
Potential for Digital Monitoring to Enhance Wellbeing at Home for People with Mild Dementia and Their Family Carers
Abstract
Digital technologies have the potential to assist people with dementia to monitor day to day activities and mitigate the risks of living independently. This purposive pilot study surveyed participants for frailty, wellbeing, and perceived carer burden using the 3Rings™ digital plug. 30 paired participants used the digital device for four months. People with dementia reported a decline in wellbeing and increased frailty. Family carers reported a decline in wellbeing but 18 reported a reduction in burden. The use of digital monitoring by family carers demonstrated a reduction in their perceived burden and the device was acceptable to people with mild dementia living alone.
INTRODUCTION
One third of people with dementia who live in the community (i.e., not in residential care) live alone [1] in the UK, amounting to more than 215,000 people. As the population of people with dementia (PwD) grows [2], the community of carers, families, and other social support will also grow in number. Frailty is strongly associated clinically diagnosed dementia among persons aged 76 and older [3] and can result in a range of functional limitations that also affect their care [4]. Older adults wish to remain living at home for as long as possible [5–7], and this is also favored by policymakers [5–8] who want family carers (FC) to support PwD at home.
Caregiving can feel stressful [9–12] with variation in wellbeing and levels of burden depending on the duration and the severity of the dementia and the consequent need of the PwD for support [4]. In primary care, for those caring at home, the level of burden was lower than reported in other settings [9]. The focus on maintaining independence and detecting decline was important to both parties [10, 11] with an important distinction between burden and wellbeing [12]. Burden appears to be associated with any behavioral changes in the PwD and the hours when care is needed [12], and overall psychological wellbeing of the carer is significantly associated with social support and coping mechanisms [13].
Home-based digital technology may provide a range of solutions to enable safe, comfortable, and acceptable means to remain at home by helping PwD, particularly in relation to routine daily living tasks. Evidence suggests that FC find tele-health devices helpful [14] and smart technologies are being developed to support FC of PwD, including provision of information about daily routine. This may also support PwD to live independently at home [15]. Smart technology is seen as a cost- effective means of maintaining the wellbeing of the PwD [5, 11, 16–18] demonstrating how most older adults recognize the convenience and support for daily activities. Barriers to digital technology usage and home monitoring are well documented too [5, 17–23], with issues of privacy invasion being the greatest concern. There is essentially a pay-off to the use of devices related to costs and benefits. Research is needed into the usefulness and acceptance of devices, along with robust evidence of the impact on health and wellbeing [24].
Smart technologies integrate physical objects, technology, and people, in order to share information [25] and this can be deployed to recognize routines and repeated activities [26, 27] of daily living. Monitoring the use of an electrical appliance in the home has the potential to demonstrate that a PwD is well and carrying out usual activities. This study sought to investigate whether a FC could check the daily routine of the PwD, and whether it reduced perceived burden felt by the FC. It also sought to identify the effect on wellbeing of both parties.
METHODS
A purposive pilot study investigated the outcomes of implementing the 3Rings™ digital plug with PwD who lived alone and their FC, over a period of four months. This study was funded by the South Yorkshire Perfect Patient Pathway (Testbed) Programme. Ethical approval ER5178396 was granted by Sheffield Hallam University Ethics Committee.
Third sector partners identified potential recruits and information was sent to the potential participants specifically excluding anyone with formal care or a live-in relative. Participant Information Sheets and consent forms were sent to FC for them to read with the PwD. Telephone contact confirmed inclusion criteria with FC and the study was explained in detail.
Formal written consent was taken from both PwD and FC in the PwD’s home and the 3Rings™ plug was installed with a routinely used electrical device, typically an electric kitchen kettle. The 3Rings™ system is set with an ‘event time’ period, where use of the appliance in this period is a significant indicator of the likelihood of the routine behavior taking place. ‘Event time’ for a kettle would cover the time-frame for a morning or evening drink. Habitual activities could be predicated with PwD and their FC, recognizing the usual routine. Other devices, i.e., a TV or bedside light were also acceptable providing they were in regular use in the PwD’s home. The plug was installed according to manufacturer’s guidance with agreement to use the smart device as part of usual daily routine. Then the FC was instructed in the use of the digital monitoring application on their mobile phone. Survey tools were used with both parties.
