
The Effectiveness of a Community Nurse-Led Support Program for Dementia Caregivers in Chinese Communities: The Chongqing Ageing and Dementia Study
Abstract
Background:
As the primary caregivers for people with dementia in China, family caregivers face a significant care burden that can negatively impact their mental and physical health. It is vital to investigate ways to support these caregivers.
Objective:
To assess the effectiveness of a program led by community nurses to support caregivers of individuals with dementia.
Methods:
A total of 30 caregivers received nurse-led support in addition to usual care, while 28 caregivers received only usual care. The primary outcome was caregivers’ sense of competency in providing dementia care, which was measured using the Short Sense of Competence Questionnaire (SSCQ). Secondary outcomes included caregivers’ ability to perform daily activities, behavioral and psychological symptoms of dementia (BPSD) using a neuropsychiatric inventory questionnaire, and quality of life using the short form health survey (SF-36). The trial was registered at the Chinese Clinical Trial Registry (ChiCTR 2300071484).
Results:
Compared to the control group, the intervention group had significantly higher SSCQ scores and a lower caregiver distress index over time. Physical and mental health-related quality of life also improved significantly among caregivers in the intervention group. However, there was no significant difference between the two groups in terms of activities of daily living and BPSD.
Conclusions:
The community nurse-led support program significantly improved caregivers’ competency in providing dementia care and quality of life and reduced distress. These findings have important implications for dementia care policies, resources, and workforce development in China, including strengthening community dementia care services through collaboration with specialists in hospitals.
INTRODUCTION
Dementia is a condition that causes gradual cognitive decline and hinders an individual’s ability to function and perform daily activities. Almost all people with dementia experience behavioral and psychological symptoms of dementia (BPSD) [1, 2]. There are approximately 50 million people worldwide with dementia and 15.07 million in China alone [3, 4]. Hospitals and some mental health centers can provide only short-term treatment-based services, and high-quality nursing homes are expensive. Therefore, family members are the primary source of caregiving for people with dementia in China [5]. It has been reported that over 96% of individuals with dementia in China are cared for at home by family members or domestic helpers outside of the families [6].
Family caregivers face great challenges in caregiving. The daily activities of people with dementia rely on assistance from their family caregivers, and most caregivers do not have the necessary knowledge and skills to provide the care needed. Progressive cognitive impairments, BPSD, uncertain prognosis, never-ending caregiving responsibilities, and sacrifices of their career and social relationships can all contribute to the heavy burden on caregivers and lead to compromised mental and physical health [5], with studies showing that 15.5% of caregivers in Hong Kong experience burnout [7]. Family caregivers have high rates of anxiety, depression, and stress, and approximately 32.32% of them experience suicidal ideation [8, 9]. Research has shown that higher levels of social support can help reduce the burden on caregivers of people with dementia [10]. However, there is a gap between the needs of caregivers and the limited services provided by communities in China, highlighting the urgent need to explore how to support family caregivers of people with dementia [5].
We developed a 1-year program led by community nurses to provide support for caregivers of people with dementia. We investigated how this program would affect caregivers in terms of feeling competent, experiencing less distress, and improving their physical and mental health-related quality of life. Furthermore, as the self-care capability and BPSD of care recipients are the main factors that cause distress among caregivers [11, 12], we also examined how the abilities of daily living (ADL) and BPSD of care recipients impacted caregivers’ levels of stress and burden. Our goal is to find a way to improve the quality of life for family caregivers, decrease the burden on society caused by dementia, and promote the health and well-being of individuals with dementia.
MATERIALS AND METHODS
Study design
This was a prospective, quasi-experimental trial conducted between June 2017 and August 2018 in community health centers in Chongqing, China. The study complied with the Declaration of Helsinki and was approved by the Human Ethics Committee of our hospital (TAHTMMU, No. 201503) in December 2014 and registered in the Chinese Clinical Trial Registry (ChiCTR2300071484). Informed consent was obtained from each participant.
Participants and allocation
Eligible caregivers were Chinese residents who met the following criteria: 1) the main caregivers of people with dementia; 2) aged 18 years or above; 3) caring for someone diagnosed with dementia; 4) living in Chongqing during the study period; and 5) willing to participate in this study. The exclusion criteria were as follows: 1) suffering from illness that hindered clinical trial execution; 2) lack of communication ability (such as hearing impairment); and 3) having previously participated in dementia education and training.
