
Inconsistent Music-Based Intervention Reporting in Dementia Studies: A Systematic Mapping Review
Abstract
Background:
Recent research has shown beneficial results for music-based interventions (MBIs) for persons living with Alzheimer’s disease and related dementias (AD/ADRD), but reports often lack sufficient detail about the MBI methodology, which reduces replicability. A detailed checklist for best practices in how to report MBIs was created in 2011 by Robb and colleagues to remedy the lack of detail in MBI descriptions. The implementation of the checklist specifically in AD/ADRD research has not been established. Given the complexity of music and the variety of uses for research and health, specific MBI descriptions are necessary for rigorous replication and validation of study results.
Objective:
This systematic mapping review utilized the “Checklist for Reporting Music-Based Interventions” to evaluate the current state of MBI descriptive specificity in AD/ADRD research.
Methods:
Research articles testing MBIs and reviews of MBI efficacy published between January 2015 and August 2023 were scored using the checklist and the results were summarized.
Results:
Forty-eight studies were screened, and reporting was inconsistent across the 11 checklist criteria. Ten out of 48 studies fully reported more than 5 of the 11 criteria. Only one of the 11 scoring criteria was at least partially reported across 47 of 48 studies.
Conclusions:
Thorough reporting of intervention detail for MBIs remains limited in AD/ADRD MBI research. This impedes study validation, replication, and slows the progress of research and potential application of music in practice. Greater implementation of the reporting guidelines provided by Robb and colleagues would move the field of MBI research for AD/ADRD forward more quickly and efficiently.
INTRODUCTION
Music-based interventions for health and wellbeing are receiving increased attention due in part to their lower cost, broader accessibility, and minimal side effects relative to pharmacological interventions. There is favorable evidence from recent research that music-based interventions (MBIs) are beneficial for people with Alzheimer’s disease and related dementias (AD/ADRD). One hypothesized reason for the effectiveness of MBIs is the observation that musical memory is retained and can still evoke a response throughout the progression of the disease, even in later stages when communication becomes more difficult.1–4 Multiple review papers have concluded that MBIs produce beneficial outcomes for people with AD/ADRD,2–15 while others have conceded that beneficial outcomes are probable although the direct evidence may be weak.16–18 Some benefits MBIs provide for people with AD/ADRD are reduced stress, reduced emotional disturbances and depression, and improved memory and cognitive function.1,2,4,6,8,10,13,14,16,18,19 These benefits may also extend to caregivers of people with AD/ADRD, who also often experience a decrease in quality of life as they care for their loved ones.8,10,20
The interest in the effectiveness of MBIs as a non-pharmacological treatment continues to grow, and evidence for their beneficial effects is favorable. However, specific features of the music need to be consistently identified and described to move music-based interventions from anecdotal evidence into the realm of prescriptive interventions. A wide variety of funding opportunities which allow for the incorporation of music-based interventions, including one specifically focused on funding MBI research, are available and will likely continue to fuel this increase in MBI research.21 However, the mechanisms which produce the beneficial effects of MBIs are not always clearly defined or understood. Understanding the underlying biological or psychological mechanism likely to be affected by the MBI gives a clearer understanding of which aspect of the intervention is producing the effect. This is also an area of interest for the NIH. Funding for dementia studies with a specific focus on the underlying mechanisms is also available, a fact which further supports both the level of importance placed on clearly defined mechanistic understanding and the necessity for more detailed and rigorous research.22
The importance of choosing specific music elements to focus on when designing and describing an intervention has been similarly highlighted by the NIH and others. Musical elements and the ways in which humans respond to these elements are both complex. This complexity requires clear descriptions of the hypothesized interactions when designing an intervention and clear reporting of the musical elements used and the methods which drive their selection. Clear description of these elements is necessary, not only to define the mechanism of the intervention and interpret results but also to aid in reproducing the effect in future studies. Establishing guidelines and frameworks for reporting is an essential part of achieving clear reporting, which has been recently provided by the NIH in the Music-Based Intervention Toolkit and in the Therapeutic Function of Music framework outlined by Dr. Deanna Hanson-Abromeit.23,24
Previously published reviews have focused on the results of music-based interventions for AD/ADRD, but few have considered the potential variability of the music interventions themselves resulting from the lack of detailed and specific descriptions. Differences and similarities between MBIs from one study to the next are difficult to determine because they are often only vaguely described. Without specific descriptions of the qualities of the music elements within music stimuli, the MBIs cannot be accurately reproduced, limiting the conclusions that can be drawn regarding efficacy. Unfortunately, reproducing individual study results in subsequent trials has proven difficult given the inconsistent levels of detail used to describe the music interventions across studies.
This gap was identified in 2011 by Dr. Sheri Robb and colleagues, who described the need for consistent and specific MBI reporting standards across inter-disciplinary research on music-therapy interventions.25 This team of music therapists and researchers created the “Checklist for Reporting Music-Based Interventions” to assist future researchers and improve transparency and rigor in music-based intervention research.25 In a 2018 follow-up review, Robb and colleagues examined the reporting specificity, based on their checklist, of MBI studies from 2010–2015 across a wide range of disciplines in healthcare. The result of their study was that consistent detailed reporting was not observed.26 To map the quality of reporting for MBIs specifically in AD/ADRD research since the previous review, we conducted an updated systematic mapping review of reporting rigor for MBI research studies in AD/ADRD from 2015–2023. For the purposes of this review, we searched for studies published since 2015 to identify studies published after the previous 2018 review by Robb and colleagues. Our aim was to discover whether reporting of MBIs for people with AD/ADRD had improved since the evaluation conducted up to 2015, and to describe any consistencies and inconsistencies that we observed in recent reporting.
METHODS
A systematic mapping review was conducted, searching PubMed, Cinahl, and Embase for papers published between January 1, 2015– August 22, 2023 related to music interventions and Alzheimer’s or dementia. The search terms used, inclusion, and exclusion criteria are in Table 1. The results of these searches were filtered, using the PubMed, Cinahl, and Embase search filters. The PubMed filters were to include only papers published between 2015–2023, with free full text in English available that were either meta-analysis, review, systematic review, or randomized controlled trials. The Cinahl filters were Boolean/Phrase, Apply equivalent subjects, Full Text, January 2015– August 2023, English Language and Randomized Controlled Trials. The Embase filters were Publication years 2015–2023 and Randomized Controlled Trial. For this review, our search was limited to papers in English as the checklist was published in English; however, evaluation of each paper included extraction of the country where the study was conducted. The resulting paper titles were screened for inclusion based on our inclusion and exclusion criteria (Table 1). Articles with titles referencing Alzheimer’s/dementia/cognitive decline and a music-based intervention were selected, and duplicate articles discovered across multiple searches were removed. The remaining articles were divided into review articles (meta-analysis, review, systematic review) and study articles (randomized controlled trial, prospective study). The review articles were then further screened based on full text review and level of relevance to MBIs for AD/ADRD. Review articles were excluded after full text review if they were not focused on AD/ADRD, if they did not include MBIs, or if AD/ADRD or MBIs were only briefly mentioned as part of a broader review. Those review articles with the highest level of relevance were retained. Review results were used to evaluate whether MBIs had beneficial outcomes, and what specific outcomes had been observed, because they synthesized a wide range of data that had already been reviewed for study quality. Each study article was further screened based on full text review and further study articles were then selected using the reference lists of the selected study articles. Screening was carried out by coauthor, BH.