Pre and post survey
Two standardized survey tools were used with the PwD and with the FC, at first meeting and after four months.
The Edmonton Frail Scale was used with the PwD as it has good construct validity and reliability [28, 29] and allows a diagnosis of frailty to be assumed from the score [28]. The Warwick-Edinburgh Mental Wellbeing Scale (short form) is a positively worded validated scale to measure wellbeing measured on a five-point Likert Scale [30, 31] and was used with both PwD and FC. These assessment tools are both validated for PwD [32]. The Zarit Burden Interview has a high reliability and validity, and is often used to measure the challenges presented to the care-giver over time [12] and was used with the FC. The relevance of this measure was associated with the wellbeing of FC and the possible difference experienced with remote digital support.
Semi-structured interview
A short interview was constructed from the literature and used with the participants. The focus was on subjective experience of using the 3Rings™ device relative to their individual context, emphasizing individual differences [33]. The data was intended to provide a narrative explanation of the findings and to generate some explanation about the value of the monitoring process to families.
Remote digital data collection
Background appliance activity is logged for each appliance, and accessed via the digital interface; usually the FC’s digital mobile phone. Daily patterns of use, using the ‘timed -event’ data is evident to the FC with alerts send when no activity occurred in a pre-set ‘event- time’ window (see Fig. 1). Alerts operated automatically irrespective of the reason for inactivity and are continuously sent until an action in response is taken. The explanation refers to the decision about whether this constituted an emergency based on the understanding of the PwD and FCs. Response to alerts by the FC were collected and the explanations categorized under four options: emergency, action needed, no action needed, false alert.
Fig.1
3Rings™ utility monitoring via digital alert data.
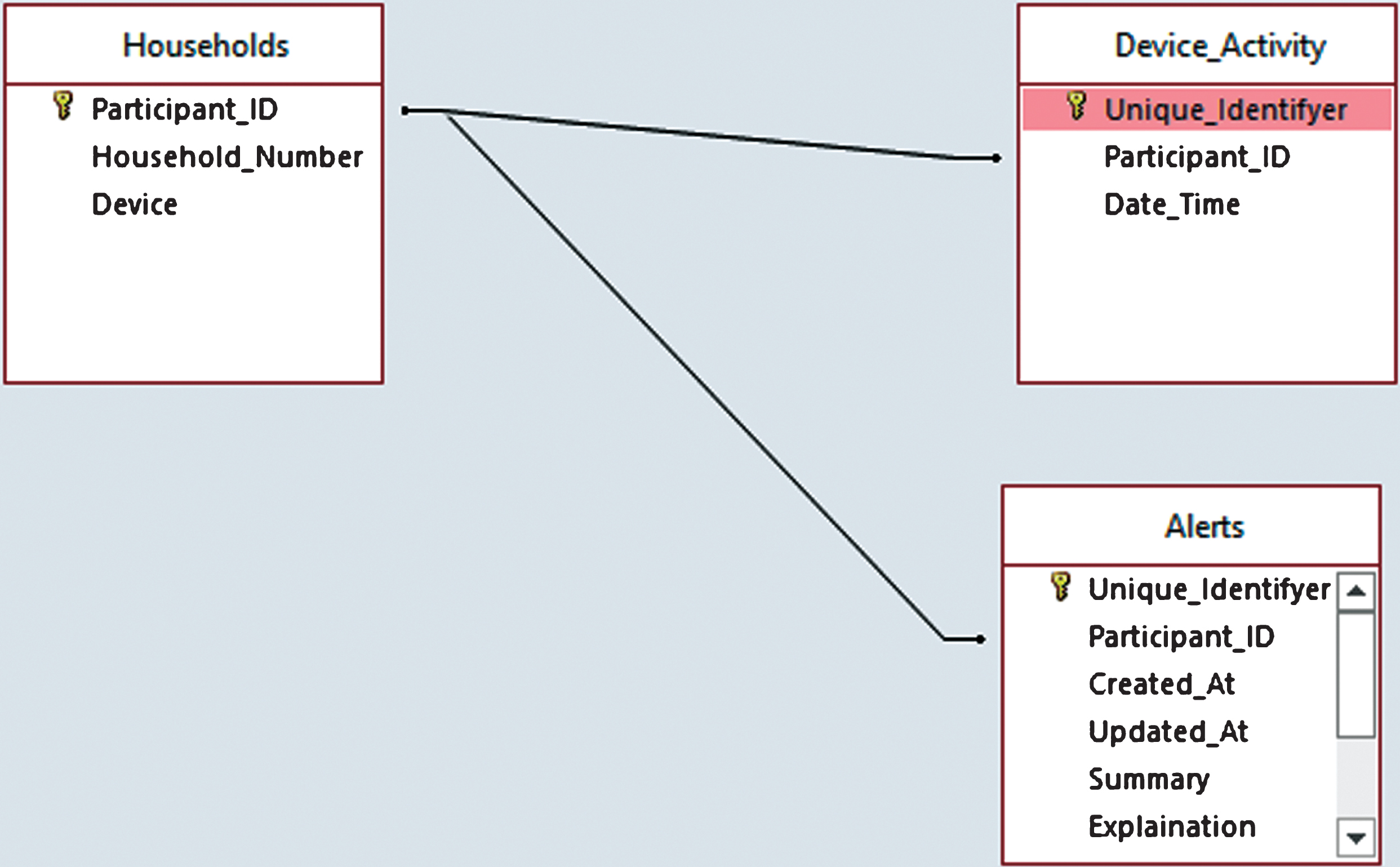
Analysis of the alerts sent and received was collated by the research team, together with summary and explanation of device usage for all PwD participant using the participant ID. This data identified the number of times that the ‘timed events’ were not carried out during the set parameters, indicating risk through unpredicted activity.
Analysis
