
Safety of Memantine in Combination with Potentially Interactive Drugs in the Real World: A Pharmacovigilance Study Using the Japanese Adverse Drug Event Report (JADER) Database
Abstract
Background:
Memantine, an NMDA receptor antagonist, is used for the treatment of Alzheimer’s disease. There is a caution to refrain from administrating memantine in combination with some specific drugs such as amantadine or dextromethorphan due to potential interactions that might augment the adverse effects of memantine.
Objective:
This notification has not been validated in real-world data, which we aim to address using a large self-reporting database from Japan.
Methods:
We conducted a disproportionality analysis using the Japanese Adverse Drug Event Report (JADER) database reported between April 2004 and March 2019 for detecting the neuropsychiatric adverse event (AE) signals associated with memantine and other potentially interactive drugs including amantadine, dextromethorphan, cimetidine, ranitidine, procainamide, quinidine, acetazolamide, citrate, and bicarbonate. Drug-drug interactions between memantine and these drugs were assessed using multiplicative and additive models.
Results:
There was no statistically robust evidence to support multiplicative or additive interactions between memantine and the aforementioned drugs to increase the reporting of any included neuropsychiatric AEs or AE categories.
Conclusion:
The real-world JADER data did not raise the concern about the interactive increase in the neuropsychiatric AEs in patients with dementia taking memantine in combination with amantadine or dextromethorphan, suggesting there may be no urgent need to prohibit the co-administration of these drugs presently.
INTRODUCTION
Memantine is one of the N-Methyl D-Aspartate (NMDA) receptor antagonists [1, 2] and has been widely used for the treatment of moderate-to-severe Alzheimer’s disease [3, 4]. Its potential neuropsychiatric adverse events include dizziness, somnolence, confusion, imbalance, or seizure [5]. The pharmacological mechanism of memantine suggests several potential drug-drug interactions, which may lead to the increased risk of adverse effects of memantine [5], e.g., amantadine, ketamine, and dextromethorphan are drugs which also act as NMDA receptor antagonists [5, 6], raising concern about the augmented pharmacological effects when co-administered with memantine. In addition, since memantine is excreted by the renal cationic transport system [5, 6], other drugs excreted using the same renal transport system, such as cimetidine, ranitidine, procainamide, quinidine, or quinine, may competitively inhibit the excretion of memantine in urine, leading to the increased plasma memantine level. Third, the excretion of memantine in urine is known to depend on the urinary pH [6, 7], so that drugs alkalinizing urine such as acetazolamide, sodium/potassium citrate, or sodium bicarbonate may cause reduced renal excretion of memantine. Based on these presumed pharmacological mechanisms, the EMA product information of memantine recommends avoiding co-administration of memantine with these potentially interactive drugs [5]. In Japan, although not prohibited, the Pharmaceuticals and Medical Devices Agency (PMDA) recommends careful administration of memantine in patients on the above-mentioned drugs [8].
Meanwhile, these cautions/notifications in drug use have not been validated in real-world data, even though indications of these potentially interactive drugs are common in the elderly population. For example, amantadine is usually prescribed for Parkinson’s disease, dextromethorphan for cough symptoms, procainamide and quinidine for arrhythmia, acetazolamide for acidosis or epilepsy, or citrate and sodium bicarbonate for the prevention of gout. Multiple diseases as mentioned and dementia is not rare in elderly patients, and therefore, it might be important for clinicians to know to what degree these potentially interactive drugs may additionally increase the adverse effect of memantine when co-administrated together. In this study, we aimed to validate this issue by a pharmacovigilance approach using a large Japanese adverse event (AE) self-reporting database. We used both the multiplicative model and additive models to examine drug-drug interactions between memantine and the above-mentioned drugs if any.
METHODS
Data acquisition and preprocessing
This was a retrospective pharmacovigilance study using the Japanese Adverse Drug Event Report (JADER) database that was provided by the Pharmaceuticals and Medical Devices Agency (PMDA). This study was approved by the University of Tokyo Graduate School of Medicine institutional ethics committee [ID: 11754-(1)]. This work was conducted in accordance with the ethical standards laid down in the Declaration of Helsinki, 1964. Informed consent was not required for this type of study. The database contains more than 500,000 case reports with potential AEs of drugs reported in Japan since 2004. We downloaded the data of 566,698 patient records reported between 2004 April and 2019 March after obtaining permission from the PMDA website (https://www.pmda.go.jp) in May 2019. The JADER database consists of four-component data tables as follows [9–11]: 1), ‘demo’, which provides the ID, sex, age in decades (e.g., ‘40s, ‘60s), reporting year, reporting route (following clinical trial or spontaneous reporting), and reporters’ demographics (like medical doctor, pharmacist, lawyer, consumer) for each unique case; 2), ‘reac’, which contains all adverse reactions potentially due to drug use by each patient; 3) ‘drug’, which includes the name, dose, indications, and date of administration and discontinuation of all the possibly associated drugs; and 4) ‘hist’, which contains the primary illness or medical history of each patient. In the ‘drug’ table, the suspected causality of each drug for the AEs is classified as ‘suspected’, ‘concomitant’, or ‘interacting’: We included all these drug categories since the accurate estimation of the causality for each drug was not always possible. Duplicated AEs in the ‘reac’ table reported from the same case ID, or the duplicated drug names in the ‘drug’ table reported from the same case ID, were deleted.
Next, since the JADER database infrequently contains potentially duplicated records derived from the same patient but reported by different reporters (e.g., both by the hospital doctor and the pharmaceutical company) with different case IDs, we excluded the reported AEs in the ‘reac’ table of which all the following data features matched completely: name of AE, outcome, date of AE onset, age in decades, sex, body weight, body height, reporting year, and the reported quarter (Q1–Q4). In addition, we excluded the reported drug information records in the ‘drug’ table if all the following features matched completely: drug name, date of drug administration and discontinuation, age in decades, sex, body weight, body height, reporting year, and the reported quarter (Q1–Q4).
