed, and synthesized into short stories. Each story was shared with the relevant family member or provider, and a collaborative editing process ensued. Families and providers were also offered the opportunity to submit visuals or poetry that represented their journeys with HIE. Written narratives and accompanying imagery were organized into a manuscript, with each participant story representing a chapter in the book.
RESULTS: 57 parents, 2 extended family members, and 13 providers completed 70 interviews. Parents were located all across the world, with eight countries represented. Providers encompassed an array of specialties including neurology, pediatrics, social work, neonatal therapy, physiatry, and nursing. A book cover (Image 1) and book title, HIElights of Hope, were chosen based on community input, speaking to two major themes that emerged from participant stories—that the definition of hope is fluid and that hope exists across a spectrum of outcomes.
CONCLUSION/IMPACT: The process of creating HIElights of Hope underscores the value of storytelling as a promising strategy to promote empathy and collaboration in family-provider interactions and to validate the emotionally-charged journeys of HIE families. It also highlights the importance of consistent collaboration with families in order to create resources that effectively meet their needs. HIElights of Hope is anticipated to be released in 2022 in both digital and print formats.
Stimulating the motor development of very premature infants: effects of early crawling training via a mini-skateboard, the Crawliskate
Barbu-Roth Ma, Dumuids Ma, Forma Va, Anderson Dd, Provasi Jb, Biran Vc
aUniversity of Paris, Integrative Neurosciences And Cognition Center UMR 8002 45 rue des Saints Peres 75006 Paris, France
bEcole Pratique des Hautes Etudes, Paris, France
cHopital Robert Debre INSERM U 1141, Paris, France
dMarian Wright Edelman Institute, San Francisco State University, USA
INTRODUCTION: The acquisition of postural control and mobility are central to human motor and cognitive development, yet these skills are delayed and compromised in very premature infants. A major, but under-investigated, question concerns the appropriate interventions for extremely premature infants who do not appear to have major brain damage. Here we present a new intervention based on very early crawling training via an innovative mini-skateboard, dubbed the Crawliskate, designed to raise the newborn’s head and trunk above the floor and permit prone propulsion in any direction (Barbu-Roth et al., 2016). Studies of one hundred typical newborns revealed that the Crawliskate preserved the natural alignment between the head, neck and spine and permitted efficient independent quadrupedal locomotion (Forma et al., 2019; Hym et al., 2020). Moreover, the Crawliskate allowed newborns to practice the coordination between their arms and legs and also practice rotations of their head and trunk.
HYPOTHESES: We hypothesized that stimulating crawling on the Crawliskate in very premature infants in the first months after discharge from the NICU would enhance their motor development in the first year of life.
METHODOLOGY: Forty-five very premature infants (born 24-32 weeks GA) without major brain damage were randomly assigned to a Crawliskate training (Crawli) or Mattress training (Mat) or non-training group (NT). Trained infants used the Crawliskate (Crawli group) or were positioned prone on a Mattress (Mat Group) for 5 min daily at home for 2 months as soon as they left the NICU. The infants’ motor development was assessed with the Bayley BSDI III at 2,6,9, and 12 months corrected age (CA).
RESULTS: BSDI III Gross motor scaled scores at all ages grouped were significantly higher in the Crawli group compared to the Mat or NT groups (p < 0.01 and no difference between Mat and NT groups). Moreover, at 12 months, 40% of Crawli group infants could walk with five independent steps compared to 21.4% in the Mat group (p<0.01) and 14.3% in the NT group (p<0.0001) with no difference between the Mat and NT groups.
CONCLUSION/IMPACT: These preliminary results show that training crawling early in extremely premature infants without major brain damage can stimulate their gross motor development. We are currently examining the effects of the intervention at later ages and on premature infants with brain damage incurred prenatally or perinatally.
Bibliography:
[1] Barbu-Roth, M. et al. (2016). Device for assisting the crawling of an infant. EP2974624A1 Forma V. et al. (2019). What does prone skateboarding in the newborn tell us about the ontogeny of human locomotion? Child Development, 90 (4), 1286-1302. DOI: 10.1111/cdev.13251
[2] Hym, C. et al. (2020). Newborn crawling and rooting in response to maternal breast odor. Developmental Science. DOI:10.1111/desc.13061.
The ALIGN framework: A parent-informed approach to prognostic communication
Barks Ma,b, Bansal Sb, Bernstein Sa, Pollak Ka, Glass Hc, Brandon Da, Lemmon Ma,b
aDuke University School of Medicine, Durham, United States
bDuke-Margolis Center for Health Policy, Durham, United States, 3UCSF School of Medicine, San Fransisco, United States
BACKGROUND AND PURPOSE: Clinicians often communicate complex, uncertain, and distressing information about neurologic prognosis to parents of critically ill infants. Few tools exist to guide prognostic communication. We aimed to develop a parent-informed framework to communicate prognostic information.
METHODOLOGY: Parents of infants with neurologic conditions in the intensive care unit were enrolled in a longitudinal study of decision-making from 2018-2020. Parents completed semi-structured interviews after meetings with the health care team, at hospital discharge, and 6 months after discharge. All interviews targeted information about parent preferences for prognostic disclosure, including a series of questions like “What has the team done well as they’ve talked with you about your child’s future?” and “What advice do you have for doctors who need to talk with families about their child’s future?” Interviews were audio-recorded, transcribed, and de-identified. We used a conventional content analysis approach to analyze the data; a codebook was developed and refined iteratively to characterize the content and context of parent preferences for prognostic communication. Two study team members coded all interview transcripts and discrepancies were resolved via team consensus. NVIVO 12 qualitative software was used index and organize codes.
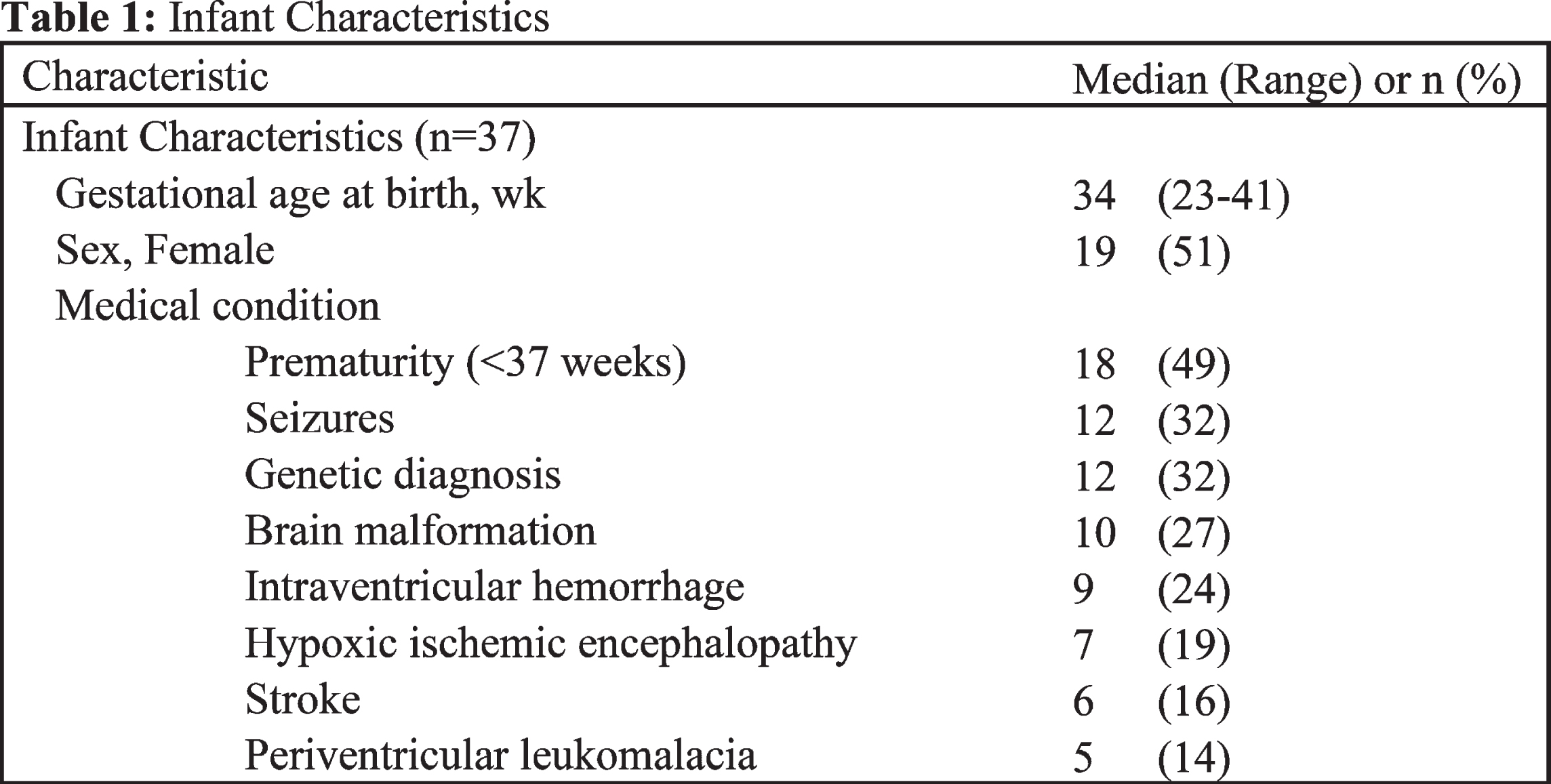
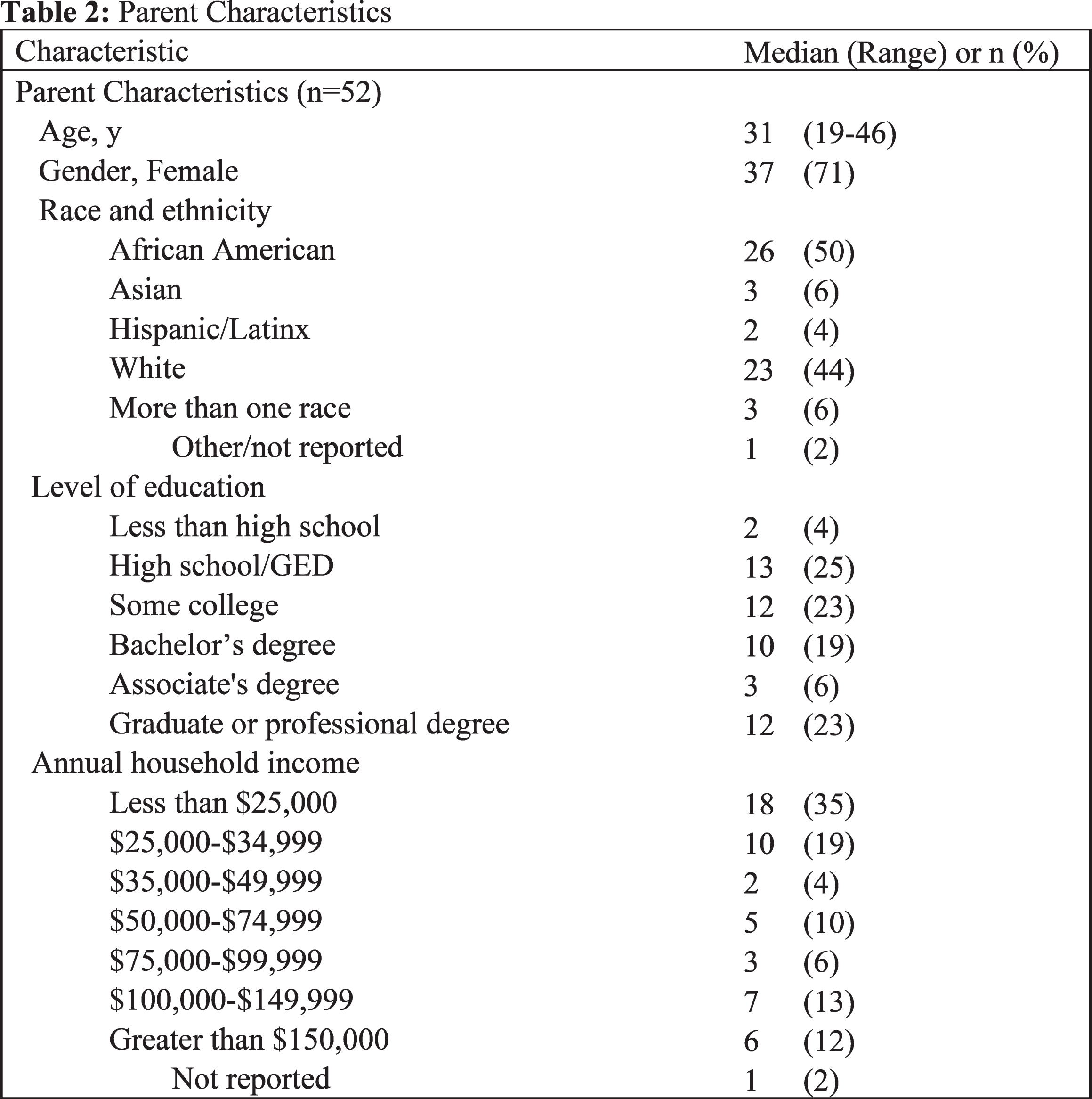
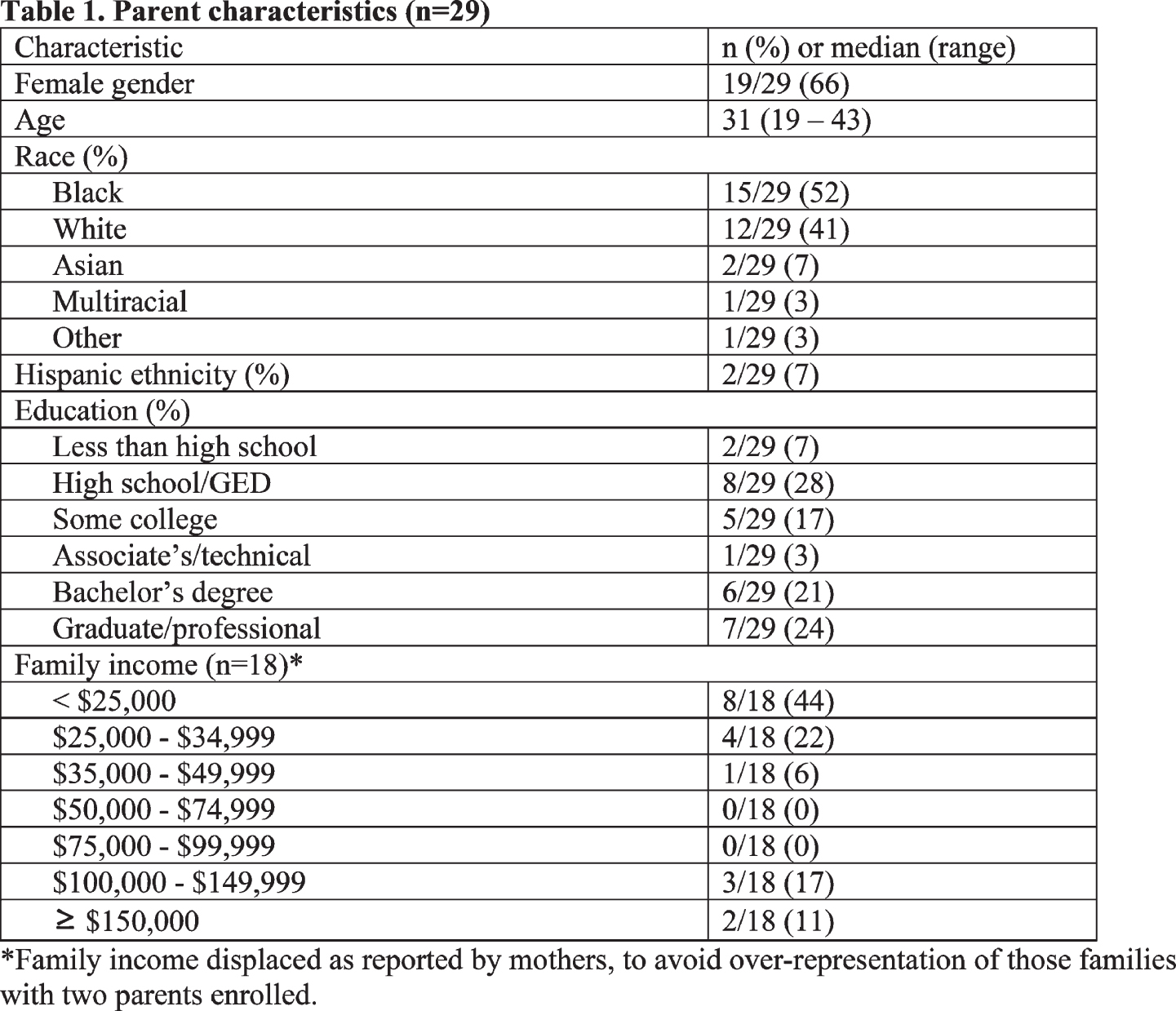
RESULTS: Fifty two parents of 37 infants completed 123 interviews (Table 1). Parents were predominantly mothers (n=37/52, 71%) with a median parent age of 31 (range 19-46). The majority identified as black (n=26/52, 50%) or white (n=23/52, 44%), and a minority reported Hispanic ethnicity (n=2/52, 4%). We identified five themes, organized into phases of prognostic communication (Approach, Learn, Inform, Give support, and Next steps: ALIGN): 1) Approach: Parents appreciated receiving frequent, consistent information about their child’s outcome from clinicians who knew their child well. 2) Learn: Parents valued when clinicians asked them how they preferred receiving information and what they already knew about their child’s outcome prior to information delivery. 3) Inform: Parents valued honest, thorough, and balanced information that disclosed prognostic uncertainty and acknowledged room for hope. 4) Give support: Parents valued empathic communication and appreciated clinicians who offered real-time emotional support. 5) Next steps: Parents appreciated clinicians who connected them to resources, including peer support.
