
Factors Associated with Mortality Including Nursing Home Transitions: A Retrospective Analysis of 25,418 People Prescribed Anti-Dementia Drugs in Northern Ireland
Abstract
Background:
Understanding factors associated with mortality after a dementia diagnosis can provide essential information to the person with dementia, their family, and caregivers. To date very little is known about the factors associated with mortality after a dementia diagnosis in Northern Ireland.
Objective:
To determine how demographic and other factors such as deprivation and comorbidity medications influence mortality rates after a dementia diagnosis in Northern Ireland and whether these factors are influenced through nursing home transitions.
Methods:
25,418 people prescribed anti-dementia medication were identified through the enhanced prescribing database between 2010 and 2016. The impact of covariates including age, gender, marital status, deprivation measure, urban/rural classification, and comorbidity medications were examined using cox proportional hazard models with hazard ratios (HR) and 95% confidence intervals.
Results:
Between 2010 and 2016, 12,129 deaths occurred, with 114 deaths/1,000 person years. Males had significantly higher mortality rates in comparison to females (HR = 1.28; 95% CI = 1.23–1.33); this was true regardless of whether the person with dementia transitioned to a nursing home. People prescribed anti-dementia drugs living with lower levels of deprivation had significantly lower mortality rates in comparison to people living with the highest levels of deprivation (HR = 0.93; 95% CI = 0.89–0.97). Diabetic (HR = 1.18; 95% CI = 1.07–1.29) and anti-arrhythmic (HR = 2.44; 95% CI = 1.01–5.91) medication in particular significantly influenced mortality.
Conclusion:
Male gender, higher comorbidity medications, and living in areas of higher deprivation significantly increased mortality rates for people prescribed anti-dementia drugs in our study population. When comorbidity medications were classified, only anti-arrhythmia and diabetic medications significantly increased mortality. Future research should continue to investigate factors which influence mortality after a dementia diagnosis.
INTRODUCTION
Dementia is defined as functional impairment on the basis of a progressive cognitive decline caused by a broad group of conditions, most commonly Alzheimer’s disease [1]. At present there is no cure for dementia; however, medication can slow down the cognitive decline and institutionalization rate in people prescribed anti-dementia drugs. The prevalence of dementia, together with the major health and social care burden associated with it, is predicted to increase considerably with the increase in the aging population [2]. For instance, in Northern Ireland (NI), current estimations suggest that 19,000 people are currently living with a dementia diagnosis [2], a number set to increase to 60,000 by 2050 [2]. Given these projections, understanding mortality rates in dementia is essential for resource planning and to adequately counsel and inform patients, family, carers, and social and healthcare professionals [3, 4]. Dementia shortens life expectancy, with some studies suggesting a survival time after diagnosis of 1–13 years [5]. However, longitudinal studies have shown that survival time could be as short as 4.5 years [5–7]. Several factors have been shown to be associated with mortality in dementia. Increasing age, lower cognition levels at time of diagnosis, and male gender are associated with increased mortality after diagnosis [8–11]. Moreover, higher levels of comorbidity medication has also been shown to increase mortality [7, 12], whereas being married may extend life expectancy [13]. Research has shown that people with dementia (PwD) who have transitioned to a care home or residential setting at least once have higher comorbidity medications and mortality [14]. Therefore, it is important to consider such factors when assessing variables which may influence mortality following a dementia diagnosis. In NI, several datasets exist which allow researchers to identify PwD and their demographic characteristics such as age, gender, marital status, whether they live in an urban or rural area, and the number of medications they have been prescribed. The aim of this study was, for the first time in NI, to explore demographic and other parameters such as deprivation and comorbidity medication which may be associated with mortality rates after a dementia diagnosis.
METHODS
Enhanced prescribing database
The National Health Service in NI provides free health care at the point of use, and medications that are prescribed by a General Practitioner (GP) incur no charge. Unique to NI, the NHS Business Service Organization implemented an electronic prescribing database (EPD) in 2008. The EPD adds a barcode to paper prescriptions dispensed by a GP which facilitates recording of the patients’ unique Health and Care Number, details of the prescribed medication, and the prescriber. At the end of each month, all information contained in each bar code is scanned and held in the EPD [15]. The Honest Broker service has indicated that approximately 80–90% of all barcodes scanned result in useable data [15]. The EPD does not currently hold data on medicines bought over-the-counter or prescribed in hospital. Diagnoses and other clinical information are not recorded in the EPD.
Within the EPD database, prescriptions are coded within the British National Formulary (BNF) sections [16], making it possible to retrieve the number of medications dispensed from each BNF section. Several other variables, such as age, marital status, whether or not the person lives in a rural or urban area, and how many times the individual transitioned into a nursing home can be retrieved by linking the patient’s unique Health and Care Number to several other datasets in the Business Service Organisation. Uniquely, the Business Service Organisation also contains information on each individuals Northern Ireland Multiple Deprivation Measure (NIMDM) [17], which is a deprivation measure ranging from 1 to 10, with higher numbers indicating less deprived areas.