Table 1
Search terms, inclusion, and exclusion criteria
| Search terms |
| “AD” OR “Alzheimer’s” AND “music” |
| “AD” AND “music” AND “intervention” |
| “Alzheimer’s” AND “music” AND “intervention” |
| “music” AND “dementia” |
| “music” AND “cognitive decline” |
| Inclusion Criteria |
| Articles published between January 1st, 2015 and August 22nd, 2023 |
| AD/ADRD focused |
| Uses music-based intervention |
| Randomized controlled trial, prospective study, meta-analysis, or review |
| Study was not included in the 2018 review by Robb and colleagues |
| Exclusion criteria |
| No music-based intervention |
| Not AD/ADRD focused |
| Study was previously included in 2018 review by Robb and colleagues |
The study articles were evaluated to determine the specificity of MBI descriptions and whether they met the standards of the “Checklist for Reporting Music-Based Interventions” (Supplementary Table 1). Each of the qualifying studies was scored based on the checklist which has 7 items. One of these items consists of 5 sub-categories which were treated as separate items for the purpose of this analysis for a total of 11 scored items. These scores were used to identify patterns of reporting across studies. Each checklist item could receive one of three possible scores, based on whether the item was found anywhere in the MBI description or within the article. The three scores were 0 (not observed/described), 0.5 (partially observed/described), or 1 (fully observed/described). A score of 0 was assigned if no description of a checklist item could be found within the full text of the report. A score of 0.5 was assigned if a description of a checklist item was found within the full text of the report, but all the item components were not described. A score of 1 was assigned if a description of a checklist item was found within the full text of the report and all item components were described. The scoring was carried out independently by two raters (Rater initials: BH and AZ). Interrater scoring disagreements were reviewed and reconciled by a third reviewer (RJL). The scoring was summed across checklist items and studies and visualized in Microsoft Excel to generate charts and observe qualitative patterns in the data. A PRISMA checklist for this systematic mapping review is provided in Supplementary Table 2.27
RESULTS
The PubMed, Cinahl, and Embase searches resulted in the selection of 113 articles which were divided between 65 studies and 48 reviews. After full text examination of the studies, 23 articles failed to meet inclusion criteria and were excluded as ineligible. The reference sections of the remaining 42 study articles were searched for additional relevant literature; 6 additional study articles were identified and included for a combined total of 48 studies. The 48 reviews were then further screened based on full text review and level of relevance to MBIs for AD/ADRD, those with insufficient relevance were removed which resulted in 19 total reviews. This screening was carried out by BH (Fig. 1, Table 2).
Fig. 1
Search results flowchart.
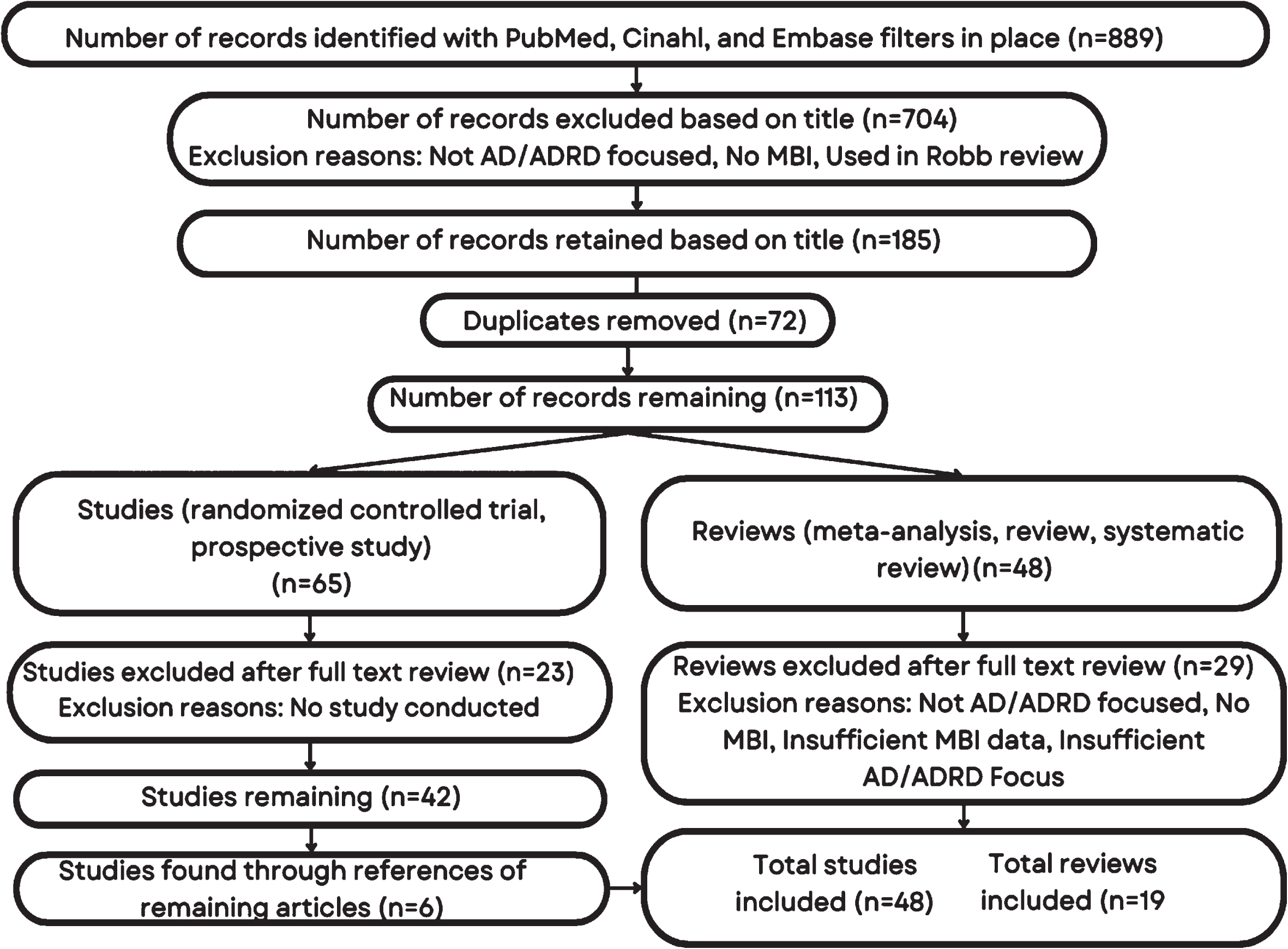
Table 2
Studies evaluated for reporting specificity (n = 48)
| Citation | Study type | Country | Intervention(s) | Participants | Description |
| 11 | Quasi-experimental cluster trial | Spain | Active music, receptive music | (n = 90) Nursing home residents with a diagnosis of probable Alzheimer’s disease or dementia | The clinical effects of two types of music intervention and a control activity were compared to determine which had the most beneficial effect on AD related symptoms including behaviour and cognition. |
| 35 | Exploratory randomized clinical trial | United States | Kirtan Kriya meditation, music listening | (n = 60) Independently living adults experiencing subjective cognitive decline | Two relaxation programs were compared to determine what effect they had on blood biomarker levels and how these levels were related to changes in cognitive function, psychosocial status, and quality of life. |
| 36 | Pilot randomized controlled trial | United States | Kirtan Kriya meditation, music listening | (n = 60) Independently living adults experiencing subjective cognitive decline | Two relaxation programs were compared to determine what effect they had on cognitive outcomes. |
| 37 | Pilot randomized controlled trial | United States | Kirtan Kriya meditation, music listening | (n = 60) Adults 50 years of age or older experiencing subjective cognitive decline | Two relaxation programs were compared to evaluate their effects on perceived stress, sleep, mood, and health-related quality of life. |
| 38 | Multicenter randomized clinical trial | France | Painting, singing | (n = 59) Adults 60 years of age or older with probable mild stage Alzheimer’s disease | A painting intervention was compared with a singing intervention to determine whether the singing intervention would have more immediate benefits on pain and wellbeing. |
| 39 | Randomized controlled trial | Korea | Recollection-based cognitive stimulus program | (n = 35) Dementia patients with mild stage Alzheimer’s disease. | Regular adult daycare activities were compared with recollection-based activities focusing on different stages of life to evaluate their effects on cognitive function, depression, and quality of life. |
| 40 | Cluster randomized controlled trial | United States | Chair yoga, music therapy, chair-based exercise | (n = 31) Community living adults 60 years of age or older diagnosed with dementia | Assessed feasibility of three nonpharmacological interventions for adults with dementia. The individual effects of the interventions on physical function, behavioral and psychological symptoms, and sleep were also compared. |
| 41 | Cluster randomized controlled trial | Australia | Group music therapy, recreational choir singing | (n = 318) Care home residents 65 years of age or older with dementia and depressive symptoms | Compared two active music interventions to identify their individual main effects and their interaction effects on depressive symptoms. |
