
The Amyloid Cascade Hypothesis 2.0: Generalization of the Concept
Abstract
Recently, we proposed the Amyloid Cascade Hypothesis 2.0 (ACH2.0), a reformulation of the ACH. In the former, in contrast to the latter, Alzheimer’s disease (AD) is driven by intraneuronal amyloid-β (iAβ) and occurs in two stages. In the first, relatively benign stage, Aβ protein precursor (AβPP)-derived iAβ activates, upon reaching a critical threshold, the AβPP-independent iAβ-generating pathway, triggering a devastating second stage resulting in neuronal death. While the ACH2.0 remains aligned with the ACH premise that Aβ is toxic, the toxicity is exerted because of intra- rather than extracellular Aβ. In this framework, a once-in-a-lifetime-only iAβ depletion treatment via transient activation of BACE1 and/or BACE2 (exploiting their Aβ-cleaving activities) or by any means appears to be the best therapeutic strategy for AD. Whereas the notion of differentially derived iAβ being the principal moving force at both AD stages is both plausible and elegant, a possibility remains that the second AD stage is enabled by an AβPP-derived iAβ-activated self-sustaining mechanism producing a yet undefined deleterious “substance X” (sX) which anchors the second AD stage. The present study generalizes the ACH2.0 by incorporating this possibility and shows that, in this scenario, the iAβ depletion therapy may be ineffective at symptomatic AD stages but fully retains its preventive potential for both AD and the aging-associated cognitive decline, which is defined in the ACH2.0 framework as the extended first stage of AD.
INTRODUCTION
In the ACH2.0, AD is caused by iAβ: Two sources of AβPP-derived iAβ
Amyloid-β (Aβ), produced by proteolysis of its Aβ protein precursor (AβPP), is known to be secreted and to accumulate extracellularly; this Aβ pool is presumed to drive Alzheimer’s disease (AD) in the long-standing “amyloid cascade hypothesis” (ACH) theory of AD [1]. Yet the recently proposed ACH2.0 interpretation of the disease [2] posits that extracellular Aβ in general and Aβ plaques in particular are largely benign and, possibly, even physiologically protective, and that AD is actually driven by intraneuronal Aβ (iAβ). In other words, while the ACH2.0 remains aligned with the ACH premise that Aβ is toxic, the toxicity is exerted because of intra- rather than extracellular Aβ. But if AβPP-derived Aβ is secreted, how does it, evidently [3–15], end up within the cell? This happens in two ways. First, via the cellular uptake of secreted Aβ, which, in effect, constitutes its conversion to iAβ [16–31]. Formation of Aβ aggregates appears to be a prerequisite to its uptake [19–21], therefore more “sticky” Aβ species, e.g., Aβ42, are taken up twice as efficiently as rather common Aβ isoforms, e.g., Aβ40 [17]. The Aβ uptake is ApoE isoform-dependent, with ApoE4 being much more efficient than other ApoE species [8, 20], and is mediated by multiple receptors [20–30]; internalization of Aβ occurs in both healthy and AD-affected individuals [31].
The second source of AβPP-derived iAβ is its retention within neurons. The vast majority of AβPP-derived Aβ results from precursor’s gamma-cleavage on the plasma membrane and is secreted. A small fraction of precursor, however, undergoes gamma-cleavage on internal membranes and resulting Aβ is retained as iAβ [32–40]. Increases in retention of AβPP-derived Aβ, resulting from various mutations, were shown to be associated with AD [41,42]. Whereas both processes, internalization of secreted Aβ and marginal retention of AβPP-derived Aβ, are not AD-specific, their combined rates appear, as described below, to define the susceptibility to and the timing of the commencement of thedisease.
Accumulation of AβPP-derived iAβ culminates in integrated stress response and constitutes only the first stage of AD
The life-long accumulation of AβPP-derived iAβ is only the first, relatively benign, AD stage that sets up conditions for the activation of the second, devastating cascade that includes tau pathology, synaptic dysfunction, and neuronal loss. The central component of these conditions appears to be the integrated stress response (ISR). The ISR is a complex signaling pathway activated in response to a wide range of cellular stresses [43–52]. Its “integrating” feature is the convergence of all ISR-activating stimuli to the one common event, phosphorylation of eIF2α at serine 51, which is catalyzed by the family of eIF2α kinases comprised of four members: PKR, PERK, GCN2, and HRI. The ISR manifests as a severe reduction in global cellular protein synthesis, and, simultaneously, as the facilitation of translation of selected mRNAs, including those encoding specific transcription factors. Plausibly, among the induced transcriptions factors, or products of genes activated by them, are crucial components necessary and sufficient for the activation of a mechanism enabling the second stage of AD [2, 53–61]. iAβ, when sufficiently accumulated, was shown to activate both the PKR [62–68] and HRI [69, 70] kinases (the former via TNFα [67] or the PKR activator PACT [68], and the latter via mitochondrial dysfunction [71–87] and OMA1-DELE1-HRI signaling pathway [69, 70]); when this occurs, the elicitation of the ISRensues.
AD IS A TWO-STAGE DISEASE: THE GENERALIZED AMYLOID CASCADE HYPOTHESIS 2.0
A special case of the ACH2.0: The second stage of AD is driven by iAβ produced independently of AβPP
In the recently described version of the ACH2.0 [2], the mechanism activated by the AβPP-derived iAβ-elicited ISR and enabling the second AD stage is the AβPP-independent iAβ generation pathway [2, 56–61, 88–90], i.e., the drivers of both stages of AD are apparently identical but produced in distinct pathways. Crucially, as described in [2, 60, 61] and in the “Validation” section below, iAβ generated in the AβPP-independent pathway can be distinguished from that produced by AβPP proteolysis. Four distinct mechanisms for AβPP-independent generation of iAβ have been proposed [2, 60, 61]. Importantly, regardless of their mechanistic nature, each one of them is self-sustaining and completely autonomous. Indeed, in all, the entire output of the AβPP-independent pathway is retained intraneuronally and supports the activity of PKR and/or HRI kinases, which, in turn, perpetuate the ISR (or a yet undefined pathway) and thus ensure the continuous operation of the AβPP-independent iAβ production pathway. Sufficient accumulation of iAβ was shown to lead to the inhibition of the ubiquitin-proteosome system, facilitation of the build-up and hyperphosphorylation of tau protein, and tau pathology [91–94]. The feedback cycles of iAβ-activated AβPP-independent pathway generating iAβ, which propagates its own production, constitutes the Engine that drives AD [2]; the disease commences only following the activation of the AD Engine. In this context the combined rates of the internalization of secreted Aβ and of the retention of AβPP-derived iAβ determine when these joint Aβ fractions would reach the critical level (another key parameter) and activate the AβPP-independent iAβ generation pathway, thus defining both the susceptibility to and the timing of the commencement of AD. Once operational, the AD Engine renders the AβPP proteolytic pathway irrelevant for the progression of AD because its contribution of iAβ becomes insignificant in comparison with that of the AβPP-independent iAβ generation pathway.
Generalization of the ACH2.0
Whereas the notion of differentially derived iAβ being the principal moving force in the first as well as in the second stages of AD is both plausible and elegant (and, to use a modern physics-derived view, the beauty of a concept is both a prerequisite for and an indication of its correctness) and is supported by experimental data [88–90, 95, 96], a possibility, nevertheless, remains that the second AD stage is enabled by an AβPP-derived iAβ-activated self-sustaining mechanism producing a yet undefined deleterious “substance X” (sX) which anchors and drives the second AD stage. This generalized version of the ACH2.0 is illustrated in Fig. 1. Conceptually, it is very similar, if not identical, to the scenario described in the preceding section, which constitutes a special case of the generalized ACH2.0 where sX = (iAβ produced in the AβPP-independent mode). The sX-producing mechanism is assumed to be activated by the same processes, i.e., the ISR or a yet undefined pathway, that are postulated to initiate the AβPP-independent iAβ production in the special ACH2.0 case discussed above. The yet to be determined sX (if not iAβ) is presumed to be capable of (a) anchoring a cascade that includes tau pathology and leads to neuronal death and (b) sustaining the activity of one or more pathways listed in the middle box of Fig. 1, thus perpetuating the feedback cycles and its own production, i.e., powering the operation of the AD Engine. When it is operational, the sX-driven AD Engine is, in similarity to its iAβ-driven counterpart in the special ACH2.0 case, completely independent from the iAβ production in the AβPP proteolytic pathway, and renders it irrelevant for the progression of AD, a notion strongly supported by observations that suppression of the AβPP proteolysis at symptomatic stages had no effect whatsoever on the progression of AD [95, 96], consistent with the autonomous operation of the AD Engine. Likewise, in the generalized ACH2.0, the rate of AβPP-derived iAβ accumulation, combined with the extent of the threshold for activation of the sX-generating pathway, defines the susceptibility to the disease and determines the timing of its commencement. However, as described below, when sX is not iAβ, the similarity of the generalized ACH2.0 with its special case version does not extend to the outcomes of the proposed therapy [2] for symptomatic stages of AD.
