
Dementia Knowledge, Attitude toward Dementia, and Confidence in Dementia Care: Impact of a Dementia Training on German Nursing Students
Abstract
Background:
The number of people with dementia (PwD) in acute care hospitals is steadily increasing, posing a challenge for those who work closely with patients. To date, no German study has addressed the extent to which prospective nurses benefit from dementia training in terms of their knowledge, attitudes, and confidence in caring for PwD.
Objective:
The aim of this study is to investigate whether a validated dementia training for registered nurses can positively change nursing students’ knowledge about dementia, their attitude toward PwD, and their confidence in caring for them, as well as the stability over time.
Methods:
In the one-group pre-test, post-test design, a sample of 81 nursing students was recruited from two nursing schools in Germany between May and June 2023. They completed a questionnaire consisting of the Dementia Knowledge Assessment Scale, the Dementia Attitude Scale, and the Confidence in Dementia Scale, as well as sociodemographic questions and experiences with PwD at three measurement points. The data were analyzed using the Wilcoxon test and repeated measures ANOVA.
Results:
The training has a significant effect on knowledge in dementia (z = –5.07, p < 0.001), attitude toward PwD (z = –4.42, p < 0.001), and confidence in caring for them at the post-test (z = –3. 21, p < 0.001, r = 0.36). The repeated measures ANOVA shows stability over time only for dementia knowledge.
Conclusions:
The results indicate the need for further research in this field as well as the validation of the dementia training specifically addressing nursing students.
INTRODUCTION
Dementia is an increasingly important issue in our aging society. In addition to the loss of memory and changes in personality, dementia can also cause problems with speech and therefore with communication. This makes it difficult for people with dementia (PwD) to perform everyday tasks and to interact with others [1]. In the efficient delivery of quality care for people with dementia, nurses play a facilitating role [2]. In addition to all professionals who work closely with PwD in hospitals, nursing students face certain challenges in interaction with PwD during their practical phase. Previous research shows that nursing staff experience deficits in their knowledge, skills, and attitudes in relation to the specific care needs PwD [3]. Low confidence in caring for PwD and a lack of dementia-specific knowledge and of mental health disorders in general can negatively impact nurses’ job satisfaction [4]. This, in turn, can have a negative impact on the quality of life of these patients. However, dementia training can help improve nurses’ knowledge and skills in dealing with dementia [5, 6]. These results should also be proved regarding nursing students. Not only knowledge about dementia but also attitudes toward dementia and confidence in caring for PwD are of great importance. Therefore, it is necessary for nurses, including nursing students, to have basic knowledge about dementia, positive attitudes toward PwD, and a high level of confidence in caring for them.
Knowledge about dementia
Knowledge is an essential variable in making appropriate interactions and decisions. A U.S. study of nursing students revealed that those who had previous practice experience with people with Alzheimer’s disease (AD) also had greater knowledge about dementia and more positive attitudes toward people with AD compared to those without such experience [7]. Social learning theorists suggest that observing the behavior of role models influences social learning and the imitation of what is seen [8]. A qualitative interview study from Norway discovered that nursing students reported a lack of role models for person-centered care during their clinical placements, which negatively affected their learning [9]. Other studies have found that clinical placements and mentoring projects can lead to improved knowledge [10, 11]. In addition, direct contact with PwD has a positive effect on knowledge. Evidence suggests that prospective nurses benefit from prolonged participation in care programs and hands-on experience with PwD, as these variables correlate with higher dementia knowledge [12].
Attitudes toward PwD
Attitudes consist of affective, cognitive, and behavioral components [13]. Applied to the work of nursing students, several aspects are important in determining attitude toward PwD. For example, if a student feels uncomfortable with PwD or actively avoids interacting with them, it is considered a negative attitude. Nevertheless, previous research results from New Zealand and Malta demonstrated positive basic attitudes of prospective nurses toward PwD [11, 14]. In German-speaking countries, there is no research on the attitudes of prospective nurses and sustainable change through training.
Confidence in working with PwD
Self-confidence describes the positive or negative assessment of one’s own abilities to perform particular actions [15]. According to the German Duden dictionary, self-confidence, self-awareness, and self-assurance are used synonymously [16]. Bandura (1997) postulated the construct of self-efficacy, which is closely related to the definition of self-confidence. Here, self-efficacy expectancy is defined as the belief in one’s own competence to perform certain behaviors successfully, even in challenging situations [17]. According to the social cognitive learning theory, self-efficacy is a central direct and indirect variable influencing behavior. There are four sources of self-efficacy: successful performance, observation of behavioral models, symbolic experiences, and arousal [18]. Positive experiences of nursing students successfully interacting with PwD can increase their confidence. The same effect can be achieved by observing experienced nurses who serve as role models. Feedback and supportive guidance from colleagues and positive emotions while caring for PwD may also contribute to higher levels of confidence. Conversely, when nursing students are stressed or overwhelmed, their confidence in their own abilities may be compromised. For this reason, it is essential to provide support through dementia training to help them cope with physical and emotional stress and to enhance their sense of competence.
This paper examines whether prospective nurses in Germany can improve their knowledge about dementia as well as their attitudes toward dementia and increase their confidence in working with PwD after completing two modules of the dementia training “Getting to know me” using the German version “Lern von mir”. Furthermore, the stability of the results over time will be investigated.
Based on the previous findings, the following hypotheses are formulated:
1. Knowledge about dementia
a. Knowledge about dementia will be greater at post-test (T1) than at pre-test (T0).
b. The results at follow-up (T2) will be still stronger than at T0 and thus stable over time.
2. Confidence in caring for PwD
a. Confidence in caring for PwD is higher at T1 than at T0.
b. The results will be higher at T2 than at T0 and thus stable over time.
3. Attitude toward PwD
a. Attitudes toward PwD are more positive at T1 than at T0.
b. Results are still more positive at T2 than at T0 and thus stable over time.