| 42 | Cluster randomized controlled trial | United States | Personalized music listening | (n = 976) Long-stay nursing home residents with dementia | Utilized an established music intervention program across multiple nursing homes to determine whether it decreased agitated behavior and medication use. |
| 43 | Cluster randomized controlled trial | China | Music with movement | (n = 100) Persons with dementia 60 years of age or older and their primary family caregivers | Evaluated the clinical efficacy of the music with movement intervention to determine the effect on anxiety and depression levels in persons with dementia, as well as caregiver stress. |
| 44 | Cluster randomized controlled trial | United Kingdom | Active music therapy | (n = 17) Care home residents 40 years of age or older with dementia | Evaluated the feasibility of an individual active music therapy intervention and its effect on dementia symptoms and levels of wellbeing. |
| 45 | Randomized active-controlled trial | Singapore | Choral singing, health education | (n = 93) Community-living adults 60-84 years of age with probable cognitive impairment or dementia risk factors | Compared the effects of a choral singing group with a health education program to determine their effects on brain structure, cognitive outcomes, and blood biomarkers. |
| 46 | Pilot randomized controlled trial | Singapore | Music reminiscence activity, art therapy | (n = 68) Community-living adults 60-85 years of age who met the criteria for mild cognitive impairment | Compared the effects of two interventions, one using music and one using art, on neuropsychological outcomes, anxiety, depression, sleep quality, and telomere length. |
| 47 | Randomized controlled trial | Finland | Singing, music listening | (n = 89) Persons with dementia and their caregivers | Examined the effects of two different caregiver-implemented activities on neuropsychological outcomes. |
| 48 | Exploratory study | United States | Music therapy, singing, music-with-movement | (n = 62) Nursing home residents with moderate dementia | Evaluated the effect of a multi-component music intervention on depression symptoms and wellbeing, beginning with music therapist administered sessions and ending with trained CNA provided interventions. |
| 49 | Randomized controlled trial | Taiwan | Group percussion | (n = 50) Male veteran’s home residents 75 years of age or older who met the criteria for probable Alzheimer’s disease | Examined the effect of an active group percussion intervention on levels of anxiety and depression. |
| 50 | Randomized controlled trial | France | Singing, painting | (n = 65) Memory clinic patients 60 years of age or older with probable Alzheimer’s disease | Compared a singing intervention and a painting intervention to identify their effects on chronic pain, mood, quality of life, and cognition. |
| 51 | Prospective study | Spain | Music therapy | (n = 25) Patients 65 years of age or older with Alzheimer’s disease | Evaluated the effect of music therapy in reducing perceived stress and anxiety, as well as how cortisol levels are correlated to these emotional states. |
| 52 | Prospective randomized controlled trial | United States | Personalized music listening | (n = 59) Long-term nursing home residents with dementia | Evaluated the effect of an established music intervention program on dementia related agitation and behavioral disorders, as well as levels of medication usage. |
| 53 | Randomized controlled trial | Taiwan | Musical dual-task training | (n = 28) Adults diagnosed with mild-to-moderate dementia | Evaluated a music-based dual-task training for effects on multiple areas including attention control, balance, and agitation. |
| 54 | Randomized controlled trial | Tunisia | Music therapy, physical rehabilitation | (n = 28) Elderly patients, 65-80 years old, with mild Alzheimer’s disease | Studied music therapy and physical rehabilitation, individually and in combination, for effects on cognition and motor function. |
| 55 | Multi-center randomized controlled trial | China | Music-with-movement, music listening, social activities | (n = 165) Residents, 65 years of age or older, with moderate dementia | Compared three separate group interventions to evaluate their effects on agitation levels. |
| 56 | Multi-center randomized controlled trial | China | Music-with-movement, music listening, social activities | (n = 165) Residents, 65 years of age or older, with moderate dementia | Compared three separate group interventions to evaluate their effects on cognitive functions, depressive symptoms, and anxiety. |
| 57 | Randomized controlled trial | Italy | Music therapy | (n = 60) Residents, more than 80 years of age, with moderate-to-severe dementia and their caregivers | Evaluated the effects of music therapy on reducing behavioral and psychological symptoms of dementia and the corresponding reduction of caregiver burden. |
| 58 | Quasi-experimental study | China | Therapeutic folk recreation program | (n = 48) Long-term care residents, 60 years of age or older, with dementia | Examined the effects on cognitive function and daily living activities of a folk recreation program; which included art, music and games. |
| 59 | Randomized clinical trial | Brazil | Physical training with music, physical training without music | (n = 18) People, 60 years of age or older, with dementia | Examined the physiological effects of music listening before exercise on heart rate, blood pressure, and heart rate variability. |
| 60 | Prospective randomized controlled study | Italy | Cognitive training, active music therapy, neuroeducation | (n = 39) Patients with mild to moderate dementia and probable Alzheimer’s disease | Compared the individual effects of cognitive training, active music therapy, and neuroeducation on initiative, episodic memory, mood, and social relationships. |
| 61 | Randomized study | Italy | Active music therapy | (n = 45) Patients with probable Alzheimer’s disease | Evaluated whether combining active music therapy with a dose of memantine improved language and communication more than a dose of memantine alone. |
| 62 | Randomized pragmatic trial | United States | Music listening, audiobook listening | (n = 158) Residents in long-term care diagnosed with Alzheimer’s disease or dementia | Compared music listening with audiobook listening to evaluate their individual effects on agitation reduction. |