Arguments for the uniform role of AβPP-derived iAβ in the first stage of AD
As described above, in the generalized ACH2.0, the second stage of AD can be envisioned in more than one iteration. On the other hand, this is apparently not the case for the first stage of the disease. The notion that it is uniformly driven by AβPP-derived iAβ is, if not a certainty, then at least a highly probable scenario. Indeed, consider the following.
Fig. 1
The generalized Amyloid Cascade Hypothesis 2.0 and the Engine that drives AD. Left Box (highlighted in gray): Life-long accumulation of AβPP-derived iAβ, through the cellular uptake of secreted peptide and intracellular retention of a fraction of AβPP-derived Aβ, to levels sufficient to ignite the AD “Engine” (rest of the figure). Middle Box: Several pathways, both actual (top two) and hypothetical (each line represent a pathway), of the Aβ-mediated elicitation of the integrated stress response or of yet unknown process capable of activating the cell-deleterious substance X (sX)-generating pathway. Top Box (highlighted in blue): Generation of intraneuronally retained sX. The yet to be determined sX is presumed to be capable of (a) anchoring a cascade that includes tau pathology and leads to neuronal death and (b) sustaining the activity of one or more pathways listed in the Middle Box, and thus perpetuating the feedback cycles and its own production. Right Box: sX rapidly accumulates intraneuronally; this sustains the operation of one or more of the AβPP-derived iAβ-mediated pathways shown in the Middle Box, which, in turn, support the generation of sX. It could be argued that the requirement that sX supports its own production is redundant in view of the continuous influx of AβPP-derived iAβ. However, this is not the case, because suppression of the AβPP proteolytic pathway at symptomatic stages of the disease in human trials had no effect whatsoever on the progression of AD [95, 96], consistent with the autonomous operation of the AD Engine. Blue and red arched arrows: Mutually propagating feedback cycles constituting an autonomous, self-perpetuating Engine that drives AD. One interesting and plausible special case of the generalized ACH2.0 is that of sX = (iAβ produced in the AβPP-independent pathway), where differentially derived iAβ runs both stages of AD. Crucially, iAβ produced independently of AβPP can be distinguished from that derived in the AβPP proteolysis, as described in the “Validation” section below. Confirmation of the occurrence of a type of iAβ originating independently of AβPP would equate it with and unequivocally establish the identity of sX.
![The generalized Amyloid Cascade Hypothesis 2.0 and the Engine that drives AD. Left Box (highlighted in gray): Life-long accumulation of AβPP-derived iAβ, through the cellular uptake of secreted peptide and intracellular retention of a fraction of AβPP-derived Aβ, to levels sufficient to ignite the AD “Engine” (rest of the figure). Middle Box: Several pathways, both actual (top two) and hypothetical (each line represent a pathway), of the Aβ-mediated elicitation of the integrated stress response or of yet unknown process capable of activating the cell-deleterious substance X (sX)-generating pathway. Top Box (highlighted in blue): Generation of intraneuronally retained sX. The yet to be determined sX is presumed to be capable of (a) anchoring a cascade that includes tau pathology and leads to neuronal death and (b) sustaining the activity of one or more pathways listed in the Middle Box, and thus perpetuating the feedback cycles and its own production. Right Box: sX rapidly accumulates intraneuronally; this sustains the operation of one or more of the AβPP-derived iAβ-mediated pathways shown in the Middle Box, which, in turn, support the generation of sX. It could be argued that the requirement that sX supports its own production is redundant in view of the continuous influx of AβPP-derived iAβ. However, this is not the case, because suppression of the AβPP proteolytic pathway at symptomatic stages of the disease in human trials had no effect whatsoever on the progression of AD [95, 96], consistent with the autonomous operation of the AD Engine. Blue and red arched arrows: Mutually propagating feedback cycles constituting an autonomous, self-perpetuating Engine that drives AD. One interesting and plausible special case of the generalized ACH2.0 is that of sX = (iAβ produced in the AβPP-independent pathway), where differentially derived iAβ runs both stages of AD. Crucially, iAβ produced independently of AβPP can be distinguished from that derived in the AβPP proteolysis, as described in the “Validation” section below. Confirmation of the occurrence of a type of iAβ originating independently of AβPP would equate it with and unequivocally establish the identity of sX.](https://content.iospress.com:443/media/adr/2023/7-1/adr-7-1-adr220079/adr-7-adr220079-g001.jpg)
1. AD is caused by Aβ, not tau; it is the overproduction of and mutations associated with the former that lead to tau pathology and the disease, but no other way around [97, 105].
2. There is no good correlation between extracellular Aβ and the disease:
3. AβPP-derived Aβ is known to physiologically accumulate intraneuronally (summarized above, reviewed in [2]).
4. Factors facilitating AβPP-derived iAβ accumulation are associated with AD:
5. Mutations causing AD (or protecting from it) interfere with accumulation of iAβ:
(a) Swedish familial AD (FAD) mutation facilitates AβPP processing on internal membranes and increases the intraneuronal retention of AβPP-derived Aβ [41]
(b) Flemish FAD mutation increases iAβ levels by interfering with BACE2-mediated iAβ cleavage [106]
(c) Protective Icelandic AβPP mutation reduces iAβ levels via stimulation of iAβ cleavage by BACE1 [107, 108]
(d) PSEN FAD mutations that increase the production of Aβ42 thus facilitating its internalization [18]
(e) PSEN FAD mutations that facilitate gamma-cleavage on internal membranes thus increasing the intraneuronal retention of AβPP-derived Aβ [42].
6. There is a good correlation between levels of iAβ and the occurrence of AD markers [15, 31].
The apparent universality of the first AD stage, i.e., the notion that, regardless of the nature of a mechanism underlying the second AD stage, its moving force is uniformly AβPP-derived iAβ, implies that a preventive AD therapy targeting AβPP-derived iAβ would be equally effective in either ACH2.0 version if administered prior to the commencement of the second AD stage, as addressed in the “Therapeutic Options” section below.
