
Iterative Review and Revision of the Enhancing Active Caregiver Training (EnACT) Intervention
Abstract
Interventions that actively engage dementia caregivers show promise in reducing the negative outcomes of caregiving but lack optimization and systematic testing. The purpose of this manuscript is to describe an iterative process developed to refine an intervention to enhance active engagement. A three-stage review process with content experts was developed to refine activities in preparation for focus group feedback and pilot testing. We identified caregiving vignettes, reorganized engagement techniques, and optimized focus group activities for online delivery to promote caregiver access and safety. The framework developed from this process is included, along with a template to guide intervention refinement.
INTRODUCTION
Behavioral symptoms such as agitation, combativeness, depression, and apathy affect up to 90% of persons living with dementia [1]. Interventions have been developed to help caregivers manage symptoms and include a variety of approaches such as professional support, psychoeducation, behavioral management/skills training, counseling/psychotherapy, and self-care/relaxation training [2–4]. Most caregiver interventions tested in controlled trials demonstrate weak to moderate effect sizes on measures of behavioral symptoms, as well as other outcomes (e.g., caregiver burden, functional independence, time to institutionalization) [2]. The most successful psychoeducational interventions use active-engagement techniques to facilitate the application of knowledge and skills [2, 5–7]. Examples of active-engagement strategies include role play, problem solving, application of new knowledge, and discussion [2–7]. Yet the methods for optimization and systematic testing of active-engagement techniques is lacking [2, 3, 5–7]. By optimizing active-engagement techniques within interventions, we may further strengthen positive outcomes for dementia caregivers.
Enhancing Active Caregiver Training (EnACT) is an arts-based intervention aimed at engaging dementia caregivers by using active-engagement techniques that allow them to better manage common behavioral symptoms associated with dementia. EnACT enhances active engagement using effective strategies found in education, communication, and the arts. For example, adult learning principles such as experiential learning [8], increases active-engagement [9], whereas multisensory experiences enhance active-engagement through understanding and awareness [10]. Structured imagination activities, such as those practiced in theatre, have been used to enhance advance preparation, which increases the detail of understanding, enhances realism, and allows people to practice and prepare for real-world experiences [11–13]. EnACT can serve as a stand-alone intervention designed to reduce caregiver burden by better preparing caregivers to deal with stressful behavioral symptoms associated with dementia, and/or be integrated into existing interventions to enhance application of active engagement. EnACT uses caregiver-informed videos depicting common caregiving vignettes [14, 15] and theatre-based role-playing exercises to create multisensory experiences that enhance active-engagement of caregivers by allowing them to practice, or rehearse, their reactions and skills within a safe environment. The development of this intervention has been guided by two theories: 1) imagined-interactions theory [16–18] and 2) the consequences of dementia caregivers’ stress process [19] with the goal of improving caregiver capacity to adapt and appraise demands of caregiving through practice.
Guided by the NIH Stage Model (Stage 1a) [20], we refined intervention components prior to eliciting feedback from dementia caregivers. We conducted multiple stages of iterative review and revision with content experts to accomplish this aim. The purpose of this manuscript is to describe the process we developed to refine the EnACT intervention and present tools that others can use as a practical guide for intervention refinement.
METHODS
As part of a larger sequential qualitative-to-quantitative mixed-method design study to develop and test EnACT, we designed and implemented an iterative three-stage process to receive and incorporate feedback into the intervention. The EnACT intervention includes three steps within each intervention session. Step one involves group viewing of a caregiving vignette from a filmed theatrical performance of the ethnodrama, Portrait of a Caregiver, developed during previous research [14, 15] portraying situations in which a caregiver is dealing with a challenging behavioral symptom. Step two involves small-group practice activities to facilitate understanding. Step three includes group processing surrounding observations. These three steps of EnACT were reviewed during a three-stage process by 1) a caregiving expert/clinician, 2) two applied humanities researchers with expertise in arts-based healthcare training, and 3) a three-person research team completing a mock focus group. Reviews were recorded using digital audio and field notes to identify problems, explore areas for improvement, and make revisions. Descriptive analysis was used to assess the process of revising and preparing intervention materials and protocols to prepare for focus group review with dementia caregivers and initial efficacy testing in a randomized controlled trial. While the larger study received approval from the University of Utah Institutional Review Board, this interval step did not require informed consent as it did not include human subjects research and focused on program development in partnership with content experts.