CONCLUSION/IMPACT: The ALIGN framework offers a novel, parent-informed strategy to effectively communicate neurologic prognosis (Figure 1). While ALIGN represents key elements of a conversation about prognosis, each clinician can adapt this framework to their own approach. Future work will assess the impact of this framework on communication quality and prognostic understanding.
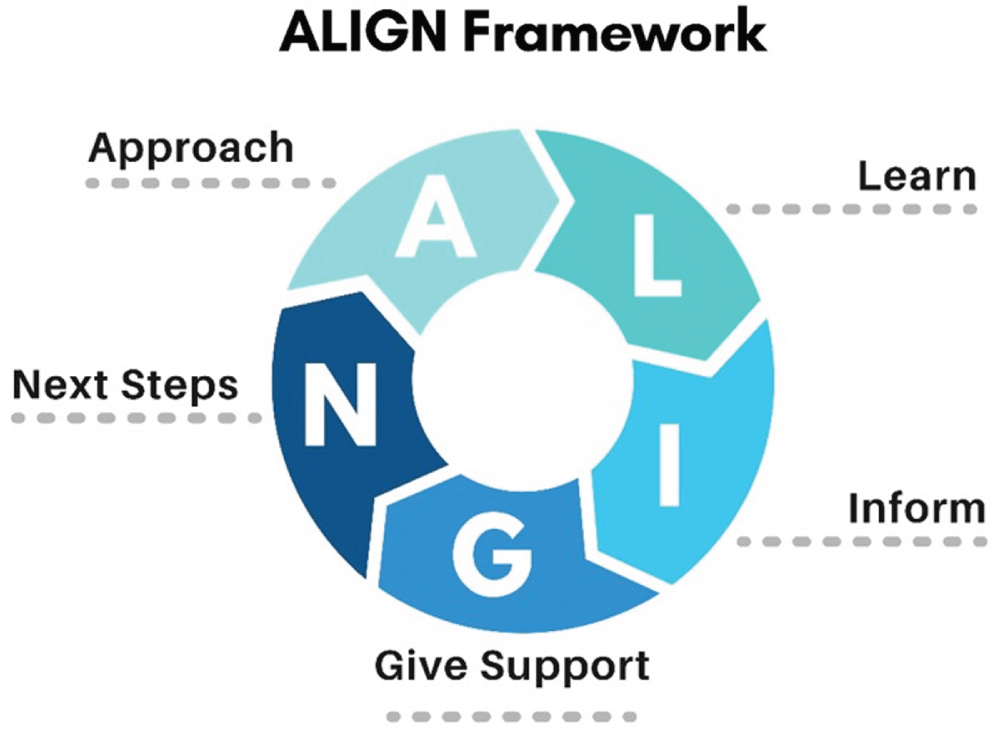
The ALIGN framework acknowledges that conversations about prognosis are often iterative and must be revisited over time. While ALIGN represents key elements of a conversation about prognosis, each clinician can adapt this framework to their own approach.
Decisional satisfaction, regret, and conflict among parents of infants with neurologic conditions in the intensive care unit
Barlet Ma, Ubel Pa,b,c, Weinfurt Kd, Glass He,f, Pollak Kd, Brandon Dg,h, Lemmon Md,h
aDuke University School of Medicine, Durham, USA
bFuqua School of Business, Duke University, Durham, USA
cSanford School of Public Policy, Duke University, Durham, USA
dDepartment of Population Health Sciences, Duke University, Durham, USA
eDepartment of Neurology and Pediatrics, University of California San Francisco, San Francisco, USA
fDepartment of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, USA
gDuke University School of Nursing, Durham, USA
hDepartment of Pediatrics, Duke University School of Medicine, Durham, USA
BACKGROUND AND PURPOSE: Parents of infants with neurologic conditions face high-stakes decisions, but little is known about their decision-making experience. The goals of this study were to (1) characterize decisional satisfaction, regret, and conflict among parents of critically ill infants with neurologic conditions and (2) characterize the relationship between maternal and paternal decision outcomes.
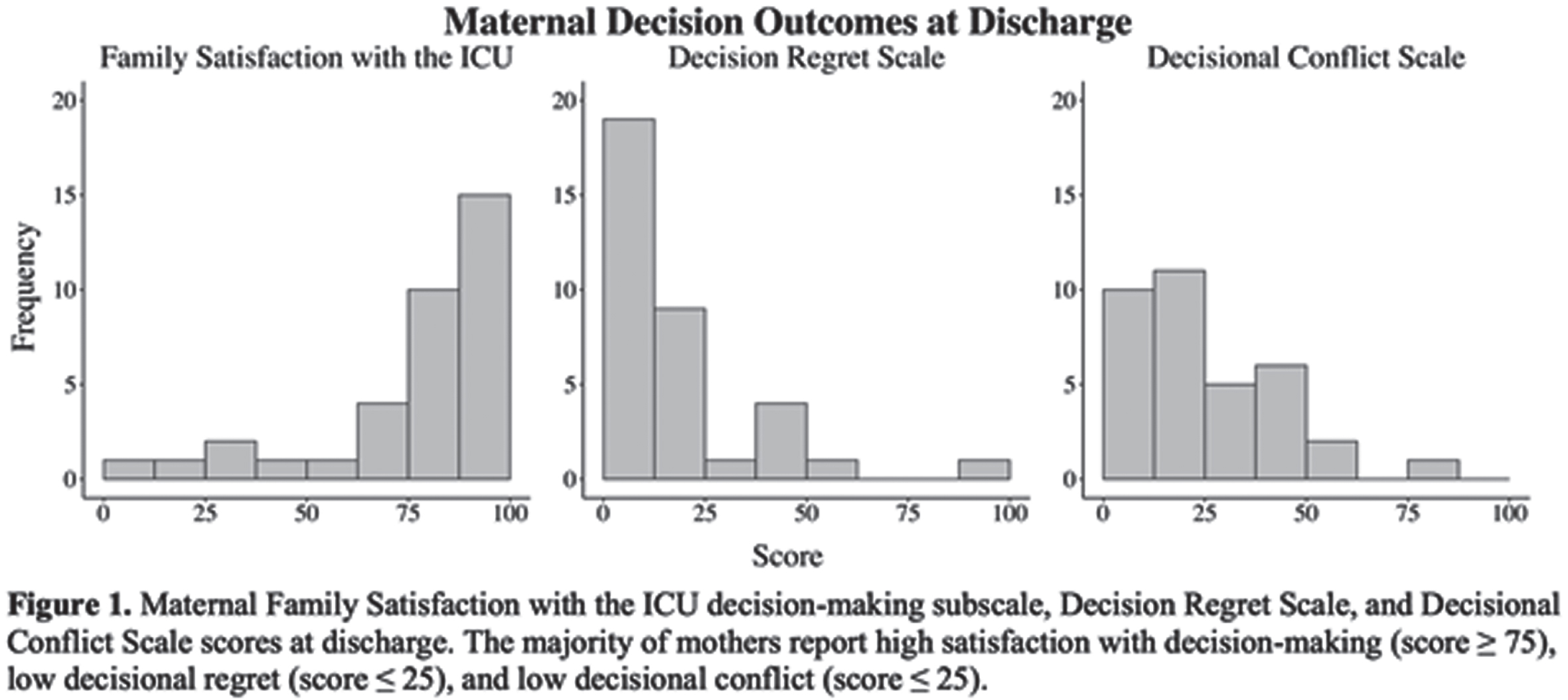
METHODOLOGY: In this prospective cohort study, we enrolled parents of infants < 1 year old with neurologic conditions who were hospitalized in the intensive care unit (ICU). Hospital discharge surveys included the validated Family Satisfaction with the ICU decision-making subscale, Decision Regret Scale, and Decisional Conflict Scale. We defined high satisfaction with decision-making as a Family Satisfaction with the ICU decision-making subscale score ≵ 75 and high decisional regret or conflict as a Decision Regret Scale or Decisional Conflict Scale score > 25, consistent with existing literature. Within-couple disagreement was defined as a difference between scores of at least 25 points.