Progression of AD in the frameworks of the special ACH2.0 case and the generalized ACH2.0
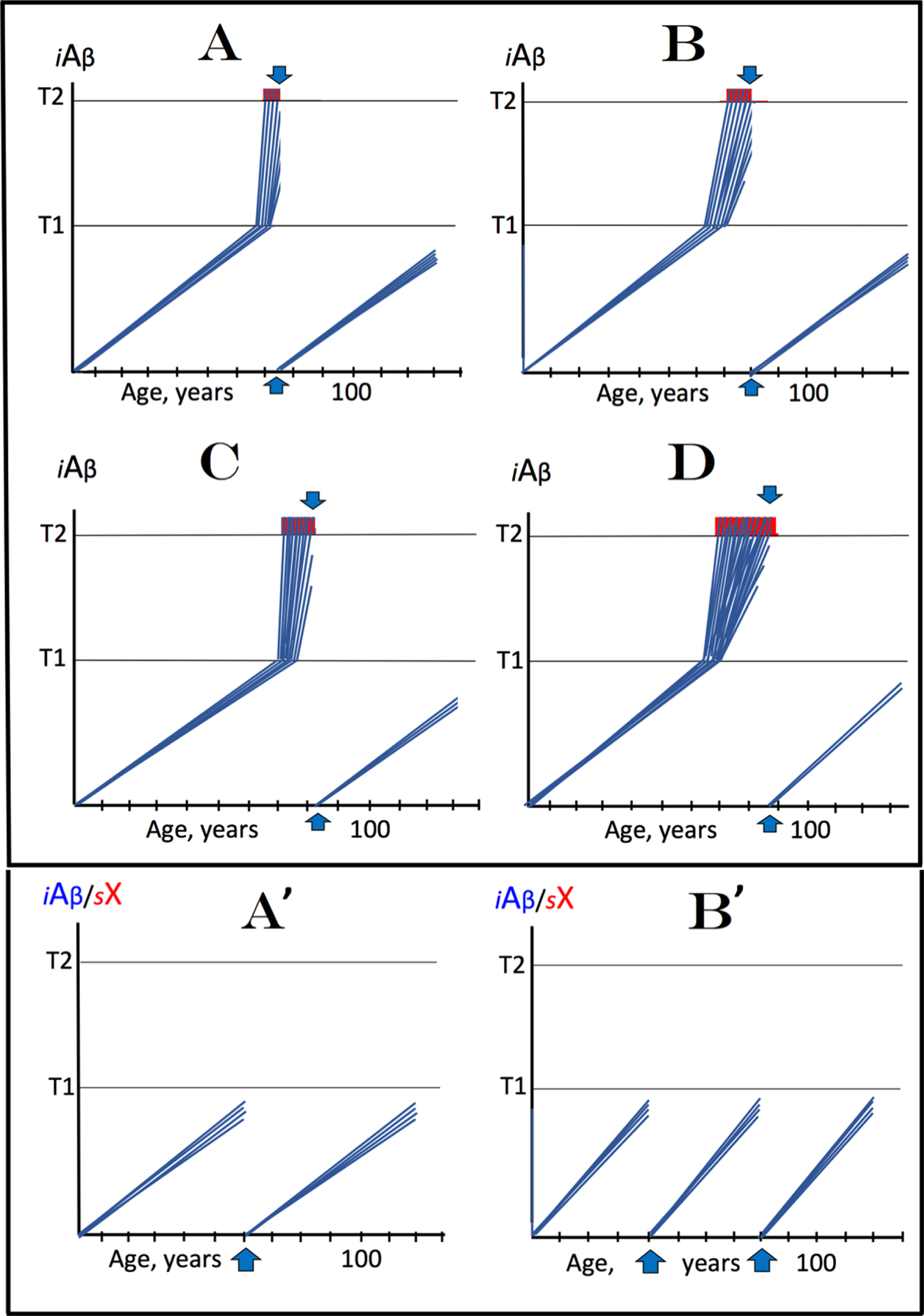
Dynamics of iAβ and sX accumulation in the affected neuronal population of an AD patient and the progression of the disease as envisioned in the special case of the ACH2.0 or in its generalized version are presented schematically in Fig. 2 (upper panels - special case; lower panels - generalized version). In both scenarios, in the first stage of the disease AβPP-derived iAβ steadily accumulates in a life-long process and its levels within the affected neurons reach the T1 threshold within a narrow temporal window [2]; no significant neurodegeneration occurs in this AD stage. At this point PKR and/or HRI kinases are activated and the second stage of AD commences. eIF2α is phosphorylated at the Ser51 and the ISR is elicited. In the special ACH2.0 case this leads to the activation of the AβPP-independent iAβ production pathway. iAβ accumulation substantially accelerates and neurodegeneration, including the formation of neurofibrillary tangles, accrues. Upon crossing the T2 threshold, neurons commit to the apoptotic pathway and eventually die. When enough cells become non-functional or die, AD symptoms manifest (Fig. 2A). With the progression of AD, additional neurons cross the T2 threshold until the disease reaches the end-stage (Fig. 2B).
Fig. 2
Dynamics of iAβ and/or sX accumulation in the affected neuronal population of an AD patient and progression of the disease. iAβ: Intraneuronal Aβ levels; sX: sX levels; T1: The level of AβPP = derived iAβ that triggers the elicitation of the ISR and activation of the AD Engine; T2: The level of iAβ or of sX that triggers cell’s commitment to the apoptotic pathway; Red blocks: Fraction of affected neurons either committed to apoptosis or dead; Vertical arrows: Indicate minimal fraction of neurons over the T2 threshold that causes symptomatic manifestation of AD. Blue lines: iAβ; Red lines: sX. Upper panels: Special ACH2.0 case with sX = (iAβ produced independently of AβPP). A) The initial symptomatic manifestation of the disease. The affected neurons reach and cross the T1 threshold within a narrow temporal window [2]; when the initial symptoms manifest, the T1 threshold has been crossed by and the AD Engine activated in all or the bulk of affected neuronal cells. B) Levels of iAβ cross the T2 threshold in a fraction of affected neurons (presumably all or most of affected neurons) sufficient to trigger the end-stage of the disease. Lower panels: ACH2.0 cases where sX is not iAβ. A’) The affected neurons cross the T1 threshold and activate the sX-generating pathway. When enough affected neurons cross the T2 threshold, AD symptoms manifest; by this time the sX production pathway has been initiated and the AD Engine activated in the bulk of affected neurons. B’) The end-stage of the disease. Note that in panels A’ and B’, the accumulation of iAβ and sX, shown above the T1 threshold, occurs in the same cells.
![Dynamics of iAβ and/or sX accumulation in the affected neuronal population of an AD patient and progression of the disease. iAβ: Intraneuronal Aβ levels; sX: sX levels; T1: The level of AβPP = derived iAβ that triggers the elicitation of the ISR and activation of the AD Engine; T2: The level of iAβ or of sX that triggers cell’s commitment to the apoptotic pathway; Red blocks: Fraction of affected neurons either committed to apoptosis or dead; Vertical arrows: Indicate minimal fraction of neurons over the T2 threshold that causes symptomatic manifestation of AD. Blue lines: iAβ; Red lines: sX. Upper panels: Special ACH2.0 case with sX = (iAβ produced independently of AβPP). A) The initial symptomatic manifestation of the disease. The affected neurons reach and cross the T1 threshold within a narrow temporal window [2]; when the initial symptoms manifest, the T1 threshold has been crossed by and the AD Engine activated in all or the bulk of affected neuronal cells. B) Levels of iAβ cross the T2 threshold in a fraction of affected neurons (presumably all or most of affected neurons) sufficient to trigger the end-stage of the disease. Lower panels: ACH2.0 cases where sX is not iAβ. A’) The affected neurons cross the T1 threshold and activate the sX-generating pathway. When enough affected neurons cross the T2 threshold, AD symptoms manifest; by this time the sX production pathway has been initiated and the AD Engine activated in the bulk of affected neurons. B’) The end-stage of the disease. Note that in panels A’ and B’, the accumulation of iAβ and sX, shown above the T1 threshold, occurs in the same cells.](https://content.iospress.com:443/media/adr/2023/7-1/adr-7-1-adr220079/adr-7-adr220079-g002.jpg)
In the generalized ACH2.0, the elicitation of the ISR leads to the activation of the sX-generating pathway and, when sX is not iAβ, to the same outcomes as discussed above, i.e., as sX accumulates, it initiates a cascade that includes tau-tangles, and neurodegeneration accrues. When enough neurons cross the T2 threshold and loose functionality, the disease reaches the symptomatic stage (Fig. 2A’); eventually more neurons cross the T2 threshold and the AD end-stage is reached (Fig. 2B’]. Importantly, in both ACH2.0 versions under discussion, by the time AD symptoms manifest, levels of AβPP-derived iAβ have crossed the T1 threshold and the AD Engine has been activated in bulk or all affected neurons; this notion is supported by experimental data [95, 96] and discussed in detail in [2].
THERAPEUTIC OPTIONS FOR AD IN THE GENERALIZED ACH2.0
The effectiveness of iAβ depletion therapy at symptomatic stages of AD in the special ACH2.0 case
It follows that by the time AD symptoms manifest, it is futile to target therapeutically the accumulation of the AβPP-derived iAβ because the self-sufficient AD Engine has been already activated in all affected neurons. At this stage, the only therapeutic option is to disable the Engine. In the special case of the ACH2.0 (sX = iAβ produced independently of AβPP), the best way to inactivate the AD Engine is to deplete iAβ to levels below those required for its activation and operation [2], the goal achievable by the activation of BACE1 and/or BACE2 and utilization of their Aβ-cleaving activities (reviewed in [2]). Importantly, iAβ depletion by any other suitable means would be as effective. The therapeutic effect of iAβ depletion treatment administered at various symptomatic stages of AD in the special case of ACH2.0 (when the disease is driven by iAβ produced in the AβPP-independent pathway) is illustrated schematically in panels A through D of Fig. 3. In this figure, it is assumed that the administration of BACE1 and/or BACE2 activator(s) (or the utilization of any suitable iAβ-depleting agent) for a limited, potentially short, duration is sufficient to completely, or nearly completely, deplete iAβ (derived in both, AβPP-dependent and –independent pathways), and that the rate of accumulation of AβPP-derived iAβ to the T1 level remains constant and linear both pre- and post-depletion treatment (additional possibilities are reviewed in [2]). In every case, the effect of the treatment would be a “RESET” of iAβ levels in surviving neurons. At this point, the de novo accumulation of AβPP-derived iAβ to the T1 threshold and the consequent activation of the AβPP-independent iAβ production pathway and of the AD Engine would require a substantial time, possibly decades, prior to the recurrence (or resumption of the progression) of the disease and may not occur in the remaining lifespan of an individual, at least in cases of sporadic AD. At the early symptomatic stages, when most of neurons are still viable (Fig. 3A), the treatment is expected to be curative; as the disease progresses and less and less affected neurons are redeemable, the treatment would stop the progression of AD but may not restore the lost cognitive functionality (Fig. 3B–D).
