
Is Engagement in Intellectual and Social Leisure Activities Protective Against Dementia Risk? Evidence from the English Longitudinal Study of Ageing1
Abstract
Background:
Studies have suggested that mentally stimulating activities and socially engaged lifestyles may reduce dementia risk; however, it is unclear which activities are more beneficial.
Objective:
We investigated intellectual and social leisure activities in relation to dementia incidence and explored the modifying role of sex and marital status in these associations.
Methods:
The sample was comprised of 8,030 participants aged 50+ from the English Longitudinal Study of Ageing, who joined at wave 1 (2002-2003), or waves 3 (2006-2007), or 4 (2008-2009). The end of the study period was wave 8 (2016-2017). Subdistribution hazard models investigated the role of leisure activities grouped into intellectual and social domains in relation to dementia while accounting for the risk of death. Subsequent analyses were conducted with individual leisure activities.
Results:
During the study period of up to 15 years, 412 participants developed dementia, and 2,192 died. We found that increased engagement in the intellectual activities’ domain was associated with a decreased dementia incidence (SHR 0.85, 95% CI 0.76–0.96, p = 0.007), independent of the risk of death in married individuals, but not in those who were single, divorced, or widowed. Individual analyses for each leisure activity showed independent associations for reading newspapers in females (SHR 0.65, 95% CI 0.49–0.84, p = 0.001), mobile phone usage in males (SHR 0.61, 95% CI 0.45–0.84, p = 0.002), and having hobbies for married individuals (SHR 0.70, 95% CI 0.51–0.95, p = 0.02).
Conclusion:
We found that intellectual leisure activities contribute to lower dementia risk in a representative population of English adults, suggesting intervention opportunities.
INTRODUCTION
Dementia continues to represent a significant cause of disability and one of the leading causes of death for older individuals [1]. With no medical cure available to date, and an increasingly aging population, understanding dementia’s modifiable protective factors is a public health priority. Lifestyle-related factors have been found to play a crucial role in modifying the risk of dementia, particularly for those activities that improve the brain’s resilience. Cognitive reserve has been proposed as the brain’s inbuilt resilience mechanism which mediates between brain pathology and the clinical manifestation of that damage [2]. Hence, improving cognitive reserve capacity through healthy lifestyle choices represents a promising preventive avenue against dementia development [3].
Leisure time activities, described as activities that are independent of work and the purpose of which is enjoyment or well-being [4], appear to have an essential role in maintaining brain health and contributing to cognitive reserve capacity [5]. Previous research has shown that engagement in physical, intellectual, and social leisure activities contribute to cognitive reserve and, thus, to a reduced dementia risk [6, 7]. This evidence has also suggested possible pathways, with intellectual and social activities having direct protective effects on brain health through their contribution to cognitive reserve [5, 8], whereas physical activity appears to have an indirect role in the brain through cardiovascular protection [9]. Furthermore, previous research has found that people engage in different types of leisure according to age, gender, and marital status [10, 11]. It has been suggested that participation in physical activities decreases with age for both genders [10]. In contrast, intellectual and social activities show more stability and even an increased engagement for females [10] and married individuals [12]. Hence, intellectual and social activities appear to be suitable for dementia prevention in aging populations.
Most research examining the relationship between engagement in intellectual and social leisure acti-vities and dementia has been carried out cross-sectionally or longitudinally with relatively shorter follow-up periods, positing the issue of reverse causality [13]. Moreover, it is still unclear which specific activities affect cognition to a greater degree and whether the favorable effects of a healthy lifestyle on the brain are independent of sex, marital status, and the risk of death.
We used data from a population-based cohort of older adults living in England to investigate engagement in intellectual and social leisure activities and dementia risk, while accounting for the risk of death over a follow-up period of up to 15 years. We explored the modifying roles of sex and marital status in the relationship between leisure activities and dementia incidence. Additionally, we examined the role of each social and intellectual leisure activity on dementia risk.
METHODS
Study population
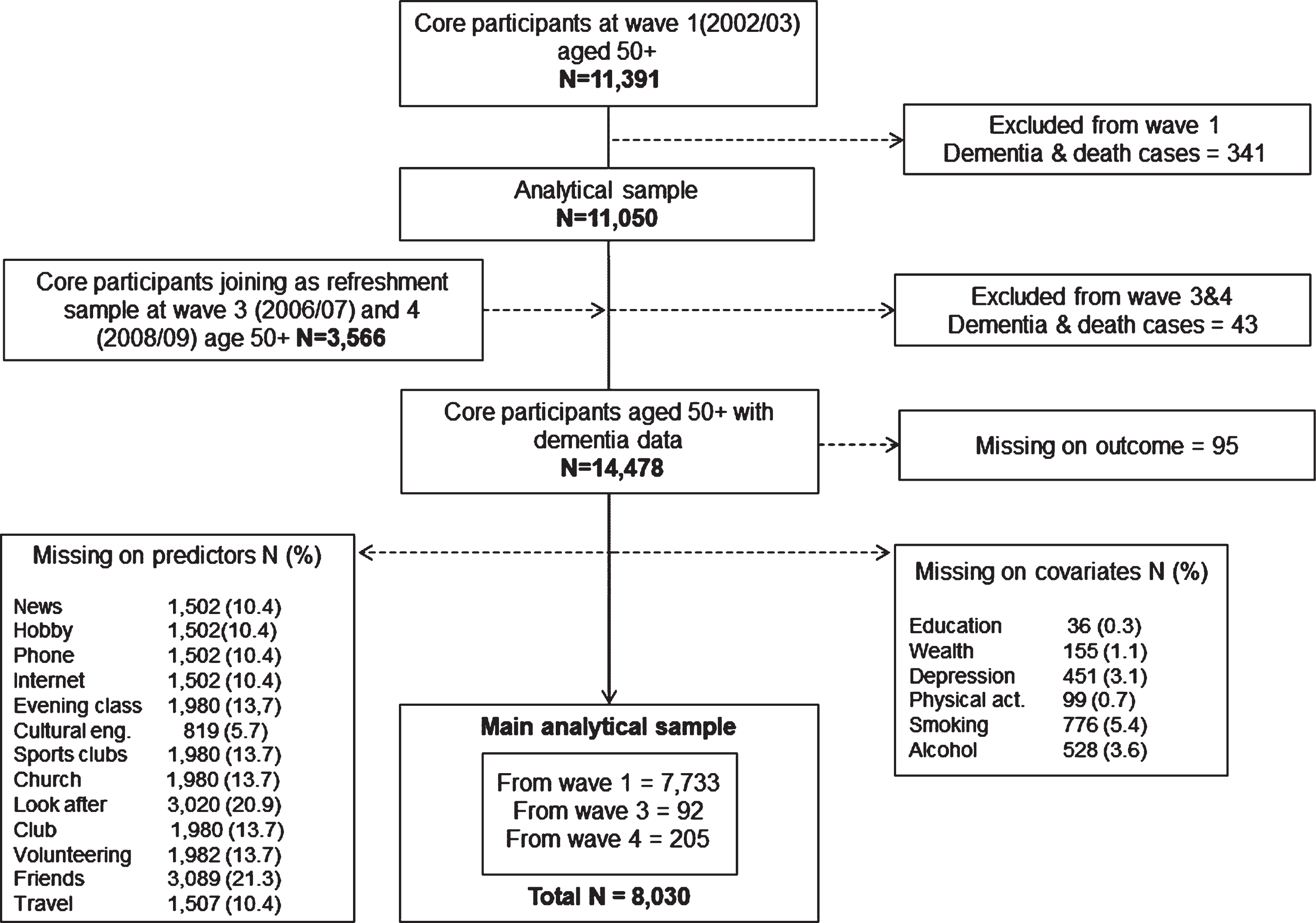
The data were extracted from the English Longitudinal Study of Ageing (ELSA), a longitudinal observational study of a representative sample of people living in England, aged fifty years and older [14]. Data collection has been carried out every two years since 2002, using computer-assisted personal interviewing (CAPI). The study sample is refreshed periodically with new participants to maintain the age structure of 50 and older. The baseline for the present analysis was either wave 1 (2002-2003) for those core members who started the study at this initial stage, or waves 3 (2006-2007) or 4 (2008-2009) for those who joined the study as refreshment samples. At the time of this analysis, the latest available data were wave 8 (2016-2017), ensuring a follow-up period of up to 15 years for those who joined at wave 1 (n = 7,733); up to 11 years for those who joined as refreshment sample at wave 3 (n = 92); and up to 9 years for those who joined as refreshment sample at wave 4 (n = 205). See Fig. 1 for the flow chart of the analytical sample. Participants with dementia at their baseline assessments were excluded.