Database search
In the JADER database, the AEs and the disease indications are given by the Preferred Terms (PTs), as determined by the Medical Dictionary for Regulatory Activities/Japanese version (MedDRA/J version. 22; https://www.pmrj.jp/jmo/php/indexe.php) in Japanese. We used the neurologically- or psychiatrically-related AE terms as listed in Supplementary Table 1 to search for cases treated with memantine and presenting with any of the neuropsychiatric AEs. Besides, since some neuropsychiatric AEs resemble with each other (e.g., anger and agitation, or somnolence and depressed level of consciousness), we arbitrarily defined the AE categories to summarize these AEs as provided in Supplementary Table 1. Briefly, the defined AE category of ‘AMS’, which denotes altered mental status, includes MedDRA PTs of ‘altered state of consciousness’, ‘somnolence’, ‘depressed level of consciousness’, ‘coma’, ‘stupor’, ‘consciousness fluctuating’, ‘delirium’, ‘disorientation’, ‘confusional state’, ‘delusion’, ‘abnormal behavior’, ‘anger’, ‘agitation’, ‘hallucination’, and ‘hallucination, visual’. We also defined the AE category of ‘LOC’, loss of consciousness, composed of MedDRA PTs of ‘loss of consciousness’ and ‘syncope’, since it can sometimes be indistinguishable from an epileptic seizure of unknown etiology. In addition, the category of ‘dizziness’ was defined to include MedDRA PTs of ‘dizziness’ and ‘dizziness postural’.
Next, we classified each reported case [12, 13] depending on the binomial factors—with/without exposure to the drugs of interest, and with/without the development of each AE or AE category of interest, regardless the timing of drug administration or AE development. We included the following drugs: memantine, amantadine (used for Parkinson’s disease or influenza), dextromethorphan, cimetidine, ranitidine, quinidine, procainamide, oral sodium bicarbonate, acetazolamide, and citrate (potassium citrate and sodium citrate, used for gout prevention). A combination of dextromethorphan and quinidine was not included in the analysis because its use is not approved in Japan.
Statistical analyses
All statistical analyses were performed using R software (version 3.5.1). For each included drug, we calculated the reporting odds ratio (ROR) to identify the drugs potentially associated with the development of each AE term/category. The (crude) ROR was calculated by a 2×2 contingency table [12, 13], where all the reports were classified by two factors for each AE term/category and each drug as described above. When the lower 95%confidential interval (CI) of ROR was > 1, the AE term/category was considered to be significantly highly reported following the use of the drug of interest as compared to following the use of all other drugs.
To assess the drug-drug interactions between memantine and other included drugs, we used two different models, the multiplicative model and the additive model [14]. The former model was calculated using multivariate binomial logistic model, with the following equation [12]:
(1)
where, memantine denotes the binomial exposure state of each case (= 0 if not used, and = 1 if used) to memantine, another drug denotes the binomial exposure to another drug of interest, and AChEI denotes the binomial concurrent exposure to any acetylcholinesterase inhibitors (AChEIs; i.e., donepezil, galantamine, or rivastigmine). We included the exposure status of the AChEIs since dementia patients on memantine are often co-administered with AChEIs. Because few patients received≥3 of these drugs simultaneously (for example memantine +amantadine + cimetidine), we only considered the drug-drug interactions model between memantine and another single drug. We did not calculate the above interactions for drugs that were not co-administered with memantine in any of the cases presenting with neuropsychiatric AEs of interest. Besides, since we adjusted age-in-decade and sex simultaneously, we excluded neuropsychiatric AEs reported by < 30 cases. Furthermore, we excluded the AEs of which the crude ROR was not significantly high with memantine as we focused on the further multiplicative increase in the reporting of neuropsychiatric AE due to interactions.
Next, for evaluating the additive model, we calculated the ‘relative excess risk due to interactions (RERI) approximated by the reporting odds ratio (ROR). When considering interactions between drug A and drug B for the development of a certain AE, the RERI was obtained by the following equation [14, 15]:
(2)
where ROR11 is the ROR of taking both drug A and drug B for developing the AE of interest, ROR10 is the ROR of taking drug A alone, ROR01 is the ROR of taking drug B alone, and ROR00 is the ROR of taking neither drug A nor drug B. To obtain the above-defined RERI, its 95%CI and the p-value, we used the additive model function implemented in R [16], which utilizes the adjusted ROR obtained from the multiplicative model of the above equation (1). This function automatically recodes the binary exposure status of which the original ROR (ROR01 or ROR10) was < 1. Since we considered the exposure status of two drugs for the additive interaction to increase the reporting of AEs, we regarded the drug-drug interactions as non-significant if this recoding imputation was conducted with the drug-drug combination.
Lastly, we also compared the frequency of each AE in cases with AChEI and with memantine, under exposure to other drugs of interest. This is because whether to use AChEI or memantine when patients had already been prescribed with the other drugs (i.e., amantadine, dextromethorphan, cimetidine, ranitidine, and sodium bicarbonate) might be another matter of interest for clinicians. This was simply conducted by the 2-by-2 contingency table as shown in Supplementary Table 2A where each case was determined whether the case includes the AE of interest, and whether the case is exposed to each combination of medications. Then we calculated p-value in Fisher’s exact test to examine whether the AE frequency differs between each combination group.
RESULTS
In total, 611,965 adverse events were reported from 395,032 unique patients following the use of 562,976 ‘suspected’ drugs, 1,175,338 ‘concurrent’ drugs, and 5,195 ‘interacted’ drugs.
There were 985 reported patients who received memantine, among whom 266 (27.0%) reported neuropsychiatric AE of our interest (Table 1). Patients with memantine usage were predominantly women with a median age-in-decades of the ‘80s (IQR: ‘70s–‘80s). Among the other included drugs, 359/1,585 (22.6%) cases with amantadine, 178/2,348 (7.6%) cases with dextromethorphan, 54/1,288 (4.2%) cases with cimetidine, 174/4,096 (4.2%) cases with ranitidine, 0/17 (0%) cases with quinidine, 8/87 (9.2%) cases with procainamide, 41/738 (5.6%) cases with peroral sodium bicarbonate, 39/638 (6.1%) cases with acetazolamide, and 34/870 (3.9%) cases with citrate (potassium citrate and sodium citrate) reported any neuropsychiatric AEs of interest.