REVIEW PROCESS
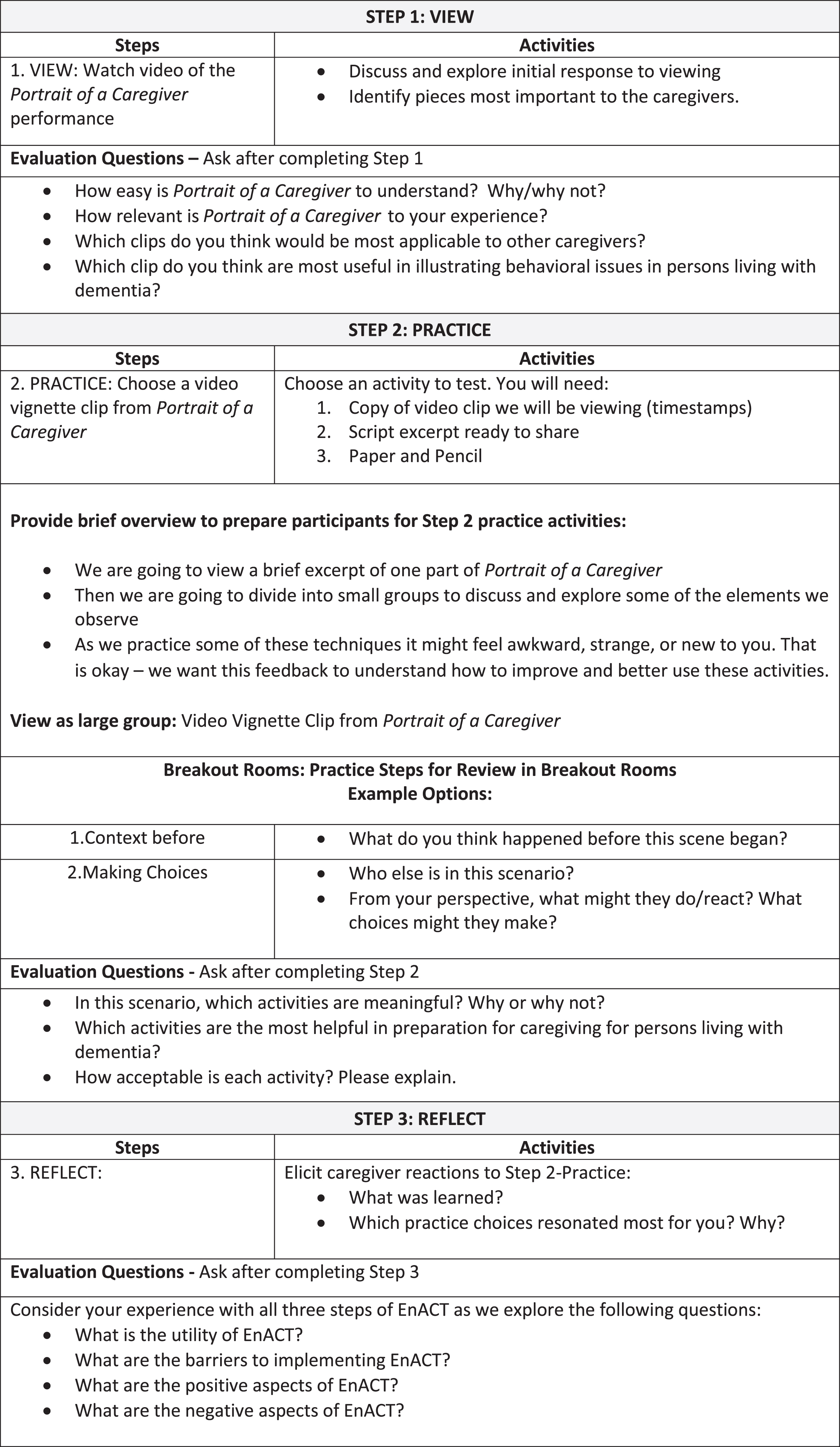
Here we describe the three-stage review process (Fig. 1), present the template we used to guide each stage (Table 1), and the final protocol prepared for future focus group testing (Table 2). Between review stages, we made specific changes to EnACT to address expert feedback.
Fig. 1
Enhancing Active Caregiver Training (EnACT) three-stage review process and revisions.