Fig. 3
Effect of the limited-duration iAβ depletion treatment, administered curatively or preventively, in AD. iAβ: Intraneuronal Aβ levels; sX: sX levels; T1: AβPP-derived iAβ level that triggers elicitation of the ISR and the activation of the AD Engine; T2: iAβ level that triggers cell’s commitment to the apoptotic pathway; Red blocks: Fraction of affected neurons committed to apoptosis or dead; Vertical arrows: Timing of the administration of iAβ depletion treatment; the drug is withdrawn after the complete or nearly complete depletion of iAβ is achieved. Upper panels (A–D): Treatments at different symptomatic stages in the special ACH2.0 case where sX = (iAβ produced independently of AβPP). A) The drug is administered at the early symptomatic stage of the disease. Levels of iAβ in surviving cells have been “reset” and the AD Engine switched off. The bulk of affected neurons, that did not yet reach the T2 threshold, recover and reconnect. At this point Aβ is produced only in the AβPP proteolytic pathway. The de novo accumulation of AβPP-derived iAβ resumes and, if its rate remains constant and linear pre- and post-treatment, iAβ levels are unlikely to reach the T1 threshold and the disease to recur within the remaining lifespan of an individual (at least in sporadic AD cases). B–D) The drug is administered at increasingly advanced stages of the disease. Outcomes are similar to that shown in panel A, except, as the disease progresses, there are less and less viable affected neurons that can be “reset” and thus redeemed. Lower panels: Preventive iAβ depletion therapy in the generalized ACH2.0. A’) Sporadic AD. The drug is administered in the early sixties; statistically prior to the late onset of the disease and before levels of AβPP-derived iAβ reach the T1 threshold in any neuronal cells. Levels of iAβ have been “reset”; the de novo accumulation of AβPP-derived iAβ to the T1 threshold would take decades and is unlikely to occur within the remaining lifespan of an individual. B’) Familial AD. The drug is administered in the early forties, and de-novo buildup of AβPP-derived iAβ to the T1 threshold could occur still within the lifespan of an individual; in such a case, a repeated administration of the drug could be required for the prevention of the disease. Note that the treatment (and its effects) depicted in A’ appear to be applicable to aging-related cognitive decline.
The effectiveness of iAβ depletion therapy at symptomatic stages of AD is conditional in the generalized ACH2.0
The iAβ depletion strategy at symptomatic stages may, however, not be effective in the generalized ACH2.0. It would, of course, work when sX = (iAβ produced in the AβPP-independent pathway) but this is the special ACH2.0 case discussed above. It would also work if the operation of the sX-producing pathway depends on sufficient levels of iAβ, by switching off the sX-generating pathway and necessitating a decades-long buildup of AβPP-derived iAβ to the T1 threshold. But whereas this type of dependency cannot be excluded, it can neither be expected, and in such a case the iAβ depletion therapy at symptomatic stages of AD would be inapplicable. Not only is iAβ depletion unlikely to work in this scenario, so is a potential depletion of sX (if it is feasible in the first place). Indeed, the sX depletion would be therapeutically ineffective because the continuous influx of AβPP-derived iAβ would keep the sX production pathway operative; an sX-depleting drug could possibly be helpful if administered unremittingly, but would certainly be inefficient as a short-duration agent; the elucidation of the nature of substance X and of the mechanism underlying the sX-generating pathway would, likely, suggest additional therapeutic options.
Prevention of AD: iAβ depletion therapy fully retains its protective effectiveness in the generalized ACH2.0
On the other hand, the limited-duration, potentially once-in-a-lifetime-only, iAβ depletion treatment constitutes, arguably, the ultimate preventive therapy for AD. This is true not only in the special ACH2.0 case but also within the framework of the generalized ACH2.0 because the preventive treatment is administered prior to the activation of the AD Engine (driven either by iAβ or sX) and to symptomatic manifestation of the disease, at the stage (the first stage of AD) when the only driving force is iAβ (AβPP-derived) that still did not reach the T1 threshold in any neurons. Moreover, the degree of certainty that the iAβ depletion treatment will be effective at this, pre-symptomatic, stage is much greater than that at the symptomatic AD stages in the special ACH2.0 case (see above). During the latter, the ability of neurons that crossed the T1, but have not yet reach the T2 threshold, to recover and reconnect following the disabling of the AD Engine would be inversely proportional to levels of iAβ (and the accompanying cellular damage) at the time of the treatment’s administration and could be compromised. There are no such uncertainties and limitations when this treatment is employed for the prevention of the disease, when no significant cellular damage yet occurred. With the complete or nearly complete depletion and “reset” of the iAβ levels and with the rate of accumulation of AβPP-derived iAβ to the T1 level remaining constant and linear both pre- and post-treatment (for additional discussion of these assumptions see [2]), one such treatment in a lifetime could be, if properly timed, i.e., close to but below the statistical age of the onset of symptomatic AD, sufficient to prevent the occurrence of the disease within the remaining lifespan of an individual. Since in prospective familial AD cases the iAβ build-up to the T1 threshold may plausibly occur within the remaining lifespan of an individual, the iAβ depletion treatment could have to be administered more than once. These scenarios are depicted in panels A’ and B’ of Fig. 3.
AGING-RELATED COGNITIVE DECLINE IN THE LIGHT OF THE ACH2.0: THE EXTENDED STAGE ONE OF AD? PROTECTIVE POTENTIAL OF lowercaseiAβ DEPLETION THERAPY
The Icelandic AβPP mutation A673T protects its carriers from AD [107, 108]. The protective effect is apparently due to the increased rate of BACE1 cleavage at residues 10/11 of Aβ (β’-site) and the consequent lowering of the rate of iAβ accumulation, effectively its depletion, within neuronal cells [107–112], precisely the therapeutic strategy proposed in the present study. The same mutation also protects from the “common” aging-associated cognitive decline [107, 108]. This is a striking observation. It implies that iAβ is somehow causatively involved in the aging-associated cognitive dysfunction. This could happen in two ways. The first one is that aging-related cognitive decline is, in fact, a “low grade”, location-restricted AD, i.e., it occurs only at particular brain locations, e.g., the anterior midcingulate cortex, associated with the retention of cognitive functionality in aging. The second, arguably more likely, explanation is that the T1 threshold is particularly low (and thus constitute an AD susceptibility factor) in AD-predisposed individuals who eventually develop the disease, while in the general population it is higher. Consequently, in the general population, AβPP-derived iAβ can accumulate (subject to the rate of its accumulation) with aging to higher (but still short of the T1 threshold) levels than in AD-predisposed individuals, sufficient to cause some neuronal damage and trigger aging-associated cognitive dysfunction but yet insufficient to ignite the AD Engine. In the framework of the ACH2.0, this description defines age-related cognitive decline as the extended first stage of AD (“extended” in terms of neurons’ augmented capacity to accumulate AβPP-derived iAβ prior to reaching the higher than in AD-predisposed individuals T1 threshold); in this scenario AβPP-derived iAβ plays the causative role in the age-related cognitive decline, just as it does in AD. The A673T mutation lowers the rate of accumulation of AβPP-derived iAβ (by facilitating its BACE1-mediated β’-site cleavage within Aβ) and it reaches neither the levels triggering aging-associated cognitive decline nor the T1 threshold (within the lifespan of a mutation carrier) thus protecting from both, aging-related cognitive dysfunction and AD. Whatever explanation is correct, a single administration of the iAβ depletion treatment, through the use of BACE1 and/or BACE2 activator(s) or via utilization of any other suitable iAβ-depleting agent, dispensed prior to the onset of the aging-related cognitive dysfunction (say, early sixties, same as for AD prevention) would prevent it, alongside with protecting from AD, by collapsing the iAβ population and necessitating its decades-long restoration as shown in panel A’ of Fig. 3. If the second explanation of iAβ role in aging-related cognitive decline were correct, the iAβ depletion treatment would also be curatively effective when administered after the cognitive dysfunction’s symptoms have manifested. If the first explanation were true, the iAβ depletion would work similarly at symptomatic stages of both AD and the age-related cognitive dysfunction; if effective at the former, it would be also effective at the latter.
