
Pilot Randomized, Double-Blind, Placebo-Controlled Crossover Trial Evaluating the Feasibility of an Intranasal Oxytocin in Improving Social Cognition in Individuals Living with Alzheimer’s Disease
Abstract
Background:
Individuals living with Alzheimer’s disease (AD) demonstrate extensive deficits in social cognition. To date, no studies have investigated the feasibility of an intranasal oxytocin (INOT) treatment to improve social cognition in individuals living with AD.
Objective:
We conducted a pilot trial to determine recruitment feasibility, enrolment acceptability, and adherence to an INOT treatment to inform on the subsequent design of a future randomized controlled trial (RCT). We also estimated the effect sizes of potential social cognitive function outcome measures related to participants and their caregivers.
Methods:
Four individuals with AD were enrolled in a single-center, randomized, double-blind, placebo-controlled crossover trial involving a one-week treatment period with both INOT (72 IU twice daily) and placebo.
Results:
All participants reported no treatment-causative or serious adverse events following repeated INOT administration. While enrolment acceptability (100%) and INOT adherence (placebo, 95%; INOT, 98%) were excellent, feasibility of recruitment was not acceptable (i.e., n = 4/58 individuals screened met inclusion criteria). However, positive/large effects were associated with secondary outcomes of self-reported health and wellbeing, caregiver ‘burden’, intimacy and interpersonal-bonding, following repeated INOT administration. No positive effects were associated with participant outcomes of social cognition.
Conclusion:
This pilot RCT provides first evidence that INOT administration in individuals living with AD is safe and well-tolerated. Despite limitations in sample size, moderate-to-large effect size improvements were identified in participant health outcomes as well as core social cognitive functions and ‘burden’ as reported by a caregiver. This suggests potential broad-ranging beneficial effects of INOT which should be assessed in future RCTs.
INTRODUCTION
Dementia is an umbrella term encompassing several syndromes with varying cognitive, behavioral, and functional symptoms that are a result of neurodegeneration. Alzheimer’s disease (AD) is the most commonly diagnosed form of dementia, accounting for an estimated 60 to 80% of all cases worldwide [1]. Within this population, approximately 80% of cases have pathological evidence of vascular dementia (VaD), referring to associated cerebral infarcts or strokes, therefore making this the most common form of mixed dementia [1–4].
A wide body of literature has shown that social cognition is impaired in AD [5–12]. Social cognition (or social cognitive function) refers to the set of cognitive processes involved in recognizing, understanding, and responding to social cues [8, 13]. From the four broad components of social cognition that have been proposed [8], impairments in Theory of Mind (ToM) or the ability to comprehend the emotional/mental state of others, as well as poorer recognition of facial emotions have been most commonly reported in individuals living with AD [5, 7, 10, 11]. Moreover, in AD and VaD, frequently observed neuropsychiatric symptoms, including aggression, apathy, depression, and psychosis, are accompanied by disruptions in the way social cognitive stimuli are perceived, recognized, and evaluated [14]. That is, deficits in global social cognitive function in AD have been associated with an indifference to interpersonal relationships, awkward social behaviors and diminished social functioning [15], poorer marital relationships, and a greater sense of caregiver ‘burden’ [16–19]. Caregiver ‘burden’ is a leading factor contributing to the placement of individuals living with dementia in residential care [20]. Since deficits in social cognitive function are often left untreated, they have the potential to contribute to an individual’s vulnerability and likelihood of being placed in residential care [21].
Studies in neuropsychiatric populations such as schizophrenia and autism spectrum disorder have demonstrated that the neuropeptide-hormone oxytocin (OT) facilitates the processing of socially relevant information [22–24]. In healthy adults, research has demonstrated that intranasal oxytocin (INOT) administration can improve social cognitive skills such as facial affect recognition [25, 26]. These improvements have been observed acutely, as early as 30 min following single-dose INOT administration [27], with studies demonstrating that INOT sustains a biological half-life of 2 h in the body and can be detected in saliva and plasma [28]. In addition, other randomized controlled trials (RCTs) investigating repeated INOT (24-40 IU) administration over two weeks, have reported improvements to overall health and wellbeing, as well as increased reports of ‘social motivation’ [29, 30]. Significant improvement has also been reported in processing of positive [22] and negative emotions [31], enhanced trust [32], and increased empathy [33]. Importantly, all studies investigating INOT administration have demonstrated that it is safe, non-invasive, and associated with replicable changes in social cognitive functioning [29, 34, 35].
To date, only two studies have investigated whether INOT administration can improve social cognitive function in dementia [35, 36]. The first randomized, double-blind, placebo-controlled crossover trial recruited twenty people with frontotemporal dementia (FTD) and investigated the effects of single-dose INOT (24 IU) administration on neuropsychiatric behaviors and emotion processing. While no change in facial emotion recognition was identified, scores on the Neuropsychiatric Inventory (NPI) [37] were significantly improved on the evening following INOT administration. The authors noted that these results warranted an RCT with a longer treatment period and a larger sample size to better understand if INOT administration can improve social cognitive function in dementia.
Consequently, several years later the same group investigated the safety and tolerability of one-week repeated INOT administration at three clinically feasible doses (24, 48, or 72 IU) in FTD [35]. The authors used a randomized, double-blind, placebo-controlled parallel-group trial and administered INOT twice daily for one week to twenty-three individuals living with behavioral variant FTD or semantic dementia using a dose-escalation design. The primary outcome measures were safety and tolerability at each dose, while secondary measures explored efficacy of repeated INOT administration for improving aspects of social cognition (i.e., social behavior) and neuropsychiatric symptoms in FTD, as reported by a caregiver. Results indicated that repeated administration of INOT was safe and well tolerated at doses up to 72 IU twice daily, and distinct trends were evident to suggest that higher doses of INOT reduced participant apathy and improved empathic concern as indexed by the Interpersonal Reactivity Index (IRI) [38].
In light of these encouraging findings, the next important step is to establish whether INOT administration improves social cognitive function in the most common forms of dementia (those with AD and/or VaD). Such a trial would also aim to elucidate whether INOT administration might also improve caregiver-patient interpersonal relationships. However, before conducting a full-scale RCT, it is necessary to first establish feasibility of the intervention, determining optimal procedures and outcome measures [39].
Aims and hypotheses
The overarching aims of this study were to conduct a pilot feasibility trial to determine optimal procedures and outcome measures, in order to plan for a larger full-scale RCT. Specifically, we sought to determine the feasibility of recruitment, the acceptability of enrolment and the adherence to trial treatments in order to inform the subsequent design of a larger full-scale RCT. In addition, we sought to determine the effect size estimates on key potential primary and secondary outcome measures related to both the participant and their respective caregiver.