Fig. 1
Flowchart of participants selected for the current analyses from the English Longitudinal Study of Ageing. *Numbers of excluded participants are non-mutually exclusive.
Ethical approval for data collection in ELSA was granted by the National Research Ethics Service (London Multicentre Research Ethics Committee) in accordance with the Declaration of Helsinki. All participants provided informed consent.
Measures
Dementia ascertainment
Dementia was determined at each wave using an algorithm based on a combination of a positive self-reported or informant reported physician diagnosis of dementia or a score above the threshold of 3.38 (specificity = 0.84 and sensitivity = 0.82) [15] on the 16-question Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) [16]. When individuals were not able to participate personally in the interview, the IQCODE questionnaire was administered to a family member or caregiver, who evaluated the changes in everyday cognitive function (e.g., remembering names of family members) compared to 2 years ago. Each IQCODE item is scored from 1 (much improved) to 5 (much worse). In the present study, 133 (32%) of 412 cases of dementia were classified with dementia via higher scores on the IQCODE scale.
Leisure activities
The 13 individual leisure activities were extracted at baseline from various questionnaires enquiring about cultural engagement, community engagement, and participation in various recreational activities. The questions had different answer categories, including binary measures or frequency of participation. Therefore, we regrouped all answers into binary responses, so one point was allocated for each individual activity. Activities that captured similar measures, such as ‘participation in social activities’ and ‘meeting with friends’, were clustered into a single variable (see Supplementary Table 1). The activities were then classified as intellectually stimulating or socially stimulating leisure activities, resulting in two aggregate scores reflecting the total number of activities participants engage in.
Intellectual leisure activities. The intellectual domain of leisure activities was composed of the following 6 individual activities: reading newspapers; having a hobby or pastime; using a mobile phone; using the internet or email; attending art or music groups; and cultural engagement.
Social leisure activities. The social domain of leisure activities contained a total of 7 individual activities including membership to sports clubs; church groups; looking after others (e.g., grandchildren); belonging to political or union group, neighborhood group, environmental group, or any other organization; engaging with charitable associations and/or volunteering; belonging to a social club and/or meeting with friends; and taking holidays in the UK, holidays abroad and/or day trips.
Covariates
Sex and marital status (categorized as married, single/divorced, and widowed) were identified as covariates as well as possible moderators. Socioeconomic covariates were captured through education and wealth. Health conditions were assessed through physician diagnoses of coronary heart disease, stroke, hypertension, diabetes. Depressive symptoms were ascertained with the 8- item Center for Epidemiologic Studies Depression Scale (CES-D), which is designed to measure depressive symptomatology in the general population [17]. Finally, lifestyle behaviors (physical activity, smoking, and alcohol intake) were also considered.
Statistical analysis
Descriptive statistics for those who remained dementia-free and those who develop dementia during the study period were carried out by level of engagement in intellectual and social leisure activities and covariates, using independent sample t-tests for continuous measures (leisure activity domains and CES-D) and Pearson chi-square test for categorical variables.
To investigate the relationship between the leisure activity categories and dementia incidence, while considering the competing risk of death, we em-ployed Fine and Gray proportional subdistribution hazard models [18]. For participants who consented to data linkage, mortality data records up to December 2018, were obtained from the National Health Service central register. Survival age was used as the underlying time variable. Survival age was derived using survival time, which was calculated using the participants’ baseline age until the age they reported dementia diagnosis or the end of the study period (i.e., last wave before dropout or wave 8). Two separate analyses were carried out for the intellectual and social leisure activity domains; each domain was defined as the number of activities performed (i.e., count variables). Additional individual analyses were carried out for each of the 13 individual leisure activities. The frequency of participation was used when available, such as cultural engagement (i.e., never, less than once a year, once or twice a year, every few months), volunteering (i.e., never, less than once a year or up to twice a year, every few months), and meeting with friends (i.e., never, once or twice a month, once or twice a week, three or more times a week). All other leisure activities were grouped into participation versus no participation (binary). Sub-hazard ratios (SHR) and their respective 95% confidence intervals (CI) were calculated using 4 models: Model 1 adjusted for sex and marital status; model 2 also included education and wealth; model 3 further adjusted for health conditions including depressive symptoms; and model 4 further adjusted for lifestyle behaviors. We additionally explored interactions with sex and marital status with all predictor variables. All explorations were carried out using complete case analysis.