MATERIALS AND METHODS
Design
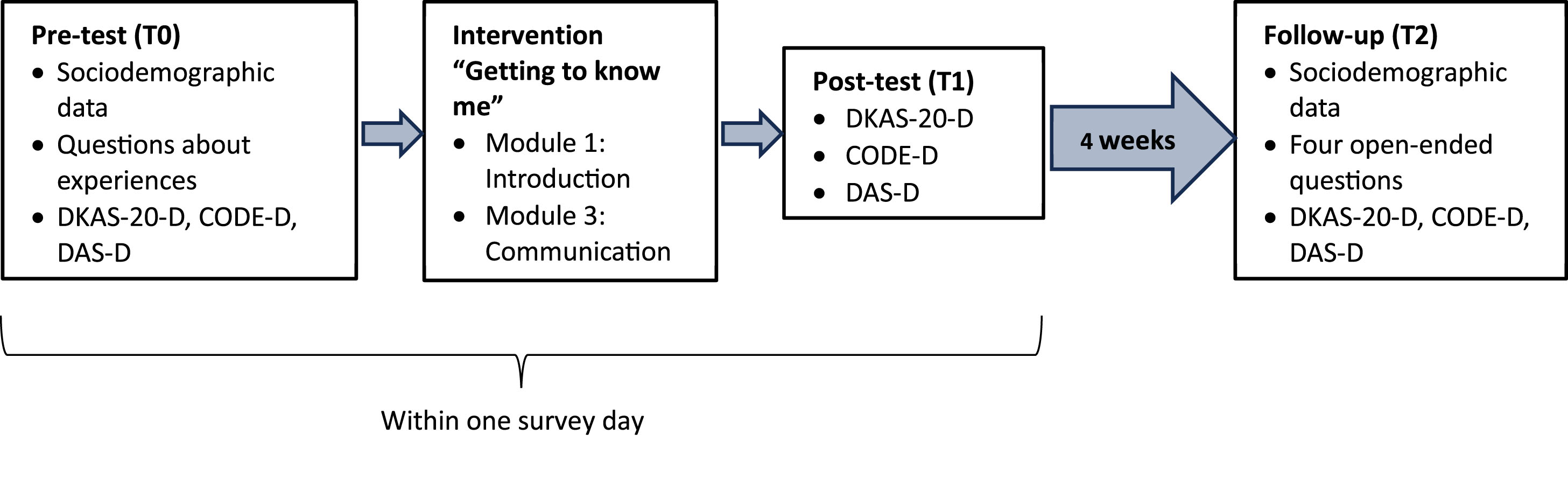
The study is a one-group pre-test, post-test design with a follow-up survey. The study design is schematically shown in Fig. 1.
Fig. 1
Study design.
Participants
The data collected is based on a sample of nursing students from two cities in Germany, who were recruited between May and June 2023. Eight nursing schools were contacted in advance, and two of them agreed to participate. In order to participate, students had to be at least 18 years old. Individuals under 18 years were allowed to participate in the training for moral reasons, but their data were not included in the analysis. This affected a total of four individuals and therefore did not systematically affect the results. In addition, the study included only nursing students, excluding geriatric nursing students.
Based on previous research, the distribution is expected to be nonparametric and to show large effects [19]. The sample size was determined using G*Power software (version 3.1.9.7), whereupon a sample size of N = 57 was targeted to detect an undirected effect with alpha = 0.05 and to expect a large effect using a Wilcoxon signed rank test. Based on previous research, we can assume that dementia training positively affects the surveyed scales. Therefore, the sample size for these directed hypotheses was n = 47 subjects. The final sample size at pre- and post-measurements was N = 81. Some individuals also participated in the four-week follow-up, forming a subgroup of n = 44.
Data collection and procedure
Data was collected by administering three paper-pencil questionnaires in which the participants provided sociodemographic data and completed three scales measuring knowledge about dementia (Dementia Knowledge Assessment Scale, DKAS-20-D; [20, 21]), confidence in caring for PwD (Confidence in Dementia Care, CODE-D; [19, 22]), and attitudes toward PwD (Dementia Attitude Scale, DAS-D; [22, 23]).
In addition, participants were asked whether they knew, cared for, or worked with PwD or were related to someone with dementia. Multiple responses were allowed. Respondents were also asked if and how often they had undergone dementia training. The questionnaires were administered once, both immediately before and after the dementia training (pre- and post-test; T0 and T1) and again after four weeks (follow-up test; T2). In addition to the three scales, four open-ended questions were asked at T2 (follow-up). The participants were asked to describe their satisfaction in dealing with PwD in their respective practice wards. Participants were also requested to report any changes they had observed in their own interactions with PwD following the training. Additionally, they were asked to indicate areas of care for PwD where they still felt uncertain or still encountered problems in their daily work with PwD. These questions were used for self-reflection as well as to stimulate further research in relation to prospective nurses. However, the open questions were not explored in detail.
A respondent code generated by the participants themselves allowed the data from the different timepoints to be combined for the analysis. After four weeks, the teacher responsible for the course distributed the follow-up questionnaire, and it was completed in class. One course did not use a paper-pencil questionnaire to collect the data at T2, but rather an online Google Form, as this course was in the practice phase at that time.
Instruments
Dementia Knowledge Assessment Scale (DKAS-20-D)
The DKAS assesses knowledge about dementia and includes 25 items that can be divided into the subscales Causes and Characteristics, Communication and Behaviors, Care Considerations, and Risks and Health Promotion, as proposed by Annear et al. (2017) [24]. The scale includes statements to be answered on a 4-point Likert scale with the response options true, probably true, probably false, or false. If individuals are unsure, they can also answer I don’t know. Statements are scored as follows: two points are awarded if the statement is true, and the person indicated true. If the person has indicated probably true instead, then he or she receives one point. All other options (probably false, false, I don’t know) are given a value of zero. Conversely, a false statement is worth two points, while a probably false statement is worth one point, and all other statements for this item are worth zero points. Consequently, the final score can range from 0 to 50 points. Higher scores indicate better knowledge of dementia. Items 1 to 4, 6, 7, 8, 11, 12, 17, and 19 are incorrect statements. The 20-item version (DKAS-20-D) is the shorter version validated in German, ranging from 0 to 40 points, which demonstrates a very good internal consistency with a Cronbach’s alpha of 0.87 [20].
Confidence in Dementia Scale (CODE-D)
The CODE scale was developed by Elvish et al. (2014) [5], and the German version was translated and validated by Teichmann et al. (2022) [22] in the general population. The nine items contain statements that are to be answered on a 5-point Likert scale with anchored ratings of not confident, somewhat confident, and very confident. Not confident is scored with one point. In ascending order, the answers up to very confident are scored with five points. It is, therefore, possible to achieve a score of between 9 and 45 points. A higher score indicates a greater self-confidence in caring for PwD. The scores 0–18 form the range of no confidence, 19–35 some confidence, and 36–45 strong confidence. The scale has reasonable appearance validity and a Cronbach’s alpha of 0.91, indicating an excellent internal consistency.