VALIDATION OF THE GENERALIZED ACH2.0 AND OF THE lowercaseiAβ DEPLETION THERAPY FOR AD
Human neuronal cells-based AD model: Principles of design
For two reasons, the best conceivable AD model is, arguably, that based on human neuronal cells. The first reason is that such model utilizes cells originating from the species known to be affected by AD. The second reason is that AD appears to be human-specific or, at least, species-specific [2, 60, 61] (further discussed below), i.e., human cells seem to possess unique feature(s), such as the ability to produce iAβ in the AβPP-independent mode [60, 61] or enact some other mechanism(s) enabling the second AD stage, that are, because of the structure of their AβPP mRNA or for other reasons, unavailable in non-human mammalian species [53–59]. Since human neurons are intrinsically capable of molecular processes underlying the disease, the design principles to generate AD model are relatively straightforward: to trigger the second stage of AD and activate the AD Engine. Once this occurs, the progression of cellular AD pathology would become self-sustaining and irreversible (unless intervened with therapeutically). The most “physiological” (i.e., emulating processes occurring in the disease) method to ignite the Engine, i.e., to activate the endogenous AβPP-independent iAβ production or the sX-generating pathway, is to rapidly accumulate iAβ to the T1 threshold. This can be achieved by transiently supplying cells with exogenous iAβ42 either by importing the peptide or by expressing it from appropriate DNA constructs or from transfected mRNA. Considering that in AD-predisposed individuals the T1 threshold could be significantly lower than in general population, it may be useful to utilize neurons differentiated from iPSCs of AD patients. Alternative, albeit less “physiological”, approaches, which bypass the iAβ accumulation stage, include the induction of mitochondrial dysfunction resulting in the HRI activation, or stressor-specific activation of one of the other eIF2α kinases, all leading to the elicitation of the ISR and, provided that the ISR alone is sufficient to activate the AD Engine, the commencement of the second AD stage.
iAβ (produced in the AβPP-independent pathway) versus sX: Distinguishing between potential principal drivers of the second AD stage
If iAβ is indeed produced independently from AβPP in the second AD stage, it (and its immediate precursor) can be readily distinguished from Aβ and C99 generated by AβPP proteolysis. This is because in every conceivable mechanism of AβPP-independent iAβ production, translation is initiated from the AUG encoding Met671 of AβPP [2, 60, 61]. The resulting primary product, therefore, is not C99 but rather C100, i.e., Met-C99. The reason for this is that because Met671 is followed by Asp (Asp1 of C99 and of Aβ), it is removed by an aminopeptidase (other than MAP1 or MAP2) post- rather than co-translationally [113] (reviewed in [2]). Therefore, a steady-state pool of Met-C99 should be present in live cells with the activated AβPP-independent iAβ production pathway, and its detection would constitute a proof of the pathway’s operation (Met-Aβ would also be present, but its usage as a biomarker may limit or complicate the second AD stage induction options, as reviewed in [2]). If such proof were obtained, it would define the mechanism enabling the second AD stage. But what if it isn’t? In such case, the biomarker for the activity of the second AD stage would be tau-tangles, a “cellular symptom” of AD pathology. Indeed, the NFTs formation was observed (but its etiology apparently misinterpreted) in exogenous Aβ-overexpressing human neuronal cells [97] (reviewed in [2]), and it is expected to occur in the proposed AD model [2]. The detection of NFTs but not of C100 would indicate that the second AD stage is powered by the sX-producing pathway (where sX is not iAβ).
Testing therapeutic potential of the iAβ depletion
To assess the therapeutic potential of iAβ depletion, BACE1 and/or BACE2 can be exogenously overexpressed from either a constitutive or an inducible promoter (the latter to allow evaluation at the different mechanistic stages). Assaying options for the assessment of the effects and consequences of BACE overexpression would depend on the determination of the mechanism underlying operation of the AD Engine, as described in the preceding section. If this mechanism is the AβPP-independent iAβ production, the assaying could be extensive. It would include monitoring the levels of the intact iAβ (expected to be reduced by Aβ-cleaving activities of BACE1 and BACE2) and testing the activity of the AβPP-independent iAβ production pathway by examining for the presence of C100 (Met-C99). If the iAβ depletion were successful, the AD Engine’s operation would cease. Consequently, C100 influx would stop and it would dissipate (this is why it cannot be present in postmortem samples: in dying neurons, C100 influx would cease while aminopeptidases are still operational); thus the occurrence of C100, or lack thereof, would report on the activity of the AβPP-independent pathway of its production. If, on the other hand, the second AD stage is driven by the sX-generating pathway (where sX is not iAβ), presently, assaying options are limited to determining levels of the intact iAβ and to monitoring hyperphosphorylation of tau and formation of NFTs; in any case, the effects of the proposed therapy could be quantified.
DISCUSSION AND CONCLUSION
In the present study, AD is envisioned as a two-stage disease. The first, relatively benign, stage is driven by the life-long accumulation of AβPP-derived iAβ, which, upon reaching the T1 threshold, activates a self-perpetuating mechanism (the AD Engine) that drives the devastating second AD stage, which culminates in neuronal loss. The susceptibility to AD is, therefore, determined by the rate of AβPP-derived iAβ accumulation combined with the extent of the T1 threshold. The mechanism underlying the second AD stage appears to be species-specific, possibly human-specific. It is inoperative in mice, which explains the inadequacy of all current mouse AD models. The above scenario constitutes the recently proposed amyloid cascade hypothesis 2.0 [2]. In this scenario, the second AD stage-enabling mechanism was initially suggested to be the AβPP-independent iAβ production [2]; i.e., the entire course of the disease is run by differentially derived iAβ. A recent work by Brewer et al. [116] proposed a modified amyloid hypothesis suggesting that the intraneuronal Aβ contains “long” Aβ species Aβ45 and Aβ49, due to incomplete activity of gamma-secretases in AD mice. Brewer et al. hypothesized that Aβ45 aggregates inside neurons and are not secreted. It was shown that iAβ contains long Aβ45 and its accumulation in mitochondria, endosomes, and autophagosomes is dramatically increased with aging [116]. It is tempting to speculate that the sX species proposed in generalized ACH 2.0 could be the “long” Aβ species that is produced independently of AβPP and accumulates in neurons causing mitochondrial dysfunction.
It was recently proposed [114, 115] that high levels (over 800 pg/ml) of extracellular soluble Aβ42 protect from AD. Indeed, in numerous studies where this parameter was measured [95, 96, 114], it was shown to be well below 800 pg/ml in AD patients, and PET brain scan-positive individuals with excessive Aβ deposition were shown to retain normal cognition above this threshold but to develop mild cognitive impairment or AD below it [114]. Mechanisms of protection from AD conferred by high levels of extracellular soluble Aβ42 remain unknown; it may interfere, for example, with the rate of accumulation of iAβ by lowering it and thus preventing or delaying iAβ from reaching the T1 threshold within the lifespan of an individual. These results, if correct, suggest that low levels of extracellular soluble Aβ42 are a precondition for development of the disease. This phenomenon, however, remains to be corroborated and its apparent inconsistence with the overproduction and, consequently, with increased extracellular levels of Aβ42 in multiple types of FAD needs to be explained. On the other hand, it should be emphasized that the above notion affects neither the concepts of the ACH2.0 nor therapeutic strategies suggested by it.
The present study generalizes the previously formulated ACH2.0 by allowing that, conceptually, the second stage of AD could be enabled by more than one deleterious substance X-, sX-producing pathway. In this framework, the AβPP-independent iAβ-generating pathway is only the special, albeit, very plausible, case where sX = (iAβ produced independently from AβPP). In this special ACH2.0 case, the iAβ-depleting therapeutic strategy would be effective at the symptomatic stages of AD, whereas in the generalized ACH2.0 there is no certainty in this respect if sX is not iAβ. There is, however, a substantial certainty that a single administration of the iAβ-depleting treatment by activator(s) of BACE1 and/or BACE2, exploiting their Aβ-cleaving activities (reviewed in [2]), or by any suitable iAβ-depleting agent would be decidedly effective in the prevention of the disease in any ACH2.0 version, a notion testable by the validation procedure described above. Proponents of the ACH have argued that candidate AD drugs that consistently failed in human trials could be, nevertheless, therapeutically effective; they just were administered too late. In the framework of the ACH2.0, these arguments are valid (however, for different reasons than those invoked in the ACH). Antibodies targeting extracellular Aβ thus suppressing its cellular uptake, and, especially, BACE1 inhibitors affecting the production of AβPP-derived Aβ and, by extension, both its intraneuronal retention and its uptake, if administered sufficiently early, would certainly delay the accumulation of AβPP-derived iAβ to the T1 levels and the initiation of the second, iAβ- (generated independently from AβPP) or sX-anchored stage (this is how the A673T mutation exerts its protective effect by suppressing, i.e., lowering the rate of, the accumulation of AβPP-derived iAβ); these drugs could even extend the duration of iAβ accumulation to the T1 threshold to that exceeding the remaining lifespan of an individual. Such drugs, however, would have only a preventive, but not curative effect; moreover, they would have to be administered unremittingly for the rest of a person’s lifespan. Moreover, if lowering soluble extracellular Aβ42 levels is detrimental as discussed above [114, 115], the ACH-based AD therapies would be inapplicable because the utilization of BACE inhibitors or Aβ antibodies would certainly lower levels of extracellular Aβ species including soluble Aβ42. On the other hand, the proposed iAβ depletion therapy would target only the intraneuronal Aβ population, would interfere with neither the production nor secretion of Ab, and would not affect extracellular levels of soluble Aβ42.
