
Factors Associated with Lumbar Puncture Participation in Alzheimer’s Disease Research
Abstract
Background:
Cerebrospinal fluid (CSF) provides insight into the spectrum of Alzheimer’s disease (AD) pathology. While lumbar punctures (LPs) for CSF collection are generally considered safe procedures, many participants remain hesitant to participate in research involving LPs.
Objective:
To explore factors associated with participant willingness to undergo a research LP at baseline and follow-up research study visit.
Methods:
We analyzed data from 700 participants with varying cognition (unimpaired, mild cognitive impairment, and dementia) in the Wisconsin Alzheimer’s Disease Research Center. We evaluated the relationship of demographic variables (age, sex, race, ethnicity, and years of education) and clinical variables (waist-to-hip ratio, body mass index, AD parental history, cognitive diagnosis) on decision to undergo baseline LP1. We evaluated the relationship of prior LP1 experience (procedure success and adverse events) with the decision to undergo follow-up LP2. The strongest predictors were incorporated into regression models.
Results:
Over half of eligible participants opted into both baseline and follow-up LP. Participants who underwent LP1 had higher mean education than those who declined (p = 0.020). White participants were more likely to choose to undergo LP1 (p < 0.001); 33% of African American participants opted in compared to 65% of white participants. Controlling for age, education, and AD parental history, race was the only significant predictor for LP1 participation. Controlling for LP1 mild adverse events, successful LP1 predicted LP2 participation.
Conclusion:
Race was the most important predictor of baseline LP participation, and successful prior LP was the most important predictor of follow-up LP participation.
INTRODUCTION
Lumbar punctures (LP) for cerebrospinal fluid (CSF) collection are a crucial component of Alzheimer’s disease (AD) prevention research. The National Institute on Aging and the Alzheimer’s Association (NIA-AA) research framework for staging AD is based on the presence or absence of AD biomarkers amyloid-β and tau proteins in the brain [1]. LP in addition to amyloid and tau positron emission tomography (PET) imaging provide AD-relevant information. However, LPs are less expensive, less time-consuming to perform, can be readily obtained in clinical settings, and provide information regarding both amyloid and tau, as well as other features of the AD pathological cascade such as neurodegeneration and gliosis [2]. Further, LPs have been established as a safe, well-tolerated procedure with minimal risk and adverse side effects, especially when performed with atraumatic, smaller-gauge Sprotte needles to collect less than 30 mL of CSF with the participant in a seated position [3–8].
Despite the overall safety and research utility of LP, recruiting participants to undergo an elective LP for research presents challenges. A survey of prospective research participants found that while 75% were willing to participate in a study that did not include an LP, only 64% were willing to participate in an identical study that included an LP [9]. Some people may have a stronger willingness to undergo an LP for clinical purposes, such as early diagnosis or individual therapies, than for research purposes [10]. Additionally, increased education about AD and the utility of CSF biomarkers for AD research does not improve a research subjects’ willingness to participate in a research LP [10].
Individuals from underrepresented groups (URGs) in particular have expressed reluctance to participate in clinical research. African Americans are more concerned about undergoing an LP than white participants and are less likely to participate in research studies due to this concern [11, 12]. Many research participants remain acutely aware of the history of medical researchers exploiting and abusing African Americans, from the Tuskegee syphilis study to even more recent ethical research violations at well-known academic institutions [13, 14]. Focus groups of African Americans weighing participation in research have cited mistrust of the medical establishment, fear of complications or injury, lack of benefit for their community and low compensation as reasons to decline participation. [11–13, 15].
While there is preliminary research regarding factors associated with LP research participation [16], there are limited studies to date that have examined potential contributing factors to participation in longitudinal CSF collection [7]. The first objective of this study was to investigate whether specific demographic or clinical factors were associated with a participant’s decision to undergo an elective lumbar puncture at the baseline visit (LP1) of a longitudinal observational research study. The second objective was to explore the association between LP1 success or adverse event occurrence and the participant’s decision to have a second elective lumbar puncture at a subsequent study visit (LP2).
METHODS
Study sample
The Wisconsin Alzheimer’s Disease Research Center (ADRC) Clinical Core is a single-center, longitudinal observational study. The study is under the purview of the University of Wisconsin Health Sciences Institutional Review Board and all activities are conducted in accordance with their ethical standards. Participants attend annual or biennial clinical visits for cognitive evaluation accompanied by a study partner and biennial biomarker visits for an MRI scan and an LP. While clinical visits and biomarker visits do not occur on the same day, each biomarker visit is associated with a clinical visit at which a cognitive diagnosis is determined.
The Clinical Core is composed of three cohorts: individuals with dementia, individuals with mild cognitive impairment (MCI), and cognitively unimpaired adults ages 45 and older both with and without parental history of dementia. Research personnel obtain informed consent from all participants, and LPs are not performed on persons without decisional capacity. Over a quarter of participants are referred to the Clinical Core by a healthcare provider, one-quarter are referred by friends, family, and other research participants, and the remainder are recruited through media promotions, public outreach events, and partner organizations including the Alzheimer’s Association and the Alzheimer’s and Dementia Alliance of Wisconsin.
