
Comparative Cognitive Effects of Choreographed Exercise and Multimodal Physical Therapy in Older Adults with Amnestic Mild Cognitive Impairment: Randomized Clinical Trial
Abstract
Background:
Recent research on mild cognitive impairment (MCI) has primarily focused on searching for measures to prevent or delay the progression of MCI to dementia. Physical exercise has shown to be effective in the prevention of age-related cognitive decline in elderly adults with MCI. However, the most effective type and dose of exercise for the improvement of cognition are yet to be determined.
Objective:
To compare the cognitive effects of choreographed exercise (Choreography group) with a multimodal physical therapy program (Physical Therapy group) in elderly adults with amnestic MCI, a population with an increased risk of developing dementia.
Methods:
We conducted a randomized clinical trial with two parallel groups under allocation concealment and assessor blinding. Participants were allocated into Choreography or Physical Therapy group and performed exercises twice per week in 60-minute sessions during 12 weeks.
Results:
Thirty-six participants with amnestic MCI, ages 65 to 85, were assessed at baseline and after 12 weeks of intervention, by comprehensive validated neuropsychological and physical assessments. A Repeated measures General Lineal Model showed statistically significant differences in cognitive and physical outcomes. Both groups significantly improved in visual delayed recall. The Choreography group exhibited significantly more benefits on verbal recognition memory than the Physical Therapy group.
Conclusion:
Greater cognitive benefits were achieved in the choreographic intervention than in the multimodal physical therapy, mainly in those functions more related to the risk of conversion to dementia. Additional studies are needed to confirm whether the observed effects are related to delayed onset of Alzheimer’s disease in elderly adults with amnestic MCI.
INTRODUCTION
It is well known that mild cognitive impairment (MCI), mainly the amnestic type (aMCI), is a high risk factor for developing dementia [1–3]. In the last decade, research on MCI has focused on searching for measures to prevent or delay the progression of aMCI to dementia [4]. The challenge, however, is to design treatments that manage to achieve that goal [5, 6].
Physical exercise is a promising intervention because it has shown to prevent age-related cognitive decline in older adults with MCI [7–9]. With aging, some cognitive functions such as learning, memory, and executive functioning gradually decline and become slower and inefficient [10]. Prospective observational studies have demonstrated that individuals who are more active in midlife and late life have lower risk of global decline and incidence of dementia than those who do not [11–14]. A meta-analysis of prospective cohort studies has identified an association between higher levels of physical exercise and a greater reduced risk of developing MCI, by at least 35% [8].
Exercise may impact the physiology of the aging brain by means of several mechanisms (e.g., reduction of cardiovascular diseases, improvement of cerebral perfusion, increase the production of neurotrophic factors, among others), thus acting as a brain neuroprotective factor [15]. The human brain undergoes morphological changes in response to various types of physical trainings [16–18]. Exercise aimed at skeletal muscle induces neuronal plasticity which may slow down, or even reverse, the pathophysiological evolution of Alzheimer’s disease (AD) [19]. The hippocampus is one of the major brain sites of neuroplasticity, with the ability to generate new neurons throughout the lifespan [20] and is sensitive to the effects of physical exercise [21, 22]. These findings are relevant, since the hippocampus and parahippocampal gyrus are the first areas of accumulation of pathology in individuals developing AD [23, 24].
Unfortunately, the most effective type of exercise for improving cognitive functions remains unclear [9]. It is hypothesized that not all physical modalities have equal effectiveness in cognitive functioning. Some recent studies have demonstrated that dancing provides healthy seniors benefits in sensory, motor, and cognitive demands, which counteract age-related decline in cognitive and physical abilities [25–29]. Long-term dance programs seem to be more effective in inducing neuroplasticity in healthy elderly brains than does engaging in repetitive physical exercise [30, 31]. However, less is known about their effectiveness in elderly people with MCI. Zhu et al. demonstrated in 2018 that using an aerobic dance routine, based on learning a sequence of movements in a specific order that requires practice and repetition, MCI individuals improved their performances on processing speed, episodic memory and global cognition after 12 weeks of training, compared to a control group where patients only received counselling on healthy life styles to prevent cognitive decline [32].
Several strategies to prevent cognitive decline and dementia in people at risk are currently being tested. Physical therapy programs applied in geriatrics incorporate the knowledge about brain plasticity and they are designed with the double aim of promoting functionality and delaying cognitive decline. However, only few randomized trials have applied multimodal interventions (training a variety of motor skills) in individuals with MCI. Suzuki et al. carried out a multicomponent exercise program, involving aerobic exercise, muscle strength, postural balance, and dual tasks, in amnestic and non-amnestic MCI participants. They found enhancements in global cognition and logical memory in amnestic-MCI exercise group compared to the controls groups [33]. Balance and coordination exercises also stimulate cognition from the sensory and motor systems and they may induce beneficial adaptations of cerebral function, when regularly practiced [34].
To our knowledge, there are few studies comparing the cognitive effects of different types of physical interventions, especially in people with aMCI [35, 36]. Extensive neuropsychological assessment is often lacking among physical exercise research. Most current studies have focused on analyzing global cognition [37, 38] or a few specific cognitive functions [33, 39, 40]. There is, consequently, a need to design studies that include comprehensive neuropsychological assessments, which could help to warrant early detection of the cognitive effects of specific physical exercise therapies. With this in mind, our study compared active experimental groups, where participants performed different types of physical exercise. They did so under the supervision of physiotherapists (PT), in contrast to studies where participants performed exercises by themselves at home, or took sedentary groups as controls [37, 41]. Thus, the aim of this study was to compare the cognitive effects of a motor learning training program based on choreographed sessions (Choreography group) with a multimodal physical therapy program that trained a variety of motor skills (Physical Therapy group), applied in elderly adults with aMCI.
MATERIALS AND METHODS
The present study is a 12-week comparative randomized controlled trial with two parallel groups, under allocation concealment and with blinding of the assessors. It adheres to the Standard Protocol Items Recommendations for Interventional Trials [42] and the Consolidated Standards of Reporting Trials (CONSORT) [43]. The study fulfils the requirements of Good Clinical Practice and ethical principles of the Declaration of Helsinki [44] and was approved by the Ethics Committee for Clinical Investigation of Hospital Clínic of Barcelona (Spain).
Participants
Participants were older adults who were visited at the Diagnostic Unit of Fundació ACE, Institut Català de Neurociències Aplicades (Barcelona, Spain), between June 2016 and May 2018. They were diagnosed with aMCI by the clinical team at daily consensus conference through the use of the Neuropsychological Battery of Fundació ACE (NBACE) [45, 46].
The following inclusion criteria were considered: (1) age older than 65 years or older; (2) literate; (3) fulfilled aMCI Petersen’s diagnostic criteria [47]; (4) normal general cognition, defined by a Mini-Mental State Examination (MMSE) [48, 49] score ≥24; (5) preserved performance in Activities of Daily Living (ADL), defined by a score <4 on the Blessed Dementia Rating Scale [50, 51]; (6) absence of dementia; (7) Clinical Dementia Rating (CDR) [52] score of 0.5; (8) no dementia medication taken (i.e., acetylcholinesterase inhibitors or memantine); (9) an objective measurable impairment in memory with or without impairment in other cognitive domains (i.e., single or multiple domain aMCI) [47]; (10) enough visual and auditory acuity to properly be able to follow group physical sessions (corrective measures such as hearing aids or glasses were allowed); and (11) informed consent signed.
The exclusion criteria were: (1) history of brain injury (e.g., cerebrovascular disease); (2) presence of psychiatric conditions (e.g., major depression, schizophrenia); (3) history of prolonged alcohol or drug abuse; (4) presence of severe cardiovascular disease (e.g., heart or respiratory insufficiency); (5) presence of musculoskeletal disorders with imbalance and gait disturbances, defined by a Berg Balance Scale (BBS) [53] score <40; Timed Up and Go Test (TUG) [54] score >20); (6) use of walking aids (e.g., sticks, crutches); and (7) participating in other clinical study.
Randomization, allocation concealment, and blinding
Regardless of their demographical characteristics, participants were randomly allocated to intervention groups using medical records numbers with “generate random groups” function of Excel (Microsoft Office Professional Plus 2010). In order to blind the allocation, an independent statistician created a matrix with the two study groups and applied the algorithm of randomization using the participants’ medical record numbers. The codes of medical records and assignation were unblinded after statistical analyses.
Participants were informed by telephone about allocation and they could choose between morning or afternoon sessions. All outcome assessors (PT and neuropsychologists) and statisticians were blinded to the allocation.