Table 1
Basic demographic characteristics of memantine and the other included drugs
| Drugs | Total no. of cases | Cases with any AE of our interest | Sex (male, %) | Median age (y) (IQR) | Suspected drug involvement | ||
| Suspected | Concomitant | Interacting | |||||
| Memantine | 985 | 266 | 427 (43.35%) | 80 (70–80) | 741 | 845 | 0 |
| Amantadine | 1,585 | 359 | 771 (48.64%) | 70 (60–80) | 1,469 | 1,500 | 12 |
| Dextromethorphan | 2,348 | 178 | 1181 (50.3%) | 60 (40–70) | 355 | 3,321 | 6 |
| Cimetidine | 1,288 | 54 | 644 (50%) | 60 (50–70) | 180 | 1,823 | 9 |
| Ranitidine | 4,096 | 174 | 1993 (48.66%) | 60 (50–70) | 775 | 5,985 | 13 |
| Quinidine | 17 | 0 | 13 (76.47%) | 70 (32.5–77.5) | 13 | 10 | 0 |
| Procainamide | 87 | 8 | 53 (60.92%) | 70 (60–80) | 38 | 101 | 0 |
| Bicarbonate | 738 | 41 | 445 (60.3%) | 60 (50–70) | 71 | 1,212 | 0 |
| Acetazolamide | 638 | 39 | 349 (54.7%) | 50 (30–70) | 219 | 1,213 | 1 |
| Potassium citrate and sodium citrate | 870 | 34 | 692 (79.54%) | 60 (50–70) | 137 | 1,296 | 0 |
| Memantine and amantadine | 22 | 6 | 10 (45.45%) | 80 (70–80) | |||
| Memantine and dextromethorphan | 5 | 2 | 1 (20%) | 90 (80–90) | |||
| Memantine and cimetidine | 4 | 4 | 1 (25%) | 80 (77.5–80) | |||
| Memantine and ranitidine | 7 | 2 | 2 (28.57%) | 80 (75–85) | |||
| Memantine and procainamide | 0 | 0 | - | - | |||
| Memantine and quinidine | 0 | 0 | - | - | |||
| Memantine and bicarbonate | 2 | 1 | 1 (50%) | 85 (82.5–87.5) | |||
| Memantine and acetazolamide | 1 | 0 | 0 (0%) | 70 (70–70) | |||
| Memantine and citrate | 3 | 0 | 2 (66.67%) | 80 (75–85) | |||
AE, adverse event; IQR, interquartile range.
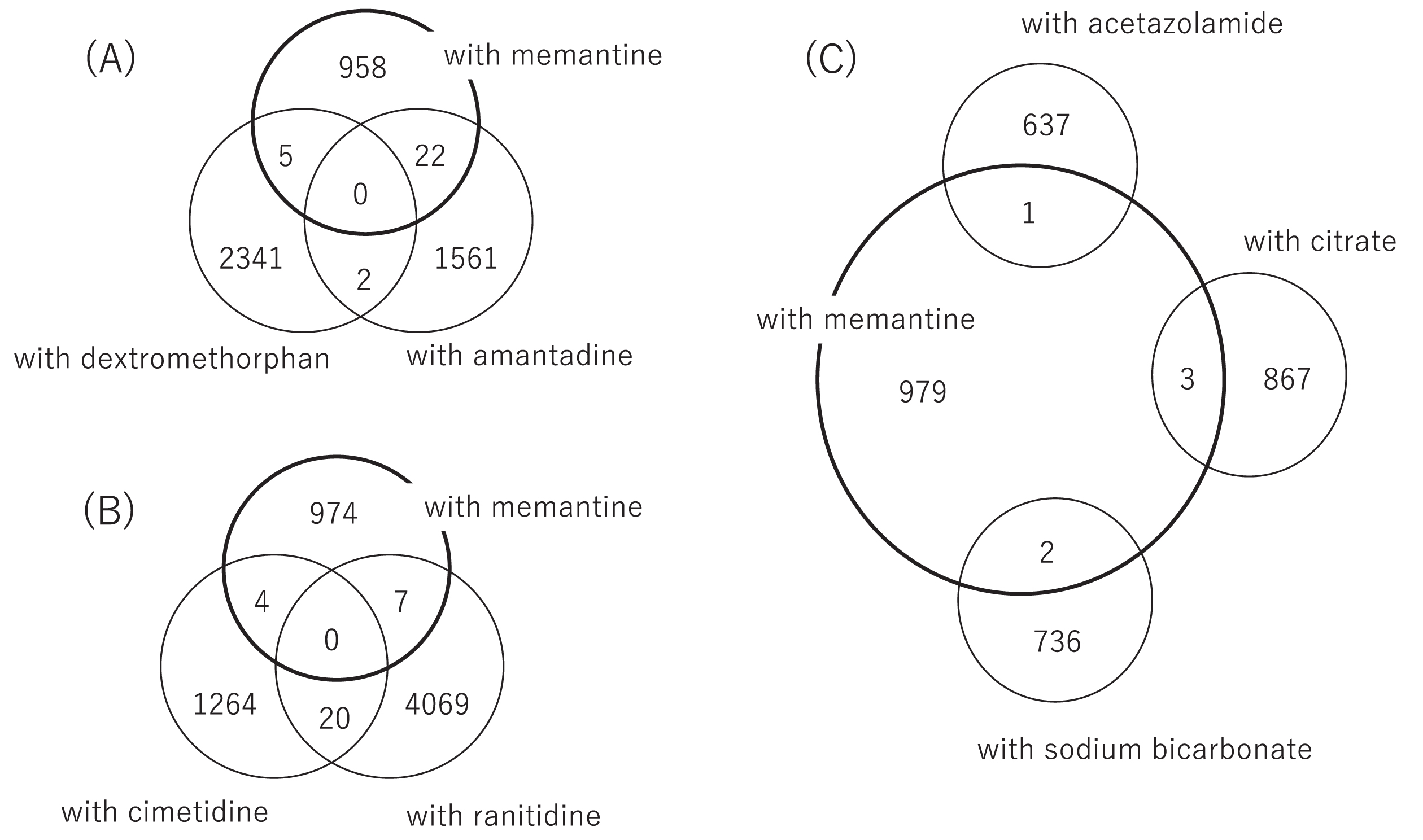
The number of cases taking memantine in combination with other drugs was relatively small (Fig. 1), and there were no cases who were administered with memantine in combination with procainamide, quinidine, acetazolamide, or citrate. The combination of memantine and amantadine was most frequently observed (n = 22) (A), followed by a combination of memantine and ranitidine (n = 7) (B), memantine and dextromethorphan (n = 5) (A), and memantine and cimetidine (n = 4) (B). There were few cases administrated with multiple types of these drugs. In addition, there were no cases with any neuropsychiatric AEs of interest and with overlapped prescription of memantine and acetazolamide, or memantine and citrate. Due to the lack of eligible cases, we excluded quinidine, procainamide, acetazolamide, and citrate from the following analysis.
Fig. 1
Cases overlapping between exposure to memantine and other drugs of interest. The number of cases taking memantine in combination with other drugs of interest was relatively small, and there were no patients who were co-administered with memantine plus procainamide, quinidine, acetazolamide, or citrate. The combination of memantine and amantadine was most frequently observed (n = 22) (A), followed by the combination of memantine plus ranitidine (n = 7) (B), memantine plus dextromethorphan (n = 5) (A), memantine plus cimetidine (n = 4) (B), and so on. There were few cases administrated with multiple kinds of these drugs.