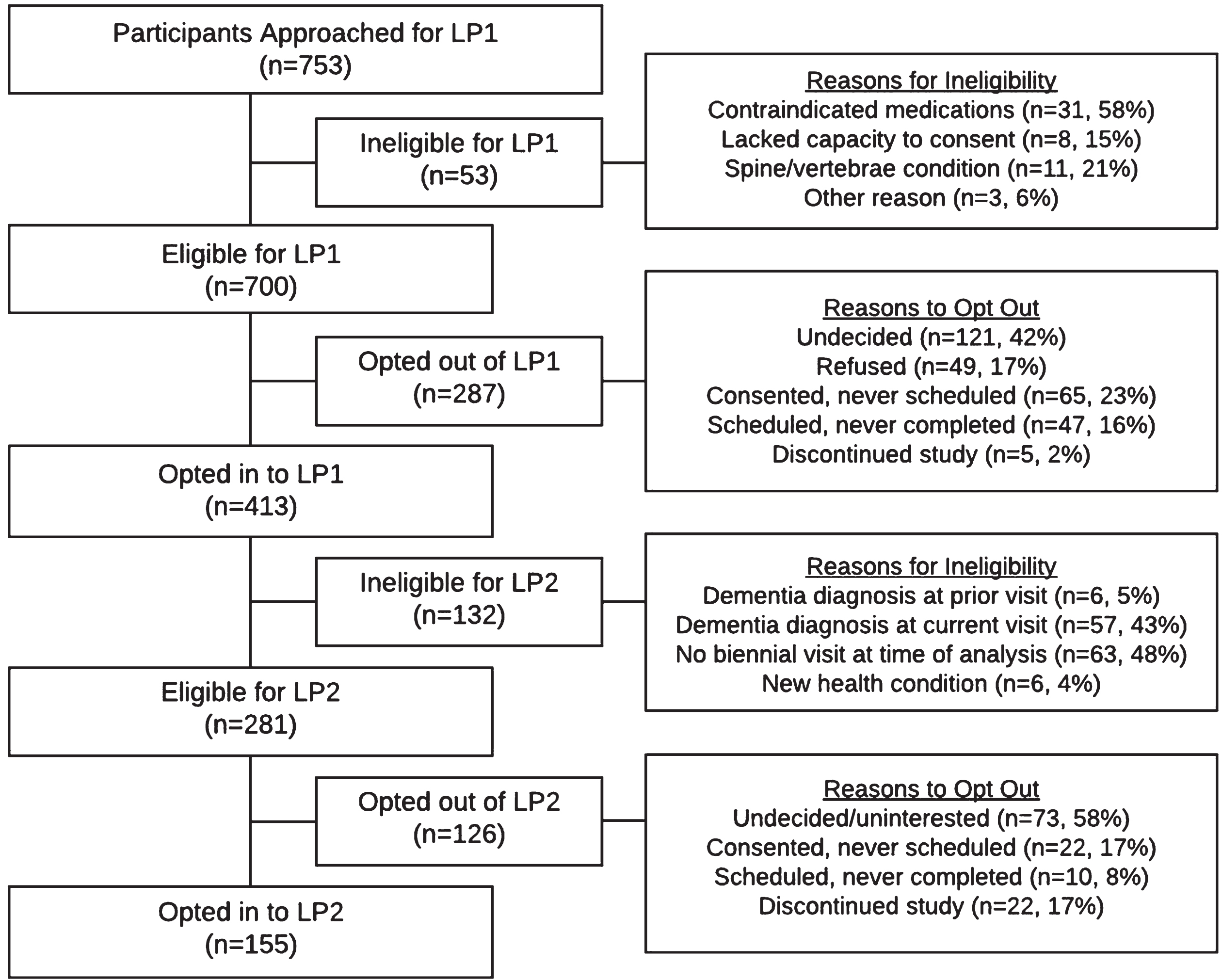
This analysis includes 753 individuals for whom LP participation was an optional procedure upon enrollment, 700 of whom were eligible for the procedure (see Fig. 1 for study flowchart and reasons for ineligibility). Only participants who enrolled in the study when LPs were an optional component of study participation were included. LP participation was an optional procedure for all participants who had their baseline clinical visit on or before October 1, 2015; after this date, only participants with dementia and individuals from URGs (across all cohorts) could opt out of the procedure. Thus, to include only participants with the choice to undergo an LP, the analyses included all participants from URGs, all participants with dementia, and all non-URG participants who completed their baseline clinical visit before October 1, 2015. The Clinical Core defines URGs according to the NIH definition: Blacks or African Americans, Hispanics or Latinos, American Indians or Alaska Natives, Native Hawaiians, and other Pacific Islanders [17].