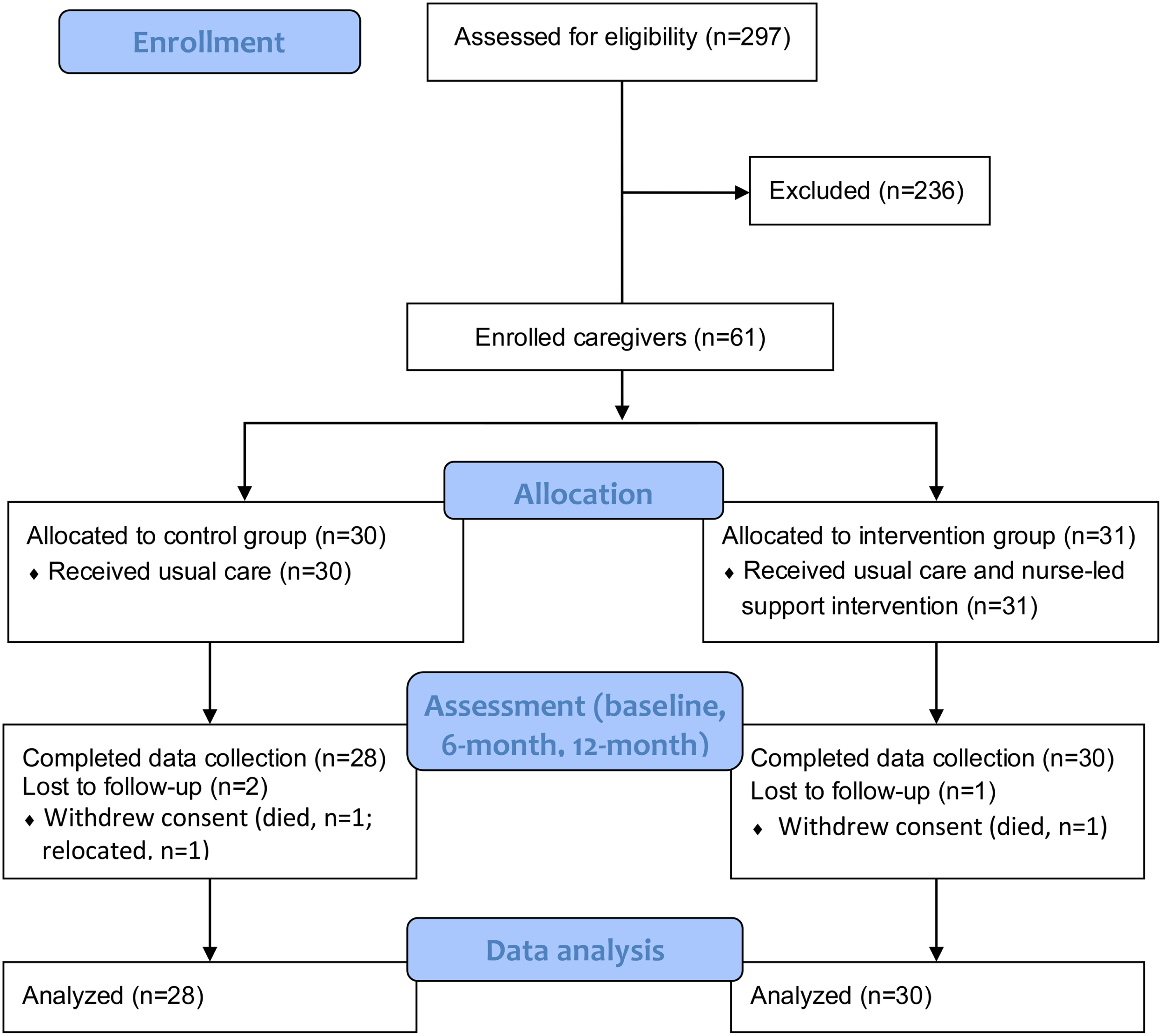
As caregivers usually held their own opinions on whether to accept the nurse-led support intervention, the caregivers were allocated based on their willingness. Figure 1 shows a flow diagram of participant enrolment.
Fig. 1
Flow diagram.
Sample size estimation
The sample size was estimated by PASS 15 (NCSS, USA) software. According to a previous study, the standard deviation of the Short Sense of Competence Questionnaire (SSCQ) (primary outcome) was 4.5 [13]. Assuming a maximum allowable error rate of 20%, a sample size of 29 in each group was required to achieve a significance level of p < 0.05 (2-tailed test) and a power (1-β) of 0.8 with a 20% dropout rate.
Usual care
All participants received the usual care provided by community health centers. As there was no specific policy about community health care for people with dementia and their caregivers, the community health workers provided services according to the policy of the National Health Commission of China and the family physician model. Community health care workers were responsible for building personal health records and providing health education and management for chronic diseases (such as cardiovascular disease, dementia, and diabetes), communicable diseases (such as tuberculosis) and other diseases. The physical examination was organized each year, and caregivers and people with dementia could go to the community health center or consult their family physician for help when they needed. Community health care workers also provided family visits for physical examination and nursing, such as examinations of blood pressure level and heart rate, taking blood specimen for laboratory test based on physician’s order, and communications about lifestyle and health status.
Nurse-led support intervention
In addition to the usual care, caregivers in the intervention group received a support program. Bandura’s self-efficacy theory was applied to the development of the support program [14]. Caregivers’ self-efficacy is dominated by their confidence in coping effectively with different types of care [15]. Bandura’s theory states that an individual’s functioning is the product of the dynamically reciprocal interplay of personal factors, behavior, and environmental influences and that learning and supportive interactions with others are the basis of an individual’s self-efficacy [16, 17]. Because nurses play a vital role in supportive care, we developed a nurse-led support program based on Bandura’s theory, the literature and China’s actual conditions [18, 19]. The support program consisted of two phases.
Phase 1: Training of community nurses. Before beginning the research, the involved community health workers received a training program developed according to the literature review and the needs of the community health workers [20, 21]. The community health workers received information about the overall design of the support program. The training program and the project information equipped them with sufficient knowledge and skills about dementia care and caregiver support and allowed them to complete the forms and scales in the study. The contents of the training consisted of the following components: 1) the purpose and method of this study, 2) basic knowledge of dementia, 3) the concept of “people-centered care”, 4) care skills for dementia, 5) available support resources, 6) nutritional assessment and support for people with dementia, 7) psychological intervention and self-adjustment strategies, and 8) use of forms and scales in this study. The training methods included knowledge lectures, operation guidance and case analysis.
During the trial, three registered nurses provided intervention for caregivers, two community doctors afforded medical support when necessary, and one community manager was responsible for supervising the intervention. To ensure that community nurses could obtain sufficient and timely support, a community support team and WeChat communication group were set up, which consisted of professionals from the neurology department, nutrition department, psychology department, geriatrics department, pharmacy department, clinical nursing experts, and community doctors.
Phase 2: Support intervention for caregivers. The period for the support intervention was 12 months. The intervention was conducted in three stages based on the Life Model of Social Work Practice [22]: the initiation phase included the establishment of a relationship, collection of information, and execution of the contract; the execution phase included developing job adaptation skills and assisting in building positive relationships in social networks; and the closing phase consisted of an evaluation of the effectiveness of the support and closure of the case. The content of the intervention was as follows.
1) In company with community managers, the community nurses informed the caregivers of the content and methods of the study, evaluated caregivers’ needs via a questionnaire that was based on the experiences of community health workers and researchers and previous studies [23] (Supplementary Table 1), and developed personalized care plans based on their needs.