| 63 | Pilot randomized controlled trial | Brazil | Physical training with music, physical training without music | (n = 18) People, 60 years of age or older, with dementia | Used several established functional and cognitive tests to examine the effects of music listening before exercise. |
| 64 | Randomized controlled trial | Germany | Individualized music listening | (n = 90) Nursing home residents with dementia | Compared individualized music listening versus standard care to determine the reductive effect on behavioral and psychological symptoms of dementia. |
| 65 | Cluster randomized controlled trial | China | Music group with multi-sensory stimulation | (n = 73) Residents with moderate dementia | Evaluated the effectiveness of a group music intervention which included multi-sensory stimulation to manage behavioral and psychological symptoms of dementia. |
| 66 | Randomized controlled trial | United States | Kirtan Kriya meditation, music listening | (n = 60) Adults, 50 years of age or older, with subjective cognitive decline | Compared meditation versus music listening to determine the feasibility and acceptability of both interventions. |
| 67 | Pilot randomized controlled trial | United States | Kirtan Kriya meditation, music listening, enhanced usual care | (n = 40) Adults, 50 years of age or older, with subjective cognitive decline | Assessed the feasibility of an enhanced usual care comparator, while also comparing its effects versus meditation or music listening. |
| 68 | Randomized controlled trial | Australia | Personalized music listening | (n = 21) Patients with dementia | Assessed the feasibility of a personalized music listening intervention and evaluated its effectiveness in reducing agitation. |
| 69 | Randomized controlled trial | China | Singing group, lyric reading group | (n = 298) Patients with a diagnosis of probable Alzheimer’s disease | Compared group music therapy versus group lyric reading to determine their effects on cognitive function, neuropsychological symptoms, and activities of daily living. |
| 28 | Randomized longitudinal trial | Spain | Multisensory stimulation environment, individualized music listening | (n = 22) Patients, 65 years of age or greater, diagnosed with dementia | Compared a multisensory stimulation environment vs individualized music sessions to determine their effects on mood, behavior, and biomedical parameters. |
| 70 | Pilot randomized controlled trial | Norway | Physical activity, singing lessons | (n = 18) Patients, still living at home, with Alzheimer’s disease | Assessed the feasibility of both a singing intervention and a physical activity intervention and gathered neuropsychological and MRI data. |
| 71 | Randomized controlled trial | Spain | Active music stimulation | (n = 119) Nursing home residents, 65 years of age or older, with dementia | Evaluated the effectiveness of a group preferred music listening intervention on functional, cognitive, and emotional domains. |
| 72 | Randomized controlled trial | United States | Tailored music listening | (n = 33) Community-dwelling adults, 60 years of age or older, with dementia or self-reported memory impairment | Assessed the feasibility and acceptability of a home-based tailored music listening intervention and evaluated its effectiveness in reducing sleep disturbances. |
| 73 | Randomized controlled trial | Germany | Music-based exercise | (n = 69) Residents, older than 70 years of age, with mild to moderate dementia | Developed a music-based exercise program and evaluated its effects on cognitive function, motor function, and quality of life. |
| 29 | Randomized controlled trial | Spain | Multisensory stimulation environment, individualized music listening | (n = 22) Residents diagnosed with dementia and cognitive decline | Compared a multisensory stimulation environment vs individualized music sessions to determine their effects on agitation, emotional and cognitive status, and dementia severity. |
| 74 | Randomized controlled trial | Iran | Physical training, physical training with music | (n = 41) Patients, 50-75 years of age, with mild to moderate dementia | Evaluated a physical training program individually and in combination with music to determine the effects on cognitive, psychological, and physical functions. |
| 75 | Randomized pilot study | Germany | Music making with exercise, music listening with exercise | (n = 38) Residents with cognitive impairment | Compared two interventions, music making with exercise and music listening with exercise, to evaluate their effects on mood and cognitive functioning. |
| 76 | Randomized controlled trial | Turkey | Music therapy | (n = 75) Dementia patients and their caregivers | Examined the effects of music therapy in reducing caregiver burden and regulating the physiological parameters of dementia patients. |
| 77 | Pilot feasibility study | United States | Group music | (n = 19) Memory care community residents with diagnosed dementia | Assessed the feasibility and acceptability of a group music intervention and evaluated its effectiveness in reducing agitation. |
| 78 | Randomized controlled trial | China | Music listening/singing | (n = 60) Hospital patients with mild Alzheimer’s disease | Compared music therapy combined with drug treatment versus drug treatment alone to evaluate the effects on cognitive function and behavior. |
| 79 | Pilot randomized controlled trial | Germany | Individualized music listening | (n = 20) Nursing home residents diagnosed with dementia | Assessed the feasibility of an individualized music intervention and evaluated its effects on sleep quality, social participation, and agitation. |
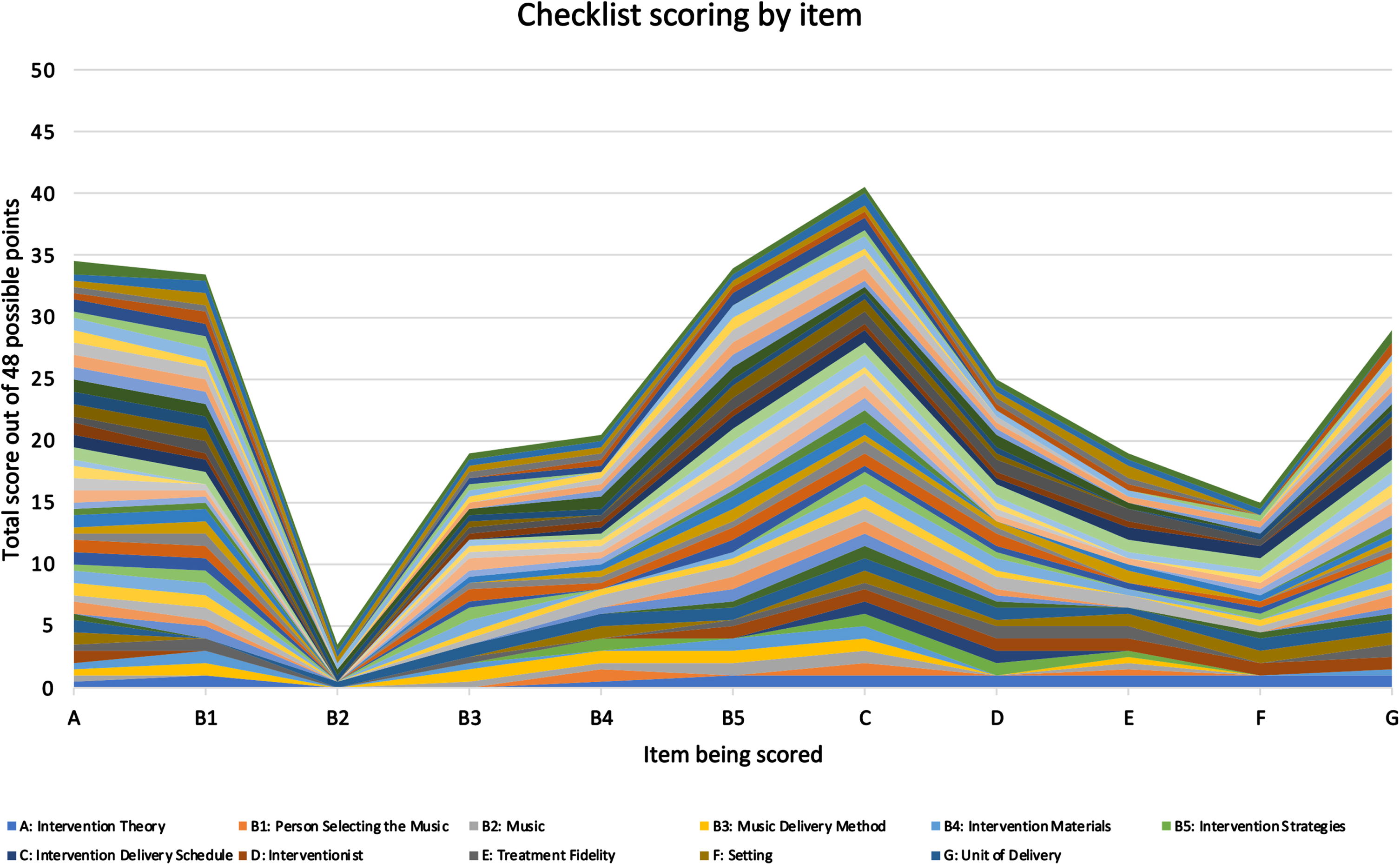