Fig. 1
Flowchart of LP participation including reasons for participant ineligibility and reasons participants opted out of LP1 and LP2.
For clinical factors incorporated in this analysis, waist-hip ratio (WHR) was calculated by measuring the circumference around the smallest part of the participant’s waist and dividing by the largest circumference around the participant’s hips. The body-mass index (BMI) was calculated by dividing a participant’s weight in kilograms by the square of the participant’s height in meters. AD parental history was determined using the Dementia Questionnaire [18]. Cognitive diagnosis (unimpaired, MCI, dementia) was determined using expert consensus panel incorporating clinical and cognitive data into the assessment.
Study exclusions
For inclusion in the analysis of LP1 participation, a participant’s first LP had to be associated with their baseline clinical visit. For inclusion in the analysis of LP2 participation, a participant had to both complete LP1 and have their second LP associated with either their third or fourth annual clinical visit.
Participants diagnosed with dementia at their baseline clinical visit were invited for an optional baseline LP, but were not invited for a follow-up LP per study protocol, given the Center’s emphasis on preclinical biomarkers. Participants diagnosed with dementia at follow-up clinical visits were also excluded from the associated biomarker visit that year. Thus, participants with a dementia diagnosis are included in the analysis of LP1 data only.
Exclusion criteria for LP included use of contraindicated medications, such as anti-coagulants, significant spinal/vertebral conditions or surgeries, and lack of capacity to consent. Participants who were ineligible for LP1 participation were not included in the analysis. Participants who reported new exclusionary health conditions at their follow-up visit or received a diagnosis of dementia between biomarker visits were deemed ineligible for LP2 participation and excluded from the current analysis.
Lumbar puncture protocol
LPs were performed by either a licensed physician or a nurse practitioner. The extensive training process for nurse practitioners to independently perform LPs includes didactic-style learning, shadowing opportunities, and simulated LPs using a training manikin. For credentialing, nurse practitioners must perform their first ten LPs on study participants under supervision of a credentialed clinician and their application must undergo a multi-step review process with a credentialing committee in the University of Wisconsin Hospitals and Clinics before the practitioner is granted privileges to independently perform LPs.
LPs were performed in the morning following a minimum 8 h fast. CSF was collected in the L4-5 or L3-4 interspace via a gentle aspiration method with participants in the seated position (or lateral decubitus position for those prone to vasovagal symptoms). Up to 22 mL of fluid was collected using 24- or 25-gauge Sprotte atraumatic needles. Any CSF collection volume greater than 3 mL was considered a successful procedure. Following the procedure, participants lay supine for 20 min. The clinician performing the procedure advised participants to refrain from strenuous activity for 48 h following the procedure, remain well-hydrated, and use caffeine and pain relievers such as acetaminophen for any post-procedure headache.
Study personnel (clinician or study coordinator) contacted participants 24 h after the procedure and documented any adverse events. Adverse events were categorized as severe, moderate, or mild. Severe adverse events required further medical attention, such as a blood patch for a post-LP headache. Moderate adverse events were a headache or low back pain that began the night of the procedure or the following day, required sustained use of pain medication to control symptoms or resulted in an inability to perform normal activities. Mild adverse events included transient radiculopathy; pain or discomfort during the procedure; vasovagal response that resolved prior to completion of the biomarker visit; and transient headache or low-back pain that began and ended while the participant was at the visit.
Statistical methods
Statistical analyses were run using IBM SPSS Statistics (Version 26). To investigate associations between demographic or clinical factors and LP participation, independent T-tests between the groups who opted in and out of the procedure were conducted for each of the following continuous measures: age; WHR; years of education; and BMI. For categorical variables, chi-square tests were conducted for race (white, African American, and other); gender; parental history of AD; clinical consensus diagnosis (dementia, MCI, or cognitively unimpaired) and a Fisher’s exact test for ethnicity (Hispanic or non-Hispanic). Variables with p-values <0.2 from the univariate analyses were included in a multivariable logistic regression to investigate their association with LP1 participation while controlling for the other variables in the model. As a follow-up analysis to understand why years of education becomes insignificant in the multivariable logistic regression, the race difference in years of education was tested using a one-way ANOVA with Tukey’s post-hoc test.
To investigate the association between LP1 experience and participation in follow-up LP, chi-square analyses were conducted for each of the following measures: success of first LP (>3 mL CSF collected), moderate headache following LP1, and mild adverse events reported following LP1. Due to the small sample size of participants experiencing low back pain, a Fisher’s exact test was conducted to evaluate association between moderate low back pain and LP2 participation. Variables with p-values <0.2 from the univariate analyses were included in a multivariable logistic regression to investigate their association with LP2 participation.