MATERIALS AND METHODS
Trial design
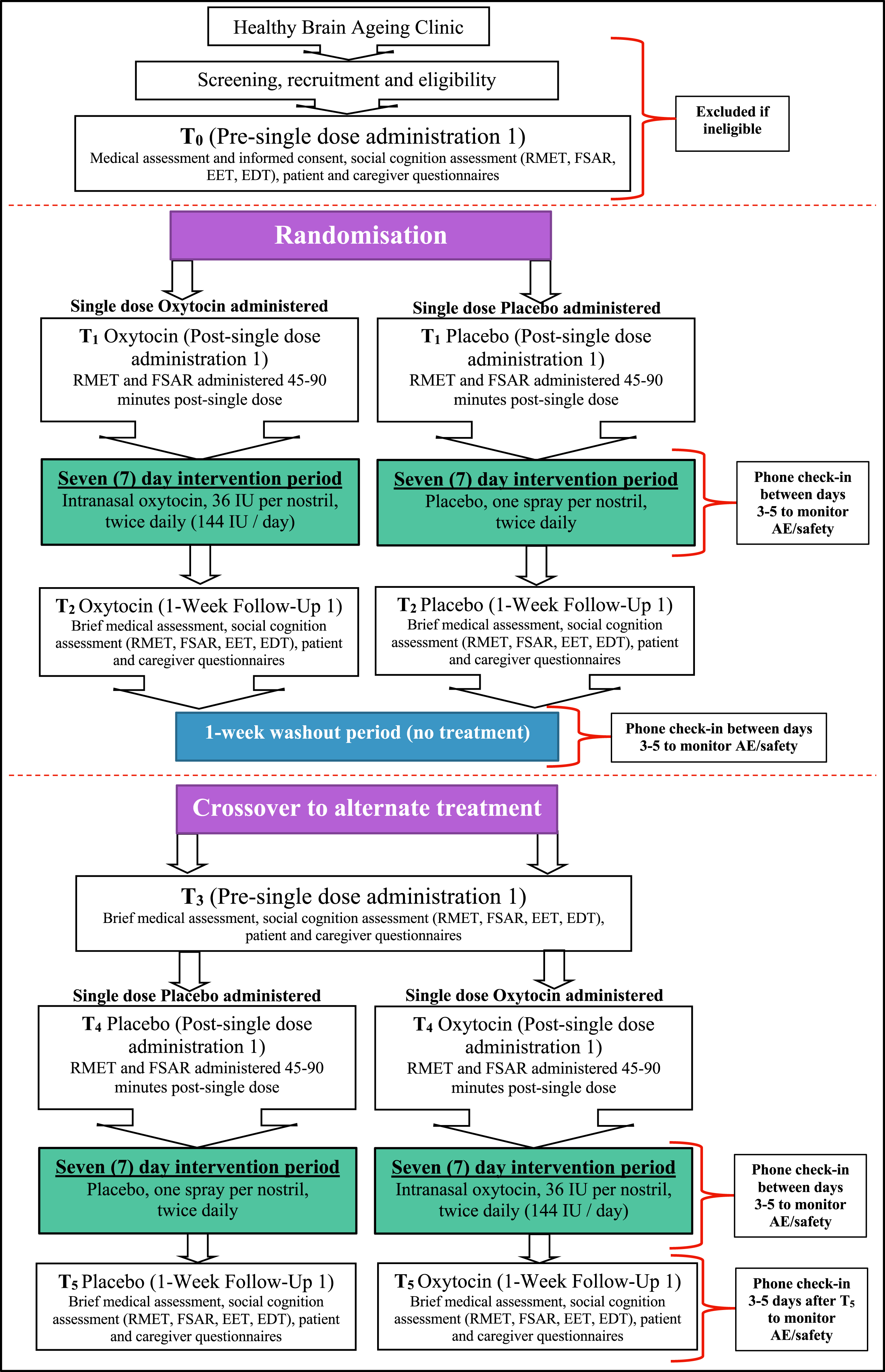
Participants were enrolled in a single-center, randomized, double-blind, placebo-controlled crossover trial involving a one-week treatment period with both INOT (72 IU) and a placebo treatment. See Fig. 1 for a graphical illustration of the trial design. There were six occasions of measurement over four distinct visits to the Trial Coordinating Centre for each participant. These were: pre-single dose administration 1 (T0) and post-single dose administration 1 (T1); one-week follow-up 1 (T2); pre-single dose administration 2 (T3) and post-single dose administration 2 (T4); and one-week follow-up 2 (T5). Participants were randomly assigned to receive either INOT or placebo for one-week (at T0), followed by a one-week washout (between T2 and T3), and crossover to the alternate treatment (administeredat T3).
Fig. 1
Flow diagram of study design, including recruitment and randomization. RMET, Reading the Mind in the Eyes Test; FSAR, Facial Speed and Recognition Task; EET, Emotion Evaluation Test; EDT, Emotion Discrimination Test; AE, Adverse Event.
Ethical considerations
The trial was approved by the Human Ethics Review Committee (RPAH Zone) of the Sydney Local Health District (Reference Number: X15-0255). The trial was prospectively registered on the Australian and New Zealand Clinical Trial Registry (ACTRN12617001531303, 03 November 2017). All participants provided written informed consent to take part in the trial, and all data was obtained in compliance with the Helsinki Declaration.
Participants
Participants were outpatients recruited from the Healthy Brain Ageing (HBA) Clinic, a specialist early intervention research clinic at the Brain and Mind Centre, The University of Sydney, Sydney, Australia (Trial Coordinating Centre). The HBA clinic recruits individuals aged over 50 years, with new onset cognitive concerns, a Mini-Mental State Examination (MMSE) Score≥20 and presenting with a referral from a General Practitioner or medical specialist. As detailed elsewhere [40], those with a history of stroke or transient ischemic attack, substance misuse, major neurological or psychiatric disease, prior head injury or substance abuse are excluded. Individuals attending the clinic receive a comprehensive medical, psychological, and neuropsychological assessment.
Inclusion criteria for this pilot trial were: 1) aged between 60 to 90 years; 2) current diagnosis of mild AD, VaD, or mixed AD/VaD (MMSE > 21); 3) have a caregiver who will live with the participant during the trial.
Exclusion criteria for this pilot trial were: 1) prior history of major psychiatric disorder (e.g., schizophrenia, bipolar disorder); 2) a score of≤40 on the Benton Facial Recognition Test [41]; 3) a score on the 18-item Hamilton Depression Rating Scale greater than 16 [42]; 4) prescription of a cholinesterase inhibitor medication for less than three months or experiencing side effects secondary to this class of medication; 5) prescription of an antidepressant medication for less than one month, experiencing side effects related to this medication or the antidepressant is contraindicated with INOT treatment; 6) prescription of the following classes of medications: non-cholinesterase inhibitor medications for dementia, antipsychotics, antidepressants, benzodiazepines, sedatives, and hypnotics; 7) prior history of neurological disorder (e.g., head injury, stroke or transient ischemic attack, epilepsy); 8) diagnosis of another neurodegenerative disease (e.g., dementia with Lewy bodies, frontotemporal dementia, Parkinson’s disease dementia); 9) an intellectual disability; 10) a current history of substance abuse; 11) history of a myocardial infarction within the last two years or congestive heart failure; 12) current uncontrolled hypertension; 13) bradycardia (rate < 50 beats per minute/bpm) or tachycardia (rate > 100 bpm); 14) diagnosis of long QT syndrome; 15) use of prostaglandins and their analogues; 16) use of any anesthetic (inhalation or caudal); 17) known allergies to oxytocin or to preservatives in the nasal spray; 18) severe nasal obstruction/blockage; 19) severely compromised hepatic function; 20) severely compromised renal function.
Interventions
All participants were randomized on a 1 : 1 basis to the order in which they received the two treatment arms:
INOT - 72 IU OT nasal spray, that is 36 IU administered per nostril, twice daily for one-week (i.e., 144 IU per day). This dosage was chosen based on prior evidence demonstrating safety and tolerability but importantly improvements in apathy and empathy measures, as well as improved patient–caregiver interactions [35].
Placebo – glycerol (2%); sorbitol crystalline powder (2%); benzyl alcohol (0.9%) and distilled water nasal spray administered once per nostril, twice daily for one-week.
Both the oxytocin and placebo nasal sprays were manufactured by Pci Pharma Services (formerly Pharmaceutical Packaging Professionals) an Australian Therapeutic Goods Administration (TGA) approved manufacturer and finisher of pharmaceutical products, who also sourced oxytocin from a local Australian manufacturer. The actuator (product ID: 10254044) and pump (product ID: 10280515) used for both nasal sprays were sourced from Aptar Pharma.
