
A 14-Year Longitudinal Analysis of Healthcare Expenditure on Dementia and Related Factors (DEMENCOST Study)
Abstract
Background:
The large number of dementia cases produces a great pressure on health and social care services, which requires efficient planning to meet the needs of patients through infrastructure, equipment, and financial, technical, and personal resources adjusted to their demands. Dementia analysis requires studies with a very precise patient characterization of both the disease and comorbidities present, and long-term follow-up of patients in clinical aspects and patterns of resource utilization and costs generated.
Objective:
To describe and quantify direct healthcare expenditure and its evolution from three years before and up to ten years after the diagnosis of dementia, compared to a matched group without dementia.
Methods:
Retrospective cohort design with follow-up from 6 to 14 years. We studied 996 people with dementia (PwD) and 2,998 controls matched for age, sex, and comorbidity. This paper adopts the provider’s perspective as the perspective of analysis and refers to the costs actually incurred in providing the services. Aggregate costs and components per patient per year were calculated and modelled.
Results:
Total health expenditure increases in PwD from the year of diagnosis and in each of the following 7 years, but not thereafter. Health status and mortality are factors explaining the evolution of direct costs. Dementia alone is not a statistically significant factor in explaining differences between groups.
Conclusion:
The incremental direct cost of dementia may not be as high or as long as studies with relatively short follow-up suggest. Dementia would have an impact on increasing disease burden and mortality.
INTRODUCTION
Dementia is a disease that generates an important impact both at the individual level in patients, caregivers, and society as a whole, as well as in the health system [1, 2]. Some estimations made for Spain show that dementia may become an unmanageable problem if a series of preventive strategies are not implemented [3]. The large number of dementia cases produces a great pressure on health and social care services, which requires efficient planning to meet the needs of patients through infrastructure, equipment, and financial, technical, and personal resources adjusted to their demands [4, 5].
The health and social care of dementia varies throughout the course of the disease and comprises many procedures, including diagnosis, treatment, and outpatient follow-up of the disease and other concomitant pathologies. Moreover, it is also necessary to provide the needs of long-term care and institutionalization in the advanced stages of the disease [6].
One of the major concerns regarding this disease is the costs associated with it [7–9]. It has been described a positive relationship between disease severity and cost of care [10, 11]. Most of the cost studies carried out are of a cross-sectional type [6, 12, 13], and some have shown that the increase in the use of healthcare resources begins before the confirmed diagnosis of the disease, and remains high after the diagnosis [14, 15]. It is therefore often inferred that the costs associated with dementia will be very high as the prevalence of cases increases in the future. On the other hand, mortality after dementia diagnosis is known to be very high and it has been described a reduction in life expectancy due to dementia of 8.8 years [16]; which would make the persistence of the high cost of the disease lower than expected. In this regard, there are longitudinal studies that show that the cost of dementia is lower than estimated in cross-sectional studies [17].
Typically, for studies of dementia-related cost, the use of cohorts including individuals without dementia has been proposed a reliable system to determine the additional cost associated with dementia [15, 18]. There is also an interest in understanding the patterns of resource utilization directly related to the disease [14, 15]. The advanced age at which dementia is usually diagnosed also means that patients usually have high comorbidity, which would explain a significant part of the costs usually attributed to dementia [19, 20]. When analyzing the cost of care, if cases and controls are not matched for comorbidity may result in a source of confounding because the age and sex paired controls are not strictly comparable.
Dementia-related costs include both those directly related to healthcare and those necessary to meet long-term inpatient needs. Also, to be considered are the costs related to the situation of dependency that determines the disease, both formal (care and specialized caregivers in home care) and informal or societal cost that fall on direct caregivers of patients, usually family members. In fact, numerous studies indicate that all these costs account for the greatest proportion of the overall costs related to the disease [13, 21–25]. Therefore, the choice of the perspective of analysis is a crucial issue in any cost analysis of dementia.
The organization of dementia care and its financing can also influence the cost analysis of the disease. A significant part of the costs depends on the degree of institutionalization of patients with dementia, and these costs are not always covered by the same funder as outpatient or inpatient care [26]. Therefore, cost assessments in the integrated framework of health management organizations (HMO) are interesting, although they are scarce and the results are not conclusive [27].
In Spain, public healthcare is universally financed through taxes. Health and Social care administration is devolved to the Autonomous Communities [28]. In Catalonia, according to its own organization, Autonomous government organizes and finances public services. The role of funder and service provider are separated. The public health financer is the Servei Català de la Salut (CatSalut), under the Department of Health, which contracts healthcare services through different programs offered by the providers. The Department of Social Services contracts and finances public places in assisted living facilities for people with different degrees of dependency. Only in pharmacy prescriptions and assisted living facilities is there a co-payment by patients. Each provider offers some or all of the services contracted [29–31].
As highlighted in this review, the study of dementia requires studies with a very precise patient characterization of both the disease and comorbidities present, and long-term follow-up of patients in clinical aspects and patterns of resource utilization and costs generated.
The DEMENCOST study aimed to describe and quantify the patterns of use and overall direct cost of direct healthcare and social services within an HMO, and their evolution from three years before and up to ten years after the diagnosis of dementia, compared to an age- and sex-matched group and comorbidity to control for potential confounding factors.
METHODS
Design
A retrospective population-based cohort was established. Selected individuals were matched for age, sex, and comorbidity with a 1:3 matching ratio between individuals with dementia and those without dementia.
Reference population and financing
We used data from Serveis de Salut Integrats Baix Empordà (SSIBE, http://www.ssibe.cat), a non-profit health management organization (HMO), that is the main provider of public healthcare and social services in the Baix Empordà county (Catalonia, Spain). The SSIBE covers the entire continuum of care at all levels for a population of 92,000 inhabitants [32]. SSIBE as an HMO offers all these services.
This paper adopts the provider’s perspective as the perspective of analysis and refers to the costs actually incurred in providing the contracted services, regardless of the financing obtained. The total healthcare expenditure of SSIBE, including pharmacy cost, in 2017 was € 65.6 M with an average expenditure per patient of € 712.6 (SD € 2,153.7).
Origin of the data
Data were extracted from the following sources:
The Registry of Dementias of Girona (ReDeGi) registers demographic and clinical data of all the incident cases of dementia diagnosed in the neurology or geriatrics outpatient consultation offices, or in the memory clinics of the seven hospitals of the public health care system of the province of Girona (Catalonia, Spain). The methodological principles of the ReDeGi have been previously described [33–36]. ReDeGi records the origin of the dementia cases included. Only the cases from SSIBE’s area of influence were selected.
The SSIBE clinical information system (La Gavina) is a database in real-world practice conditions that collects all the healthcare activity developed in the various SSIBE centers. It is a single register of patients that links each of the care contacts they make with the various centers and services. Each contact is required to be linked to one or more ICD-9-CM codes, ensuring the completeness of the clinical coding. This makes it possible to accurately analyze the episodes of care in relation to the reasons for consultation and the pathologies identified [32, 37]. In addition, by aggregating all episodes for each patient, it facilitates the construction of morbidity profiles using the 3Mtrademark Clinical Risk Groups (CRG) grouper software [38, 39].
A record is available of all the healthcare activities carried out by SSIBE, grouped into 15 partial categories that include primary and specialized care, emergencies, hospitalizations in acute and socio-healthcare hospitals (subacute, hospice care, nursing skilled); residence in assisted living facilities; treatment costs (dialysis, rehabilitation, operating room, etc..), diagnostic tests (imaging, laboratory, etc.) and pharmaceutical costs. The cost of each of the above categories was calculated, as well as the total cost per patient. The costing system developed in SSIBE, Full-costing methodology, was used to determine the aggregate cost per patient and year as previously described [40–43]. To ensure the comparability of costs between the different years of the study, we proceeded to calculate their value updated to 2017 euros, using the system for updating rents with the general CPI (CPI system base 2016) for full annual periods of the Spanish National Statistics Institute (INE, https://www.ine.es/calcula/calcula.do).
Constitution of the cohort and variables
The study used a cohort comprising cases and controls (Fig. 1).
Fig. 1
Cohort composition: Cases, Year of study assignment, Year of inclusion and follow-up period, valid observations per follow-up year.