RESULTS
Study sample
The study population comprised middle-aged to older adults, ranging from 43–94 years of age. The majority were white, women, cognitively unimpaired, and had a parental history of AD dementia (Table 1). While 753 participants were screened for LP at baseline, only 700 were eligible to undergo the procedure. Figure 1 displays the number of participants who opted in for each research LP and the factors associated with ineligibility or opting out of the procedure. Participants were included in the opt-out categories for each LP for the following reasons: undecided regarding LP participation, refused LP participation, consented to the procedure but never scheduled their visit, scheduled their visit but did not attend their visit, or discontinued their Clinical Core participation prior to biomarker visit (Fig. 1).
Table 1
Descriptive statistics for all participants eligible for optional LP1 and for participants grouped by decision to undergo LP1
| Participant Demographics | All participants eligible for LP1 | Opted In for LP1 | Opted Out of LP1 | P* (opt in versus opt out) |
| (n = 700) | (n = 413, 59%) | (n = 287, 41%) | ||
| Age [mean, (SD)] | 64.2 (10.3) | 63.7 (9.6) | 64.8 (11.2) | 0.174 |
| Sex [n female, (%)] | 428 (61.1) | 246 (59.5) | 182 (63.4) | 0.304 |
| Race [n, (%)] | ||||
| White | 555 (79.3) | 360 (87.2) | 195 (67.9) | < 0.0001 |
| African American | 123 (17.6) | 41 (9.9) | 82 (28.6) | |
| Other | 22 (3.1) | 12 (2.9) | 10 (3.5) | |
| Hispanic ethnicity [n, (%)] | 6 (1) | 4 (0.01) | 2 (0.01) | 0.651 |
| Parental History of AD [n, (%)] | 402 (57.4) | 246 (60.0) | 156 (57.8) | 0.170 |
| Years of Education [mean, (SD)] | 15.6 (2.8) | 15.8 (2.7) | 15.3 (2.9) | 0.020 |
| Waist-to-Hip Ratio [mean, (SD)] | 0.91 (0.095) | 0.91 (0.09) | 0.91 (0.1) | 0.451 |
| Body Mass Index [mean, (SD)] | 29.3 (6.2) | 29.1 (5.8) | 29.6 (6.8) | 0.396 |
| Diagnosis [n, (%)] | ||||
| Cognitively Unimpaired | 493 (70.4) | 299 (72.4) | 194 (68.6) | 0.367 |
| Mild Cognitive Impairment | 104 (14.9) | 56 (13.6) | 48 (16.7) | |
| Dementia | 103 (14.7) | 58 (14.0) | 45 (15.7) | |
| LP1 Success [n, (%)] | 366 (88.6) | N/A |
*The p-value reflects the results from the independent T-test (age, years of education, waist-to-hip ratio, body mass index); Chi-square analysis (sex, race, parental history of AD, diagnosis); and Fisher’s exact test (Hispanic ethnicity.).
LP1 participation
Of the 700 participants eligible for the procedure, 59.0% opted in with an LP success rate of 88.6%. A comparison of demographic and clinical variables for participants who opted in versus who opted out for LP1 is summarized in Table 1. The participants who opted into the baseline procedure were disproportionately more likely to be white and have higher mean years of education. URG participants comprised 22.5% of the cognitively unimpaired group, 26.0% of the MCI group, but only 6.0% of the dementia cohort. While African American participants comprised 17.6% of eligible participants for LP1, they represented only 9.9% of the opt-in group and 28.6% of the opt-out group. In comparison, white participants comprised 79.3% of the total LP1-eligible population but represented 87.2% of the opt-in group and 67.9% of the opt-out group. Overall, one-third of eligible African American participants opted into LP1, compared to 65.0% of eligible white participants (Table 1).
A logistic regression testing race, parental history, education, and age indicated that race was a significant predictor of LP1 participation, where white was the default variable and nonwhite participants were less likely than white participants to participate (OR = 0.742, [95% CI 0.675–0.817], p < 0.0001; χ2 for model fit = 0.229). Age (OR = 0.997, [95% CI 0.993–1], trend at p = 0.08), and AD parental history (OR = 0.953, [95% CI 0.881–1.03], p = 0.23) were not predictors of opting in for LP1. While mean years of education predicted LP participation in the univariate analysis, education was no longer a significant predictor in the regression model (OR = 1.01, [95% CI.992–1.02], p = 0.45).
A one-way ANOVA with Tukey’s post-hoc test showed that African American participants had fewer years of education (14.20±2.9 years) than white participants (15.96±2.6 years, p < 0.001). No difference in years of education was noted between white participants and participants of other racial identities (15.36±3.0 years, p = 0.563) and African American participants and participants of other racial identities (p = 0.149).
LP2 participation
As shown in Table 2, participants who opted in for LP2 were more likely to have had a successful LP1. The group that opted in for LP2 had a 98% success rate from LP1, compared to an 83% success rate for the people who opted out of LP2. Of the 24 participants with unsuccessful LP1, half experienced vasovagal symptoms during the LP so the procedure was discontinued; two participants experienced discomfort during the procedure; and seven participants experienced an unsuccessful LP1 due to clinician inability to locate CSF. Two participants presented to their visit with unrelated pain and one with high blood pressure and heart rate the day of the procedure, so the clinician decided not to perform the LP. Only three (12%) participants with an unsuccessful LP1 opted in for LP2.