2) At the first visit (approximately 2 h), community nurses provided one-on-one support for dementia care and communication skills, available support resources, psychological self-adjustment skills, the prevention of dementia-related complications (including falls, malnutrition, urinary tract infection and pneumonia, and pressure ulcers), and drug management and safety management methods. They also provided materials, such as a brochure on “knowledge and essentials about how to care for people with dementia”. The brochure presented the common symptoms, risk factors and treatments for dementia and useful skills for caring for people with dementia, including how to deal with their BPSD. Then, home visits were conducted to provide support and monitor the effects [21]. Specifically, community nurses provided a family guidance visit for 30–40 min once a month and telephone support once a week for 15–20 min to learn about the difficulties encountered by caregivers and to further provide guidance about dementia care and psychological self-adjustment skills.
3) Lectures and experience exchange meetings for caregivers were held each quarter. The contents of the lectures included basic knowledge of dementia, nutritional support, and functional training methods for people with dementia as well as psychological self-adjustment strategies of caregivers.
4) Community nurses instructed caregivers to establish a “family caregiver diary” to record the BPSD of people with dementia and care difficulties [13], which facilitated the caregivers’ communication with nurses over the phone or during family visits. In addition, at the 6-month and 12-month follow-ups, the researchers temporarily collected these “family caregiver diaries” to summarize existing problems and provide personalized caregiving support based on these problems.
Measurements
General characteristics. The sociodemographic data of the caregivers (age, sex, and educational level) and care recipients (age, sex, educational level, dementia severity, and dementia duration), years of care, days of care per week, hours of care per day, cohabitation time, economic affordability, and number of assistants were collected in the intervention and control groups at baseline.
Primary outcome. The primary outcome was the SSCQ score [24], which was evaluated among caregivers in both groups at baseline and 6 months and 12 months after enrolment. The SSCQ consists of 7 items, each of which is rated on a 5-point Likert scale (1 for “strongly agree” and 5 for “strongly disagree”). A higher score indicates that caregivers have a better sense of competency in caring for people with dementia.
Secondary outcomes. Activities of daily living (ADL), the Neuropsychiatric Inventory Questionnaire (NPI-Q), and quality of life (SF-36) were evaluated at baseline, 6 months, and 12 months after enrollment. The contents of these outcomes were as follows.
1) ADL includes a physical self-maintenance scale and instrumental activities of daily living scale, which was used to evaluate the ability of daily living of people with dementia [25]. It consists of 20 items, and a higher score indicates worse self-care ability.
2) The NPI-Q includes 12 items for evaluating BPSD symptoms in people with dementia (NPI-S) and caregiver distress (NPI-D) [26]. For the NPI-S, the severity of symptoms (3-point Likert scale) and their frequency (4-point Likert scale) were multiplied for the total score. A higher score indicated more severe BPSD symptoms of people with dementia. For the NPI-D (6-point Likert scale), a higher score indicated that the caregiver was more distressed about the BPSD symptoms.
3) The SF-36 is a generic instrument for measuring quality of life in healthy persons and in patients with different diseases as individuals with good mental and physical health generally experience a higher overall quality of life [27, 28]. The SF-36 is composed of 36 items related to physical health (physical functioning, role-physical, bodily pain, and general health) and mental health (vitality, social functional, role-emotional, mental health) to reflect the quality of life, with a higher score indicating better quality of life [29].
Others. A service satisfaction questionnaire was applied to investigate the degree of satisfaction of caregivers in the intervention group when the support intervention was finished (12-month follow-up).
Validity and reliability
1) The 3 community nurses received unified training for the scales to ensure consistency before the beginning of the study. Kendall’s W test was used to evaluate the interobserver agreement of the SSCQ (Kendall W value of 0.633), ADL (Kendall’s W value of 0.929), NPI-S (Kendall’s W value of 0.819), NPI-D (Kendall’s W value of 0.864), and SF-36 (Kendall’s W value of 1.000) based on the results of the 3 community nurses by evaluating 5 caregivers independently.
2) The scales were completed by caregivers one on one with community nurses, who subsequently checked the data after completion to prevent the omission of items.
3) Data collection and statistical analysis were completed by 2 independent researchers who were blind to the grouping of the participants.
4) One community manager was responsible for coordinating and supervising the support intervention.
Statistical analysis
The statistical analysis was conducted with SPSS software (version 22.0, IBM Corp, USA). Qualitative data are described as frequencies and percentages and were analyzed by Pearson’s chi-squared test. Non-normally distributed continuous data are described by the median and interquartile range, and normally distributed continuous data are described by the mean with standard deviation and were analyzed by the Mann–Whitney U test and Student’s t test, respectively. A linear mixed model was applied to analyze the relationship between groups over time (baseline, 6 months, 12 months) and was fitted with group and time as fixed effects. A p value < 0.05 was considered statistically significant.
RESULTS
General characteristics
During the 12-month study period, 297 caregivers were screened for eligibility and 61 were enrolled, with 31 in the intervention group and 30 in the control group. Three participants withdrew consent because 2 care recipients died and 1 moved to another city and changed caregivers (Fig. 1).
As shown in Table 1, all baseline characteristics between both groups of caregivers and care recipients were comparable, except that the number of assistants (p < 0.05) was greater and physical (p < 0.05) and mental health (p < 0.001) were worse in the intervention group, suggesting that a high care burden and worse living quality made the caregivers choose to receive support intervention.