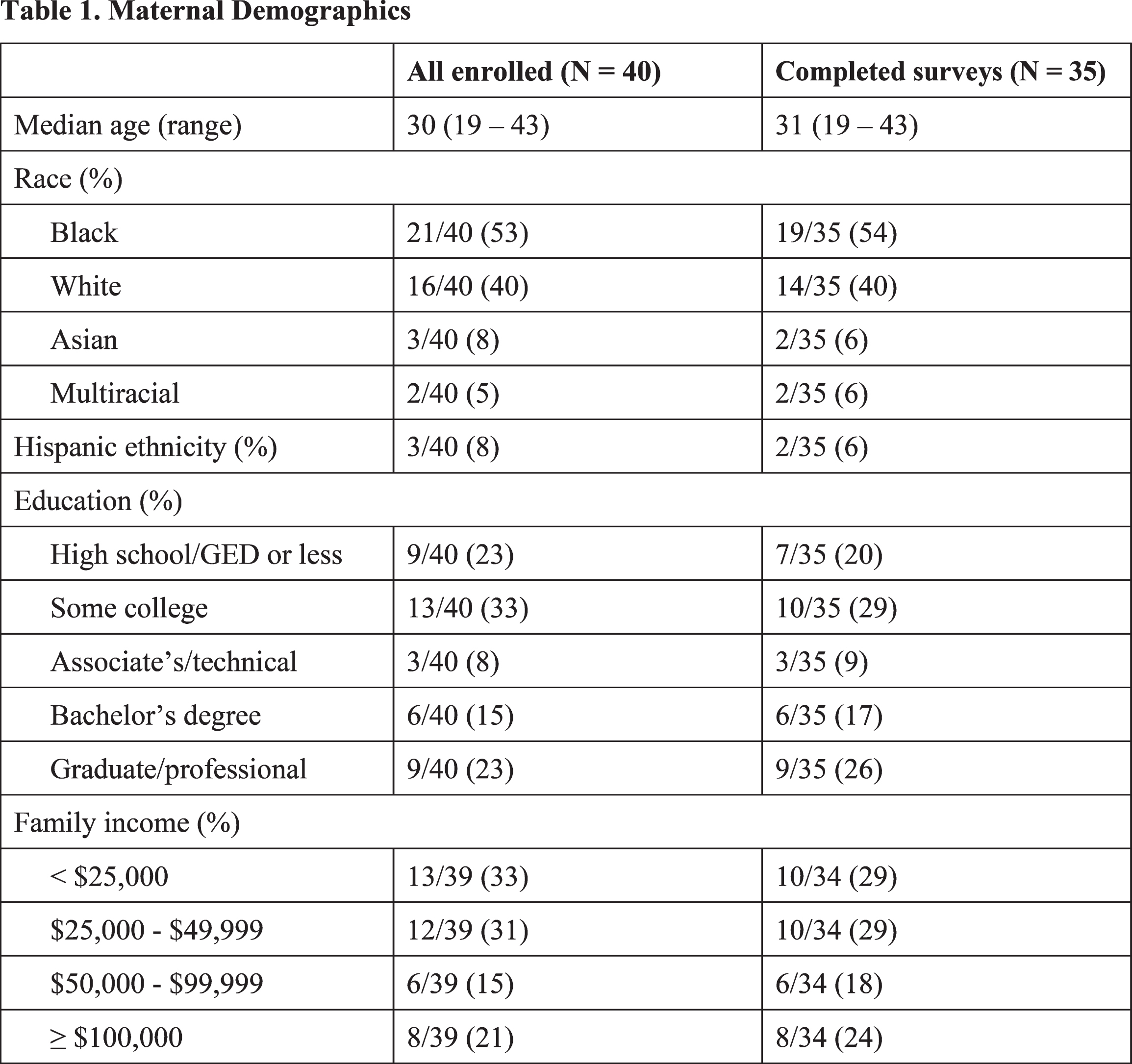
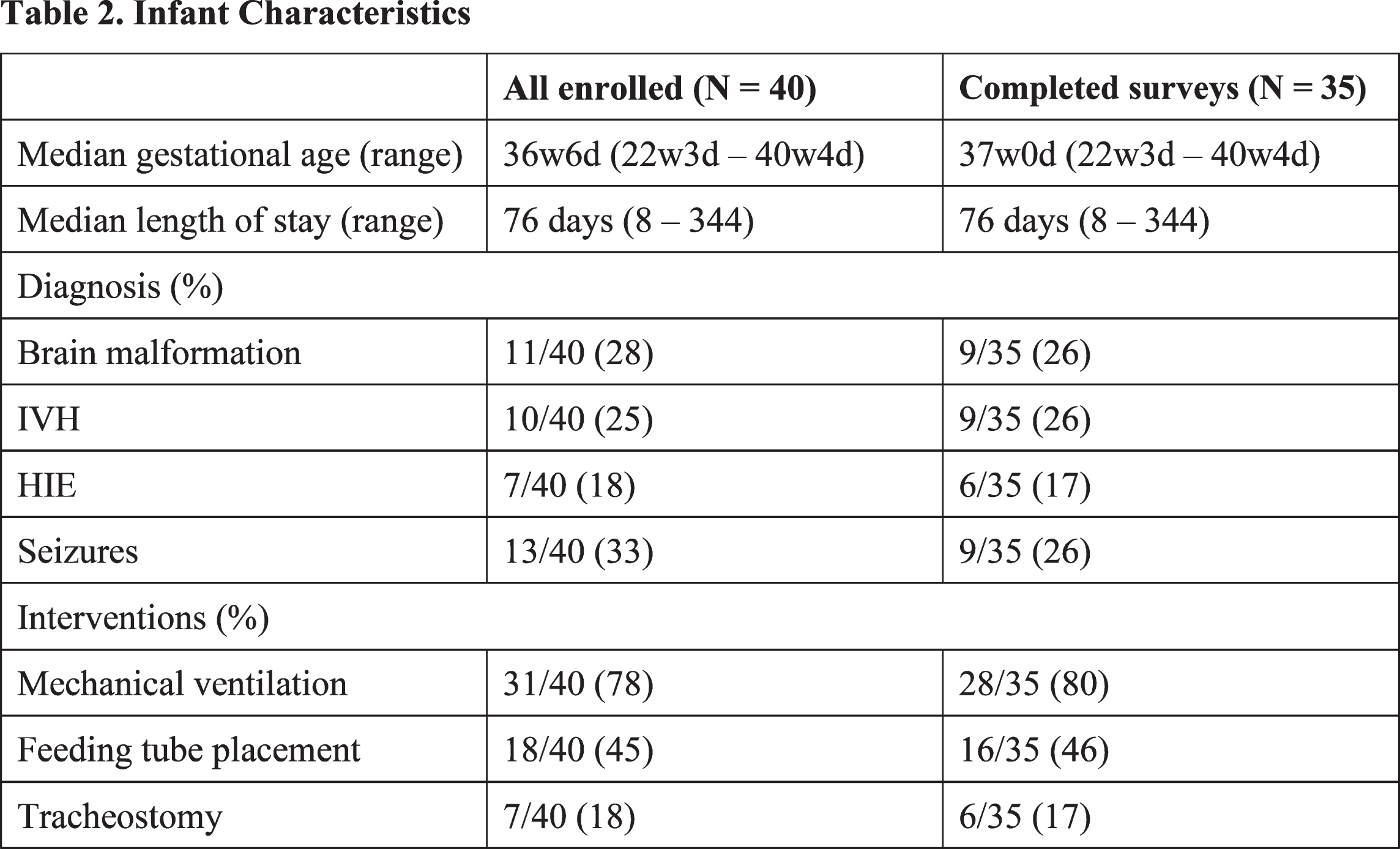
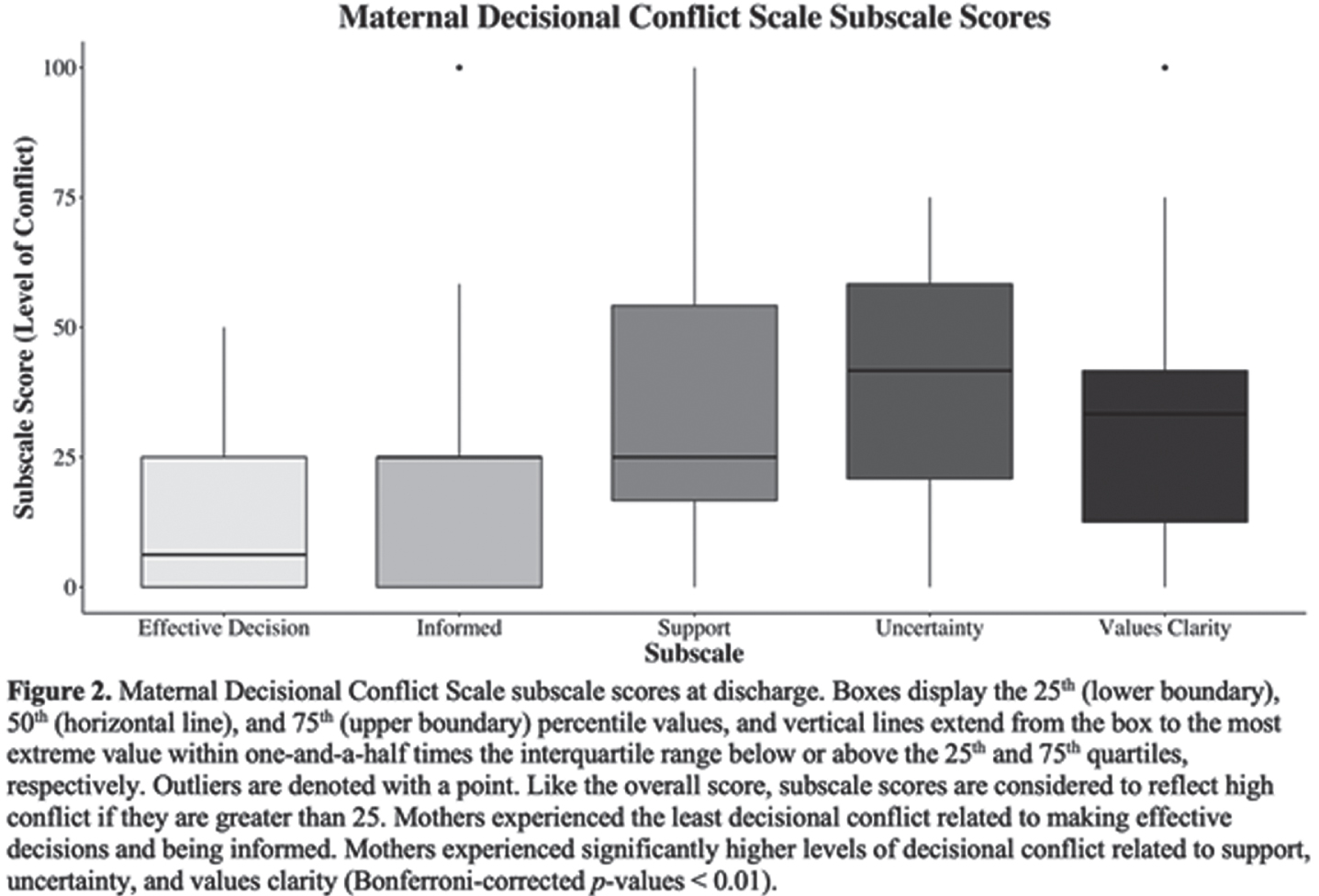
RESULTS: We enrolled 61 parents of 40 infants (n = 40 mothers, n = 21 fathers) (Tables 1 and 2). Thirty-five mothers and 15 fathers completed discharge surveys. The median maternal Family Satisfaction with the ICU decision-making subscale score was 87.5, with 77% reporting high satisfaction with decision-making. The median maternal Decision Regret Scale score was 10, with 20% reporting high decisional regret. The median maternal Decisional Conflict Scale score was 23.4, with 40% reporting high decisional conflict (Figure 1). Among Decisional Conflict Scale subscales, mothers reported significantly more conflict in the domains of support, uncertainty, and values clarity as compared to the domains of making effective decisions or being informed (Bonferroni corrected p-values < 0.01) (Figure 2). There were no significant average differences between mothers and fathers for any decisional outcome. While maternal and paternal scores were moderately positively correlated for the Family Satisfaction with the ICU decision-making subscale (τ = 0.59, p = 0.004), there was no statistically significant correlation between maternal and paternal scores for the Decision Regret Scale or Decisional Conflict Scale. Nearly half of couples had disagreement between Decisional Regret Scale scores (n = 7/15) and one-third had disagreement between Decisional Conflict Scale scores (n = 5/15).
CONCLUSION: While most parents of critically ill infants with neurologic conditions have high satisfaction with decision making and low decisional regret, a substantial proportion experience decisional conflict. There were no significant group-level differences in decisional outcomes for mothers and fathers, but individual couples frequently experienced different levels of decisional regret and conflict. These results suggest that the decision-making process is challenging for parents even if they are ultimately satisfied with their decisions, underscoring the need for decision interventions that target parents individually and address the domains of support, uncertainty, and values clarity.
Development outcome of preterm infants at high risk of perinatal brain damage with early treatment
Barrera Resendiz Ja, Harmony Tb
aNational School of Higher Studies Unit Leon, Leon, Mexico
bNeurodevelopment Research Unit, Institute of Neurobiology, Santiago de Queretaro, Mexico
BACKGROUND: The prognosis in the neuro development of premature infants will always be reserved, because it varies greatly between each individual and is directly linked to the type and number of risk factors to which they were exposed, the week of gestation in which the event occurred, among others; which can result in different patterns of injury, among which is the decrease in the growth of brain structures. Early treatment aims to minimize the expression of the sequelae of perinatal brain damage by seeking psychomotor development as close as possible to normality.
PURPOSE: To analyze psychomotor development in preterm infants at high risk of brain damage with physical treatment during the first two years.