Therefore, considering the alternative, ACH-based AD therapies is not a good option. The proposed ACH2.0-based therapeutic strategy, a limited-duration, once-in-a-lifetime-only iAβ-depleting treatment for prevention and, potentially, cure of not only AD but also of the “common” aging-associated cognitive decline defined, in the context of the ACH2.0, as the extended first stage of AD, is, undoubtedly, a preferable solution.
ACKNOWLEDGMENTS
The authors are grateful to Dr. Bjorn R. Olsen (Harvard Medical School) for his support.
FUNDING
This study was supported by the National Institutes of Health (R21 GM056179; R01 AR036819).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCES
[1] | Hardy JA , Higgins GA ((1992) ) Alzheimer’s disease: The amyloid cascade hypothesis. Science 256: , 184–185. |
[2] | Volloch V , Rits-Volloch S ((2022) ) The Amyloid Cascade Hypothesis 2.0: On the possibility of once-in-a-lifetime-only treatment for prevention of Alzheimer’s disease and for its potential cure at symptomatic stages. J Alzheimers Dis Rep 6: , 369–399. |
[3] | Casas C , Sergeant N , Itier JM , Blanchard V , Wirths O , van der Kolk N , Vingtdeux V , van de Steeg E , Ret G , Canton T , Drobecq H , Clark A , Bonici B , Delacourte A , Benavides J , Schmitz C , Tremp G , Bayer TA , Benoit P , Pradier L ((2004) ) Massive CA1/2 neuronal loss with intraneuronal and N-terminal truncated Abeta42 accumulation in a novel Alzheimer transgenic model. Am J Pathol 165: , 1289–1300. |
[4] | Bayer TA , Wirths O ((2008) ) Review on the APP/PS1KI mouse model: Intraneuronal Abeta accumulation triggers opathy, neuron loss and working memory impairment. Genes Brain Behav 7: , 6–11 axon. |
[5] | Bayer TA , Breyhan H , Duan K , Rettig J , Wirths O ((2008) ) Intraneuronal beta-amyloid is a major risk factor–novel evidence from the APP/PS1KI mouse model. Neurodegener Dis 5: , 140–142. |
[6] | Wirths O , Breyhan H , Cynis H , Schilling S , Demuth HU , Bayer TA ((2009) ) Intraneuronal pyroglutamate-Abeta 3-42 triggers neurodegeneration and lethal neurological deficits in a transgenic mouse model. Acta Neuropathol 118: , 487–496. |
[7] | Christensen DZ , Bayer TA , Wirths O ((2010) ) Intracellular Abeta triggers neuron loss in the cholinergic system of the APP/PS1KI mouse model of Alzheimer’s disease. Neurobiol Aging 31: , 1153–1163. |
[8] | Christensen DZ , Schneider-Axmann T , Lucassen PJ , Bayer TA , Wirths O ((2010) ) Accumulation of intraneuronal Abeta correlates with ApoE4 genotype. Acta Neuropathol 119: , 555–566. |
[9] | Bayer TA , Wirths O ((2010) ) Intracellular accumulation of amyloid-Beta - a predictor for synaptic dysfunction and neuron loss in Alzheimer’s disease. Front Aging Neurosci 2: , 8. |
[10] | Bayer TA , Wirths O ((2011) ) Intraneuronal Abeta as a trigger for neuron loss: Can this be translated into human pathology? Biochem Soc Trans 39: , 857–861. |
[11] | Wirths O , Bayer TA ((2012) ) Intraneuronal Abeta accumulation and neurodegeneration: Lessons from transgenic models. Life Sci 91: , 1148–1152. |
[12] | Kumar S , Wirths O , Theil S , Gerth J , Bayer TA , Walter J ((2013) ) Early intraneuronal accumulation and increased aggregation of phosphorylated Abeta in a mouse model of Alzheimer’s disease. Acta Neuropathol 125: , 699–709. |
[13] | Ripoli C , Cocco S , Li Puma DD , Piacentini R , Mastrodonato A , Scala F , Puzzo D , D’Ascenzo M , Grassi C ((2014) ) Intracellular accumulation of amyloid-beta (Abeta) protein plays a major role in Abeta-induced alterations of glutamatergic synaptic transmission and plasticity. J Neurosci 34: , 12893–12903. |
[14] | Scala F , Fusco S , Ripoli C , Piacentini R , Li Puma DD , Spinelli M , Laezza F , Grassi C , D’Ascenzo M ((2015) ) Intraneuronal Abeta accumulation induces hippocampal neuron hyperexcitability through A-type K(+) current inhibition mediated by activation of caspases and GSK-3. Neurobiol Aging 36: , 886–900. |
[15] | Christensen DZ , Kraus SL , Flohr A , Cotel MC , Wirths O , Bayer TA ((2008) ) Transient intraneuronal Abeta rather than extracellular plaque pathology correlates with neuron loss in the frontal cortex of APP/PS1KI mice. Acta Neuropathol 116: , 647–655. |
[16] | Chafekar S , Baas F , Scheper W ((2008) ) Oligomer-specific amyloid-beta toxicity in cell models is mediated by selective uptake. Biochem Biophys Acta 9: , 523–531. |
[17] | Wesen E , Jeffries G , Dzebo M , Esbjorner M ((2017) ) Endocytic uptake of monomeric amyloid-peptides is clathrin- and dynamin-independent and results in selective accumulation of Abeta (1–42) compared to Abeta (1–40). Sci Rep 7: , 2021. |
[18] | Kumar-Singh S , Theuns J , Van Broeck B , Pirici D , Vennekens K , Corsmit E , Cruts M , Dermaut B , Wang R , Van Broeckhoven C ((2006) ) Mean age-of-onset of familial Alzheimer disease caused by presenilin mutations correlates with both increased Abeta42 and decreased Abeta40. Hum Mutat 27: , 686–695. |
[19] | Hu X , Crick SL , Bu G , Frieden C , Pappu RV , Lee JM ((2009) ) Amyloid seeds formed by cellular uptake, concentration, and aggregation of the amyloid-beta peptide. Proc Natl Acad Sci U S A 106: , 20324–20329. |
[20] | Yajima R , Tokutake T , Koyama A , Kasuga K , Tezuka T , Nishizawa M , Ikeuchi T ((2015) ) ApoE-isoform-dependent cellular uptake of amyloid-beta is mediated by lipoprotein receptor LR11/SorLA. Biochem Biophys Res Commun 456: , 482–488. |
[21] | Omtri RS , Davidson MW , Arumugam B , Poduslo JF , Kandimalla KK ((2012) ) Differences in the cellular uptake and intracellular itineraries of amyloid beta proteins 40 and 42: Ramifications for the Alzheimer’s drug discovery. Mol Pharm 9: , 1887. |
[22] | Bu G , Cam J , Zerbinatti C ((2006) ) LRP in amyloid-beta production and metabolism. Ann N Y Acad Sci 1086: , 35–53. |
[23] | Wang HY , Lee DH , D’Andrea MR , Peterson PA , Shank RP , Reitz AB ((2000) ) beta-Amyloid (1-42) binds to alpha 7 nicotinic acetylcholine receptor with high affinity. Implications for Alzheimer’s disease pathology. J Biol Chem 275: , 5626–5632. |
[24] | Nagele R , D’Andrea , M , Anderson , W , Wang H ((2002) ) Intracellular accumulation of Abeta 42 in neurons is facilitated by the alpha 7 nicotinic acetylcholine receptor in Alzheimer’s disease. Neuroscience 110: , 199–211. |
[25] | Oddo S , Caccamo A , Green KN , Liang K , Tran L , Chen Y , Leslie FM , LaFerla FM ((2005) ) Chronic nicotine administration exacerbates tau pathology in a transgenic model of Alzheimer’s disease. Proc Natl Acad Sci U S A 102: , 3046–3051. |
[26] | Yan SD , Chen X , Fu J , Chen M , Zhu H , Roher A , Slattery T , Zhao L , Nagashima M , Morser J , Migheli A , Nawroth P , Stern D , Schmidt AM ((1996) ) RAGE and amyloid-beta peptide neurotoxicity in Alzheimer’s disease. Nature 382: , 685–691. |
[27] | Sasaki N , Toki S , Chowei H , Saito T , Nakano N , Hayashi Y , Takeuchi M , Makita Z ((2001) ) Immunohistochemical distribution of the receptor for advanced glycation end products in neurons and astrocytes in Alzheimer’s disease. Brain Res 888: , 256–262. |