Table 1
Characteristics of the caregivers and care recipients in the intervention and control groups at baseline
| Characteristics | Intervention (n = 30) | Control (n = 28) | p |
| Caregivers | |||
| Age, y, median (IQR) | 59.0 (55.8–63.3) | 67.0 (48.0–68.0) | 0.14b |
| Sex, female, n (%) | 26 (86.7) | 21 (67.7) | 0.08a |
| Educational level, n (%) | 0.86a | ||
| Primary school or less | 7 (23.3) | 6 (21.4) | |
| Junior high school or above | 23 (76.7) | 22 (78.6) | |
| Years of care, median (IQR) | 5.0 (2.8–6.3) | 3.0 (2.0–6.0) | 0.08b |
| Days of care/week, median (IQR) | 7.0 (7.0–7.0) | 7.0 (7.0–7.0) | > 0.99b |
| Hours of care/day, median (IQR) | 9.0 (6.0–12.0) | 8.0 (6.0–10.0) | 0.25b |
| Cohabitation time, y, median (IQR) | 35.0 (18.8–46.3) | 36.5 (26.5–51.4) | 0.56b |
| Economic affordability, n (%) | 19 (63.3) | 22 (78.6) | 0.20a |
| Number of assistants, n (%) | 10 (33.3) | 18 (64.3) | 0.02a |
| SSCQ, median (IQR) | 19.0 (15.8–22.0) | 19.5 (17.3–23.8) | 0.25b |
| Caregiver distress index (NPI-D), median (IQR) | 15.0 (8.0–30.0) | 9.5 (5.0–19.5) | 0.09b |
| Physical health (SF-36), median (IQR) | 59.0 (55.2–61.0) | 61.5 (58.7–65.8) | 0.03b |
| Mental health (SF-36), median (IQR) | 36.5 (30.8–43.0) | 50.5 (43.5–53.8) | < 0.001b |
| Care recipient | |||
| Age, y, median (IQR) | 82.0 (77.8–86.0) | 84.0 (74.5–87.8) | 0.48b |
| Sex, female, n (%) | 21 (70.0) | 14 (50.0) | 0.12a |
| Educational level, n (%) | 0.81a | ||
| Primary school or less | 17 (56.7) | 15 (53.6) | |
| Junior high school or above | 13 (43.3) | 13 (46.4) | |
| Dementia severity, n (%) | 0.98a | ||
| Mild | 18 (60.0) | 16 (57.2) | |
| Moderate | 8 (26.7) | 9 (32.1) | |
| Severe | 4 (13.3) | 3 (10.7) | |
| Dementia duration, month, median (IQR) | 51.0 (35.0–111.8) | 44.5 (29.0–87.8) | 0.39b |
| ADL, median (IQR) | 15.0 (13.0–21.0) | 17.0 (12.3–18.8) | 0.83b |
| BPSD severity of people with dementia (NPI-S), median (IQR) | 15.0 (8.0–30.0) | 9.5 (5.0–19.5) | 0.06b |
aPearson’s chi-squared test; bMann–Whitney U test. ADL, activities of daily life; BPSD, behavioral and psychological symptoms of dementia; IQR, interquartile range; NPI, neuropsychiatric inventory; SSCQ, short sense of competence questionnaire.
Support needs of caregivers
The support needs of caregivers in the intervention group were surveyed before the intervention. Among a total of 31 caregivers, 28 participated in the survey and had a strong need for caregiving support (Supplementary Table 1). All caregivers expected to receive guidance about relieving stress and depressive symptoms due to the care of people with dementia, and 92.9% and 96.4% of caregivers wondered how to exercise and relax and to relieve pressure, respectively. Approximately 89.3% of the caregivers needed skills to care for BPSD symptoms of people with dementia, and 82.1% and 71.4% of caregivers desired information about available support and how to contact nursing support services, respectively. Furthermore, 71.4% of caregivers expected methods of hiring temporary caregivers. The personalized care plan was developed based on their answers.
Three caregivers refused to be surveyed because they did not believe the intervention could improve their quality of life due to the social environment. Thus, their personalized care plans were determined by problems identified by community nurses through communication and observation.
Primary and secondary outcomes
Compared with the control group, there was a significant difference in the SSCQ score (p < 0.05) and caregiver distress index (NPI-D) (p < 0.05) over time between the intervention and control groups. Caregivers in the intervention group had a better sense of competence and a lower degree of distress (Table 2).
Table 2
Primary and secondary outcome analyses at each follow-up visit
| Characteristic, | Baseline, | 6-month, | 12-month, | p | ||
| group | mean (SD) | mean (SD) | mean (SD) | Within groups | Between groups | Interaction |
| SSCQ | 0.02 | 0.04 | 0.001 | |||
| Intervention | 18.9 (4.4) | 19.8 (4.1) | 19.0 (4.1) | |||
| Control | 20.8 (5.2) | 20.0 (5.3) | 17.7 (5.2) | |||
| ADL | 0.07 | 0.38 | 0.004 | |||
| Intervention | 15.8 (5.4) | 16.1 (5.9) | 16.0 (5.1) | |||
| Control | 15.2 (5.9) | 16.7 (5.7) | 17.6 (5.7) | |||
| Physical health (SF-36) | 0.004 | 0.01 | <0.001 | |||
| Intervention | 58.2 (5.5) | 60.3 (6.3) | 59.7 (6.5) | |||
| Control | 61.0 (5.9) | 58.2 (5.4) | 56.5 (6.0) | |||
| Mental health (SF-36) | < 0.001 | < 0.001 | < 0.001 | |||
| Intervention | 37.8 (9.8) | 41.1 (9.8) | 41.3 (10.3) | |||
| Control | 49.0 (6.3) | 37.7 (7.3) | 34.7 (8.4) | |||
| BPSD severity of people with dementia (NPI-S) | 0.22 | 0.290 | 0.74 | |||
| Intervention | 19.4 (14.8) | 19.9 (16.5) | 25.6 (17.7) | |||
| Control | 12.5 (9.5) | 19.8 (10.9) | 23.5 (12.7) | |||
| Caregiver distress index (NPI-D) | 0.56 | 0.04 | 0.09 | |||
| Intervention | 5.5 (5.5) | 4.4 (3.9) | 6.7 (5.2) | |||
| Control | 3.2 (3.0) | 3.6 (3.6) | 6.8 (4.3) | |||
Intervention group, n = 30; control group, n = 28. ADL, activities of daily life; BPSD, behavioral and psychological symptoms of dementia; NPI, neuropsychiatric inventory; SD, standard deviation; SSCQ, short sense of competence questionnaire.
Although the physical health and mental health evaluated by the SF-36 were worse in caregivers of the intervention group at baseline, after the 12-month nurse-led support intervention, physical health (p < 0.01) and mental health (p < 0.001) were both significantly improved among caregivers in the intervention group compared to the control group (Table 2). Specifically, bodily pain (p < 0.05) for “physical health” and vitality (p < 0.001), social functioning (p < 0.001), and mental health (p < 0.001) for “mental health” were significantly better in caregivers in the intervention group over time than in the control group (Table 3).