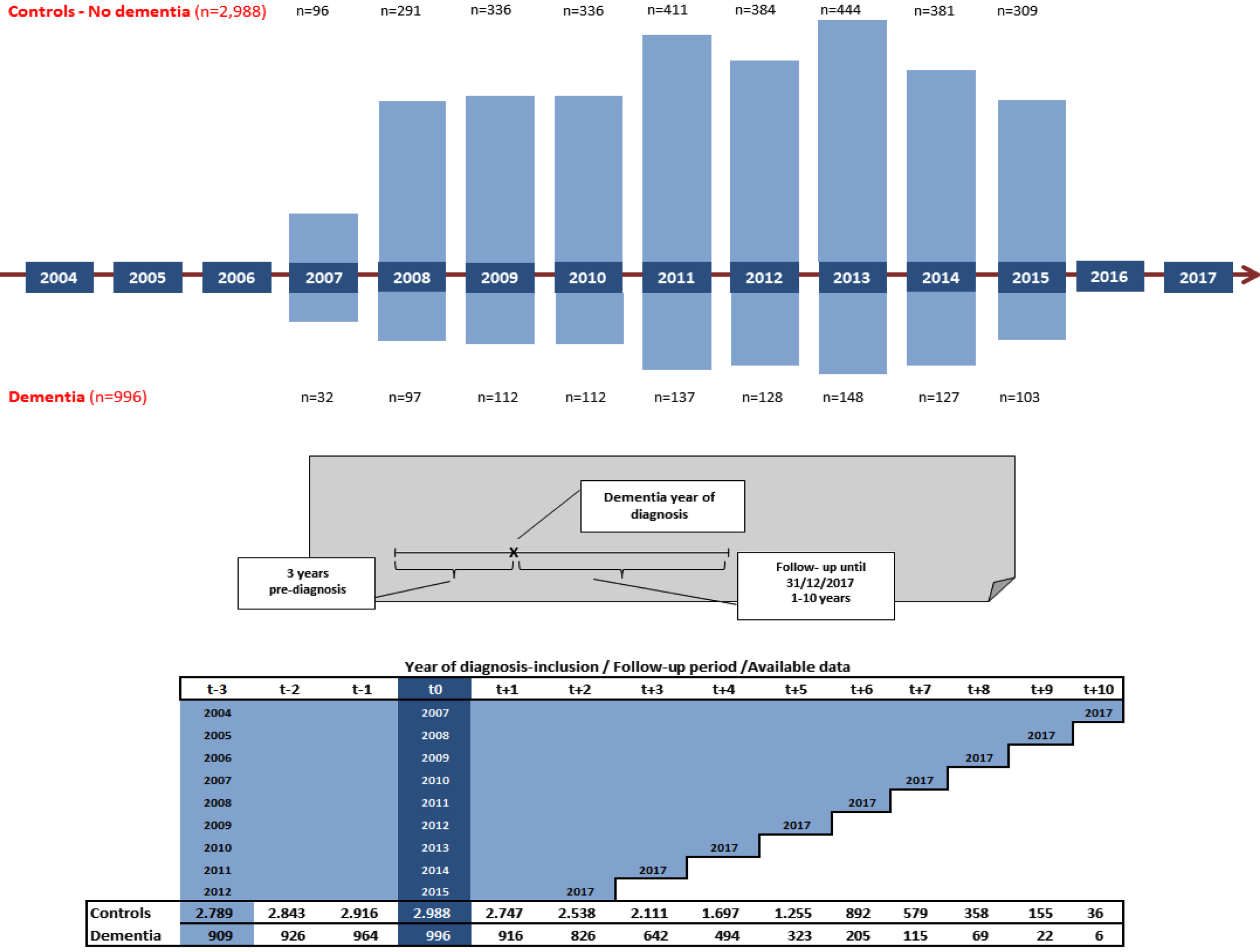
Dementia (Cases): 996 patients diagnosed with dementia by SSIBE and registered by the ReDeGi between 2007–2015 were included.
Non-Dementia (Controls): People residing in the same area with similar characteristics of age, sex, and comorbidity for each of the years included, not diagnosed with dementia before or during the entire follow-up period, were retrospectively selected. Controls were selected from a stratified random sample of the reference population in a 3:1 ratio to cases. A total of 2,988 persons were included. For each year, the baseline population of the same year of inclusion of patients with dementia was used [16].
For each person in the cohort the following variables were recorded: age, sex, and study group, date of inclusion, date of death or exit, and burden of disease each year of the study. Each of the 15 types of healthcare activity listed above was accounted for in each of the study years, as well as the individual cost of each type of healthcare activity, and the overall cost for each of the study years. For dementia, the type and severity as well as various clinical indices in the year of inclusion were added.
Matching
The matching procedure included age, sex, and comorbidity as measured by CRGs. In the CRG model, individuals are classified into individual, mutually exclusive, and exhaustive categories. The highest level of grouping called health status (9 categories) was used. The CRG health status correlates well with healthcare expenditure and allows grouping patients with similar disease burden and healthcare cost characteristics [38, 40]. The health status corresponding to the year of the start of follow-up was used.
Classifications and follow-up
ReDeGi classifies dementia subtypes into the following categories: Alzheimer’s disease (AD); Vascular Dementia; Other degenerative dementias (frontotemporal dementia (FTD) (including FTD behavior variant), Lewy body dementia (LBD), Parkinson-Plus syndrome (PPS) (including dementia in Parkinson’s disease, progressive supranuclear palsy and corticobasal degeneration); Secondary Dementia and Dementias no otherwise specified (DNS) [16]. The year of inclusion in ReDeGi was used as the start date of follow-up. The severity of dementia in the year of diagnosis was assessed using the Clinical Dementia Rating [44].
Comorbidity: Measured by Clinical Risk Groups. Health status was recorded for each year of the study. In addition, the presence of 18 chronic diseases especially relevant and usually related to dementia was recorded.
Longitudinal follow-up of variables: Patients in the cohort were followed up from three years prior to inclusion year and until 12/31/2017 or death or loss to follow-up. The time horizon spans from 2004 to 2017. Follow-up ranged from 6 to 14 years (Fig. 1; Table 1)
Table 1
Cohort composition: results of the matching process by sex, age and health status and severity of dementia
| Controls | Dementia | Alzheimer’s disease | Vascular Dementia | Other degenerative dementias | Secondary Dementia | Dementia NOS | |||||||||
| N | % N | N | % N | N | % N | N | % N | N | % N | N | % N | N | % N | ||
| Sex | Men | 1,062 | 35.5% | 354 | 35.5% | 211 | 31.4% | 74 | 40.7% | 53 | 54.6% | 9 | 33.3% | 7 | 36.8% |
| Women | 1,926 | 64.5% | 642 | 64.5% | 460 | 68.6% | 108 | 59.3% | 44 | 45.4% | 18 | 66.7% | 12 | 63.2% | |
| <65 y | 71 | 2.4% | 23 | 2.3% | 13 | 1.9% | 4 | 2.2% | 4 | 4.1% | 2 | 7.4% | 0 | 0.0% | |
| 64– 75 y | 403 | 13.5% | 130 | 13.1% | 83 | 12.4% | 25 | 13.7% | 16 | 16.5% | 2 | 7.4% | 4 | 21.1% | |
| 75– 84 y | 1,691 | 56.6% | 564 | 56.6% | 383 | 57.1% | 107 | 58.8% | 49 | 50.5% | 17 | 63.0% | 8 | 42.1% | |
| >84 y | 823 | 27.5% | 279 | 28.0% | 192 | 28.6% | 46 | 25.3% | 28 | 28.9% | 6 | 22.2% | 7 | 36.8% | |
| Age | Mean | 80.3 | 80.3 | 80.6 | 80.1 | 80.1 | 79.5 | 79.5 | 79.3 | 79.3 | 80.1 | 80.1 | |||
| SD | 6.5 | 6.4 | 6.2 | 6.2 | 6.2 | 7.5 | 7.5 | 7.5 | 7.5 | 6.1 | 6.1 | ||||
| Median | 81.0 | 81.0 | 81.0 | 81 | 81 | 80 | 80 | 81 | 81 | 80 | 80 | ||||
| p25 | 77.0 | 77.0 | 77.0 | 77 | 77 | 75 | 75 | 77 | 77 | 77 | 77 | ||||
| p75 | 85.0 | 85.0 | 85.0 | 85 | 85 | 85 | 85 | 84 | 84 | 86 | 86 | ||||
| Single Minor Chronic Disease | 12 | 0.4% | 1 | 0.1% | 1 | 0.1% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | |
| Minor Chronic Disease In Multiple Organ Systems | 6 | 0.2% | 1 | 0.1% | 0 | 0.0% | 1 | 0.5% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | |
| Single Dominant Or Moderate Chronic Disease | 459 | 15.4% | 135 | 13.6% | 102 | 15.2% | 19 | 10.4% | 8 | 8.2% | 0 | 0.0% | 3 | 15.8% | |
| CRG Status | Significant Chronic Disease In Multiple Organ Systems | 1,861 | 62.3% | 598 | 60.0% | 421 | 62.7% | 94 | 51.6% | 60 | 61.9% | 26 | 61.9% | 8 | 42.1% |
| Dominant Chronic Disease In Three Or More Organ Systems | 563 | 18.8% | 234 | 23.5% | 132 | 19.7% | 62 | 34.1% | 25 | 25.8% | 15 | 35.7% | 8 | 42.1% | |
| Dominant, Metastatic, And Complicated Malignancies | 77 | 2.6% | 24 | 2.4% | 15 | 2.2% | 5 | 2.7% | 3 | 3.1% | 1 | 2.4% | 0 | 0.0% | |
| Catastrophic Conditions | 10 | 0.3% | 3 | 0.3% | 0 | 0.0% | 1 | 0.5% | 1 | 1.0% | 0 | 0.0% | 0 | 0.0% | |
| Clinical | Mild | 675 | 67.91% | 510 | 76.0% | 100 | 54.9% | 48 | 49.5% | 12 | 44.4% | 5 | 29.4% | ||
| Dementia | Moderate | 222 | 22.33% | 117 | 17.4% | 57 | 31.3% | 34 | 35.1% | 11 | 40.7% | 3 | 17.6% | ||
| Rate (CDR) | Severe | 97 | 9.76% | 44 | 6.6% | 25 | 13.7% | 15 | 15.5% | 4 | 14.8% | 9 | 52.9% | ||
CDR score in 2 cases missed.