Dementia Attitude Scale (DAS-D)
The DAS-D contains a total of 20 items and is answered on a 7-point Likert scale. It measures the attitude toward PwD [23]. Response options are given in a range from 1 to 7 or from Strongly Disagree to Neutral to Strongly Agree. The items of the English version can be combined into the subscales Social Comfort and Dementia Knowledge and have a high internal consistency with Cronbach’s alpha = 0.83–0.85. The total score can range from 20 to 140, with higher scores indicating a more positive attitude toward PwD. Six items (2, 6, 8, 9, 16, 17) are reverse scored and need, therefore, to be recoded. The English version was also translated into German and validated with the general population [22]. It shows excellent internal reliability, with Cronbach’s alpha = 0.90.
Statistical analysis
The IBM SPSS Statistics version 27 program was used for descriptive and inferential statistical analysis of the data.
Reliability analysis
At baseline, Cronbach’s alpha was calculated for the three scales to check for internal validity in the sample of nursing students. As Terwee et al. (2007) stated, it is important to define a Cronbach alpha for each scale to prove whether it is an adequate measurement for the targeted variable in this population [25]. The quality of the scores can be classified as unacceptable (Cronbach’s alpha≤0.5), poor (Cronbach’s alpha > 0.5), questionable (Cronbach’s alpha > 0.6), acceptable (Cronbach’s alpha > 0.7), good (Cronbach’s alpha > 0.8), and excellent (Cronbach’s alpha > 0.9) [26].
Pre- and post-test differences
The three scales were tested for normal distribution using the Shapiro-Wilk test. The data showed a significant deviation from the normal distribution hypothesis (p < 0.05). Therefore, it should not be assumed that the data are normally distributed. Consequently, nonparametric tests were used. The Wilcoxon test was applied to the CODE-D, DKAT-20-D, and DAS-D data at pre- and post-measurement (T0, T1) to analyze significant differences immediately before and after the intervention. The alpha level was set at 0.025 (two-sided test). Statistical significance was assumed when p-values were less than or equal to 0.025. These values are based on the work of Elvish et al. (2014) [19]. Effect sizes for a Wilcoxon signed-rank test were calculated using the Pearson correlation coefficient |r| = z/√n and the determination coefficient R2 = z2/N [27]. We interpreted the values according to Cohen [28]. Correlation coefficients were classified as weak (|r| = 0.1), moderate (|r| = 0.3), and strong (|r| = 0.5). Effects can also be interpreted as weak (R2 = 0.02), moderate (R2 = 0.13), and strong (R2 = 0.26).
Temporal stability: ANOVA with repeated measures
A repeated measure ANOVA was performed to determine if the results differed within the measurement time points. In addition, it can be used to examine the stability of the results over time. This test for group differences was chosen because it is relatively robust to violations of the normal distribution assumption [29, 30]. According to the number of participants who completed the follow-up, n = 33 participants have been included for the DKAS-20-D, n = 41 for the CODE-D, and n = 34 for the DAS-D. A result of p < 0.05 indicates that at least two groups are significantly different. After a significant result, post-hoc tests are calculated to identify the groups in question. If sphericity is violated, a Greenhouse-Geisser correction is applied, and the results are interpreted using the appropriately corrected values.
The partial effect size η2 assesses the practical significance of a found effect and can be used to compare different studies. It is calculated by dividing the sum squares of the effect by adding the sum squares of the effect and the error [31]. For a better interpretability, the partial η2 (
The classification of the f values is based on Cohen’s classification [33], where f = 0.10 corresponds to a weak effect, f = 0.25 to a medium effect, and f = 0.40 to a strong effect.
Correlation
Correlations between data were calculated using Spearman rank correlation due to the lack of normal distribution [34]. This measures the strength and correlation between the ranks of variables related to each other and can be interpreted according to Cohen’s guidelines [28]. In the present work, we calculated correlations of gender, age of participants, individual levels of previous experience with PwD, and frequency of participation in dementia training with the scale scores of the DKAS-20-D, CODE-D, and DAS-D at the pre-test.
The intervention
The training took place in a single day and lasted for a total of 2.5 hours, which included a break and the processing of the questionnaires. Two modules (Module 1 Introduction and Module 3 Communication) of the German adapted version of “Getting to know me” [5] were conducted by the first author (HS) of this paper. Studies on the effectiveness of this training confirmed a significant increase in participants’ knowledge after the training. In addition, a significant increase in confidence in caring for PwD as well as in control beliefs was observed [5, 19]. However, validation of the program using appropriate scales is not yet available for German-speaking countries. The materials in German translation are available as freely available PDF documents on the homepage of the Diaconia University of Applied Sciences Bielefeld [35].
In the first module of the training, participants received a comprehensive introduction to the topic of dementia including mentalization exercises and facts about the prevalence and different forms of dementia. The third module was dedicated in detail to communication skills in the context of PwD in the hospital. It included information on non-verbal and verbal communication, as well as interactive elements such as videos of PwD and open discussions of possible solutions in difficult situations.
Missing data
During the data analysis, we discovered that the last item of the DKAS-20-D scale was not completed in the initial courses. Accordingly, this scale was adjusted by excluding item 20 from further analysis. Therefore, the maximum score for this scale is 38 instead of 40. Individual missing data in the CODE-D scale were replaced by the calculated scale mean. Single missing data in the DAS-D scale were excluded from further DAS-D-related calculations, as this affected only four individuals at the pre-test and nine individuals at the post-test.
Ethics
The study was performed according to the ethical standards outlined in the Declaration of Helsinki. Respondents participated voluntarily in the study after being informed about the aim of the study and subsequently provided their written consent for participation. The General Data Protection Regulation (GDPR) in a research context [36] was respected by ensuring the confidentiality and anonymity of the data.
RESULTS
Subject characteristics and sociodemographic data
A total of 83 subjects were recruited for the study. Individuals under the age of 18 were allowed to participate in the training but did not participate in the questionnaire survey and were not included in the descriptive and inferential statistical analyses. In total, N = 81 participants completed the pre-test and post-test during the initial survey. The key characteristics of the sample included in the analysis at each measurement time point are presented in Table 1.