Procedures
Two study groups were set up, Choreography and Physical Therapy. Interventions were conducted at Fundació ACE’s Day Care Hospital, from April to June 2018 (12 weeks), and consisted of twice weekly sessions of 60-min, which followed identical structure for both groups: a 5-min warm up, 50-min of choreography or physical therapy, followed by a 5-min cool down. Choreography and Physical Therapy groups received the same warm up and cool down and both interventions were based on skill acquisition in response to external stimulus, using repetition as a learning strategy. Each group consisted of 8 participants and was guided by a PT specializing in geriatrics and who was trained ad hoc. PTs were trained on how to carry out the same intervention in each group by means of consensual meetings with the main researchers.
Both interventions were planned as light-to-moderate intensity, based on levels of perceived exertion. Participants were instructed to carry out their intervention activities without exceeding 2-3 points on the Borg Scale [55]. Physiotherapists in each group regularly enquired participants about their perceived fatigue levels during activities and helped them to maintain the target level of effort. Likewise, activities such as dancing or conditioning exercise are considered light-to moderate intensity (<6 METs), as per the METs Values of Common Physical Activities by the American College of Sports Medicine [56] and the Compendium of Physical Activities [57].
In the Choreography group, participants performed choreographed aerobic dances. A total of 12 video tutorials were prepared by a professional choreographer, and a variety of music styles were used (salsa, rock, rumba, pop, jive). Choreography videos were projected on a screen for visual support, while the PT taught and re-iterated the steps, in order to reinforce acquisition. Choreographed sessions followed an invariable structure: 1st) Learning the steps: participants learned the steps fractionally, following the instructions from the PT and watching the tutorial videos without music (1 attempt); 2nd) Performing choreography: participants put the learned steps into practice, repeating the choreographed video with music (4-5 attempts); 3rd) Music support only: participants reproduced the sequence of learned steps without visual support, by only listening to the music (1 attempt). Periods of rest where participants could sit down and drink water were included after each attempt.
In the Physical Therapy group, participants performed physical exercises following a multimodal physical therapy program. Different motor abilities, such as strength, endurance, flexibility, balance, coordination and gait were trained, according to physiotherapeutic common practices. Strength training was designed to help individuals maintain mobility and muscle strength, in order to be able to safely perform ADL. Flexibility was trained by performing gentle stretches to increase participants’ awareness of their muscles, and to help maintain adequate range of motion and mobility of their joints. Balance training aimed to allow individuals to achieve safe mobility, body awareness and to facilitate correct posture so as to avoid falls. Gait training was designed to train walk posture, coordination, aerobic endurance, and balance. Different materials were used during the execution of exercises (mats, wrist and ankle weights, sticks, balloons, balls, fit-balls, bosu, therabands, balance pads, and a metronome). The multimodal physical therapy followed a monthly structure of well-defined exercises, progressively increasing difficulty and load each month, increasing the number of repetitions per series and changing the base of support and the surfaces on which exercises were performed (Tables 1 and 2). Participants gradually progressed from exercising in sitting, stable positions (month 1) to doing so in standing (month 2) and on unstable surfaces and four-point keeling positions, where appropriate. Adaptations in exercise position, training load and number of repetitions were made according to individual physical condition, presence of comorbidities and tolerance of each participant. The reduced number (only eight) of participants per group allowed for a close monitoring of participants’ specific physical conditions.
Table 1
Temporal distribution of multimodal Physical Therapy
| Month | Week | Multimodal Physical Therapy |
| 1 | 1 | Stable sitting balance, stretching, flexibility, muscular strength (0 kg or 0.5 kg according to tolerance) |
| 2 | Unstable sitting balance, flexibility, coordination, resistance training | |
| 3 | Dynamic standing balance, strength and resistance training | |
| 4 | Dynamic gait, resistance training, coordination, dual tasks | |
| 2 | 5 | Unstable sitting balance, stretching, flexibility, coordination |
| 6 | Static sitting balance over unstable surfaces, flexibility, resistance | |
| 7 | Dynamic standing balance, strength and resistance training (0.5 kg or 1 kg according to tolerance) | |
| 8 | Gait circuit, resistance training, coordination, dual tasks | |
| 3 | 9 | Quadruped balance, flexibility, coordination |
| 10 | Standing equilibrium over unstable surfaces, strength and resistance training (0.5 kg or 1 kg according to tolerance) | |
| 11 | Gait circuit with somatosensory cues, resistance training, coordination | |
| 12 | Adapted playful game, coordination, resistance training, dual tasks |
Table 2
Example of a physical therapy session (week 11)
| Time wise | Week 11: Gait circuit, resistance and coordination training |
| Warm-up 5’ | Gentle body mobilization |
| Physical Therapy 50’ | Lengthening steps (cues on the floor) |
| Higher steps overcoming obstacles, hand to knee, hand to foot | |
| Forward/Backwards/Lateral | |
| Heels/Tip toe | |
| Arm swing (psychomotricity sticks) | |
| Tandem dynamic | |
| Walk with a fit-ball between hands, carrying a bag (dual task) | |
| Zig-zag, turns, stops | |
| Ankle weights (resistance, 0.5 kg or 1 kg according to tolerance) | |
| Change gait rhythm (metronome) | |
| Cool down 5’ | Stretching, breathing and relaxing exercises |
Clinical assessment
Participants received standardized neuropsychological and physical assessments at baseline, as well as upon completion of the intervention (at 12 weeks). A comprehensive standardized neuropsychological battery of tests was administered, which included the Word List Learning test from the Wechsler Memory Scale-Third Edition (WMS-III) [45, 58], the Visual Memory subtest of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) [59, 60], Trail Making Test [61, 62] (A and B), Letter Verbal Fluency (LVF) and Category Verbal Fluency (CVF) [63–66], Boston Naming Test (BNT) [67, 68], and Judgment of Line Orientation [69, 70]. Moreover, global cognition was measured by the Spanish version of the Mini-Mental State Examination (MMSE) [48, 49], while psycho-affective symptoms and quality of life were assessed by the Hospital Anxiety and Depression Scale (HADS) [71, 72] and the 36-Short Form (36-SF) [73, 74], respectively.
With regard to the physical functioning assessment, we used the Berg Balance Scale (BBS) [53] a standardized measurement tool to assess balance status and falls risk in elderly individuals (0–20: high risk of falling, 21–40: moderate risk, 41–56: slight risk). The Timed Up and Go Test (TUG) [54] was used to evaluate functional mobility (<10’: free mobility,<20’: mostly independent, 20’–29’: variable mobility,>20’: impaired mobility). To measure habitual physical activity, the Baecke Physical Activity Questionnaire for the Elderly [75, 76] was administered. This questionnaire takes into account usual household, leisure and sporting activities, on a one-year basis, to avoid seasonal bias. According to its total resulting score, individuals are categorized into sedentary (<9 points), moderately sedentary (9–16 points) or active (>16 points).
The primary outcome of the study was an improvement between baseline and 12-week follow-up on verbal memory performance, as measured by the Word List Learning test from the WMS-III. Changes in the Visual Memory subtest of the RBANS and the rest of cognitive tests scores were considered as secondary outcomes.
Sample size calculation
The sample size was calculated considering changes between baseline and 12-week follow-up in the verbal recognition memory task of the Word List Learning test from the WMS-III. A difference in this main variable of ≥2.5 points was assumed as clinically relevant. Knowing the dispersion of this variable in the so-far accumulated MCI samples [77], taking a risk alpha of 5% and a beta risk of 20% or less, it was estimated that each study group should be made up of 18 subjects. A dropout rate of 10% was estimated.
Statistical analysis
Statistical analysis was performed using the program SPSS for Windows (version 22.0, SPSS, Chicago, IL, USA). Neuropsychological and physical functioning outcomes included all participants who carried out the full intervention and completed final assessment. Quantitative variables that followed a normal distribution were presented as mean and standard deviation (SD). Also for these variables, Kolmogorov-Smirnov and Shapiro-Wilks tests were used for the assessment of normality, along with the use of QQ-Plot normal distribution graphics. Categorical variables were presented by their absolute frequencies and percentages. Between-group (Choreography versus Physical Therapy) differences, from baseline to end of study, were analyzed using a repeated measures General Lineal Model (GLM) covariating by age. All statistical tests of hypotheses were two-sided and employed a significance level of α= 0.05. In addition, and following the recommendations for reporting statistics in journals by the American Physiological Society [78], we considered to highlight those values lower than 0.01 (*p < 0.05; **p < 0.01). Analyses were based on per-protocol approach.