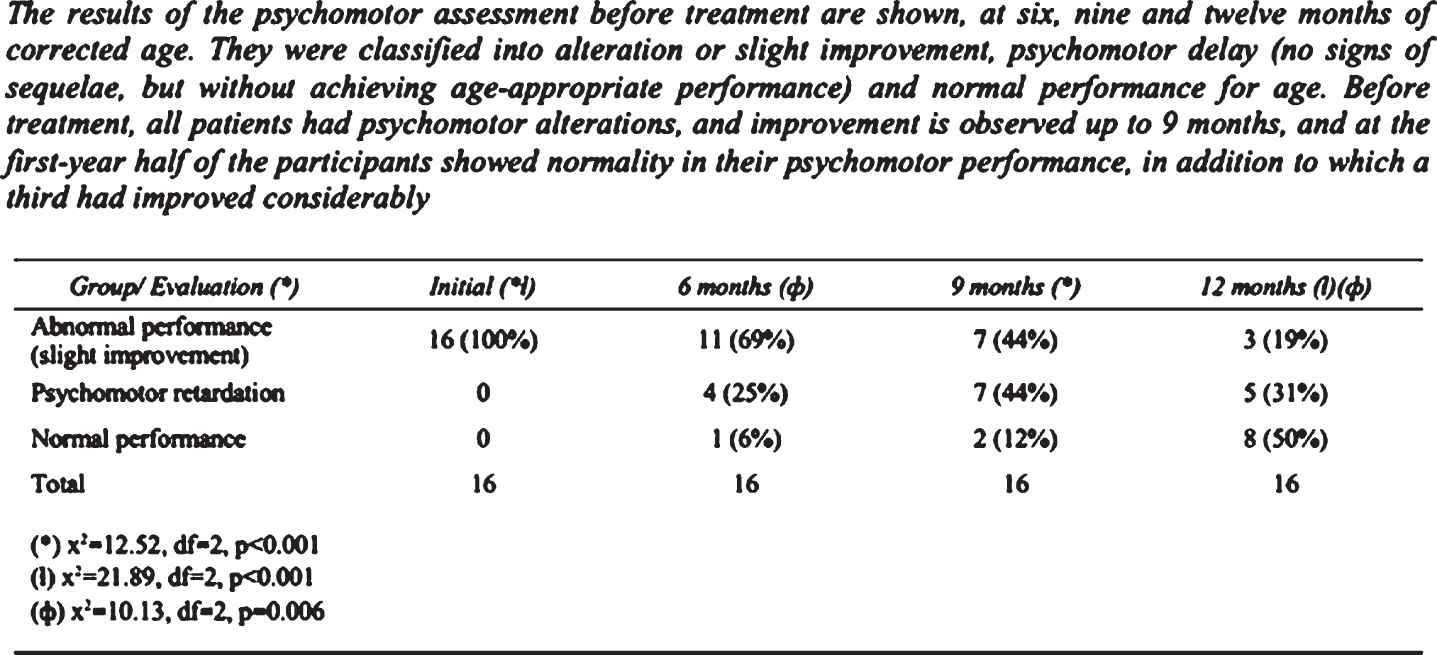
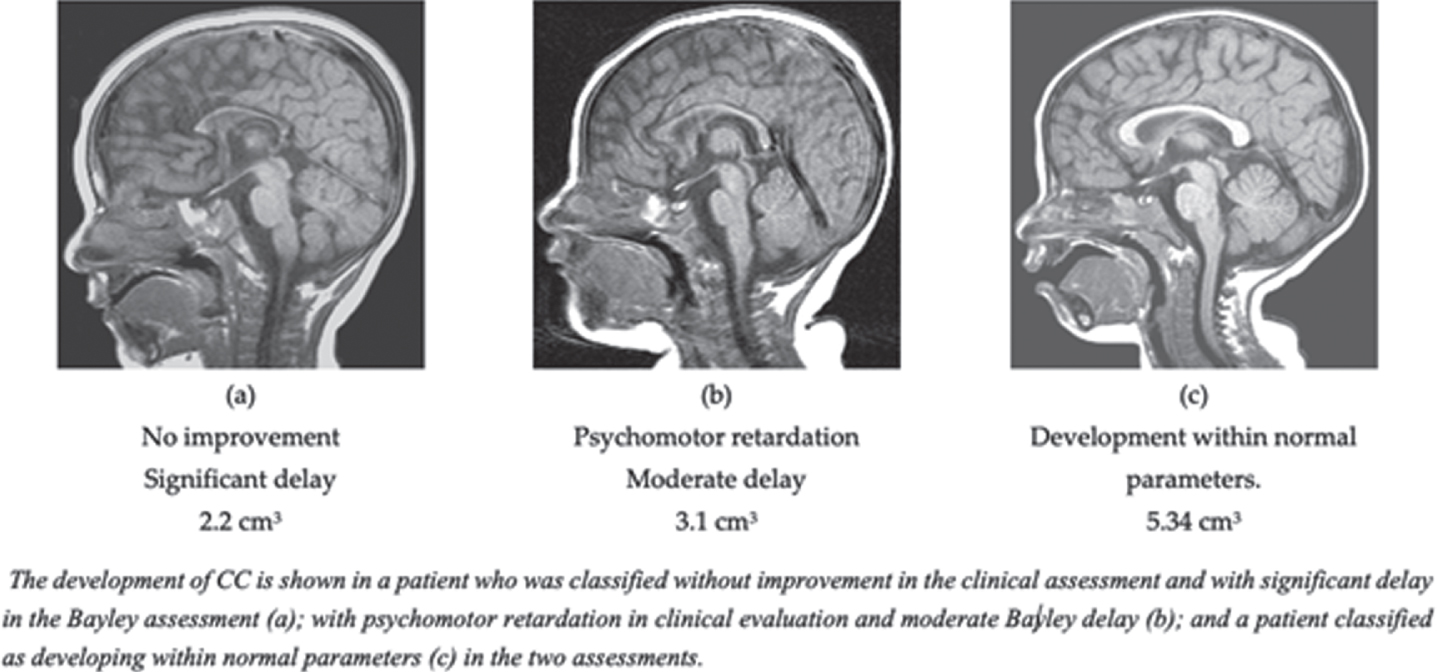
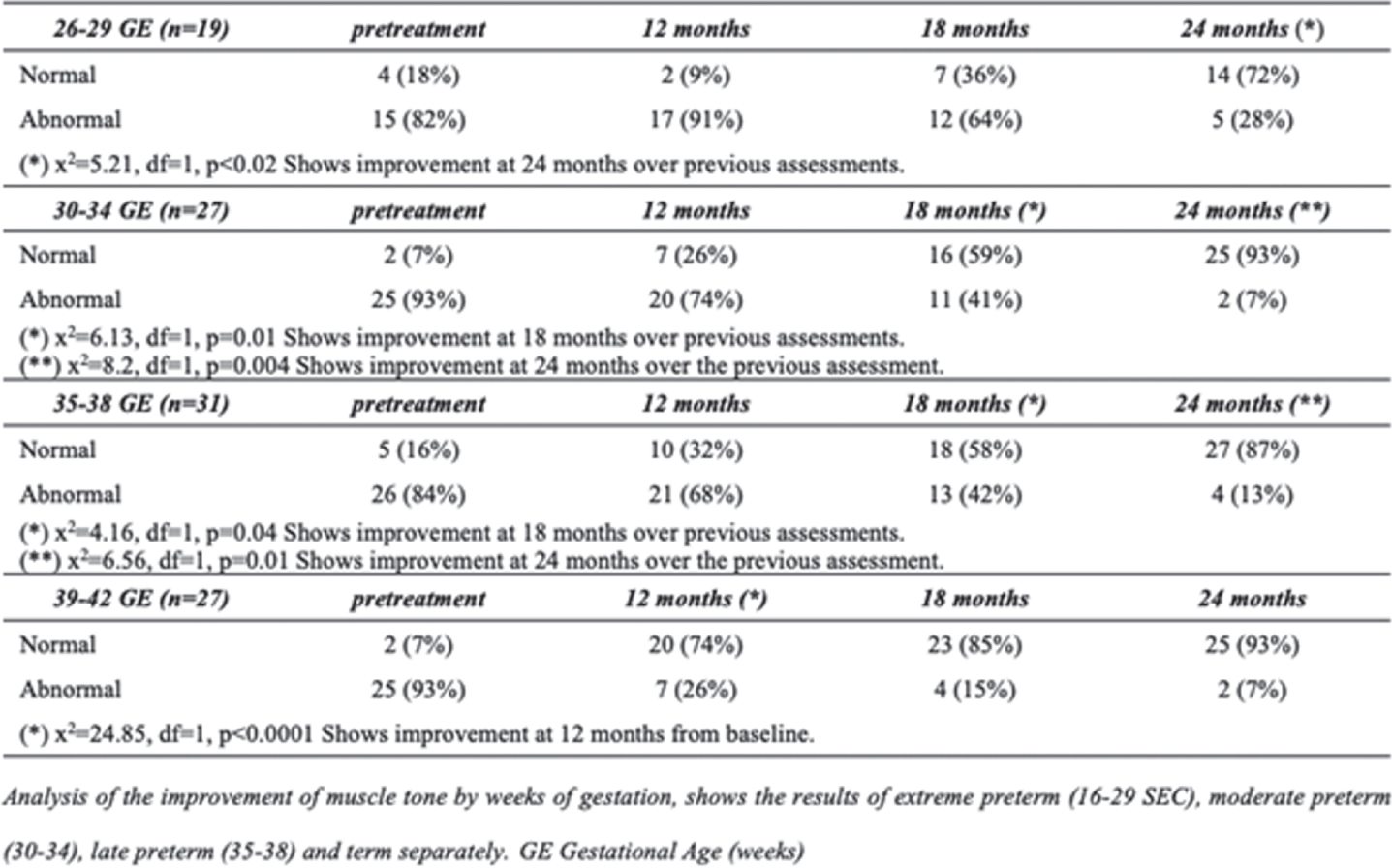
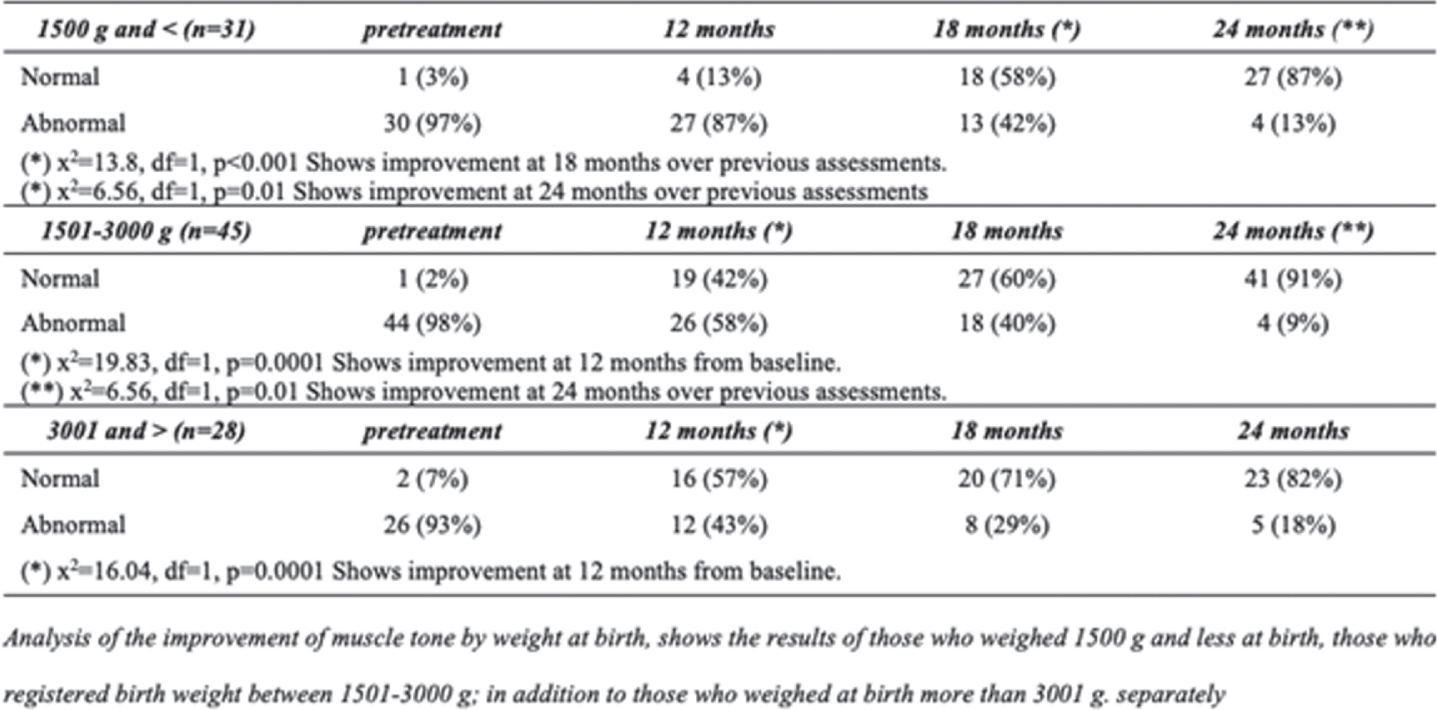
MATERIALS AND METHODS: Preterm infants at high risk of brain damage in the period 2008-2018 were included. Treatment was started before eight weeks of corrected age, it was performed once a day for the first two years. Evaluations were performed before starting treatment, at 4-8-12-18 and 24 months of age corrected with the Bayley-II Child Development Scale, the Amiel-Tisson neuropediatric evaluation and by a rehabilitation doctor, in addition the MRI study was carried out to assess brain volumetry.
RESULTS: Preterm infants with early treatment improve (p>0.05) their clinical conditions in neuropaediatric evaluation and rehabilitation, presented Bayley mental and motor scale scores within normal parameters for age and the development of the corpus callosum is related to psychomotor performance.
CONCLUSIONS: Early treatment allows to minimize the expression of sequelae in preterm infants at high risk of brain damage when two important points of treatment follow: start before eight weeks of corrected age and constancy in treatment until at least 24 months.
Bibliography: Barrera-Reséndiz, J. E. (2015). Terapia Neurohabilitatoria. Ciudad de México: Publicaciones y Fomento Editorial. UNAM. Garófalo-Gómez, N., et al. (2019). Outcome at Age Five Years or Older for Children with Perinatal Brain Injury Treated With Neurohabilitation or Neurodevelopmental. EC PAEDIATRICS, 8(10), 1090–1098. Harmony, T. (2017). Outcome of Infants at Risk of Brain Damage after Katona Neurohabilitation Therapy. International Journal of Neurorehabilitation, 04(03). https://doi.org/10.4172/2376-0281.1000277
Discussion of neuroimaging with parents of critically ill infants
Canfora Ma, Barks Mb, Barlet Mb, Bernstein Sc, Lemmon Mb
aDepartment of Neuroscience, Duke University Trinity College, Durham, United States
bDuke University School of Medicine, Durham, United States
cUniversity of Utah School of Medicine, Salt Lake City, United States
Objectives: Clinicians in the neonatal intensive care unit (NICU) use neuroimaging to inform prognostication. Parents often rely on information gained from brain imaging to understand their child’s diagnosis, prepare for life at home, and support complex decision-making. This study aimed to characterize the behavior and language that clinicians use to communicate neuroimaging results during family conferences in the NICU.
METHODS: In this longitudinal, mixed methods study, we enrolled parents of critically ill infants with a diagnosed neurologic condition and planned family conference. Family meetings between clinicians and parents of enrolled infants were audio recorded, transcribed, and de-identified. Transcripts were screened for discussions of neuroimaging. Emergent themes and subthemes were identified using a conventional content analysis approach. Each transcript was independently coded by at least two team members (MCB, MHB, MC) and differences were resolved in consensus with the senior author. NVIVO 12 was used to index and organize codes. We reviewed infant charts and parent surveys to obtain demographic and clinical information.