Study population
The dataset for this study contained information on all patients in NI who were dispensed at least one medicine for dementia management (BNF section 4.11) between January 1, 2010 – December 31, 2016. This section contains cholinesterase inhibitors and memantine and these medications were used as a proxy for a dementia diagnosis as they are not prescribed for any other illness [18]. Similar to the methodology followed by Barry et al. [18] to identify people prescribed anti-dementia drugs, we used the first date that a dementia management medication was prescribed as a proxy for date of diagnosis. Moreover, the final data set also contained information on whether individuals lived in a rural/urban area, the number of times (if any) each individual transitioned into nursing home care between 2010–2016, if a person was known to have transitioned to a care home at least once in any quarter of any year from 2010–2016, we were provided with a “1” for that year and for no transitions a “0”, the sum of which was “total number of care home transitions”. Marital status was included; however, the date of this was inputted to the enhanced prescribing database at different times between 2010–2016. The number of medications per year dispensed to each person from the following BNF sections between January 1, 2010–December 31, 2016; BNF section 6.1 (diabetes), BNF section 4.3 (antidepressants), BNF section 4.2.1 (antipsychotics), BNF section 4.1 (hypnotics and anxiolytics), BNF section 2.3.2, (arrhythmia), and BNF section 2.5 (hypertension). We included these specific BNF sections due to past research suggesting that they influence prevalence of dementia and mortality [19–24]. For each of the BNF sections, we generated a variable “comorbidity”, variable which equaled 1 if a person was dispensed at least one item from that section, otherwise 0; this allowed us to estimate the number of people with each comorbidity in the data set. For instance, if a person was prescribed at least one medication from BNF section 6.1, we labelled them as having diabetes. We summed the total number of comorbidity items dispensed between January 1, 2010–December 31, 2016 which was then categorized into 0, 1–5 = 1, 6–10 = 2, 11–15 = 3, and ≥16 = 4.
Statistical analysis
To identify factors associated with mortality between people who had been in a care home at least once and those who had not after dementia diagnosis, we used Cox proportional hazard regression models. Results are shown as hazard ratios with 95% confidence intervals. Independent variables included, gender, age category, marital status, urban/rural classification, NIMDM, and total number of comorbidity medications. A second Cox proportional hazard model was estimated which replaced “total number of comorbidity medications” with “type of comorbidity” in order to determine which comorbidities influence mortality rates after diagnosis. As well as the frequencies for each of the independent variables, we also report total person years at risk (total number of years people in the cohort lived with dementia before mortality) and deaths/1000 person years (the number of people likely to die with dementia within the next 1000 years). Statistical significance at p < 0.05 was assumed. We also conducted a series of independent t-tests to assess whether age and total number of comorbidity items was significantly different between people who had been to a care home at least once and those who had not.
RESULTS
Demographic characteristics are presented in Table 1. A total number of 25,418 people prescribed anti-dementia drugs were included in the dataset. At the time of analysis 13,289 people were living with a dementia diagnosis and 12,129 people had died. The average survival time was 4.2 years, after the date of diagnosis. Sixty-five percent of the study population was female. Mean age was 77.3 years (SD = 8.4 years). A third (32%) of the study population were married; for 35% of the population, data regarding marital status was not available. More deaths occurred in PwD who had transitioned to a care home at least once (n = 6,797) in comparison to PwD who had never transitioned to a care home (n = 3,066). Person years at risk and deaths per 1000 years was also higher among PwD who had transitioned to a care home at least once (6,797 deaths) in comparison to PwD who had never transitioned to a care home (3,066 deaths). A large majority had a high level of comorbidity medications, with 84% of subjects having more than 15 comorbidity medications. Forty-two percent lived in the higher category of the NIMDM (less deprived). A series of independent sample t tests found that on average, PwD who have been in a care home at least once were significantly older (t (25416) = –42; p = <0.0001) in comparison to those who had never been in a care home and that comorbidity medications were significantly higher among those who had not transitioned to a care home (t (25416) = –4.9; p < 0.0001).
Table 1
Study cohort characteristics
| Number of patients (%) | Deaths | PY at risk | Deaths/1000 PY | Number of patients (%) | Deaths | PY at risk | Deaths/1000 PY | Number of patients (%) | Deaths | PY at risk | Deaths/1000 PY | |
| All data (n = 25,418) | No care home transitions (n = 14,564) | At least one care home transition (n = 10,854) | ||||||||||
| Gender | ||||||||||||
| All | 25418 | 12129 | 106743 | 114 | 14564 (57%) | 3066 | 32153 | 95 | 10854 (43%) | 6797 | 54567 | 121 |
| Male | 8881 (35%) | 4471 | 36102 | 106 | 5609 (39%) | 2266 | 20023 | 113 | 3272 (30%) | 4592 | 16079 | 119 |