RESULTS
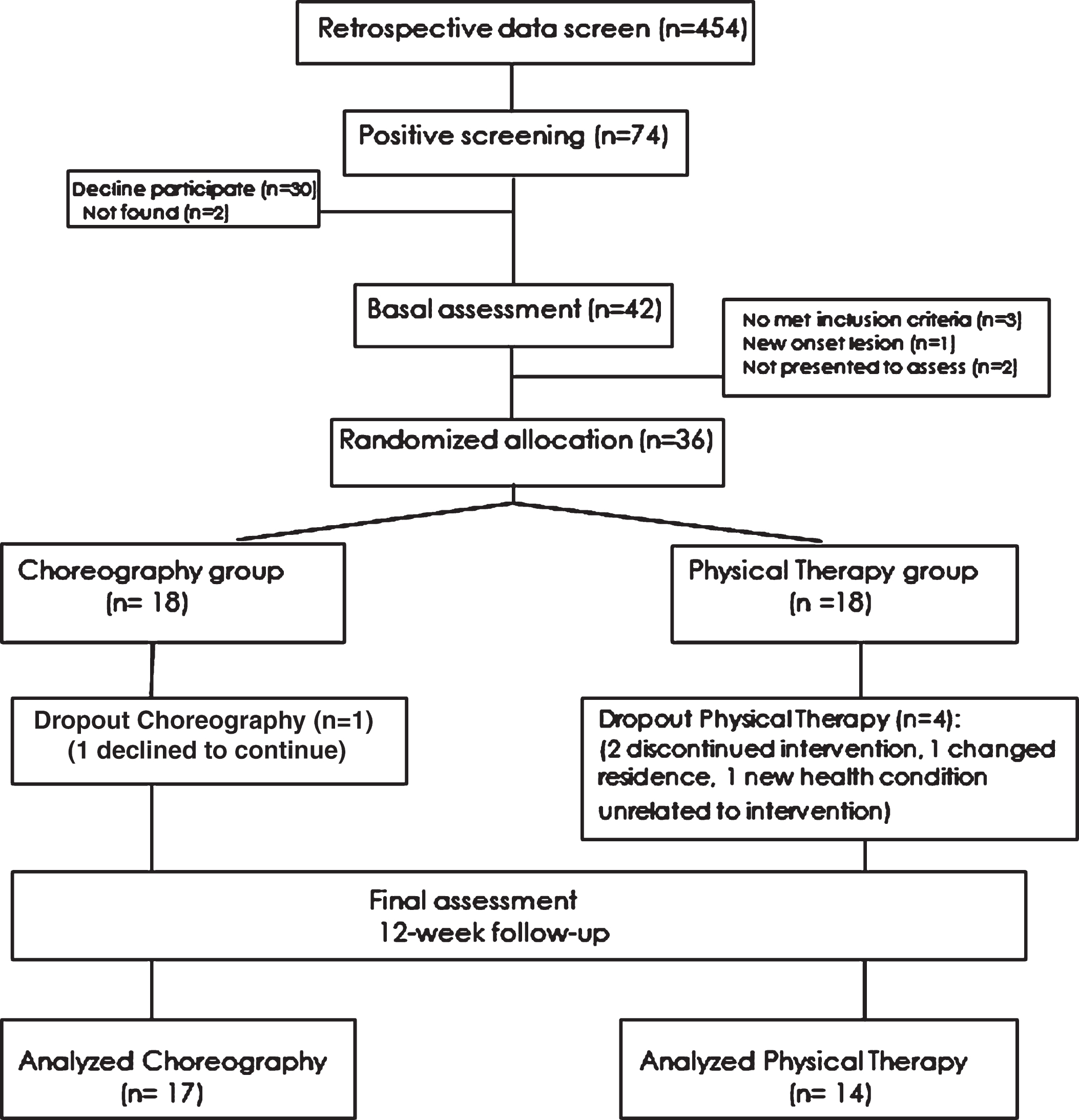
The flow of participants from screening to study completion at 12-week follow-up is detailed in Fig. 1. A total of 31 participants completed the study (17 in the Choreography group and 14 in the Physical Therapy group).
Fig.1
Flow diagram from initial contact to study completion.
Sample characteristics
At baseline, Choreography and Physical Therapy groups were statistically similar in terms of sex, years of formal education, usual physical activity and global cognition (Table 3). However, subjects in the Physical Therapy group were statistically significantly older than those in the Choreography group. In regard to the usual physical activity of participants, the whole sample was moderately sedentary according to the total scores obtained in the Baecke Physical Activity Questionnaire for Elderly Subjects (Table 3).
Table 3
Demographic information at baseline of analyzed participants (n = 31)
| Choreography group (n = 17) | Physiotherapy group (n = 14) | ||||
| Mean | SD | Mean | SD | p-value | |
| Age [y]* | 72.88 | 5.60 | 77.29 | 5.16 | .032* |
| Gender [% ]a | 52.9% male | 50% male | .578 | ||
| Education [y] | 7.88 | 3.79 | 8.64 | 3.92 | .588 |
| MMSE [points] | 27.24 | 1.92 | 27.36 | 2.09 | .867 |
| Baecke [points] | 15.78 | 8.00 | 10.70 | 5.91 | .058 |
SD, standard deviation; aGender Chi-square; MMSE, Mini-Mental State Examination; Baecke Physical Activity Questionnaire for Elderly Subjects; *p < 0.05 statistical significance; y, years.
In regard to attendance, training sessions achieved a high global attendance in both groups (Choreography group: 95.1%; Physical Therapy group: 94.9%) and the total dropout rate was of 13%. In the Physical Therapy group, two participants were withdrawn for discontinued intervention attendance due to medical factors (double cataract surgery and cold complications); one for change of residence and one for a health condition unrelated to the intervention (ankle sprain in the street). In the Choreography group, one participant declined to continue for personal reasons. Those participants who were withdrawn or not completed the study were excluded from the attendance rate and were treated as dropout percentage. Dropout rate in the Physical Therapy group (22%) was higher than in the Choreography group (5%).
Neuropsychological changes
Table 4 shows changes in cognitive performances over the intervention period. First, the between-group comparison showed at 12-week follow-up a main effect. The Choreography group obtained statistically significant greater benefits in verbal recognition memory from the WMS-III than the Physical Therapy group (mean diff. 95% CI: 1.03 [0.15, 1.91]; p = 0.003**) (Table 4, Fig. 2). Besides, CFV showed a statistically significant main effect in the Physical Therapy group (mean diff. 95% CI: 0.29 [0.11, 1.23]; p = 0.013*) (Table 4).