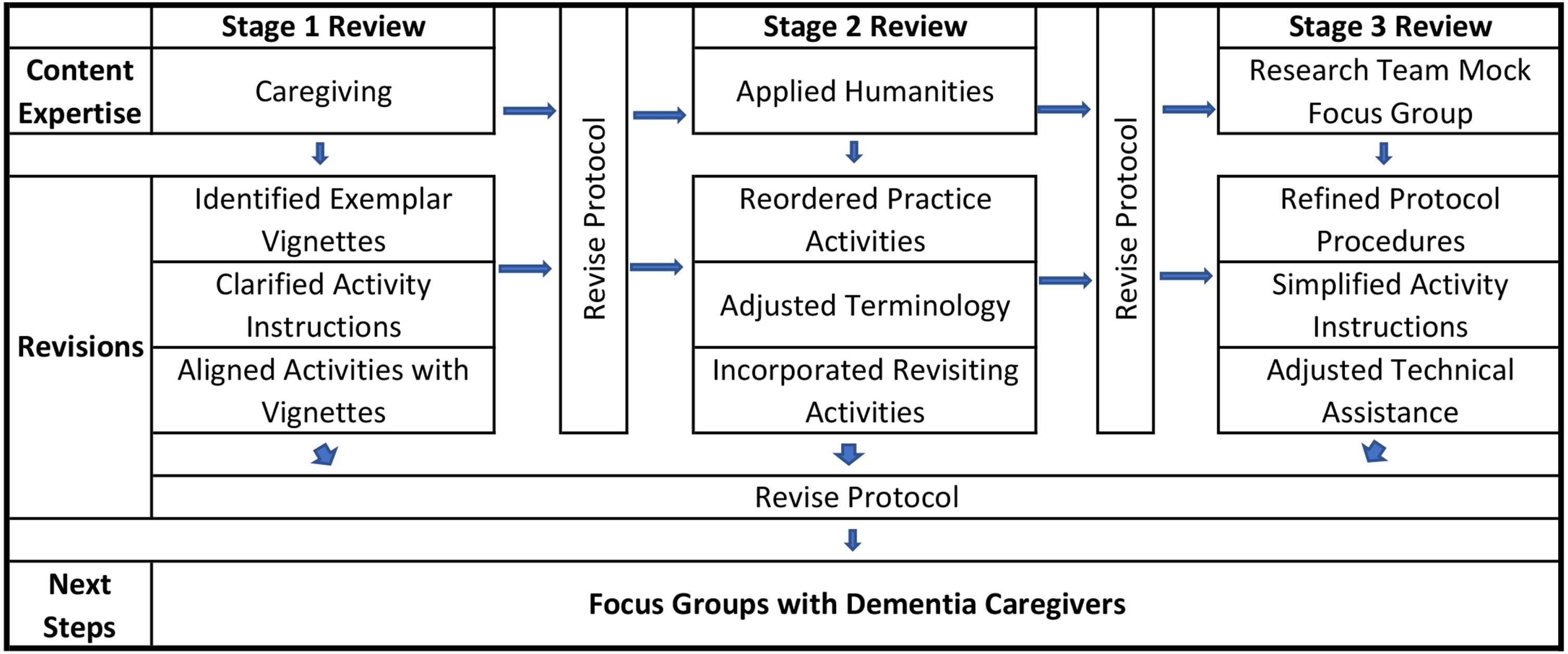
Table 1
Template for iterative review and revision during intervention development
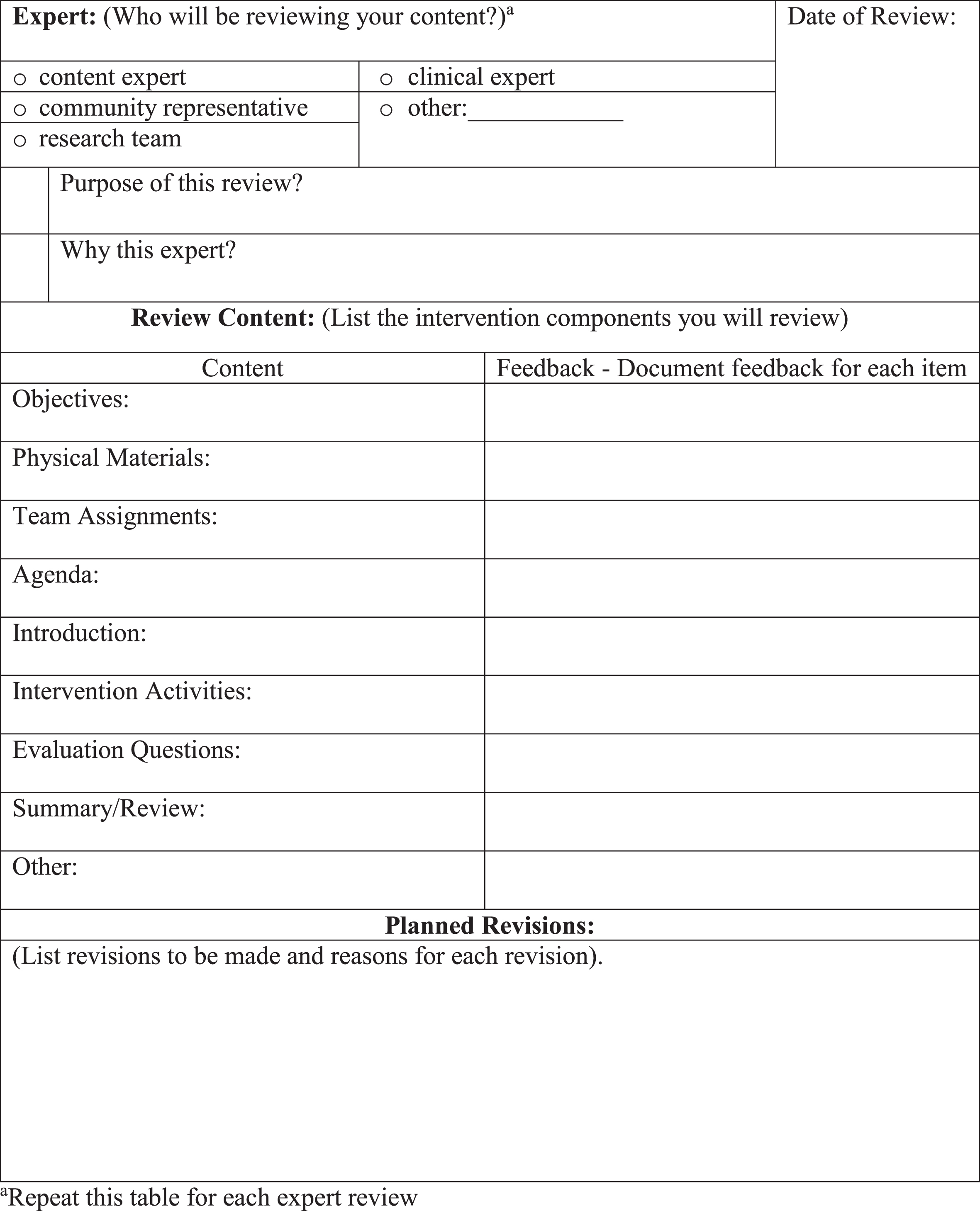 |
Table 2
EnACT protocol developed for focus group testing
 |
Stage one: Review by content expert in caregiving
In stage one, we provided a draft of our intervention to a social worker with expertise in dementia caregiver training and support. We asked for initial reactions and feedback as we presented the three EnACT steps. For step one, this caregiving expert recommended that participants view the 40-minute Portrait of a Caregiver theatrical performance [14, 15] before discussing behavior-specific vignettes, in order to understand the overall production. During review of step two, practice activities, the expert recommended that caregivers reflect on what happened before and after the behavioral symptom (as demonstrated in a video clip) that may have influenced the behavior. Additionally, the expert emphasized that practice activities should help caregivers explore what the person living with dementia is trying to express through their behavior. The expert found some of the practice activities confusing (e.g., asking individuals to explore what is missing in vignettes) and suggested clarification. In addition, the expert identified vignettes they felt best aligned with specific practice activities. Finally, they noted that some of the practice activities seemed to overlap with others and recommended that we choose one activity for each vignette.
Stage two: Review by content experts in applied humanities
During stage two, two subject matter experts in arts-based healthcare training reviewed the revised intervention materials. Overall feedback focused on terminology, narrative structure, and applied techniques to incorporate in preparation for focus group review. They recommended taking one vignette and working through multiple activities to explore the narrative of each vignette more fully. They also recommended that the dementia caregiver focus group selects the vignettes they find most meaningful for inclusion. In the future, this would allow those using the intervention, to choose from a variety of vignettes and activities that align with didactic training topics and caregiver needs.