Several sensitivity analyses were carried out to assess the dementia diagnosis procedure, the varying study entries, and data missingness. The first sensitivity analysis addressed the different classifications of dementia diagnosis (i.e., doctor diagnosis and IQCODE scores) by excluding participants that were classified as having dementia through the IQCODE score. The second sensitivity analysis addressed the varying baseline assessments by excluding participants who joined the study as refreshment samples at waves 3 or 4. The final sensitivity analyses were conducted to assess the impact of missing data by performing multiple imputations using chained equations and repeating the analyses for the leisure domains.
All analyses were weighted using the baseline cross-sectional weights derived in ELSA to ensure the sample is representative of the English population. All analyses were conducted in Stata MP, Version 16 (Stata Corp). Statistical significance was at or below the 0.05 level.
RESULTS
Descriptive statistics
The analytical sample was comprised of 8,030 participants (81, 726.92 person-years) with an average baseline age of 63.8 (SD = 9.60) years. The sample consisted of 3,568 (44%) males and 4,462 (56%) females. At the time of the event or last wave of follow-up, the mean age for all participants was 74 (SD = 9.31) years, ranging from 52 to 102.
From the overall sample, 412 participants were diagnosed with dementia, accounting for 5.13% cumulative incidence during the 15-year follow-up period. The group of individuals with dementia included 180 (44%) males and 232 (56%) females with a median age of 81 (SD = 8.22) years at the time of dementia diagnosis. Furthermore, 2,192 (27%) participants died within the study period, with a mean age at death of 81 (SD = 9.53) years. From this group, 274 died after receiving a dementia diagnosis.
Initial statistical investigation showed that participants who developed dementia were older, had less education, were more likely to be widowed, and were diagnosed with comorbidities at baseline (see Table 1). The group of participants who developed dementia generally engaged in less intellectual and social leisure activities than those who did not develop dementia. The percentages of the baseline sample engaging in each leisure activity are also presented in Table 1.
Table 1
Baseline characteristics of participants with and without dementia at follow-up
| Characteristics | No dementia | Dementia | p |
| (n = 7,618) | (n = 412) | ||
| Age: 50–59 | 3,224 (42%) | 37 (9%) | < 0.001 |
| 60–69 | 2,382 (31%) | 114 (28%) | |
| 70–79 | 1,501 (20%) | 156 (38%) | |
| ≥80 | 511 (7%) | 105 (25%) | |
| Sex: Male | 3,388 (44%) | 180 (44%) | 0.755 |
| Female | 4,230 (56%) | 232 (56%) | |
| Marital status: Married or remarried | 5,258 (69%) | 243 (59%) | < 0.001 |
| Single/divorced or legally separated | 1,249 (16%) | 48 (12%) | |
| Widowed | 1,111 (15%) | 121 (29%) | |
| Education: Higher education | 2,014 (26%) | 70 (17%) | < 0.001 |
| A-levels | 1,887 (25%) | 78 (19%) | |
| < A-levels | 345 (5%) | 22 (5%) | |
| Foreign/other | 673 (9%) | 39 (10%) | |
| No qualification | 2,699 (35%) | 203 (49%) | |
| Wealth: 5 (highest) | 1,118 (15%) | 98 (24%) | < 0.001 |
| 4 | 1,411 (19%) | 77 (19%) | |
| 3 | 1,558 (20%) | 93 (22%) | |
| 2 | 1,705 (22%) | 70 (17%) | |
| 1 (lowest) | 1,826 (24%) | 74 (18%) | |
| CHD: No | 6,904 (91%) | 333 (81%) | < 0.001 |
| Yes | 714 (9%) | 79 (19%) | |
| Stroke: No | 7,392 (97%) | 382 (93%) | < 0.001 |
| Yes | 226 (3%) | 30 (7%) | |
| Hypertension: No | 4,900 (64%) | 228 (55%) | < 0.001 |
| Yes | 2,718 (36%) | 184 (45%) | |
| Diabetes: No | 7,145 (94%) | 375 (91%) | 0.025 |
| Yes | 473 (6%) | 37 (9%) | |
| Depressive symptoms (CES-D) * | 1.40(1.85) | 1.91 (1.99) | < 0.001 |
| Physical activity: Sedentary | 1,084 (14%) | 110 (27%) | < 0.001 |
| 1 | 1,114 (15%) | 81 (20%) | |
| 2 | 2,296 (30%) | 119 (29%) | |
| 3 | 1,590 (21%) | 63 (15%) | |
| Active | 1,534 (20%) | 39 (9%) | |
| Smoke: No | 6,325 (83%) | 355 (86%) | 0.097 |
| Yes | 1,293 (17%) | 57 (14%) | |
| Alcohol: 1-2 month/never | 2,851 (37%) | 194 (47%) | < 0.001 |
| 1-2 week/daily | 4,767 (63%) | 218 (53%) | |
| Newspaper: No | 2,308 (30%) | 133 (32%) | 0.394 |
| Yes | 5,310 (70%) | 279 (68%) | |
| Hobby: No | 1,340 (18%) | 106 (26%) | < 0.001 |
| Yes | 6,278 (82%) | 306 (74%) | |
| Phone: No | 2,792 (37%) | 237 (57%) | < 0.001 |
| Yes | 4,826 (63%) | 175 (43%) | |
| Internet: No | 4,855 (64%) | 342 (83%) | < 0.001 |
| Yes | 2,763 (36%) | 70 (17%) | |
| Cultural engagement: Never | 4,704 (62%) | 311 (75%) | < 0.001 |
| Less than once a year | 1,430 (19%) | 52 (13%) | |
| Once or twice a year | 1,074 (14%) | 30 (7%) | |
| Every few months | 410 (5%) | 19 (5%) | |
| Art or music groups: No | 6,476 (85%) | 358 (87%) | 0.295 |
| Yes | 1,142 (15%) | 54 (13%) | |
| Sports clubs: No | 5,977 (78%) | 363 (88%) | < 0.001 |
| Yes | 1,641 (22%) | 49 (12%) | |
| Church: No | 5,940 (78%) | 294 (71%) | 0.002 |
| Yes | 1,678 (22%) | 118 (29%) | |
| Look after others: No | 5,951 (78%) | 349 (85%) | 0.002 |
| Yes | 1,667 (22%) | 63 (15%) | |
| Club or organization: No | 4,134 (54%) | 239 (58%) | 0.137 |
| Yes | 3,484 (46%) | 173 (42%) | |
| Volunteering: Never | 5,202 (68%) | 309 (75%) | 0.004 |
| Once to twice a year or less | 457 (6%) | 12 (3%) | |
| Every few months or more | 1,959 (26%) | 91 (22%) | |
| Social club: No | 5,958 (78%) | 324 (79%) | 0.836 |
| Yes | 1,660 (22%) | 88 (21%) | |
| Meeting friends: Every few months or never | 1,182 (15%) | 72 (17%) | 0.390 |
| Once or twice a month | 1,879 (25%) | 99 (24%) | |
| Once or twice a week | 3,288 (43%) | 164 (40%) | |
| Three or more times a week | 1,269 (17%) | 77 (19%) | |
| Travel: No | 809 (11%) | 77 (19%) | < 0.001 |
| Yes | 6,809 (89%) | 335 (81%) | |
| Intellectual leisure activities domain* | 3.08 (1.39) | 2.46 (1.31) | < 0.001 |
| Social leisure activities domain* | 3.20 (1.37) | 2.94 (1.38) | < 0.001 |
Data displayed as n (%) or *means±SD. CHD, coronary heart disease; CES-D, Center for Epidemiologic Studies Depression Scale.