Follow-up: Given the characteristics of the cost system that covers the calendar year period, the date of inclusion in the registry is December 31 of the year of declaration. From that moment on, the time spent in the study is calculated until its completion (12/31/2017) or by exit from the study (in case of death the date of death; in case of loss of follow-up the year of loss).
Data analysis
The data, regardless of the calendar year in which they are obtained, are shown taking as reference the year of inclusion of the dementia case in the ReDeGi (t0), being the same for the controls. Likewise, they are calculated for previous (t– 1; t– 2; t– 3) and subsequent years (t+1, t+2…t+10) (Fig. 1). The number of observations available in each of the follow-up years (t+1, t+2…, t+10) is descending considering deaths and loss to follow-up (Fig. 1). Measures of central tendency, dispersion and coefficient of variation are shown. In addition, comparison of proportions (chi-square) and comparison of means (analysis of variance and t-student).
Although the data are generally presented for all cases of dementia, considering the high prevalence of Alzheimer’s disease, some data have been calculated specifically for this variant of dementia.
We assumed that the costs per individual and per period can be modelled using a panel data generalized linear mixed model (GLMM) with a log-link:
the subscripts i and t denoted the individual and the period of costs respectively.
Moreover, we assumed the individual costs were gamma distributed, with the following density:
Finally, to explain the individual healthcare cost, we introduced the relevant variables into the additive linear predictor η of the GLMM:
Where possible values for variables are: Dementia (YES/NO), Age group (<65 y; 65–74 y; 75–84 y;>84 y); Sex (Male/Female); Follow up (number of months); Death (YES/NO); CRG Status (1 Healthy; 2 History Of Significant Acute Disease; 3 Single Minor Chronic Disease; 4 Minor Chronic Disease In Multiple Organ Systems; 5 Single Dominant Or Moderate Chronic Disease; 6 Significant Chronic Disease In Multiple Organ Systems; 7 Dominant Chronic Disease In Three Or More Organ Systems; 8 Dominant, Metastatic, And Complicated Malignancies; 9 Catastrophic Conditions).
We included in the models unstructured random effect (identically and independently distributed) indexed on the subject (either case or control), β0i. These capture both, the dependence of the individuals measured repeatedly in time and individual heterogeneity, that is, unobserved factors associated with each subject invariant over time that could explain the costs.
Given the complexity of our model, we preferred to perform inferences using a Bayesian framework. In particular, we followed the Integrated Nested Laplace Approximation (INLA) approach, within a Bayesian framework [45, 46]. We used penalizing complexity (PC) priors. These priors are robust in the sense that they do not have an impact on the results and, in addition, they have an epidemiological interpretation [47].
The selection of the best GLMM-log Gamma specification was supported by WAIC (Watanabe-Akaike information criteria) and DIC (Deviance information criteria) statistics obtained from preliminary tests.
Analyses were carried out using the IBM SPSSTM (version 25.0) and free software R (https://www.r-project.org) (version 4.2.0), through the INLA package (http://www.r-inla.org/home).
Ethical aspects
The study protocol and the use of anonymized data were approved by the Institutional Review Board of the IDIAP Jordi Gol (P16/066), and the SSIBE Research Committee (Minutes March 24th, 2015). Written informed consent was obtained from patients registered by ReDeGi. Between ReDeGi and SSIBE there is a data exchange agreement in accordance with Spanish personal data protection legislation.
For the controls, the requirement to request signed consent was waived, considering the methodology of the study, based on retrospective review of aggregated clinical-administrative records, developed under real world practice conditions and that there was no recruitment process of the subjects or any specific registry.
SSIBE has a data integrity assurance policy and protocols for data mining for research purposes. Data extraction was performed by a SSIBE professional, and its management was anonymous and unlinked to the original registry. Data available in SSIBE at the time of extraction were collected. No special treatment of missing data was made.
RESULTS
Cohort comparison
A cohort of patients with dementia (N = 996) and without dementia (N = 2,988) were followed up. Table 1 shows, that after the matching process, both groups are comparable, with no relevant differences regarding the distribution by sex, age, and morbidity profile in the year in which they were selected. The distribution of dementia cases by subtypes is shown, and for each of them the same variables mentioned, as well as the degree of severity, also in the year in which each case was diagnosed and included in the dementia registry. In the Dementia group, the proportion of women is higher than that of men (approximately 2:1). Most cases of dementia are diagnosed between 75–84 years old; the mean age is 80.3 (SD±6.4). An average of 31.5 months (SD±20.1) elapses between the onset of symptoms and the diagnosis of dementia. AD is the most common subtype of dementia (67.4% of all cases). According to CRG health status, about 60% of patients are included in the Significant Chronic Disease in Multiple Organ Systems health status. A more disaggregated analysis shows small differences in disease burden between the two groups for a set of 18 different chronic diseases. Overall, controls have a higher proportion of patients with diabetes, ischemic heart disease, hypertension, respiratory disease, and neoplasms than the dementia group, although the magnitude of cases in both groups is similar (Supplementary Table 1). The severity of dementia, according to the Clinical Dementia Rating (CDR) score, shows that 67.9% of cases have mild severity at diagnosis, 22.3% are moderately severe cases and 9.8% are advanced cases; in the case of AD these proportions are 76%, 17.4%, and 6.6% respectively (Table 1). Additional characteristics of dementias are listed in Supplementary Table 2.
Follow-up
The median follow-up was 96 months with an interquartile range of 72–120 months. Mean follow-up was longer in controls than in patients with dementia (97.3±30.9 versus 91.3±27.5; p < 0.001). The cumulative mortality rate during follow-up is 52.2% for the dementia group versus 36.4% in the controls (p < 0.001) justifying the difference in follow-up noted above (Supplementary Table 3). The severity of dementia at the time of diagnosis also influences mortality, so that among mild cases 43.5% of deaths are recorded at follow-up; 66.7% of moderate cases die and in severe cases 79.4% of deaths are reached at the end of follow-up, these differences also being significant (p < 0.001).