| Female | 16537 (65%) | 7658 | 70641 | 120 | 8955 (61%) | 3066 | 32153 | 95 | 7582 (70%) | 2205 | 38487 | 137 |
| Age | ||||||||||||
| <65 | 1772 (7%) | 385 | 6061 | 63 | 1377 (9%) | 226 | 4238 | 53 | 395 (4%) | 159 | 1822 | 87 |
| 65–74 | 6643 (26%) | 1991 | 23841 | 83 | 4682 (32%) | 1063 | 14597 | 72 | 1961 (18%) | 928 | 9244 | 100 |
| 75–84 | 12139 (48%) | 6018 | 51441 | 116 | 6688 (45%) | 2741 | 24579 | 111 | 5451 (50%) | 3277 | 26861 | 121 |
| 85 | 4864 (19%) | 3735 | 25400 | 147 | 1817 (12%) | 1302 | 8761 | 148 | 3047 (28%) | 2433 | 16639 | 140 |
| Mean (SD) | ||||||||||||
| Marital status | ||||||||||||
| Married | 8256 (32%) | 3306 | 31697 | 104 | 5675 (38%) | 1870 | 19159 | 93 | 2581 (23%) | 1436 | 12537 | 114 |
| Single | 1633 (6%) | 782 | 6492 | 120 | 668 (4%) | 227 | 2151 | 92 | 965 (9%) | 555 | 4341 | 127 |
| Divorced (Separated) | 504 (2%) | 174 | 1721 | 101 | 291 (2%) | 71 | 832 | 85 | 213 (2%) | 103 | 889 | 115 |
| Widowed | 6052 (24%) | 3036 | 24947 | 121 | 3018 (20%) | 1169 | 10501 | 111 | 3034 (28%) | 1867 | 14446 | 129 |
| Unknown | 8973 (35%) | 4831 | 41885 | 115 | 4912 (33%) | 1995 | 19532 | 97 | 4061 (37%) | 2836 | 22352 | 126 |
| Urban / Rural (2010) | ||||||||||||
| Rural | 7131 (28%) | 3157 | 29116 | 108 | 4662 (32%) | 1673 | 16737 | 99 | 2469 (22%) | 1484 | 12379 | 119 |
| Urban | 17560 (69%) | 8649 | 74957 | 115 | 9468 (65%) | 3496 | 33996 | 102 | 8092 (75%) | 5153 | 40960 | 125 |
| Missing | 727 (3%) | 434 (3%) | 293 (3%) | |||||||||
| Comorbidity medications | ||||||||||||
| 0 | 1211 (5%) | 616 | 5198 | 118 | 803 (5%) | 318 | 2985 | 106 | 408 (4%) | 298 | 2213 | 134 |
| 1–5 | 1188 (5%) | 686 | 5314 | 129 | 796 (5%) | 391 | 3163 | 123 | 392 (4%) | 295 | 2150 | 137 |
| 6–10 | 835 (3%) | 540 | 3918 | 137 | 508 (3%) | 258 | 2018 | 127 | 327 (3%) | 282 | 1899 | 148 |
| 11–15 | 749 (3%) | 476 | 3514 | 135 | 448 (3%) | 236 | 1882 | 125 | 301 (3∧) | 240 | 1631 | 147 |
| ≥16 | 21435 (84%) | 9811 | 88798 | 110 | 12009 (82%) | 4129 | 42126 | 98 | 9426 (87%) | 5682 | 46671 | 121 |
| NIMDM (2010) | ||||||||||||
| 1–3 | 7021 (28%) | 3285 | 28835 | 113 | 4240 (28%) | 1600 | 15162 | 105 | 2781 (26%) | 1685 | 13673 | 123 |
| 4–6 | 7109 (28%) | 3319 | 29734 | 111 | 4196 (28%) | 1540 | 15155 | 101 | 2913 (27%) | 1779 | 14578 | 122 |
| 7–10 | 10561 (42%) | 5202 | 45504 | 114 | 5694 (42%) | 2029 | 20416 | 99 | 4867 (45%) | 3173 | 25088 | 126 |
| Missing | 727 (3%) | 434 | 293 (3%) | |||||||||
NIMDM, Northern Ireland Multiple Deprivation Measure.
Mortality by demographic characteristics
Results of Cox proportional hazard models are shown in Tables 2 and 3. In comparison to females, men had a significant higher risk of mortality (HR 1.28, 95% CI 1.23–1.33, p < 0.001). This was also true for PwD who had been in a care home at least once (HR 1.28, 95% CI = 1.21–1.35, p < 0.001) and for PwD who have never been in a care home (HR 1.26, 95% CI = 1.19–1.34, p < 0.001). PwD in older age categories had significantly higher mortality rates. When considering all the data, people in the higher category of NIMDM, i.e., those living in less deprived areas, had significantly lower mortality rates in comparison to those in the lowest categories (HR 0.93, 95% CI = 0.89–97, p < 0.001). Urban/rural classification did not significantly affect mortality rates. People who were divorced, single, and widowed had significantly higher risk of mortality after diagnosis; these results held when the data was split between PwD who had transitioned to a care home at least once and those who had not.
Table 2
Cox proportional hazard model assessing factors associated with mortality
| HR (95% CI) | Std Err. | HR (95% CI) | Std Err. | HR (95% CI) | Std Err. | |
| All data (n = 25,418) | No care home transitions (n = 14,564) | At least one care home transition (n = 10,854) | ||||
| Gender | ||||||
| Female | Ref. | Ref. | Ref. | |||
| Male | 1.28 (1.23–1.33)** | 0.02 | 1.26 (1.19–1.34)** | 0.03 | 1.28 (1.21–1.35)** | 0.03 |
| Age | ||||||
| <65 | Ref. | Ref. | Ref. | |||
| 65–74 | 1.20 (1.07–1.34)** | 0.06 | 1.27 (1.10–1.47)** | 0.09 | 1.11 (0.93–1.3) | 0.09 |
| 75–84 | 1.50 (1.35–1.67)** | 0.08 | 1.73 (1.50–1.99)** | 0.12 | 1.30 (1.10–1.53)** | 0.10 |
| 85 | 1.65 (1.48–1.85)** | 0.09 | 1.94 (1.67–2.25)** | 0.14 | 1.45 (1.23–1.71)** | 0.12 |
| Mean (SD) | ||||||
| Marital status | ||||||
| Married | Ref. | Ref. | Ref. | |||
| Single | 1.15 (1.06–1.25)** | 0.04 | 1.08 (0.94–1.25) | 0.07 | 1.26 (1.14–1.39)** | 0.06 |
| Divorced (Separated) | 1.25 (1.07–1.46)* | 0.09 | 1.28 (1.00–1.64)* | 0.07 | 1.28 (1.05–1.57)* | 0.13 |
| Widowed | 1.10 (1.04–1.16)** | 1.10 | 1.08 (0.94–1.25)* | 0.16 | 1.15 (1.07–1.24)** | 1.15 |
| Unknown | 0.80 (0.77–0.84)** | 0.80 | 0.76 (0.71–0.82)** | 0.02 | 0.86 (0.80–0.92)** | 0.02 |
| Urban / Rural (2010) | ||||||
| Rural | Ref. | Ref. | Ref. | |||
| Urban | 0.99 (0.95–1.03) | 0.02 | 0.99 (0.93–1.05) | 0.03 | 1.02 (0.96–1.08) | 0.03 |
| Comorbidity medications | ||||||
| 0 | Ref. | Ref. | Ref. | |||
| 1–5 | 1.07 (0.96–1.20) | 0.06 | 1.11 (0.95–1.30) | 0.08 | 1.03 (0.87–1.21) | 0.08 |
| 6–10 | 1.10 (0.98–1.24) | 0.06 | 1.20 (1.02–1.42)* | 0.10 | 1.04 (0.88–1.22) | 0.08 |
| 11–15 | 1.16 (1.03–1.31)* | 0.07 | 1.16 (0.97–1.37) | 0.10 | 1.18 (0.99–1.40) | 0.10 |
| ≥16 | 1.08 (1.00–1.18)* | 0.04 | 1.11 (0.98–1.25) | 0.06 | 1.09 (0.97–1.23) | 0.06 |
| NIMDM (2010) | ||||||
| 1–3 | Ref. | Ref. | Ref. | |||
| 4–6 | 0.95 (0.90–1.00) | 0.02 | 0.94 (0.88–1.02) | 0.03 | 0.96 (0.90–1.03) | 0.03 |
| 7–10 | 0.93 (0.89–0.97)** | 0.02 | 0.93 (0.87–1.00) | 0.03 | 0.94 (0.89–1.00) | 0.02 |
*p < 0.05, **p < 0.001; NIMDM, Northern Ireland Multiple Deprivation Measure.