Survival analyses
The variance inflation factor for all variables included in these analyses was < 1.39, suggesting no multicollinearity since values greater than 2.5 are considered high. The highest correlation was a moderate-low association between cognitive leisure activities and education (r = 0.43, p < 0.001). Using the Schoenfeld residuals, it was found that the cognitive leisure and social leisure domains met the proportional hazard assumption.
The intellectual domain of leisure activities
At baseline, most participants (70%) engaged in 2 to 4 intellectual activities, with only 3% of the participants reporting no engagement in any intellectual leisure activities and 4% participating in 6 activities (see Supplementary Figure 1).
The competing risk regression showed a significant association between intellectual leisure activities and dementia after controlling for all covariates (SHR: 0.91, 95% CI 0.83–0.99, p = 0.003). This model also showed a positive association for increased depressive symptomatology (Model 4 SHR: 1.08, 95% CI 1.02–1.23, p = 0.004) and dementia incidence, and a negative significant association with increased physical activity (Model 4 SHR 0.61, 95% CI 0.41–0.92, p = 0.02) and dementia incidence.
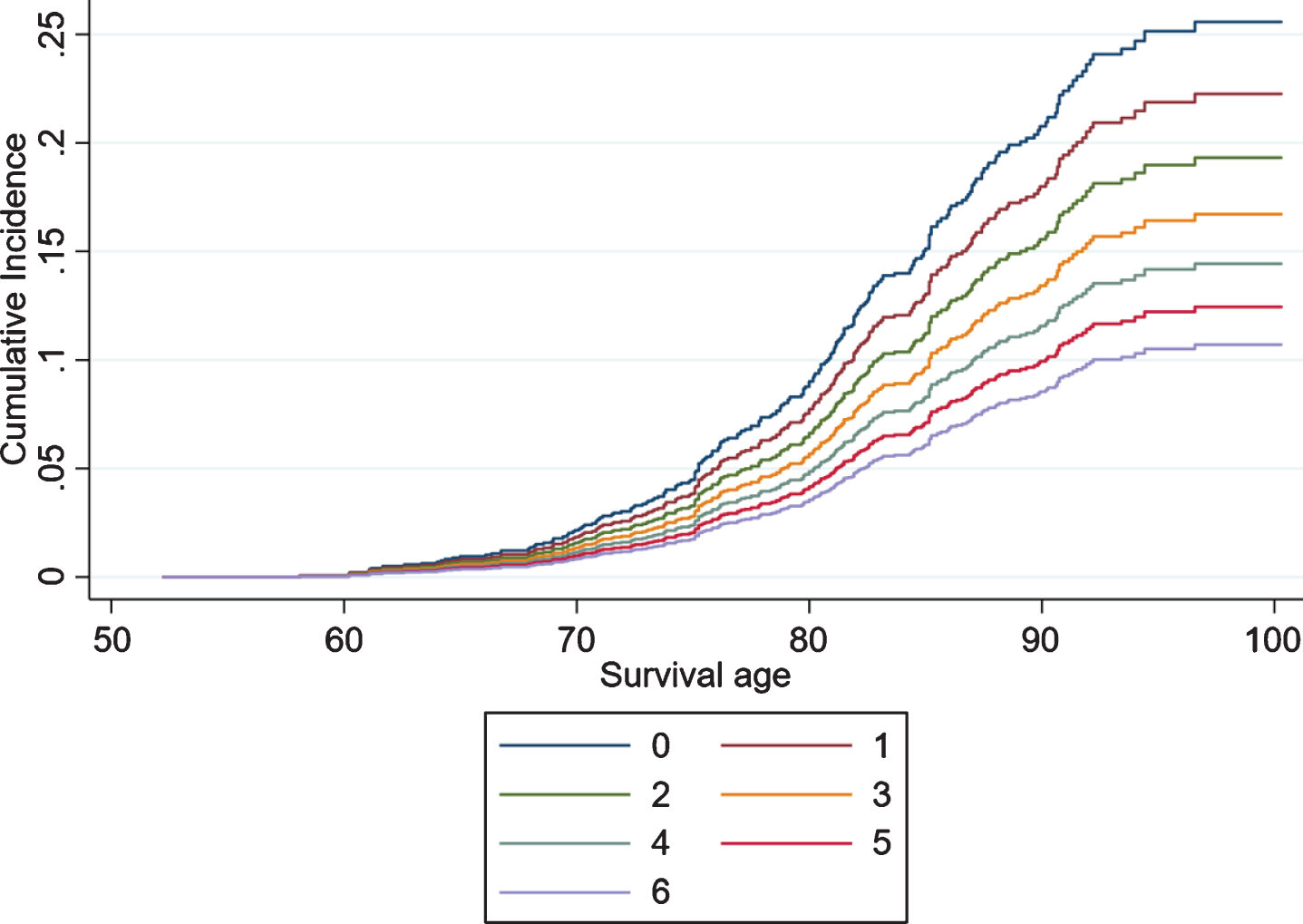
Additional exploration for effect measure modification by marital status showed a marginally significant interaction (p = 0.05). As presented in Table 2, after stratification for marital status, it was found that in the fully adjusted model, an increased engagement in intellectual leisure activities was associated with a decreased incidence of dementia for married individuals (n = 5,501; SHR: 0.85, 95% CI 0.76–0.96, p = 0.007) (see Fig. 2). The association between intellectual leisure activities and dementia was non-significant for the single/divorced (n = 1,297; Model 4 SHR: 1.11, 95% CI 0.85–1.45, p = 0.46) and widowed (n = 1,232; Model 4 SHR: 0.98, 95% CI 0.83–1.17, p = 0.86) stratum. The interaction between the intellectual leisure activities domain and sex was non-significant (p = 0.79).