We calculated the crude ROR for each neuropsychiatric AE following the use of memantine, amantadine, dextromethorphan (Table 2A), cimetidine, ranitidine, and sodium bicarbonate (Table 2B). In Table 2A and 2B, the crude ROR and its 95%CI and the number of reports with each drug and their percentage to all the JADER reports with the drug are provided. The largest number of neuropsychiatric AE categories/terms showed significantly high crude ROR with the use of memantine, followed by amantadine and dextromethorphan. In particular, memantine, amantadine, dextromethorphan, and sodium bicarbonate had significantly high crude ROR for the ‘AMS’ category.
Table 2
Crude ROR of the defined AE categories or AE terms following the usage of each drug. Crude ROR of AEs following the use of memantine, amantadine, or dextromethorphan
| Memantine | Amantadine | Dextromethorphan | |||||
| Frequency (%) (%) | Crude ROR (95%CI) | Frequency (%) | Crude ROR (95%CI) | Frequency (%) | Crude ROR (95%CI) | ||
| Defined categories | AMS | 131/10,804 (1.21%) | 5.51 (4.54–6.64) | 287/10,804 (2.66%) | 8.05 (7.05–9.17) | 104/10,804 (0.96%) | 1.65 (1.34–2.02) |
| Fall | 36/1,317 (2.73%) | 11.63 (8.06–16.3) | 24/1,317 (1.82%) | 4.66 (2.97–6.99) | 8/1,317 (0.61%) | 1.02 (0.44–2.02) | |
| Seizure | 44/3,671 (1.2%) | 5.03 (3.63–6.82) | 59/3,671 (1.61%) | 4.17 (3.15–5.43) | 32/3,671 (0.87%) | 1.48 (1.01–2.1) | |
| LOC | 59/3,383 (1.74%) | 7.49 (5.64–9.77) | 19/3,383 (0.56%) | 1.41 (0.84–2.21) | 42/3,383 (1.24%) | 2.12 (1.52–2.88) | |
| Dizziness | 35/2,012 (1.74%) | 7.31 (5.04–10.27) | 12/2,012 (0.6%) | 1.49 (0.77–2.62) | 12/2,012 (0.6%) | 1 (0.52–1.76) | |
| MedDRA terms | Altered state of consciousness | 37/3,422 (1.08%) | 4.5 (3.15–6.27) | 62/3,422 (1.81%) | 4.73 (3.6–6.11) | 22/3,422 (0.64%) | 1.08 (0.68–1.65) |
| Somnolence | 29/1,078 (2.69%) | 11.36 (7.53–16.53) | 13/1,078 (1.21%) | 3.05 (1.61–5.25) | 5/1,078 (0.46%) | 0.78 (0.25–1.83) | |
| Depressed level of consciousness | 19/1,667 (1.14%) | 4.68 (2.8–7.38) | 12/1,667 (0.72%) | 1.81 (0.93–3.17) | 14/1,667 (0.84%) | 1.42 (0.77–2.39) | |
| Coma | 5/305 (1.64%) | 6.7 (2.15–15.86) | 2/305 (0.66%) | 1.64 (0.2–5.98) | 1/305 (0.33%) | 0.55 (0.01–3.09) | |
| Stupor | 1/103 (0.97%) | 3.92 (0.1–22.4) | 2/103 (1.94%) | 4.92 (0.59–18.27) | 0/103 (0%) | NA | |
| Consciousness fluctuating | 1/5 (20%) | 100.29 (2.03–993.56) | 0/5 (0%) | NA | 0/5 (0%) | NA | |
| Delirium | 17/1,636 (1.04%) | 4.26 (2.46–6.87) | 44/1,636 (2.69%) | 7.03 (5.06–9.52) | 13/1,636 (0.79%) | 1.34 (0.71–2.31) | |
| Disorientation | 1/260 (0.38%) | 1.55 (0.04–8.7) | 10/260 (3.85%) | 9.98 (4.72–18.72) | 3/260 (1.15%) | 1.95 (0.4–5.78) | |
| Confusional state | 3/338 (0.89%) | 3.59 (0.74–10.62) | 10/338 (2.96%) | 7.61 (3.61–14.21) | 4/338 (1.18%) | 2 (0.54–5.19) | |
| Delusion | 11/454 (2.42%) | 10.03 (4.96–18.21) | 25/454 (5.51%) | 14.68 (9.37–22.04) | 1/454 (0.22%) | 0.37 (0.01–2.07) | |
| Abnormal behavior | 6/932 (0.64%) | 2.6 (0.95–5.71) | 13/932 (1.39%) | 3.53 (1.87–6.09) | 29/932 (3.11%) | 5.43 (3.6–7.87) | |
| Anger | 4/68 (5.88%) | 25.1 (6.63–67.65) | 1/68 (1.47%) | 3.71 (0.09–21.4) | 0/68 (0%) | NA | |
| Agitation | 12/399 (3.01%) | 12.54 (6.4–22.28) | 18/399 (4.51%) | 11.85 (6.93–19.06) | 5/399 (1.25%) | 2.12 (0.69–5.01) | |
| Hallucination | 4/1117 (0.36%) | 1.44 (0.39–3.71) | 111/1117 (9.94%) | 29.38 (23.77–36.01) | 15/1117 (1.34%) | 2.28 (1.27–3.79) | |
| Hallucination, visual | 3/381 (0.79%) | 3.18 (0.65–9.4) | 41/381 (10.76%) | 30.7 (21.56–42.73) | 3/381 (0.79%) | 1.33 (0.27–3.91) | |
| Fall | 36/1317 (2.73%) | 11.63 (8.06–16.3) | 24/1317 (1.82%) | 4.66 (2.97–6.99) | 8/1317 (0.61%) | 1.02 (0.44–2.02) | |
| Seizure | 44/3671 (1.2%) | 5.03 (3.63–6.82) | 59/3671 (1.61%) | 4.17 (3.15–5.43) | 32/3671 (0.87%) | 1.48 (1.01–2.1) | |
| Loss of consciousness | 46/2685 (1.71%) | 7.27 (5.27–9.8) | 9/2685 (0.34%) | 0.83 (0.38–1.59) | 34/2685 (1.27%) | 2.16 (1.49–3.04) | |
| Syncope | 13/721 (1.8%) | 7.43 (3.92–12.85) | 10/721 (1.39%) | 3.51 (1.67–6.51) | 9/721 (1.25%) | 2.12 (0.96–4.05) | |
| Dizziness | 35/1940 (1.8%) | 7.58 (5.23–10.66) | 11/1940 (0.57%) | 1.42 (0.71–2.55) | 12/1940 (0.62%) | 1.04 (0.54–1.83) | |
| Dizziness postural | 1/110 (0.91%) | 3.67 (0.09–20.95) | 1/110 (0.91%) | 2.28 (0.06–12.98) | 0/110 (0%) | NA | |
Table 2B
Crude ROR of the AEs following the use of cimetidine, ranitidine, or sodium bicarbonate
| Cimetidine | Ranitidine | Sodium bicarbonate | |||||
| Frequency (%) | Crude ROR (95%CI) | Frequency (%) | Crude ROR (95%CI) | Frequency (%) | Crude ROR (95%CI) | ||