Table 2
Descriptive statistics of healthcare cost per study year in both groups of patients. Mean differences and statistical significance
| Cohort Dementia | HCE (t-3) | HCE (t-2) | HCE (t-1) | HCE (t0) | HCE (t + 1) | HCE (t + 2) | HCE (t + 3) | HCE (t + 4) | HCE (t + 5) | HCE (t + 6) | HCE (t + 7) | HCE (t + 8) | HCE (t + 9) | HCE (t + 10) |
| N | 909 | 926 | 964 | 996 | 916 | 826 | 642 | 494 | 323 | 205 | 115 | 69 | 22 | 6 |
| Sum | 1,833,511.47 | 2,166,323.96 | 2,407,274.67 | 3,901,720.44 | 4,159,721.29 | 3,917,262.58 | 3,164,354.57 | 2,518,698.24 | 1,796,723.19 | 1,191,071.50 | 620,756.49 | 223,722.30 | 49,678.81 | 9,448.12 |
| Mean | 2,017.06 | 2,339.44 | 2,497.17 | 3,917.39 | 4,541.18 | 4,742.45 | 4,928.90 | 5,098.58 | 5,562.61 | 5,810.10 | 5,397.88 | 3,242.35 | 2,258.13 | 1,574.69 |
| Standard Deviation | 2,686.47 | 3,361.71 | 3,422.25 | 4,986.58 | 5,794.63 | 6,818.34 | 7,437.73 | 8,365.36 | 9,713.73 | 9,880.21 | 8,985.30 | 5,121.31 | 1,822.70 | 997.09 |
| Variation coefficient | 1.33 | 1.44 | 1.37 | 1.27 | 1.28 | 1.44 | 1.51 | 1.64 | 1.75 | 1.70 | 1.66 | 1.58 | 0.81 | 0.63 |
| Max | 35,099.70 | 41,437.02 | 35,641.51 | 53,227.30 | 60,814.23 | 63,701.28 | 63,272.78 | 64,666.56 | 60,579.95 | 60,522.75 | 36,697.41 | 35,066.18 | 9,226.67 | 3,433.22 |
| Median | 1,306.92 | 1,374.33 | 1,436.39 | 2,312.55 | 2,794.49 | 2,666.95 | 2,628.71 | 2,595.04 | 2,396.80 | 2,411.24 | 2,243.32 | 1,960.88 | 2,156.79 | 1,422.12 |
| Percentil 25 | 693.93 | 718.98 | 759.16 | 1,445.66 | 1,769.85 | 1,682.10 | 1,622.99 | 1,455.11 | 1,409.11 | 1,464.93 | 1,401.95 | 1,093.91 | 943.31 | 843.34 |
| Percentil 75 | 2,403.23 | 2,558.85 | 2,771.75 | 4,069.54 | 4,595.83 | 4,668.60 | 4,591.89 | 4,632.77 | 4,560.14 | 4,812.17 | 3,167.07 | 2,958.32 | 2,470.81 | 1,707.39 |
| Percentil 95 | 5,931.38 | 8,648.83 | 9,097.31 | 13,550.82 | 14,832.82 | 16,465.01 | 17,015.82 | 18,186.51 | 26,047.56 | 29,682.89 | 33,214.81 | 10,560.54 | 4,060.40 | 3,433.22 |
| Cohort controls | ||||||||||||||
| N | 2,789 | 2,843 | 2,916 | 2,988 | 2,747 | 2,538 | 2,111 | 1,697 | 1,255 | 892 | 579 | 358 | 155 | 36 |
| Sum | 5,682,927.15 | 6,358,533.01 | 7,144,592.98 | 9,140,452.26 | 7,560,419.52 | 6,938,929.38 | 5,988,079.51 | 4,769,342.86 | 3,426,146.17 | 2,563,894.23 | 1,867,900.14 | 1,051,132.44 | 398,873.02 | 75,575.41 |
| Mean | 2,037.62 | 2,236.56 | 2,450.13 | 3,059.05 | 2,752.25 | 2,734.01 | 2,836.61 | 2,810.46 | 2,730.00 | 2,874.32 | 3,226.08 | 2,936.12 | 2,573.37 | 2,099.32 |
| Standard Deviation | 2,924.21 | 3,400.10 | 4,120.88 | 4,372.45 | 4,401.90 | 4,451.47 | 4,919.45 | 4,831.71 | 4,469.94 | 5,473.71 | 6,039.73 | 4,654.23 | 4,414.12 | 1,925.08 |
| Variation coefficient | 1.44 | 1.52 | 1.68 | 1.43 | 1.60 | 1.63 | 1.73 | 1.72 | 1.64 | 1.90 | 1.87 | 1.59 | 1.72 | 0.92 |
| Max | 43,830.72 | 60,433.82 | 54,713.14 | 47,286.72 | 61,065.75 | 60,642.96 | 61,363.56 | 59,488.56 | 64,074.10 | 60,726.05 | 60,139.98 | 36,179.30 | 30,996.60 | 8,562.77 |
| Median | 1,290.77 | 1,329.18 | 1,394.95 | 1,609.93 | 1,515.24 | 1,490.85 | 1,431.24 | 1,406.25 | 1,413.86 | 1,385.03 | 1,284.25 | 1,430.10 | 1,222.83 | 1,540.01 |
| Percentil 25 | 668.00 | 702.68 | 718.81 | 829.92 | 799.66 | 755.50 | 774.41 | 774.74 | 755.82 | 741.70 | 745.78 | 730.64 | 737.29 | 1,057.67 |
| Percentil 75 | 2,270.73 | 2,406.71 | 2,506.31 | 3,198.85 | 2,789.08 | 2,805.50 | 2,726.83 | 2,732.13 | 2,671.84 | 2,735.56 | 2,872.81 | 2,809.94 | 2,363.83 | 2,312.74 |
| Percentil 95 | 6,576.99 | 7,137.28 | 7,462.75 | 11,152.31 | 9,030.24 | 9,170.57 | 10,315.65 | 9,785.18 | 10,370.45 | 9,595.30 | 12,323.71 | 11,297.35 | 8,111.97 | 7,080.97 |
| Differences | ||||||||||||||
| Mean | – 20.56 | 102.88 | 47.04 | 858.34 | 1788.93 | 2008.44 | 2092.29 | 2288.12 | 2832.61 | 2935.78 | 2171.8 | 306.23 | – 315.24 | – 524.63 |
| Median | 16.15 | 45.15 | 41.44 | 702.62 | 1279.25 | 1176.1 | 1197.47 | 1188.79 | 982.94 | 1026.21 | 959.07 | 530.78 | 933.96 | – 117.89 |
| t-student p < | NS | NS | NS | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.014 | NS | NS | NS |
HCE: Healthcare Expenditure. Euros 2017; NS: Not significant.
Comparison of healthcare cost
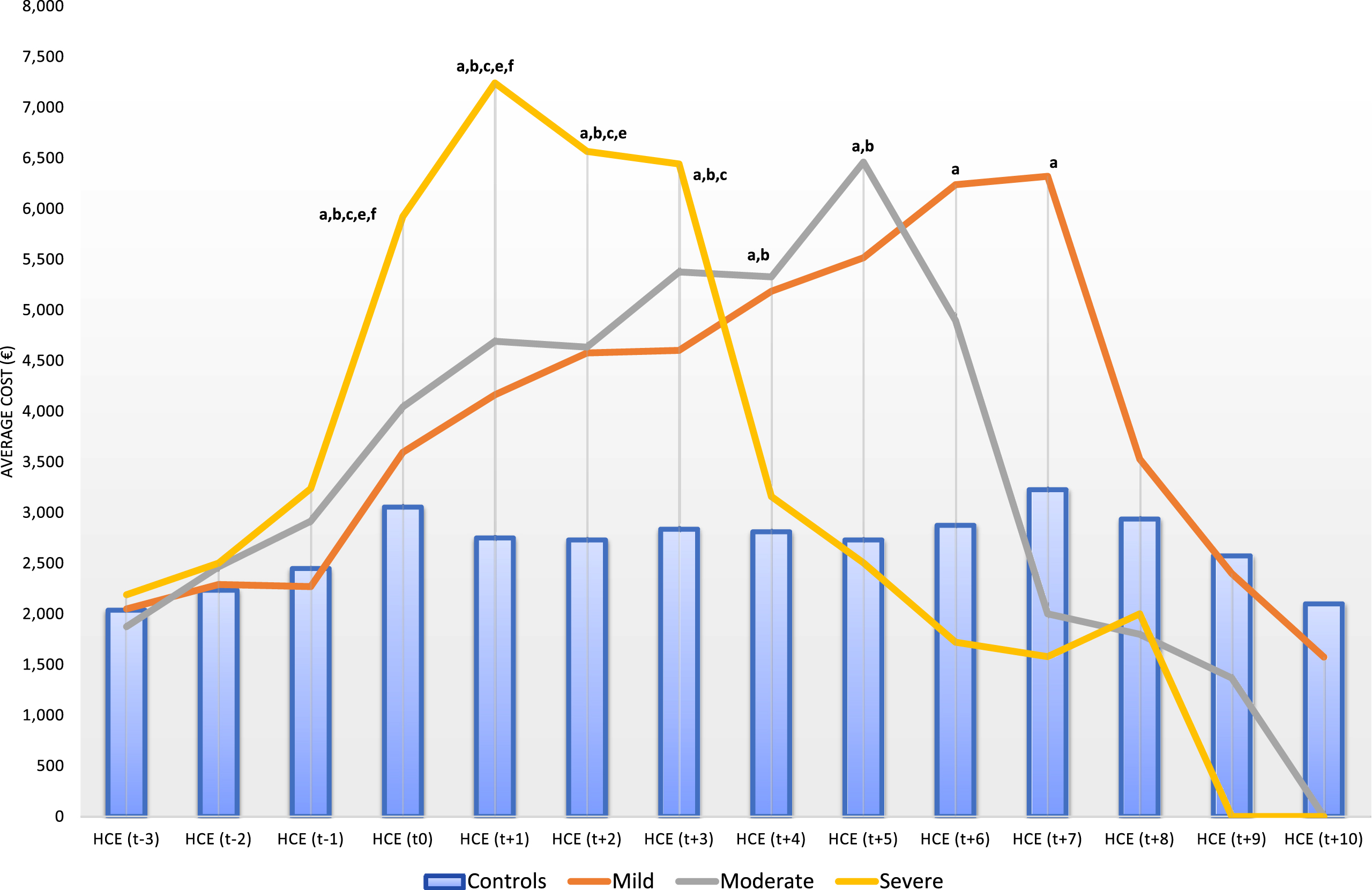
To evaluate the annual direct cost differential between the two groups of patients, healthcare expenditure was monitored from the year of diagnosis of the disease and inclusion in the study. The diagnosis process, from the onset of symptoms to definitive diagnosis, takes an average of 2.5 years and therefore the costs of the three years prior to diagnosis were analyzed. In the year of diagnosis of dementia, the median cost is € 2,312.55 (IR € 1,445.66 – 4,069.54) with an increase of € 702.62 compared to controls. Six years after diagnosis, the maximum mean direct cost of € 5,810.10 (SD 702.62) is reached and the difference compared to controls is € 2,937.78 (p < 0.001) (Table 2). The total healthcare direct cost increases statistically significantly in the dementia group from the year of diagnosis and in each of the following 7 years (p < 0.001) (Table 2, Fig. 2; Supplementary Table 4). In the three years prior to diagnosis and from 8 years of follow-up the difference is not significant (Table 2; Fig. 2).
The behavior is similarly reproduced when considering the severity of dementia (CDR score) at diagnosis. However, in the most severe cases of dementia the maximum increase occurs only one year after diagnosis and remains significantly elevated only 2 more years (Fig. 2). There are no statistically significant differences between patients with mild or moderate disease but with patients with severe dementia, although the maximum increase occurs earlier the more severe the disease (Fig. 2).
Fig. 2
Evolution of average total healthcare expenditure of patients by year of diagnosis and severity of the disease. Differences Statistically significant (p < 0.01): a) Control versus Mild; b) Control versus Moderate; c) Control versus Severe; d) Mild versus Moderate; e) Mild versus Severe; f) Moderate versus Severe.
Alzheimer’s disease analysis
When we consider two groups of dementias (AD and Other Dementias), the behavior is slightly different in the case of AD. In the year of diagnosis and previous years, no differences are observed with respect to controls. This significant increase occurs from the year following diagnosis and the progression in the increase in cost is slower and sustained over time until it reaches a maximum 6 years after diagnosis. Statistically significant differences disappear 8 years after diagnosis (Supplementary Figure 1). Similarly, when considered according to the severity of AD, the evolution of costs is smoother (Supplementary Figure 2).