Table 1
Participants’ characteristics of the total sample and the subgroups
| T0 &T1 | T2 | |||
| (N = 81)1 | (n = 44)2 | |||
| Characteristics | n | % | n | % |
| Age | ||||
| mean (SD) | 21.82 (4.199) | 21.93 (3.944) | ||
| Gender | ||||
| male | 24 | 29.6% | 14 | 31.8% |
| female | 55 | 67.9% | 30 | 68.2% |
| No answer | 2 | 2.5% | 0 | 0.0% |
| Education | ||||
| 9 years middle school | 2 | 2.5% | 0 | 0.0% |
| 10 years middle school | 38 | 46.9% | 19 | 43.2% |
| 12-13 years | 31 | 38.3% | 17 | 38.6% |
| Vocational training | 7 | 8.6% | 6 | 13.6% |
| Bachelor’s degree | 3 | 3.7% | 2 | 4.5% |
| Experiences with PWD | ||||
| I know/knew one or more PwD. | 50 | 61,7% | ||
| I care/cared for a PwD. | 27 | 33.3% | ||
| I work/worked with PwD. | 80 | 55.6% | ||
| In relation to a PwD. | 19 | 23.5% | ||
| Others | 4 | 4.9% | ||
| Participation in a program about dementia | ||||
| Yes | 16 | 19.8% | ||
| No | 63 | 77.8% | ||
| No answer | 2 | 2.5% | ||
| Frequency of participation in dementia course | ||||
| Once | 9 | 11.1% | ||
| 2–4 times | 7 | 8.6% | ||
| 5 and more times | 1 | 1.2% | ||
| Never | 63 | 77.8% | ||
| No answer | 1 | 1.2% | ||
1Sample directly before and after the intervention. 2Subgroup after four weeks for the follow up, here without measurements about Experiences with PWD, Participation in dementia course and Frequency of participation in dementia course.
Most participants were female (68%) and had an average age of 22 years. In addition, most subjects had a secondary school diploma as their highest educational attainment. At the time of the surveys, the participants were students in nursing, and most of them knew a PwD. Slightly more than half had worked with PwD before, but the vast majority had not yet participated in dementia training.
Reliability analysis
Cronbach’s alpha was calculated to examine the internal validity of the scales. Internal consistency was acceptable with Cronbach’s alpha = 0.74 for DKAS-20-D, 0.78 for CODE-D, and 0.78 for DAS-D.
Pre-test and post-test analyses
We used a Wilcoxon test to determine whether there were significant differences in knowledge, confidence in caring for PwD, and attitudes toward PwD before and after receiving dementia training. Descriptive statistics for this test are shown in Table 2.
Table 2
Descriptive statistics of Wilcoxon test
| N1 | Mean | SD | Minimum | Maximum | |
| DKAS-20-D pre-test | 72 | 20.13 | 5.879 | 8 | 31 |
| CODE-D pre-test | 78 | 35.60 | 4.148 | 18 | 43 |
| DAS-D pre-test | 77 | 111.51 | 10.862 | 89 | 136 |
| DKAS-20-D post-test | 78 | 24.10 | 5.605 | 10 | 36 |
| CODE-D post-test | 81 | 36.75 | 3.951 | 27 | 45 |
| DAS-D post-test | 72 | 115.63 | 11.789 | 86 | 139 |
1N corresponds to all adjusted data without missing values. The Wilcoxon test uses a listwise exclusion to account for missing data.
Immediately after the dementia training, the participants showed significant positive differences in knowledge about dementia with a strong effect (z = –5.07, p < 0.001, r = 0.61, R2 = 0.37). Additionally, there were significant positive differences in confidence in caring for people with dementia with a weak effect (z = –3. 21, p < 0.001, r = 0.36, R2 = 0.12) and significantly positive differences in attitude toward people with dementia with a moderate effect (z = –4.42, p < 0.001, r = 0.53, R2 = 0.15) compared to the pre-test.
Temporal stability
A repeated measures ANOVA was performed on all three scale scores. Table 3 demonstrates the summary descriptive scores for all three scales. The results of the repeated measures ANOVA are presented below.
Table 3
Descriptive statistics for all three measurement time points of the scale means
| DKAS-20-D | CODE-D | DAS-D | |||||||
| Characteristics | M | SD | N1 | M | SD | N1 | M | SD | N1 |
| Pre-test | 20.73 | 5.944 | 33 | 35.80 | 4.406 | 41 | 111.91 | 11.371 | 34 |
| Post-test | 25.00 | 5.984 | 33 | 37.15 | 4.041 | 41 | 116.21 | 12.249 | 34 |
| Follow-up | 24.55 | 6.870 | 33 | 35.32 | 5.208 | 41 | 111.03 | 17.027 | 34 |
1N corresponds to the number of individuals who participated at all three measurement time points and whose data were complete and could be linked.
DKAS-20-D
The repeated measures ANOVA indicated a statistically significant difference in knowledge about dementia between conditions, F(2, 64) = 8.73, p < 0.001, and partial η2 = 0.21. Conversion to Cohen’s f revealed a weak effect with f = 0.21.
Subsequent post-hoc tests (Dunn-Bonferroni tests) showed significant mean differences between pre- and post-test (MDiff = –4.27, 95% CI [–7.22, –1.33], p = 0.003) as well as between pre-test and follow-up (MDiff = –3.82, 95% CI [–6.71, –0.93], p = 0.006). These results indicate a significant increase in knowledge that remained stable over time.
CODE-D
Mean confidence in caring for PwD did not show a statistically significant difference between the three-time measurements as indicated by a repeated measures ANOVA with Greenhouse-Geisser correction, F(1.71, 68.58) = 43.18, p = 0.055, and partial η2 = 0.07.
DAS-D
After conducting a repeated measures ANOVA with Greenhouse-Geisser correction, it has been demonstrated that the mean scores of nursing students’ attitude toward PwD were statistically significantly different (F(1.40, 46.29) = 4.76, p = 0.023, partial η2 = 0.13). Conversion with Cohen’s f revealed a weak effect with f = 0.13.
Subsequent post-hoc tests (specifically, Dunn-Bonferroni tests) showed significant mean differences between the pre- and post-test (MDiff = –4.29, 95% -CI [–6.99, –1.60], p < 0.001), indicating an improvement in the DAS-D scores.
Correlations between previous experiences and targeted variables
Correlations were found between various variables. These are shown in Table 5. Knowledge about dementia at the pre-test correlated moderately positively with attending a dementia course (r = 0.379, p = 0.001). Specifically, the level of knowledge about dementia showed a weak positive correlation with never having attended a dementia course once (r = 0.25, p = 0.034) and moderately negatively correlated with having never attended a dementia course (r = –0.321, p = 0.006). In addition, the pre-test knowledge was weakly positively related to the statement “I work/have worked with people with dementia” (r = 0.289, p = 0.15).