| Defined categories | AMS | 29/10,804 (0.27%) | 0.82 (0.55–1.18) | 97/10,804 (0.9%) | 0.86 (0.7–1.05) | 31/10,804 (0.29%) | 1.56 (1.05–2.24) |
| Fall | 6/1,317 (0.46%) | 1.4 (0.51–3.07) | 8/1,317 (0.61%) | 0.58 (0.25–1.15) | 1/1,317 (0.08%) | 0.41 (0.01–2.27) | |
| Seizure | 9/3,671 (0.25%) | 0.75 (0.34–1.43) | 25/3,671 (0.68%) | 0.65 (0.42–0.97) | 8/3,671 (0.22%) | 1.17 (0.5–2.32) | |
| LOC | 10/3,383 (0.3%) | 0.91 (0.43–1.67) | 28/3,383 (0.83%) | 0.8 (0.53–1.15) | 2/3,383 (0.06%) | 0.31 (0.04–1.14) | |
| Dizziness | 6/2,012 (0.3%) | 0.91 (0.33–2) | 30/2,012 (1.49%) | 1.45 (0.97–2.08) | 1/2,012 (0.05%) | 0.26 (0.01–1.48) | |
| MedDRA terms | Altered state of consciousness | 9/3,422 (0.26%) | 0.8 (0.37–1.53) | 42/3,422 (1.23%) | 1.19 (0.85–1.61) | 20/3,422 (0.58%) | 3.2 (1.94–4.99) |
| Somnolence | 5/1,078 (0.46%) | 1.43 (0.46–3.35) | 5/1,078 (0.46%) | 0.44 (0.14–1.04) | 3/1,078 (0.28%) | 1.49 (0.31–4.39) | |
| Depressed level of consciousness | 4/1,667 (0.24%) | 0.73 (0.2–1.89) | 17/1,667 (1.02%) | 0.98 (0.57–1.58) | 0/1,667 (0%) | NA | |
| Coma | 0/305 (0%) | NA | 2/305 (0.66%) | 0.63 (0.08–2.3) | 1/305 (0.33%) | 1.76 (0.04–9.9) | |
| Stupor | 0/103 (0%) | NA | 0/103 (0%) | NA | 0/103 (0%) | NA | |
| Consciousness fluctuating | 0/5 (0%) | NA | 0/5 (0%) | NA | 0/5 (0%) | NA | |
| Delirium | 5/1,636 (0.31%) | 0.94 (0.3–2.2) | 16/1,636 (0.98%) | 0.94 (0.54–1.54) | 4/1,636 (0.24%) | 1.31 (0.36–3.38) | |
| Disorientation | 0/260 (0%) | NA | 1/260 (0.38%) | 0.37 (0.01–2.07) | 3/260 (1.15%) | 6.26 (1.28–18.56) | |
| Confusional state | 2/338 (0.59%) | 1.82 (0.22–6.64) | 2/338 (0.59%) | 0.57 (0.07–2.07) | 1/338 (0.3%) | 1.59 (0.04–8.93) | |
| Delusion | 1/454 (0.22%) | 0.67 (0.02–3.78) | 2/454 (0.44%) | 0.42 (0.05–1.53) | 0/454 (0%) | NA | |
| Abnormal behavior | 2/932 (0.21%) | 0.66 (0.08–2.38) | 2/932 (0.21%) | 0.2 (0.02–0.74) | 0/932 (0%) | NA | |
| Anger | 0/68 (0%) | NA | 0/68 (0%) | NA | 0/68 (0%) | NA | |
| Agitation | 0/399 (0%) | NA | 4/399 (1%) | 0.97 (0.26–2.5) | 0/399 (0%) | NA | |
| Hallucination | 1/1,117 (0.09%) | 0.27 (0.01–1.53) | 8/1,117 (0.72%) | 0.69 (0.3–1.36) | 0/1,117 (0%) | NA | |
| Hallucination, visual | 1/381 (0.26%) | 0.8 (0.02–4.52) | 4/381 (1.05%) | 1.01 (0.27–2.62) | 0/381 (0%) | NA | |
| Fall | 6/1,317 (0.46%) | 1.4 (0.51–3.07) | 8/1,317 (0.61%) | 0.58 (0.25–1.15) | 1/1,317 (0.08%) | 0.41 (0.01–2.27) | |
| Seizure | 9/3,671 (0.25%) | 0.75 (0.34–1.43) | 25/3,671 (0.68%) | 0.65 (0.42–0.97) | 8/3,671 (0.22%) | 1.17 (0.5–2.32) | |
| Loss of consciousness | 9/2,685 (0.34%) | 1.03 (0.47–1.96) | 18/2,685 (0.67%) | 0.64 (0.38–1.02) | 2/2,685 (0.07%) | 0.4 (0.05–1.44) | |
| Syncope | 1/721 (0.14%) | 0.42 (0.01–2.37) | 10/721 (1.39%) | 1.34 (0.64–2.49) | 0/721 (0%) | NA | |
| Dizziness | 6/1,940 (0.31%) | 0.95 (0.35–2.07) | 30/1,940 (1.55%) | 1.5 (1.01–2.16) | 1/1,940 (0.05%) | 0.27 (0.01–1.54) | |
| Dizziness postural | 0/110 (0%) | NA | 0/110 (0%) | NA | 0/110 (0%) | NA | |
The significantly high RORs (lower 95%CI > 1) of the drug-AE combinations are shown in bold. AE, adverse event; ROR, reporting odds ratio; CI, confidence interval; LOC, loss of consciousness; AMS, altered mental status.
Next, we conducted a drug-drug interaction assessment. In the multiplicative model, we calculated the adjusted ROR of the interactions between memantine and another included drug for the development of eligible neuropsychiatric AEs. In the additive model, we calculated the RERIROR and its p-value as shown in Table 3. In the interaction model of memantine and amantadine (model 1), the interaction did not show a significantly higher reporting in the multiplicative model (lower adjusted ROR≤1) or the additive model (RERIROR p-value≥0.05) for any of the eligible neuropsychiatric AEs. Similarly, a non-significant higher reporting was observed with the interaction between memantine and dextromethorphan (model 2), memantine and ranitidine (model 4), and memantine and sodium bicarbonate (model 5). Meanwhile, in the multiplicative interaction between memantine and cimetidine (model 3), the interaction showed a significantly and prominently higher ROR as compared to that of memantine [for example, for ‘AMS’ category the memantine ROR was 2.86 (95%CI: 2.31–3.52) while the interaction ROR was 29.7 (95%CI: 3.3–641.1)]. In the additive model, however, this increased interaction was not replicated since the binary recoding was required and the RERI p-value was non-significant (p = 1.000).