Table 4
Comparison of neuropsychological and physical changes between the two study groups, adjusted by age
| Outcome by group | Summary at different time point mean (SD) | From baseline to 12-week follow-up | At 12-week follow-up | |||
| Baseline | 12-week | Diff. within-group change (95% CI) | p | Diff. between-group change (95% CI) | p | |
| VERBAL MEMORY | ||||||
| Delayed Recall WMS-III | ||||||
| Choreo | 2.24 (2.01) | 2.76 (2.04) | 0.53(–0.15, 1.21) | 0.120 | 0.32 (–0.15, 0.79) | 0.291 |
| Physio | 1.86 (1.46) | 1.93 (1.64) | 0.07(–0.63, 0.77) | 0.828 | ||
| Recognition WMS-III | ||||||
| Choreo | 17.18 (3.00) | 19.24 (2.61) | 2.06 (0.79, 3.32)** | 0.003 ** | 1.03 (0.15, 1.91) ** | 0.003 ** |
| Physio | 18.36 (2.85) | 18.14 (2.77) | –0.21 (–1.18, 0.75) | 0.640 | ||
| VISUAL MEMORY | ||||||
| Delayed Recall RBANS | ||||||
| Choreo | 5.65 (5.36) | 7.94 (4.54) | 2.29 (0.38, 4.21) ** | 0.022* | 1.97 (–0.81, 3.13) | 0.462 |
| Physio | 5.86 (5.17) | 7.43 (5.05) | 1.57 (0.18, 2.96)* | 0.030* | ||
| Recognition RBANS | ||||||
| Choreo | 6.29 (2.75) | 6.12 (1.65) | –0.18 (–1.49, 1.14) | 0.779 | –0.35 (–1.24, 0.53) | 0.864 |
| Physio | 6.71 (2.13) | 6.14 (2.28) | –0.57(–1.89, 0.74) | 0.365 | ||
| SPEED PROCESSING | ||||||
| TMT-A (seconds) | ||||||
| Choreo | 71.35 (28.99) | 76.29 (42.07) | 4.94(–8.73, 18.62) | 0.455 | –3.48(–15.89,8.92) | 0.188 |
| Physio | 94.36 (69.02) | 80.64 (38.07) | –13.71(–36.55, 9.12) | 0.217 | ||
| EXECUTIVE FUNCTIONS | ||||||
| TMT-B (seconds) | ||||||
| Choreo | 239.12 (118.15) | 223. 47 (98.57) | –15.65(–50.07, 18.78) | 0.350 | –23.87 (–47.81, 0.07) | 0.597 |
| Physio | 264.36 (165.27) | 230.50 (137.40) | –33.86 (–70.88,3.17) | 0.070 | ||
| LVF | ||||||
| Choreo | 9.65 (5.70) | 10.18 (5.91) | 0.53 (–1.36, 2.42) | 0.561 | –0.03 (–1.29, 1.23) | 0.372 |
| Physio | 10.07 (4.27) | 9.36 (5.34) | –0.71 (–2.50, 1.08) | 0.404 | ||
| LANGUAGE | ||||||
| BNT | ||||||
| Choreo | 45.47 (6.28) | 45.71 (6.58) | 0.24 (–0.75, 1.22) | 0.620 | –0.03 (–0.88, 0.81) | 0.735 |
| Physio | 43.93 (5.36) | 43.57 (5.96) | –0.36 (–1.94, 1.22) | 0.633 | ||
| CVF | ||||||
| Choreo | 14.24 (4.60) | 13.41 (4.66) | –0.82 (–2.71, 1.06) | 0.367 | 0.29 (0.11, 1.23)* | 0.013* |
| Physio | 11.86 (3.26) | 13.50 (2.85) | 1.64 (–0.08, 3.36) | 0.059 | ||
| VISUOSPATIAL | ||||||
| JLO (total) | ||||||
| Choreo | 17.76 (5.75) | 16.88 (6.92) | –0.88 (–3.38, 1.62) | 0.465 | 0.10 (–1.57, 1.77) | 0.178 |
| Physio | 16.00 (5.31) | 17.38 (5.87) | 1.38 (–0.86, 3.63) | 0.203 | ||
| GLOBAL COGNITION | ||||||
| MMSE | ||||||
| Choreo | 27.24 (1.92) | 27.47 (2.15) | 0.24 (–0.83, 1.30) | 0.647 | 0.23 (–0.39, 0.84) | 0.896 |
| Physio | 27.36 (2.10) | 27.57 (2.03) | 0.21 (–0.43, 0.86) | 0.487 | ||
| EMOTIONAL STATUS | ||||||
| HADS-anxiety | ||||||
| Choreo | 8.65 (4.18) | 8.82 (3.25) | 0.18 (–1.25, 1.60) | 0.796 | –0.16 (–1.19, 0.87) | 0.384 |
| Physio | 6.00 (4.13) | 5.43 ((2.98) | –0.57 (–2.25, 1.10) | 0.474 | ||
| HADS-depression | ||||||
| Choreo | 6.59 (3.00) | 6.00 (3.43) | 0.59 (–1.72, 0.55) | 0.289 | –0.61 (–1.58, 0.36) | 0.623 |
| Physio | 6.00 (3.06) | 5.36 (3.50) | –0.64 (–2.48, 1.19) | 0.462 | ||
| QoL | ||||||
| SF-36 (total score) | ||||||
| Choreo | 102.59 (5.47) | 99.76 (6.77) | –2.82 (–6.12, 0.47) | 0.088 | –0.39 (–3.31, 2.53) | 0.109 |
| Physio | 99.71 (8.91) | 102.29 (4.41) | 2.57 (–2.54, 7.68) | 0.297 | ||
| PHYSICAL FUNCTIONING | ||||||
| BBS | ||||||
| Choreo | 52.94 (2.82) | 53.94 (1.92) | 1.00 (–0.11 2.11,) | 0.073 | 1.58 (–0.50, 2.66) | 0.506 |
| Physio | 50.36 (4.55) | 52.64 (2.13) | 2.29 (0.17, 4.40)* | 0.036* | ||
| TUG | ||||||
| Choreo | 9.04 (1.56) | 8.15 (1.37) | –0.89 (–1.64, –0.14)* | 0.022* | –1.26 (–1.82, 0.71) | 0.210 |
| Physio | 10.72 (2.82) | 9.01 (1.75) | –1.71 (–0.85, –2.58)* | 0.001 ** | ||
Diff., Difference, CI, confidence interval; SD, standard deviation Choreo: choreography; Physio: physical therapy; WMS-III, Wechsler Memory Scale Third Edition; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; TMT-A/B, Trail Making Test A/B; LVF, Letter Verbal Fluency; BNT, Boston Naming Test; CVF, Category Verbal Fluency; JLO, Judgment of Line Orientation; MMSE, Mini-Mental State Examination; HADS, Hospital Anxiety and Depression Scale; QoL, Quality of Life; 36-SF, 36 items Short Form; BBS, Berg Balance Scale; TUG, Timed Up and Go Test; *p < 0.05; **p < 0.01.
Fig.2
Verbal recognition memory from WMS-III: Interaction between time and group factors.
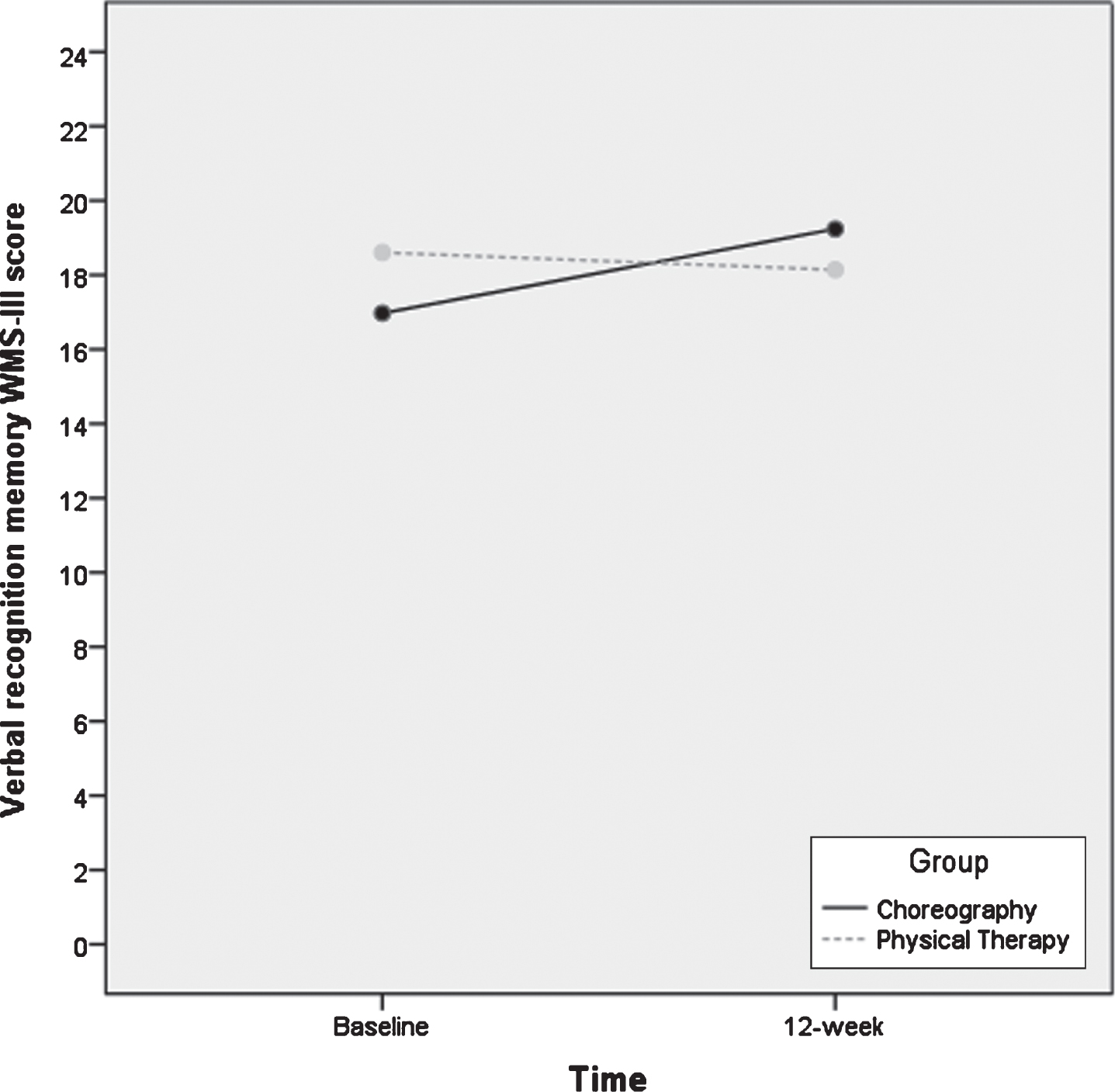
Second, the within-group comparison (from baseline to 12-week, in each group independently), showed a statistically significant improvement in the verbal recognition memory from WMS-III in the Choreography group (mean diff. 95% CI: 2.06 [0.79, 3.32]; p = 0.003**). Both groups showed better significant performance in visual delayed recall from RBANS (Choreography: mean diff. 95% CI: 2.29 [0.38, 4.21-] p = 0.022*; Physical Therapy: mean diff. 95% CI 1.57 [0.18, 2.96]; p = 0.030*) (Table 4).