Table 3
Cox proportional hazard model assessing factors and type of comorbidity medication associated with mortality
| HR (95% CI) | Std Err. | HR (95% CI) | Std Err. | HR (95% CI) | Std Err. | |
| All data (n = 25,418) | No care home transitions (n = 14,564) | At least one care home transition (n = 10854) | ||||
| Gender | ||||||
| Female | Ref. | Ref. | Ref. | |||
| Male | 1.27 (1.22–1.32)** | 0.02 | 1.26 (1.19–1.34)** | 0.03 | 1.27 (1.21–1.34)** | 0.03 |
| Age | ||||||
| <65 | Ref. | Ref. | Ref. | |||
| 65–74 | 1.19 (1.07–1.34)** | 0.06 | 1.27 (1.10–1.47)** | 0.09 | 1.11 (0.93–1.32) | 0.09 |
| 75–84 | 1.50 (1.35–1.67)** | 0.08 | 1.74 (1.51–2.00)** | 0.12 | 1.30 (1.10–1.53)** | 0.10 |
| 85 | 1.65 (1.48–184)** | 0.09 | 1.95 (1.68–2.27)** | 0.14 | 1.45 (1.23–1.71)** | 0.12 |
| Mean (SD) | ||||||
| Marital status | ||||||
| Married | Ref. | Ref. | Ref. | |||
| Single | 1.16 (1.07–1.25)** | 0.04 | 1.08 (0.94–1.25)* | 0.07 | 1.27 (1.15–1.40)** | 0.13 |
| Divorced (Separated) | 1.25 (1.07–1.46)* | 0.09 | 1.28 (1.00–1.63) | 0.15 | 1.28 (1.05–1.57)* | 0.06 |
| Widowed | 1.10 (1.05–1.16)** | 0.02 | 1.09 (1.00–1.18)** | 0.04 | 0.86 (0.81–.92)** | 0.02 |
| Unknown | 0.81 (0.77–0.85)** | 0.01 | 0.77 (0.72–0.82)* | 0.02 | 1.16 (1.07–1.24)** | 0.04 |
| Urban / Rural (2010) | ||||||
| Rural | Ref. | Ref. | Ref. | |||
| Urban | 0.99 (0.95–1.03) | 0.02 | 0.99 (0.94–1.06) | 0.03 | 1.02 (0.96–1.08) | 0.03 |
| Type of comorbidity medications | ||||||
| No comorbidity medication | Ref. | Ref. | Ref. | |||
| Arrhythmic | 2.44 (1.01–5.91)* | 1.10 | 4.14 (1.5–11.14)* | 2.09 | 0.92 (0.12–6.60) | 0.92 |
| Hypertension | 1.13 (0.95–1.34) | 0.10 | 1.10 (0.87–1.40) | 0.13 | 1.14 (0.88–1.48) | 0.15 |
| Lipid regulating | 1.02 (0.91–1.14) | 0.05 | 0.99 (0.85–1.16) | 0.07 | 1.03 (0.86–1.23) | 0.09 |
| Hypnotics and anxiolytics | 1.08 (0.98–1.19) | 0.05 | 1.10 (0.95–1.26) | 0.07 | 1.07 (0.93–1.24) | 0.07 |
| Antipsychotic | 1.06 (0.97–1.17) | 0.05 | 1.17 (1.02–1.34)* | 0.08 | 1.03 (0.91–1.18) | 0.06 |
| Antidepressant | 1.08 (0.99–1.17) | 0.04 | 1.10 (0.98–1.25) | 0.06 | 1.09 (0.96–1.23) | 0.06 |
| Diabetic | 1.18 (1.07–1.29)** | 0.05 | 1.19 (1.04–1.36)* | 0.08 | 1.19 (1.04–1.36)** | 0.08 |
| NIMDM (2010) | ||||||
| 1–3 | Ref. | Ref. | Ref. | |||
| 4–6 | 0.95 (0.90–1.00) | 0.02 | 0.95 (0.88–1.02) | 0.03 | 0.96 (0.89–1.03) | 1.03 |
| 7–10 | 0.93 (0.89–0.98)** | 0.02 | 0.94 (0.88–1.00) | 0.03 | 0.94 (0.89–1.00) | 1.00 |
*p < 0.05, **p < 0.001; NIMDM, Northern Ireland Multiple Deprivation Measure.