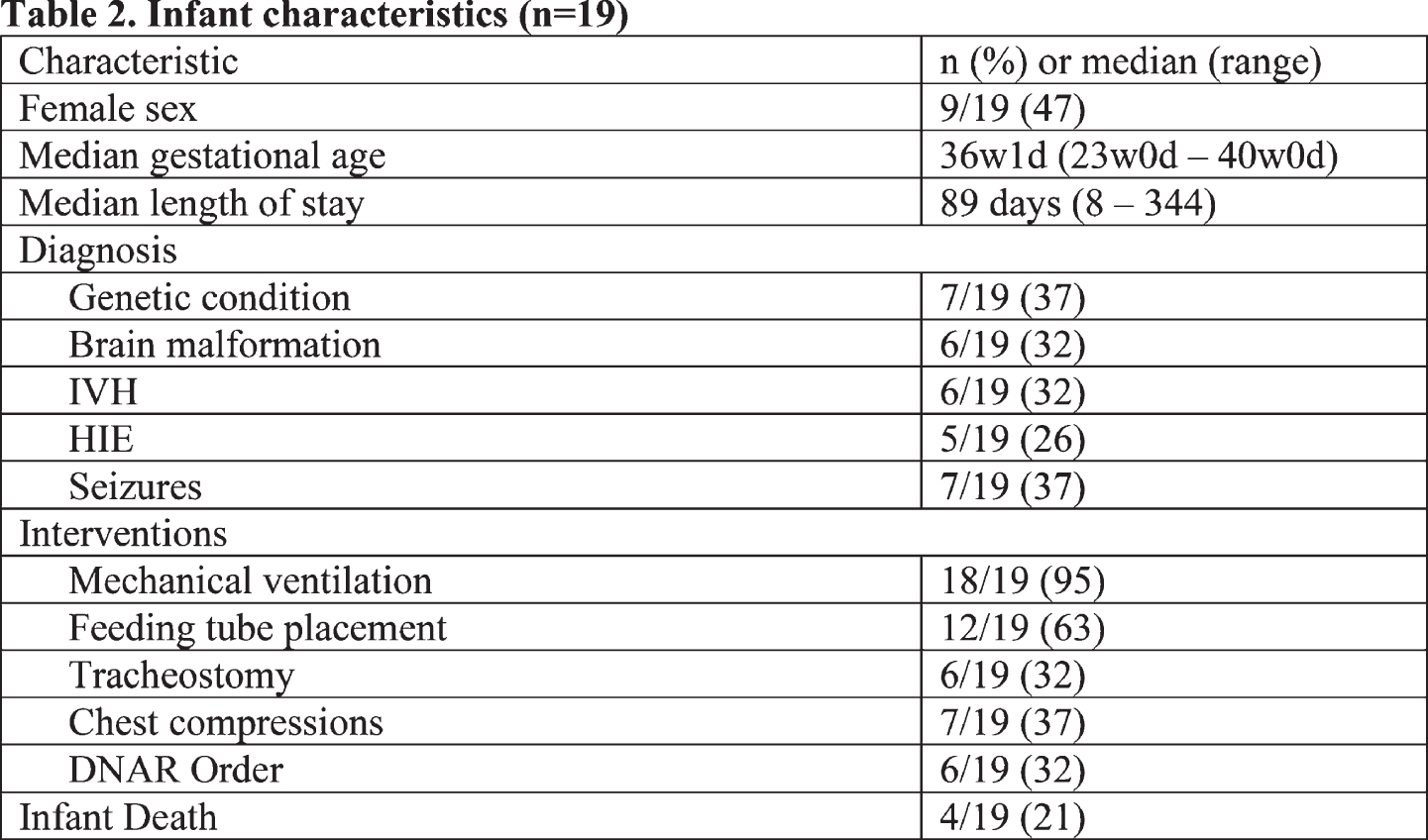
RESULTS: Sixty-eight family conferences involving 36 parents of 24 infants were screened for neuroimaging discussion. Nineteen infants and 29 parents had one or more family conference where neuroimaging, including discussion of magnetic resonance imaging and head ultrasound, were present (n=37/68, 54%) (Tables 1 and 2). Clinicians initiated neuroimaging discussions the majority of the time (n=22/37, 59%); in a minority of meetings, clinicians began discussions by assessing parents’ baseline understanding of their child’s neuroimaging findings (n = 9/37, 24%). In most conferences (n = 30/37, 81%), clinicians and parents discussed the results of infants’ neuroimaging; the majority of these conferences included discussions of abnormal findings (n=26/30, 81%). Clinicians reviewed the primary image with parents in nearly one-third of conferences where results were discussed (n=9/30, 30%). Clinicians who reviewed imaging in real-time always oriented parents to the location of the brain’s anatomical structures (n=9/9, 100%) while reviewing the primary image; in two meetings (n=2/9, 22%) clinicians sketched a picture of the infants’ brain to help parents recognize specific findings. Clinicians described how an infant’s neuroimaging results were related to their current clinical presentation (n=25/37, 68%) and future neurodevelopmental outcomes (n=26/37, 70%) in the majority of meetings; how results were relevant to clinical decision-making was discussed in 41% of meetings (n=15/37). Approximately half of discussion of neuroimaging results included outlining limitations of the modality (n=20/37, 54%).
CONCLUSIONS: In this study, we characterized the content and nature of neuroimaging discussion for a cohort of critically ill infants. This discussion was typically clinician-initiated and used to inform discussion of an infant’s current status, expected outcome, and clinical decision-making. Future directions include obtaining parent perspectives on preferred communication behaviors and the development of communication tools to facilitate communication of neuroimaging results.
The Impact of Holding during Hypothermia on Infant Vital Signs and Salivary Cortisol Levels
Craig Aa, Fox La, Deerwester Ka, Kaneko-Tarui Tb, Cutler Ac, Maron Jd
aBarbara Bush Children’s Hospital at Maine Medical Center, Portland, United States
bMother Infant Research Institute, Boston, United States
cCenter for Outcomes Research at Maine Medical Center Research Institute, Portland, United States
dWomen & Infants Hospital of Rhode Island, Providence, United States
Background: The inability to hold an infant undergoing therapeutic hypothermia (TH) is a significant source of parental stress. Maternal holding for 30-minutes has been shown to be feasible in 10 neonates undergoing TH. We assessed the impact of holding on infant vital signs and maternal and infant salivary cortisol levels.
METHODS: Single-center, prospective crossover study with infants randomized to a 30-minute holding intervention on day-2 vs. day-3 of TH. We used a 90cm x 60cm x 0.65cm foam insulating pad to create a thermal barrier between mother and infant during holding. We recorded the neonatal heart rate, respiratory rate, mean arterial pressure (MAP) and esophageal temperature every 2-minutes for 30-minutes on the day the infant was held and also at the same time on the alternate day when the infant was not held (“no-holding day”). We collected saliva samples pre- and post- both holding and no-holding. To account for the crossover design, mixed effects models assessing the association between infant outcomes and holding treatment also included the interaction of treatment with the sequence (holding on day-2 vs. day-3) and a random subject effect. For outcomes measured every 2-minutes during the observation period, time was also included as a fixed effect to assess change during the observation period.
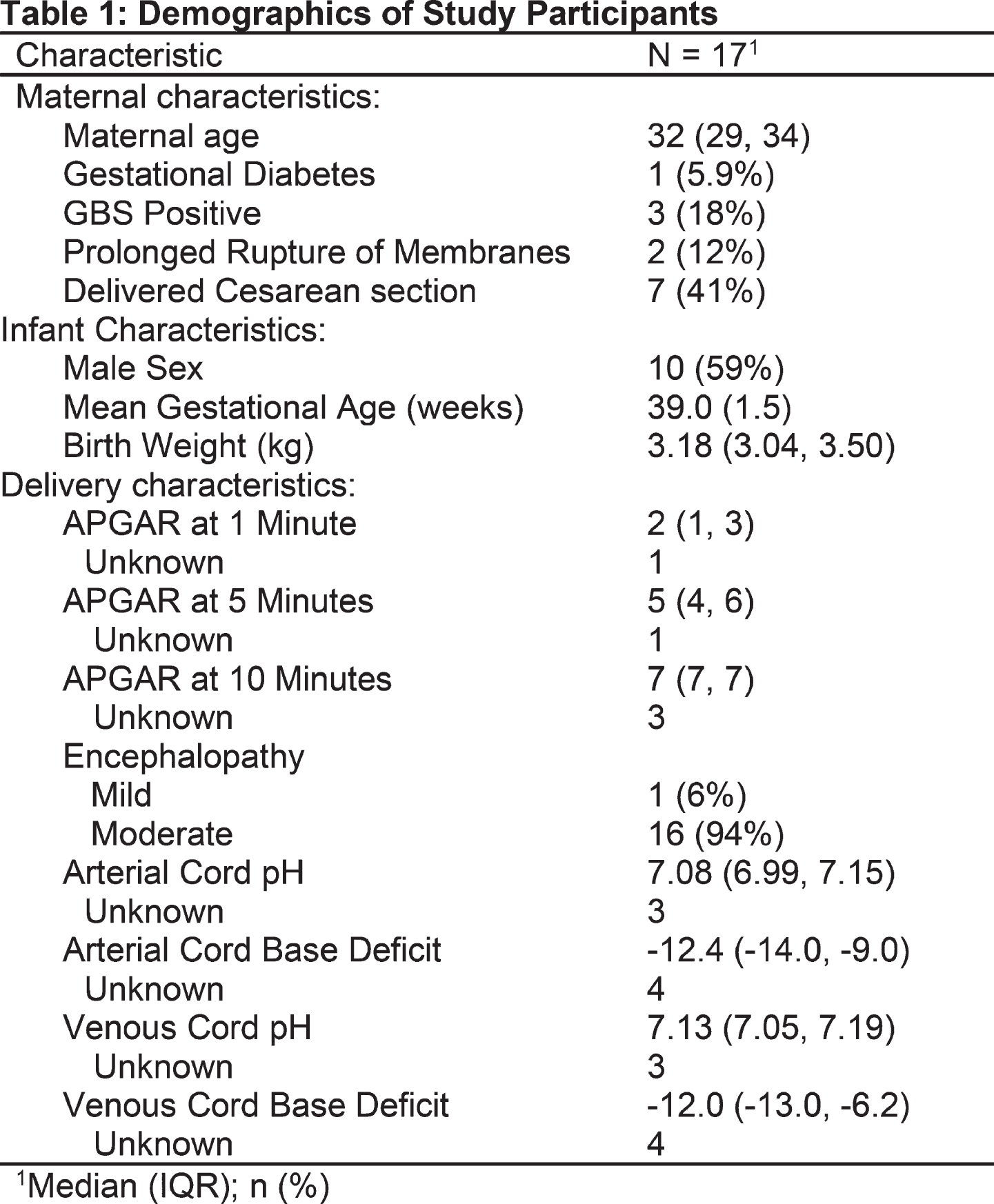
RESULTS: 17 mother-infant dyads participated; the median maternal age was 32 years (IQR 29, 34) and 41% delivered by C-section. Ten neonates were male (59%) with mean gestational age of 39 (SD 1.5) weeks (Table 1).
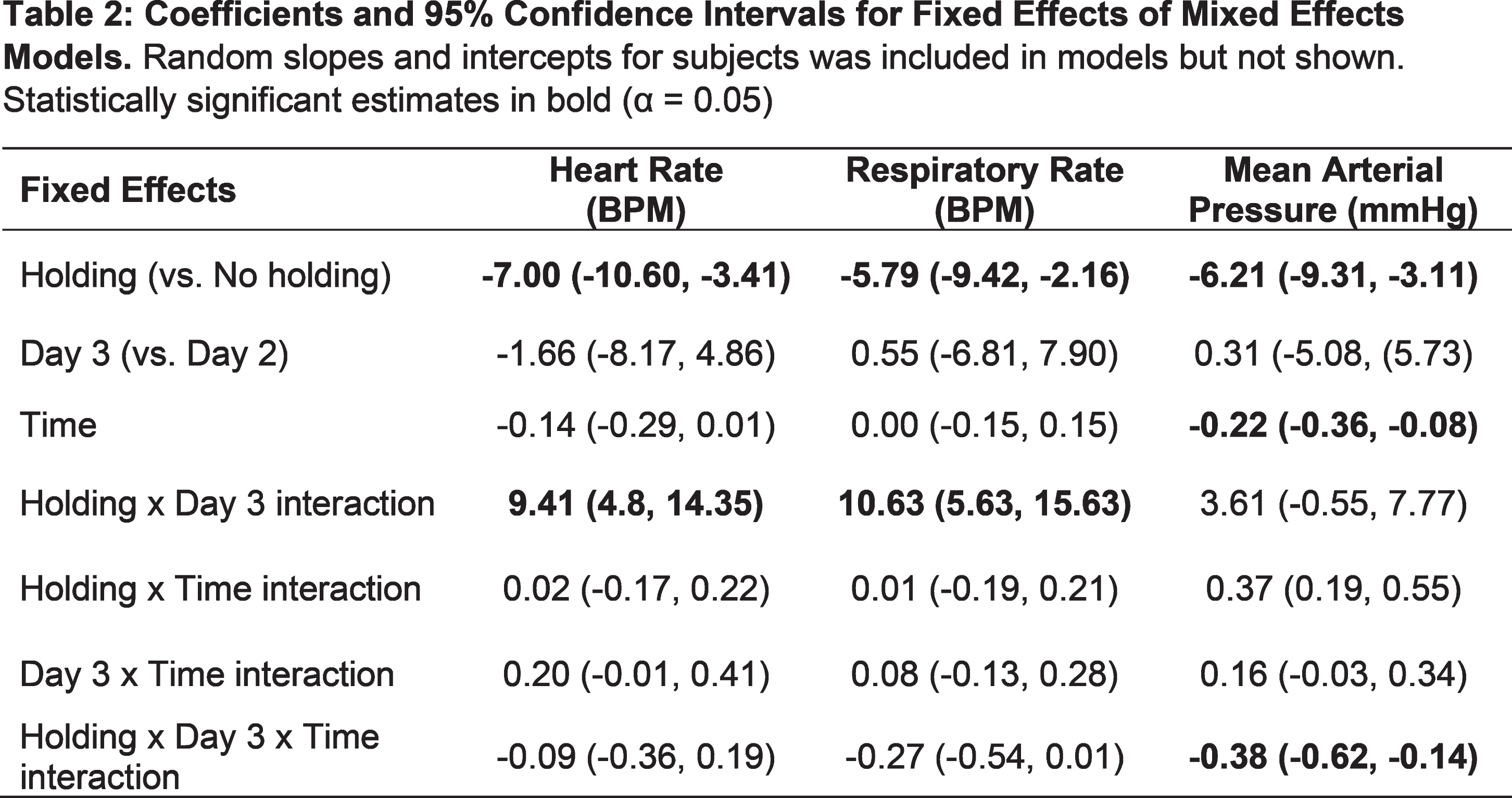
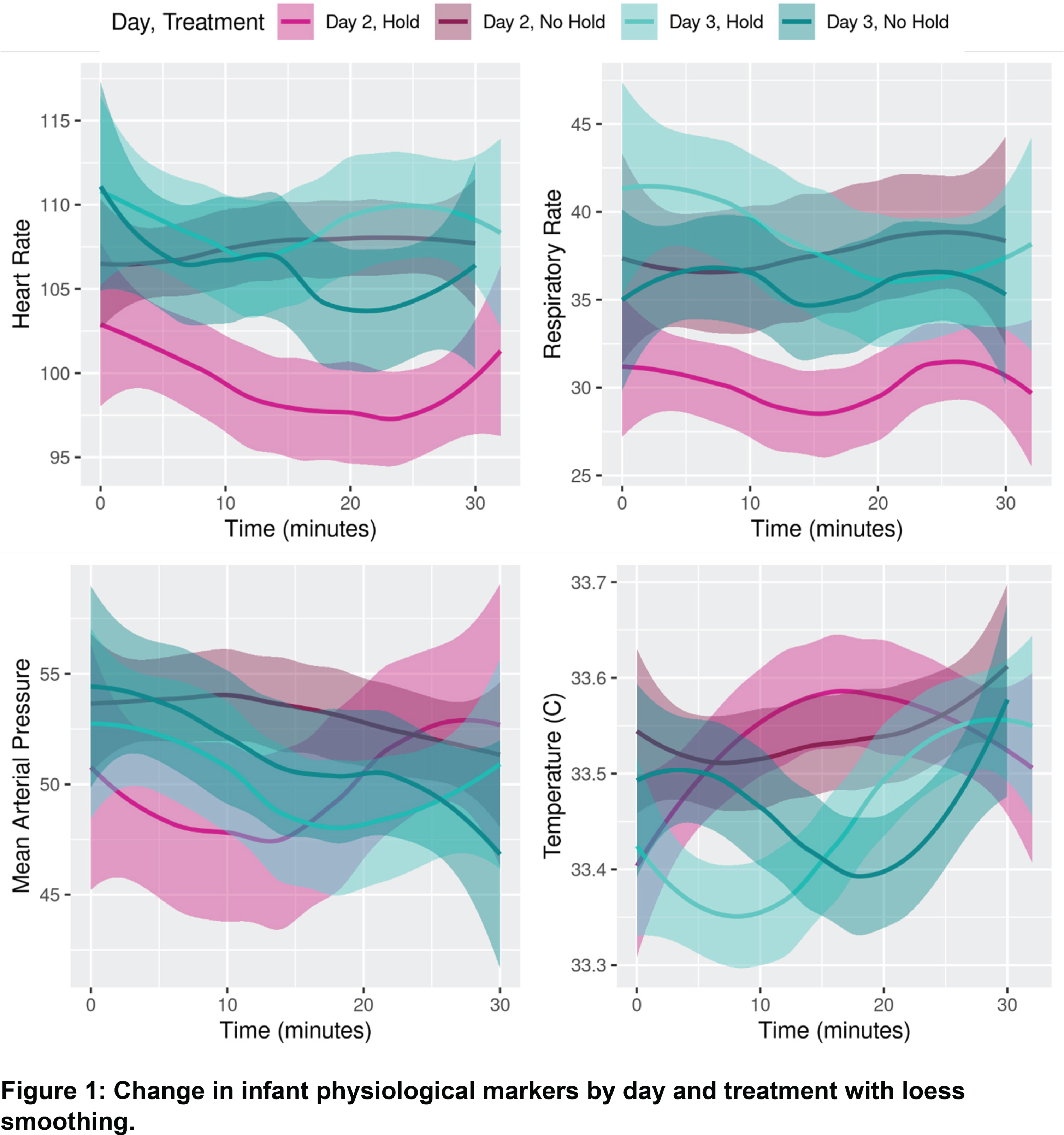
The temperature did not differ between the holding or no-holding days (p=0.58). There were fluctuations in temperature, but all within the accepted range of 33-34°C (Figure 1). The heart rate, respiratory rate and MAP all demonstrated statistically significantly lower values on the holding day (Table 2). There was a significant interaction for the effect of holding with the day holding occurred (Table 2), with holding only having an effect on day-2, not on day-3.