Moreover, no statistically significant worsening of any neuropsychological variable was found.
Physical functioning changes
For physical functioning parameters, the within-group comparison showed significant main effects in both groups in TUG (Choreography: mean diff 95% CI: –0.89 [–1.64, –0.14]; p = 0.022*; Physical Therapy: mean diff. 95% CI: –1.71 [–0.85, –2.58]; p = 0.001**). With regard to balance, only participants in the Physical Therapy group exhibited significant better performance in the BBS (mean diff. 95% CI: –2.29 (–4.40, –0.17]; p = 0.036*) (Table 4).
DISCUSSION
This study contributes to increase the available evidence on the effects of physical exercise in early stages of cognitive decline in elderly individuals, when there is a high risk of conversion to dementia. At 12 weeks, we compared the cognitive effects of a motor learning intervention, based on dancing choreographies versus a conventional multimodal physical therapy program, in older adults with aMCI. The Choreography intervention required constant learning of new step sequences, one each week. In contrast, the multimodal physical therapy program focused mainly on the repetition of motor exercises, training a variety of motor-skills (including balance and coordination among others) with monthly increases in difficulty.
In regard to neuropsychological changes, our main finding was that the Choreography intervention, requiring motor-skill learning, produced greater benefits in verbal recognition memory than did the Physical Therapy group. Consistent with studies supporting the involvement of the hippocampus in spatial navigation [79], spatial memory [80], and motor sequence consolidation [81], choreographed sessions could enhance recognition memory arguably due to its spatial and memory requirements. The constant learning of choreographed steps presumably demands more spatial functioning memory than a physical training based on the repetition of exercises. Given that memory loss and spatial disorientation are among the first early behavioral manifestations of neurodegeneration in dementia [23], our findings suggest that choreographed learning could promote its maintenance.
Likewise, recognition memory discrimination has been found to be strongly related to the entorhinal cortex, one of the first areas affected in AD [82]. Poor verbal recognition memory reflects a deficit in memory storage and familiarity-based memory, and it is, in turn, related to an increased risk of conversion to dementia in MCI individuals [83–86]. Moreover, in early AD stages, better verbal recognition memory performances have been found to be related to better performances on executive function tests [87], suggesting a close relationship between executive functioning and the ability to recognize information that has been previously presented. Recognition verbal memory provides relevant information about early stages of AD and its assessment has not been included in many studies about physical activity. If choreography training facilitates superior recognition of verbal information, new rehabilitation strategies may want to target this specific cognitive domain, so as to promote better retrieval of learned information.
Our second main finding was the significant improvement in the delayed recall visual memory (RBANS) in both groups after the within-group analysis. This result could be conceived encouraging because in a longitudinal study with aMCI, lower performance on the RBANS visual memory subtest was found not only to be associated with an increased risk of conversion to dementia, but also, with a faster conversion [83]. Better performances on RBANS visual recall were found related to increased brain perfusion in dorsolateral prefrontal and visual associative areas, confirming the overlap between memory pathways and AD pathogenesis [83]. Delayed recall visual memory, assessed by the RBANS figure subtest, has demonstrated to be a useful predictor for the early detection of clinical dysfunction underlying AD [83]. Consequently, an improvement in visual memory in aMCI individuals could possibly delay conversion to dementia.
Other beneficial effect was detected in our study. The multimodal Physical Therapy program significantly improved performance on CVF. It is known that CVF involves search of the semantic network and it significantly worsens in aMCI and mild AD dementia [88–90]. The improvement found in CVF in the Physical Therapy group could be due to language tasks performed during some motor exercises. The multimodal physical program applied included dual-task training. Participants in the Physical Therapy group were asked to evoke some nouns during exercises (i.e., to name cities while walking) or walk with a fit-ball between hands. In daily life, balance or gait act most of the time in dual or multitasking contexts, for this reason we included this type of tasks during the performance of balance or gait exercises. Suzuki et al. (2013) also included dual-task training in their multicomponent exercise program applied in older adults with MCI. Participants were asked to walk while inventing their own poem. Although their results do not provide direct evidence for the positive effect of dual-task training, they believe that dual-task may have a greater effect on various cognitive functions than interventions that only focused on aerobic exercise. We also believe that the CVF improvement could be dependent to the dual-task training included in the multimodal physical therapy program. However, this finding should be confirmed by future research.
The main findings on cognition of the present study confirm the need for an exhaustive neuropsychological assessment including visual and verbal memory tests, in order to detect early cognitive changes in MCI. With regard to the other cognitive functions analyzed, cognitive scores did not materially decline in either intervention group. That is to say, by the end of the study, both groups remained cognitively stable or improved slightly.
With regard to changes in physical functioning, the Choreography and Physical Therapy groups enhanced their functional mobility baseline status, as per TUG measurements, revealing that participants were able to transfer from a seated to a standing position and walk a 3-meter distance faster by the end of the study. In spite of improvements having been observed for both groups, only the Physical Therapy group achieved a decrease in TUG times of more than 1 second. Our results are in accordance with the latest meta-analysis, published by Lam et al. [40] about the effectiveness of exercise in improving physical functions in MCI. People with various levels of cognitive impairments can benefit from supervised multimodal exercise, showing a significant reduction (1-s decrease) of the time required to complete the TUG test [91].
Moreover, it is well known that exercise produces benefits in balance in people with MCI [91]. This is relevant, since the risk of falling is assumed to be higher in MCI than in non-MCI subjects [92]. Regarding the balance examination, it is important to bear in mind that the BBS is a specific static balance assessment tool. In the present study, the Physical Therapy group improved performance on BBS, possibly due to the fact that this group was more specifically trained on static balance, compared to the Choreography group where balance was trained in a dynamic way. The results obtained are very encouraging, since older adults with aMCI have an increased risk of falls and mobility decline [93] which, in turn, may interfere with the functionality of their daily living and negatively impact their cognitive capacities. Functional restrictions behave as a decisive marker of global progressive decline and can appear as soon as 10 years ahead of the clinical diagnosis of dementia [94]. In addition, since balance has been linked to the hippocampus and its connections [27], balance training could become a tool to holistically treat early stages of cognitive decline by using a physical approach easily accessible to physiotherapists aiming to promote and prevent disability.
This study has some noteworthy features: it is replicable, it compares individuals with similar levels of physical activity and takes into account factors to facilitate adherence to therapies for clinical application. Our study has been rigorously standardized and protocolled. The twelve video tutorials for the choreographies are readily available, and so are the multimodal programs practiced by the Physical Therapy group. This allows other researchers to replicate this investigation in the future, if desired. The study assessed the participants’ baseline physical activity (by means of the Baecke Questionnaire) in order to know if our sample was sedentary, moderately sedentary, or active. Our participants’ scores indicated that they were moderately sedentary. For us, it was a requirement to assess the baseline activity level before starting any physical training, as to not obtain exaggerated outcomes if an excessively sedentary sample was chosen. Very few published papers reported data on participants’ usual level of physical activity. Researchers frequently compare physically active experimental groups with sedentary controls [33, 37], which in our opinion sets the project up with a strong bias.
How exactly adherence to treatment influences outcomes remains uncertain. The type of exercise adopted, the individuals’ cognitive ability, their level of physical functioning and the involvement of the family/caregiver [91] may play a role in attendance rates. However, for the present study, we took into account factors which increase adherence, by designing motivating activities, assessing the physical level of functioning to ensure that participants attended the intervention center and involving families to facilitate attendance.