Analysis of the country where each study was conducted revealed that the included studies originated from North America, South America, Europe, Asia, and Australia. No studies were included that were conducted in Africa (Table 2). It should be noted that only one of the 48 studies included in this review cited the 2018 paper by Robb and colleagues which included the reporting checklist,26 and that study did not include the checklist as a table or supplementary material identifying where each item was located within their manuscript. Consequently, the studies cannot be reasonably expected to include the checklist items verbatim. However, the checklist still serves as a valuable reference for determining how specific the descriptions were. The checklist items are “A: Intervention Theory”, “B: Intervention Content” (contains five sub-categories), “C: Intervention Delivery Schedule”, “D: Interventionist”, “E: Treatment Fidelity”, “F: Setting”, and “G: Unit of Delivery.”25 The MBI descriptions in the study articles were limited, and full points were rarely awarded. Two studies received full points for eight items, three received full points for seven items, five received full points for six items, four received full points for five items, and the remaining 34 studies received full points for four or fewer items. Figure 2 displays the total score each study received, with each bar section color coded to show the point value contributed by each checklist item. Studies are not identified in the scoring as the goal of this analysis was to highlight the general pattern of reporting rather than to identify specific authors for lack of clarity in reporting as the checklist was not specifically used in any of the papers. The data supporting the findings of this study are available on request from the corresponding author (RJL). Full points and half points are indicated by the height of each column section. The maximum score each study could receive was 11. As seen in Fig. 2, only ten studies fully described more than five of the 11 items on the checklist, and when accounting for partial scoring, only 23 of the 48 studies achieved a score exceeding 5.5 out of 11. Figure 3 shows the total score for each checklist item across all studies, each section of the mountain plot is color coded to identify which study contributed the point value, full points and half points are indicated by the height of the section. The maximum score each checklist item could receive was 48 (the number of studies). As shown in Fig. 3, the most consistently described item was “C: Intervention Delivery Schedule”. Thirty-four studies fully reported item C, 13 partially reported item C, and only one study failed to report item C. The least reported item was “B.2: Music”, with only seven studies partially reporting this item. Despite achieving an upper range score, item “A: Intervention Theory” was also underreported, with only 25 studies fully reporting a theoretical rationale for how the MBI was hypothesized to effect change and 19 out of 48 studies partially reporting this item.
Fig. 2
Number of checklist items reported in each study. Whole or half points are represented for each checklist item by the color coding described in the legend.
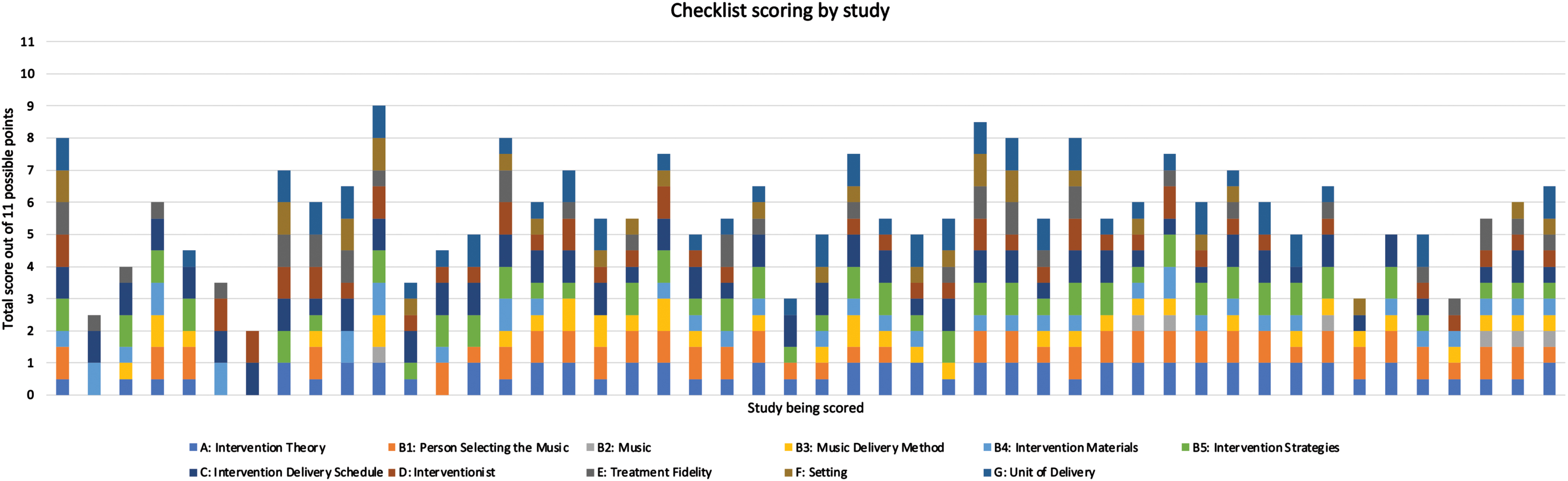
Fig. 3
Number of studies reporting each checklist item. Each study is represented by a unique color on the mountain plot. Checklist items are labelled in the legend according to the original checklist (Supplementary Table 1).
Frequency and duration of the interventions were some of the most consistently reported details. Because of this, it was possible to discern that the frequency and duration of MBIs for AD/ADRD varied widely between the studies. No other details could be accurately compared because of the inconsistent item reporting and lack of detailed intervention descriptions across the studies. Specific songs or music genre used in the MBI was rarely reported, and the environment in which the music was delivered was rarely described. Within the manuscript text, the location of the specific details of the music interventions also varied. Most often, specific descriptions were reported in the methods section. However, some details were only found in the introduction or discussion sections, or could only be inferred from the descriptions as they were not overtly stated. This added difficulty when identifying whether a checklist item had been fulfilled, because it required careful and repeated reads through the papers to locate each specific item. Beyond the difficulty of locating the information, the specific details included in the intervention descriptions varied so greatly that precise replication of a reported intervention would be nearly impossible.
DISCUSSION
There is favorable evidence that MBIs produce beneficial outcomes for those living with AD/ADRD and their caregivers. However, the lack of consistency in which details are reported combined with the lack of detailed descriptions of the specific components of these MBIs makes accurate reproduction of these interventions nearly impossible. Without the ability to accurately reproduce these interventions, validation of their results remains inconsistent. The specific music used in interventions was the most underreported checklist category, which is unfortunate because it is the foundation of a music-based intervention. Music is a diverse and general term, and even if a specific genre or song title is provided there is still variation in music components across performers and performances. These subtle musical variations could greatly influence the results of the intervention.25
One of the most underreported items across studies was “B.2: Music”. Most studies described intervention duration, frequency, and group size, but few offered more than a vague description of music type, and specific songs and artists were rarely included. Several studies narrowed music intervention into active or passive categories, but these categories give little insight into the nature of the music itself. Most studies did not describe delivery volume, tempo, location or any other specifically descriptive categories. Replicating an MBI when the only details which have been provided are duration and frequency of the intervention is bound to result in a host of differing musical components which will cause changes in the effects produced. Providing specific references and descriptions of the music used in an intervention would allow more replicability for independent validation of an MBIs results.