Table 2
Sub-hazard ratios and 95% confidence intervals of the competing risk models indicating the incidence of dementia for engagement in leisure activities
| Domains | N | Model 1 | Model 2 | Model 3 | Model 4 |
| Intellectual leisure activities | |||||
| Married | 5,501 | 0.80 (0.73–0.89)** | 0.83 (0.74–0.92)** | 0.84 (0.76–0.94)* | 0.85 (0.76–0.96)* |
| Single or divorced | 1,297 | 0.99 (0.79–1.24) | 0.99 (0.77–1.27) | 1.07 (0.84–1.36) | 1.11 (0.85–1.45) |
| Widowed | 1,232 | 0.96 (0.82–1.11) | 0.96 (0.82–1.13) | 0.97 (0.83–1.14) | 0.98 (0.83–1.17) |
| Social leisure activities | 8,030 | 0.92 (0.86–0.99)* | 0.95 (0.88–1.03) | 0.97 (0.89–1.04) | 0.98 (0.90–1.06) |
Intellectual leisure activities are stratified by marital status. Model 1: Sex and marital status. Model 2: Model 1 + education and wealth. Model 3: Model 2 + physical health covariates and depression. Model 4: Model 3 + lifestyle factors. *p < 0.05, **p≤0.001.
Fig. 2
Competing risk regressions by the number of intellectual activities performed by married individuals aged 50+ in the English Longitudinal Study of Ageing.
The social domain of leisure activities
As in the case of intellectual activities, 72% of participants reported 2 to 4 social leisure activities., while 1% did not engage in any social activity. Only 0.64% of the participants engaged in 7 social activities (see Supplementary Figure 1). The association between the social domain of leisure activities and dementia incidence is presented in Table 2. The minimally adjusted model showed a significant association between engagement in social leisure activities and dementia incidence (SHR 0.92, 95% CI 0.86–0.99, p = 0.03). However, in Model 2, the association between social leisure and dementia was explained after adjusting for educational attainment and wealth (SHR: 0.95, 95% CI 0.88–1.03, p = 0.20). The interactions between the social leisure domain and sex (p = 0.70) or marital status (single/divorced p = 0.09; widowed p = 0.12) were non-significant.
In terms of covariates, we found that increased depressive symptomatology (Model 4 SHR: 1.08, 95% CI 1.03–1.13, p = 0.003) and physical activity (Model 4 SHR: 0.59, 95% CI 0.39–0.88, p = 0.01) were significantly associated with a reduced dementia incidence.
Individual leisure activities
Table 3 summarizes the competing risk regressions indicating the incidence of dementia for individual leisure activities. Model 1 showed a significant association between individual activities and dementia incidence for reading the newspapers (SHR 0.77, 95% CI 0.63–0.95, p = 0.02), having a hobby (SHR 0.72, 95% CI 0.58–0.91, p = 0.005), using the mobile phone (SHR 0.74, 95% CI 0.60–0.91, p = 0.004), using the internet (SHR 0.74, 95% CI 0.56–0.97, p = 0.03), cultural engagement for those who do it once or twice a year (SHR 0.66, 95% CI 0.45–0.97, p = 0.03), sports clubs (SHR 0.67, 95% CI 0.50–0.91, p = 0.01), and volunteering for those who engage in the activity every few months (SHR 0.78, 95% CI 0.62–0.99, p = 0.05). However, after adjustment for all covariates, it was found that only two activities: reading the newspaper (SHR 0.79, 95% CI 0.64–0.98, p = 0.03) and using a mobile phone (SHR 0.80, 95% CI 0.65–0.99, p = 0.04) maintained a significant and independent association with dementia incidence.
Table 3
Sub-hazard ratios and 95% confidence intervals of the competing risk models indicating the incidence of dementia for individual leisure activities
| Domains | Model 1 | Model 2 | Model 3 | Model 4 |
| Intellectual leisure activities | ||||
| Reading newspapers: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.77 0.63–0.95)* | 0.78 (0.63–0.97)* | 0.79 (0.64–0.98) | 0.79 (0.64–0.98)* |
| Having a hobby or pastime: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.72 (0.58–0.91)* | 0.77 (0.61–0.97)* | 0.81 (0.64–1.03) | 0.85 (0.66–1.08) |
| Using a mobile phone: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.74 (0.60–0.91)* | 0.78 (0.63–0.97) | 0.79 (0.64–0.98) | 0.80 (0.65–0.99)* |
| Using the internet: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.74 (0.56–0.97)* | 0.79 (0.59–1.05) | 0.81 (0.61–1.08) | 0.82 (0.61–1.09) |
| Art or music groups: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.96 (0.71–1.28) | 1.09 (0.80–1.48) | 1.11 (0.82–1.51) | 1.14 (0.84–1.56) |
| Cultural engagement: Never | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Less than once a year | 0.84 (0.62–1.13) | 0.93 (0.68–1.28) | 0.97 (0.71–1.33) | 1.01 (0.74–1.38) |
| Once or twice a year | 0.66 (0.45–0.97)* | 0.75 (0.50–1.12) | 0.79 (0.53–1.18) | 0.83 (0.55–1.24) |
| Every few months | 1.25 (0.78–2.01) | 1.49 (0.91–2.44) | 1.55 (0.95–2.54) | 1.63 (0.99–2.68) |
| Social leisure activities | ||||
| Sports clubs: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.67 (0.50–0.91)* | 0.72 (0.53–0.98)* | 0.74 (0.54–1.00) | 0.83 (0.60–1.14) |
| Church groups: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 1.10 (0.89–1.37) | 1.18 (0.94–1.47) | 1.18 (0.94–1.48) | 1.16 (0.93–1.46) |
| Look after others: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.81 (0.61–1.06) | 0.78 (0.59–1.03) | 0.78 (0.59–1.02) | 0.79 (0.60–1.04) |
| Organization membership: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.90 (0.73–1.09) | 0.98 (0.79–1.21) | 0.99 (0.80–1.23) | 1.01 (0.81–1.26) |
| Volunteering: Never | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Less than once a year or up to twice a year | 0.67 (0.37–1.19) | 0.71 (0.40–1.27) | 0.73 (0.41–1.30) | 0.75 (0.42–1.33) |
| Every few months | 0.78 (0.62–0.99)* | 0.84 (0.66–1.08) | 0.88 (0.69–1.14) | 0.91 (0.70–1.17) |
| Meeting with friends: Never | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Once or twice a month | 1.01 (0.74–1.37) | 1.05 (0.77–1.42) | 1.07 (0.79–1.46) | 1.08 (0.80–1.48) |
| Once or twice a week | 0.80 (0.61–1.07) | 0.82 (0.62–1.08) | 0.84 (0.63–1.11) | 0.87 (0.66–1.16) |
| Three or more times a week | 0.92 (0.66–1.29) | 0.90 (0.64–1.25) | 0.92 (0.66–1.28) | 0.96 (0.69–1.34) |
| Holiday: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.82 (0.63–1.06) | 0.87 (0.67–1.14) | 0.94 (0.71–1.23) | 0.97 (0.74–1.27) |
Model 1: Sex and marital status. Model 2: Model 1+ education and wealth. Model 3: Model 2+ physical health covariates and depression. Model 4: Model 3+ lifestyle factors. *p < 0.05, **p≤0.001.