Table 3
Subdimensions of the SF-36 at each follow-up visit
| Characteristic, | Baseline, | 6-month, | 12-month, | p | ||
| group | mean (SD) | mean (SD) | mean (SD) | Within | Between | Interaction |
| groups | groups | |||||
| Physical functioning | 0.10 | 0.85 | 0.46 | |||
| Intervention | 27.5 (2.0) | 27.6 (2.1) | 27.3 (2.5) | |||
| Control | 27.2 (3.3) | 27.1 (3.0) | 26.6 (3.2) | |||
| Role-physical | 0.53 | 0.08 | 0.01 | |||
| Intervention | 4.8 (1.5) | 5.8 (2.0) | 5.5 (2.0) | |||
| Control | 5.4 (1.7) | 5.1 (1.7) | 4.6 (1.2) | |||
| Bodily pain | 0.04 | 0.02 | 0.02 | |||
| Intervention | 10.8 (1.9) | 10.7 (1.9) | 10.8 (1.9) | |||
| Control | 11.4 (1.0) | 10.7 (1.8) | 10.3 (1.9) | |||
| General health | < 0.001 | 0.92 | 0.28 | |||
| Intervention | 17.1 (2.6) | 16.1 (2.5) | 15.9 (2.2) | |||
| Control | 17.0 (2.2) | 15.3 (1.3) | 15.0 (2.0) | |||
| Vitality | < 0.001 | < 0.001 | < 0.001 | |||
| Intervention | 11.5 (3.5) | 13.3 (3.5) | 12.7 (3.2) | |||
| Control | 15.9 (2.1) | 11.9 (2.3) | 10.8 (2.9) | |||
| Social functioning | < 0.001 | < 0.001 | < 0.001 | |||
| Intervention | 6.5 (2.1) | 6.8 (2.3) | 6.9 (2.0) | |||
| Control | 8.6 (1.3) | 6.4 (1.5) | 5.9 (1.5) | |||
| Role-emotional | 0.97 | 0.11 | 0.01 | |||
| Intervention | 3.6 (1.1) | 3.8 (1.3) | 4.1 (1.4) | |||
| Control | 3.9 (1.4) | 3.4 (0.9) | 3.3 (0.9) | |||
| Mental health | < 0.001 | < 0.001 | < 0.001 | |||
| Intervention | 16.2 (4.3) | 18.1 (3.9) | 17.3 (4.1) | |||
| Control | 20.8 (3.2) | 19.8 (3.5) | 14.8 (3.8) | |||
Intervention group, n = 30; Control group, n = 28. SD, standard deviation.
There was no significant difference between the intervention group and the control group in the ADL and BPSD severity of people with dementia (NPI-S) after the 12-month support intervention (Table 2).
Degree of satisfaction of caregivers
All caregivers who received the nurse-led support intervention were surveyed at the end of the 12-month intervention for service satisfaction. The data showed that all caregivers were satisfied with the support intervention provided by community nurses, 80% of caregivers considered this community service to be very helpful for them, and 20% thought it was somewhat helpful (Supplementary Table 2).
DISCUSSION
In China, caregivers of people with dementia face great challenges that put them at increased risk of depression and compromised physical health. We developed a 1-year nurse-led support intervention for caregivers of people with dementia and found that the intervention had significant beneficial effects in terms of improving caregivers’ competency and quality of life and relieving the degree of caregiving distress, while it had no effects on ADL or the severity of BPSD in people with dementia.
Strengthening support for caregivers and community health workers
In this study, we found that the sense of competency, degree of caregiver distress, and quality of life (reflected by physical health and mental health) were improved in caregivers who received a 12-month nurse-led support intervention. Learning and supportive interactions with trained community nurses could build self-efficacy in caregivers of people with dementia and improve caregivers’ cognitive, motivational, affective, and behavioral development [17]. Self-efficacy is related to competency and contributes to a better quality of life for caregivers [15, 30, 31]. These results indicate that the nurse-led support program based on Bandura’s self-efficacy theory can improve dementia caregivers’ beliefs about their capability in managing dementia at home and reduce their negative thoughts about their dementia care. In addition, the majority of the care recipients in our study had mild or moderate dementia. Given that the severity of dementia has a clear association with the caregiver burden, quality of life and support needs of caregivers [32–34], we conclude that the community nurse-led support intervention is effective and necessary for caregivers of people with mild and moderate dementia.
However, in comparison with Australia [13], the differences in the competency of caregivers at the 12-month follow-up between the intervention and control groups were smaller in our study; specifically, the improvement in competency was less pronounced than in foreign studies. The possible explanations are as follows: 1) the interventionists in the Australian study were highly experienced professionals, whereas the community nurses in this study had no previous experience in supporting dementia caregivers, and 2) there are many dementia care support facilities and institutions other than caregiving skills training and dementia education in Australia and caregivers can receive multifaceted support in multiple ways, while there is a lack of a well-developed support system in China [35, 36]. This implies that in addition to caregivers, community health workers need sufficient support. It is urgent to strengthen the training of community health workers in caregiver support and establish an effective support system in China.
Emphasizing the development of caregivers’ ability to manage BPSD symptoms in people with dementia
In this study, 89.3% of caregivers in the intervention group were eager to gain knowledge and skills about BPSD symptom management. In addition, we found synchronous changes between the severity of BPSD and the caregiver’s sense of competence, vitality, and mental health as well as caregivers’ distress during the 12-month follow-up. The values of these indices at 6 months were all better than those at 12 months postintervention. These results imply that BPSD is the major source of caregivers’ stress and burden [37, 38]. Thus, the impact of BPSD on caregivers should be emphasized in future caregiver support intervention studies, and managing BPSD and coping with the stress it causes should be the key elements of caregiving support.
Establishing a caregiver support approach according to China’s actual conditions
The BPSD of people with dementia is an important factor that causes a high caregiving burden and psychiatric symptoms in caregivers [39]. This study found that both groups of caregivers had low distress scores for the BPSD symptoms of care recipients, in contrast to studies from other countries. This may be because the spirit of Confucian culture has been advocated in China, and the concepts of filial piety, family harmony, gratitude, and hard work are widely accepted. Thus, caregivers are more likely to accept BPSD symptoms and consider caring to be their duty and obligation. In addition, people in China often keep a wary eye on unfamiliar people and are reluctant to reveal their true feelings for reasons such as fear of discrimination by others. Therefore, support for people with dementia and their caregivers should be developed based on China’s actual conditions. In addition, local community health workers who are familiar with people with dementia and their caregivers are more suitable for identifying care problems and providing support. Caregiver support should be a long-term process that will help community health workers establish closer ties with families of people with dementia.