Table 3A
Multiplicative and additive effects of the interactions between memantine and other drugs. Interactions between memantine and amantadine (model 1), dextromethorphan (model 2), or cimetidine (model 3)
| Model 1: Memantine×amantadine | Model 2: memantine×dextromethorphan | Model 3: memantine×cimetidine | |||||||||||
| Memantine | Amantadine | Interaction | Memantine | Dextromethorphan | Interaction | Memantine | Cimetidine | Interaction | |||||
| Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | RERI (95%CI), p | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | RERI, p | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | RERI, p | ||
| Defined categories | AMS | 3.18(2.56–3.91) | 7.61 (6.6–8.73) | 0.14 (0.03–0.43) | –6.5 [(–10.8)–(2.2)], | 2.94 (2.37–3.61) | 1.55 (1.23–1.91) | 0.92 (0.05–6.85) | 0.71 [(–8.7)–(10.1)], | 2.86 (2.31–3.52) | 0.82 (0.54–1.18) | 29.7 (3.32–641.1) | –81.8 [(–101.5)–(62.1)]a |
| p = 1.000 | p = 0.44 | p = 1.00 | |||||||||||
| Fall | 4.87 (3.24–7.09) | 3.62 (2.29–5.41) | 0.36 (0.02–1.98) | –1.1 [(–14.2)–(12)], | 4.58 (3.05–6.68) | 0.94 (0.29–2.2) | 8.99 (0.38–98.6) | –36.4 [(–55.8)–(–17.0)]b, | |||||
| p = 0.570 | p = 1.00 | ||||||||||||
| Seizure | 3.87 (2.65–5.5) | 4.74 (3.47–6.3) | 1.02 (0.26–3.22) | 11.1 [(–10.4)–(32.6)], | 3.83 (2.65–5.4) | 1.48 (0.98–2.14) | 3.7 (0.18–28.12) | 16.7 [(–30.1)–(63.5)], | |||||
| p = 0.16 | p = 0.24 | ||||||||||||
| LOC | 3.89 (2.83–5.25) | 1.22 (0.71–1.93) | 0.59 (0.03–3.26) | –1.33 [(–7.1) –(4.4)], | 3.79 (2.75–5.11) | 0.88 (0.42–1.6) | 5.95 (0.26–59.15) | –18.4 [(–30.6)–(6.2)]b, | |||||
| p = 0.68 | p = 1.00 | ||||||||||||
| Dizziness | 6.05 (3.99–8.88) | 1.5 (0.78–2.59) | 0.87 (0.05–5.02) | 1.33 [(–14.7)–(17.4)], | |||||||||
| p = 0.44 | |||||||||||||
| MedDRA terms | Altered state of consciousness | 2.47 (1.67–3.53) | 4.23 (3.2–5.48) | 0.65 (0.1–2.47) | 1.08 [(–8.95)–(11.1)], | 2.29 (1.55–3.28) | 0.65 (0.28–1.26) | 43.06 (4.36–432.17) | –95.8 [(–133.3)–(58.2)]b, | ||||
| p = 0.42 | p = 1.00 | ||||||||||||
| Somnolence | 9.3 (5.75–14.53) | 3.15 (1.62–5.45) | 0.48 (0.03–2.84) | 2.7 [(–26.1)–(31.5)], | |||||||||
| p = 0.43 | |||||||||||||
| Depressed level of consciousness | 2.63 (1.51–4.29) | 1.46 (0.8–2.41) | 7.57 (0.36–62.19) | 25.8 [(–39.0)–(90.6)], | 2.61 (1.5–4.26) | 0.57 (0.14–1.49) | 29.51 (1.21–360.33) | –73.1 [(–114.1)–(32.1)]b, | |||||
| p = 0.22 | p = 1.00 | ||||||||||||
| Agitation | 5.08 (2.3–10.36) | 13.48 (7.63–22.18) | 0.27 (0.01–1.82) | 0.81 [(–38.3)–(39.9)], | |||||||||
| p = 0.48 | |||||||||||||
| Fall | 4.87 (3.24–7.09) | 3.62 (2.29–5.41) | 0.36 (0.02–1.98) | –1.1 [(–14.2)–(12)], | 4.58 (3.05–6.68) | 0.94 (0.29–2.2) | 8.99 (0.38–98.63) | –36.4 [(–55.8)–(–17.0)]b, | |||||
| p = 0.57 | p = 1.00 | ||||||||||||
| Seizure | 3.87 (2.65–5.5) | 4.74 (3.47–6.3) | 1.02 (0.26–3.22) | 11.12 [(–10.4)–(32.6)], | 3.83 (2.65–5.4) | 1.48 (0.98–2.14) | 3.7 (0.18–28.12) | 16.7 [(–30.1)–(63.5)], | |||||
| p = 0.16 | p = 0.24 | ||||||||||||
| Loss of consciousness | 4.75 (3.3–6.68) | 0.7 (0.3–1.37) | 1.37 (0.07–8.57) | –0.16 [(–14.0)–(13.7)]a, | 4.67 (3.25–6.57) | 0.99 (0.45–1.85) | 7.02 (0.32–67.28) | –28.1 [(–43.8)–(–12.4)]b, | |||||
| p = 0.51 | p = 1.00 | ||||||||||||
| Dizziness | 6.09 (4.01–8.94) | 1.4 (0.7–2.47) | 0.94 (0.05–5.5) | 1.49 [(–14.7)–(17.7)], | |||||||||
| p = 0.43 | |||||||||||||
aReference was recoded automatically as memantine = 0 and amantadine = 1 (= 0 by default). bReference was recoded automatically as memantine = 0 and cimetidine = 1 (= 0 by default). The significantly high RORs (lower 95%CI > 1) of the drug-AE combinations are shown in bold. Non-eligible AE-drug combinations for which we could not compute the adjusted ROR due to a limited number of eligible cases with the AE-memantine combination are left blank. LOC, loss of consciousness; AMS, altered mental status.