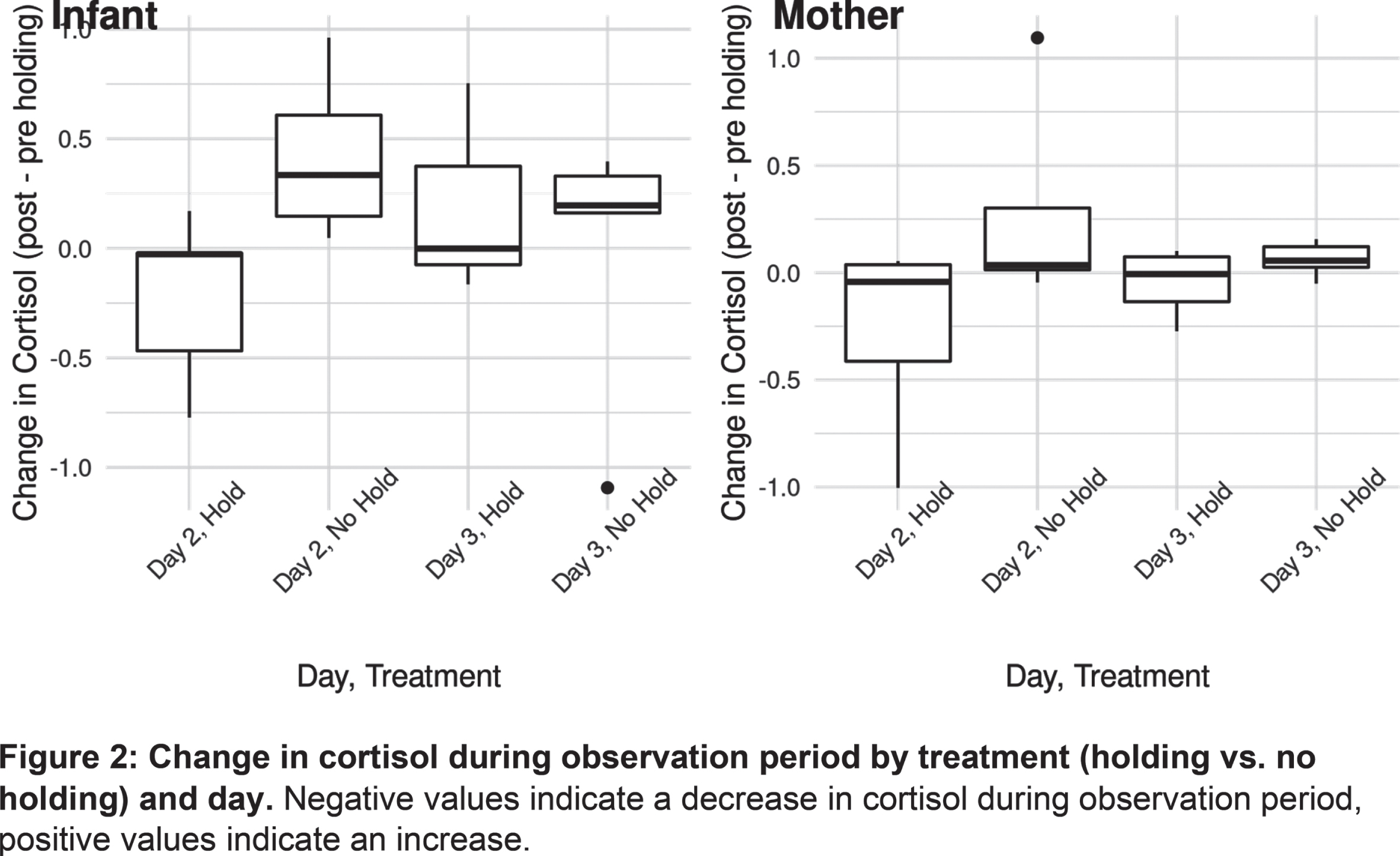
Cortisol significantly decreased during holding in both infants (p = 0.02) and mothers (p=0.01) (Figure 2). Additionally, infants had a significantly larger drop in cortisol on day-2 compared to day-3 (p=0.03), whereas mothers did not have a significant difference in cortisol change by day (p=0.10).
CONCLUSION: Our data show significantly lower infant heart rate, respiratory rate and MAP during holding on day-2 with a corresponding decrease in salivary cortisol when compared to “no-holding”. Unexpectedly, this effect was not evident when the infant was held on day-3. The reason for a lack of response on day-3 is unclear at this time and future investigation will evaluate the effect of holding on days 1, 2 and 3 in a larger cohort to ascertain if these results are reproducible.
A Music-Based Intervention to Reduce Stress in the Hospitalized Preterm Infant
Forde Ma, Sunwoo J, El-Dib M, Inder T, Erdei C
aBrigham and Women’s Hospital, Boston, United States
BACKGROUND AND PURPOSE: Preterm infants experience increased stress while hospitalized in the Neonatal Intensive Care Unit (NICU), (1) which can disturb their physiologic state and contribute to later developmental impairments. (1,2) Music-based interventions are enriching experiences that may reduce stress and improve high-risk infant neurodevelopment. (3-5) Little is known about which music conditions and stimulus characteristics correlate with improvement of physiologic measures of stress in preterm infants. (3) This study aims to explore the relationships between types of music, and physiologic and behavioral responses in hospitalized preterm infants.
MATERIALS OR METHODOLOGY: This study employs three different 15-minute original music segments composed in partnership with Bose Corporation following principles of music theory. Sample includes 20 preterm infants with postmenstrual ages between 30 weeks and 35 weeks, 6 days. Each patient undergoes 12 interventions in a random order (three exposures for each music condition and silence). Outcomes include continuous recordings of heart rate, respiratory rate, oxygen saturation, behavioral state organization, and regional cerebral oxygen saturation. A repeated measures ANOVA (Linear Mixed Model) is employed to analyze vital sign pattern after each music exposure (Condition 1, 2, 3) compared with silence (Condition 4).
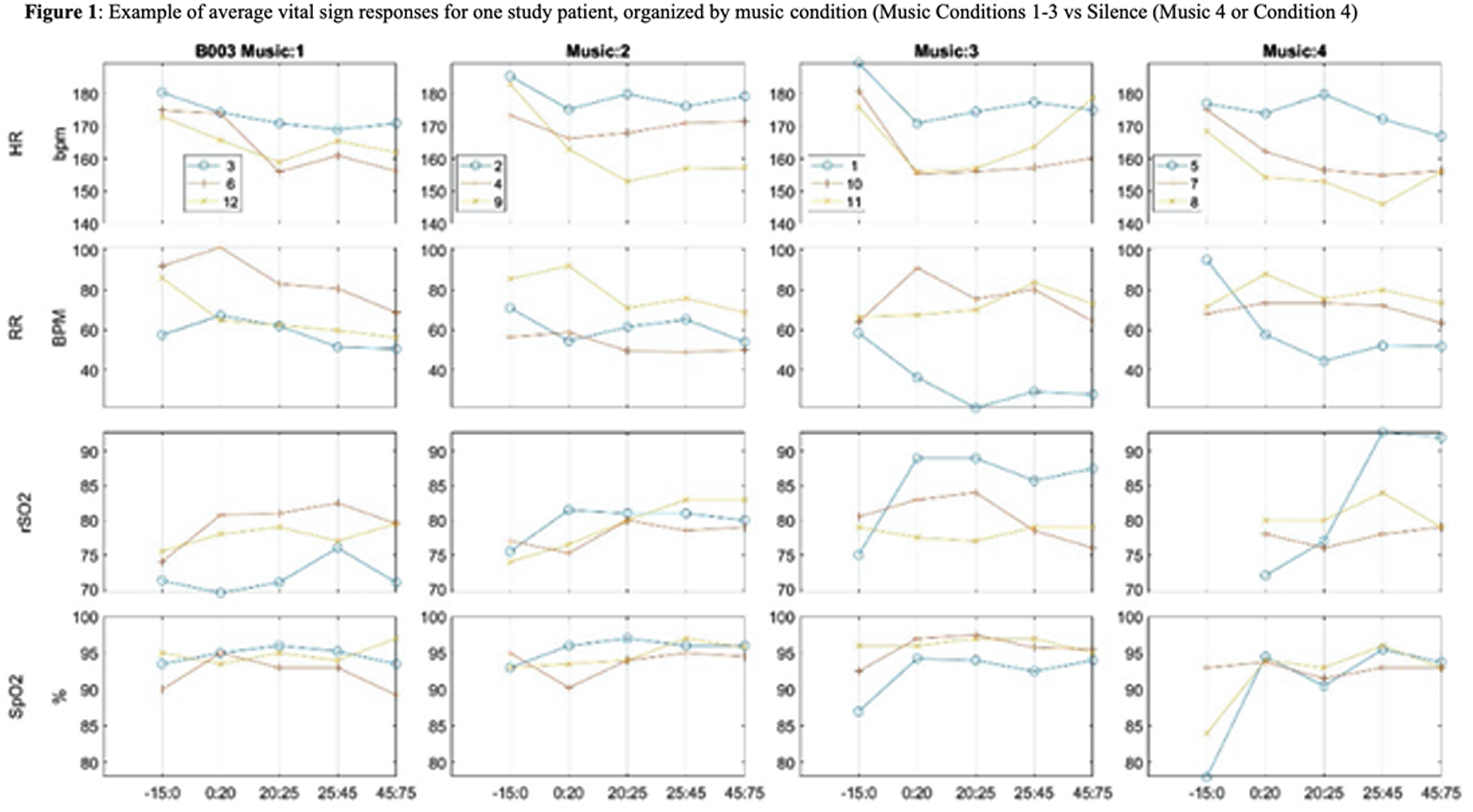
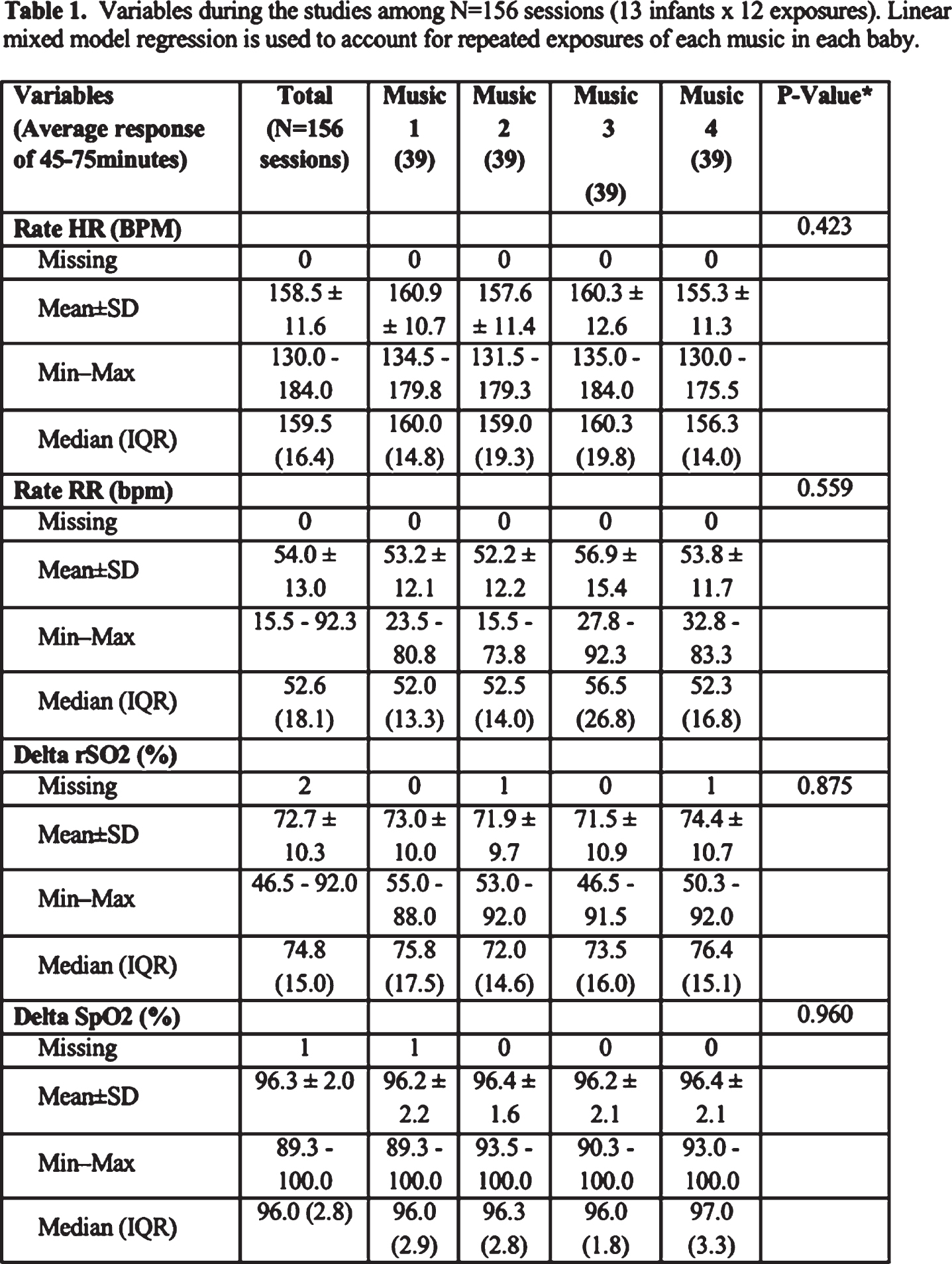