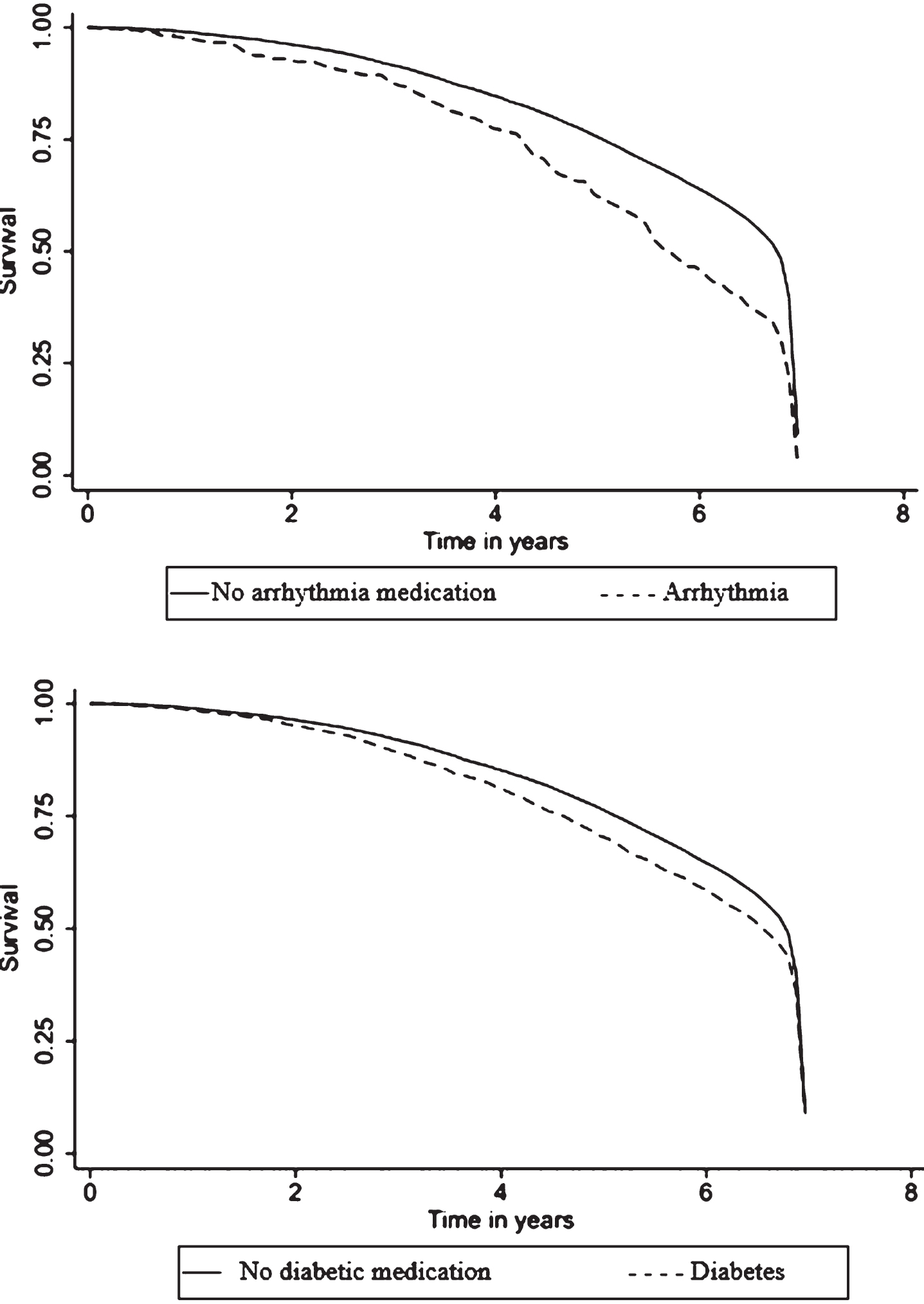
In comparison to those people with no comorbidity medications, people who had been dispensed between 11–15 comorbidity medications (HR 1.16, 95% CI = 1.03–1.31, p < 0.001) or 16 or more medications (HR 1.08, 95% CI 1.00–1.18, p < 0.001) had significantly higher mortality rates when compared to people with no comorbidity medications. However, this effect disappears when the data is split between PwD who have been in a care home at least once and those that have not. Table 3 closely reflects the findings of Table 2, but also highlights that diabetic medication in particular significantly increases mortality rates in comparison to people who have no comorbidities (HR 1.18, 95% CI = 1.07–1.29, p < 0.001). This was also true for PwD who have been in a care home at least once (HR 1.19, 95% CI = 1.04–1.36, p < 0.001) and those that have not (HR 1.19, 95% CI = 1.04–1.36, p < 0.001). Anti-arrhythmic medication significantly increases mortality rates for PwD who have never been in a care home (HR 4.14, 95% CI = 1.5–11.14, p < 0.001) and when all data is analyzed together (HR 2.44, 95% CI = 1.01–5.91, p < 0.001), but not for PwD who have been transitioned to a care home at least once (HR 0.92, 95% CI = 0.12–6.60, p < 0.001). Figure 1 displays Kaplan-Meier survival functions for PwD who have taken anti-arrhythmia and diabetic medication in comparison to those who have not.
Fig.1
Survival function derived from cox proportional hazard regression adjusted for covariates in Table 3. Y axis denotes estimated survival percentages. X axis is time in years. Of the different classes of medication extracted from the enhanced prescribing database, only anti-arrhythmic and diabetic medication significantly increased mortality rates among people prescribed anti-dementia drugs in our study population.