Table 3B
Interactions between memantine and ranitidine (model 4), or bicarbonate (model 5)
| Model 4: memantine×ranitidine | Model 5: memantine×bicarbonate | ||||||||
| Memantine | Ranitidine | Interaction | Memantine | Bicarbonate | Interaction | ||||
| Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | RERI, p | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | Adjusted ROR (95%CI) | RERI, p | ||
| Defined categories | AMS | 2.94 (2.37–3.61) | 0.91 (0.74–1.11) | 0.91 (0.05–5.68) | 0.45 [(–6.47)–(7.37)]a, | ||||
| p = 0.45 | |||||||||
| Fall | |||||||||
| Seizure | 3.81 (2.64–5.37) | 1.21 (0.48–2.47) | 25.23 (0.78–825.4) | 112.3 [(–240.1)–(464.8)], | |||||
| p = 0.27 | |||||||||
| LOC | |||||||||
| Dizziness | 5.96 (3.93–8.75) | 1.45 (0.98–2.05) | 2.8 (0.14–18.04) | 17.7 [(–33.4)–(69.3)], | |||||
| p = 0.25 | |||||||||
| MedDRA terms | Altered state of consciousness | ||||||||
| Somnolence | |||||||||
| Depressed level of consciousness | 2.63 (1.51–4.29) | 0.95 (0.55–1.49) | 7.43 (0.37–51.74) | –16.8 | |||||
| [(–28.4)–(–5.3)]a, | |||||||||
| p = 1.00 | |||||||||
| Agitation | |||||||||
| Fall | |||||||||
| Seizure | 3.81 (2.64–5.37) | 1.21 (0.48–2.47) | 25.23 (0.78–825.4) | 112.3 [(–240.1)–(464.8)], | |||||
| p = 0.27 | |||||||||
| Loss of consciousness | |||||||||
| Dizziness | 6.01 (3.96–8.83) | 1.5 (1.01–2.12) | 2.68 (0.14–17.28) | ||||||
| 17.7 [(–34.0)–(69.4)], | |||||||||
| p = 0.25 | |||||||||
aReference was recoded automatically as memantine = 0 and ranitidine = 1 (= 0 by default). The significantly high RORs (lower 95%CI > 1) of the drug-AE combinations are shown in bold. Non-eligible AE-drug combinations for which we could not compute the adjusted ROR due to a limited number of eligible cases with the AE-memantine combination are left blank. LOC, loss of consciousness; AMS, altered mental status.
And lastly, results p-value of Fisher’s exact test are summarized in Supplementary Table 2B, where there were no significant tests (p < 0.05) for any of combinations 1–5 or any AEs examined. This means that there was no significant increase in the reporting of neuropsychiatric AEs following the use of memantine in comparison with any AChEI drugs, in combination with other drugs of examined.
DISCUSSION
In this study, we investigated the reports of neuropsychiatric AEs developed following treatment with memantine and the potentially interactive drugs. Our study has a major strength that it is a pharmacovigilance study based on a self-reporting database reported from a large number of Japanese patients in the real world, and also has a certain significance despite the several limitations posed by the nature of self-reporting data [17]. Our current results demonstrated no statistically consistent reporting of neuropsychiatric AEs due to the interactions of memantine and other potentially interactive drugs, suggesting that there is no robust evidence to support the concern about the increase in neuropsychiatric AEs of memantine when co-administrated with other suspected drugs. This means that, currently, there might not be an urgent need to prohibit co-administration of memantine and its theoretically-interactive drugs.
The interaction between memantine and cimetidine showed inconsistent results between the multiplicative and the additive models [14]—significantly high reporting of the AMS category in the multiplicative model but non-significantly high reporting of AMS in the additive model. Cimetidine, an H2 blocker used for gastritis, is known to cause drug-induced cognitive decline in the elderly population [18–20]. Therefore, a higher adjusted ROR for the interaction between memantine and cimetidine may rather be explained as a direct adverse effect of cimetidine in patients old enough to develop dementia. The observation that the crude ROR of cimetidine was not significantly high for any of the neuropsychiatric AEs included, should then be explained by the younger age of the overall cases taking cimetidine (median age-in-decade, ‘60s) as compared to the older age of those taking memantine (median age-in-decade, ‘80s). Meanwhile, because cimetidine is also reported to increase the intestinal permeability of memantine [21], memantine-cimetidine interaction leading to an increase in the frequency of AEs, cannot always be denied. Since the multiplicative model-based results were not replicated in the additive model which is reported to be generally more sensitive than the multiplicative model [14], currently we consider that we cannot conclude on the unfavorable interactions between memantine and cimetidine, and it needs further investigations.
It is noteworthy that dextromethorphan showed a significantly high reporting of AMS, even after adjustment with of-in-decade, sex, and AChEI agents. Dextromethorphan is a frequently used cough suppressant in the presence of cold. Due to its dissociative effect like that of ketamine or phencyclidine [22], it can be abused, especially by young people. When overdosed, it causes dose-dependent neuropsychiatric toxicity, such as imbalance or hallucinations at a dose of 2.5–7.5 mg/kg or impaired consciousness at a dose of 7.5–15 mg/kg [22, 23]. These adverse effects of overdosed dextromethorphan are not always adequately recognized in Japan, where it is allowed to prescribe at a regular dose of 15–120 mg per day [24]. Based on mild overdose (2.5–7.5 mg/kg) to cause symptoms, it is not unacceptable to observe the neuropsychiatric symptoms in elderly patients with impaired metabolism even after administrating regular doses of dextromethorphan. In line with the significantly high reporting of AMS in the current results, there was a phase III clinical trial conducted using dextromethorphan/quinidine (AVP-786) [25] to treat agitation in AD patients (NCT02442764). Although further validation in the cohort study is needed, it is suggested that we might consider the risks and benefits before prescribing dextromethorphan to elderly individuals or patients with dementia.
Our study has some limitations due to the use of self-reporting database [17], including several kinds of bias that cannot be eliminated from this type of study. First, there may be prescription and reporting bias: Caution has already been noted in the package insert of memantine regarding its co-administration with amantadine or dextromethorphan, making physicians hesitant to prescribe memantine and these drugs simultaneously in patients with seemingly-higher risk (e.g., elderly ones or those with a history of drug-induced neuropsychiatric AEs), or making the adverse events after such co-administration less likely to be reported to JADER. In addition, due to the lack of denominators, we could not discuss the incidence rate of each neuropsychiatric AE, and the kind of neuropsychiatric AEs which are more likely to be seen as a result of drug-drug interactions. Furthermore, in the multivariate adjustment, we have not considered other kinds of medications or concurrent/past medical histories that are potentially related to the development/worsening of dementia symptoms. We also have not included the timing of memantine and other drugs or the total dose of these drugs into consideration in the analysis. Lastly, the potentially duplicated cases might have been over-excluded or under-excluded, since, in the JADER database, there is no established method to exclude the potentially duplicated cases reported from the same patient.