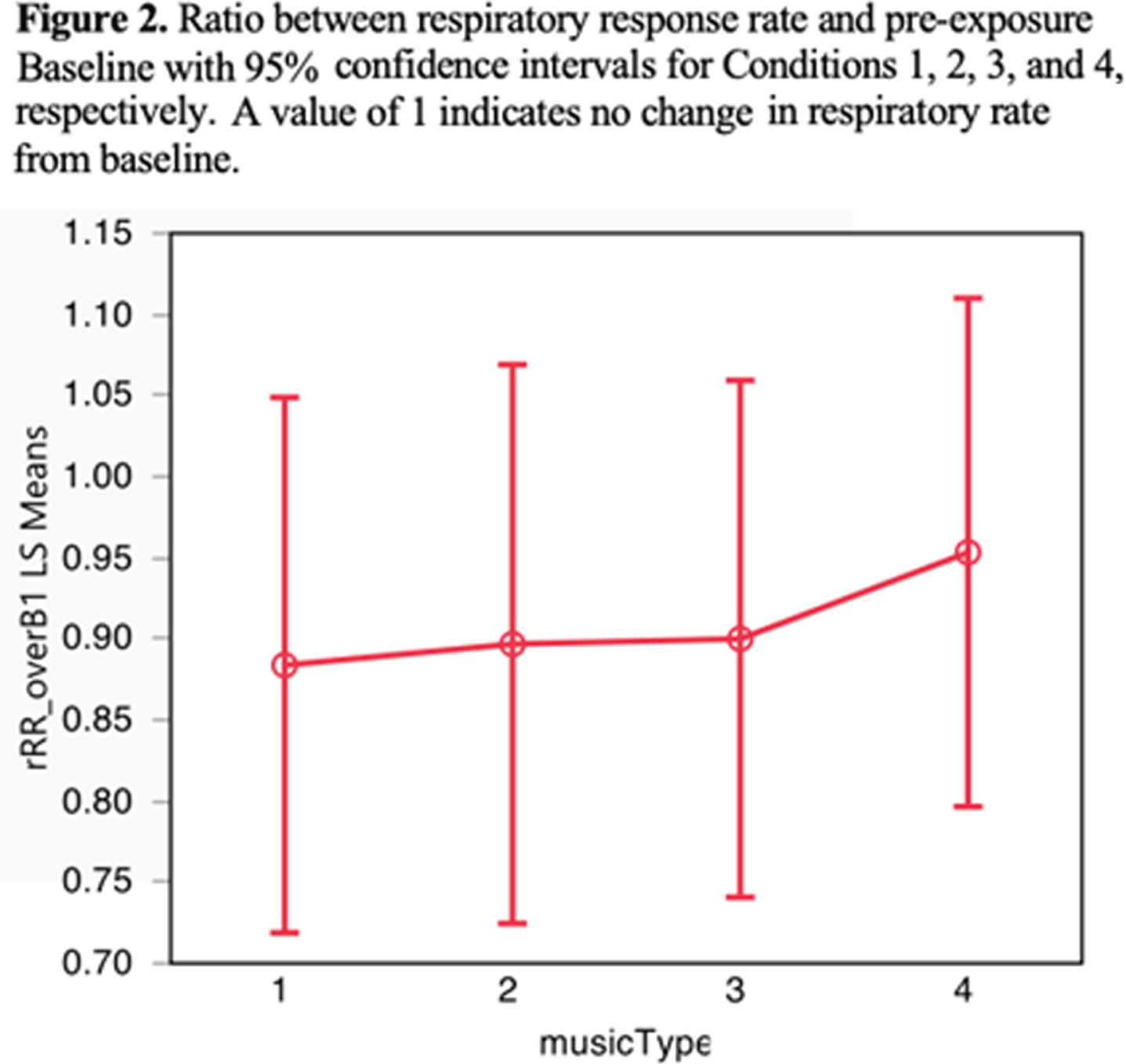
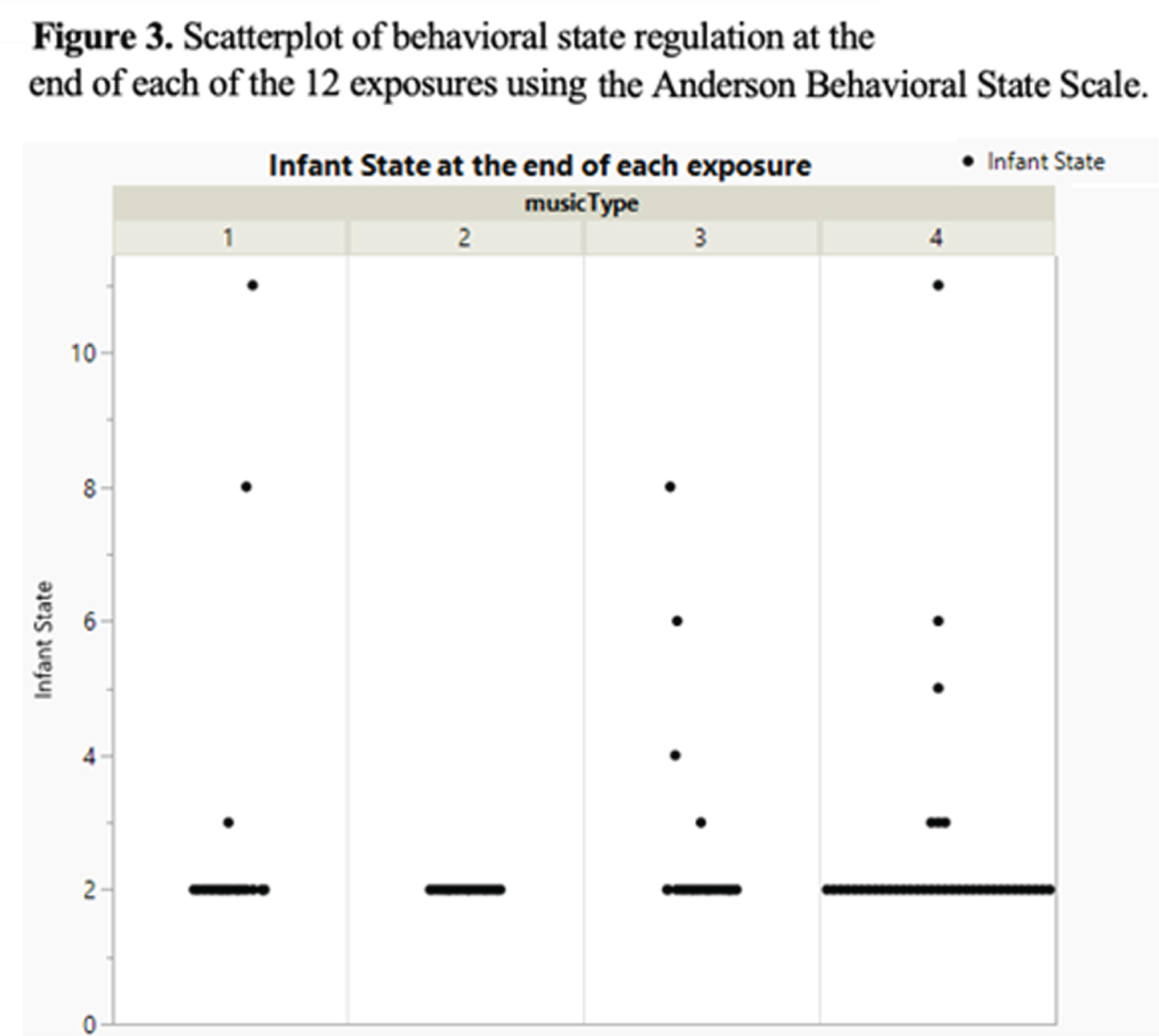
RESULTS: Enrollment is ongoing, with interim analyses using data collected from 13 patients presented here. An example of the average vital sign responses before, during, and up to 60 minutes after each intervention for one study patient is presented (Figure 1). No statistically significant changes were observed in vital sign patterns after each type of exposure (music or silence) when compared with baseline vital signs patterns pre-exposure (Table 1). We note that respiratory rates tend to decrease after each music condition (Condition 1, 2, or 3) when compared with silence (Figure 2), however differences are small and do not reach statistical significance. Further, when analyzing the respiratory rate pattern during and 5 minutes after each Condition, we observe a significant reduction with Condition 2 compared with silence (Tukey Post-Hoc p= 0.056). Infant behavioral state regulation ratings trend in the desired (lower) direction one hour after all Conditions (1, 2, 3, and 4), and remain most stable at the lowest (desired) rating after exposure to Condition 2 (Figure 3). This Condition consists of a low, repetitive, and rhythmically consistent entrainment stimulus. Further statistical analyses inclusive of modeling and multivariate regressions will be conducted on the complete sample to inform more conclusive results.
CONCLUSION: This study will provide insight into which specific music characteristics are most strongly associated with physiologic measures of stress.
Bibliography:
[1] Smith et al. Ann Neurol, 2011
[2] Cheong et al. J Neural Transm. 2020
[3] Mikulis et al. Acta Paediatr. 2021
[4] Filippa et. al. Pediatr Res. 2020
[5] Sa de Almeida J et al. Neuroimage. 2020
Long term outcome after hypothermia-treated hypoxic-ischaemic encephalopathy
Robertsson Grossmann Ka, Eriksson Westblad Ma, Blennow Ma, Lindström Ka
aDepartment of CLINTEC, Karolinska Institutet, Stockholm, Sweden
BACKGROUND: Therapeutic hypothermia has been shown to reduce the combined outcome of death or severe disability at 18-24 months in term/near-term infants with moderate-severe hypoxic-ischaemic encephalopathy (HIE). The risk of morbidity among survivors remains high. Studies from the pre-hypothermia era have reported high incidences of more subtle cognitive difficulties in survivors free of neuromotor impairment. To date, there are no reports on outcome in early adolescence after hypothermia-treated HIE.