Another highly underreported item, “A: Intervention Theory”, is also a crucial component of any study. Without a clear theory underlying the music intervention design, the biological mechanism being targeted, and the expected results; it is difficult to determine whether the intervention was truly effective. Studies frequently reported large conceptual domains that could be affected by music, such as memory or cognition, but rarely described how music specifically was hypothesized to affect a specific change. Results may be observed, but understanding what intervention component is producing them and what biological mechanism is being utilized is challenging if the theory has not been clearly defined and utilized in intervention design. This further contributes to the difficulty in replication and validation.
Limitations of this review include records only in English and one reviewer (BH) for record screening. It is possible that some papers published in other languages were excluded. However, the analysis of the country where the study was conducted revealed that the search included publications from across the globe. Our review does not explicitly include sound stimulation like vibroacoustic therapy as all search terms and combinations included the word, “music,” and therefore does not capture the use of auditory stimulation not described by the authors as music. However, two studies did include multisensory stimulation as a comparison to the music condition.28,29 Rigor was increased by having two independent scorers (BH, AZ) and a third scorer (RJL) to review and reconcile any interrater disagreement in scoring.
Our mapping of the current literature provides evidence that reporting music-based interventions with enough detail to replicate and validate the fidelity of interventions remains limited, thus restricting progress in the development and efficacy of music-based interventions for AD/ADRD. One goal of intervention research is to influence effective clinical practice. Translation of research into clinical practice has historically been lengthy, taking an average of 17 years.30 Systematic reviews are one way to translate evidence-based research into clinical practice;31 however, transparent reporting is needed within primary research studies to effectively support translation of clinical research to practice. According to Google Scholar, there are over 300 citations of the Reporting Guidelines for Music-based Interventions. The original article, published in 2011 in the Journal of Health Psychology, was also reprinted that same year in Music and Medicine, an interdisciplinary journal of the International Association of Music and Medicine that is specific to music-based intervention research and clinical practice.32 The reporting guidelines for music-based interventions are easily accessible but have not been adopted as quickly as needed to align with trends in transparent reporting of health interventions, such as recommendations by the Equator Network.33 Use of the checklist is encouraged and cited by the recent NIH Music-Based Intervention Toolkit, and the implementation of those standards for researchers seeking NIH funding may increase adoption.23 Other opportunities to encourage use specifically for AD/ADRD research could include presentations at Alzheimer’s disease focused conferences, such as those highlighted on the Journal of Alzheimer’s Disease website.34 Journals could also encourage usage in their reporting standard guidelines for authors or by publishing editorial commentaries on the topic. Finally, cross-disciplinary collaborations are critical to align standards across music therapy, MBI research, and aging and AD/ADRD research.We urge researchers to include music therapists or other music-based intervention experts into the conceptualization and operationalization of music-based interventions to ensure the intervention details are evident within the intervention manual and protocol implementation and to align with recommendations to advance rigor, replication, and translation of music-based interventions.23,25
Replication and validation of results is a crucial component of scientific progress. A theory cannot be refined without repeated testing. A lack of clear and detailed descriptions of the theory behind an intervention design or the musical components of an intervention would be problematic if only one of these items was not reported. The lack of both of these items from a report makes replication and validation nearly impossible. The “Checklist for Reporting Music-Based Interventions” contains both of these items along with other important details and has been freely available since 2011. It was created with scientific rigor and for a specific purpose. Following this checklist will provide a framework to aid in consistent reproducibility of studies, and validation or invalidation of reported results. However, the checklist was only cited by one of the 48 studies we reviewed and was not included as a table or supplemental material by any studies. The checklist can be reproduced without permission in the same way that the PRISMA checklist is intended to be used, identifying the page numbers where each element can be found within a manuscript, and we recommend this practice to standardize reporting.27 If MBIs cannot be consistently validated their observed results will remain anecdotal in nature. To move MBIs from the realm of anecdotal evidence into the realm of prescriptive intervention, a consistent and ordered method of reporting is necessary. This method has already been provided, now is the time to put it to use.
AUTHOR CONTRIBUTIONS
Rebecca J. Lepping (Conceptualization; Formal analysis; Funding acquisition; Investigation; Methodology; Resources; Supervision; Validation; Writing – original draft; Writing – review & editing); Benjamin J. Hess (Data curation; Formal analysis; Investigation; Visualization; Writing – original draft; Writing – review & editing); Jasmine M. Taylor (Writing – review & editing); Deanna Hanson-Abromeit (Methodology; Writing – review & editing); Kristine N. Williams (Funding acquisition; Methodology; Writing – review & editing).
ACKNOWLEDGMENTS
The authors thank Ava Zatloukal (AZ) for assistance scoring the study articles.
FUNDING
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under the Award Number UL1TR002366. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
This review was not registered and a protocol was not prepared. The data supporting the findings of this study are available on request from the corresponding author.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-240255.
REFERENCES
1. | Groussard M , Chan TG , Coppalle R , et al. Preservation of musical memory throughout the progression of Alzheimer’s disease? Toward a reconciliation of theoretical, clinical, and neuroimaging evidence. J Alzheimers Dis (2019) ; 68: : 857–883. |
2. | Gomez-Romero M , Jimenez-Palomares M , Rodriguez-Mansilla J , et al. Benefits of music therapy on behaviour disorders in subjects diagnosed with dementia: a systematic review. Neurologia (2017) ; 32: : 253–263. |
3. | Soufineyestani M , Khan A and Sufineyestani M . Impacts of music intervention on dementia: a review using meta-narrative method and agenda for future research. Neurol Int (2021) ; 13: : 1–17. |
4. | Sarkamo T . Cognitive, emotional, and neural benefits of musical leisure activities in aging and neurological rehabilitation: A critical review. Ann Phys Rehabil Med (2018) ; 61: : 414–418. |
5. | Dorris JL , Neely S , Terhorst L , et al. Effects of music participation for mild cognitive impairment and dementia: A systematic review and meta-analysis. J Am Geriatr Soc (2021) ; 69: : 2659–2667. |