To conclude, our present results demonstrated no statistically significant reporting of neuropsychiatric AEs due to interactions between memantine and other potentially interactive drugs, suggesting that there might not be an urgent need to prohibit co-administration of memantine with the theoretically-interactive drugs. Our results also suggested the potential involvement of neuropsychiatric AEs by dextromethorphan in elderly individuals even when it is not abused. Since this study is based on a self-reporting database that might have several biases, cohort studies are needed to validate these results and conclude the safety of co-administration of these drugs.
ACKNOWLEDGMENTS
This study was performed using the Japanese Adverse Drug Event Report (JADER) database, which was provided by Pharmaceuticals and Medical Devices Agency (PMDA), a Japanese governmental organization. The information, results, or interpretation of the current study do not represent any opinions of the PMDA.
This study was supported by the Japan Agency for Medical Research and Development grants 17dk0207028, 19dk0207048, 19dk0207048h0001, 16dk0207028h0001, and 21dk0207057h0001.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0524r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-210524.
REFERENCES
[1] | Kornhuber J , Weller M , Schoppmeyer K , Riederer P ((1994) ) Amantadine and memantine are NMDA receptor antagonists with neuroprotective properties (1994). J Neural Transm Suppl 43: , 91–104. |
[2] | Rogawski MA , Wenk GL ((2003) ) The neuropharmacological basis for the use of memantine in the treatment of Alzheimer’s disease. CNS Drug Rev 9: , 275–308. |
[3] | Kumar S ((2004) ) Memantine: Pharmacological properties and clinical uses. Neurol India 52: , 307–309. |
[4] | Olivares D , Deshpande VK , Shi Y , Lahiri DK , Greig NH , Rogers JT , Huang X ((2012) ) N-methyl D-aspartate (NMDA) receptor antagonists and memantine treatment for Alzheimer’s disease, vascular dementia and Parkinson’s disease. Curr Alzheimer Res 9: , 746–758. |
[5] | European Medicine Agency. Ebixa Tablets SPC, Summary of Product Characteristics. European Medicine Agency (EMA). http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000463/WC500058763.pdf, Accessed on October 17, 2019. |
[6] | Pasqualetti G , Tognini S , Calsolaro V , Polini A , Monzani F ((2015) ) Potential drug-drug interactions in Alzheimer patients with behavioral symptoms. Clin Interv Aging 10: , 1457–1466. |
[7] | Freudenthaler S , Meineke I , Schreeb KH , Boakye E , Gundert-Remy U , Gleiter CH ((1998) ) Influence of urine pH and urinary flow on the renal excretion of memantine. Br J Clin Pharmacol 46: , 541–546. |
[8] | Pharmaceuticals and Medical Devices Agency, MEMARY Tablets. Attached document (in Japanese). http://www.pmda.go.jp/PmdaSearch/iyakuDetail/ResultDataSetPDF/430574_1190018F1023_1_17, accessed on October 17, 2019. |
[9] | Nomura K , Takahashi K , Hinomura Y , Kawaguchi G , Matsushita Y , Marui H , Anzai T , Hashiguchi M , Mochizuki M ((2015) ) Effect of database profile variation on drug safety assessment: An analysis of spontaneous adverse event reports of Japanese cases. Drug Des Devel Ther 9: , 3031–3041. |
[10] | Sato K , Mano T , Iwata A , Toda T ((2019) ) Neurological and related adverse events in immune checkpoint inhibitors: A pharmacovigilance study from the Japanese Adverse Drug Event Report database. J Neurooncol 145: , 1–9. |
[11] | Sato K , Mano T , Iwata A , Toda T ((2019) ) Subtype-dependent reporting of stroke with SGLT2 inhibitors: Implications from a Japanese pharmacovigilance study. J Clin Pharmacol 60: , 629–635. |
[12] | Van Puijenbroek EP , Egberts AC , Meyboom RH , Leufkens HG ((1999) ) Signalling possible drug-drug interactions in a spontaneous reporting system: Delay of withdrawal bleeding during concomitant use of oral contraceptives and itraconazole. Br J Clin Pharmacol 47: , 689–693. |
[13] | Rothman KJ , Lanes S , Sacks ST ((2004) ) The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiol Drug Saf 13: , 519–523. |
[14] | Thakrar BT , Grundschober SB , Doessegger L ((2007) ) Detecting signals of drug-drug interactions in a spontaneous reports database. Br J Clin Pharmacol 64: , 489–495. |
[15] | VanderWeele TJ , Knol MJ ((2014) ) A tutorial on interaction. Epidemiol Methods 3: , 33–72. |
[16] | Mathur MB , VanderWeele TJ ((2018) ) R function for additive interaction measures. Epidemiology 29: , e5–e6. |
[17] | Michel C , Scosyrev E , Petrin M , Schmouder R ((2017) ) Can disproportionality analysis of post-marketing case reports be used for comparison of drug safety profiles? Clin Drug Investig 37: , 415–422. |
[18] | Cantú TG , Korek JS ((1991) ) Central nervous system reactions to histamine-2 receptor blockers. Ann Intern Med 114: , 1027–1034. |
[19] | Hanlon JT , Landerman LR , Artz MB , Gray SL , Fillenbaum GG , Schmader KE ((2004) ) Histamine2 receptor antagonist use and decline in cognitive function among community dwelling elderly. Pharmacoepidemiol Drug Saf 13: , 781–787. |
[20] | Boustani M , Hall KS , Lane KA , Aljadhey H , Gao S , Unverzagt F , Murray MD , Ogunniyi A , Hendrie H ((2007) ) The association between cognition and histamine-2 receptor antagonists in African Americans. J Am Geriatr Soc 55: , 1248–1253. |
[21] | Choi YA , Song IS , Choi MK ((2018) ) Pharmacokinetic drug-drug interaction and responsible mechanism between memantine and cimetidine. Pharmaceutics 10: , E119. |
[22] | Romanelli F , Smith KM ((2009) ) Dextromethorphan abuse: Clinical effects and management. J Am Pharm Assoc (2003) 49: , e20–5; quiz e26-7. |
[23] | Martinak B , Bolis RA , Black JR , Fargason RE , Birur B ((2017) ) Dextromethorphan in cough syrup: The poor man’s psychosis. Psychopharmacol Bull 47: , 59–63. |
[24] | Pharmaceuticals and Medical Devices Agency, Medicon. Attached document (in Japanese). http://www.pmda.go.jp/PmdaSearch/iyakuDetail/ResultDataSetPDF/340018_2223001B1210_1_05, accessed on October 17, 2019. |
[25] | Garay RP , Grossberg GT ((2017) ) AVP-786 for the treatment of agitation in dementia of the Alzheimer’s type. Expert Opin Investig Drugs 26: , 121–132. |