DISCUSSION
Given the numerous studies which have assessed factors associated with mortality after a dementia diagnosis [8, 9, 25, 26], understanding these factors within the context of dementia in NI is also essential, as it may help provide valuable information to the person with dementia, their family, carers, and medical team. To the best of our knowledge, this is the first retrospective analysis to investigate factors that influence mortality after a dementia diagnosis in NI. Our data suggested that there was 13,289 people prescribed anti-dementia drugs currently living with dementia in NI. However, given that we used a proxy measure for dementia diagnosis it is likely that some people with dementia in NI are missing from our cohort. The true number is likely between the number we report (13,289) and the number reported in the NI dementia strategy (19,000) [2]. The results of the present study show that increasing age and higher numbers of comorbidity medications are significantly associated with increased mortality after dementia diagnosis. When considering the entire cohort, the deaths per 1000 PY was 114, a number which is slightly lower than similar cohorts which have investigated mortality rates after diagnosis [12, 27], but also lower than others [11]. However, these previous cohorts, which used data from the Swedish dementia registry [12], the Neurological Disorders in Central Spain [27], and the Registry of Dementias of Girona, all analyzed PwD over a longer time frame, possibly leading to a higher deaths per 1000 person years. Average survival time after diagnosis was 4.5 years and deaths/1000 person years was 114, which are very similar figures to those observed in other mortality studies over similar time frames [6, 7]. This discrepancy between official government statistics and our analysis could be explained through some of the limitations in our analysis, such as using dementia medication as a proxy for diagnosis, as this proxy measure means that PwD who are not taking dementia medication are not included in the analysis. Most people on cholinesterase inhibitors and memantine have a diagnosis of Alzheimer’s disease, mixed dementia, or Parkinson’s disease and Lewy body dementia. Patients with vascular dementia and frontotemporal dementia are excluded from the dataset as these medications are not licensed for these conditions. Patients intolerant of cholinesterase inhibitors and memantine are also likely excluded from the dataset. Significantly lower mortality risk was found in women in comparison to men (Table 2), which concurs with past research [8–10]. This is of interest as prevalence rates are so much higher in women with 65% of our dataset being female in keeping with national statistics [28]. Mortality rates were not influenced by whether the person lived in an urban or rural area. Our analysis aligns the findings of past research which have indicated that marriage may lower mortality rates after diagnosis [7, 29], as people who are divorced, separated, or widowed had significantly higher mortality rates in comparison to those who are married. It is unlikely that this finding suggests that people who are unmarried are at an elevated risk of dementia, but rather suggests a positive relationship between marriage and lifestyle factors which may reduce mortality rates after a dementia diagnosis. For instance, PwD who are married might be more likely to be diagnosed earlier, as a result of a spouse noticing behaviors which may be indicative of dementia. The spouse may also ensure the PwD is more socially, physically, and mentally active after a dementia diagnosis; factors that have been proven to be of benefit [30, 31], Additionally, spouses may be more than likely to play an active role in medication management [32]. However, we emphasize that for the marriage variable, 35% of data was missing. Additionally, information on marriage was not recorded at baseline (2010) but rather at different times between 2010–2016, therefore the results with respect to marriage should be interpreted with caution. We also found that PwD who had not transitioned to a care home had more comorbidity medications (Table 1), in comparison to PwD who had transitioned to a care home. This finding disagrees with past research which has suggested that PwD often have more comorbidity medications if they have transitioned to a care home at least once [14]. We also noted that more deaths occurred in PwD who had transitioned to a care home at least once (n = 6797) in comparison to PwD who had not transitioned to a care home (n = 3066). Moreover, many more females had transitioned to a care home at least once (n = 7852) in comparison to males (n = 3272); however, mortality rates were significantly higher for males in comparison to females if they had transitioned to a care home at least once (Table 2).
Research has highlighted that there is a need for an elevated focus on assessing and monitoring comorbidities and their associated medications in PwD [33, 34]. Comorbidity medication was high for most of the PwD in our dataset, as over 85% had been prescribed 15 or more comorbidity medications between 2010 and 2016. Although we have looked at comorbidity medications over a seven-year period, recent studies have shown that at any given point in time, PwD had an average of 5.4 comorbidity medications [35]. For several BNF sections, we had access to the number of items prescribed to each patient between 2010 and 2016. We noted that when analyzing all of the data together, higher levels of comorbidity medication was associated with significantly higher mortality rates. Indeed, a higher number of comorbidity medications has been consistently associated with higher mortality rates in past research [12, 21, 27]. When the BNF sections are categorized into different types of comorbidity medications (Table 3), those on anti-arrhythmic and diabetic medication had significantly higher mortality rates in comparison to PwD with no comorbidities. Although this finding should be interpreted with caution, as it is a proxy measure rather than an official diagnosis of the comorbidities, the findings dovetail those of recent studies which suggest that those with diabetes and arrhythmic conditions have higher mortality rates [36, 37]. Moreover, PwD who have also been diagnosed with dementia have poorer medication management and are less likely to receive the recommended annual monitoring for diabetes than people without dementia [38]. This might explain why PwD in our cohort who had been dispensed diabetic medication and had transitioned to a care home at least once did not have significantly higher mortality rates, as their diabetes may have been controlled better in a care home setting. Given that some comorbidity medications such as those with a high anticholinergic burden are likely to counteract the effects of dementia management medications [39], careful monitoring and management of comorbidity medications could potentially lower mortality rates after a dementia diagnosis.
In NI, the NIMDM is often used to determine an individual’s deprivation score [17]. The NIMDM ranges from 1–10, with lower values indicating higher levels of deprivation. Previous work in NI has indicated that people with lower NIMDM scores have higher levels of mental illness and poorer mental health [40]. Moreover, recent research which looked at nationwide data of PwD between 2000 and 2010 has shown that both males and females with dementia who lived in more deprived areas had higher levels of mortality in comparison to PwD who lived in less deprived areas [41]. Our findings align with those of past research, as we found that people in the less deprived areas (NIMDM scores 7–10) had significantly lower levels of mortality in comparison to people living in more deprived areas. Additional post hoc analysis also showed that PwD in deprived areas had a significantly higher number of average comorbidity medications (t (24689) = 14.9; p = <0.0001). Given the unfavorable prognosis that may await people in deprived areas after a dementia diagnosis, future research should continue to assess and understand why mortality rates are higher for PwD in more deprived areas and an integrated response between dementia specialists, clinicians, carers, and researchers may be needed to improve the outcomes of PwD in highly deprived areas.