Following is a list of the limitations we were able to establish. Firstly, we lack a non-interventional control group to compare our data. This was, nonetheless, done purposefully; our aim was to compare active treatment groups in which participants could perform some type of physical exercise under the same methodology and conditions, instead of comparing to sedentary control groups that could magnify the outcomes. For those reasons, we assessed baseline accustomed physical activity and created the same intervention environment for each group. Secondly, the selection of eligibility criteria, individuals who accepted to participate, and possibly the unknown group differences may affect the external validity of our findings. Thirdly, the sample size was not as large as we would have hoped for, although it did meet sample size calculation criteria. Fourthly, the dropout exceeded the expected dropout rate by 3% and it was higher in Physical Therapy group than in Choreography one. However, the abandonment factors were neither due to the intervention nor the type of intervention. Fifthly, results should be interpreted with caution due to the election of verbal recognition memory as the main variable of the study, so the inference of secondary outcomes was not controlled for multiple testing. Moreover, the fact that it was a single-center study means that conclusions are not transferrable to all subjects with aMCI.
Despite its limitations, this study constitutes a first step, which will enable researchers to further investigate and study larger samples, to potentially confirm our findings. It is also important to note that our study had the advantage that all of the participants were prospectively enrolled in the same center, that all variables were collected at baseline and follow up, that only a small number of subjects discontinued the study and, finally, that the interventions presented had been systematically created (the twelve choreographic videos and the physical therapy program are available). This should immensely aid our team or others to replicate the protocol. Further longitudinal studies will be needed to determine whether Choreography or Physiotherapy may delay the conversion from MCI to dementia.
Conclusion
Our study provides evidence about how different ways of exercising enhance neuropsychological and physical functions. Neuropsychological outcomes suggest that while a motor learning intervention with choreography sessions improves verbal recognition memory, a multimodal physical therapy program which included dual-task training improves CVF. Both groups also improve in visual delayed recall. The observed cognitive findings are remarkable because they occur in those functions most related to the risk of conversion to dementia and in the most vulnerable population to develop dementia, the aMCI individuals. Moreover, choreography and physical therapy lead to improved balance and gait performances, two essential motor abilities for the maintenance of ADL in late adulthood. If we accept that the acquisition of new motor skills leads to increased functionality, then it would be reasonable to consider that it also affects cognition positively. Further longitudinal studies are needed to determine whether the effects observed by our team are indeed associated with prevention or delayed onset of AD in older adults with aMCI.
ACKNOWLEDGMENTS
The authors thank all participants and their families for their contribution, without which this work would have not been possible. We are extremely grateful to Fundació ACE: Mercè Boada, MD & PhD Chief Medical Officer and Lluís Tárraga, Chief Executive Officer who were determinant in turning the project into a reality; Montserrat Girabent, PhD and Sergi Valero, PhD Head of Clinical Psychology Research for their statistical counselling; Amèrica Morera, Subirector of Day Care Centers, Anna Gailhajanet, Coordinator of the Day Hospital and their team (Vicki Alentorn, Carmen Fernández, Eva Huillca, Joan Carles Ribes and Berta Rodríguez) for helping us during the interventions; to Marta Molins, Blanquerna Research fellow, for helping with the neuropsychological assessment.
The present study has been performed as part of the doctor of philosophy program of Marta Bisbe’s, at Ramon Llull University, Barcelona (Spain).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0552r3).
REFERENCES
[1] | Oltra-Cucarella J , Ferrer-Cascales R , Alegret M , Gasparini R , Díaz-Ortiz LM , Ríos R , Martínez-Nogueras ÁL , Onandia I , Pérez-Vicente JA , Cabello-Rodríguez L , Sánchez-Sansegundo M ((2018) ) Risk of progression to Alzheimer’s disease for different neuropsychological mild cognitive impairment subtypes: A hierarchical meta-analysis of longitudinal studies. Psychol Aging 33: , 1007–1021. |
[2] | Espinosa A , Alegret M , Valero S , Vinyes-Junqué G , Hernández I , Mauleón A , Rosende-Roca M , Ruiz A , López O , Tárraga L , Boada M ((2013) ) A longitudinal follow-up of 550 mild cognitive impairment patients: Evidence for large conversion to dementia rates and detection of major risk factors involved. J Alzheimers Dis 34: , 769–780. |
[3] | Tabert M , Manly J , Liu X , Pelton G , Rosenblum S , Jacobs M , Zamora D , Goodking M , Bell K , Stern Y , Devanand D ((2006) ) Neuropsychological prediction of conversion to alzheimer disease in patients with mild cognitive impairment. Arch Gen Psychiatry 63: , 916–924. |
[4] | Sperling RA , Aisen PS , Beckett LA , Bennett DA , Craft S , Fagan AM , Iwatsubo T , Jack CRJ , Kaye J , Montine TJ , Park DC , Reiman EM , Rowe CC , Siemers E , Stern Y , Yaffe K , Carrillo MC , Thies B , Morrison-Bogorad M , Wagster M V , Phelps CH ((2011) ) Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 280–292. |
[5] | World Health Organization ((2015) ) First WHO Ministerial Conference on Global Action Against Dementia. In Call for action WHO, Geneva. |
[6] | World Health Organization ((2019) ) Risk reduction of cognitive decline and dementia: WHO guidelines, WHO, Geneva. |
[7] | Cai Y , Abrahamson K ((2016) ) How exercise influences cognitive performance when mild cognitive impairment exists: A literature review. J Psychosoc Nurs Ment Health Serv 54: , 25–35. |
[8] | Sofi F , Valecchi D , Bacci D , Abbate R , Gensini GF , Casini A , Macchi C ((2011) ) Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J Intern Med 269: , 107–117. |
[9] | Cai Y , Abrahamson K ((2015) ) Does exercise impact cognitive performance in community-dwelling older adults with mild cognitive impairment? A systematic review. Qual Prim Care 23: , 214–222. |
[10] | Haradaa CN , Natelson Lovec MC , Triebel K ((2013) ) Normal cognitive aging. Clin Geriatr Med 29: , 737–752. |
[11] | Abbott RD , White LR , Ross GW , Masaki KH , Curb JD , Petrovitch H ((2004) ) Walking and dementia in physically capable elderly men. J Am Med Assoc 292: , 1447–1453. |
[12] | Hamer M , Chida Y ((2009) ) Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol Med 39: , 3–11. |
[13] | Blondell SJ , Hammersley-Mather R , Veerman JL ((2014) ) Does physical activity prevent cognitive decline and dementia?: A systematic review and meta-analysis of longitudinal studies. BMC Public Health 14: , 510. |
[14] | Guure CB , Ibrahim NA , Adam MB , Said SM ((2017) ) Impact of physical activity on cognitive decline, dementia, and its subtypes: Meta-analysis of prospective studies. BioMed Res Int 2017: , 9016924. |
[15] | Etgen T , Sander D , Bickel H , Förstl H ((2011) ) Mild cognitive impairment and dementia. Dtsch Arztebl Int 108: , 743–750. |
[16] | Draganski B , Gaser C , Busch V , Schuierer G , Bogdahn U , May A ((2004) ) Changes in grey matter induced by training. Nature 427: , 311–312. |
[17] | Taubert M , Draganski B , Anwander A , Muller K , Horstmann A , Villringer A , Ragert P ((2010) ) Dynamic properties of human brain structure: Learning-related changes in cortical areas and associated fiber Connections. J Neurosci 30: , 11670–11677. |
[18] | Boyke J , Driemeyer J , Gaser C , Buchel C , May A ((2008) ) Training-induced brain structure changes in the elderly. J Neurosci 28: , 7031–7035. |