Cost component analysis
An analysis of the different components of total direct cost has been performed. In general, there is a significant increase in the cost of pharmacy, the cost of long-stay hospitalization (subacute, hospice, nursing skilled) and specific day hospital for patients with dementia as well as institutionalization facilities expenditures (nursing home, assisted living facilities). These differences appear from the year of diagnosis of the disease and are maintained for 5–7 years after diagnosis (Fig. 3; Supplementary Table 5). In contrast, the cost in primary care decreases in the dementia group as well as the cost of hospitalization for acute problems of any cause not strictly related to dementia. These differences are statistically significant from the year of diagnosis and during the following 8 years in the case of visits to the primary care physician. Hospitalization costs for acute problems in the dementia group is lower than controls between 4–7 years after diagnosis, which could be explained by the differences between the two groups in the burden of chronic diseases (Supplementary Tables 1 and 5). Pharmaceutical expenditure represents about 50–55% of the total cost in both controls and dementia cases at the time of diagnosis, although it gradually decreases to about 25% seven years after inclusion in the study (Fig. 3), as the need for short and long stay hospitalization increases and evolves in the opposite direction.
The average cumulative total direct cost from diagnosis of dementia to the end of follow-up was € 21,588.5 (SD € 28,426.4) compared to € 14,629.8 (SD € 18,567.2) in controls, which means that the additional cost associated with dementia in the years of follow-up from diagnosis is € 6,958.6 (95% CI±1,537.9). The total cumulative direct cost according to the severity of dementia at diagnosis (CDR) is, in mild dementia € 22,561.9 (SD € 29,197.1), in moderate dementia € 19,000.9 (SD € 26,033.8€) and in severe dementia € 21,192.6 (SD € 27,805.4). There are no statistically significant differences between degrees of severity, although there are differences with respect to controls. The cumulative direct cost values in the case of AD are € 27,609.4 (SD € 32,132.5), € 23,259.2 (SD € 23,757.1), and € 24,265.6 (SD € 23,974.6) for mild, moderate, and severe cases, respectively.
Fig. 3
Cost components and annual evolution in both groups of patients according to year of diagnosis/inclusion. Only cost components (columns) whose cost is significantly higher in the dementia group than in the control group are shown. All years are shown although in some years there is no difference.

Other healthcare resource utilization
We have not detected differences in the consumption of acute hospital stays between controls and dementia cases even when considering the levels of severity of the disease, with annual consumption being around 80 stays/100 persons (Supplementary Figure 4). On the other hand, the consumption of skilled nursing stays increases considerably. This increase is progressive from the year of diagnosis in the dementia cohort and ranges from 390 stays/100 patients to 1,729 stays/100 patients (maximum 5 years after diagnosis) compared to 232 stays/100 patients in the control group (Supplementary Figure 5). It is also interesting to note that since the diagnosis of dementia, the rate of people using institutionalization services (assisted living facilities and skilled nursing facilities) increases from about 5% in controls to between 9–14% in patients with dementia in the seven years after diagnosis to equalize later (Supplementary Figure 6).
Cost modelling
The model estimates healthcare direct cost over the full follow-up period and shows the factors that are statistically significant in shaping it. The dataset includes 35,830 person-year observations. The final model includes the factors dementia, age, sex, disease burden, mortality, and length of follow-up, as well as interactions between them (mortality and health status; dementia and health status) (Table 3). Since it was not possible to specifically follow the clinical course of dementia, we used the annual evolution of health status (measured as CRG status) as a proxy for this evolution (Supplementary Figure 3).
Table 3
Generalized linear mixed model (GLMM) on healthcare expenditure over the full follow-up period
| Reference category | Factor | Main Coefficients | RR (95% CI) | Significant at |
| Intercept | 8.0024 | 4.8116–11.1918 | 95% | |
| Dementia = NO | Dementia = YES | 0.3098 | – 4.189–4.8067 | NS |
| Age <65 y | age 64–75 y | 0.0739 | 0.0231–0.1246 | 95% |
| age 75–84 y | – 0.0789 | – 0.1193– – 0.0385 | 95% | |
| age >84y | – 0.0210 | – 0.0482–0.0062 | 90% | |
| Sex = Male | sexe = female | 0.0486 | 0.0325–0.0646 | 95% |
| Follow-up = 0 | Follow_up months | 0.0010 | 0.0006–0.0014 | 95% |
| CRG Status = 1 Healthy | status = 2 | 1.6766 | 1.5216–1.8316 | 95% |
| status = 3 | 1.6113 | 1.4656–1.7568 | 95% | |
| status = 4 | – 0.0639 | – 0.1976–0.0697 | NS | |
| status = 5 | – 0.0142 | – 0.1414–0.1129 | NS | |
| status = 6 | 0.5745 | 0.4505–0.6984 | 95% | |
| status = 7 | 0.0391 | – 0.054–0.1321 | NS | |
| status = 8 | 0.0723 | – 0.0141–0.1588 | 90% | |
| status = 9 | 0.1122 | 0.0417–0.1826 | 95% | |
| Exitus = NO | Exitus = Yes | 0.4411 | 0.3921–0.4901 | 95% |
| CRG Status = 1 Healthy * Dementia = NO | status = 2*Dementia = YES | – 0.7484 | – 0.9782– – 0.5188 | 95% |
| status = 3*Dementia = YES | 0.5324 | 0.3139–0.7507 | 95% | |
| status = 4*Dementia = YES | – 0.2353 | – 0.4332– – 0.0374 | 95% | |
| status = 5*Dementia = YES | 0.0171 | – 0.1655–0.1995 | NS | |
| status = 6*Dementia = YES | 0.3052 | 0.1322–0.478 | 95% | |
| status = 7*Dementia = YES | – 0.3745 | – 0.5044– – 0.2446 | 95% | |
| status = 8*Dementia = YES | – 0.0778 | – 0.1973–0.0417 | NS | |
| status = 9*Dementia = YES | 0.1940 | 0.0971–0.2909 | 95% | |
| CRG Status = 1 Healthy * Exitus = NO | status = 2*Exitus = YES | – 0.4600 | – 0.6396– – 0.2806 | 95% |
| status = 3*Exitus = YES | 0.2118 | 0.0397–0.3837 | 95% | |
| status = 4*Exitus = YES | 0.1152 | – 0.0432–0.2734 | 90% | |
| status = 5*Exitus = YES | – 0.2470 | – 0.3944– – 0.0997 | 95% | |
| status = 6*Exitus = YES | 0.2579 | 0.1111–0.4045 | 95% | |
| status = 7*Exitus = YES | – 0.0588 | – 0.1684–0.0507 | NS | |
| status = 8*Exitus = YES | – 0.0895 | – 0.2042–0.0252 | 90% | |
| status = 9*Exitus = YES | 0.1315 | 0.0336–0.2292 | 95% |
CRG Status (1 Healthy; 2 History of Significant Acute Disease; 3 Single Minor Chronic Disease; 4 Minor Chronic Disease in Multiple Organ Systems; 5 Single Dominant Or Moderate Chronic Disease; 6 Significant Chronic Disease In Multiple Organ Systems; 7 Dominant Chronic Disease In Three Or More Organ Systems; 8 Dominant, Metastatic, And Complicated Malignancies; 9 Catastrophic Conditions). NS, not significant.
The model shows that CRG health status and death are the main factors explaining the evolution of direct costs and the differences between the two groups (Table 3). Dementia alone is not a statistically significant factor in explaining the differences between the two groups, unlike the burden of disease as measured by CRG health status. This finding confirms the one found in which the same model was evaluated but without introducing disease burden as an explanatory factor. In this previous model the dementia factor is also not significant and only age; sex and mortality are significant (Supplementary Table 6). Consequently, the overall burden of disease may be absorbing the explanatory power of the dementia factor. Age, sex, and length of follow-up are other factors that contribute significantly to shaping the total cost of patients during the follow-up period. Disease severity, as measured by the CDR score, was considered in the choice of the best GLMM model but was discarded as it was not significant (Supplementary Tables 7 and 8).
The interrelationship between dementia, burden of disease, and mortality is a complex issue, as is evident when analyzing the interrelationships between these factors that we have introduced into the model (Table 3).
If we consider the data shown as a whole (Tables 2 and 3; Fig. 2), the most plausible interpretation is to speak of a concentration of costs in dementia patients in the first years after diagnosis, particularly in the most severe cases of dementia, where significant cross-sectional differences are observed. However, overall, when considering a follow-up long enough to include the life expectancy of these patients, the volume of costs for dementia patients is lower than estimated in the short-term studies.
DISCUSSION
The DEMENCOST study has shown that the diagnosis of dementia, in any of its clinical varieties, increases the direct healthcare costs of patients with dementia when compared to a group of patients with similar characteristics in age, sex, and disease burden. From the year of diagnosis, there are increases in annual costs that are maintained for the following 6–7 years, and then become like those of the control group. Therefore, we can speak of a concentration of healthcare expenditure during the first years of the disease which, ultimately, represents a lower increase in direct healthcare expenditure than is seen in those first years.
Probably in the final years of the disease, there is a limitation of the therapeutic effort conditioned by the advanced age of the patients, the high burden of comorbidity and the evolution of dementia itself. It should also be noted that between 85–90% of patients usually remain at home where they receive most of the care. We do not have an estimate of the other costs associated with this care. However, attributing all these other costs exclusively to dementia may be excessive if we consider the factors outlined above.