The first and second wellbeing questionnaire scores, burden scale, and the frailty data were manually input into an Excel spreadsheet and difference was calculated. Descriptive analysis was applied to correlate frailty and wellbeing for the PwD, and level of burden and wellbeing for the FC. The digital monitoring data was then compared with the questionnaire results to generate some explanation about the value of the monitoring process to families. Other qualitative data was collated using simple content analysis to identify subjective experiences aiming to illustrate the usefulness or problems with adoption of digital monitoring.
RESULTS
Recruitment and retention
46 potential participants were identified and 31 participant pairs (PwD and FC) were recruited. The analysis was completed on 30 pairs who were retained for the full period of the study and who used the device for four months. Population reach [34] was calculated at 0.75% of the total population of people living in the region who have dementia and live alone based on a third of those diagnosed with dementia in the region [35]. The demographic characteristics of the group (Table 1) were representative of the population.
Table 1
The demographics of the paired participants
| Participants | Number | Gender | Age range | Relative |
| Persons with Dementia | 30 | Male – 7 | Male – 65–92 | |
| Female – 23 | Female – 78–96 | |||
| Family Carers | 30 | Male – 8 | Male – 28–62 | Son – 7 |
| Other – 1 | ||||
| Female – 22 | Female – 30–65 | Daughter – 16 | ||
| Other – 6 |
Digital monitoring data
The mean number of alerts in the first two months was < 3 per participant pair and decreased to < 2 or less at 4 months. This reflects a pattern of highly routine behaviors, within the event-times configured at device set-up. The median value of alerts throughout the study was 1 per PwD. Only 5 alerts out of 266 in total required an action by the FC (215 ‘no action needed’ 46 ‘false alerts’, 0 ‘emergencies’, and 5 ‘Action needed’). One FC failed to understand the device and its alert management process, resulting in 19 alerts in the first month. One PwD unplugged the device as part of their evening routine causing ‘false alerts’. However, all FC learned how to resolve the alerts quickly after a short period of use.
Survey data
All 30 paired participants completed pre and post survey tools allowing scores to be analyzed. Table 2 shows that around half the PwD (17) and FC (15) reported a decline in wellbeing. 17 of 30 PWD’s frailty improved or stayed the same with 13 demonstrating a decline in scores of the Edmonton Frail Scale. 18 of 30 FC reported a decrease in burden; almost double the number that reported an increase in burden.