Our findings should be interpreted within the context of several limitations. We have used the first prescription date of cholinesterase inhibitors as a proxy for dementia diagnosis and length of time on anti-dementia drugs as a proxy for dementia severity, a methodology which has been used to identify PwD from the EPD in past research [18] but which may lead to underestimation of dementia rates and exclusion of people with other forms of dementia. Drugs for dementia are licensed only for the treatment of mild to severe dementia in Alzheimer’s disease and mild to moderate dementia in Parkinson’s disease. As stated previously using medication as a proxy for dementia diagnosis therefore may exclude people with dementias caused by other diseases and prevented us from investigating mortality rates in different types of dementia [16]. As a case in point, recent research has indicated that dementia with Lewy bodies is the second most common degenerative dementia and dementia with Lewy bodies has a higher mortality rate relative to Alzheimer’s disease [12, 42]. However, using our proxy measure, we were unable to add to these findings. A date of dementia diagnosis was determined as the first date that a dementia medication was prescribed; however, dementia is likely to be present years or decades before an official diagnosis is recorded [6]. Although the Enhanced Prescribing Database provides a wealth of data for researchers, it is only able to scan approximately 80–90% of all prescribed medications. Further, the lack of over-the-counter and hospital medications in the EPD mean that there may be an under prevalence of comorbidity medications in the data set. Finally, we conducted a series of t-tests, and although research has suggested that it may not be necessary to change the level of significance [43], this multiple testing could have potentially lead to an overestimation of effects [44].
Conclusions
In our cohort of PwD, male gender, higher levels of comorbidity medication, higher levels of deprivation, and anti-arrhythmic and diabetic medication were associated with increased mortality. There was a higher number of deaths and person years at risk among people with dementia who had transitioned to a care home at least once. More research is needed to determine why PwD in more deprived areas have higher mortality rates.
ACKNOWLEDGMENTS
The authors would like to thank staff at the Honest Broker Service, Northern Ireland for extracting data for analysis and providing clearance of statistical analysis. The authors would like to thank the Atlantic Philanthropies, the Office of the First and Deputy First Minister and the Department of Health for funding this study.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0751r2).
REFERENCES
[1] | Hofmann-Apitius M ((2015) ) Is dementia research ready for big data approaches? BMC Med 13: , 145. |
[2] | Department of Health Social Services and Public Safety Northern Ireland ((2011) ) Improving Dementia Services in Northern Ireland. |
[3] | Ganguli M , Dodge HH , Shen C , Pandav RS , DeKosky ST ((2005) ) Alzheimer disease and mortality: A 15-year epidemiological study. Arch Neurol 62: , 779–784. |
[4] | Wolfson C , Wolfson DB , Asgharian M , M’Lan CE , Østbye T , Rockwood K , Hogan DB ((2001) ) A reevaluation of the duration of survival after the onset of dementia. N Engl J Med 344: , 1111–1116. |
[5] | Steenland K , MacNeil J , Seals R , Levey A ((2010) ) Factors affecting survival of patients with neurodegenerative disease. Neuroepidemiology 35: , 28–35. |
[6] | Eriksdotter M ((2014) ) Mortality risk after dementia diagnosis by dementia type and underlying factors: A cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis 41: , 467–477. |
[7] | Xie J , Brayne C , Matthews FE ((2008) ) Survival times in people with dementia: Analysis from population based cohort study with 14 year follow-up. BMJ 336: , 258–262. |
[8] | Dewey ME , Saz P ((2001) ) Dementia, cognitive impairment and mortality in persons aged 65 and over living in the community: A systematic review of the literature. Int J Geriatr Psychiatry 16: , 751–761. |
[9] | Agüero-Torres H , Fratiglioni L , Guo Z , Viitanen M , Winblad B ((1999) ) Mortality from dementia in advanced age: A 5-year follow-up study of incident dementia cases. J Clin Epidemiol 52: , 737–743. |
[10] | Aevarsson Ó , Svanborg A , Skoog I ((1998) ) Seven-year survival rate after age 85 years: Relation to alzheimer disease and vascular dementia. Arch Neurol 55: , 1226–1232. |
[11] | Garre-Olmo J , Ponjoan A , Inoriza JM , Blanch J , Sánchez-Pérez I , Cubí R , de Eugenio R , Turró-Garriga O , Vilalta-Franch J ((2019) ) Survival, effect measures, and impact numbers after dementia diagnosis: A matched cohort study. Clin Epidemiol 11: , 525–542. |
[12] | Garcia-Ptacek S , Farahmand B , Kåreholt I , Religa D , Cuadrado ML , Eriksdotter M ((2014) ) Mortality risk after dementia diagnosis by dementia type and underlying factors: A cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis 41: , 467–77. |
[13] | Østbye T , Steenhuis R , Wolfson C , Walton R , Hill G ((1999) ) Predictors of five-year mortality in older Canadians: The Canadian study of health and aging. J Am Geriatr Soc 47: , 1249–1254. |
[14] | Vossius C , Selbæk G , Šaltytė Benth J , Bergh S ((2018) ) Mortality in nursing home residents: A longitudinal study over three years. PLoS One 13: , e0203480. |
[15] | Davis P ((2007) ) Northern Ireland’s electronic prescribing and eligibility system. Br J Healthc Comput Inf Manag 24: , 12. |