Additional interaction analyses were carried out for each leisure activity. As presented in Table 4, we found a marginally significant interaction between sex and reading the news (p = 0.06) and between sex and phone use (p = 0.06). We also found a significant interaction between marital status and having a hobby (p = 0.04). After stratification, we found that reading the newspapers was significantly associated with a decreased incidence of dementia in females (Model 4 SHR 0.65 95% CI 0.49–0.84, p = 0.001), mobile phone usage in males (Model 4 SHR 0.61, 95% CI 0.45–0.84, p = 0.002), and having hobbies in married individuals (Model 4 SHR 0.70, 95% CI 0.51–0.95, p = 0.02), independent of all covariates.
Table 4
Sub-hazard ratios and 95% confidence intervals of the competing risk models indicating the incidence of dementia for individual activities with significant interactions for sex and marital status
| Individual leisure activities | Model 1 | Model 2 | Model 3 | Model 4 |
| Reading newspapers*sex (p = 0.061) | ||||
| Males: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 1.03 (0.73–1.46) | 1.02 (0.72–1.46) | 1.02 (0.72–1.47) | 1.04 (0.73–1.50) |
| Females: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.64 (0.49–0.84)** | 0.65 (0.50–0.85)* | 0.65 (0.50–0.86)* | 0.65 (0.49–0.84)** |
| Phone use*sex (p = 0.056) | ||||
| Males: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.58 (0.42–0.79)** | 0.62 (0.45–0.84)* | 0.62 (0.45–0.85)* | 0.61 (0.45–0.84)* |
| Females: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.95 (0.73–1.24) | 0.98 (0.74–1.31) | 0.99 (0.75–1.33) | 1.05 (0.78–1.40) |
| Hobby*marital status (p = 0.044) | ||||
| Single or divorced: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.58 (0.43–0.77)** | 0.62 (0.46–0.85)* | 0.66 (0.49–0.89)* | 0.70 (0.51–0.95)* |
| Married or remarried: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 1.14 (0.57–2.26) | 1.09 (0.54–2.20) | 1.42 (0.67–3.01) | 1.43 (0.67–3.07) |
| Widowed: No | 1 [Reference] | 1 [Reference] | 1 [Reference] | 1 [Reference] |
| Yes | 0.91 (0.60–1.41) | 0.93 (0.60–1.44) | 0.98 (0.63–1.52) | 1.01 (0.64–1.60) |
Model 1: Sex and marital status. Model 2: Model 1+ education and wealth. Model 3: Model 2+ physical health covariates and depression. Model 4: Model 3+ lifestyle factors. *p < 0.05, **p≤0.001.
Sensitivity analyses
All sensitivity analyses confirmed the results found in our primary analyses. Supplementary Tables 2 and 3 present the results for the first two sensitivity analyses using complete data. Sensitivity analysis 3 showed that after performing multiple imputation, the results for the intellectual leisure activity domain were similar for married individuals (Model 4: SHR 0.90, 95% CI 0.81–0.99, p = 0.04). Furthermore, comparably to the analysis performed using complete data, the results for the social activity domain were non-significant (Model 4: SHR 0.96, 95% CI 0.90–1.03, p = 0.27).
DISCUSSION
This study investigated the association between leisure activities, categorized into two distinctive domains of intellectual and social activities, in relation to dementia incidence in a representative sample of the English population aged 50 years and older. We found that increased engagement in intellectual leisure activities was negatively and independently associated with dementia incidence in married individuals, but not in those who were single, divorced, or widowed. The individual investigation of leisure activities suggested that reading the newspaper in females, mobile phones use in males, and engaging in hobbies in married individuals have a reduced risk of dementia. All analyses accounted for the competing risk of death. The findings were independent of important risk factors such as education, wealth, vascular health, diabetes, depressive symptoms, physical activity, smoking, and alcohol intake.
Previous studies have suggested that marital status has a moderating role in the association between leisure activities and successful aging. A systematic review highlighted that being married is associated with healthier lifestyle behaviors, and consequently, to a reduced risk of dementia [19]. Additionally, there is a growing body of evidence from observational studies suggesting that an intellectually engaged lifestyle is associated with a reduced risk of dementia [8]. Furthermore, the findings from our intellectual domain exploration are in accordance with a meta-analysis comprising 19 studies that found significant evidence for the association between participation in mentally stimulating activities and a reduced risk of cognitive impairment or dementia in later life [20]. Leisure time activities that are cognitively stimulating, such as reading, solving puzzles, and learning experiences, may protect the brain by improving and maintaining the brain’s flexibility and adaptability, directly contributing to cognitive reserve [2, 21]. Furthermore, intellectual activities involving cultural engagement have also shown an association with reduced dementia risk, possibly due to the activities providing individuals with novel experiences and opportunities to engage socially, contributing a positive affect and cognitive reserve simultaneously [22].