Confidence in caring for PwD was also moderately positively correlated with the variable “I work/have worked with people with dementia” (r = 0.357, p = 0.001). There was also a positive correlation between confidence and previous participation in a dementia course (r = 0.303, p = 0.008). One-time participation was weakly positively related to confidence (r = 0.255, p = 0.025), while no previous participation was weakly negatively related to confidence (r = 0.276, p = 0.15). Additionally, the attitude toward PwD was moderately positively correlated with previous dementia course attendance (r = 0.3, p = 0.009), with one-time attendance being weakly positively related (r = 0.314, p = 0.006) and no previous attendance being moderately negatively related (r = –0.3, p = 0.009).
There were moderately significant positive correlations among the scale scores (rDKAS - 20,CODE - D = 0.42, p < 0.001; rDKAS - 20,DAS - D = 0.45, p < 0.001; rDAS - D,CODE - D = 0.52, p < 0.001).
DISCUSSION
Nursing students have rarely been the subject of research when it comes to working with PwD. The aim of this study was to investigate the extent to which nursing students benefit from dementia training and whether the results of training remain stable over time. Three scales assessing dementia knowledge (DKAS-20-D), confidence in caring for PwD (CODE-D), and attitude toward PwD (DAS-D) were used at three different measurement time points. Results indicated a significant effect of training on all three variables immediately after training, with only dementia knowledge remaining stable over time after four weeks. Thus, the first hypothesis was fully supported. Hypotheses two and three were confirmed only with respect to improvement at T1. There is no evidence for stability over time in improvements in attitudes toward PwD and confidence in caring for PwD. Furthermore, the correlation matrix revealed weak positive correlations between the scale values of dementia knowledge, self-confidence in caring for PwD and attitude toward PwD. Also, all three values are positively correlated with one-time participation in a dementia course. In addition, there are positive associations between previous work with PwD and dementia knowledge as well as confidence in caring for PwD.
Internal consistency
The results showed acceptable internal consistencies at baseline for all three scales. However, the German validation study in the general population showed good internal consistency with Cronbach’s alpha 0.83 –0.85 for the DAS-D [22], good internal consistency with Cronbach’s alpha of 0.87 for the DKAS-20-D [20], and excellent internal consistency with a Cronbach’s alpha of 0.91 for the CODE-D [22]. These differences between the original validation study and the present study may be due, among other things, to the fact that the scales in German were originally validated on the general population, whereas in the current study, they were transferred to the targeted group.
Similar results in internal consistency of the DKAS have been found in a Spanish-speaking study with nursing students, with a Cronbach’s alpha of 0.76 [37]. None of the other scales has been validated in nursing students, but the Greek version of DAS and CODE has been validated in psychology students, showing adequate results for DAS-GR, with alpha = 0.74 and good internal consistency for CODE-GR (alpha = 0.85) [38].
Spector et al. (2012) found in their systematic literature review of different measurement instruments for dementia knowledge that the internal consistencies of a scale differ depending on the population. Thereby, population comparisons within a scale mostly varied between acceptable and very good internal consistency [39]. This also seems to be relevant in the present work.
Training effect
Training had a significant positive effect, with a strong effect on knowledge of dementia, a weak positive effect on confidence in caring for PwD and moderate positive effect on attitudes toward PwD. These findings are consistent with previous research, which has consistently demonstrated rather strong positive effects of dementia training on confidence in dementia care [5, 38]. A systematic literature review by Surr et al. (2017) showed that 85% of 152 included studies reported an increase in knowledge following dementia training. The results of this study review also demonstrated that the majority of studies with attitudinal outcomes reported positive improvements in attitudes after dementia training, with 27% of included studies showing no significant changes [40]. This can be explained, among other variables, by using inadequate scales, such as the KIDE scale in the German population, which failed to detect any improvements in knowledge about dementia after a dementia training [41] and failed to do so when comparing pre- and post-tests [20].
The findings of improvements are consistent with Bandura’s social cognitive theory presented earlier in this paper [18]. Practical learning experiences, such as the discussions or mentalizing exercises may have contributed to increased understanding and skills in dealing with PwD, which in turn may have led to increased confidence in caring for PwD. In addition, the principle of empowerment may have been applied by providing the students with the knowledge and resources needed to successfully complete the tasks. This may subsequently stimulate the four cognitions of empowerment, namely feelings of competence, meaningfulness, influence, and self-determination, which in turn may have positive effects on job satisfaction and mental health [42].
Stronger effects in confidence could have been more realistic with a longer time period between the measures, allowing students to apply what they have learned. Unlike the DAS-D and the DKAS-20-D, which are more focused on knowledge, CODE-D places a greater emphasis on practical application.
Stability over time
A repeated measures ANOVA followed by post-hoc tests showed that knowledge of dementia improved significantly with training and remained stable over time. There are some studies reporting that dementia-specific courses or training have a positive effect on nursing students’ attitudes, knowledge, confidence, and empathy [43–45]. Therefore, the effects found in the present study can be considered consistent with previous literature.
For self-confidence in caring for PwD, the repeated-measures ANOVA showed no statistically significant difference. This could be because the attrition rate for this analysis was very low, reaching almost 50%, which may be attributed to missing data or no re-participation. There is a difference in the results of the post-hoc tests and the Wilcoxon test, where there was a statistically significant positive effect of training on confidence. Previous research has been less concerned with temporally stable effects of dementia training (follow-up designs) on confidence in caring for PwD, compared to the direct influence immediately after an intervention (pre- and post-designs) in nursing students or professionals. However, in agreement with the present results, significant improvements were shown after dementia training.