Caregivers were asked to administer the nasal spray, once per nostril twice daily. To ensure the correct technique was used for nasal spray administration, the caregiver was required to administer the first dose at T0 and T3 in the presence of clinicians at the Trial Coordinating Centre.
Monitoring and adverse reporting
Compliance and safety monitoring was conducted by telephone assessment (as indicated in Supplementary Table 1) and at each scheduled clinical review and follow-up assessment. Participants were required to return any unused portion of the nasal spray bottle as well as their medication-tracking calendar to trial clinicians at T2 and T5. Nasal spray compliance was assessed by weighing each nasal spray bottle before and after each treatment period.
Throughout the trial, details of current and new concomitant medications were recorded and clarified with a medical practitioner. Specific attention was focused on medications that were likely to interfere with INOT, as detailed in the Investigators’ Brochure. Participants and their caregiver were informed of all medications that were considered to be contraindicated with INOT before trial randomization and asked to inform the investigators on the commencement of any medications during the trial period.
Outcomes
Feasibility outcome measures were obtained at each visit (T0 - 5) by assessors blind to treatment allocation.
Trial feasibility outcomes
Three trial feasibility outcomes were measured adopting guidelines from the most recent Consolidated Standards of Reporting Trials (CONSORT) statement for a pilot and feasibility RCTs [43], each to inform towards progression of a larger full-scale RCT:
i) Feasibility of recruitment of eligible patients who consent to trial enrolment. Our ‘stop-go’ measures related to feasibility of recruitment were:
• Greater than 50% eligible to enroll are enrolled - continue to main trial.
• Between 30–50% eligible to enroll are enrolled - consider a modified trial.
• Less than 30% eligible to enroll are enrolled - do not progress to a main trial using this model.
ii) Acceptability: proportion of randomized participants who complete their final 1-week follow-up (T5) assessment. In addition, percentage of randomized participants who were lost to follow up.
iii) Adherence to trial treatments: proportion of randomized participants that adhere to 70% or more (≥10/14 INOT doses) of the allocated treatment.
Effect size estimates for expected primary participant and caregiver outcomes for a larger full-scale RCT
It was expected that for a larger trial the primary outcome for the participant would be ToM abilities as assessed by performance on the Reading the Mind in the Eyes Test (RMET) [44] following single-dose INOT administration. The RMET is a well-validated social cognitive task, that measures a participant’s ability to make mentalistic inferences based on eye gaze cues. Possible raw scores on the RMET range from 0 to 36. For the caregiver it was expected that for a larger trial the primary outcome would be observed changes in the participant’s perspective-taking and empathic-concern, as measured using the IRI [38], following one-week repeated INOT administration.
Effect size estimates for expected secondary participant and caregiver outcomes for a larger full-scale RCT
It was expected that for a larger trial the secondary outcomes for the participant and caregiver would be further separated following single-dose administration and one-week repeated administration.
Following single-dose INOT administration
The Facial Speed and Recognition task [45] simultaneously measures the participant’s accuracy and speed of emotion recognition from well-validated facial images (the Karolinska Directed Emotional Faces database [46, 47]), varying in emotional intensity from 10% to 100% over a 10 second period. Possible raw scores on the Facial Speed and Recognition task range from 0 to 36.
Following daily INOT administration for one-week
Social cognitive
The Emotion Evaluation Test (EET) is a test of social perception from The Awareness of Social Interference Test (TASIT) that measures the participant’s interpretation of naturalistic emotional cues including facial movement, tone of voice and gestures [48]. Possible raw scores on the TASIT range from 0 to 28. The Emotion Discrimination Test (EDT) also provides an index of social perception. This measure is adapted from the Facial Expressions of Emotion: Stimuli and Tests [49], and measures the participants ability to identify facial emotions (anger, sadness, happiness, disgust or surprise) from photographs. Possible raw scores on the EDT range from 0 to 24. The Facial Speed and Recognition task was also used to measure speed and accuracy of emotion recognition.
Questionnaires (participant focused)
Apathy was assessed using the Apathy Evaluation Scale [50], and overall well-being and quality of life with the WHO (Five) Well-being Index (WHO-5) [51]. Depression was assessed using the 15-item Geriatric Depression Scale (GDS-15) [52]. Functional status and sleeping habits were assessed with the HBA Functional Assessment and Sleep Questionnaires, respectively (questionnaires that are routinely administered in the HBA clinic). The Socioemotional Dysfunction Scale (SDS) [53] was used to index social behavior, while the [54] was used to index broader behavioral disturbances.
Questionnaires (caregiver focused)
Patient-caregiver relationships were assessed with the Intimate Bond Measure (IBM) [55], while caregiver ‘burden’ was assessed with Zarit Burden Interview (ZBI) [56]. Caregivers’ well-being and quality of life was assessed with the WHO-5, while depression was assessed using the GDS-15.
Randomization and blinding
Trial randomization codes were computer-generated by the Trial Manager, who had no contact with the participants, using a random block size that was not available to any study personnel. These randomization codes were held by the pharmacy for the duration of the trial. At T0, the Trial Medical Officer assigned the participant to the next randomization number, which was provided to the pharmacist who prepared and dispensed the treatments as per the randomization list. For the purposes of blinding, the placebo nasal spray was manufactured to be identical in appearance and weight to the OT nasal spray. Apart from the Trial Manager and the dispensing Pharmacist, all study personnel involved in the conduction of assessments with the participant were blinded throughout the study, including data analysis.
Statistical methods
Statistical analysis was conducted using SPSS Version 25 (SPSS Inc., Chicago, IL, USA). Descriptive analyses (i.e., frequencies, means, standard deviations) were performed to provide an overview of the data. Where appropriate, treatment (OT, Placebo)×exposure treatment period (pre-single dose versus post single-dose; pre-single dose versus one-week follow up) repeated-measure ANOVAs were conducted. Due to the limited sample size (n = 4), we focused on reporting mean differences and the effect size partial eta squared (ηp2).