One major suggestion was to change the order of practice activities to reflect a narrative flow, which may help participants think through each vignette in a logical manner from beginning, through the middle, to the end. The experts also introduced the idea of revisiting activities in the context of other explorations. For example, when assessing the thoughts of one character early in the group discussion, it would be beneficial to return and reassess the character’s thoughts after exploring the perspectives of other characters in the scene.
The reviewers recommended changing activity terminology to encourage exploration. For example, one activity was titled “Opposite Perceptions.” Reviewers suggested removing the word “opposite,” which is a term that may be viewed as only the direct opposite of something observed. Instead, reviewers recommended changing the activity title to “Other Perspectives” to elicit answers that explore observations beyond just the opposite. Finally, recommendations were made to revise discussion questions to explore how to improve outcomes for the caregiver and the person living with dementia and to facilitate more concrete examples, such as “ ... now that we have other choices, what other endings can you imagine?”
Stage three: Research team review
In stage three, the research team (PI and two graduate research assistants) tested the protocol procedures in a mock focus group. Feedback from stages one and two led to the recommendation to move focus groups to an online Zoom platform to reduce caregiver burden and promote access and safety during COVID. In preparation, we met with our Information Technology Department (IT) and other research teams familiar with running online focus groups. We developed a system for technical assistance and online setup, to reduce potential technology problems.
The research team held a mock focus group using the revised protocol. The PI facilitated, while the two research assistants served as practice participants. This allowed us to a) work through the protocol procedures and intervention materials and b) assess potential problems with technology. We clarified unclear activity instructions, added expected waiting time for responses, and planned for potential difficulties when facilitating the groups in a virtual environment. This session helped us identify a need to assign research team members specific roles to reduce problems. These assignments included: observational field notes, monitoring waiting room and chat functions, primary recording and backup, and screensharing. We also decided to mail participants hard copies of materials to facilitate intervention review.
Summary of intervention protocol
The protocol developed for focus group testing outlined the three-step intervention process: 1) view, 2) practice, 3) reflect (Table 2). Step one in this process includes viewing the full 40-minute video of Portrait of a Caregiver in the initial focus group. The viewing is followed by asking participants to identify moments that resonate with them in order to identify which clips will be used as part of EnACT. We anticipate that caregivers will be interested in exploring vignettes associated with behavioral symptoms, such as: putting clothes on backwards, mirroring eating, hallucinations, and perseveration. The second part of the protocol focuses on practicing for caregiving using theatre-based exploration through storytelling, improvisation, changing the narrative, and writing prompts. These activities were developed to actively engage participants in exploring the caregiving vignettes viewed in step one. Activities were organized for both small and large groups. Finally, participants reflect on the experience in step three, where participants identify what is learned, what choices were explored, and reactions to the experience.
In addition to having caregivers participate in these intervention activities, we plan to ask caregivers participating in focus groups to evaluate each component of the intervention. This will allow us to evaluate which aspects of the intervention work, the acceptability of each component, and determine the elements that are most difficult or do not work. Following caregiver focus group feedback, we will revise each component of the intervention and test implementation in a future randomized controlled trial (RCT). The RCT will assess the influence of EnACT on outcomes such as caregiver burden, perceived stress, and caregiver wellbeing.
DISCUSSION
This research report provides practical steps research teams may take to enhance intervention content and procedures in preparation for intervention development guided by the NIH Stage Model [20]. Testing this process in advance facilitated procedural revisions with the goal of enhancing engagement and reducing barriers to participation. After working with a series of subject matter experts, our next step in this research is to conduct focus groups with family caregivers of persons living with dementia. The focus groups will allow us to refine the EnACT intervention for future feasibility and pilot testing and identify how this process influences outcomes for caregivers of persons living with dementia. When preparing to conduct a feasibility trial for a behavioral intervention, seeking feedback enhances protocols to improve intervention processes and community partnerships. Future researchers should consider publishing similar processes to promote transparency and reproducibility. Iterative review has the potential to reduce extraneous problems, enhancing the ability of the research team to focus on participant feedback specific to dementia caregivers and their needs.
ACKNOWLEDGMENTS
We acknowledge with gratitude content expertise from Nancy Madsen-Wilkerson, Dr. Gretchen Case, and Dr. Sydney Cheek-O’Donnell, in addition to research methods support from Dr. Katherine Supiano, and Dr. Rebecca Utz. We are also grateful for information technology support from Mike Mcintosh and the College of Nursing, University of Utah.