Table 2
LP1 success and adverse events among participants who opted in for LP1 and were eligible for LP2, grouped by decision to undergo LP2
| LP 1 Success &Adverse Events | Opted In for LP2 | Opted Out of LP2 | P* |
| (Total eligible for LP2, n = 281) | (n = 155, 55%) | (n = 126, 45%) | |
| LP1 Success (>3 mL CSF) [n, (%)] | 152 (98.1) | 105 (83.3) | < 0.0001 |
| LP1 Severe Adverse Events [n, (%)] | |||
| Blood patch for post-LP headache | 1 (0.65) | 0 (0) | |
| LP1 Moderate Adverse Events [n, (%)] | |||
| Post-LP headache | 6 (3.9) | 6 (4.8) | 0.763 |
| Post-LP low back pain | 3 (1.9) | 5 (3.9) | 0.476 |
| LP1 Mild Adverse Events [n, (%)] | 51 (32.8) | 52 (41.2) | 0.127 |
| Radiculopathy | 3 (1.9) | 3 (2.4) | |
| Pain/discomfort | 2 (1.3) | 3 (2.4) | |
| Vasovagal response | 7 (4.5) | 11 (8.7) | |
| Transient HA/LBP | 28 (18.0) | 24 (19.0) | |
| Multiple side effects | 11 (7.1) | 11 (8.7) |
*The p-value reflects the results from the Chi-square analysis (LP1 success, moderate post-LP headache, mild adverse events) and Fisher’s exact text (moderate post-LP low back pain).
Out of all LP1 participants who were eligible for LP2 (n = 281), only one (0.4%) had a severe adverse event with a post-LP headache requiring blood patch; 4.3% (n = 12) experienced a moderate post-LP headache, and 2.8% experienced moderate post-LP low back pain (Table 2). Among LP1 participants, 36.5% experienced some form of mild adverse event (Table 2). Experiencing either moderate or mild adverse events from LP1 was not associated with a participant’s decision to undergo LP2. A logistic regression testing LP1 success and experience of mild adverse events indicated that successful LP1 was the only predictor of LP2 participation (OR = 1.58, [95% CI 1.28–1.95], p < 0.001; χ2 for model fit = 0.233). Experience of any mild adverse event did not predict LP2 participation in this model (OR = 0.98, [95% CI 0.872–1.10], p = 0.733).
DISCUSSION
Analysis of factors associated with baseline LP participation
We investigated the associations between demographic and clinical factors and participation in an optional LP for AD research. White participants were more likely to participate in an LP at their baseline visit than nonwhite participants. Participants with higher mean years of education were more likely to undergo a baseline LP, consistent with prior research that found both greater education and higher levels of income to be associated with greater willingness to undergo LPs [10]. However, after adjusting for age, years of education, and parental history of AD, race was the only significant predictor for LP1 participation.
Factors associated with LP participation vary across studies. Another Alzheimer’s Disease Research Center (ADRC) recently reported that participants who were younger, had normal cognition and no history of heart disease or seizures were more likely to complete three LPs [7]. In a survey of Alzheimer’s Disease Centers across the United States, Asian race and a negative perception of the procedure were associated with the decision to opt out of LP [19]. Our site’s finding that race predicts LP participation highlights a continued need to develop both strategies for improving research LP participation and strategies for identifying and overcoming race-related participation barriers.
A recent review of AD-related research participation found that while there is much small-scale and situational research on successful recruitment techniques for underrepresented groups, evidence-based recruitment research and additional context surrounding successful recruitment environments is needed [20]. Despite the limited rigorous empirical recruitment science, many studies have identified potentially effective techniques for recruiting from underrepresented groups. Research teams may consider hiring diverse staff, utilizing snowball sampling techniques and employing a field-based approach focused on developing long-term, trusting relationships with the target communities [12, 15, 21, 22]. Fostering trust and comfort regarding LPs may also increase participation for underrepresented groups.
Referrals from trusted friends, family members, or physicians has been shown to positively influence participation in clinical research [16, 23]. Additionally, research participants who previously underwent an LP or knew someone who did so were more likely to agree to undergo the procedure [10], indicating that comfort with the procedure may positively influence participation. It is important to briefly note that researchers carry sole responsibility of improving research participation among underrepresented groups. Especially given the historical context of Africans Americans in medical research, the medical establishment will have to make a concerted effort to ensure that AD research is conducted within a safe and accessible environment for African Americans.
Of the 287 individuals who opted-out of LP1, 39% either scheduled and then cancelled their visit (47 participants) or consented to LP and never scheduled (65 participants). We suggest that participants may have grown hesitant or uninterested between initially consenting to the LP and scheduling the procedure. Thus, it may be beneficial to schedule as soon as possible after participants consent and either present participants with available dates at their consenting visit or contact them shortly after their visit to schedule the LP.