Our findings for the social leisure domain and dementia incidence are in accordance with previous studies with extended follow-up periods (two decades) that have found non-significant associations between engagement in social activities and dementia [23, 24]. However, these findings are in contrast with more recent investigations supporting this association. A systematic review and meta-analysis, comprising 19 longitudinal cohorts with 2 to 15 years follow-up, exploring the impact of participating in various social activities, found an increased risk of dementia for individuals who reported less social engagement [25]. Furthermore, our analyses on both leisure activity domains highlighted the influence of depressive symptoms and engagement in physical activities in the incidence of dementia. Depression has been widely recognized as an important risk factor for dementia [26]. Depressive symptomatology might reduce the direct opportunities for engagement in leisure activities and indirectly for cognitive reserve enhancement due to its debilitating impact on behavior and social withdrawal [27]. On the other hand, physical and social engagement in various leisure activities might positively affect stress reduction and improved neurotransmission, thereby enhancing cognitive reserve and brain health maintenance [28].
Our investigation on the modifying effects of sex and marital status on individual leisure activities and dementia highlighted some differences in dementia incidence with a reduced risk for females who read the newspapers, males who use a mobile phone, and married individuals who participate in hobbies. Reading has robustly shown a contribution to health through various studies, supporting the idea that solitary non-strenuous activities contribute to cognitive reserve and successful aging [29, 30]. Furthermore, an earlier longitudinal study investigating mobile phone use and cognition in the elderly found that frequent long-term use of a mobile phone was associated with better cognitive function [31]. This research by Ng and colleges [31] found that mobile phone users were more likely to be males who work and are socially active, both activities being predictors of healthy cognitive aging. Similarly, engaging in a wide variety of hobbies has been found to have protective effects against dementia onset, with a previous study finding a 14% decreased risk of dementia for those who report engaging in a higher number of activities [32].
Our findings differ from those of a previous ELSA analysis, which found a significant association between internet use during midlife and incident dementia. In their study, d’Orsi et al. [33] used data from 8,238 participants with a 10-year follow-up from baseline at wave 1 (2002-2003) to wave 6 (2006–2013), and controlled for similar covariates to the ones introduced in our study. Despite using a similar approach to investigate this association, the difference in findings might suggest a reduction in the protective effect of internet use over time. A previous study examining leisure activity participation and found a significant association with dementia incidence when ascertained for a short period of time after baseline (1–5 years), but not when ascertained for more extended periods of time (6–10 and 11–15 years) [34]. Hence, these findings support the idea that different leisure activities might have short-term or long-term effects on the risk of dementia development. Alternatively, it is also possible that older participants who have started using the internet in their older age had an above-average level of cognitive functioning and therefore compensated for the potential neurological damage occurring and delaying the time to dementia diagnosis.
Dementia may develop insidiously for years before the onset of the clinical symptomatology, often making it difficult to establish a temporal sequence between risk factors and dementia diagnosis. Hence, longitudinal studies, such as this one, are required to better understand the protective lifestyle factors of dementia. With a 15-year follow-up, we were able to ascertain a lower dementia incidence for married individuals who engage in intellectual leisure activities, minimizing the issue of reverse-causality while accounting for the competing risk of death. Furthermore, we benefitted of a large population sample in comparison to previous studies that might have extended follow-up periods but had a reduced power. The study also controlled for relevant covariates that have been identified as confounders in the association between dementia and a comprehensive set of leisure activities. To preserve the analytical sample, we did not introduce additional covariates such as APOE ɛ4 since biomarker data was only collected from a sub-sample of ELSA. Additionally, the association between cognitive reserve markers and dementia controlling for genetic risk has been researched before in this dataset [35]. However, an important methodological issue that needs to be considered is the classification of leisure activities into either intellectual or social domains. Some activities considered in this study involve both intellectual and social engagement; hence their type might be somewhat arbitrary due to the overlap between the two domains. Another methodological issue is related to the self-report dementia diagnosis, which could underestimate the number of participants with dementia in the study due to misclassification of cases. However, our sensitivity analysis, excluding individuals classified with dementia via high IQCODE scores, found similar results to those of our main analysis. Lastly, there is a potential attrition bias due to the longitudinal nature of the study (Supplementary Table 4).
Future work investigating the role of leisure activities on cognitive decline trajectories related to subsequent dementia risk could further elucidate the mechanisms involved in these associations during the prodromal stages of the disease. More research is needed to understand the association between individual leisure activities as markers of cognitive reserve and dementia risk. Future work could consider the role of different follow-up periods and the onset and time of exposure to a particular activity. Furthermore, since participation in leisure activities tends to decline in the preclinical phases of dementia [36], longitudinal studies with extended follow-up periods are desirable.
In conclusion, this study provides sound evidence for the contribution of intellectual leisure activities to cognitive reserve and subsequent reduced risk of dementia incidence. Our findings highlight the importance of assessing the role of sex and marital status on the association between leisure activities and dementia risk, providing opportunities for tailored interventions to improve cognitive reserve capacity.
ACKNOWLEDGMENTS
The work was supported by the National Institute on Aging (grants R01AG7644-01A1 & RO1AG017644); Economic and Social Research Council (grant ES/S013830/1). The English Longitudinal Study of Ageing is funded by the National Institute on Aging (Grant R01AG7644) and by a consortium of UK government departments coordinated by the Economic and Social Research Council and the Office for National Statistics. The funding sources were not involved in the study design, analysis, and interpretation of data, writing of the report, nor in the decision to submit the article for publication. PA-M is supported by Alzheimer’s Society (grant 477, AS-PhD-18b-022). DC is supported by the Economic and Social Research Council (ESRC, Grant ES/T014091/1).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0952r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-200952.