[19] | Foster PP , Rosenblatt KP , Kuljiš RO ((2011) ) Exercise-induced cognitive plasticity, implications for mild cognitive impairment and Alzheimer’s disease. Front Neurol 28: , 1–15. |
[20] | Kempermann G , Fabel K , Ehninger D , Babu H , Leal-Galicia P , Garthe A , Wolf SA ((2010) ) Why and how physical activity promotes experience-induced brain plasticity. Front Neurosci 4: , 1–9. |
[21] | Cotman CW , Berchtold NC , Christie LA ((2007) ) Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci 30: , 464–472. |
[22] | de Assis GG , de Almondes KM ((2017) ) Exercise-dependent BDNF as a modulatory factor for the executive processing of individuals in course of cognitive decline. A systematic review. Front Psychol 8: , 584. |
[23] | Braak H , Braak E , Bohl J ((1993) ) Staging of Alzheimer-related cortical destruction. Eur Neurol 33: , 403–408. |
[24] | Tward DJ , Sicat CS , Brown T , Bakker A , Gallagher M , Albert M , Miller M ((2017) ) Entorhinal and transentorhinal atrophy in mild cognitive impairment using longitudinal diffeomorphometry. Alzheimers Dement 9: , 41–50. |
[25] | Kattenstroth JC , Kalisch T , Holt S , Tegenthoff M , Dinse HR ((2013) ) Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front Aging Neurosci 5: , 1–16. |
[26] | Coubard OA , Duretz S , Lefebvre V , Lapalus P , Ferrufino L ((2011) ) Practice of contemporary dance improves cognitive flexibility in aging. Front Aging Neurosci 3: , 1–12. |
[27] | Hufner K , Binetti C , Hamilton DA , Stephan T , Flanagin VL , Linn J , Labudda K , Markowitsch H , Glasauer S , Jahn K , Strupp M , Brandt T ((2011) ) Structural and functional plasticity of the hippocampal formation in professional dancers and slackliners. Hippocampus 21: , 855–865. |
[28] | Alpert PT , Miller SK , Wallmann H , Havey R , Cross C , Chevalia T , Gillis CB , Kodandapari K ((2009) ) The effect of modified jazz dance on balance, cognition, and mood in older adults. J Am Acad Nurse Pract 21: , 108–115. |
[29] | Verghese J ((2006) ) Cognitive and mobility profile of older social dancers. J Am Geriatr Soc 54: , I241–I244. |
[30] | Müller P , Rehfeld K , Schmicker M , Hökelmann A , Dordevic M , Lessmann V , Brigadski T , Kaufmann J , Müller NG ((2017) ) Evolution of neuroplasticity in response to physical activity in old age: The case for dancing. Front Aging Neurosci 9: , 1–8. |
[31] | Rehfeld K , Müller P , Aye N , Schmicker M , Dordevic M , Kaufmann J , Hökelmann A , Müller NG ((2017) ) Dancing or fitness sport? The effects of two training programs on hippocampal plasticity and balance abilities in healthy seniors. Front Hum Neurosci 11: , 1–9. |
[32] | Zhu Y , Wu H , Qi M , Wang S , Zhang Q , Zhou L , Wang S , Wang W , Wu T , Xiao M , Yang S , Chen H , Zhang L , Zhang KC , Ma J , Wang T ((2018) ) Effects of a specially designed aerobic dance routine on mild cognitive impairment. Clin Interv Aging 13: , 1691–1700. |
[33] | SuzukiT, ShimadaH, MakizakoH, DoiT, YoshidaD, ItoK, ShimokataH, WashimiY, EndoH, KatoT ((2013) ) A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS One 8: , e61483. |
[34] | Paillard T ((2015) ) Preventive effects of regular physical exercise against cognitive decline and the risk of dementia with age advancement. Sports Med Open 1: , 16–21. |
[35] | Nagamatsu L , Handy T , Hsu CL , Voss M , Chan A , Davis JC , Beattie BL , Graf P , Liu-Ambrose T ((2012) ) Resistance training promotes cognitive functions and functional plasticity in senior women with probable mild cognitive impairment: A six-month randomized controlled trial. Alzheimers Dement 8: , P522–P523. |
[36] | Baker LD , Frank LL , Foster-Schubert K , Green PS , Wilkinson CW , McTiernan A , Plymate SR , Fishel MA , Watson GS , Cholerton BA , Duncan GE , Mehta PD , Craft S ((2010) ) Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch Neurol 67: , 71–79. |
[37] | Lautenschlager NT , Cox KL , Flicker L , Foster JK , van Bockxmeer FM , Xiao J , Greenop KR , Almeida OP ((2008) ) Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 300: , 1027–1037. |
[38] | Lam LC , Chau RC , Wong BM , Fung AW , Tam CW , Leung GT , Kwok TC , Leung TY , Ng SP , Chan WM ((2012) ) A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 13: , 568.e15–568.e20. |
[39] | van Uffelen JGZ , Chinapaw MJM , Hopman-Rock M , van Mechelen W ((2009) ) Feasibility and effectiveness of a walking program for community-dwelling older adults with mild cognitive impairment. J Aging Phys Act 17: , 398–415. |
[40] | Lam L , Chau R , Wong B , Fung A , Lui V , Tam C , Leung G , Kwok T , Hiu H , Ng S , Chan W ((2011) ) Interim follow-up of a randomized controlled trial comparing Chinese style mind body (Tai Chi) and stretching exercises on cognitive function in subjects at risk of progressive cognitive decline. Int J Geriatr Psychiatry 26: , 733–740. |
[41] | Liu-Ambrose T , Donaldson MG , Ahamed Y , Graf P , Cook WL , Close J , Lord SR , Khan KM ((2008) ) Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J Am Geriatr Soc 56: , 1821–1830. |
[42] | Chan A , Tetzlaff JM , Altman DG , Laupacis A , Gøtzsche PC , Krleža-jeric K , Hrobjartsson A , Mann H , Dickersin K , Berlin JA , Dore CJ , Parulekar WR , Summerskill WSM , Groves T , Schulz KF , Sox HC , Rockhold FW , Rennie D , Moher D ((2015) ) Declaración SPIRIT 2013: Definición de los elementos estándares del protocolo de un ensayo clínico*. Rev Panam Salud Publica 38: , 506–514. |
[43] | Moher D , Hopewell S , Schulz KF , Montori V , Gøtzsche PC , Devereaux PJ , Elbourne D , Egger M , Altman DG ((2010) ) CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 340: , c869. |
[44] | World Medical Association ((2013) ) World medical association declaration of helsinki ethical principles for medical research involving human subjects. JAMA 310: , 2191–2194. |
[45] | Alegret M , Espinosa A , Vinyes-Junqué G , Valero S , Hernández I , Tárraga L , Becker JT ((2012) ) Normative data of a brief neuropsychological battery for Spanish individuals older than 49. J Clin Exp Neuropsychol 34: , 209–219. |
[46] | Boada M , Tárraga L , Hernández I , Valero S , Alegret M , Ruiz A , Lopez OL , Becker JT ((2014) ) Design of a comprehensive Alzheimer’s disease clinic and research center in Spain to meet critical patient and family needs. Alzheimers Dement 10: , 409–415. |
[47] | Petersen RC ((2004) ) Mild cognitive impairment as a diagnostic entity. J Intern Med 256: , 183–194. |
[48] | Folstein MF , Folstein SE , McHugh PR ((1975) ) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[49] | Blesa R , Pujol M , Aguilar M , Santacruz P , Bertran-Serra I , Hernandez G , Sol JM , Pena-Casanova J ((2001) ) Clinical validity of the “mini-mental state” for Spanish speaking communities. Neuropsychologia 39: , 1150–1157. |
[50] | Blessed G , Tomlinson BE , Roth M ((1968) ) The association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects. Br J Psychiatry 114: , 797–811. |
[51] | Pena-Casanova J , Aguilar M , Bertran-Serra I , Santacruz P , Hernandez G , Insa R , Pujol A , Sol JM , Blesa R ((1997) ) Normalization of cognitive and functional assessment instruments for dementia (NORMACODEM) (I): Objectives, content and population. Neurologia 12: , 61–68. |
[52] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[53] | Berg KO , Wood-Dauphinee SL , Williams JI , Maki B ((1992) ) Measuring balance in the elderly: Validation of an instrument. Can J Public Health 83: Suppl 2, S7–11. |
[54] | Podsiadlo D , Richardson S ((1991) ) The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39: , 142–148. |
[55] | Borg GA ((1982) ) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14: , 377–381. |
[56] | American College of Sports Medicine ((2013) ) Guidelines for exercise testing and prescrption, Lippincott Williams & Wilkins, Philadelphia. |
[57] | Ainsworth BE , Haskell WL , Herrmann SD , Meckes N , Bassett DR Jr , Tudor-Locke C , Greer JL , Vezina J , Whitt-Glover MC , Leon AS ((2011) ) 2011 Compendium of Physical Activities: A second update of codes and MET values. Med Sci Sports Exerc 43: , 1575–1581. |
[58] | Weschler D ((1997) ) Wechsler Adult Intelligence Test-3rd Edition, The Psychological Corporation, San Antonio, Texas. |