Optimizing the role of community health workers in post-diagnostic support for people with dementia
In China, the majority of families choose home-based care for people with dementia, and community-based support services are the most accessible source for family caregivers. Notably, community health workers, especially nurses, played crucial roles and were the determinants of the achievements of the support program in our study. They can provide professional support and prevent changes in living environments and high financial expenses. However, there is room for improvement in China. In terms of policy, the role of community health workers in the dementia care support system is unclear, and community health centers lack the service duties and responsibilities to provide support for caregivers. In addition, due to insufficient manpower, lack of skills training and support, inadequate government input and multichannel compensation mechanisms, community health workers lack sufficient motivation and service capability [40–42]. Our study found that systemic training and support for community health workers helped them fulfil their roles in supporting caregivers of people with dementia. Therefore, strengthening the support of community health institutions and workers may be a way to promote the quality of life of home-care people with dementia and their caregivers. Our study can provide a basis and reference for community-based post-diagnostic support for dementia caregivers in China.
Implications for a future support system for caregivers of people with dementia in communities in China
The data from this study revealed that a high care burden and low quality of life motivated caregivers to receive the support intervention, and caregivers in the intervention group expressed demands for almost all of the items in the questionnaire. This finding reflects the strong desire of caregivers to receive support as well as the lack of a support system in communities in China. Currently, many countries are exploring various forms of support systems for people with dementia and their families [43, 44]. In Sweden, people with dementia are managed and cared for according to the severity of dementia. People with severe dementia can live in long-term care centers; people with moderate dementia can choose a day-care center in the daytime and go home at night; and people with mild dementia are mainly cared for by family caregivers. In Japan, the “New Orange Plan” was formulated to promote community-based care systems that integrate secure medical care, long-term care and prevention, housing, and day-to-day support for people with dementia [45]. In America, casualty care research centers and institutions, adult day care services, and online social support platforms are established to provide care services for dementia [46]. In addition, commercial insurance companies develop long-term care insurance to meet long-term care needs.
Nurses who work in UK communities are trained to undertake reception for patients, nursing, health education, and hospice care, and their specialist training is based on competency-based training courses [47]. In the USA, colleges and universities develop curricula with a focus on enhancing health care students’ core competencies, including a scientific foundation, leadership, quality, practice inquiry, technology and information literacy, policy, the health delivery system, ethics and independent practice competencies [47]. These experiences from developed countries along with our findings have implications for dementia care policy and service development. First, it is imperative to establish dementia care support systems for people with dementia and their caregivers to effectively reduce the care burden of caregivers while improving the health and well-being of people with dementia. Second, the government plays a leading role in health and social care systems; thus, government-initiated, funded, and regulated community aged care services, which include dementia care, are needed. Third, community aged care and hospital care resources need to be integrated to establish a “hospital-community-family” management system to reflect that people with dementia need to use both health care and social care. In addition, nurses and general practitioners in community care settings play a vital role in the care of people with dementia and support for their caregivers. Thus, education and training in dementia care need to be developed to meet their professional development needs.
It is worth noting that social and cultural differences can significantly influence dementia training programs designed for nurses. Social and cultural backgrounds, attitudes and beliefs, family involvement and traditional care practices differ between China and other countries. Therefore, incorporating awareness of social and cultural differences in dementia training programs for nurses is crucial for providing culturally competent and person-centered care for people with dementia and their caregivers. The emphasis on culturally appropriate care through dementia education and training for nurses will ensure that care is respectful, inclusive, and tailored to the unique needs and backgrounds of individuals and their families.
Limitations
First, this study was conducted in urban Chongqing, and the nurses who led the support intervention were mainly from one community health center. Large-scale and multicenter studies are needed to further investigate the effectiveness of nurse-led support interventions for caregivers of people with dementia in China. Second, only four scales were applied in the study, which may be inadequate to evaluate the effects of the intervention on caregivers. Third, the study only investigated cooperation between general hospitals and community health centers and did not include other community resources, such as volunteers and elderly institutions, nor did it explore the effects of policies, funding, law, and other factors on the support effects. Fourth, in the intervention group of our study, the personalized care plans were determined by both the personal opinions of caregivers and the problems identified by community nurses for 27 patients with dementia, while for the other three patients, their personalized care plans were determined based on the problems found by community nurses. This may lead to variation in the support plans and cause some bias in the interventional outcomes. Fifth, the caregiving burden, quality of life, and support needs of caregivers vary with different severities of dementia. The majority of the care recipients in our study had mild or moderate dementia, and the conclusions drawn may not apply entirely to patients with severe dementia.
Conclusions
This study showed that a community nurse-led support intervention for dementia caregivers is a feasible and effective way to improve caregivers’ dementia care competencies and quality of life and reduce the distress of caregivers in China. Based on the successful experiences of developed countries and the health care system in China, a government-initiated, community-based, and hospital-cooperative support system for people with dementia and their caregivers is needed to relieve the disease burden on society and families and improve the quality of life of people with dementia and their family caregivers in China.
ACKNOWLEDGMENTS
The authors have no acknowledgements to report.
FUNDING
This work was supported by the National Natural Science Foundation of China (92249305), the Chongqing Social Science Foundation (2015YBSH142) and a grant from Third Military Medical University.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data supporting the findings of this study are available on request from the corresponding authors.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ADR-230067.