[28] | Deane R , Du Yan S , Submamaryan RK , LaRue B , Jovanovic S , Hogg E , Welch D , Manness L , Lin C , Yu J , Zhu H , Ghiso J , Frangione B , Stern A , Schmidt AM , Armstrong DL , Arnold B , Liliensiek B , Nawroth P , Hofman F , Kindy M , Stern D , Zlokovic B ((2003) ) RAGE mediates amyloid-beta peptide transport across the blood–brain barrier and accumulation in brain. Nat Med 9: , 907–913. |
[29] | Iribarren P , Zhou Y , Hu J , Le Y , Wang , J ((2005) ) Role of formyl peptide receptor-like 1 (FPRL1/FPR2) in mononuclear phagocyte responses in Alzheimer disease. Immunol Res 31: , 165–176. |
[30] | Snyder EM , Nong Y , Almeida CG , Paul S , Moran T , Choi EY , Nairn AC , Salter MW , Lombroso PJ , Gouras GK , Greengard P ((2005) ) Regulation of NMDA receptor trafficking by amyloid-beta. Nat Neurosci 8: , 1051–1058. |
[31] | LaFerla F , Green K , Oddo S ((2007) ) Intracellular amyloid-beta in Alzheimer’s disease. Nat Rev Neurosci 8: , 499–509. |
[32] | Kinoshita A , Fukumoto H , Shah T , Whelan CM , Irizarry MC , Hyman BT ((2003) ) Demonstration by FRET of BACE interaction with the amyloid precursor protein at the cell surface and in early endosomes. J Cell Sci 116: , 3339–3346. |
[33] | Xu H , Greengard P , Gandy S ((1995) ) Regulated formation of Golgi secretory vesicles containing Alzheimer beta-amyloid precursor protein. J Biol Chem 270: , 23243–23245. |
[34] | Mizuguchi M , Ikeda K , Kim S ((1992) ) Differential distribution of cellular forms of beta-amyloid precursor protein in murine glial cell cultures. Brain Res 584: , 219–225. |
[35] | Cook DG , Forman MS , Sung JC , Leight S , Kolson DL , Iwatsubo T , Lee VM , Doms RW ((1997) ) Alzheimer’s Abeta 42 is generated in the endoplasmic reticulum/intermediate compartment of NT2N cells. Nat Med 3: , 1021–1023. |
[36] | Hartmann T , Bieger SC , Brühl B , Tienari PJ , Ida N , Allsop D , Roberts GW , Masters CL , Dotti CG , Unsicker K , Beyreuther K ((1997) ) Distinct sites of intracellular production for Alzheimer’s disease Abeta 40/42 amyloid peptides. Nat Med 3: , 1016–1020. |
[37] | Wild-Bode C , Yamazaki T , Capell A , Leimer U , Steiner H , Ihara Y , Haass C ((1997) ) Intracellular generation and accumulation of amyloid beta-peptide terminating at amino acid 42. J Biol Chem 272: , 16085–16088. |
[38] | Lee SJ , Liyanage U , Bickel PE , Xia W , Lansbury PT Jr , Kosik KS ((1998) ) A detergent-insoluble membrane compartment contains Abeta in vivo. Nat Med 4: , 730–734. |
[39] | Skovronsky D , Doms R , Lee V ((1998) ) Detection of a novel intraneuronal pool of insoluble amyloid protein that accumulates with time in culture. J Cell Biol 141: , 1031–1039. |
[40] | Manczak M , Anekonda TS , Henson E , Park BS , Quinn J , Reddy PH ((2006) ) Mitochondria are a direct site of Abeta accumulation in Alzheimer’s disease neurons: Implications for free radical generation and oxidative damage in disease progression. Hum Mol Genet 15: , 1437–1449. |
[41] | Martin B , Schrader-Fischer G , Busciglio J , Duke M , Paganetti P , Yankner B ((1995) ) Intracellular accumulation of beta-amyloid in cells expressing the Swedish mutant amyloid precursor protein. J Biol Chem 270: , 26727–26730. |
[42] | Sannerud R , Esselens C , Ejsmont P , Mattera R , Rochin L , Tharkeshwar AK , De Baets G , De Wever V , Habets R , Baert V , Vermeire W , Michiels C , Groot AJ , Wouters R , Dillen K , Vints K , Baatsen P , Munck S , Derua R , Waelkens E , Basi GS , Mercken M , Vooijs M , Bollen M , Schymkowitz J , Rousseau F , Bonifacino JS , Van Niel G , De Strooper B , Annaert W ((2016) ) Restricted location of PSEN2/gamma-secretase determines substrate specificity and generates an intracellular Abeta pool. Cell 166: , 193–208. |
[43] | Pakos-Zebrucka K , Koryga I , Mnich K , Ljujic M , Samali A , Gorman AM ((2016) ) The integrated stress response. EMBO Rep 17: , 1374–1395. |
[44] | Ron D ((2002) ) Translational control in the endoplasmic reticulum stress response. J Clin Invest 110: , 1383–1388. |
[45] | Harding HP , Zhang Y , Zeng H , Novoa I , Lu PD , Calfon M , Sadri N , Yun C , Popko B , Paules R , Stojdl DF , Bell JC , Hettmann T , Leiden JM , Ron D ((2003) ) An integrated stress response regulates amino acid metabolism and resistance to oxidative stress. Mol Cell 11: , 619–633. |
[46] | Brostrom CO , Prostko CR , Kaufman RJ , Brostrom MA ((1996) ) Inhibition of translational initiation by activators of the glucose-regulated stress protein and heat shock protein stress response systems. Role of the interferon-inducible double-stranded RNA-activated eukaryotic initiation factor 2alpha kinase. J Biol Chem 271: , 24995–25002. |
[47] | Dever TE , Feng L , Wek RC , Hinnebusch AG ((1992) ) Phosphorylation of initiation factor 2 alpha by protein kinase GCN2 mediates gene-specific translational control of GCN4 in yeast. Cell 68: , 585–596. |
[48] | Wek RC , Jiang HY , Anthony TG ((2006) ) Coping with stress: eIF2 kinases and translational control. Biochem Soc Trans 34: , 7–11. |
[49] | Rzymski T , Milani M , Pike L , Buffa F , Mellor HR , Winchester L , Pires I , Hammond E , Ragoussis I , Harris AL ((2010) ) Regulation of autophagy by ATF4 in response to severe hypoxia. Oncogene 29: , 4424–4435. |
[50] | Ye J , Kumanova M , Hart LS , Sloane K , Zhang H , De Panis DN , Bobrovnikova-Marjon E , Diehl JA , Ron D , Koumenis C ((2010) ) The GCN2-ATF4 pathway is critical for tumour cell survival and proliferation in response to nutrient deprivation. EMBO J 29: , 2082–2096. |
[51] | Garcia MA , Meurs EF , Esteban M ((2007) ) The dsRNA protein kinase PKR: Virus and cell control. Biochimie 89: , 799–811. |
[52] | Harding HP , Zhang Y , Ron D ((1999) ) Protein translation and folding are coupled by an endoplasmic-reticulum-resident kinase. Nature 397: , 271–274. |
[53] | Volloch V ((2019) ) Protein-encoding RNA-to-RNA information transfer in mammalian cells: Principles of RNA-dependent mRNA amplification. Ann Integr Mol Med 1: , 1002. |
[54] | Rits S , Olsen B , Volloch V ((2019) ) Protein-encoding RNA to RNA information transfer in mammalian cells: RNA-dependent mRNA amplification. Identification of chimeric RNA intermediates and putative RNA end products. Ann Integr Mol Med 1: , 23–47. |
[55] | Volloch V , Rits S , Olsen B ((2019) ) RNA-dependent amplification of mammalian mRNA encoding extracellullar matrix proteins: Identification of chimeric RNA intermediates for 1alpha, 1beta, and 1gamma chains of laminin. Ann Integr Mol Med 1: , 48–60. |
[56] | Volloch V , Olsen B , Rits S ((2019) ) Precursor-independent overproduction of beta-amyloid in AD: Mitochondrial dysfunction as possible initiator of asymmetric RNA-dependent APP mRNA amplification. An engine that drives Alzheimer’s disease. Ann Integr Mol Med 1: , 61–74. |
[57] | Volloch V , Olsen B , Rits S ((2020) ) AD “Statin”: Alzheimer’s disorder is a “fast” disease preventable by therapeutic intervention initiated even late in life and reversible at the early stages. Ann Integr Mol Med 2: , 75–89. |
[58] | Volloch V , Olsen B , Rits S ((2020) ) Alzheimer’s disease is driven by intraneuronally retained beta-amyloid produced in the AD-specific, APP-independent pathway: Current perspective and experimental models for tomorrow. Ann Integr Mol Med 2: , 90–114. |