REFERENCES
[1] | Ritchie H , Roser M ((2018) ) Causes of death. Our World in Data, https://ourworldindata.org/causes-of-death. |
[2] | Barulli D , Stern Y ((2013) ) Efficiency, capacity, compensation, maintenance, plasticity: Emerging concepts in cognitive reserve. Trends Cogn Sci 17: , 502–509. |
[3] | Stern Y ((2012) ) Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol 11: , 1006–1012. |
[4] | Verghese J , LeValley A , Derby C , Kuslansky G , Katz M , Hall C , Buschke H , Lipton RB ((2006) ) Leisure activities and the risk of amnestic mild cognitive impairment in the elderly. Neurology 66: , 821–827. |
[5] | Wang HX , Karp A , Winblad B , Fratiglioni L ((2002) ) Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: A longitudinal study from the Kungsholmen project. Am J Epidemiol 155: , 1081–1087. |
[6] | Fratiglioni L , Paillard-Borg S , Winblad B ((2004) ) An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol 3: , 343–353. |
[7] | Karp A , Paillard-Borg S , Wang HX , Silverstein M , Winblad B , Fratiglioni L ((2006) ) Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dement Geriatr Cogn Disord 21: , 65–73. |
[8] | Scarmeas N , Stern Y ((2003) ) Cognitive reserve and lifestyle. J Clin Exp Neuropsychol 25: , 625–633. |
[9] | Churchill JD , Galvez R , Colcombe S , Swain RA , Kramer AF , Greenough WT ((2002) ) Exercise, experience and the aging brain. Neurobiol Aging 23: , 941–955. |
[10] | Finkel D , Andel R , Pedersen NL ((2018) ) Gender differences in longitudinal trajectories of change in physical, social, and cognitive/sedentary leisure activities. J Gerontol Ser B Psychol Sci Soc Sci 73: , 1491–1500. |
[11] | Hu YH , Chiu CJ , Wong JD , Lin DC , Wray LA ((2018) ) The role of leisure activities in the relationship between marital transition in later midlife and psychological well-being trajectories. Int J Aging Hum Dev 86: , 327–346. |
[12] | Montgomery SS , Robinson MD ((2010) ) Empirical evidence of the effects of marriage on male and female attendance at sports and arts. Soc Sci Q 91: , 99–116. |
[13] | Fallahpour M , Borell L , Luborsky M , Nygård L ((2015) ) Leisure-activity participation to prevent later-life cognitive decline: A systematic review. Scand J Occup Ther 23: , 162–197. |
[14] | Steptoe A , Breeze E , Banks J , Nazroo J ((2013) ) Cohort profile: The English Longitudinal Study of Ageing. Int J Epidemiol 42: , 1640–1648. |
[15] | Quinn TJ , Fearon P , Noel-Storr AH , Young C , McShane R , Stott DJ ((2014) ) Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) for the diagnosis of dementia within community-dwelling populations. Cochrane Database Syst Rev, CD010079. |
[16] | Jorm AF ((1994) ) A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): Development and cross-validation. Psychol Med 24: , 145–153. |
[17] | Radloff LS ((1977) ) The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1: , 385–401. |
[18] | Fine JP , Gray RJ ((1999) ) A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94: , 496–509. |
[19] | Sommerlad A , Ruegger J , Singh-Manoux A , Lewis G , Livingston G ((2018) ) Marriage and risk of dementia: Systematic review and meta-analysis of observational studies. J Neurol Neurosurg Psychiatry 89: , 231–238. |
[20] | Yates LA , Ziser S , Spector A , Orrell M ((2016) ) Cognitive leisure activities and future risk of cognitive impairment and dementia: Systematic review and meta-analysis. Int Psychogeriatrics 28: , 1791–1806. |
[21] | Wilson RS , Barnes LL , Aggarwal NT , Boyle PA , Hebert LE , Mendes De Leon CF , Evans DA ((2010) ) Cognitive activity and the cognitive morbidity of Alzheimer disease. Neurology 75: , 990–996. |
[22] | Fancourt D , Steptoe A , Cadar D ((2018) ) Cultural engagement and cognitive reserve: Museum attendance and dementia incidence over a 10-year period. Br J Psychiatry 213: , 661–663. |
[23] | Ingemar K , Lennartsson C , Gatz M , Parker MG ((2011) ) Baseline leisure time activity and cognition more than two decades later. Int J Geriatr Psychiatry 26: , 65–74. |
[24] | Stoykova R , Matharan F ((2011) ) Impact of social network on cognitive performances and age-related cognitive decline across a 20-year follow-up. Int Psychogeriatr 23: , 1405–1412. |
[25] | Kuiper JS , Zuidersma M , Oude Voshaar RC , Zuidema SU , van den Heuvel ER , Stolk RP , Smidt N ((2015) ) Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev 22: , 39–57. |
[26] | Santabárbara J , Villagrasa B ((2020) ) Does depression increase the risk of dementia? Updated meta-analysis of prospective studies. Actas Españolas Psiquiatr 48: , 169–180. |
[27] | Derntl B , Seidel E , Eickhoff SB , Kellermann T , Gur C , Schneider F , Habel U , Derntl B , Seidel E , Eickhoff SB , Kellermann T , Derntl B , Seidel E , Eickhoff SB , Kellermann T , Gur RC , Schneider F , Habel U ((2011) ) Neural correlates of social approach and withdrawal in patients with major depression. Soc Neurosci 6: , 482–501. |
[28] | Krell-Roesch J , Feder NT , Roberts RO , Mielke MM , Christianson TJ , Knopman DS , Petersen RC , Geda YE ((2018) ) Leisure-time physical activity and the risk of incident dementia: The Mayo Clinic Study of Aging. J Alzheimers Dis 63: , 149–155. |
[29] | Jacobs JM , Hammerman-Rozenberg R , Cohen A , Stessman J ((2008) ) Reading daily predicts reduced mortality among men from a cohort of community-dwelling 70-year-olds. J Gerontol Ser B Psychol Sci Soc Sci 63: , 73–80. |
[30] | Lee Y , Chi I ((2016) ) Do cognitive leisure activities really matter in the relationship between education and cognition? Evidence from the aging, demographics, and memory study (ADAMS). Aging Ment Health 20: , 252–261. |
[31] | Ng TP , Lim ML , Niti M , Collinson S ((2012) ) Long-term digital mobile phone use and cognitive decline in the elderly. Bioelectromagnetics 33: , 176–185. |
[32] | Hughes TF , Chang CCH , Vander Bilt J , Ganguli M ((2010) ) Engagement in reading and hobbies and risk of incident dementia: The MoVIES project. Am J Alzheimers Dis Other Demen 25: , 432–438. |
[33] | d’Orsi E , Xavier AJ , Rafnsson SB , Steptoe A , Hogervorst E , Orrell M ((2018) ) Is use of the internet in midlife associated with lower dementia incidence? Results from the English Longitudinal Study of Ageing. Aging Ment Health 22: , 1525–1533. |
[34] | Eriksson Sörman D , Sundström A , Rönnlund M , Adolfsson R , Nilsson LG ((2014) ) Leisure activity in old age and risk of dementia: A 15-Year prospective study. J Gerontol Ser B Psychol Sci Soc Sci 69: , 493–501. |
[35] | Almeida-Meza P , Steptoe A , Cadar D ((2020) ) Markers of cognitive reserve and dementia incidence in the English Longitudinal Study of Ageing. Br J Psychiatry, doi: 10.1192/bjp.2020.54 |
[36] | Sommerlad A , Sabia S , Livingston G , Kivimäki M , Lewis G , Singh-Manoux A ((2020) ) Leisure activity participation and risk of dementia. Neurology 95: , e2803–e2815. |