REFERENCES
[1] | Gedde MH , Husebo BS , Mannseth J , Naik M , Selbaek G , Vislapuu M , Berge LI ((2022) ) The impact of medication reviews by general practitioners on psychotropic drug use and behavioral and psychological symptoms in home-dwelling people with dementia: Results from the multicomponent cluster randomized controlled [email protected] trial. BMC Med 20: , 186. |
[2] | Cai W , Li L , Sang S , Pan X , Zhong C ((2023) ) Physiological roles of β-amyloid in regulating synaptic function: Implications for AD pathophysiology. Neurosci Bull 39: , 1289–1308. |
[3] | Jia L , Du Y , Chu L , Zhang Z , Li F , Lyu D , Li Y , Li Y , Zhu M , Jiao H , Song Y , Shi Y , Zhang H , Gong M , Wei C , Tang Y , Fang B , Guo D , Wang F , Zhou A , Chu C , Zuo X , Yu Y , Yuan Q , Wang W , Li F , Shi S , Yang H , Zhou C , Liao Z , Lv Y , Li Y , Kan M , Zhao H , Wang S , Yang S , Li H , Liu Z , Wang Q , Qin W , Jia J , Group C ((2020) ) Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet Public Health 5: , e661–e671. |
[4] | Zhang R , Xu X , Yu H , Xu X , Wang M , Le W ((2022) ) Factors influencing Alzheimer’s disease risk: Whether and how they are related to the APOE genotype. Neurosci Bull 38: , 809–819. |
[5] | Liu Z , Sun W , Chen H , Zhuang J , Wu B , Xu H , Li P , Chen X , Li J , Yin Y ((2022) ) Caregiver burden and its associated factors among family caregivers of persons with dementia in Shanghai, China: A cross-sectional study. BMJ Open 12: , e057817. |
[6] | Wang S , Cheung DSK , Leung AYM ((2019) ) Overview of dementia care under the three-tier long-term care system of China. Public Health Nurs 36: , 199–206. |
[7] | Chan CY , Cheung G , Martinez-Ruiz A , Chau PYK , Wang K , Yeoh EK , Wong ELY ((2021) ) Caregiving burnout of community-dwelling people with dementia in Hong Kong and New Zealand: A cross-sectional study. BMC Geriatr 21: , 261. |
[8] | Hosseini L , Sharif Nia H , Ashghali Farahani M ((2021) ) Hardiness in family caregivers during caring from persons with Alzheimer’s disease: A deductive content analysis study. Front Psychiatry 12: , 770717. |
[9] | Solimando L , Fasulo M , Cavallero S , Veronese N , Smith L , Vernuccio L , Bolzetta F , Dominguez LJ , Barbagallo M ((2022) ) Suicide risk in caregivers of people with dementia: A systematic review and meta-analysis. Aging Clin Exp Res 34: , 2255–2260. |
[10] | Nemcikova M , Katreniakova Z , Nagyova I ((2023) ) Social support, positive caregiving experience, and caregiver burden in informal caregivers of older adults with dementia. Front Public Health 11: , 1104250. |
[11] | Albrecht T , Schroeder M , LeCaire T , Endicott S , Marschall K , Felten K , Sayavedra N , Russmann S , Kern V , Blazek MC , Kales HC , Carlsson CM , Mahoney J , Walaszek A ((2022) ) Training dementia care professionals to help caregivers improve the management of behavioral and psychological symptoms of dementia using the DICE Approach: A pilot study. Geriatr Nurs 48: , 74–79. |
[12] | Owokuhaisa J , Kamoga R , Musinguzi P , Muwanguzi M , Natukunda S , Mubangizi V , Asiime K , Rukundo GZ ((2023) ) Burden of care and coping strategies among informal caregivers of people with behavioral and psychological symptoms of dementia in rural south-western Uganda. BMC Geriatr 23: , 475. |
[13] | Xiao LD , De Bellis A , Kyriazopoulos H , Draper B , Ullah S ((2016) ) The effect of a personalized dementia care intervention for caregivers from Australian minority groups. Am J Alzheimers Dis Other Demen 31: , 57–67. |
[14] | Bandura A ((1993) ) Perceived self-efficacy in cognitive development and functioning. Educ Psychol 28: , 117–148. |
[15] | Farina N , Page TE , Daley S , Brown A , Bowling A , Basset T , Livingston G , Knapp M , Murray J , Banerjee S ((2017) ) Factors associated with the quality of life of family carers of people with dementia: A systematic review. Alzheimers Dement 13: , 572–581. |
[16] | Tsang SK , Hui EK , Law BC ((2012) ) Self-efficacy as a positive youth development construct: A conceptual review. ScientificWorldJournal 2012: , 452327. |
[17] | Xiao LD , Wang J , Ratcliffe J , Ullah S , Brodaty H , Brijnath B , Chang HR , Wang H , Chang CC , Kwok T , Zhu M ((2022) ) A nurse-led multicentre randomized controlled trial on effectiveness and cost-effectiveness of Chinese iSupport for dementia program: A study protocol. J Adv Nurs 78: , 1524–1533. |
[18] | Kim HJ , Shim YS , Park KH , Lee CN , Jung S , Yoon SJ , Jeong SK , Jeong JH , Choi SH , Kim EJ , Jang JW , Kang K , Yang Y , Kim S ((2021) ) Impact of an education program for caregivers of patients with Alzheimer’s disease on treatment discontinuation and compliance in Korea. J Clin Neurol 17: , 368–375. |
[19] | Yamakawa M , Kanamori T , Fukahori H , Sakai I ((2022) ) Sustainable nurse-led care for people with dementia including mild cognitive impairment and their family in an ambulatory care setting: A scoping review. Int J Nurs Pract 28: , e13008. |
[20] | Wang Y , Xiao LD , Ullah S , He GP , De Bellis A ((2017) ) Evaluation of a nurse-led dementia education and knowledge translation programme in primary care: A cluster randomized controlled trial. Nurse Educ Today 49: , 1–7. |
[21] | Dreier A , Thyrian JR , Eichler T , Hoffmann W ((2016) ) Qualifications for nurses for the care of patients with dementia and support to their caregivers: A pilot evaluation of the dementia care management curriculum. Nurse Educ Today 36: , 310–317. |
[22] | Gitterman A , Knight C , Germain C ((2021) ) The Life Model of Social Work Practice: Advances in Theory and Practice, 4th edition. Columbia University Press, New York. |