RESULTS
Participants, randomization, and baseline characteristics
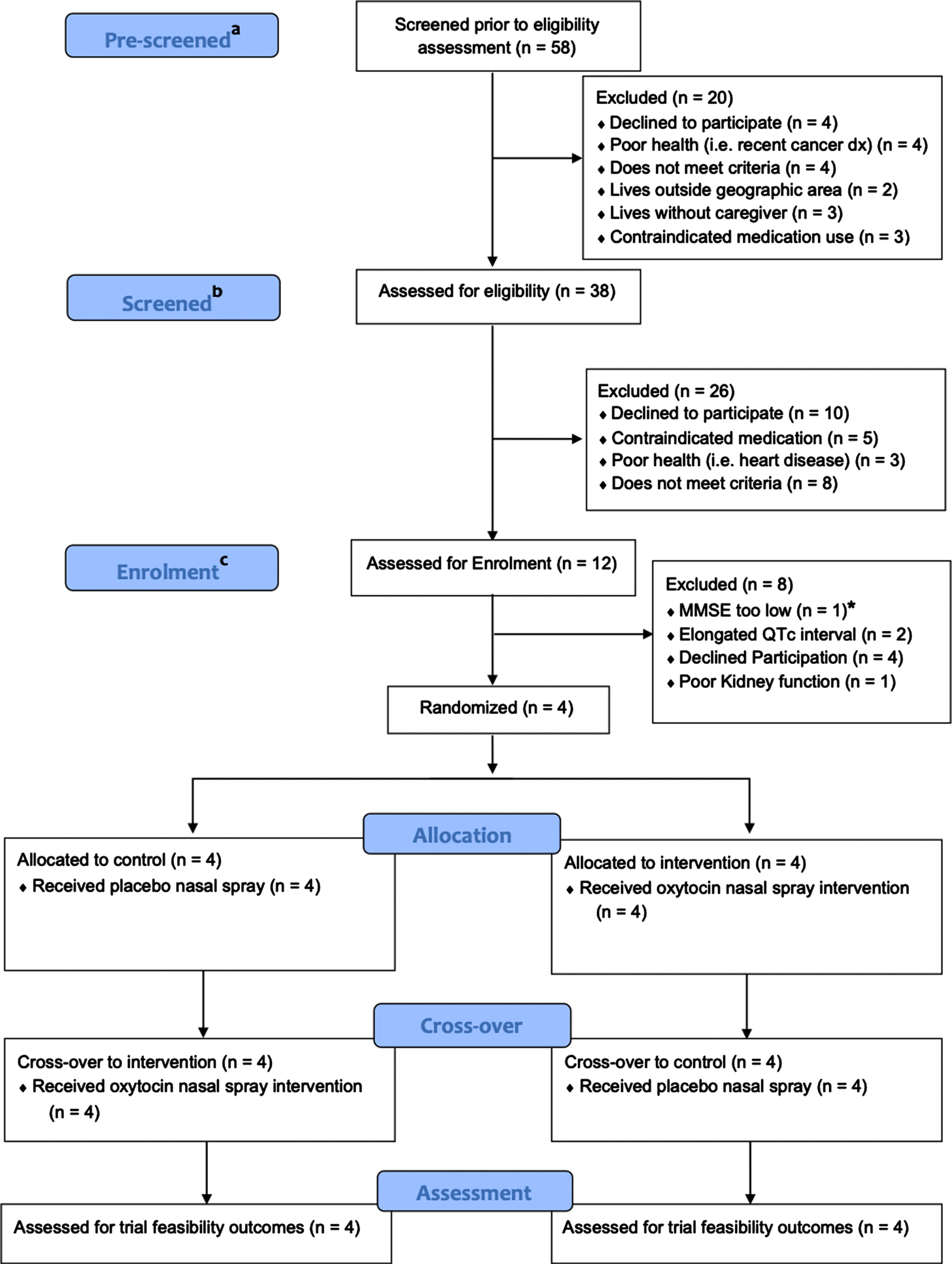
As illustrated in Fig. 2, participant recruitment occurred between February 2018 and February 2020 with a total of four participants randomized. All four participants had a clinical diagnosis of AD. Individual participant medications used are listed in Supplementary Table 6, with no participant reporting any change in medication use or dose duringthe trial.
Fig. 2
CONSORT Flow Chart. aTelephone-screened, prior to receiving participant information statement (i.e., declined immediately); bTelephone-screened, following provision of the participant information statement; cBooked-in for baseline assessment. * Excluded before randomization as baseline MMSE < 21.
Participants at time of randomization had a mean age of 72.3 years, with secondary level of education (mean = 12.5 years). Importantly, the mean MMSE score reported of 25.5 was within our criteria of early-to-mid AD (MMSE score 20–26 [57]). Other participant characteristics are reported in Supplementary Table 2.
Feasibility outcomes
Of the 58 individuals screened for eligibility and enrolment in the current trial (Fig. 2) over a 24-month recruitment period, 48% (n = 28/58) were screened retrospectively from an existing pool that presented for assessment to the HBA clinic within the prior 12 months and received a diagnosis of dementia. The remaining 52% (n = 30/58) of individuals living with dementia were prospectively pre-screened for the trial.
More specifically, pre-screening failure following active file review was 34.4% (n = 20/58), yielding a screening sample of 38. Approximately, a further half of the sample were excluded (n = 26/58, 44%) following screening, resulting in a total of 12 potential participants that were assessed for enrolment and booked in for T0. From this sample, a third subsequently enrolled into the trial (n = 4/12, 33%). Therefore, in total, four individuals (n = 4/58, 7%) enrolled and were randomized of which all were a part of the retrospectively screened pool. All four (100%) randomized participants completed their final follow-up assessment showing high acceptability of the protocol. Importantly, adherence to placebo and OT nasal sprays were very high (as measured by a medication tracking calendar completed by the caregiver), with 95% of all placebo doses and 98% of OT doses administered correctly as prescribed (Supplementary Table 5).
Effect sizes on expected primary outcomes for a larger full-scale RCT
Given that this was a pilot trial, with a limited sample size (n = 4), with a focus on feasibility related to recruitment, enrolment, and adherence to trial treatments, we report the effect size estimates for expected primary outcomes for a larger full-scale RCT related to both the participants and their respective caregivers. As shown in Table 1A, following single-dose INOT (72 IU) administration, no meaningful effect size for RMET performance was observed. With respect to the caregiver, following one-week repeated INOT administration, participant’s perspective-taking abilities as rated by their caregiver remained stable, compared to a mean worsening (mean difference = -2.3) for participants administered the placebo nasal spray. This corresponded to a large effect size (ηp2 = 0.18) (Table 2).
Table 1A
Social cognitive performance (mean ± S.D.) before pre-single dose administration and following post-single dose administration for placebo and oxytocin treatment groups
| Social cognition Test | Placebo Nasal Spray | Oxytocin Nasal Spray | Overall | |||||||
| Pre-single dose administration | Post-single dose administration | Mean difference | Pre-single dose administration | Post-single dose administration | Mean difference | Partial Eta Squared | 90% Confidence Interval | F (1,6) | p | |
| RMET, raw score | 27.0±1.8 | 26.3±3.8 | -0.7 | 27.5±1.7 | 25.8±5.0 | -1.7 | 0.02 | 0.00-0.31 | 0.14 | 0.72 |
| FSAR, total | 18.5±8.8 | 22.0±5.7 | 3.5 | 20.5±2.4 | 20.0±6.5 | -0.5 | 0.09 | 0.00-0.41 | 0.62 | 0.46 |
| FSAR, mean speed | 7.9±1.7 | 8.1±0.5 | 0.2 | 7.9±0.9 | 8.1±1.3 | -0.2 | 0.00 | 0.00-0.05 | 0.01 | 0.94 |
RMET, Reading the Mind in the Eyes Test; FSAR, Facial Speed and Recognition Task.
Effect sizes on expected secondary outcomes for a larger full-scale RCT
Social cognition
As reported in Table 1B, following one-week repeated INOT administration, no meaningful effect size between OT and placebo groups were observed for RMET performance or speed and accuracy of recognition as assessed by the Facial Speed and Recognition Task (FSAR). While there were mean reductions in performance on the EDT and EET between OT and placebo groups following a one-week treatment period, reductions were greater for participants administering placebo on both the EDT and EET, such that a medium effect size was observed when compared to those administering INOT (ηp2 = 0.05 and ηp2 = 0.04, respectively).