Table 2
A summary of the comparison of the survey scores pre and post showing the number of scores that improved or declined
| PwD Short WarwickEdinburgh | PwD Edmonton Frail Scale | FC Short Warwick | FC Zarit Burden Edinburgh | |
| Improvement | 13 | 7 | 10 | 18 |
| Decline | 17 | 13 | 15 | 10 |
| Stayed the same | 0 | 10 | 5 | 2 |
Subjective experience
There were a number of comments from the FC interviews that can be reported with the following experiences:
• The PwD had patterns of behavior that were predictable and the ‘timed events’ led to a re-assurance that their relation was ‘okay’ at home.
• The use of the device promoted less checking and a more satisfactory relationship based on better quality social contact.
• For PwD, there was an appreciation that they were ‘connected’ to their FC through the device.
• FC reported that they waited for the timed event period to pass each morning and then when there were no alerts they would relax.
DISCUSSION
PwD and FC agreed to the use of digital monitoring and understood the implications, recognizing the connectivity that the device afforded their families [7]. This study adds to the understanding of the potential benefits of using a monitoring device and the impact on wellbeing insofar as participants found the technology acceptable and usefully demonstrated the relative stability of routine for PwD. There were a low number of missed event-times causing few alerts that suggested routine behaviors over the four-month period. This stability was useful as additional information to support family care.
The reported reduction in burden for the FC group (18 of 30) was noted and important to recognize in relation to both increases in PwD frailty and decline in PwD wellbeing. This supports the suggestion that remote monitoring technology has the potential to reduce the stress and burden felt by FC [11], perhaps due to the behavioral feedback and regular patterns [12], which gives families ‘peace of mind’ [18, 35]. While FC mostly want to support PwD to maintain their independence and ‘age in place’ for as long as possible [1, 17], many FC have a range of other social commitments and caring responsibilities that are competing for their attention. Remote monitoring can enable FC to have a greater understanding of their relative’s daily routine [11, 36], which can assist in planning and reduce conflicting demands; this is a direct product of being able to predict risk and assume routine behaviors. It may also provide useful insights on behaviors they were not aware of [37], for example, where early rising or night time routines diverted from a regular pattern and an intervention can be planned [6].
A PwD who lives alone but who is at ease with their surroundings was able to repeat daily tasks (as indicated by the 3Rings device), in a safe and familiar way, albeit for the relatively short period of this study. Dementia is considered to be a progressive condition [38, 39] with a variable trajectory of gradual decline in function [11, 37]. The importance of habit and routine as an indicator of wellbeing is an under researched area and has been shown to have potential to facilitate independence. The PwD may accommodate to privacy and intrusion if the alternative would be going into a care home [6, 11, 16, 18, 19], and monitoring could provide a means of connection resulting in feeling safer [18, 36] and cared for [22,]. Lower burden and higher wellbeing in FC appear to directly benefit the PwD, sometimes irrespective of the PwD’s functional status and personal wellbeing. The monitoring of a valued routine can be an important indicator of continued ability for the PwD to remain at home.
Strengths and limitations
The study was a time-limited study using a simple device that had the advantage of engaging paired participants who were new users of technology with FC and PwD participating equally.
Conclusion
This paper reports on the benefits of digital monitoring to PwD and FC, in relation to predicted patterns of PwD behavior, demonstrating a regular daily routine that could be predicted. This is important for FC in relation to burden over time. Overall this study contributes to the understanding of how digital monitoring devices have the potential to facilitate independence for PwD living alone. It provides because this may reduce the stress that carers experience, particularly if they do not live close to their relatives.
ACKNOWLEDGMENTS
Financial support for the research was received from NHS England Testbed programme, Westfield Health, and Sheffield Hallam University.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0844r2).