Analysis of factors associated with follow-up LP participation
Participants with a successful LP1 were more likely to opt into a second LP at their follow-up biomarker visit. Adverse events were not associated with a participant’s decision to undergo LP2. Most participants (59.1%) were willing to undergo a baseline LP and participation rates were similar for LP2 (55.0%), indicating that retention of participants for multiple LPs is a feasible goal for AD research. Recent research from another ADRC also supports the feasibility of longitudinal participation, reporting that LP completion rates at their site dipped below 50% for second and third LPs but eventually plateaued around 70% by the fifth LP [7].
AD research centers may seek to bolster LP participation rates with improved clinician training protocol to increase the rate of successful LP. While there is no standardized training procedure for clinicians performing research LPs, simulation-based learning has been effective for medical residents learning to perform LPs [24, 25]. Training could focus on increasing clinician comfort with the procedure, since clinician stress has been associated with increased risk of post-procedure headache and is linked to patient’s confidence [26]. At our site, LPs are performed by either a licensed physician or a nurse practitioner who has undergone extensive training before independently performing LPs, including didactics, simulation-based learning, and supervised LPs followed by a multi-step review process. Just seven of the 413 (1.7%) baseline LPs conducted were unsuccessful due to an inability to locate CSF, indicating that the stringent training practices in place at our site may be effective in minimizing the rate of LP failure.
Standardized procedures that incorporated evidence-based techniques may also improve experience of adverse events. Adverse event rates across cohorts vary widely: in our cohort, 36.5% of participants experienced any mild adverse event during or after their LP, a broad category of minor side effects, with a moderate or severe headache in 4.6% of individuals and moderate low back pain in 2.8%. Other studies have reported moderate to severe headache rates ranging from 2.5% –9% and overall adverse event rates up to 22.3%, much of which were mild [3–5, 7, 27]. A recent analysis of LP techniques and associated symptoms found a low total adverse event rate of 2.72% (0.49% post-LP headache; 0.74% low back pain; 1.48% vasovagal response or mild headache) when following much of the current evidence-based methodology (seated position, use of L4-5 interspace, standardized atraumatic needle use, aspiration method) in addition to use of topical benzocaine prior to lidocaine injection, timed waiting period following lidocaine injection and benzocaine application, and ultrasound use for select patients [8]. Other studies have also indicated use of ultrasound to assist LP is associated with less pain and an increase in the number of successful procedures [28, 29]. Overall, AD researchers may be able to use the available evidence surrounding effective LP techniques and robust clinician training to improve overall LP participation rates by increasing LP success rate and minimizing side effects.
Finally, participants may be motivated by a desire to make a meaningful contribution to research and value their ability to provide CSF over their negative experience of side effects. There is some evidence that even older adults with a moderate burden of illness may be willing and motivated to participate in research for altruistic reasons [9]. Focus groups of African Americans weighing research participation cited a desire to help their community as a motivating factor for participation [12]. Considering that African American individuals are at an increased risk for AD compared to white individuals [30], this factor may be an especially salient motivator for the African American community. Researchers could additionally implement some effective strategies for overall study retention, including maintaining regular contact with participants, making follow-up phone calls following study visits, and ensuring fair compensation for participation [15]. While it is unavoidable that some participants will ultimately have an unsuccessful procedure, research staff could implement these retention strategies to keep participants engaged and continue to appeal to possible altruistic motivations.
Future directions and conclusions
This analysis utilized a large sample size of individuals with varying age and cognitive status. LP participation was an optional component of overall study participation for the individuals included in this analysis, allowing us to evaluate individuals choosing between identical studies with and without an LP. The proportion of African Americans in the study population (18%), while still low compared to the proportion of white participants, is overrepresented compared to the proportion of African Americans in the surrounding community (6%) [31]. However, the study is nonetheless limited by the lack of racial and ethnic diversity across educational levels. Future analysis could incorporate more robust qualitative research investigating the reasons that participants choose to opt in or out of LP to supplement the results found in this study.
Overall, our results indicate that large-scale longitudinal participation in LPs for AD research is feasible, and keeping participants engaged in LP research will require a multifaceted approach. Thoughtful recruitment and retention efforts for underrepresented communities will be necessary to ensure AD biomarker research is safe, accessible to all groups, and produces scientific results generalizable to diverse communities. Researchers may find success in efficient scheduling of the LP or appealing to a participant’s desire to contribute to important research through providing feedback to keep them engaged in the effort. Since successful prior LP was the key predictor for continued participation, research centers may want to closely examine their LP procedure for areas of improvement and ensure that effective training is in place for clinicians performing the procedure.