The drivers of direct healthcare expenditure in both the dementia and the control group are the overall burden of disease, mortality, age, and being female. The higher mortality caused by dementia, particularly in the most severe cases of the disease, shortens the follow-up period of these patients and ultimately seems to determine that the overall direct healthcare expenditure does not differ so much between the two groups of patients. Dementia has an impact on increasing disease burden and mortality.
Two fundamental ideas underlie our findings. On the one hand, our results show that burden of disease is the factor that seems to best explain healthcare costs in people in the last years of life, as reported previously [43]. This idea also coincides with that of Kollerupp et al. who show that the development of cardiovascular or oncological diseases represents a significant increase in cost, although it is the overall burden of disease that determines the population cost [48]. In our case, dementia would have a similar behavior to that described by these authors.
The other idea underlying the findings we show is that the incremental direct cost of dementia may not be as high or as long as suggested by most studies with relatively short follow-ups of patients of similar age, sex, and disease burden. This idea had previously been suggested by Yang et al, where they demonstrated through simulation studies that the net costs of dementia were lower than those shown in cross-sectional studies of relatively short duration [17].
To our knowledge, the DEMENCOST study, based on individual real-world patient data, has the longest follow-up of those published so far and shows that incremental cost has specific characteristics that are not captured by most published studies, as they are generally cross-sectional studies or with shorter follow-up periods [49–51]. The only two studies of which we are aware with prolonged follow-up are those of Sopina et al. in Denmark and Persson et al. in Sweden [52, 53].
Sopina et al. include a follow-up of the 10 years prior to the diagnosis of AD and five years afterwards [52]. Persson et al. include data from 10 years prior to diagnosis, the year of diagnosis, and the following six years [53]. There are similarities and differences between these two studies. In Denmark only AD is included, while the Swedish study includes all types of dementia. In both studies they analyze a period of 10 years before diagnosis although the findings are significantly different, probably because in the Swedish study the matching is only done by age, sex, and municipality of residence, while in the Danish case they also take into account the burden of disease. In both cases there is a rise in costs immediately after diagnosis, but they remain high for about four years in Sweden and about 5 years in Denmark, although the behavior is similar in both cases. Another similarity is that in both cases the costs related to nursing homes are excluded. The costs of the Swedish study do not include pharmaceutical costs either.
Our study includes a matching by age, sex, and comorbidity from the start of follow-up with a control group in a 3:1 to cases, which partly compensates for the smaller size of our sample in relation to the aforementioned studies. On the other hand, a wider range of services and a longer duration of follow-up are included. When compared, the results shown by these authors are like those shown by us in the first 5–6 years after diagnosis. However, they are not able to detect the decrease in cost that we detected in our study, since this occurs approximately from the time when these authors end their follow-up. Nevertheless, the conclusions of Sopina et al. are like those of our study.
Strengths
Our study has several important strengths to highlight. Case-control matching at the beginning of follow-up has been performed, considering not only age and sex, but also burden of disease, which has allowed for a more accurate determination of the dementia-related cost burden, as has been shown previously [54].
The second strength is the duration of the study, which, based on real-world data, obtains individual data for people aged between 6 and 14 years, making it possible to appreciate the evolution of the costs analyzed over a horizon in line with the expected survival of the patients [16].
Finally, the DEMENCOST study, conducted in an HMO, has adopted the perspective of the healthcare provider who must consider the health care and social demands of the population it serves to plan the necessary health care resources. In this regard, the analysis of the cost components has established that the greatest needs are directed towards the availability of nursing homes and specialized care facilities, as well as day centers specially designed for these patients, and is substantially in line with findings in a similar setting [55]. Overall, the rest of the components show similar behavior to the control group with a similar burden of disease.
Limitations
The choice of the perspective of the analysis also becomes the main limitation of our study, as it does not consider informal and societal costs as highlighted previously [24, 25, 56, 57]. Our data include, at least, the costs related to the institutionalization of these patients, which are publicly funded through healthcare and social care providers as discussed in the Introduction. Leitch et al. find that impairment of basic and instrumental activities of daily living as the main determinants of costs and suggest that nursing home admission costs decrease societal costs although this should not be the preferred option [58].
Nevertheless, informal professional or non-professional care (usually related to the family) is not included. In Spain, professional care of this type is financed through the so-called Dependency Law by means of personal benefits for each patient [59].
The societal costs associated with non-professional care are high and depend on the methodology used to calculate them [60–62]. Regardless of these considerations, these studies, at least to our knowledge, do not usually perform matching processes such as the one we performed, especially regarding the burden of disease. Therefore, they could tend to attribute excess informal costs to the disease studied without elucidating which part is related to the disease analyzed and which part to other comorbidities. In this regard, it is equally important to highlight our findings on the different duration of the increase in healthcare cost in relation to disease severity and mortality. Considering our results, we suggest that this could be a new line of research in the future.
Another limitation is that we have not been able to relate the clinical and functional deterioration caused by dementia to the increase in costs detected because of the lack of clinical follow-up data [58, 63]. However, the degree of severity at diagnosis, as measured by the CDR score, indicates that greater severity implies an increase in cost earlier and of shorter duration but of equal magnitude to cases of lesser severity.
ReDeGi records data on educational level, marital status, and professional category. These data are not systematically recorded in the SSIBE database. The study protocol did not contemplate active recruitment of controls, only collection of routinely available data. This limitation therefore does not allow these variables of interest to be used as possible confounding factors in comparative analyses of the two groups.
External validity and extrapolation of results
As in any other study, but especially in cost studies, we must consider the external validity of our results. In this respect, differences between countries, with different organizational and funding models, as well as in the perspective chosen for the analysis may be important, as has been pointed out in the literature referring to this disease [13, 61, 62, 64–66]; especially when some studies have already shown differences between cohorts of dementia patients in different countries in relation to socio-demographic and clinical factors [67, 68]. Moreover, we must consider recent studies that indicate a probable relative decrease in the population impact of dementia. Thus, Wolters et al. suggest a certain decrease in incidence in Europe and the United States [69], and Pierse et al. revise downwards the projection of dementia cases in the coming years in Ireland, with a methodology that can be generalized to other countries [70]. This leads us to believe that, without taking these projections into account and based on limited cost projections, the estimate of the costs needed for dementia care may have been magnified.
The DEMENCOST study, given its unique characteristics, population scope, long-term follow-up of patients, and focus on a single provider offering the full range of services, may be useful to estimate the diverse needs of patients who develop and live with dementia. In this way, it can improve the planning of health and social resources certainly in Catalonia and most likely in Spain. Its translation to other countries with different lifestyles and organizational structures, as well as differentiated funding systems should be done in a prudent way. Further studies in other regions and countries would be needed to confirm the results we have shown.
ACKNOWLEDGMENTS
To the members of the SSIBE Cognitive Disorders Unit who have identified, diagnosed, treated, and registered the data of our patients in the Girona Dementia Registry (ReDeGi) during the years of inclusion of patients in the study.
To Inma Sanchez who carried out the selection of the cohort of patients and their matching.
To Montse Rovira for her editorial work in the development of the project.
FUNDING
This study has been partially funded by Instituto de Salud Carlos III through the project “PI15/01980” (Co-funded by European Regional Development Fund/European Social Fund “A way to make Europe”/“Investing in your future”). The funder had no role in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; or the preparation, review, or approval of the manuscript.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data available on request due to privacy/ethical restrictions.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-221220.