FUNDING
This work was supported by funding from the National Institute on Aging [Eaton, K01AG065623] and the National Institute of Nursing Research [Neller, T32NR013456].
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCES
[1] | Robinson KM , Crawford TN , Buckwalter KC , Casey DA ((2018) ) Outcomes of a two-component intervention on behavioral symptoms in persons with dementia and symptom response in their caregivers. J Appl Gerontol 37: , 570–594. |
[2] | Walter E , Pinquart M ((2019) ) How effective are dementia caregiver interventions? An updated comprehensive meta-analysis. Gerontologist 60: , e609–e619. |
[3] | Gilhooly KJ , Gilhooly ML , Sullivan MP , McIntyre A , Wilson L , Harding E , Woodbridge R , Crutch S ((2016) ) A meta-review of stress, coping and interventions in dementia and dementia caregiving. BMC Geriatr 16: , 106. |
[4] | Gaugler J , Jutkowitz E , Shippee TP , Brasure M ((2017) ) Consistency of dementia caregiver intervention classification: An evidence-based synthesis. Int Psychogeriatr 29: , 19–30. |
[5] | Witlatch CJ , Orsulic-Jeras S ((2018) ) Meeting the information, educational, and psychosocial support needs of persons living with dementia and their family caregivers. Gerontologist 58: , S58–S73. |
[6] | Tang S , Chio O , Chang L , Mao H , Chen L , Yip P , Hwang J ((2018) ) Caregiver active participation in psychoeducational intervention improved caregiving skills and competency. Geriatr Gerontol Int 18: , 750–757. |
[7] | Pinquart M , Sörensen S ((2006) ) Helping caregivers of persons with dementia: Which interventions work and how large are their effects? Int Psychogeriatr 18: , 577–595. |
[8] | Kolb D ((1984) ) Experiential Learning: Experience as the Source of Learning and Development, Prentice Hall, Englewood Cliffs NJ. |
[9] | Knowles MS , Holton RA , Swanson RA ((2011) ) The Adult Learner, Elsevier, Burlington MA. |
[10] | Choi CW , Honeycutt JM , Bodie GD ((2015) ) Effects of imagined interactions and rehearsal on speaking performance. Commun Educ 64: , 25–44. |
[11] | Ray CD , Floyd K , Mongeau PA , Mark L , Shufford KN , Niess L ((2019) ) Planning improves vocal fluency and the appearance of concern when communicating emotional support. Commun Res Rep 36: , 57–66. |
[12] | Bodie GD , Honeycutt JM , Vickery AJ ((2013) ) An analysis of the correspondence between imagined interaction attributes and functions. Hum Commun Res 39: , 157–183. |
[13] | Bruneau TJ ((1989) ) The deep structure of intrapersonal communication processes. In Intrapersonal Communication Processes: Original Essays, RobertsCV, WatsonKW, eds. SPECTRA, New Orleans LA, pp. 63–81. |
[14] | Eaton J , Madsen-Wilkerson N ((2017) ) Staging advocacy: Portrait of a caregiver. Public Policy Aging Rep 27: , S27–S30. |
[15] | Eaton J , Madsen-Wilkerson N ((2020) ) Portrait of a caregiver: Ethnodrama development and its influence on caregiver wellbeing. Gerontologist 60: , 1169–1178. |
[16] | Honeycutt JM ((2003) ) Imagined Interactions: Daydreaming About Communication, Hampton Press, Cresskill, NJ. |
[17] | Honeycutt JM ((2010) ) Imagine That: Studies in Imagined Interaction, Hampton, Cresskill, NJ. |
[18] | Honeycutt JM ((2019) ) Intrapersonal communication and imagined interactions: A musical application. In An Integrated Approach to Communication Theory and Research, StacksDW, SalwenMB, EichhornKC, eds. Routledge, New York, NY, pp. 321–332. |
[19] | Campbell JL , Rowe MA , Marsiske M ((2011) ) Behavioral symptoms of dementia: A dyadic effect of caregivers’ stress process? Res Gerontol Nurs 4: , 168–184. |
[20] | Onken LS , Caroll KM , Shoham V , Cuthbert BN , Riddle M ((2014) ) Reenvisioning clinical science: Unifying the discipline to improve the public health. Clin Psychol Sci 2: , 22–34. |