6. | Millan-Calenti JC , Lorenzo-Lopez L , Alonso-Bua B , et al. Optimal nonpharmacological management of agitation in Alzheimer’s disease: challenges and solutions. Clin Interv Aging (2016) ; 11: : 175–184. |
7. | Li K , Cui C , Zhang H , et al. Exploration of combined physical activity and music for patients with Alzheimer’s disease: A systematic review. Front Aging Neurosci (2022) ; 14: : 962475. |
8. | Garcia-Navarro EB , Buzon-Perez A and Cabillas-Romero M . Effect of music therapy as a non-pharmacological measure applied to Alzheimer’s disease patients: a systematic review. Nurs Rep (2022) ; 12: : 775–790. |
9. | Moreira SV , Justi F and Moreira M . Can musical intervention improve memory in Alzheimer’s patients? Evidence from a systematic review. Dement Neuropsychol (2018) ; 12: : 133–142. |
10. | Popa LC , Manea MC , Velcea D , et al. Impact of Alzheimer’s dementia on caregivers and quality improvement through art and music therapy. Healthcare (Basel) (2021) ; 9: : 698. |
11. | Gomez-Gallego M , Gomez-Gallego JC , Gallego-Mellado M , et al. Comparative efficacy of active group music intervention versus group music listening in Alzheimer’s disease. Int J Environ Res Public Health (2021) ; 18: : 8067. |
12. | Moreno-Morales C , Calero R , Moreno-Morales P , et al. Music therapy in the treatment of dementia: a systematic review and meta-analysis. Front Med (Lausanne) (2020) ; 7: : 160. |
13. | Lam HL , Li WTV , Laher I , et al. Effects of music therapy on patients with dementia-a systematic review. Geriatrics (Basel) (2020) ; 5: : 62. |
14. | Ito E , Nouchi R , Dinet J , et al. The effect of music-based intervention on general cognitive and executive functions, and episodic memory in people with mild cognitive impairment and dementia: a systematic review and meta-analysis of recent randomized controlled trials. Healthcare (Basel) (2022) ; 10: : 1462. |
15. | van der Steen JT , Smaling HJ , van der Wouden JC , et al. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst Rev (2018) ; 7: : CD003477. |
16. | Matziorinis AM and Koelsch S . The promise of music therapy for Alzheimer’s disease: A review. Ann N Y Acad Sci (2022) ; 1516: : 11–17. |
17. | Fang R , Ye S , Huangfu J , et al. Music therapy is a potential intervention for cognition of Alzheimer’s disease: a mini-review. Transl Neurodegener (2017) ; 6: : 2. |
18. | Bleibel M , El Cheikh A , Sadier NS , et al. The effect of music therapy on cognitive functions in patients with Alzheimer’s disease: a systematic review of randomized controlled trials. Alzheimers Res Ther (2023) ; 15: : 65. |
19. | Lai X , Wen H , Li Y , et al. The comparative efficacy of multiple interventions for mild cognitive impairment in Alzheimer’s disease: a Bayesian network meta-analysis. Front Aging Neurosci (2020) ; 12: : 121. |
20. | Lee S , Allison T , O’Neill D , et al. Integrative review of singing and music interventions for family carers of people living with dementia. Health Promot Int (2022) ; 37: : i49–i61. |
21. | National Institutes of Health. Notices of Funding Opportunities That Allow Music-Based Interventions, https://www.nccih.nih.gov/research/notices-of-funding-opportunities-that-allow-music-based-interventions (2024). |
22. | National Institutes of Health. Dementia Care and Caregiver Support Intervention Research (R01 Clinical Trial Required), https://grants.nih.gov/grants/guide/pa-files/PAR-21-307.html (2021). |
23. | Edwards E , St Hillaire-Clarke C , Frankowski DW , et al. NIH Music-Based Intervention Toolkit: music-based interventions for brain disorders of aging. Neurology (2023) ; 100: : 868–878. |
24. | Hanson-Abromeit D . A conceptual methodology to define the Therapeutic Function of Music. Music Ther Perspect (2015) ; 33: : 25–38. |
25. | Robb SL , Burns DS and Carpenter JS . Reporting guidelines for music-based interventions. J Health Psychol (2011) ; 16: : 342–352. |
26. | Robb SL , Hanson-Abromeit D , May L , et al. Reporting quality of music intervention research in healthcare: A systematic review. Complement Ther Med (2018) ; 38: : 24–41. |
27. | Page MJ , Moher D , Bossuyt PM , et al. PRISMA explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (2021) ; 372: : n160. |
28. | Maseda A , Cibeira N , Lorenzo-Lopez L , et al. Multisensory stimulation and individualized music sessions on older adults with severe dementia: effects on mood, behavior, and biomedical parameters. J Alzheimers Dis (2018) ; 63: : 1415–1425. |
29. | Sanchez A , Maseda A , Marante-Moar MP , et al. Comparing the effects of multisensory stimulation and individualized music sessions on elderly people with severe dementia: a randomized controlled trial. J Alzheimers Dis (2016) ; 52: : 303–315. |
30. | Rubin R . It takes an average of 17 years for evidence to change practice-the burgeoning field of implementation science seeks to speed things up. JAMA (2023) ; 329: : 1333–1336. |
31. | Tracy SL . From bench-top to chair-side: How scientific evidence is incorporated into clinical practice. Dent Mater (2014) ; 30: : 1–15. |
32. | Robb SL , Burns DS and Carpenter JS . Reporting guidelines for music-based interventions. Music Med (2011) ; 3: : 271–279. |
33. | Equator Network. Enhancing the QUAlity and Transparency Of health Research, https://www.equator-network.org/reporting-guidelines/ (2024). |
34. | Journal of Alzheimer’s Disease. Upcoming Meetings, https://www.j-alz.com/conferences (2024, accessed May 30 2024). |
35. | Innes KE , Selfe TK , Brundage K , et al. Effects of meditation and music-listening on blood biomarkers of cellular aging and Alzheimer’s disease in adults with subjective cognitive decline: an exploratory randomized clinical trial. J Alzheimers Dis (2018) ; 66: : 947–970. |
36. | Innes KE , Selfe TK , Khalsa DS , et al. Meditation and music improve memory and cognitive function in adults with subjective cognitive decline: a pilot randomized controlled trial. J Alzheimers Dis (2017) ; 56: : 899–916. |
37. | Innes KE , Selfe TK , Khalsa DS , et al. Effects of meditation versus music listening on perceived stress, mood, sleep, and quality of life in adults with early memory loss: a pilot randomized controlled trial. J Alzheimers Dis (2016) ; 52: : 1277–1298. |
38. | Pongan E , Delphin-Combe F , Krolak-Salmon P , et al. Immediate benefit of art on pain and well-being in community-dwelling patients with mild Alzheimer’s. Am J Alzheimers Dis Other Demen (2020) ; 35: : 1533317519859202. |
39. | Kim D . The effects of a recollection-based occupational therapy program of Alzheimer’s disease: a randomized controlled trial. Occup Ther Int (2020) ;6305727. |
40. | Park J , Tolea MI , Sherman D , et al. Feasibility of conducting nonpharmacological interventions to manage dementia symptoms in community-dwelling older adults: a cluster randomized controlled trial. Am J Alzheimers Dis Other Demen (2020) ; 35: : 1533317519872635. |
41. | Baker FA , Lee YC , Sousa TV , et al. Clinical effectiveness of music interventions for dementia and depression in elderly care (MIDDEL): Australian cohort of an international pragmatic cluster-randomised controlled trial. Lancet Healthy Longev (2022) ; 3: : e153–e165. |
42. | McCreedy EM , Sisti A , Gutman R , et al. Pragmatic trial of personalized music for agitation and antipsychotic use in nursing home residents with dementia. J Am Med Dir Assoc (2022) ; 23: : 1171–1177. |
43. | Cheung DSK , Ho LYW , Chan LCK , et al. A home-based dyadic music-with-movement intervention for people with dementia and caregivers: a hybrid type 2 cluster-randomized effectiveness-implementation design. Clin Interv Aging (2022) ; 17: : 1199–1216. |
44. | Hsu MH , Flowerdew R , Parker M , et al. Individual music therapy for managing neuropsychiatric symptoms for people with dementia and their carers: a cluster randomised controlled feasibility study. BMC Geriatr (2015) ; 15: : 84. |