As with dementia knowledge, the training led to improved attitudes toward PwD. This result shows that the dementia training “Getting to know me” can help improve attitudes in the short term. In practice, this may subsequently reduce ageism in hospital settings, as attitudes and discrimination are closely linked [46]. However, in the present study, this improvement did not remain stable over time and showed only weak effects on dementia knowledge and attitude. Thus, the results are not consistent with previous findings on the effectiveness of dementia training for nurses. For example, Schneider et al. (2020) evaluated a two-day training that included communication and basic information about dementia and had positive and stable effects on dementia attitudes [41]. One explanation for the inconsistent findings is provided by cognitive dissonance theory, in which psychological dissonance is adjusted by changes in attitude. The training may have induced cognitive dissonance in the nursing students that should have been reduced by the change in attitude. In the weeks between the post-test and the follow-up, the urgency of the training that initially created the cognitive dissonance may have diminished, resulting in a corresponding adjustment in attitude. Since most of the participants from the follow-up survey did not have a practice assignment in the interim, the relevance of confronting one’s own attitudes and prejudices toward PwD may have been less relevant. Another explanation could be the lack of direct contact with PwD. According to a systematic literature review, personal contact of nursing students with PwD had a great effect on their attitudes and skills [45]. As nursing students move between practical placements and teaching blocks during their training, it is quite possible that the participants of the present study did not have enough contact with PwD. Only 56% of the test persons had already worked with PwD on the day of the training. Another argument is that only two of the six modules were used. The two modules may have been too short to make a lasting change in attitude.
Correlations between DAS-D, DKAS-20-D, and CODE-D
All three scales are positively correlated with each other at baseline. Previous research has shown that greater knowledge of dementia is associated with a more positive attitude [41, 47]. It can be assumed that the scales measure similar items in terms of content or are related as constructs. For example, knowledge about dementia is also related to confidence in dealing with PwD [48]. In addition, both low knowledge and confidence in caring for PwD contribute to negative attitudes toward these individuals, which consist of affect, behavior, and cognition components [49]. Further research should explore the relationship between these three variables in an empirical context in order to, among other things, optimize dementia training.
Contrary to what has been postulated in the literature, in our targeted group of nursing students, educational level is not positively correlated with knowledge about dementia [50]. In fact, it can be assumed that there is no correlation between the two variables. This may be due to the fact that nearly half of the nursing students had a secondary school diploma, and almost 40% had a high school diploma. Thus, there was no heterogeneity in ascending educational attainment, as only 9% had recognized vocational training, and 4% held a bachelor’s degree.
Limitations and strengths
The present study is not free of limitations. First, the sample, consisting of courses from two nursing schools in the Heidelberg district, cannot be considered representative of all German nursing schools. Variability between schools in terms of the content taught may lead to different results, as the topic of dementia may be treated with different intensity in different schools. Furthermore, no randomized control group was used, severely limiting the study’s validity. The low response rate to follow-up may also have introduced bias in the results of the repeated-measures ANOVA. Moreover, one course was in the practice phase at the time and could not be surveyed within the classroom.
Likewise, the course setting itself may have introduced bias. For example, the test persons sat next to each other in rows. This could have increased the pressure of social desirability since the people sitting next to each other had the opportunity to look at each other’s questionnaires. These environmental factors could also have led to a loss of attention or motivation since there was restlessness and cloister-like characteristics of the situation. The length of the questionnaire with three scales may also have increased these effects.
Another difficulty was the selection of the paper-pencil questionnaire. In the first two courses, for example, students systematically forgot to fill in the last question of the first scale (DKAS-20-D). As a result, the questionnaire had to be completely redesigned for the further courses, and item 20 was excluded from the analysis. Therefore, to prevent missing values, it would be beneficial for future studies to use an online questionnaire with appropriate functions or conduct individual interviews in which no questions are omitted.
For the interpretation of the results, it is worth mentioning that the scales have only been validated in relation to the overall population in German-speaking countries and not specifically in relation to the target group of nursing students. In addition, although the training has been validated and replicated in the original, there is no study in the German-speaking countries that addresses validation in relation to German nurse practitioners, let alone nursing students. Further studies should address the validation of the training and scales in German-speaking countries and in relation to nursing students. Accompanying qualitative interviews can provide profitable details on nursing students’ wishes and ideas regarding training needs and knowledge gaps that cannot be measured by quantitative questionnaires. According to the study by Schneider et al. (2020), nursing staff desires experienced individuals from the health care sector as trainers for dementia training [51]. This suggests that nursing students may have more negative attitudes toward the training and less motivation to actively participate due to less practical experience of the trainer and the small age gap. Therefore, for more practical guidance and advice, it would therefore be useful to conduct this training with registered nurses as trainers who have sufficient experience with PwD.
As we have already reported in the discussion, a further limitation of the study is the use of only two of the six modules. The two modules may have been too short to achieve a lasting change in attitude.
Another limiting aspect is the lack of native language recording. Persons whose native language is not German may have had difficulty understanding the questionnaire. However, it would have been unrepresentative of this occupational group to exclude them from the analysis, as the percentage of foreigners in the German nursing workforce is not negligible at 13% [52]. In addition, nursing students usually must prove that they already have sufficient German language skills when applying. Nonetheless, an additional assessment tool would be desirable to take this into account appropriately. Possibly, individual interviews with standardized German explanations could be helpful.
Nonetheless, some strengths of this study should be noted as well. Both the questionnaires and the training program are freely available and facilitate the replicability of the study. The sample used for the study is appropriately large for pre-post-test measurement and allows for meaningful results. The questionnaires were completed independently of the investigator and are objective in that regard. The emphasis on the anonymity of responses may also have resulted in honest responses, especially on sensitive questions such as attitudes toward PwD (DAS-D). Another positive aspect of this study is the long-term observation of the students over a period of four weeks, including pre-measurement, post-measurement, and follow-up. Although an even longer period would have been desirable, this was not feasible in the context of a final thesis and could, however, be taken up for future research. Nevertheless, the sustainability of the training and temporal effects could be observed over a more extended period of time, thus contributing to the strengthening of the results.
Implications and conclusion
It would be valuable for future research to validate the scales used in relation to the target group of students. In addition, a scientific review of the “Getting to know me” (Lern von mir) training should be conducted in German-speaking countries to validate and, if necessary, adapt it. In general, more interdisciplinary research groups should address the development of appropriate dementia training for the hospital setting, as this would be of immense added value for both hospital staff and PwD. Since the training materials and questionnaires are freely available, future research could replicate this work and seek methodological improvements, e.g., including a randomized control group, to strengthen the validity.
The present work makes an important contribution to research on the attitudes, knowledge, and self-confidence of nursing students toward dementia. Based on the results of this study, further steps can be taken to research optimal working and learning conditions for nursing students, which at the same time can have an influence on the stress reduction and job satisfaction of the future nurses and on the quality of life of PwD in acute care hospitals.