REFERENCES
[1] | Miranda-Castillo C , Woods B , Orrell M ((2010) ) People with dementia living alone: what are their needs and what kind of support are they receiving? Int Psychogeriatr 22: , 607–617. |
[2] | National Institute for Health and Care Excellence (UK) ((2018) ) Dementia: assessment, management and support for people living with dementia and their carers. |
[3] | Kulmala J , Nykänen I , Mänty M , Hartikainen S ((2014) ) Association between frailty and dementia: a population-based study. Gerontology 60: , 16–21. |
[4] | von Känel R , Mausbach BT , Dimsdale JE , Ziegler MG , Mills PJ , Allison MA , Patterson TL , Ancoli-Israel S , Grant I ((2019) ) Refining caregiver vulnerability for clinical practice: determinants of self-rated health in spousal dementia caregivers. BMC Geriatr 19: , 18. |
[5] | Peek STM , Wouters EJM , Van Hoo J , Luijkx KG , Boeije HR , Vrijhoef HJM ((2014) ) Factors influencing acceptance of technology for aging in place: A systematic review. Int J Med Inform 83: , 235–248. |
[6] | Kim K , Gollamudi SS , Steinhubl S ((2017) ) Digital technology to enable aging in place. Exp Gerontol 88: , 25–31. |
[7] | Essen A ((2008) ) The two facets of electronic care surveillance: An exploration of the views of older people who live with monitoring devices. Soc Sci Med 67: , 128–136. |
[8] | Sutcliffe CL , Giebel CM , Jolley D , Challis DJ ((2016) ) Experience of burden in carers of people with dementia on the margins of long-term care. Int J Geriatr Psychiatry 31: , 101–108. |
[9] | Thyrian J , Winter P , Eichler T , Reimann M , Wucherer D , Dreier A , Michalowsky B , Zarm K. Hoffmann W ((2017) ) Relatives’ burden of caring for people screened positive for dementia in primary care. Z Gerontol Geriatr 50: , 4–13. |
[10] | Wild K , Boise L , Lundell J , Foucek A ((2008) ) Unobtrusive in-home monitoring of cognitive and physical health: reactions and perceptions of older adults. J Appl Gerontol 27: , 181–200. |
[11] | Malmgren Fange A , Schmidt SM , Nilsson MH , Carlsson G , Liwander A , Dahlgren Bergstrom C , Olivetti P , Johansson P , Chiatti C ((2017) ) The TECH@HOME study, a technological intervention to reduce caregiver burden for informal caregivers of people with dementia: study protocol for a randomized controlled trial. Trials 18: , 63. |
[12] | Chappell NL , Reid RC ((2002) ) Burden and well-being among caregivers: examining the distinction. Gerontology 42: , 772–780. |
[13] | Chaaya M , Phung K , Atweh S , El Asmar K , Karam G , Khoury R , Ghandour L , Ghusn H , Assaad S , Prince M , Waldemar G ((2017) ) Dementia and family burden of care in Lebanon. BJPsych Int 14: , 7–9. |
[14] | Torkamani M , McDonald L , Aguayo IS , Kanios C , Katsanou MN , Madeley L , Limousin PD , Lees AJ , Haritou M , Jahanshahi M ((2014) ) A randomized controlled pilot study to evaluate a technology platform for the assisted living of people with dementia and their carers. J Alzheimers Dis 41: , 515–523. |
[15] | Bossen AL , Kim H , Williams KN , Steinhoff AE , Strieker M ((2015) ) Emerging roles for telemedicine and smart technologies in dementia care. Smart Homecare Technol Telehealth 3: , 49–57. |
[16] | Mitzner TL , Boron JB , Fausset CB , Adams AE , Charness N , Czaja SJ , Dijkstra K , Fisk AD , Rogers WA , Sharit J ((2010) ) Older adults talk technology: Technology usage and attitudes. Comput Human Behav 26: , 1710–1721. |
[17] | Berridge C ((2016) ) Breathing room in monitored space: the impact of passive monitoring technology on privacy in independent living. Gerontology 56: , 807–816. |
[18] | Zwijsen SA , Niemeijer AR , Hertogh CM ((2011) ) Ethics of using assistive technology in the care for community-dwelling elderly people: An overview of the literature. Aging Ment Health 15: , 419–427. |