ACKNOWLEDGMENTS
We would like to thank the participants, faculty and staff of the Wisconsin Alzheimer’s Disease Research Center for their contributions. This work was supported by the National Institute of Aging [P50-AG033514, PI: Asthana], the Clinical and Translational Science Award program [CTSA-1UL1TR002373], and African Americans Fighting Alzheimer’s in Midlife [R01AG054059, PI: Gleason]. This manuscript is the result of work supported with resources and use of facilities at the William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin. This is VA GRECC manuscript number 011-2020.
The sponsors of the study did not play a role in study design; data collection, analysis and interpretation; writing of the report; or the decision to submit this article.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0394r2).
REFERENCES
[1] | Jack CR , Bennett DA , Blennow K , Carrillo MC , Dunn B , Haeberlein SB , Holtzman DM , Jagust W , Jessen F , Karlawish J , Liu E , Molinuevo JL , Montine T , Phelps C , Rankin KP , Rowe CC , Scheltens P , Siemers E , Snyder HM , Sperling R ((2018) ) NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement 14: , 535–562. |
[2] | Palmqvist S , Zetterberg H , Mattsson N , Johansson P , Minthon L , Blennow K , Olsson M , Hansson O ((2015) ) Detailed comparison of amyloid PET and CSF biomarkers for identifying early Alzheimer disease. Neurology 85: , 1240–1249. |
[3] | Monserrate AE , Ryman DC , Ma S , Xiong C , Noble JM , Ringman JM , Morris JC , Danek A , Müller-Sarnowski F , Clifford DB , McDade EM , Brooks WS , Darby DG , Masters CL , Weston PSJ , Farlow MR , Graff-Radford NR , Salloway SP , Fagan AM , Oliver A , Bateman RJ ((2015) ) Factors associated with the onset and persistence of post–lumbar puncture headache. JAMA Neurol 72: , 325–332. |
[4] | Duits FH , Martinez-Lage P , Paquet C , Engelborghs S , Lleó A , Hausner L , Molinuevo JL , Stomrud E , Farotti L , Ramakers IHGB , Tsolaki M , Skarsgård C , Åstrand R , Wallin A , Vyhnalek M , Holmber-Clausen M , Forlenza OV , Ghezzi L , Ingelsson M , Hoff EI , Roks G , de Mendonça A , Papma JM , Izagirre A , Taga M , Struyfs H , Alcolea DA , Frölich L , Balasa M , Minthon L , Twisk JWR , Persson S , Zetterberg H , van der Flier WM , Teunissen CE , Scheltens P , Blennow K ((2016) ) Performance and complications of lumbar puncture in memory clinics: Results of the multicenter lumbar puncture feasibility study. Alzheimers Dement 12: , 154–163. |
[5] | Peskind E , Nordberg A , Darreh-Shori T , Soininen H ((2009) ) Safety of lumbar puncture procedures in patients with Alzheimer’s disease. Curr Alzheimer Res 6: , 290–292. |
[6] | Cole A , Van Hulle CA , Chin NA , Blazel H , Clark LR , Lazar KK , Johnson SC , Bendlin BB , Okonkwo OC , Gleason CE , Edwards DF , Wahoske ML , Blazel M , Asthana S , Carlsson CM ((2018) ) Lumbar punture side effect rates in a research setting. Alzheimers Dement 14: , P1180–P1181. |
[7] | Day GS , Rappai T , Sathyan S , Morris JC ((2020) ) Deciphering the factors that influence participation in studies requiring serial lumbar punctures. Alzheimers Dement (Amst) 12: , e12003. |
[8] | Nobuhara CK , Bullock WM , Bunning T , Colin B , Cooter M , Devinney MJ , Ferrandino MN , Gadsden J , Garrigues G , Habib AS , Moretti E , Moul J , Ohlendorf B , Sandler A , Scheri R , Sharma B , Thomas JP , Young C , Mathew JP , Berger M ; MADCO-PC and INTUIT Investigators Teams ((2020) ) A protocol to reduce self-reported pain scores and adverse events following lumbar punctures in older adults. J Neurol 267: , 2002–2006. |
[9] | Marcantonio ER , Aneja J , Jones RN , Alsop DC , Fong TG , Crosby GJ , Culley DJ , Cupples LA , Inouye SK ((2008) ) Maximizing clinical research participation in vulnerable older persons. J Am Geriatr Soc 56: , 1522–1527. |
[10] | Tsvetkova DZ , Bergquist SH , Parker MW , Jarrett TL , Howell JC , Watts KD , Kollhoff A , Roberts DL , Hu WT ((2017) ) Fear and uncertainty do not influence reported willingness to undergo lumbar punctures in a U.S. multi-cultural cohort. Front Aging Neurosci 9: , 22. |
[11] | Howell JC , Parker MW , Watts KD , Kollhoff A , Tsvetkova DZ , Hu WT ((2016) ) Research lumbar punctures among African Americans and Caucasians: Perception predicts experience. Front Aging Neurosci 8: , 296. |