Table 1B
Social cognitive performance (mean±S.D.) before pre-single dose administration and after one-week follow-up for placebo and oxytocin treatment groups
| Social cognition Test | Placebo Nasal Spray | Oxytocin Nasal Spray | Overall | |||||||
| Pre-single dose administration | One-week Follow-Up | Mean difference | Pre-single dose administration | One-week Follow-Up | Mean difference | Partial Eta Squared | 90% Confidence Interval | F (1,6) | p | |
| RMET, raw score | 27.0±1.8 | 25.8±5.3 | -1.2 | 27.5±1.7 | 27.0±2.9 | -0.5 | 0.01 | 0.00-0.28 | 0.09 | 0.78 |
| FSAR, total | 18.5±8.8 | 21.5±4.7 | 3.0 | 20.5±2.4 | 23.3±3.4 | 2.8 | 0.00 | - | 0.00 | 0.96 |
| FSAR, mean speed | 7.9±1.7 | 8.1±0.5 | -0.2 | 7.9±0.9 | 8.1±1.3 | -0.2 | 0.00 | - | 0.00 | 0.96 |
| EET | 17.8±4.7 | 16.8±5.4 | -1.0 | 18.0±5.0 | 15.5±3.9 | -2.5 | 0.05 | 0.00-0.36 | 0.34 | 0.58 |
| EDT | 16.5±2.4 | 16.0±2.4 | -0.5 | 15.8±3.2 | 14.8±4.0 | -1.0 | 0.04 | 0.00-0.34 | 0.23 | 0.65 |
RMET, Reading the Mind in the Eyes Test; FSAR, Facial Speed and Recognition Task; EET, Emotion Evaluation Test; EDT, Emotion Discrimination Test.
Additionally, following single-dose administration with the placebo nasal spray, a mean increase in participants’ emotion recognition accuracy as indexed by the FSAR was reported, corresponding to a medium effect size (ηp2 = 0.09) (Table 1A).
See Supplementary Table 3 for individual participant pre-single dose administration, post-single dose administration and one-week follow up social cognitive test scores following placebo and oxytocin treatment.
Caregiver and self-reports
As reported in Table 2, following one-week repeated INOT administration, caregivers reported a mean reduction in ‘burden’ as assessed by the ZBI corresponding to a large effect size (ηp2 = 0.19) compared to when participants were administering the placebo nasal spray. Improved intimacy and interpersonal bonding were also observed by respective caregivers, with an effect size approaching large in magnitude (ηp2 = 0.14), following one-week repeated INOT administration.
Table 2
Questionnaire data (mean±S.D.) before pre-single dose administration and after one-week follow up for placebo and oxytocin treatment groups
| Questionnaire | Placebo Nasal Spray | Oxytocin Nasal Spray | Overall | |||||||
| Pre-single dose administration | One-week Follow-Up | Mean difference | Pre-single dose administration | One-week Follow-Up | Mean difference | Partial Eta Squared | 90% Confidence Interval | F (1,6) | p | |
| Caregiver-report | ||||||||||
| AES | 29.5±11.0 | 28.0±13.4 | -1.5 | 27.5±12.1 | 25.3±15.7 | -2.2 | 0.01 | - | 0.00 | 0.81 |
| GDS-15 | 2.8±2.5 | 2.3±2.6 | -0.5 | 2.5±2.9 | 1.8±1.7 | -0.7 | 0.01 | 0.00-0.14 | 0.03 | 0.86 |
| HBA FAQ | 43.5±45.6 | 25.5±39.1 | -18.0 | 28.8±39.7 | 0.5±1.0 | -28.3 | 0.03 | 0.00-0.33 | 0.18 | 0.69 |
| HBA SQ | 12.3±8.5 | 8.5±5.4 | -3.8 | 7.8±2.5 | 8.5±4.7 | 0.7 | 0.33 | 0.00-0.60 | 2.98 | 0.14 |
| IBM | 30.5±13.8 | 31.8±10.5 | 1.3 | 31.3±13.4 | 36.0±17.3 | 4.7 | 0.14 | 0.00-0.46 | 0.98 | 0.36 |
| IRI-EC | 17.5±3.9 | 18.0±5.5 | -0.5 | 16.8±4.2 | 17.3±6.0 | 0.5 | 0.00 | - | 0.00 | 1.00 |
| IRI-PT | 13.8±2.8 | 11.5±4.7 | -2.3 | 13.3±1.0 | 13.3±2.6 | 0.0 | 0.18 | 0.00-0.49 | 1.30 | 0.30 |
| NPI | 13.5±7.0 | 18.8±16.5 | 5.3 | 10.3±3.6 | 15.0±4.9 | 4.7 | 0.00 | 0.00-0.51 | 0.01 | 0.94 |
| SDS | 106.8±17.6 | 104.5±18.2 | -2.3 | 100.5±30.6 | 95.5±23.9 | -5.0 | 0.04 | 0.00-0.35 | 0.27 | 0.62 |
| WHO-5 | 14.5±2.4 | 16.0±4.2 | 1.5 | 13.8±5.7 | 15.8±3.7 | 2.0 | 0.01 | 0.00-0.14 | 0.03 | 0.87 |
| ZBI | 40.0±12.7 | 41.0±15.2 | 1.0 | 41.0±13.0 | 38.3±13.5 | -2.7 | 0.19 | 0.00-0.51 | 1.40 | 0.28 |
| Self-report | ||||||||||
| WHO-5 | 19.0±4.2 | 19.3±2.2 | 0.3 | 18.3±4.3 | 20.0±3.6 | 1.7 | 0.09 | 0.00-0.41 | 0.62 | 0.46 |
| GDS-15 | 2.3±1.3 | 1.8±1.0 | -0.5 | 1.3±0.5 | 2.0±1.8 | 0.7 | 0.17 | 0.00-0.48 | 1.19 | 0.32 |
AES, Apathy Evaluation Scale; GDS-15, 15-item Geriatric Depression Scale; HBA FAQ, Healthy Brain Ageing Functional Assessment Questionnaire; HBA SQ, Healthy Brain Ageing Sleep Questionnaire; IBM, Intimate Bond Measure; IRI-EC/PT, Interpersonal Reactivity Index-Empathic Concern/Perspective-Taking subscales; NPI, Neuropsychiatric Inventory; SDS, Socioemotional Dysfunction Scale; WHO-5, World Health Organization (Five) Well-Being Index; ZBI, Zarit Burden Interview.
Participants reported a mean improvement in their health and well-being as assessed by the WHO-5 following one-week repeated INOT administration, corresponding to a medium effect size (ηp2 = 0.09). Interestingly however, following one-week repeated INOT administration there was a mean increase in self-reported depressive symptoms on the GDS-15, corresponding to large effect size (ηp2 = 0.17).
See Supplementary Table 4 for individual participant self-report questionnaire data before pre-single dose administration and after one-week follow up for placebo and oxytocin treatment groups.
Treatment tolerability, adverse events and blinding
Participation rates were high, with all sessions attended by each participant. No significant adverse events were reported by any participant on either the INOT or placebo treatment. Notably, two participants reported an increase in sexual behavior; interestingly, however, one participant’s report of change (8 on a scale of 0 to 10) was during the placebo treatment, while the other participant (3 on a scale of 0 to 10) was during the INOT treatment. See Supplementary Table 7 for individual frequencies of side effects reported. Lastly, while both participants and their caregivers were blinded to each treatment while enrolled in the trial, participants along with their caregivers were asked whether they could identify the treatment at the end of each intervention period (T3 and T5). While no participant was able to correctly determine either treatment, three out of four caregivers correctly determined both treatments in correct order.
DISCUSSION
This is the first study to investigate the feasibility of a trial administering one-week of repeated INOT (72 IU) for social cognitive function in participants living with mild dementia, and their caregivers. The trial outcomes focused on feasibility, acceptability, adherence, and suitability of outcome measures. The first key finding was that our data showed that over a 24-month trial period, our feasibility of recruitment (to inform the design of a potential larger full-scale RCT), was not acceptable. With only four of fifty-eight individuals with dementia screened meeting eligibility criteria, the method of recruitment used here is unsuitable for progressing to a larger full-scale RCT.