[16] | Committee JF ((2015) ) British National Formulary 69th edition, BMJ Group and Pharmaceutical Press, London, UK. |
[17] | Northern Ireland Multiple Deprivation Measure 2017 (NIMDM2017). Northern Ireland Statistics and Research Agency. |
[18] | Barry HE , Cooper JA , Ryan C , Passmore AP , Robinson AL , Molloy GJ , Darcy CM , Buchanan H , Hughes CM ((2016) ) Undefined Potentially inappropriate prescribing among people with dementia in primary care: A retrospective cross-sectional study using the enhanced prescribing database. J Alzheimers Dis 52: , 1503–1513. |
[19] | Gudala K , Bansal D , Schifano F , Bhansali A ((2013) ) Diabetes mellitus and risk of dementia: A meta-analysis of prospective observational studies. J Diabetes Investig 4: , 640–650. |
[20] | Enache D ((2016) ) Antidepressants and mortality risk in a dementia cohort: Data from SveDem, the Swedish Dementia Registry. |
[21] | Kales HC , Valenstein M , Kim HM , McCarthy JF , Ganoczy D , Cunningham F , Blow FC ((2007) ) Mortality risk in patients with dementia treated with antipsychotics versus other psychiatric medications. Am J Psychiatry 164: , 1568–1576. |
[22] | Guthrie B , Clark SA , Mccowan C ((2010) ) The burden of psychotropic drug prescribing in people with dementia: A population database study. Age Ageing 39: , 637–642. |
[23] | Hernandez I ((2016) ) Risk factors for cardiovascular events of antidementia drugs in Alzheimer’s disease patients. J Clin Gerontol Geriatr 7: , 77–82. |
[24] | Lyles CR , Lyles CR , Parker MM , Karter AJ , Huang ES , Whitmer RA ((2012) ) Association of depression with increased risk of dementia in patients with type 2 diabetes. Arch Gen Psychiatry 69: , 410–417. |
[25] | Todd S , Barr S , Roberts M , Passmore AP ((2013) ) Survival in dementia and predictors of mortality: A review. Int J Geriatr Psychiatry 28: , 1109–1124. |
[26] | Aneshensel CS , Pearlin LI , Schuler RH ((2000) ) Mortality among people with dementia. J Gerontol Soc Sci 55: , 152–162. |
[27] | Villarejo A , Benito-León J , Trincado R , Posada IJ , Puertas-Martín V , Boix R , Medrano MRAJ , Bermejo-Pareja F ((2011) ) Dementia-associated mortality at thirteen years in the NEDICES Cohort Study. J Alzheimers Dis 26: , 543–551. |
[28] | Prevalence by gender in the UK | Dementia Statistics Hub. |
[29] | Sommerlad A , Ruegger J , Singh-Manoux A , Lewis G , Livingston G ((2018) ) Marriage and risk of dementia: Systematic review and meta-analysis of observational studies. J Neurol Neurosurg Psychiatry 89: , 231–238. |
[30] | Blondell SJ , Hammersley-Mather R , Veerman JL ((2014) ) Does physical activity prevent cognitive decline and dementia?: A systematic review and meta-analysis of longitudinal studies. BMC Public Health 14: , 510. |
[31] | Anderson K , Grossberg GT ((2014) ) Brain games to slow cognitive decline in Alzheimer’s disease. J Am Med Dir Assoc 15: , 536–537. |
[32] | While C , Duane F , Beanland C , Koch S ((2013) ) Medication management: The perspectives of people with dementia and family carers. Dementia 12: , 734–750. |
[33] | Fox C , Smith T , Maidment I , Hebding J , Madzima T , Cheater F , Cross J , Poland F , White J , Young J ((2014) ) The importance of detecting and managing comorbidities in people with dementia? Age Ageing 43: , 741–743. |
[34] | Subramaniam H ((2019) ) Comorbidities in dementia: Time to focus more on assessing and managing comorbidities. Age Ageing 48: , 314–315. |
[35] | Clague F , Mercer SW , McLean G , Reynish E , Guthrie B ((2016) ) Comorbidity and polypharmacy in people with dementia: Insights from a large, population-based cross-sectional analysis of primary care data. Age Ageing 46: , 33–39. |
[36] | Tilvis RS , Kahonen-Vare MH , Jolkkonen J , Valvanne J , Pitkala KH , Strandberg TE ((2004) ) Predictors of cognitive decline and mortality of aged people over a 10-year period. J Gerontol 59A: , 268–274. |
[37] | Danielsson B , Collin J , Jonasdottir Bergman G , Borg N , Salmi P , Fastbom J ((2016) ) Antidepressants and antipsychotics classified with torsades de pointes arrhythmia risk and mortality in older adults - A Swedish nationwide study. Br J Clin Pharmacol 81: , 773–783. |
[38] | Thorpe CT , Thorpe JM , Kind AJH , Bartels CM , Everett CM , Smith MA ((2012) ) Receipt of monitoring of diabetes mellitus in older adults with comorbid dementia. J Am Geriatr Soc 60: , 644–651. |
[39] | Fox C , Livingston G , Maidment ID , Coulton S , Smithard DG , Boustani M , Katona C ((2011) ) The impact of anticholinergic burden in Alzheimer’s dementia-the LASER-AD study. Age Ageing 40: , 730–735. |
[40] | Maguire A , French D , Reilly DO ((2016) ) Residential segregation, dividing walls and mental health: A population-based record linkage study. J Epidemiol Community Health 70: , 845–854. |
[41] | van de Vorst IE , Koek HL , Stein CE , Bots ML , Vaartjes I ((2016) ) Socioeconomic disparities and mortality after a diagnosis of dementia: Results from a nationwide registry linkage study. Am J Epidemiol 184: , 219–226. |
[42] | Moylett S , Price A , Cardinal RN , Aarsland D , Mueller C , Stewart R , O’Brien JT ((2019) ) Clinical presentation, diagnostic features, and mortality in dementia with Lewy bodies. J Alzheimers Dis 67: , 995–1005. |
[43] | Perneger TV ((1999) ) Adjusting for multiple testing in studies is less important than other concerns. BMJ 318: , 1288–1288. |
[44] | Althouse AD ((2016) ) Adjust for multiple comparisons? It’s not that simple. Ann Thorac Surg 101: , 1644–1645. |