[23] | Xiao LD , Habel L , De Bellis A ((2015) ) Perceived challenges in dementia care by Vietnamese family caregivers and care workers in South Australia. J Cross Cult Gerontol 30: , 333–352. |
[24] | Vernooij-Dassen MJ , Felling AJ , Brummelkamp E , Dauzenberg MG , van den Bos GA , Grol R ((1999) ) Assessment of caregiver’s competence in dealing with the burden of caregiving for a dementia patient: A Short Sense of Competence Questionnaire (SSCQ) suitable for clinical practice. J Am Geriatr Soc 47: , 256–257. |
[25] | Weng Y , Huang J ((2014) ) Reliability and validity of the Chinese version of the Alzheimer’s Disease Rating Scale-Cognitive Component and the Ability to Perform Daily Activities Scale for the evaluation of vascular dementia. Chin J Gerontol 34: , 1751–1753. |
[26] | Ma WF , Tsai GE , Chang JP , Lane HY ((2010) ) Reliability and validity of three Chinese-version tasks of Mayer-Salovey-Caruso Emotional Intelligence Test. J Clin Nurs 19: , 2656–2658. |
[27] | Cardaillac C , Levesque A , Riant T , Mortier A , Neunlist M , Perrouin-Verbe M-A , Volteau C , Thubert T , Brochard C , Ploteau S (2023) Evaluation of a scoring system for the detection of central sensitizat ion among women with chronic pelvic pain. Am J Obstet Gynecol, doi: 10.1016/j.ajog.2023.07.044. |
[28] | Geschke K , Fellgiebel A , Laux N , Schermuly I , Scheurich A ((2013) ) Quality of life in dementia: Impact of cognition and insight on applicability of the SF-36. Am J Geriatr Psychiatry 21: , 646–654. |
[29] | Ware JE Jr., Sherbourne CD ((1992) ) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30: , 473–483. |
[30] | Fortinsky RH , Kercher K , Burant CJ ((2002) ) Measurement and correlates of family caregiver self-efficacy for managing dementia. Aging Ment Health 6: , 153–160. |
[31] | Nogales-González C , Romero-Moreno R , Losada A , Márquez-González M , Zarit SH ((2015) ) Moderating effect of self-efficacy on the relation between behavior problems in persons with dementia and the distress they cause in caregivers. Aging Ment Health 19: , 1022–1030. |
[32] | Wang L , Zhou Y , Fang X , Qu G ((2022) ) Care burden on family caregivers of patients with dementia and affecting factors in China: A systematic review. Front Psychiatry 13: , 1004552. |
[33] | Nasrun MWS , Kusumaningrum P , Redayani P , Lahino HL , Mardhiyah FS , Basfiansa AD , Nadila N ((2021) ) Relationship between quality of life of people with dementia and their caregivers in Indonesia. J Alzheimers Dis 81: , 1311–1320. |
[34] | Contreras M , Mioshi E , Kishita N ((2021) ) What are the educational and support needs of family carers looking after someone in the early stages of Alzheimer’s disease? A qualitative retrospective approach. Health Soc Care Comm 30: , 1726–1734. |
[35] | Su JA , Chang CC ((2020) ) Association between family caregiver burden and affiliate stigma in the families of people with dementia. Int J Environ Res Public Health 17: , 2772. |
[36] | Lin W ((2016) ) Community service contracting for older people in urban China: A case study in Guangdong Province. Aust J Prim Health 22: , 55–62. |
[37] | Pinyopornpanish K , Soontornpun A , Wongpakaran T , Wongpakaran N , Tanprawate S , Pinyopornpanish K , Nadsasarn A , Pinyopornpanish M ((2022) ) Impact of behavioral and psychological symptoms of Alzheimer’s disease on caregiver outcomes. Sci Rep 12: , 14138. |
[38] | Kamoga R , Mubangizi V , Owokuhaisa J , Muwanguzi M , Natakunda S , Rukundo GZ ((2023) ) Behavioral and psychological symptoms of dementia: Prevalence, symptom severity, and caregiver distress in South-Western Uganda-a quantitative cross-sectional study. Int J Environ Res Public Health 20: , 2336. |
[39] | Losada-Baltar A , Kishita N , Jiménez-Gonzalo L , Fernandes-Pires J , Huertas-Domingo C , Contreras M , Van Hout E , Olazarán J , Martínez-Huertas J , Márquez-González M ((2022) ) Cross-cultural analysis of the role of ambivalent feelings for understanding caregivers’ depressive symptoms. Aging Ment Health 27: , 1307–1312. |
[40] | Long H , Huang W , Zheng P , Li J , Tao S , Tang S , Abdullah AS ((2018) ) Barriers and facilitators of engaging community health workers in non-communicable disease (NCD) prevention and control in China: A systematic review (2006-2016). Int J Environ Res Public Health 15: , 2378. |
[41] | Shao S , Wu T , Guo A , Jin G , Chen R , Zhao Y , Du J , Lu X ((2018) ) The training contents, problems and needs of doctors in urban community health service institutions in China. BMC Fam Pract 19: , 182. |
[42] | Li B ((2022) ) Study on the allocation and forecast of health human resources in primary medical institutions in China. China Health Industry 19: , 13–18. |
[43] | Kim G , Jeon H , Park S , Lim Y ((2019) ) Care support system using ontological model of caring patient with dementia. Alzheimers Dement 15: , P1449–P1450. |
[44] | Elliott J , Stolee P , Mairs K , Kothari A , Conklin J ((2023) ) A community of practice on environmental design for long-term care residents with dementia. Can J Aging 42: , 404–425. |
[45] | Kyou Y , Oishi S , Takizawa T , Suzuki R , Nakamura N , Arai H , Miyaoka H ((2020) ) A retrospective study on the diagnosis and treatment of dementia in patients referred to the Sagamihara Municipal Medical Center for Dementia for consultation. Psychogeriatrics 20: , 247–253. |
[46] | Yang YT , Peng L ((2022) ) Insights of the development of hospital-community-home continuum of care for patients with Alzheimer’s disease. J Nurs 29: , 32–37. |
[47] | Yan X , Chen L , Chen Y ((2020) ) Current status and research progress of community-based specialist nurse training. J Nurs 27: , 14–17. |