However, regarding our other key feasibility outcomes, the acceptability of enrolment for those randomized to the trial was excellent (100%) and their adherence to trial treatments was extremely high (placebo, 95%; OT, 98%) for a study of this nature [58]. Moreover, no serious adverse events, or treatment-causative adverse events, resulted from an INOT treatment. In terms of our expected primary outcomes for a larger full-scale RCT, we found only a small negative/negligible effect on RMET performance, suggesting that single-dose INOT administration may have few if any effects on ToM abilities. Caregivers of participants administering INOT reported improvements in the participant’s perspective-taking abilities (as assessed by the IRI) following one-week repeated INOT administration, corresponding to a large effect size. Positive/large effects were also evident in key secondary outcomes focused on self-reported health and wellbeing, caregiver ‘burden’, intimacy, and interpersonal bonding.
This trial was built on the successes of INOT use in neuropsychiatric populations such as schizophrenia and autism spectrum disorder [22–24], and recent evidence of its safety and tolerability in FTD, with preliminary evidence showing improvements in apathy and patient-caregiver interactions [35]. As Finger et al. (2015) have reported that one-week repeated administration of all doses of INOT (24, 48, and 72 IU) may be considered safe and well tolerated in FTD, we report that for participants living with AD too, one-week repeated INOT (72 IU) administration can also be regarded as safe and well tolerated. Indeed, INOT-treatment adherence was extremely high, with 98% of all OT doses timely administered (compared to 95% for placebo), and no adverse events reported related to trial treatment.
Poor recruitment for a trial of this nature is not uncommon. Indeed, a recent report has described that more than one quarter of RCTs are prematurely discontinued due to poor recruitment [59]. Given that this was a pilot feasibility trial, with outcomes to inform towards the progression of a larger full-scale RCT, it is most important to discern the reasons why participants were excluded or declined to participate. Between the period of February 2018 and April 2020, of the 58 individuals with dementia assessed for eligibility, 36/54 (67%) were deemed ineligible due to meeting the strict exclusion criteria (i.e., contraindicated medication use, poor health, elongated QTc interval, no caregiver present to support) that could not be modified for a trial of this nature with an experimental treatment that required close monitoring. It is most often studies trialing a novel medical drug/device, requiring narrower eligibility criteria to accurately capture their clinical sample, that subsequently experience poor recruitment [59]. Thus, in informing the design of a larger full-scale RCT, the results from this trial suggest that with such strict eligibility criteria, an increase in the recruitment pool, change of setting and/or a multi-site study is needed. In this trial, individuals living with dementia were recruited from a specialist ‘early intervention’ HBA research clinic focused on those with early forms of cognitive decline such as mild cognitive impairment and with an MMSE≥20. Over the 24-month recruitment period, the HBA clinic assessed 283 patients (between 3-6 patients per week), of which 11% (n = 32/382) received a diagnosis of dementia. In a general memory clinic service, on average 25% of patients presenting to the clinic met a dementia diagnosis [60]. While recruitment from the HBA clinic in this trial has provided great insight into recruitment strategy and trial enrolment, it may be more appropriate for a larger full-scale RCT to recruit from a general memory clinic setting across multiple sites [61]. It is also reasonable to suggest a that loosening of the exclusion criteria is explored where there is no compromise to the health and safety of participants enrolled in the trial.
Beyond feasibility outcomes, we were interested in whether INOT administration can improve social cognitive function, in particular ToM and emotion recognition. Following both single-dose INOT administration and one-week repeated INOT administration, no meaningful change was observed on any test of social cognition (RMET, FSAR, EDT, or EET). At the case level too, it appeared that INOT did not improve performance on any test of social cognitive function (see Supplementary Table 4). While the reasons for these null findings are not entirely clear, given reports indicating that INOT administration improves social cognitive function in FTD and other neuropsychiatric populations [23, 36, 62], a possible explanation might be that our participant group had relatively preserved social cognitive function at baseline. For example, all four participants’ baseline RMET performance (z-score range, -0.3 to 0.8) would not be indicative of impairments in ToM abilities, particularly when compared to those adults living with MCI (a potential ‘prodromal stage’ of dementia) that have been shown to demonstrate greater impairments in ToM abilities as assessed by the RMET (n = 114; mean z-score=-0.4; z-score range = -4.8 to 2.2) [63]. Given the small sample size and the fact that this was the first study to investigate whether INOT administration can improve social cognitive function for participants living with AD, further investigations are warranted, ideally with a larger, more heterogeneous group of people living with AD, including those with pronounced social cognitive impairment at baseline.
Following one-week repeated INOT administration, we also identified medium-to-large effect size improvements in participants’ self-reported health and wellbeing and perspective-taking ability, as well as in caregiver reports of ‘burden’ and patient-caregiver intimacy and bonding. Firstly, these observed improvements in participants’ health and wellbeing, align with a large body of research involving children with autism spectrum disorder, healthy adult controls, and adults with schizophrenia [29, 30, 64]. Secondly, given the physiological role of OT in mediating social behaviors of bonding, intimacy and interpersonal relationships [30], where caregiver reported mean reductions in ‘burden’ (as assessed by the ZBI [56]) and increases in interpersonal bonding (as assessed by the IBM [55]) following repeated INOT administration, these data provide encouraging preliminary evidence that INOT treatment not only benefits an individual living with AD, but may also improve caregiver sense of ‘burden’ and facilitate improvements in interpersonal relationships. Indeed, these reductions in caregiver ‘burden’ and improvements in interpersonal bonding, may be associated with perspective-taking abilities, or the ability for a person to look beyond their own point of view, considering how someone else may think or feel about something [65]. We report that following one-week repeated INOT administration a participant’s INOT perspective-taking abilities remained unchanged (mean difference = 0) compared to a mean reduction in the placebo group (mean difference = -2.3), corresponding to a large effect size (ηp2 = 0.18). In fact, these results corroborate previous reports that INOT has the propensity to improve or at least maintain perspective-taking abilities in individuals with schizophrenia [66]. Nevertheless, while these interpretations are reported cautiously due to the limited sample size, our study adds to growing literature, suggesting that OT may be able to improve aspects of health and well-being, and patient-caregiver interpersonal relationships.
Altogether, our negligible effect findings on participant social cognitive function and our large effect findings of improvements to caregiver ‘burden’, intimacy, and bonding following repeated INOT administration provide valuable insights toward the design of outcome measures for a larger full-scale RCT. As previously mentioned, because OT serves an important physiological role in mediating interpersonal relationships [15–17, 19], it is not surprising that the largest effect sizes reported in this trial were those secondary outcomes focused on interpersonal relationships from a caregiver’s perspective. Two studies investigating INOT in FTD reported no improvement in facial affect recognition but significant improvements in neuropsychiatric symptoms as rated by the caregiver [35, 36]. Future full-scale RCTs should therefore examine an INOT treatment in dementia from multiple perspectives, including around a caregiver’s sense of ‘burden’ which is considered to be a leading factor contributing to the placement of an individual living with dementia in residential care [20].
In summary, our study provides initial evidence demonstrating the safety and tolerability of INOT (72 IU) administration in individuals living with dementia. No serious adverse events, or treatment-causative adverse events, resulted from INOT treatment, and although we had a limited sample in this study, we report medium-to-large effect size improvements in patient self-reported health and wellbeing as well as in critical aspects of social cognitive function including perspective-taking, caregiver ‘burden’ and interpersonal relationships. This suggests the potential broad-ranging beneficial effects of INOT should be assessed in future RCTs from multiple perspectives. Further, while future work will be required to modify the study design in order to address poor recruitment, the acceptability of enrolment and the adherence to study treatments were extremely high for a study of this nature.
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This trial was supported by the Alzheimer’s Australia Dementia Research Foundation (now Dementia Australia) [Grant number DGP14-36] and the Mason Foundation [Grant number CT 21357].
