
Implementing Delirium Prevention in the Era of COVID-19
Abstract
Patients admitted with COVID-19 can develop delirium due to predisposing factors, isolation, and the illness itself. Standard delirium prevention methods focus on interaction and stimulation. It can be challenging to deliver these methods of care in COVID settings where it is necessary to increase patient isolation. This paper presents a typical clinical vignette of representative patients in a tertiary care hospital and how a medical team modified an evidence-based delirium prevention model to deliver high-quality care to COVID-19 patients. The implemented model focuses on four areas of delirium-prevention: Mobility, Sleep, Cognitive Stimulation, and Nutrition. Future studies will be needed to track quantitative outcome measures.
INTRODUCTION
The prevalence of delirium in inpatient medicine/surgical units is 15-50% and leads to significant short-term morbidity such as prolonged hospital stays, pressure ulcers, and falls [1–3]. Patients with the novel coronavirus (COVID-19) can have multiple neuropsychiatric sequelae including delirium [4–6]. The hospitalization of patients with COVID-19 has revealed additional challenges with delirium prevention [7]. Standard delirium prevention methods such as “4M” (What Matters, Medication, Mentation, and Mobility) [8] require frequent interaction. Personal protective equipment (PPE), isolation, and limited interactions with COVID-19 patients interferes with the initiation of these pathways. Patients may have baseline cognitive and memory difficulties which compound the negative consequences of isolation, novel medications, and the infection itself. The PPE that clinicians wear can be additionally disorienting for patients with baseline confusion and cognitive impairment symptoms.
Pre-COVID-19, researchers showed us that the etiology for delirium in most cases is multifactorial with specific predisposing risk factors, independent of precipitating factors such as acute incidents or iatrogenic events, increasing the susceptibility for this behavioral presentation [9]. Identified risk factors include advanced age with increased susceptibility in dementia, illness severity, vision impairment, urinary catheterization, low albumin, and length of hospital stay. Additional risk factors consist of physical restraints, sleep disturbance, immobility, urinary retention, dehydration, electrolyte abnormalities, polypharmacy, and infection [10, 11].
For these reasons, our pre-COVID-19 tertiary care hospital had been focusing on these factors for delirium prevention and particularly for adults age 65 or older [12, 13]. The team had existing strategies for delirium prevention upon admission—with this even including screening for cognitive impairment [13]. There were also dedicated geriatric resource nurses providing inpatient interaction, and inclusion of volunteers to engage patients in interactive activities, and focus time toward mobility and maintaining daytime wakefulness. Medical teams also encouraged family members to be at the bedside to help re-orient patients.
COVID-19, however, rapidly altered our Florida based hospital’s pre-existing delirium intervention and management efforts [14]. The infection poses a risk with potential direct CNS infection or inflammation, cerebral vascular incident, hypoxia, pyrexia, and ventilation with sedation [15]. Another contributing factor was isolation from family and reduction in staff interaction in attempts to conserve PPE and risk for exposure given unknown mode of transmission at the time. Isolation limited cognitive stimulation and mobility and reduced a significant component of nonpharmacological methods of delirium prevention and management [16]. PPE including masks, face shields, and gowns were not only impersonal but visually overwhelming and limited clear, audible communication to patients and families [17]. Furthermore, the risk for polypharmacy, QTc prolongation, hypoglycemia, and multiple drug interactions was increased with the use of hydroxychloroquine during the initial treatment trials for COVID infection [18]. Required COVID-19 isolation procedures revealed, for our team, highly concerning changes in patient behaviors and a need for urgent multidisciplinary team adaptation.
The present report highlights: 1) a case necessitating team reorganization during the early months of the pandemic, and 2) how the team adapted a delirium during the time of COVID-19 in order to maintain holistic patient-centered care.
CLINICAL VIGNETTE
A 77-year-old male with Alzheimer’s disease presented to the emergency department after being found unresponsive in a nursing home facility. At baseline, he was oriented only to self with fluent but nonsensical speech and intermittently following commands. At the nursing facility, his medications included donepezil 5 mg daily, mirtazapine 15 mg nightly, and quetiapine 50 mg BID. On exam, the patient had a Glasgow Coma Scale [19] of 10 with no asymmetry. A computed tomography (CT) scan and computed tomography angiography (CTA) brain scan with a stroke protocol showed no new ischemia. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was detected by nasal swab.