REFERENCES
[1] | Nichols E , Steinmetz JD , Vollset SE , Fukutaki K , Chalek J , Abd-Allah F , Abdoli A , Abualhasan A , Abu-Gharbieh E , Akram TT , et al. ((2022) ) Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7: , e105–e125. |
[2] | Livingston G , Huntley J , Sommerlad A , Ames D , Ballard C , Banerjee S , Brayne C , Burns A , Cohen-Mansfield J , Cooper C , Costafreda SG , Dias A , Fox N , Gitlin LN , Howard R , Kales HC , Kivimäki M , Larson EB , Ogunniyi A , Orgeta V , Ritchie K , Rockwood K , Sampson EL , Samus Q , Schneider LS , Selbæk G , Teri L , Mukadam N ((2020) ) Dementiaprevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396: , 413–446. |
[3] | Soto-Gordoa M , Arrospide A , Moreno-Izco F , Martínez-Lage P , Castilla I , Mar J ((2015) ) Projecting burden of dementia in Spain, 2010–2050: Impact of modifying risk factors. J Alzheimers Dis 48: , 721–730. |
[4] | Prince M , Guerchet M , Prina M , International AD ((2013) ) Policy brief for Heads of Government: The global impact of dementia 2013–2050. London. https://www.alz.co.uk/research/GlobalImpactDementia2013.pdf. |
[5] | Wu YT , Fratiglioni L , Matthews FE , Lobo A , Breteler MMBB , Skoog I , Brayne C ((2016) ) Dementia in western Europe: Epidemiological evidence and implications for policy making. Lancet Neurol 15: , 116–124. |
[6] | Jönsson L , Wimo A ((2009) ) The cost of dementia in Europe: A review of the evidence, and methodological considerations. Pharmacoeconomics 27: , 391–403. |
[7] | Wimo A , Guerchet M , Ali G-CC , Wu Y-TT , Prina AM , Winblad B , Jönsson L , Liu Z , Prince M ((2017) ) The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement 13: , 1–7. |
[8] | Wimo A , Jönsson L , Gustavsson A , McDaid D , Ersek K , Georges J , Gulácsi L , Karpati K , Kenigsberg P , Valtonen H ((2011) ) The economic impact of dementia in Europe in 2008-cost estimates from the Eurocode project. Int J Geriatr Psychiatry 26: , 825–832. |
[9] | Gustavsson A , Brinck P , Bergvall N , Kolasa K , Wimo A , Winblad B , Jönsson L ((2011) ) Predictors of costs of care in Alzheimer’s disease: A multinational sample of 1222 patients. Alzheimers Dement 7: , 318–327. |
[10] | Leicht H , Heinrich S , Heider D , Bachmann C , Bickel H , van den Bussche H , Fuchs A , Luppa M , Maier W , Mösch E , Pentzek M , Rieder-Heller SG , Tebarth F , Werle J , Weyerer S , Wiese B , Zimmermann T , König HH ; AgeCoDe study group ((2011) ) Net costs of dementia by disease stage. Acta Psychiatr Scand 124: , 384–395. |
[11] | Quentin W , Riedel-Heller SG , Luppa M , Rudolph A , König H-HH ((2010) ) Cost-of-illness studies of dementia: A systematic review focusing on stage dependency of costs. Acta Psychiatr Scand 121: , 243–259. |
[12] | Takizawa C , Thompson PL , Van Walsem A , Faure C , Maier WC ((2015) ) Epidemiological and economic burden of Alzheimer’s disease: A systematic literature review of data across Europe and the United States of America. J Alzheimers Dis 43: , 1271–1284. |
[13] | Cantarero-Prieto D , Leon PL , Blazquez-Fernandez C , Juan PS , Cobo CS ((2020) ) The economic cost of dementia: A systematic review. Dementia (London) 19: , 2637–2657. |
[14] | Eisele M , Van Den Bussche H , Koller D , Wiese B , Kaduszkiewicz H , Maier W , Glaeske G , Steinmann S , Wegscheider K , Schön G ((2010) ) Utilization patterns of ambulatory medical care before and after the diagnosis of dementia in Germany - Results of a case-control study. Dement Geriatr Cogn Disord 29: , 475–483. |
[15] | Chen L , Reed C , Happich M , Nyhuis A , Lenox-Smith A ((2014) ) Health care resource utilisation in primary care prior to and after a diagnosis of Alzheimer’s disease: A retrospective, matched case– control study in the United Kingdom. BMC Geriatr 14: , 76. |
[16] | Garre-Olmo J , Ponjoan A , Inoriza JM , Blanch J , Sánchez-Pérez I , Cubí R , de Eugenio R , Turró-Garriga O , Vilalta-Franch J ((2019) ) Survival, effect measures, and impact numbers after dementiadiagnosis: A matched cohort study. Clin Epidemiol 11: , 525–542. |
[17] | Yang Z , Zhang K , Lin P-JJ , Clevenger C , Atherly A ((2012) ) A longitudinal analysis of the lifetime cost of dementia. Health Serv Res 47: , 1660–1678. |
[18] | Schwarzkopf L , Menn P , Leidl R , Wunder S , Mehlig H , Marx P , Graessel E , Holle R ((2012) ) Excess costs of dementia disorders and the role of age and gender - an analysis of German health and long-term care insurance claims data. BMC Health Serv Res 12: , 165. |
[19] | Poblador-Plou B , Calderón-Larrañaga A , Marta-Moreno J , Hancco-Saavedra J , Sicras-Mainar A , Soljak M , Prados-Torres A , Calderon-Larranaga A , Marta-Moreno J , Hancco-Saavedra J , Sicras-Mainar A , Soljak M , Prados-Torres A ((2014) ) Comorbidity of dementia: A cross-sectional study of primary care older patients. BMC Psychiatry 14: , 84. |
[20] | Zhu CW , Cosentino S , Ornstein KA , Gu Y , Andrews H , Stern Y ((2017) ) Interactive effects of dementia severity and comorbidities on medicare expenditures. J Alzheimers Dis 57: , 305–315. |
[21] | Ruiz-Adame Reina M ((2018) ) Estudios de costes sociales, directos e indirectos, de la atención a personas con demencias tipo alzheimer en Andalucía. Thesis. Universidad de Granada. |
[22] | Peña-Longobardo LM , Rodríguez-Sánchez B , Oliva-Moreno J , Aranda-Reneo I , López-Bastida J ((2019) ) How relevant are social costs in economic evaluations? The case of Alzheimer’s disease. Eur J Health Econ 20: , 1207–1236. |
[23] | Farré M , Haro JM , Kostov B , Alvira C , Risco E , Miguel S , Cabrera E , Zabalegui A ((2016) ) Direct and indirectcosts and resource use in dementia care: A cross-sectional study in patients living at home. Int J NursStud 55: , 39–49. |
[24] | Ruiz-Adame Reina M , Correa M , Burton K ((2019) ) The opportunity costs of caring for people with dementia in Southern Spain. Gac Sanit 33: , 17–23. |
[25] | Turró-Garriga O , López-Pousa S , Vilalta-Franch J , Turon-Estrada A , Pericot-nierga I , Lozano-Gallego M , Hernández-Ferràndiz M , Soler-cors O , Planas-Pujol X , Monserrat-Vila S , Garre-olmo J ((2010) ) Valoreconómico anual de la asistencia informal en la enfermedad de Alzheimer. Rev Neurol 51: , 201–207. |
[26] | Rice DP , Fillit HM , Max W , Knopman DS , Lloyd JR , Duttagupta S ((2001) ) Prevalence, costs, and treatment of Alzheimer’s disease and related dementia: A managed care perspective. Am J Manag Care 7: , 809–818. |
[27] | Fishman P , Coe NB , White L , Crane PK , Park S , Ingraham B , Larson EB ((2019) ) Cost of dementia in Medicare managed care: A systematic literature review. Am J Manag Care 25: , e247–e253. |
[28] | Bernal-Delgado E , García-Armesto S , Oliva J , Sánchez Martínez F , Repullo J , Peña- Longobardo L , Ridao-López M , Hernández-Quevedo C ((2018) ) Spain Health system review. Health Syst Transit 20: , 1–179. |
[29] | Ministerio de Sanidad Servicios Sociales e Igualdad ((2018) ) Orden SSI/1344/2017, de 29 de diciembre, por la que se establecen para el año 2017 los precios unitarios correspondientes a la contraprestación de los servicios llevados a cabo por los centros sociosanitarios, BOE-A-2018-599. Madrid. https://www.boe.es/diario_boe/txt.php?id=BOE-A-2018-599. |
[30] | Presidencia de la Generalitat ((1990) ) DECRETO 215/1990, de 30 de Julio, de promoción y financiación de la atención sociosanitaria. https://portaljuridic.gencat.cat/eli/es-ct/d/1990/07/30/215. |
[31] | Bullich-Marín I , Sánchez-Ferrín P , Cabanes-Duran C , Salvà-Casanovas A ((2017) ) Situación actualRecursos sociosanitarios en Cataluña. Rev Esp Geriatr Gerontol 52: , 342–347. |
[32] | Inoriza JM ((2015) ) Morbilidad, Utilización De Recursos y Costes Sanitarios En la Comarca del Baix Empordà. TDX (Tesis Dr en Xarxa). http://www.tdx.cat/handle/10803/301435. |
[33] | Garre-Olmo J , Flaqué M , Gich J , Pulido TO , Turbau J , Vallmajo N , Viñas M , López-Pousa S ((2009) ) Aclinical registry of dementia based on the principle of epidemiological surveillance. BMC Neurol 9: , 5. |
[34] | Calvo-Perxas L , Osuna MT , Gich J , Eligio-Hernandez E , Linares M , Vinas M , Casas I , Turro-Garriga O , Lopez-Pousa S , Garre-Olmo J , En Representación Del Grupo de Estudio Del Registro de Demencias de Girona ((2012) ) [Clinical and demographic characteristics of the cases of dementia diagnosed in the Health District of Girona throughout the period 2007-2010: Data from the Girona Dementia Registry (ReDeGi)]. Rev Neurol 54: , 399–406. |