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data are not publicly available due to privacy or ethical restrictions.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ADR-230013.
REFERENCES
[1] | Prince MJ , Wimo A , Guerchet MM , Ali GC , Wu Y-T , Prina M ((2015) ) World Alzheimer Report 2015. The Global Impact of Dementia: An analysis of prevalence, incidence, cost and trends. Alzheimer’s Disease International, London. |
[2] | Fernando MS , Ince PG ((2004) ) Vascular pathologies and cognition in a population-based cohort of elderly people. J Neurol Sci 226: , 13–17. |
[3] | McAleese KE , Alafuzoff I , Charidimou A , De Reuck J , Grinberg LT , Hainsworth AH , Hortobagyi T , Ince P , Jellinger K , Gao J ((2016) ) Post-mortem assessment in vascular dementia: Advances and aspirations. BMC Med 14: , 1–16. |
[4] | Schneider JA , Arvanitakis Z , Bang W , Bennett DA ((2007) ) Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 69: , 2197–2204. |
[5] | Bediou B , Ryff I , Mercier B , Milliery M , Hénaff MA , D’Amato T , Bonnefoy M , Vighetto A , Krolak-Salmon P ((2009) ) Impaired social cognition in mild Alzheimer disease. J Geriatr Psychiatry Neurol 22: , 130–140. |
[6] | Elamin M , Pender N , Hardiman O , Abrahams S ((2012) ) Social cognition in neurodegenerative disorders: A systematic review. J Neurol Neurosurg Psychiatry 83: , 1071–1079. |
[7] | Hargrave R , Maddock RJ , Stone V ((2002) ) Impaired recognition of facial expressions of emotion in Alzheimer’s disease. J Neuropsychiatry Clin Neurosci 14: , 64–71. |
[8] | Henry JD , Von Hippel W , Molenberghs P , Lee T , Sachdev PS ((2016) ) Clinical assessment of social cognitive function in neurological disorders. Nat Rev Neurol 12: , 28. |
[9] | Kessels RP , Waanders-Oude Elferink M , van Tilborg I ((2021) ) Social cognition and social functioning in patients with amnestic mild cognitive impairment or Alzheimer’s dementia. J Neuropsychol 15: , 186–203. |
[10] | Laisney M , Bon L , Guiziou C , Daluzeau N , Eustache F , Desgranges B ((2012) ) Cognitive and affective Theory of Mind in mild to moderate Alzheimer’s disease. J Neuropsychol 7: , 107–120. |
[11] | McLellan T , Johnston L , Dalrymple-Alford J , Porter R ((2008) ) The recognition of facial expressions of emotion in Alzheimer’s disease: A review of findings. Acta Neuropsychiatr 20: , 236–250. |
[12] | Yi Z , Zhao P , Zhang H , Shi Y , Shi H , Zhong J , Pan P ((2020) ) Theory of mind in Alzheimer’s disease and amnestic mild cognitive impairment: A meta-analysis. Neurol Sci 41: , 1027–1039. |
[13] | Beer JS , Ochsner KN ((2006) ) Social cognition: A multi level analysis. Brain Res 1079: , 98–105. |
[14] | Leppanen JM ((2006) ) Emotional information processing in mood disorders: A review of behavioral and neuroimaging findings. Curr Opin Psychiatry 19: , 34–39. |
[15] | Shimokawa A , Yatomi N , Anamizu S , Torii S , Isono H , Sugai Y , Kohno M ((2001) ) Influence of deteriorating ability of emotional comprehension on interpersonal behavior in Alzheimer-type dementia. Brain Cogn 47: , 423–433. |
[16] | Greve KW , Cadieux N , Hale MA ((1994) ) Emotion processing and caregiver stress in Alzheimer’s disease: A preliminary report. Clin Gerontol 15: , 85–78. |
[17] | Moore MJ , Zhu CW , Clipp EC ((2001) ) Informal costs of dementia care: Estimates from the National Longitudinal Caregiver Study. J Gerontol B Psychol Sci Soc Sci 56: , S219–S228. |
[18] | McCade D , Savage G , Guastella A , Hickie IB , Lewis SJG , Naismith SL ((2013) ) Emotion recognition in mild cognitive impairment: Relationship to psychosocial disability and caregiver burden. J Geriatr Psychiatry Neurol 26: , 165–173. |
[19] | Spitzer N , Shafir T , Lerman Y , Werner P ((2019) ) The relationship between caregiver burden and emotion recognition deficits in persons with MCI and early AD. Alzheimer Dis Assoc Disord 33: , 266–271. |
[20] | Cepoiu-Martin M , Tam-Tham H , Patten S , Maxwell Colleen J , Hogan David B ((2016) ) Predictors of long-term care placement in persons with dementia: A systematic review and meta-analysis. Int J Geriatr Psychiatry 31: , 1151–1171. |
[21] | Brodaty H ((1997) ) Caregivers and behavioral disturbances: Effects and interventions. Int Psychogeriatr 8: , 455–458. |
[22] | Guastella AJ , Mitchell PB , Mathews F ((2008) ) Oxytocin enhances the encoding of positive social memories in humans. Biol Psychiatry 64: , 256–258. |
[23] | Guastella AJ , Einfeld SL , Gray KM , Rinehart NJ , Tonge BJ , Lambert TJ , Hickie IB ((2010) ) Intranasal oxytocin improves emotion recognition for youth with autism spectrum disorders. Biol Psychiatry 67: , 692–694. |
[24] | Guastella AJ , MacLeod C ((2012) ) A critical review of the influence of oxytocin nasal spray on social cognition in humans: Evidence and future directions. Hormones Behav 61: , 410–418. |
[25] | Marsh AA , Yu HH , Pine DS , Blair RJ ((2010) ) Oxytocin improves specific recognition of positive facial expressions. Psychopharmacology (Berl) 209: , 225–232. |
[26] | Ulrike R , Karin H , Markus H , Peter K ((2009) ) Oxytocin makes a face in memory familiar. J Neurosci 29: , 38. |
[27] | Hubble K , Daughters K , Manstead AS , Rees A , Thapar A , van Goozen SH ((2017) ) Oxytocin reduces face processing time but leaves recognition accuracy and eye-gaze unaffected. J Int Neuropsychol Soc 23: , 23–33. |
[28] | Weisman O , Zagoory-Sharon O , Feldman R ((2012) ) Intranasal oxytocin administration is reflected in human saliva. Psychoneuroendocrinology 37: , 1582–1586. |
[29] | Barraza JA , Grewal NS , Ropacki S , Perez P , Gonzalez A , Zak PJ ((2013) ) Effects of a 10-day oxytocin trial in older adults on health and well-being. Exp Clin Psychopharmacol 21: , 85–92. |
[30] | Bernaerts S , Prinsen J , Berra E , Bosmans G , Steyaert J , Alaerts K ((2017) ) Long-term oxytocin administration enhances the experience of attachment. Psychoneuroendocrinology 78: , 1–9. |
[31] | Fischer-Shofty M , Shamay-Tsoory SG , Harari H , Levkovitz Y ((2010) ) The effect of intranasal administration of oxytocin on fear recognition. Neuropsychologia 48: , 179–184. |
[32] | Kosfeld M , Heinrichs M , Zak PJ , Fischbacher U , Fehr E ((2005) ) Oxytocin increases trust in humans. Nature 435: , 673–676. |
[33] | Hurlemann R , Patin A , Onur OA , Cohen MX , Baumgartner T , Metzler S , Dziobek I , Gallinat J , Wagner M , Maier W , Kendrick KM ((2010) ) Oxytocin enhances amygdala-dependent, socially reinforced learning and emotional empathy in humans. J Neurosci 30: , 4999–5007. |
[34] | Baumgart M , Snyder HM , Carrillo MC , Fazio S , Kim H , Johns H ((2015) ) Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimers Dement 11: , 718–726. |