Hospital course
The patient was admitted with a diagnosis of COVID-19 related encephalopathy. Per the treatment guidance, at the time, after consultation with infectious disease, the patient was started on hydroxychloroquine. He had baseline prolonged corrected QT interval (QTc; 491 ms), so his quetiapine and mirtazapine were stopped. The patient was placed on continuous pulse oximetry, telemetry for QTc monitoring. To preserve PPE and minimize interactions, he had a urinary and fecal management system placed. The patient did not develop respiratory symptoms but did manifest waxing and waning severe agitation alternating with somnolence. The patient was not compliant with the recommended mask-wearing and was violent with staff with episodes of spitting. Family visitation was not possible and maintaining daytime wakefulness was difficult as staff had to don full PPE to see the patient. The patient’s delirium worsened and he required restraints for patient and staff safety. This clinical vignette is an example of the challenges our team faced during the early months of the COVID-19 pandemic.
COVID-19 DELIRIUM PREVENTION PROJECT METHODS
As exemplified in the above case, delirium was a significant issue for our team. Many individuals were admitted to our hospital were arriving from nursing homes with known risk factors for delirium, such as reduced cognitive status [20]. Although a review of data using qualitative review records (UF Office of Clinical Quality & Patient Safety Record Review approval #1382) reports only 7% of inpatients during the months of the pandemic had a formal ICD-10 [21] diagnosis of dementia, research reports a poor correlation between hospital code records and actual dementia presence [22]; cognitive impairment is likely higher (up to 20%) within the community [23] and hospital settings [13, 24]. Additionally, due to PPE and visit restrictions, it was challenging to continue many of pre-existing interventions (e.g., maintaining daytime wakefulness, frequent re-orientation). Mobility was limited as many patients had a concomitant fall risk and so could not sit in a chair unsupervised in isolation. Family members were also under visitor restrictions.
While some patient factors may not be modifiable, research shows that delirium can be preventable [25, 26]. Consequently, COVID floor front-line physicians and nurses approached physician, delirium researchers, and nursing leadership to identify resources to deliver evidence-based methods for delirium prevention [27]. Via collaboration with nursing leadership and clinical leader registered nurses redeployed from other