AUTHOR CONTRIBUTIONS
Henriette Seltmann (Conceptualization; Data curation; Formal analysis; Methodology; Project administration; Validation; Writing – original draft); Birgit Teichmann (Conceptualization; Formal analysis; Methodology; Supervision; Validation; Writing – Review & Editing).
ACKNOWLEDGMENTS
This study is independent research. The views expressed in this publication are those of the authors. We want to thank all the cooperating nursing schools as well as Taisiya Baysalova for the English correction.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
B.T. is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
H.S. has no conflict of interest to report.
DATA AVAILABILITY
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-231338.
REFERENCES
[1] | Förstl H , Lang C (2011) Was ist “Demenz”? In Demenzen in Theorie und Praxis, Förstl H, ed. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 3-9. |
[2] | Yaghmour SM ((2022) ) Impact of settings and culture on nurses’ knowledge of and attitudes and perceptions towards people with dementia: An integrative literature review. Nurs Open 9: , 66–93. |
[3] | Keuning-Plantinga A , Roodbol PF , Krijnen WP , Finnema EJ ((2022) ) Nurses’ perceptions in caring for people with dementia in Dutch acute hospitals. . J Clin Nurs 31: , 1800–1816. |
[4] | Digby R , Lee S , Williams A ((2017) ) The experience of people with dementia and nurses in hospital: An integrative review. . J Clin Nurs 26: , 1152–1171. |
[5] | Elvish R , Burrow S , Cawley R , Harney K , Graham P , Pilling M ((2014) ) ‘Getting to Know Me’: The development and evaluation of a training programme for enhancing skills in the care of people with dementia in general hospital settings. . Aging Ment Health 18: , 481–488. |
[6] | Gehr TJ , Sieber CC , Freiberger E , Engel SA ((2021) ) “EduKation demenz® Nursing” in the acute hospital setting. . Z Gerontol Geriatr 54: , 659–666. |
[7] | Kimzey M , Mastel-Smith B , Alfred D ((2016) ) The impact of educational experiences on nursing students’ knowledge and attitudes toward people with Alzheimer’s disease: A mixed method study. . Nurse Educ Today 46: , 57–63. |
[8] | Bandura A , Ross D , Ross SA ((1961) ) Transmission of aggression through imitation of aggressive models. . J Abnorm Soc Psychol 63: , 575–582. |
[9] | Skaalvik MW , Normann HK , Henriksen N ((2010) ) Student experiences in learning person-centred care of patients with Alzheimer’s disease as perceived by nursing students and supervising nurses. . J Clin Nurs 19: , 2639–2648. |
[10] | Eccleston CEA , Lea EJ , McInerney F , Crisp E , Marlow A , Robinson AL ((2015) ) An investigation of nursing students’ knowledge of dementia: A questionnaire study. . Nurse Educ Today 35: , 800–805. |
[11] | Scerri A , Scerri C ((2013) ) Nursing students’ knowledge and attitudes towards dementia —A questionnaire survey. . Nurse Educ Today 33: , 962–968. |
[12] | Parra-Anguita L , López-Franco María D , Del-Pino-Casado R , García-Fernández FP , Pancorbo-Hidalgo LP ((2022) ) Undergraduate nursing students’ knowledge of Alzheimer’s disease and related dementias care. . J Prof Nurs 39: , 101–108. |
[13] | Rosenberg MJ , Hovland CI (1960) Chapter 1. Cognitive, affective, and behavioral components of attitudes. In Attitude Organization and Change, Hovland CI, Rosenberg MJ, eds. Yale University Press, New Haven. |
[14] | de Vries K , Drury-Ruddlesden J , McGill G ((2020) ) Investigation into attitudes towards older people with dementia in acute hospital using the Approaches to Dementia Questionnaire. . Dementia 19: , 2761–2779. |
[15] | Jünemann A-K (2016) Selbstwert und Selbstvertrauen In Psychologie der Werte: Von Achtsamkeit bis Zivilcourage –Basiswissen aus Psychologie und Philosophie, Frey D, ed. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 187-199. |
[16] | Duden.de, Selbstsicherheit, https://www.duden.de/node/164314/revision/1246838. Accessed June 12, 2023. |
[17] | Bandura A (1997) Self-efficacy: The exercise of control, W.H. Freeman and Company, New York. |
[18] | Bandura A ((2004) ) Health Promotion by Social Cognitive Means. Health Educ Behav 31: , 22S. |
[19] | Elvish R , Burrow S , Cawley R , Harney K , Pilling M , Gregory J , Keady J ((2018) ) ‘Getting to Know Me’: The second phase roll-out of a staff training programme for supporting people with dementia in general hospitals. . Dementia 17: , 96–109. |
[20] | Melchior F , Teichmann B ((2023) ) Measuring dementia knowledge in German: Validation and comparison of the Dementia Knowledge Assessment Scale, the Knowledge in Dementia Scale, and the Dementia Knowledge Assessment Tool 2. . J Alzheimers Dis 94: , 669–684. |
[21] | Annear MJ , Toye CM , Eccleston CE , McInerney FJ , Elliott K-EJ , Tranter BK , Hartley T , Robinson AL ((2015) ) Dementia Knowledge Assessment Scale: Development and preliminary psychometric properties. . J Am Geriatr Soc 63: , 2375–2381. |
[22] | Teichmann B , Melchior F , Kruse A ((2022) ) Validation of the Adapted German Versions of the Dementia Knowledge Assessment Tool 2, the Dementia Attitude Scale, and the Confidence in Dementia Scale for the General Population. . J Alzheimers Dis 90: , 97–108. |
[23] | O’Connor ML , McFadden SH ((2010) ) Development and psychometric validation of the Dementia Attitudes Scale. . Int J Alzheimers Dis 2010: , 454218. |
[24] | Annear MJ , Toye C , Elliott K-EJ , McInerney F , Eccleston C , Robinson A ((2017) ) Dementia knowledge assessment scale (DKAS): Confirmatory factor analysis and comparative subscale scores among an international cohort. . BMC Geriatrics 17: , 168. |
[25] | Terwee CB , Bot SDM , de Boer MR , van der Windt DAWM , Knol DL , Dekker J , Bouter LM , de Vet HCW ((2007) ) Quality criteria were proposed for measurement properties of health status questionnaires. . J Clin Epidemiol 60: , 34–42. |