[59] | Randolph C ((1998) ) Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), Pearson, Chicago. |
[60] | Muntal Encinas S , Gramunt-Fombuena N , Badenes Guia D , Casas Hernanz L , Aguilar Barbera M ((2012) ) Traducción y adaptación española de la batería neuropsicológica Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) forma A en una muestra piloto. Neurologia 27: , 531–546. |
[61] | Reitan RM ((1992) ) Trail Making Test: Manual for administration and scoring, Neuropsychology Laboratory, Tucson, Arizona. |
[62] | Tamayo F , Casals-Coll M , Sanchez-Benavides G , Quintana M , Manero RM , Rognoni T , Calvo L , Palomo R , Aranciva F , Pena-Casanova J ((2012) ) Spanish normative studies in a young adult population (NEURONORMA young adults Project): Norms for the verbal span, visuospatial span, Letter-Number Sequencing, Trail Making Test and Symbol Digit Modalities Test. Neurologia 27: , 319–329. |
[63] | Artiola L , Hermosillo D , Heaton R , Pardee R ((1999) ) Manual de normas y procedimientos para la batería neuropsicológica en español. M Press, Tucson, AZ. |
[64] | Goodglass H , Kaplan E ((1983) ) The assessment of aphasia and related disorders, Lea & Febiger, Philadelphia, PA. |
[65] | Abraham M , Valentina RD , Gauchat S , Marino JC ((2008) ) Valores normativos de la prueba de fluidez de acción (nombramiento de verbos). Rev Neuropsicol Neuropsiquiatr Neuroci 8: , 11–19. |
[66] | Casals-Coll M , Sanchez-Benavides G , Quintana M , Manero RM , Rognoni T , Calvo L , Palomo R , Aranciva F , Tamayo F , Pena-Casanova J ((2013) ) Spanish normative studies in young adults (NEURONORMA young adults project): Norms for verbal fluency tests. Neurologia 28: , 33–40. |
[67] | Kaplan EF , Goodglass H , Weintraub S ((1978) ) The Boston Naming Test, Lea & Febiger, Philadelphia. |
[68] | Peña-Casanova J , Quiñones-Úbeda S , Gramunt-Fombuena N , Aguilar M , Casas L , Molinuevo JL , Robles A , Rodríguez D , Barquero MS , Antúnez C , Martínez-Parra C , Frank-García A , Fernández M , Molano A , Alfonso V , Sol JM , Blesa R ((2009) ) Spanish multicenter normative studies (NEURONORMA project): Norms for boston naming test and token test. Arch Clin Neuropsychol 24: , 343–354. |
[69] | Benton A , Varney N , Hamsher K ((1978) ) Visuospatial judgment: A clinical test. Arch Neurol 35: , 364–367. |
[70] | Calvo L , Casals-Coll M , Sanchez-Benavides G , Quintana M , Manero RM , Rognoni T , Palomo R , Aranciva F , Tamayo F , Pena-Casanova J ((2013) ) Spanish normative studies in young adults (NEURONORMA young adults project): Norms for the Visual Object and Space Perception Battery and Judgment of Line Orientation tests. Neurologia 28: , 153–159. |
[71] | Zigmond AS , Snaith RP ((1983) ) The hospital anxiety and depression scale. Acta Psychiatr Scand 67: , 361–370. |
[72] | De las Cuevas Castresana C , Garcia-Estrada Perez A , Gonzalez de Rivera JL ((1995) ) “Hospital anxiety and depression scale” y psicopatología afectiva. Anales Psiquiatr 11: , 126–130. |
[73] | Jenkinson C , Coulter A , Wright L ((1993) ) Short form 36 (SF36) health survey questionnaire: Normative data for adults of working age. BMJ 306: , 1437–1440. |
[74] | Alonso J , Prieto L , Anto JM ((1995) ) The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med Clin 104: , 771–776. |
[75] | Baecke JA , Burema J , Frijters JE ((1982) ) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36: , 936–942. |
[76] | Vilaro J , Gimeno E , Sanchez Ferez N , Hernando C , Diaz I , Ferrerc M , Roca J , Alonso J ((2007) ) Daily living activity in chronic obstructive pulmonary disease: Validation of the Spanish version and comparative analysis of 2 questionnaires. Med Clin 129: , 326–332. |
[77] | Alegret M , Espinosa A , Valero S , Vinyes-Junque G , Ruiz A , Hernandez I , Rosende-Roca M , Mauleon A , Becker JT , Tarraga L , Boada M ((2013) ) Cut-off scores of a brief neuropsychological battery (NBACE) for Spanish individual adults older than 44 years old. PloS One 8: , e76436. |
[78] | Curran-Everett D , Benos DJ ((2007) ) Guidelines for reporting statistics in journals published by the American Physiological Society: The sequel. Adv Physiol Educ 31: , 295–298. |
[79] | O’Keefe J ((1990) ) A computational theory of the hippocampal cognitive map. Prog Brain Res 83: , 301–312. |
[80] | Bannerman DM , Rawlins JNP , McHugh SB , Deacon RMJ , Yee BK , Bast T , Zhang W-N , Pothuizen HHJ , Feldon J ((2004) ) Regional dissociations within the hippocampus-memory and anxiety. Neurosci Biobehav Rev 28: , 273–283. |
[81] | Albouy G , Sterpenich V , Balteau E , Vandewalle G , Desseilles M , Dang-Vu T , Darsaud A , Ruby P , Luppi PH , Degueldre C , Peigneux P , Luxen A , Maquet P ((2008) ) Both the hippocampus and striatum are involved in consolidation of motor sequence memory. Neuron 58: , 261–272. |
[82] | Wolk DA , Dickerson BC ((2011) ) Fractionating verbal episodic memory in Alzheimer’s disease. Neuroimage 54: , 1530–1539. |
[83] | Alegret M , Cuberas-Borrós G , Espinosa A , Valero S , Hernández I , Ruíz A , Becker JT , Rosende-Roca M , Mauleón A , Sotolongo O , Castell-Conesa J , Roca I , Tárraga L , Boada M ((2014) ) Cognitive, genetic, and brain perfusion factors associated with four year incidence of Alzheimer’s disease from mild cognitive impairment. J Alzheimers Dis 41: , 739–748. |
[84] | Rabin LA , Pare N , Saykin AJ , Brown MJ , Wishart HA , Flashman LA , Santulli RB ((2009) ) Differential memory test sensitivity for diagnosing amnestic mild cognitive impairment and predicting conversion to Alzheimer’s disease. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 16: , 357–376. |
[85] | Braaten AJ , Parsons TD , McCue R , Sellers A , Burns WJ ((2006) ) Neurocognitive differential diagnosis of dementing diseases: Alzheimer’s dementia, vascular dementia, frontotemporal dementia, and major depressive disorder. Int J Neurosci 116: , 1271–1293. |
[86] | Golden Z , Bouvier M , Selden J , Mattis K , Todd M , Golden C ((2005) ) Differential performance of Alzheimer’s and vascular dementia patients on a brief battery of neuropsychological tests. Int J Neurosci 115: , 1569–1577. |
[87] | Gleichgerrcht E , Torralva T , Martinez D , Roca M ((2011) ) Impact of executive dysfunction on verbal memory performance in patients with Alzheimer’s disease. J Alzheimers Dis 23: , 79–85. |
[88] | Rinehardt E , Eichstaedt K , Schinka JA , Loewenstein DA , Mattingly M , Fils J , Duara R , Schoenberg MR ((2014) ) Verbal fluency patterns in mild cognitive impairment and Alzheimer’s disease. Dement Geriatr Cogn Disord 38: , 1–9. |
[89] | Teng E , Leone-Friedman J , Lee GJ , Stephanie W , Apostolova LG , Harrell S , Ringman JM , Lu PH ((2013) ) Similar verbal fluency patterns in amnestic mild cognitive impairment and alzheimer’s disease. Arch Clin Neuropsychol 28: , 400–410. |
[90] | Alegret M , Vinyes-Junqué G , Boada M , Martínez-Lage P , Cuberas G , Espinosa A , Roca I , Hernández I , Valero S , Rosende-Roca M , Mauleón A , Becker And JT , Tárraga L ((2010) ) Brain perfusion correlates of visuoperceptual deficits in mild cognitive impairment and mild Alzheimer’s disease. J Alzheimers Dis 21: , 557–567. |
[91] | Lam , Huang M , Liao L , Chung R , Kwok T , Pang M ((2018) ) Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: A systematic review and meta-analysis. J Physiother 64: , 4–15. |
[92] | Shin BM , Han SJ , Jung JH , Kim JE , Fregni F ((2011) ) Effect of mild cognitive impairment on balance. J Neurol Sci 305: , 121–125. |
[93] | Davis JC , Best J , Hsu CL , Nagamatsu LS , Dao E , Liu-Ambrose T ((2015) ) Examining the effect of the relationship between falls and mild cognitive impairment on mobility and executive functions in community-dwelling older adults. J Am Geriatr Soc 63: , 590–593. |
[94] | Peres K , Helmer C , Amieva H , Orgogozo J-M , Rouch I , Dartigues J-F , Barberger-Gateau P ((2008) ) Natural history of decline in instrumental activities of daily living performance over the 10 years preceding the clinical diagnosis of dementia: A prospective population-based study. J Am Geriatr Soc 56: , 37–44. |