[35] | Calvó-Perxas L , Belchí O , Turon-Estrada A , Van Eendenburg C , Linares M , Viñas M , Manzano A , Turró-Garriga O , Vilalta-Franch J , Garre-Olmo J , Alemany B , Coll C , Cots A , Hernández M , Gich J , López-Pousa S , Lozano M , Molins A , Pericot-Nierga I , Ramió-Torrentà L , Robles R , Salavedra J , Serena J , Silva Y , Solano B , Terceño M , Estrada AT , Vilalta-Franch J , Alsina E , Belchí O , de Eugenio R , Hernández E , Flaqué M , Carmona O , Cullell M , Osuna T , Fernández M del M , Van Eendenburg C , Bisbe J , Linares M , Daniel FM , Vallmajó N , Perkal H , Viñas M , Casas I , Turbau J , Cuy JM , Manzano A , Roig AM , Coromina J , Soto MP ((2019) ) Incidence and characteristics of uncommon dementia subtypes: Results from 10 years ofclinical surveillance by the Registry of Dementia of Girona. Alzheimers Dement 15: , 917–926. |
[36] | Turró-Garriga O , Calvó-Perxas L , Vilalta-Franch J , Hernández-Ferrándiz M , Flaqué M , Linares M , Cullell M , Gich J , Casas I , Perkal H , Garre-Olmo J ((2017) ) Adherence to clinical practice guidelines during dementia work-up in a real-world setting: A study from the Registry of Dementias of Girona. J Alzheimers Dis 59: , 997–1007. |
[37] | Inoriza JM , Pérez M , Cols M , Sánchez I , Carreras M , Coderch J ((2013) ) Análisis de la poblacióndiabética de una comarca: Perfil de morbilidad, utilización de recursos, complicaciones y controlmetabólico. Aten Primaria 45: , 461–475. |
[38] | Hughes JS , Averill RF , Eisenhandler J , Goldfield NI , Muldoon J , Neff JM , Gay JC ((2004) ) Clinical Risk Groups (CRGs). Med Care 42: , 81–90. |
[39] | Inoriza JM , Coderch J , Carreras M , Vall-llosera L , García-Goñi M , Lisbona JM , Ibern P ((2009) ) La medida de la morbilidad atendida en una organización sanitaria integrada. Gac Sanit 23: , 29–37. |
[40] | Carreras M , Ibern P , Coderch J , Inoriza JM ((2010) ) Anàlisi de costos per pacient en una organitzaciósanitària integrada. Fulls Econ 39: , 28–37. |
[41] | Carreras M , Ibern P , Coderch J , Sánchez I , Inoriza JM ((2013) ) Estimating lifetime healthcare costs with morbidity data. BMC Health Serv Res 13: , 440. |
[42] | Carreras M , Sánchez-Pérez I , Ibern P , Inoriza JM , Coderch J , Inoriza JM ((2016) ) Analysing the costs ofintegrated care: A case on model selection for chronic care purposes. Int J Integr Care 16: , 10. |
[43] | Carreras M , Ibern P , Inoriza JM ((2018) ) Ageing and healthcare expenditures: Exploring the role of individual health status. Health Econ 27: , 865–876. |
[44] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[45] | Simpson D , Rue H , Riebler A , Martins TG , Sørbye SH ((2017) ) Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. Stat Sci 32: , 319–392. |
[46] | Rue H , Riebler A , Sørbye SH , Illian JB , Simpson DP , Lindgren FK ((2017) ) Bayesian computing with INLA: A review. Annu Rev Stat Its Appl 4: , 395–421. |
[47] | Simpson D , Rue H , Riebler A , Martins TG , Sørbye SH ((2017) ) Penalising model component complexity: A principled, practical approach to constructing priors. Stat Sci 32: , 1–28. |
[48] | Kollerup A , Kjellberg J , Ibsen R ((2022) ) Ageing and health care expenditures: The importance of age per se, steepening of the individual-level expenditure curve, and the role of morbidity. Eur J Health Econ 23: , 1121–1149. |
[49] | Vossius C , Rongve A , Testad I , Wimo A , Aarsland D ((2014) ) The use and costs of formal care in newly diagnosed dementia: A three-year prospective follow-up study. Am J Geriatr Psychiatry 22: , 381–388. |
[50] | Olazarán J , Agüera-Ortiz L , Argimón JM , Reed C , Ciudad A , Andrade P , Dilla T ((2017) ) Costs and qualityof life in community-dwelling patients with Alzheimer’s disease in Spain: Results from the GERAS II observationalstudy. Int Psychogeriatr 29: , 2081–2093. |
[51] | Rapp T , Andrieu S , Chartier F , Deberdt W , Reed C , Belger M , Vellas B ((2018) ) Resource use and cost of Alzheimer’s disease in France: 18-month results from the GERAS Observational Study. Value Health 21: , 295–303. |
[52] | Sopina E , Spackman E , Martikainen J , Waldemar G , Sørensen J ((2019) ) Long-term medical costs of Alzheimer’s disease: Matched cohort analysis. Eur J Health Econ 20: , 333–342. |
[53] | Persson S , Saha S , Gerdtham U , Toresson H , Trépel D , Jarl J ((2022) ) Healthcare costs of dementia diseases before, during and after diagnosis: Longitudinal analysis of 17 years of Swedish register data. Alzheimers Dement 18: , 2560–2569. |
[54] | Kaczynski A , Michalowsky B , Eichler T , Thyrian JR , Wucherer D , Zwingmann I , Hoffmann W ((2019) ) Comorbidity in dementia diseases and associated health care resources utilization and cost. J Alzheimers Dis 68: , 635–646. |
[55] | Fishman PA , White L , Ingraham B , Park S , Larson EB , Crane P , Coe NB ((2020) ) Health care costs of Alzheimer’s and related dementias within a Medicare managed care provider. Med Care 58: , 833–841. |
[56] | Peña-Longobardo LM , Oliva-Moreno J ((2014) ) Caregiver burden in Alzheimer’s disease patients in Spain. J Alzheimers Dis 43: , 1293–1302. |
[57] | Farré M , Kostov B , Haro JM , Cabrera E , Risco E , Alvira Mc , Miguel S , Zabalegui A ((2018) ) Costs and burden associated with loss of labor productivity in informal caregivers of people with dementia. J Occup EnvironMed 60: , 449–456. |
[58] | Leicht H , König H-H , Stuhldreher N , Bachmann C , Bickel H , Fuchs A , Heser K , Jessen F , Köhler M , Luppa M , Mösch E , Pentzek M , Riedel-Heller S , Scherer M , Werle J , Weyerer S , Wiese B , Maier W ((2013) ) Predictors of costs in dementia in a longitudinal perspective. PLoS One 8: , e70018. |
[59] | Gobierno de España ((2006) ) Ley 39/2006, de 14 de diciembre, de Promoción de la Autonomí 1085 a Personal y Atencioó a las personas en situacioó de dependencia, BOE-A-2006-21990. https://www.boe.es/buscar/act.php?id=BOE-A-2006-21990. |
[60] | Pitkala KH , Laakkonen M-LL , Kallio E-LL , Kautiainen H , Raivio MM , Tilvis RS , Strandberg TE , Ohman H ((2021) ) Monetary value of informal caregiving in dementia from a societal perspective. Age Ageing 50: , 861–867. |
[61] | Meijer E , Casanova M , Kim H , Llena-Nozal A , Lee J ((2022) ) Economic costs of dementia in 11 countries in Europe: Estimates from nationally representative cohorts of a panel study. Lancet Reg Health Eur 20: , 100445. |
[62] | Engel L , Ajdukovic M , Bucholc J , McCaffrey N ((2021) ) Valuation of informal care provided to people living with dementia: A systematic literature review. Value Health 24: , 1863–1870. |
[63] | Wittenberg R , Knapp M , Hu B , Comas-Herrera A , King D , Rehill A , Shi C , Banerjee S , Patel A , Jagger C , Kingston A ((2019) ) The costs of dementia in England. Int J Geriatr Psychiatry 34: , 1095–1103. |
[64] | Connolly S ((2020) ) Economics of dementia: A review of methods. Dementia 19: , 1426–1440. |
[65] | Leniz J , Yi D , Yorganci E , Williamson LE , Suji T , Cripps R , Higginson IJ , Sleeman KE ((2021) ) Exploring costs, cost components, and associated factors among people with dementia approaching the end of life: A systematic review. Alzheimers Dement (N Y) 7: , e12198. |
[66] | Sontheimer N , Konnopka A , König H-H ((2021) ) The excess costs of dementia: A systematic review and meta-analysis. J Alzheimers Dis 83: , 333–354. |
[67] | Garre-Olmo J , Garcia-Ptacek S , Calvó-Perxas L , Turró-Garriga O , López-Pousa S , Eriksdotter M ((2016) ) Diagnosis of dementia in the specialist setting: A comparison between the Swedish Dementia Registry (SveDem) and the Registry of Dementias of Girona (ReDeGi). J Alzheimers Dis 53: , 1341–1351. |
[68] | Aranda MP , Kremer IN , Hinton L , Zissimopoulos J , Whitmer RA , Hummel CH , Trejo L , Fabius C ((2021) ) Impact of dementia: Health disparities, population trends, care interventions, and economic costs. J Am Geriatr Soc 69: , 1774–1783. |
[69] | Wolters FJ , Chibnik LB , Waziry R , Anderson R , Berr C , Beiser A , Bis JC , Blacker D , Bos D , Brayne C , Dartigues JF , Darweesh SKL , Davis-Plourde KL , de Wolf F , Debette S , Dufouil C , Fornage M , Goudsmit J , Grasset L , Gudnason V , Hadjichrysanthou C , Helmer C , Ikram MA , Ikram MK , Joas E , Kern S , Kuller LH , Launer L , Lopez OL , Matthews FE , McRae-McKee K , Meirelles O , Mosley TH , Pase MP , Psaty BM , Satizabal CL , Seshadri S , Skoog I , Stephan BCM , Wetterberg H , Wong MM , Zettergren A , Hofman A ((2020) ) Twenty-seven-year time trends in dementia incidence in Europe and the United States: The Alzheimer Cohorts Consortium. Neurology 95: , .e519–e531. |
[70] | Pierse T , Keogh F , O’Neill S ((2020) ) Generating national projections of dementia cases for Ireland using a calibrated macro-simulation model. BMJ Open 10: , e035463. |