floors, the teams added national management suggestions [28] and implemented a novel delirium prevention project for COVID-19 patients. In the early days of the pandemic, the Persons Under Investigation (PUIs) were also under isolation and so this project applied to those patients since it often took days for the SARS-CoV-2 test to result. This has become less of an issue now that the test results within hours so the project has now become limited to COVID-19 patients. The delirium prevention project focuses on key nursing interventions intended to maximize function, maintain or improve cognition, and support adequate nutrition (Fig. 1). Teams provided the following to all non-ICU patients with confirmed positive tests for COVID.
Fig. 1
Figure demonstrating the delirium prevention project. A “delirium prevention champion” is a nursing staff member who addresses these four interventions on a daily basis for COVID positive patients.
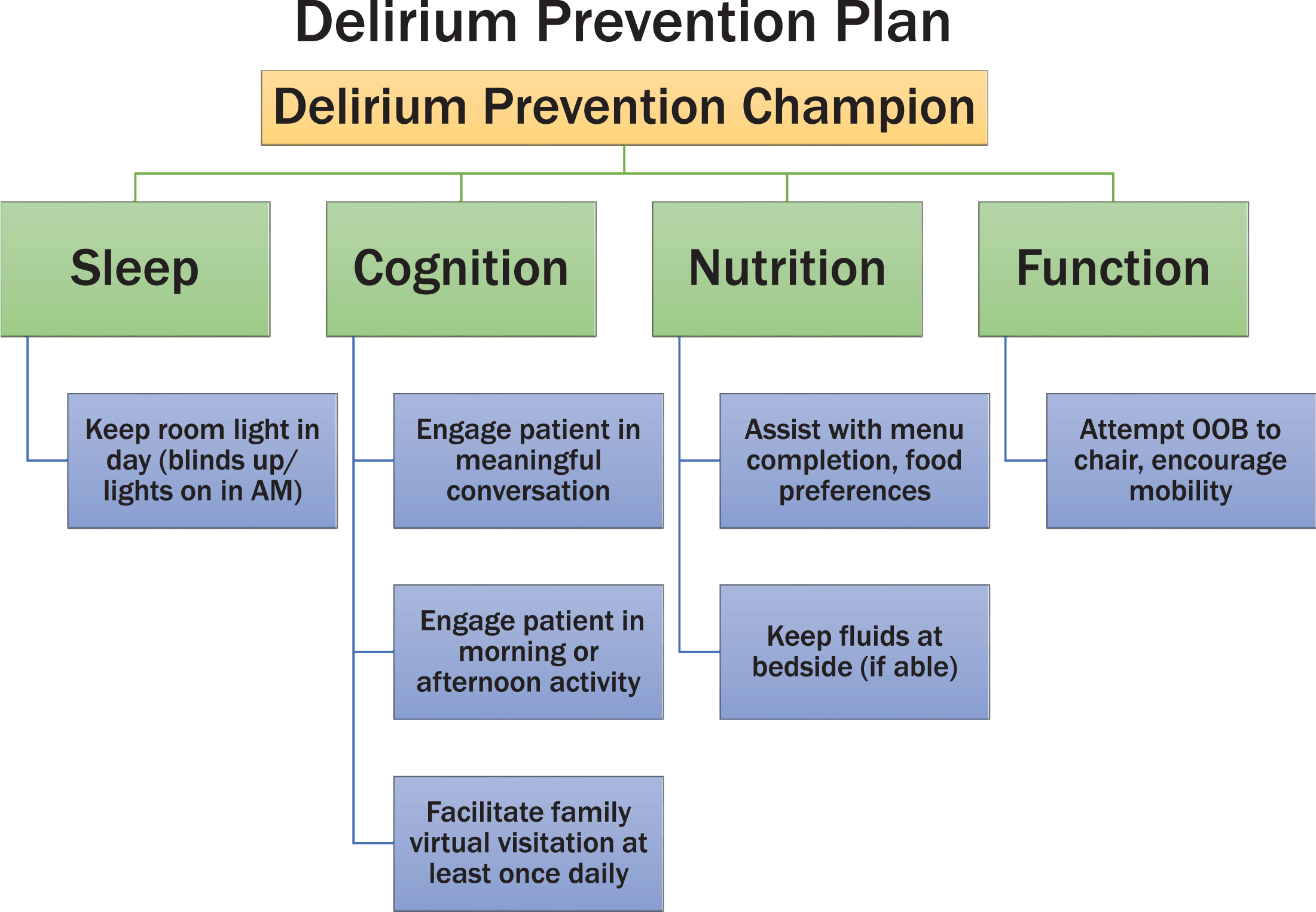
Specialized delirium prevention rounds were created and implemented (Fig. 1) to begin at 0800 and include an introduction and an explanation of role and purpose. Four patient plans were created centering on the following:
Mobility
Patients are offered mobility assistance to exit the bed and sit in the chair or walk. The delirium prevention champion stays with the patient in order to minimize fall risks. Mobility assistance was offered daily and took place in the room for infection control purposes.
Sleep
Lights are adjusted to normal day-light stimulation and blinds remain open until evening.
Cognitive stimulation
This involves three components: 1) Offer of an engaging activity including art supplies (paints, crayons, colored pencils, sketchpads), books, puzzles, movies, or music; 2) Video-conference relaxation sessions, visual arts, music therapy, and creative writing sessions provided by arts-in-medicine team; 3) Participation in a phone call or video conference with a family member or friend. Patients were offered choices of the cognitive activities and could choose more than one.
Nutrition
Face-to-face meal ordering is no longer possible, and so orders are taken by phone. Older adult patients are at times unable to answer the phone, hear the caller due to hearing impairment, fail to understand their meal options, or have difficulty reading the menu due to visual difficulties or cognitive impairment. Patients with dementia or delirium could not order appropriate meals for their optimal nutrition. Rounds offering meal ordering assistance stimulate patient engagement in the meal ordering process and foster optimal intake.