[35] | Finger EC , MacKinley J , Blair M , Oliver LD , Jesso S , Tartaglia MC , Borrie M , Wells J , Dziobek I , Pasternak S , Mitchell DGV , Rankin K , Kertesz A , Boxer A ((2015) ) Oxytocin for frontotemporal dementia: A randomized dose-finding study of safety and tolerability. Neurology 84: , 174–181. |
[36] | Jesso S , Morlog D , Ross S , Pell MD , Pasternak SH , Mitchell DG , Kertesz A , Finger EC ((2011) ) The effects of oxytocin on social cognition and behaviour in frontotemporal dementia. Brain 134: , 2493–2501. |
[37] | Cummings JL ((1997) ) The Neuropsychiatric Inventory. Neurology 48: , 10S. |
[38] | Davis MH ((1983) ) Measuring individual differences in empathy: Evidence for a multidimensional approach. J Pers Soc Psychol 44: , 113–126. |
[39] | Livingston G , Rapaport P ((2020) ) Implementation should now be considered in parallel with designing clinical research. Int Psychogeriatr 32: , 1393–1395. |
[40] | Lin P , LaMonica HM , Naismith SL , Mowszowski L ((2022) ) Identifying subtle functional change in individuals with mild cognitive impairment: Development and validation of the Healthy Brain Ageing – Functional Assessment Questionnaire. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 30: , 536–554. |
[41] | Benton A , Sivan A , Hamsher K , Varney N , Spreen O ((1994) ), Contributions to neuropsychological assessment: A clinical manual. Oxford University Press, New York. |
[42] | Hamilton M ((1960) ) A rating scale for depression. J Neurol Neurosurg Psychiatry 23: , 56. |
[43] | Eldridge SM , Chan CL , Campbell MJ , Bond CM , Hopewell S , Thabane L , Lancaster GA ((2016) ) CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 355: , i5239. |
[44] | Baron-Cohen S , Wheelwright S , Hill J , Raste Y , Plumb I ((2001) ) The “Reading the Mind in the Eyes” Test Revised Version: A study with normal adults, and adults with asperger syndrome or high-functioning autism. J Child Psychol Psychiatry 42: , 241–251. |
[45] | Quintana DS , Westlye LT , Hope S , NT , Elvsåshagen T , Dørum E , Rustan Ø , Valstad M , Rezvaya L , Lishaugen H , Stensønes E , Yaqub S , Smerud KT , Mahmoud RA , Djupesland PG , Andreassen OA ((2017) ) Dose-dependent social-cognitive effects of intranasal oxytocin delivered with novel Breath Powered device in adults with autism spectrum disorder: A randomized placebo-controlled double-blind crossover trial. Transl Psychiatry 7: , e1136. |
[46] | Garrido MV , Prada M ((2017) ) KDEF-PT: Valence, emotional intensity, familiarity and attractiveness ratings of angry, neutral, and happy faces. Front Psychol 8: , 2181. |
[47] | Goeleven E , De Raedt R , Leyman L , Verschuere B ((2008) ) The Karolinska Directed Emotional Faces: A validation study. Cogn Emotion 22: , 1094–1118. |
[48] | McDonald S , Flanagan S , Rollins J , Kinch J ((2003) ) TASIT: A new clinical tool for assessing social perception after traumatic brain injury. J Head Trauma Rehabil 18: , 219–238. |
[49] | Young A , Perrett DI , Calder A , Sprengelmeyer RH , Ekman P ((2002) ) Facial expressions of emotion: Stimuli and Test (FEEST). Thames Valley Test Company, Bury St Edmunds, Suffolk. |
[50] | Marin RS , Biedrzycki RC , Firinciogullari S ((1991) ) Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res 38: , 143–162. |
[51] | Heun R , Bonsignore M , Barkow K , Jessen F ((2001) ) Validity of the five-item WHO Well-Being Index (WHO-5) in an elderly population. Eur Arch Psychiatry Clin Neurosci 251: , 27–31. |
[52] | Sheikh JI , Yesavage JA ((1986) ) Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin Gerontol 5: , 165–173. |
[53] | Barsuglia JP , Kaiser NC , Wilkins SS , Joshi A , Barrows RJ , Paholpak P , Panchal HV , Jimenez EE , Mather MJ , Mendez MF ((2014) ) A scale of socioemotional dysfunction in frontotemporal dementia. Arch Clin Neuropsychol 29: , 793–805. |
[54] | Cummings JL ((1997) ) The Neuropsychiatric Inventory: Assessing psychopathology in dementia patients. Neurology 48: , S10–S16. |
[55] | Wilhelm K , Parker G ((1988) ) The development of a measure of intimate bonds. Psychol Med 18: , 225–234. |
[56] | Bédard M , Molloy DW , Squire L , Dubois S , Lever JA , O’Donnell M ((2001) ) The Zarit Burden Interview: A new short version and screening version. Gerontologist 41: , 652–657. |
[57] | Wattmo C , Minthon L , Wallin ÅK ((2016) ) Mild versus moderate stages of Alzheimer’s disease: Three-year outcomes in a routine clinical setting of cholinesterase inhibitor therapy. Alzheimers Res Therapy 8: , 7. |
[58] | Shiovitz TM , Bain EE , McCann DJ , Skolnick P , Laughren T , Hanina A , Burch D ((2016) ) Mitigating the effects of nonadherence in clinical trials. J Clin Pharmacol 56: , 1151–1164. |
[59] | Briel M , Speich B , von Elm E , Gloy V ((2019) ) Comparison of randomized controlled trials discontinued or revised for poor recruitment and completed trials with the same research question: A matched qualitative study. Trials 20: , 800. |
[60] | Rozsa M , Ford A , Flicker L ((2016) ) Assessing people with dementia: The role of the aged care assessment team and memory clinics. Intern Med J 46: , 1081–1088. |
[61] | Jeon Y-H , Simpson JM , Low L-F , Woods R , Norman R , Mowszowski L , Clemson L , Naismith SL , Brodaty H , Hilmer S ((2019) ) A pragmatic randomised controlled trial (RCT) and realist evaluation of the interdisciplinary home-bAsed Reablement program (I-HARP) for improving functional independence of community dwelling older people with dementia: An effectiveness-implementation hybrid design. BMC Geriatr 19: , 199. |
[62] | Guastella AJ , Ward PB , Hickie IB , Shahrestani S , Hodge MA , Scott EM , Langdon R ((2015) ) A single dose of oxytocin nasal spray improves higher-order social cognition in schizophrenia. Schizophr Res 168: , 628–633. |
[63] | Michaelian JC , Mowszowski L , Guastella AJ , Henry JD , Duffy S , McCade D , Naismith SL ((2019) ) Theory of mind in mild cognitive impairment – relationship with limbic structures and behavioural change. J Int Neuropsychol Soc 25: , 1023–1034. |
[64] | Ishak WW , Kahloon M , Fakhry H ((2011) ) Oxytocin role in enhancing well-being: A literature review. J Affect Disord 130: , 1–9. |
[65] | Galinsky AD , Ku G , Wang CS ((2005) ) Perspective-taking and self-other overlap: Fostering social bonds and facilitating social coordination. Group Process Intergroup Relat 8: , 109–124. |
[66] | Gibson CM , Penn DL , Smedley KL , Leserman J , Elliott T , Pedersen CA ((2014) ) A pilot six-week randomized controlled trial of oxytocin on social cognition and social skills in schizophrenia. Schizophr Res 156: , 261–265. |