[12] | Williams MM , Scharff DP , Mathews KJ , Hoffsuemmer JS , Jackson P , Morris JC , Edwards DF ((2010) ) 4- barriers and facilitators of African American participation in Alzheimer’s disease biomarker research. Alzheimer Dis Assoc Disord 24: , S24–S29. |
[13] | Scharff DP , Mathews KJ , Jackson P , Hoffsuemmer J , Emeobong M , Edwards D ((2010) ) More than Tuskegee: Understanding mistrust about research participation. J Health Care Poor Underserved 21: , 879–897. |
[14] | Rosner D , Markowitz G ((2012) ) With the best intentions: Lead research and the challenge to public health. Am J Public Health 102: , e19–e33. |
[15] | Otado J , Kwagyan J , Edwards D , Ukaegbu A , Rockcliffe F , Osafo N ((2015) ) Culturally competent strategies for recruitment and retention of African American populations into clinical trials. Clin Transl Sci 8: , 460–466. |
[16] | Edwards DF , Dowling NM , Dykema J ((2015) ) Factors associated with the likelihood of providing cerebrospinal fluid for a medical research study in an ethnically diverse sample of adults. Alzheimers Dement 11: , P779–P780. |
[17] | Notice of NIH’s Interest in Diversity, https://grants.nih.gov/grants/guide/notice-files/NOT-OD-20-031.html, Last updated November 22, 2019, Accessed on November 22, 2019. |
[18] | Kawas C , Segal J , Stewart WF , Corrada M , Thal LJ ((1994) ) A validation study of the dementia questionnaire. Arch Neurol 51: , 901–906. |
[19] | Moulder KL , Besser LM , Beekly D , Blennow K , Kukull W , Morris JC ((2017) ) Factors influencing successful lumbar puncture in Alzheimer research. Alzheimer Dis Assoc Disord 31: , 287–294. |
[20] | Gilmore-Bykovskyi AL , Jin Y , Gleason C , Flowers-Benton S , Block LM , Dilworth-Anderson P , Barnes LL , Shah MN , Zuelsdorff M ((2019) ) Recruitment and retention of underrepresented populations in Alzheimer’s disease research: A systematic review. Alzheimers Dement (N Y) 5: , 751–770. |
[21] | Green-Harris G , Coley SL , Koscik RL , Norris NC , Houston SL , Sager MA , Johnson SC , Edwards DF ((2019) ) Addressing disparities in Alzheimer’s disease and African-American participation in research: An asset-based community development approach. Front Aging Neurosci 11: , 125. |
[22] | Wilkins CH ((2018) ) Effective engagement requires trust and being trustworthy. Med Care 56: , S6–S8. |
[23] | Graham LA , Ngwa J , Ntekim O , Ogunlana O , Wolday S , Johnson S , Johnson M , Castor C , Fungwe TV , Obisesan TO ((2017) ) Best strategies to recruit and enroll elderly Blacks into clinical and biomedical research. Clin Interv Aging 13: , 43–50. |
[24] | Barsuk JH , Cohen ER , Caprio T , McGaghie WC , Simuni T , Wayne DB ((2012) ) Simulation-based education with mastery learning improves residents’ lumbar puncture skills. Neurology 79: , 132–137. |
[25] | McMillan HJ , Writer H , Moreau KA , Eady K , Sell E , Lobos AT , Grabowski J , Doja A ((2016) ) Lumbar puncture simulation in pediatric residency training: Improving procedural competence and decreasing anxiety. BMC Med Educ 16: , 198. |
[26] | Henriksen MJV , Wienecke T , Kristiansen J , Park YS , Ringsted C , Konge L ((2018) ) Opinion and special articles: Stress when performing the first lumbar puncture may compromise patient safety. Neurology 90: , 981–987. |
[27] | Alcolea D , Martinez-Lage P , Izagirre A , Clerigue M , Carmona-Iragui M , Alvarez R , Fortea J , Balasa M , Morenas-Rodriguez E , Llado A , Grau O , Blennow K , Lleo A , Molinuevo J ((2014) ) Feasibility of lumbar puncture in the study of cerebrospinal fluid biomarkers for Alzheimer’s disease: A multicenter study in Spain. J Alzheimers Dis 39: , 719–726. |
[28] | Abraham A , Breiner A , Katzberg HD , Lovblom LE , Bril V ((2019) ) Ultrasound-assisted Lumbar Puncture in a neuromuscular clinic has a high success rate and less pain. Can J Neurol Sci 46: , 79–82. |
[29] | Gottlieb M , Holladay D , Peksa GD ((2019) ) Ultrasound-assisted lumbar punctures: A systematic review and meta-analysis. Acad Emerg Med 26: , 85–96. |
[30] | Steenland K , Goldstein F , Levey A ((2016) ) A meta-analysis of Alzheimer’s disease incidence and prevalence comparing African-Americans and Caucasians. J Alzheimers Dis 50: , 71–76. |
[31] | U.S. Census Bureau QuickFacts: Dane County, Wisconsin, https://www.census.gov/quickfacts/danecountywisconsin |