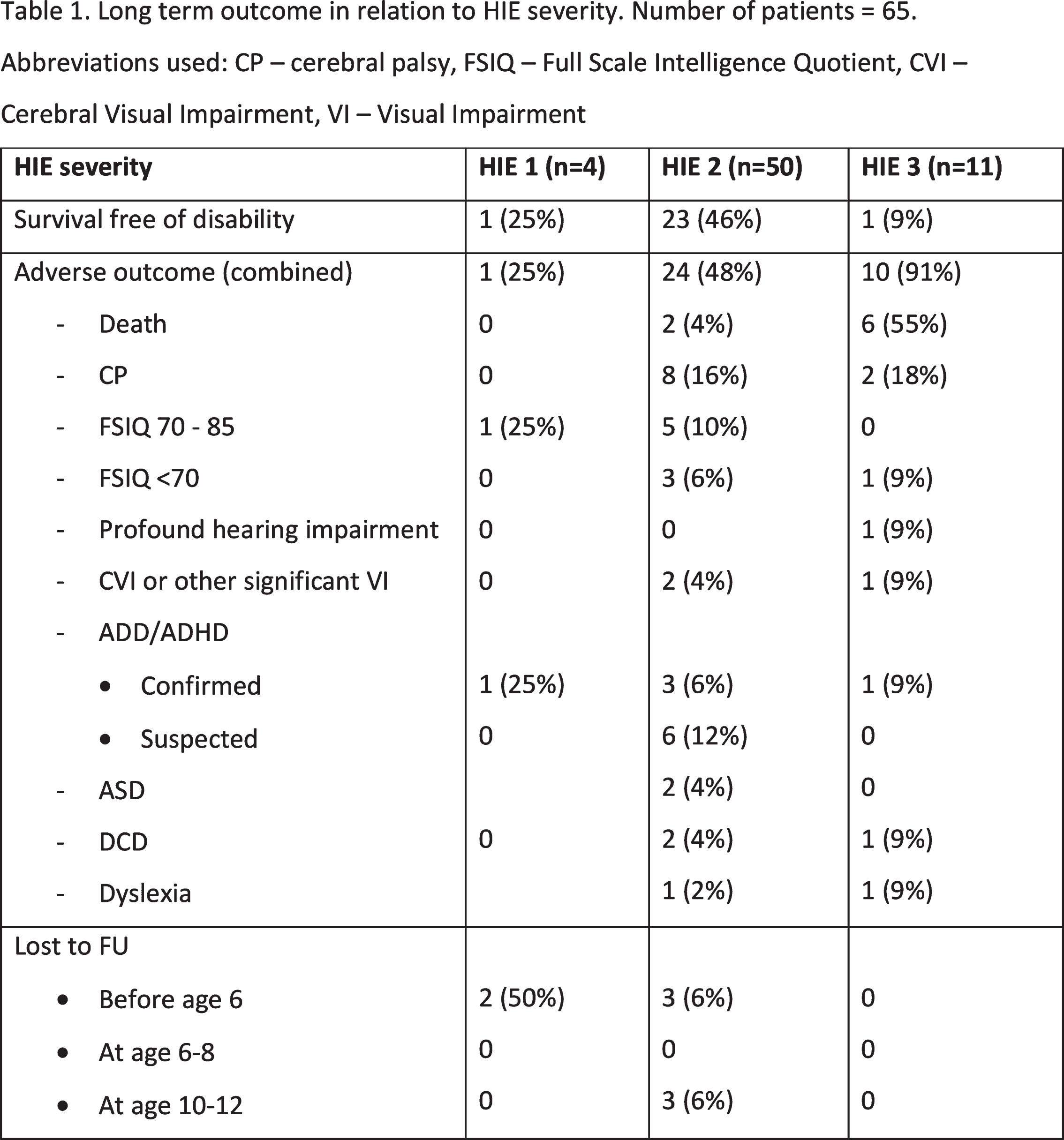
MATERIALS: This prospective, population-based study includes all infants born in the greater Stockholm region between January 1st 2007 and December 31st 2009 treated with hypothermia in addition to conventional neonatal intensive care due to HIE. All survivors still residing in Sweden were invited for a structured, comprehensive assessment at age 6-8 and 10-12. Motor and neurologic function was assessed with Movement Assessment Battery for Children 2 (M-ABC 2) and a standardized neurologic examination, respectively. Cognitive performance was assessed using the Wechsler Intelligence Scales for Children (WISC), 4th edition at age 6-8 and 5th edition at age 10-12. Parents were asked to fill out the Five-to-Fifteen (FTF) questionnaire to screen for developmental and behavioral disorders. Adverse outcome among survivors was defined as cerebral palsy (CP), epilepsy, full scale intelligence quotient (FSIQ) < 85, autism spectrum disorder (ASD), attention deficit disorder with/without hyperactivity (ADD/ADHD), developmental co-ordination disorder (DCD), severe visual or hearing impairment, or dyslexia.
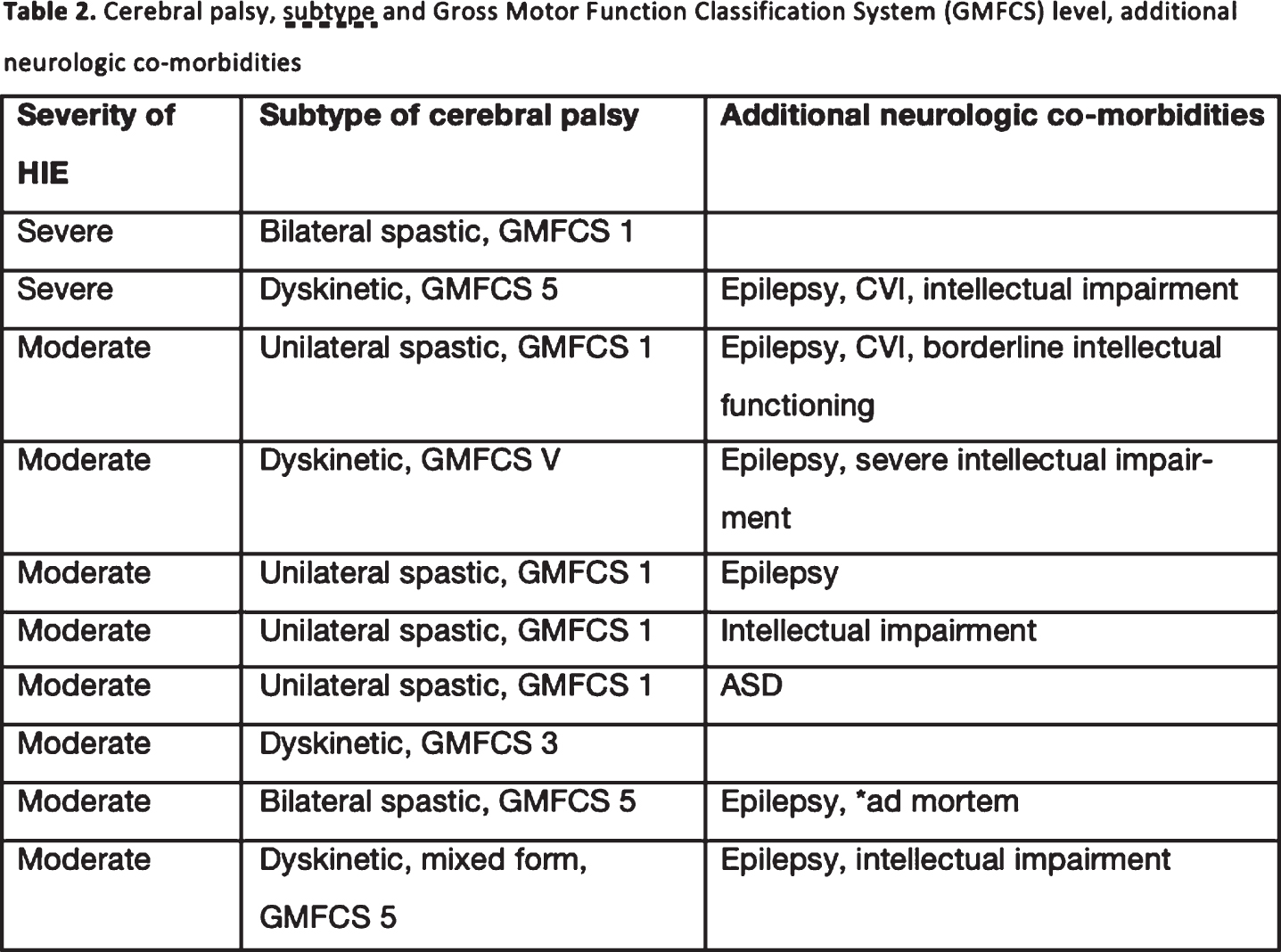
RESULTS: Sixty-six infants were treated with therapeutic hypothermia. One infant was later excluded due to a genetic syndrome. Mortality was 12%. Long term outcome is summarized in Table 1, severity and subtype of CP is outlined in Table 2. Mean FSIQ was normal among survivors without moderate-severe CP, with no difference between boys and girls (Figure 1). On both occasions, the incidence of a M-ABC 2 score indicating risk of motor difficulty was significantly higher compared to norms. Despite normal results at age 6-8, the incidence of a FTF score indicating obvious difficulties was significantly increased compared to norms at age 10-12 for the domains motor and executive function, perception, memory and language. Additional difficulties were detected at age 10-12 on thirteen occasions.
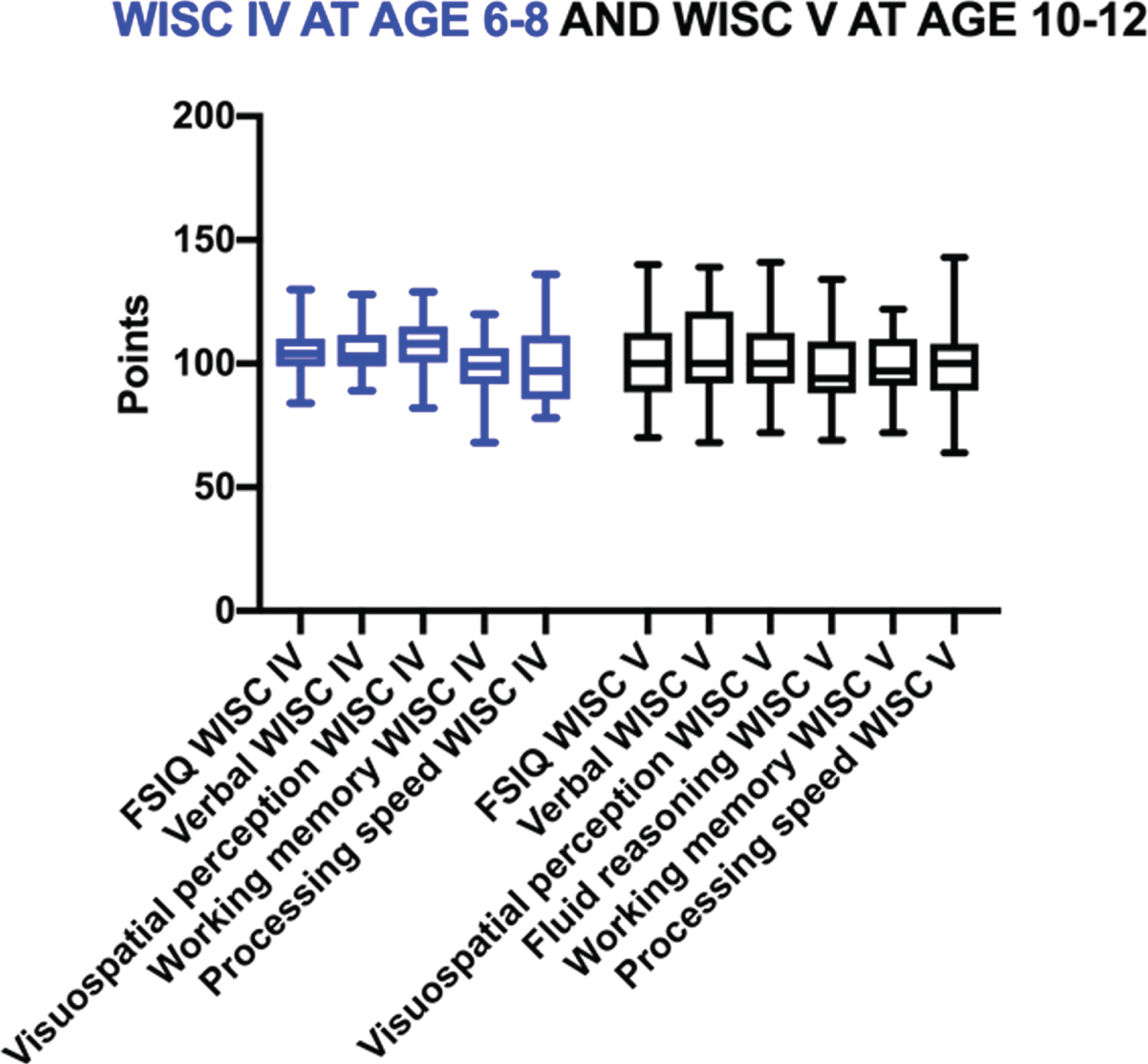
CONCLUSION: While mean FSIQ was normal among survivors free of major neuromotor impairment after hypothermia-treated HIE, the incidence of more subtle impairments increased upon renewed assessment in early adolescence, indicating the need for continued follow-up in this high-risk patient population.
Bibliography: Jacobs SE, et al. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Review, 2013
HIE grade, time to achieve target temperature, and brain MRI in infants with neonatal encephalopathy and therapeutic hypothermia. Do they correlate with developmental outcome at the age of two years? One-year data from a tertiary neonatal unit
Kumar Aa, Vatsavai Sb, Kapadia Jc, Vakharia Bd
aLuton & Dunstable University Hospital NHS Trust, Luton, United Kingdom
bLuton & Dunstable University Hospital NHS Trust, Luton, United Kingdom
cLuton & Dunstable University Hospital NHS Trust, Luton, United Kingdom
dLuton & Dunstable University Hospital NHS Trust, Luton, United Kingdom
Background: Hypoxic-ischemic encephalopathy (HIE) is a leading cause of long-term neurological sequel or death in full term babies. This study aims to correlate the initial neurological status and magnetic resonance imaging (MRI) in babies with HIE who underwent therapeutic hypothermia, with their neurodevelopmental outcome at two years.
METHODOLOGY: This is a retrospective cross sectional study at a tertiary neonatal unit. Data was collected on all infants with neonatal encephalopathy who underwent therapeutic hypothermia from June 2018 to June 2019. Developmental follow up was assessed at the age of 2 years using the Bayley Scales of Infant Development (BSID-III). If the 2-year clinic follow up was missing, information was obtained over the phone using a standard parental questionnaire. All infants had a brain MRI around day 7 of age, which was reported by a neonatal neuro-radiologist.
RESULTS: Complete information was available for 34 of the 37 eligible infants. Seven of the 34 infants were in-born; the rest were referrals from neighbouring hospitals within the East of England. Six infants had a diagnosis of severe HIE, 18 suffered from moderate HIE, and 10 had mild HIE. Time to achieve target temperature (33.5C to 34.5C) ranged from 1.5 to 11.5 hours; 27/34 infants achieved their target temperature within 6 hours of age (6/7 in the in-born group). There was no correlation between time to achieve target temperature and outcomes at 2 years age.
Two-thirds (23/34, 67%) of infants had normal development at the age of two years (BSID-III). Of these, 6 had abnormal MRI. Cerebral palsy developed in three infants of whom two had moderate HIE & one had severe HIE. They achieved target temperature between 3.5 and 7 hours. All three had significantly abnormal MRI findings.
Two infants showing early signs of possible autistic spectrum disorder had mild HIE with normal MRI. Two other infants who reported challenges with receptive and expressive speech also had mild HIE with normal MRI. Of the four infants who died in the neonatal period, 3 had severe HIE and the 4th had moderate HIE with an underlying genetic condition. Two had severely abnormal MRI, whereas the other two infants had re-direction of care and did not have an MRI.
CONCLUSION: In our study, there was no correlation between time taken to achieve target temperature (in the first 12 hours of birth) and outcome at 2 years. All infants with mild HIE had a normal developmental outcome. All three infants with cerebral palsy had either moderate or severe HIE. Significantly abnormal MRI correlated well with death or poor development and cerebral palsy. Six infants with an abnormal MRI had normal development at 2 years. Reassuringly, all the babies with normal MRI had a normal 2-year developmental outcome.