[26] | Cronbach LJ ((1951) ) Coefficient alpha and the internal structure of tests. . Psychometrika 16: , 297–334. |
[27] | Fritz CO , Morris PE , Richler JJ ((2012) ) Effect size estimates: Current use, calculations, and interpretation. . J Exp Psychol Gen 141: , 2–18. |
[28] | Cohen J (1988) Chapter 3. The Significance of a Product Moment rs. In Statistical power analysis for the behavioral sciences, Erlbaum, Hillsdale, NJ [u.a.], pp. 75-108. |
[29] | Blanca MJ , Alarcón R , Arnau J , Bono R , Bendayan R ((2017) ) Non-normal data: Is ANOVA still a valid option? . Psicothema 29: , 552–557. |
[30] | Schmider E , Ziegler M , Danay E , Beyer L , Bühner M ((2010) ) Is it really robust? . Methodology 6: , 147–151. |
[31] | Döring N , Bortz J (2016) Bestimmung von Teststärke, Effektgröße und optimalem Stichprobenumfang. In Forschungsmethoden und Evaluation in den Sozial- und Humanwissenschaften, Döring N, Bortz J, eds. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 807-866. |
[32] | Rasch B , Friese M , Hofmann W , Naumann E (2021)Varianzanalyse mit MesswiederholungVarianzanalysemit Messwiederholung. In Quantitative Methoden 2: Einführung in die Statistik für Psychologie, Sozial- & Erziehungswissenschaften, Rasch B, Friese M, Hofmann W, Naumann E, eds. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 75-103. |
[33] | Cohen J (1988) Chapter 8. The Analysis of Variance and Covariance. In Statistical power analysis for the behavioral sciences. Erlbaum, Hillsdale, NJ, pp. 273-406. |
[34] | Rasch B , Friese M , Hofmann W , Naumann E (2021) Merkmalszusammenhänge. In Quantitative Methoden 1: Einführung in die Statistik für Psychologie, Sozial- & Erziehungswissenschaften, Rasch B, Friese M, Hofmann W, Naumann E, eds. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 87-123. |
[35] | Rüdiger N, , Baumeister M, , Löhr M, “Lern von mir” - Unterstützung von Menschen mit Demenz in Allgemeinkrankenhäusern,Fachhochschule der Diakonie, http://lernvonmir.fh-diakonie.de/,Accessed June 20, 2023. |
[36] | Mondschein CF , Monda C (2019) The EU’s General Data Protection Regulation (GDPR) in a Research Context. In Fundamentals of Clinical Data Science, Kubben P, Dumontier M, Dekker A, eds. Springer International Publishing, Cham, pp. 55-71 |
[37] | Carnes-Vendrell A , Barallat-Gimeno E , Lara B , Lladó A , Escobar-Bravo M , Reivan-Ortiz G , Maxi-Maxi E , Martínez-Suárez P , Ramírez-Coronel A , Piñol-Ripoll G ((2023) ) Spanish-Dementia Knowledge Assessment Scale (DKAS-S): Ecuadorian validation and comparison among Spanish health students. BMC Geriatr 23: , 210. |
[38] | Gkioka M , Tsolaki M , Papagianopoulos S , Teichmann B , Moraitou D ((2020) ) Psychometric properties of dementia attitudes scale, dementia knowledge assessment tool 2 and confidence in dementia scale in a Greek sample. . Nursing Open 7: , 1623–1633. |
[39] | Spector A , Orrell M , Schepers A , Shanahan N ((2012) ) A systematic review of ‘knowledge of dementia’ outcome measures. . Ageing Res Rev 11: , 67–77. |
[40] | Surr CA , Gates C , Irving D , Oyebode J , Smith SJ , Parveen S ((2017) ) Effective dementia education and training for the health and social care workforce: A systematic review of the literature. . Rev Educ Res 87: , 966–1002. |
[41] | Schneider J , Schönstein A , Teschauer W , Kruse A , Teichmann B ((2020) ) Hospital staff’s attitudes toward and knowledge about dementia before and after a two-day dementia training program. . J Alzheimers Dis 77: , 355–365. |
[42] | Schermuly CC (2020) Empowerment: Die Mitarbeiter stärken und entwickeln. In Handbuch Mitarbeiterführung: Wirtschaftspsychologisches Praxiswissen für Fach- und Führungskräfte, Felfe J, van Dick R, eds. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 1-14. |
[43] | Kimzey M , Mastel-Smith B , Seale A ((2019) ) Effects of dementia-specific education for nursing students. Nurse Educ 44: , 338–341. |
[44] | Mastel-Smith B , Kimzey M , He Z ((2019) ) Dementia care education for nursing students. . J Nurs Educ 58: , 136–143. |
[45] | Adewuyi M , Morales K , Lindsey A ((2022) ) Impact of experiential dementia care learning on knowledge, skills and attitudes of nursing students: A systematic literature review. . Nurse Educ Practice 62: , 103351. |
[46] | Haddock G , Maio GR (2023) Einstellungen. In Sozialpsychologie, Ullrich J, Stroebe W, Hewstone M, eds. Springer Berlin Heidelberg, Berlin, Heidelberg, pp. 193-226. |
[47] | Teichmann B , Gkioka M , Kruse A , Tsolaki M ((2022) ) Informal caregivers’ attitude toward dementia: The impact of dementia knowledge, confidence in dementia care, and the behavioral and psychological symptoms of the person with dementia. A cross-sectional study. . J Alzheimers Dis 88: , 971–984. |
[48] | Hughes J , Bagley H , Reilly S , Burns A , Challis D ((2008) ) Care staff working with people with dementia: Training, knowledge and confidence. . Dementia 7: , 227–238. |
[49] | Breckler SJ ((1984) ) Empirical validation of affect, behavior, and cognition as distinct components of attitude. . J Person Soc Psychol 47: , 1191–1205. |
[50] | Langa KM , Levine DA ((2014) ) The diagnosis and management of mild cognitive impairment: A clinical review. . JAMA 312: , 2551–2561. |
[51] | Schneider J , Miller J , Teschauer W , Kruse A , Teichmann B ((2021) ) Evaluation and effectiveness of a two-day dementia training program for hospital staff working in an emergency department. J Alzheimers Dis 84: , 1631–1644. |
[52] | Bundesagentur für Arbeit, Ausländeranteil unter sozi-alversicherungspflichtig Beschäftigten in der Pflege und insgesamt in Deutschland im Jahr 2021 [Graph], https://de.statista.com/statistik/daten/studie/1029896/umfrage/aus-laenderanteil-an-pflegekraeften-in-deutschland-nach-pfle-geart/, Accessed June 20, 2023. |