DISCUSSION
COVID patients and the healthcare teams are facing unique challenges together. Extensive PPE requirements and lack of visitation has resulted in a rare form of increased isolation and delirium risk for individuals of all ages, but particularly older adults [7]. Family visitation has been limited or eliminated for COVID-19 hospitalized patients. National guidelines have been published for COVID-19 management [28] and delirium management suggestions provided by national experts [27]. Despite this, hospital teams still face an unprecedented challenge to mitigating patient isolation and decreasing delirium. While some risk factors for delirium cannot be modified, environmental precipitating factors can be modified. The four care areas that the team focused on: mobility, sleep, cognitive stimulation, and nutrition are some of the areas with modifiable risk factors. Individuals with Alzheimer’s disease or related dementias are at particular risk for delirium [29–31]. Healthcare teams will need to identify models of care to mitigate delirium risk in these older adults who will be increasing exponentially in the years to come [32].
Our team identified that routine daily rounds, family connection via video platforms, and face-to-face meal ordering were preventative measures for delirium. While we did not collect data or surveys due to the rapidly evolving nature of COVID-10 care in the past six months, patients and families have commented on the unique psychological and emotional support that family video-conferencing has provided. Family members can assist with orientation and a sense of well-being, and provide patient information regarding likes, dislikes, food preferences, and activity preferences. Although qualitative, we observed an increase in meal consumption and improved mobility status even among confused patients. Staff members also verbally reported an improved sense of control and closeness to patients.
For the clinical vignette described above, once the hydroxychloroquine was completed, the patient was placed back on outpatient medications. He slowly improved and returned to the nursing home after a 16 day length-of-stay. While hydroxychloroquine is no longer being used routinely, patients are now receiving dexamethasone which is known to cause delirium [33, 34].
The ongoing COVID-19 pandemic has greatly impacted patients and the direct bedside care providers. The highly contagious nature of the disease process has made care providers consider novel initiatives to help meet the needs of COVID positive patients while protecting clinical staff from infection. Additionally, the early recommend treatment for these patients with anti-viral medications made standard pharmacologic psychotropic medications even more dangerous due to arrhythmia risk. We were challenged to manage this with rapid cycle changes. We had certain factors in place which facilitated the modification of our delirium prevention program. One was the existing focus on delirium-prevention and previous expertise in delirium prevention. The other factor was the existing collaboration between and nursing and physician leadership as this enabled rapid implementation of the modified program. Finally, during the early days of the pandemic, certain hospital services such as elective surgery were paused. This allowed us to re-deploy nurses from other units to participate as delirium-prevention champions on the COVID unit. Now that all services have been re-opened, nurses on the COVID unit have been designated and trained as delirium-prevention champions. We experienced some barriers to implementation of this program. The main limitation was the ability of family members to have access to a platform for video-conferencing and also knowledge of how to use the platforms for video-conferencing. The delirium prevention champions had to spend extra time to teach patients’ family members how to use the video-conferencing platforms. Another limitation to mobility was that patients with COVID-19 could not walk in the hallway. Thus their mobility was limited to within the hospital room.
For next steps, nursing and physical therapy are coordinating a mobility/sensory activity room staffed by physical therapy and nursing staff to benefit COVID positive patients. These and other innovative compassionate patient-care methods will need to be developed to meet the challenges of the COVID-19 pandemic. Our model highlights that innovation and partnership with nursing and other clinical disciplines can result in improved patient care through rapid-cycle intervention.
As noted in a recent letter, “Mitigating delirium during this chaotic time is possible with interdisciplinary teamwork and flexibility in roles” [35]. The present report summarizes a hospital team’s response to actively prevent delirium for COVID-19 patients on an in-patient medical floor. The team strategically implemented delirium prevention rounds incorporating cognitive and nutrition modifications. It remains unknown if the modifications will remain once COVID-19 cases reduce and staff members are reduced.
Given the increasing numbers of older adults entering hospitals and the likelihood of additional viral waves, we now need prospective research to address the value of these interventions for the near and long-term particularly for patients with Alzheimer’s disease.
ACKNOWLEDGMENTS
The authors wish to thank Wanda Whittet RN for her assistance with this project.
This work was conducted at the University of Florida. Sources of funding include NIH K07AG066813 (CP) and UL1TR001427 (CTSA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging or the National Institutes of Health.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0696r2).