[19] | Mihailidas A , Cockburn A , Longley C , Boger J ((2008) ) The acceptability of home monitoring technology among community-dwelling older adults and baby boomers. Assist Technol 20: , 1–12. |
[20] | Suryadevara NK , Mukopadhyay SC ((2012) ) Wireless sensor network based home monitoring system for wellness determination of elderly. IEEE Sens J 12: , 1965–1972. |
[21] | Azimi I , Rahmani AM , Liljegerg P , Tenhunen H ((2017) ) Internet of things for remote elderly monitoring: a study from user-centred perspective. J Ambient Intell Human Comput 8: , 273–289. |
[22] | Epstein I , Aligato A , Krimmel T , Mihailidis A ((2016) ) Older adults’ and caregivers’ perspectives on in-home monitoring technology. Gerontol Nurs 42: , 43–50. |
[23] | Niemela-Nyrhinen J ((2007) ) Baby boom consumers and technology: shooting down stereotypes. J Int Consum Mark 24: , 305–312. |
[24] | Carrillo MC , Dishman E , Plowman T ((2009) ) Everyday technologies for Alzheimer’s disease care: Research findings, directions, and challenges. Alzheimers Dement 5: , 479–488. |
[25] | Atzori L , Iera A , Morabito G ((2017) ) Understanding the Internet of Things: definition, potentials, and societal role of a fast evolving paradigm. Ad Hoc Networks 56: , 122–140. |
[26] | Mazar A , Wood W ((2018) ) Defining habit in psychology. In The Psychology of Habit, VerplankenB, ed. Springer, Cham, pp. 13–29. |
[27] | Gardner B , Lally P ((2018) ) Modelling habit formation and its determinants. In The Psychology of Habit, VerplankenB, ed. Springer, Cham, pp. 207–229. |
[28] | Rolfson DB , Majumdar SR , Tsuyuki RT , Tahir A , Rockwood K ((2006) ) Validity and reliability of the Edmonton Frail Scale. Age Ageing 35: , 526–529. |
[29] | Perna S , Francis MD , Bologna C , Moncaglieri F , Riva A , Morazzoni P , Allegrini P , Isu A , Vigo B , Guerriero F , Rondanelli M ((2017) ) Performance of Edmonton Frail Scale on frailty assessment: its association with multi-dimensional geriatric conditions assessed with specific screening tools. BMC Geriatr 17: , 2. |
[30] | Ng Fat L , Scholes S , Boniface S , Mindell J , Stewart-Brown S ((2017) ) Evaluating and establishing national norms for mental wellbeing using the short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS): findings from the Health Survey for England. Qual Life Res 26: , 1129–1144. |
[31] | Tennant R , Hiller L , Fishwick R , Platt S , Joseph S , Weich S , Parkinson J , Secher J , Stewart-Brown S ((2007) ) The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 5: , 63. |
[32] | Allward C , Dunn R , Forshaw G , Rewston C , Wass N ((2017) ) Mental wellbeing in people with dementia following Cognitive Stimulation Therapy: Innovative practice. Dementia (London), doi: 10.1177/1471301217722443. |
[33] | Graneheim UH , Lundman B ((2004) ) Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 24: , 105–112. |
[34] | Glasgow RE , Vogt TM , Boles SM ((1999) ) Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health 89: , 1322–1327. |
[35] | Rowan J , Mynatt ED ((2005) ) Digital Family Portrait Field Trial: support for aging in place. CHI ’05 Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, pp. 521–530. |
[36] | Iman A , Amir M. Rahmani P , Liljeberg A , Tenhunen H ((2017) ) Internet of things for remote elderly monitoring: a study from user-centered perspective. J Ambient Intell Humaniz Comput 8: , 273–289. |
[37] | Woodbridge R , Sullivan M , Harding E , CrutchS , Gilhooley K , Gilhooly M , McIntyre A , Wilson L ((2018) ) Use of the physical environment to support everyday activities for people with dementia: A systematic review. Dementia 17: , 533–572. |
[38] | National Institute for Health Research Dissemination Centre ((2018) ) Help at Home - Use of assistive technology for older people. https://discover.dc.nihr.ac.uk/content/themedreview-03385/help-at-home-use-of-assistive-technology-for-older-people. |