45. | Feng L , Romero-Garcia R , Suckling J , et al. Effects of choral singing versus health education on cognitive decline and aging: a randomized controlled trial. Aging (Albany NY) (2020) ; 12: : 24798–24816. |
46. | Mahendran R , Gandhi M , Moorakonda RB , et al. Art therapy is associated with sustained improvement in cognitive function in the elderly with mild neurocognitive disorder: findings from a pilot randomized controlled trial for art therapy and music reminiscence activity versus usual care. Trials (2018) ; 19: : 615. |
47. | Sarkamo T , Laitinen S , Numminen A , et al. Clinical and demographic factors associated with the cognitive and emotional efficacy of regular musical activities in dementia. J Alzheimers Dis (2016) ; 49: : 767–781. |
48. | Ray KD and Gotell E . The use of music and music therapy in ameliorating depression symptoms and improving well-being in nursing home residents with dementia. Front Med (Lausanne) (2018) ; 5: : 287. |
49. | Liu MN , Liou YJ , Wang WC , et al. Group music intervention using percussion instruments to reduce anxiety among elderly male Veterans with Alzheimer disease. Med Sci Monit (2021) ; 27: : e928714. |
50. | Pongan E , Tillmann B , Leveque Y , et al. Can musical or painting interventions improve chronic pain, mood, quality of life, and cognition in patients with mild Alzheimer’s disease? Evidence from a randomized controlled trial. J Alzheimers Dis (2017) ; 60: : 663–677. |
51. | de la Rubia Orti JE , Garcia-Pardo MP , Iranzo CC , et al. Does music therapy improve anxiety and depression in Alzheimer’s patients? J Altern Complement Med (2018) ; 24: : 33–36. |
52. | Kwak J , Anderson K and O’Connell Valuch K . Findings from a prospective randomized controlled trial of an individualized music listening program for persons with dementia. J Appl Gerontol (2020) ; 39: : 567–575. |
53. | Chen YL and Pei YC . Musical dual-task training in patients with mild-to-moderate dementia: a randomized controlled trial. Neuropsychiatr Dis Treat (2018) ; 14: : 1381–1393. |
54. | Cheour S , Cheour C , Gendreau T , et al. Remediation of cognitive and motor functions in Tunisian elderly patients with mild Alzheimer’s disease: implications of music therapy and/or physical rehabilitation. Front Aging Neurosci (2023) ; 15: : 1216052. |
55. | Cheung DSK , Lai CKY , Wong FKY , et al. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate dementia? A randomized controlled trial. Dementia (London) (2020) ; 19: : 1413–1425. |
56. | Cheung DSK , Lai CKY , Wong FKY , et al. The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: a randomized controlled trial. Aging Ment Health (2018) ; 22: : 306–315. |
57. | D’Aniello GE , Cammisuli DM , Cattaneo A , et al. Effect of a music therapy intervention using Gerdner and colleagues’ protocol for caregivers and elderly patients with dementia: a single-blind randomized controlled study. J Pers Med (2021) ; 11: : 455. |
58. | Li DM and Li XX . The effect of folk recreation program in improving symptoms: a study of Chinese elder dementia patients. Int J Geriatr Psychiatry (2017) ; 32: : 901–908. |
59. | Izzo TF , Candanedo MJBL , Higuti AY , et al. Immediate physiological effects of listening to music before physical exercise in institutionalized older people with dementia. Fisoterapia Pesquisa (2021) ; 28: : 308–317. |
60. | Giovagnoli AR , Manfredi V , Parente A , et al. Cognitive training in Alzheimer’s disease: a controlled randomized study. Neurol Sci (2017) ; 38: : 1485–1493. |
61. | Giovagnoli AR , Manfredi V , Schifano L , et al. Combining drug and music therapy in patients with moderate Alzheimer’s disease: a randomized study. Neurol Sci (2018) ; 39: : 1021–1028. |
62. | Harrison TC , Blozis SA , Schmidt B , et al. Music compared with auditory books: a randomized controlled study among long-term care residents with Alzheimer’s disease or related dementia. J Am Med Dir Assoc (2021) ; 22: : 1415–1420. |
63. | Higuti AY , Barbosa SRM , Correa LM , et al. Effects of listening to music and practicing physical exercise on functional and cognitive aspects in institutionalized older adults with dementia: Pilot study. Explore (NY) (2021) ; 17: : 292–296. |
64. | Hillebrand MC , Weise L and Wilz G . Immediate effects of individualized music listening on behavioral and psychological symptoms of dementia: A randomized controlled trial. Int J Geriatr Psychiatry (2023) ; 38: : e5893. |
65. | Ho RT , Fong TC , Sing CY , et al. Managing behavioral and psychological symptoms in Chinese elderly with dementia via group-based music intervention: A cluster randomized controlled trial. Dementia (London) (2019) ; 18: : 2785–2798. |
66. | Innes KE , Selfe TK , Khalsa DS , et al. A randomized controlled trial of two simple mind-body programs, Kirtan Kriya meditation and music listening, for adults with subjective cognitive decline: Feasibility and acceptability. Complement Ther Med (2016) ; 26: : 98–107. |
67. | Innes KE , Montgomery C , Selfe TK , et al. Incorporating a usual care comparator into a study of meditation and music listening for older adults with subjective cognitive decline: a randomized feasibility trial. J Alzheimers Dis Rep (2021) ; 5: : 187–206. |
68. | Lee S , Chan L and Maddison J . Can a personalised music listening intervention decrease agitation in hospitalised patients with dementia? A feasibility trial. Front Psychiatry (2023) ; 14: : 1186043. |
69. | Lyu J , Zhang J , Mu H , et al. The effects of music therapy on cognition, psychiatric symptoms, and activities of daily living in patients with Alzheimer’s disease. J Alzheimers Dis (2018) ; 64: : 1347–1358. |
70. | Matziorinis AM , Flo BK , Skouras S , et al. A 12-month randomised pilot trial of the Alzheimer’s and music therapy study: a feasibility assessment of music therapy and physical activity in patients with mild-to-moderate Alzheimer’s disease. Pilot Feasibility Stud (2023) ; 9: : 61. |
71. | Perez-Ros P , Cubero-Plazas L , Mejias-Serrano T , et al. Preferred music listening intervention in nursing home residents with cognitive impairment: a randomized intervention study. J Alzheimers Dis (2019) ; 70: : 433–442. |
72. | Petrovsky DV , Bradt J , McPhillips MV , et al. Tailored music listening in persons with dementia: a feasibility randomized clinical trial. Am J Alzheimers Dis Other Demen (2023) ; 38: : 15333175231186728. |
73. | Prinz A , Schumacher A and Witte K . Changes in selected cognitive and motor skills as well as the quality of life after a 24-week multidimensional music-based exercise program in people with dementia. Am J Alzheimers Dis Other Demen (2023) ; 38: : 15333175231191022. |
74. | Shokri G , Mohammadian F , Noroozian M , et al. Effects of remote combine exercise-music training on physical and cognitive performance in patients with Alzheimer’s disease: a randomized controlled trial. Front Aging Neurosci (2023) ; 15: : 1283927. |
75. | Strong JV , Arnold M , Schneider L , et al. Enhanced short-term memory function in older adults with dementia following music-feedback physical training: a pilot study. Brain Sci (2022) ; 12: : 1260. |
76. | Gok Ugur H , Orak OS , Yaman Aktas Y , et al. [Effects of music therapy on the care burden of in-home caregivers and physiological parameters of their in-home dementia patients: a randomized controlled trial]. Complement Med Res (2019) ; 26: : 22–30. |
77. | Veal BM , Dobbs D , Lee S , et al. Feasibility and acceptability of a group music intervention in memory care communities. J Appl Gerontol (2022) ; 41: : 1528–1538. |
78. | Wang ZM , Li ZS , Xie JD , et al. Music therapy improves cognitive function and behavior in patients with moderate Alzheimer’s disease. Int J Clin Exp Med (2018) ; 11: : 4808–4814. |
79. | Weise L , Töpfer NF , Deux J , et al. Feasibility and effects of individualized recorded music for people with dementia: A pilot RCT study. Nord J Music Ther (2020) ; 29: : 39–56. |