REFERENCES
[1] | Inouye SK , Westendorp RG , Saczynski JS ((2014) ) Delirium in elderly people. Lancet 383: , 911–922. |
[2] | Bellelli G , Frisoni GB , Turco R , Lucchi E , Magnifico F , Trabucchi M ((2007) ) Delirium superimposed on dementia predicts 12-month survival in elderly patients discharged from a postacute rehabilitation facility. J Gerontol A Biol Sci Med Sci 62: , 1306–1309. |
[3] | Fick DM , Steis MR , Waller JL , Inouye SK ((2013) ) Delirium superimposed on dementia is associated with prolonged length of stay and poor outcomes in hospitalized older adults. J Hosp Med 8: , 500–505. |
[4] | Troyer EA , Kohn JN , Hong S ((2020) ) Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav Immun 87: , 34–39. |
[5] | Ticinesi A , Cerundolo N , Parise A , Nouvenne A , Prati B , Guerra A , Lauretani F , Maggio M , Meschi T ((2020) ) Delirium in COVID-19: Epidemiology and clinical correlations in a large group of patients admitted to an academic hospital. Aging Clin Exp Res 32: , 2159–2166. |
[6] | Zazzara MB , Penfold RS , Roberts AL , Lee KA , Dooley H , Sudre CH , Welch C , Bowyer RCE , Visconti A , Mangino M , Freydin MB , El-Sayed Moustafa JS , Small K , Murray B , Modat M , Wolf J , Ourselin S , Graham MS , Martin FC , Steves CJ , Lochlainn MN ((2020) ) Probable delirium is a presenting symptom of COVID-19 in frail, older adults: A cohort study of 322 hospitalised and 535 community-based older adults. Age Ageing, doi: 10.1093/ageing/afaa223 |
[7] | O’Hanlon S , Inouye SK ((2020) ) Delirium: A missing piece in the COVID-19 pandemic puzzle. Age Ageing 49: , 497–498. |
[8] | Institute for Healthcare Improvement (IHI) ((2019) ) Age-Friendly Health Systems: Guide to Using the 4Ms in the Care of Older Adults. Age-Friendly Health Systems. John A. Hartford Foundation and Institute for Healthcare Improve-ment in partnernship with American Hospital Association and Catholic Health Association of the United States. https://www.aha.org/system/files/media/file/2019/07/IHIAgeFriendlyHealthSystems_GuidetoUsing4MsCare.pdf. |
[9] | Inouye SK , Charpentier PA ((1996) ) Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 275: , 852–857. |
[10] | Ahmed S , Leurent B , Sampson EL ((2014) ) Risk factors for incident delirium among older people in acute hospital medical units: A systematic review and meta-analysis. Age Ageing 43: , 326–333. |
[11] | Inouye SK , Viscoli CM , Horwitz RI , Hurst LD , Tinetti ME ((1993) ) A predictive model for delirium in hospitalized elderly medical patients based on admission characteristics. Ann Intern Med 119: , 474–481. |
[12] | Fulmer TT ((2019) ) Nurses Improving Care for Healthsystems Elders, Springer Publishing, New York. |
[13] | Amini S , Crowley S , Hizel L , Arias F , Libon DJ , Tighe P , Giordano C , Garvan CW , Enneking FK , Price CC ((2019) ) Feasibility and rationale for incorporating frailty and cognitive screening protocols in a preoperative anesthesia clinic. Anesth Analg 129: , 830–838. |
[14] | Miglietta A , Levi M ((2020) ) Documented early circulation of Coronavirus Disease 2019 (COVID-19) in Florida, USA, since February 2020. J Public Health (Oxf) 42: , 517–518. |
[15] | Asadi-Pooya AA , Simani L ((2020) ) Central nervous system manifestations of COVID-19: A systematic review. J Neurol Sci 413: , 116832. |
[16] | Hshieh TT , Yue J , Oh E , Puelle M , Dowal S , Travison T , Inouye SK ((2015) ) Effectiveness of multicomponent nonpharmacological delirium interventions: A meta-analysis. JAMA Intern Med 175: , 512–520. |
[17] | Emmerton D , Abdelhafiz A ((2020) ) Delirium in older people with COVID-19: Clinical scenario and literature review. SN Compr Clin Med, doi: 10.1007/s42399-020-00474-y |
[18] | Ross SB , Wilson MG , Papillon-Ferland L , Elsayed S , Wu PE , Battu K , Porter S , Rashidi B , Tamblyn R , Pilote L , Downar J , Bonnici A , Huang A , Lee TC , McDonald EG ((2020) ) COVID-SAFER: Deprescribing guidance for hydroxychloroquine drug interactions in older adults. J Am Geriatr Soc 68: , 1636–1646. |
[19] | Teasdale G , Jennett B ((1974) ) Assessment of coma and impaired consciousness. A practical scale. Lancet 2: , 81–84. |
[20] | Oresanya LB , Lyons WL , Finlayson E ((2014) ) Preoperative assessment of the older patient: A narrative review. JAMA 311: , 2110–2120. |
[21] | American Health Information Management Association ICD-10-CM code book for physicians. American Health Information Management Association, Chicago, IL. |
[22] | Cummings E , Maher R , Showell CM , Croft T , Tolman J , Vickers J , Stirling C , Robinson A , Turner P ((2011) ) Hospital coding of dementia: Is it accurate? Health Inf Manag 40: , 5–11. |
[23] | Luck T , Then FS , Schroeter ML , Witte V , Engel C , Loeffler M , Thiery J , Villringer A , Riedel-Heller SG ((2017) ) Prevalence of DSM-5 mild neurocognitive disorder in dementia-free older adults: Results of the population-based LIFE-Adult-Study. Am J Geriatr Psychiatry 25: , 328–339. |
[24] | Culley DJ , Flaherty D , Reddy S , Fahey MC , Rudolph J , Huang CC , Liu X , Xie Z , Bader AM , Hyman BT , Blacker D , Crosby G ((2016) ) Preoperative cognitive stratification of older elective surgical patients: A cross-sectional study. Anesth Analg 123: , 186–192. |
[25] | Bjorkelund KB , Hommel A , Thorngren KG , Gustafson L , Larsson S , Lundberg D ((2010) ) Reducing delirium in elderly patients with hip fracture: A multi-factorial intervention study. Acta Anaesthesiol Scand 54: , 678–688. |
[26] | Boltz M , Capezuti L , Fulmer TT , Zwicker D ((2020) ) Evidence-based geriatric nursing protocols for best practice. Springer Publishing Company, New York. |
[27] | The Hospital Elder Life Program ((2020) ) COVID-19 and Delirium: HELP Resources. The Hospital Elder Life Program, https://www.hospitalelderlifeprogram.org/news/covid-19-and-delirium-help-resources/, |
[28] | National Institute for Health and Care Excellence (NICE) in collaboration with NHS England and NHS Improvement ((2020) ) Managing COVID-19 symptoms (including at the end of life) in the community: Summary of NICE guidelines. BMJ 369: , m1461. |
[29] | Fong TG , Tulebaev SR , Inouye SK ((2009) ) Delirium in elderly adults: Diagnosis, prevention and treatment. Nat Rev Neurol 5: , 210–220. |
[30] | Oh ES , Fong TG , Hshieh TT , Inouye SK ((2017) ) Delirium in older persons: Advances in diagnosis and treatment. JAMA 318: , 1161–1174. |
[31] | Fong TG , Vasunilashorn SM , Libermann T , Marcantonio ER , Inouye SK ((2019) ) Delirium and Alzheimer disease: A proposed model for shared pathophysiology. Int J Geriatr Psychiatry 34: , 781–789. |
[32] | He Z , Bian J , Carretta HJ , Lee J , Hogan WR , Shenkman E , Charness N ((2018) ) Prevalence of multiple chronic conditions among older adults in Florida and the United States: Comparative analysis of the OneFlorida Data Trust and National Inpatient Sample. J Med Internet Res 20: , e137. |
[33] | O’Keeffe ST , Devlin JG ((1994) ) Delirium and the dexamethasone suppression test in the elderly. Neuropsychobiology 30: , 153–156. |
[34] | RECOVERY Collaborative Group, Horby P , Lim WS , Emberson JR , Mafham M , Bell JL , Linsell L , Staplin N , Brightling C , Ustianowski A , Elmahi E , Prudon B , Green C , Felton T , Chadwick D , Rege K , Fegan C , Chappell LC , Faust SN , Jaki T , Jeffery K , Montgomery A , Rowan K , Juszczak E , Baillie JK , Haynes R , Landray MJ ((2020) ) Dexamethasone in hospitalized patients with Covid-19 - preliminary report. N Engl J Med, doi: 10.1056/NEJMoa2021436 |
[35] | LaHue SC , James TC , Newman JC , Esmaili AM , Ormseth CH , Ely EW ((2020) ) Collaborative delirium prevention in the age of COVID-19. J Am Geriatr Soc 68: , 947–949. |