[59] | Volloch V , Olsen B , Rits S ((2020) ) Alzheimer’s disease prevention and treatment: Case for optimism. Ann Integr Mol Med 2: , 115–130. |
[60] | Volloch V , Rits-Volloch S ((2021) ) News from Mars: Two-tier paradox, intracellular PCR, chimeric junction shift, dark matter mRNA and other remarkable features of mammalian RNA-dependent mRNA amplification. Implications for Alzheimer’s disease, RNA-based vaccines and mRNA therapeutics. Ann Integr Mol Med 2: , 131–173. |
[61] | Volloch V , Rits-Volloch S ((2021) ) Alzheimer’s disease is driven by beta-amyloid generated in the amyloid precursor protein-independent pathway and retained intraneuronally: Research and therapeutic strategies in a new AD paradigm. Ann Integr Mol Med 2: , 1010. |
[62] | Chang RC , Suen KC , Ma CH , Elyaman W , Ng HK , Hugon J ((2002) ) Involvement of double-stranded RNA-dependent protein kinase and phosphorylation of eukaryotic initiation factor-2alpha in neuronal degeneration. J Neurochem 83: , 1215–1225. |
[63] | Peel AL ((2004) ) PKR activation in neurodegenerative disease. J Neuropathol Exp Neurol 63: , 97–105. |
[64] | Peel AL , Bredesen DE ((2003) ) Activation of the cell stress kinase PKR in Alzheimer’s disease and human amyloid precursor protein transgenic mice. Neurobiol Dis 14: , 52–62. |
[65] | Chang RC , Wong AK , Ng HK , Hugon J ((2002) ) Phosphorylation of eukaryotic initiation factor-2alpha (eIF2alpha) is associated with neuronal degeneration in Alzheimer’s disease. Neuroreport 13: , 2429–2432. |
[66] | Onuki R , Bando Y , Suyama E , Katayama T , Kawasaki H , Baba T , Tohyama M , Taira K ((2004) ) An RNA- dependent protein kinase is involved in tunicamycin-induced apoptosis and Alzheimer’s disease. EMBO J 23: , 959–968. |
[67] | Lourenco MV , Clarke JR , Frozza RL , Bomfim TR , Forny-Germano L , Batista AF , Sathler LB , Brito-Moreira J , Amaral OB , Silva CA , Freitas-Correa L , Espirito-Santo S , Campello-Costa P , Houzel JC , Klein WL , Holscher C , Carvalheira JB , Silva AM , Velloso LA , Munoz DP , Ferreira ST , De Felice FG ((2013) ) TNF-alpha mediates PKR- dependent memory impairment and brain IRS-1 inhibition induced by Alzheimer’s beta-amyloid oligomers in mice and monkeys. Cell Metab 18: , 831–843. |
[68] | Paquet C , Mouton-Liger F , Meurs EF , Mazot P , Bouras C , Pradier L , Gray F , Hugon J ((2012) ) The PKR activator PACT is induced by Abeta: Involvement in Alzheimer’s disease. Brain Pathol 22: , 219–229. |
[69] | Guo X , Aviles G , Liu Y , Tian R , Unger BA , Lin YT , Wiita AP , Xu K , Correia MA , Kampmann M ((2020) ) Mitochondrial stress is relayed to the cytosol by an OMA1-DELE1-HRI pathway. Nature 579: , 427–432. |
[70] | Fessler E , Eckl EM , Schmitt S , Mancilla IA , Meyer-Bender MF , Hanf M , Philippou-Massier J , Krebs S , Zischka H , Jae LT ((2020) ) A pathway coordinated by DELE1 relays mitochondrial stress to the cytosol. Nature 579: , 433–437. |
[71] | Zhu X , Perry G , Moreira PI , Aliev G , Cash AD , Hirai K , Smith MA ((2006) ) Mitochondrial abnormalities and oxidative imbalance in Alzheimer disease. J Alzheimers Dis 9: , 147–153. |
[72] | Blass JP ((2000) ) The mitochondrial spiral. An adequate cause of dementia in the Alzheimer’s syndrome. Ann N Y Acad Sci 92: , 170–183. |
[73] | Manczak M , Park BS , Jung Y , Reddy PH ((2004) ) Differential expression of oxidative phosphorylation genes in patients with Alzheimer’s disease: Implications for early mitochondrial dysfunction and oxidative damage. Neuromolecular Med 5: , 147–162. |
[74] | Qin W , Haroutunian V , Katsel P , Cardozo CP , Ho L , Buxbaum JD , Pasinetti GM ((2009) ) PGC-1alpha expression decreases in the Alzheimer disease brain as a function of dementia. Arch Neurol 66: , 352–361. |
[75] | Du H , Guo L , Yan S , Sosunov AA , McKhann GM , Yan SS ((2010) ) Early deficits in synaptic mitochondria in an Alzheimer’s disease mouse model. Proc Natl Acad Sci U S A 107: , 18670–18675. |
[76] | Lin MT , Simon DK , Ahn CH , Kim LM , Beal MF ((2002) ) High aggregate burden of somatic mtDNA point mutations in aging and Alzheimer’s disease brain. Hum Mol Genet 11: , 133–145. |
[77] | Calkins M , Manczak M , Mao P , Shirendeb U , Reddy PH ((2011) ) Impaired mitochondrial biogenesis, defective axonal transport of mitochondria, abnormal mitochondrial dynamics and synaptic degeneration in a mouse model of Alzheimer’s disease. Hum Mol Genet 20: , 4515–4529 . |
[78] | Anandatheerthavarada HK , Biswas G , Robin MA , Avadhani NG ((2003) ) Mitochondrial targeting and a novel transmembrane arrest of Alzheimer’s amyloid precursor protein impairs mitochondrial function in neuronal cells. J Cell Biol 161: , 41–54. |
[79] | Caspersen C , Wang N , Yao J , Sosunov A , Chen X , Lustbader JW , Xu HW , Stern D , McKhann G , Yan SD ((2005) ) Mitochondrial Abeta: A potential focal point for neuronal metabolic dysfunction in Alzheimer’s disease. FASEB J 19: , 2040–2041. |
[80] | Chen JX , Yan SS ((2010) ) Role of mitochondrial amyloidbeta in Alzheimer’s disease. J Alzheimers Dis 20: (Suppl 2), 569–578. |
[81] | Hansson Petersen CA , Alikhani N , Behbahani H , Wiehager B , Pavlov PF , Alafuzoff I , Leinonen V , Ito A , Winblad B , Glaser E , Ankarcrona M ((2008) ) The amyloid beta-peptide is imported into mitochondria via the TOM import machinery and localized to mitochondrial cristae. Proc Natl Acad Sci U S A 105: , 13145–13150. |
[82] | de la Monte SM , Luong T , Neely TR , Robinson D , Wands JR ((2000) ) Mitochondrial DNA damage as a mechanism of cell loss in Alzheimer’s disease. Lab Invest 80: , 1323–1335. |
[83] | Brooks WM , Lynch PJ , Ingle CC , Hatton A , Emson PC , Faull RL , Starkey MP ((2007) ) Gene expression profiles of metabolic enzyme transcripts in Alzheimer’s disease. Brain Res 1127: , 127–135. |
[84] | Wang X , Perry G , Smith MA , Zhu X ((2007) ) Amyloid-beta-derived diffusible ligands cause impaired axonal transport of mitochondria in neurons. Neurodegener Dis 7: , 56–59. |
[85] | Wang X , Su B , Fujioka H , Zhu X ((2008) ) Dynamin-like protein 1 reduction underlies mitochondrial morphology and distribution abnormalities in fibroblasts from sporadic Alzheimer’s disease patients. Am J Pathol 173: , 470–482. |
[86] | Wang X , Su B , Lee HG , Li X , Perry G , Smith MA , Zhu X ((2009) ) Impaired balance of mitochondrial fission and fusion in Alzheimer’s disease. J Neurosci 29: , 9090–9103. |
[87] | Wang X , Su B , Siedlak SL , Moreira PI , Fujioka H , Wang Y , Casadesus G , Zhu X ((2008) ) Amyloid-beta overproduction causes abnormal mitochondrial dynamics via differential modulation of mitochondrial fission/fusion proteins. Proc Natl Acad Sci U S A 105: , 19318–19323. |
[88] | Volloch V ((1996) ) A mechanism for beta-amyloid overproduction in Alzheimer’s disease: Precursor-independent generation of beta-amyloid via antisense RNA-primed mRNA synthesis. FEBS Lett 390: , 124–128. |
[89] | Volloch V ((1997) ) Mechanism for beta-amyloid overproduction in sporadic Alzheimer’s disease: Possible antisense RNA-mediated generation of a 5’-truncated βAPP mRNA encoding 12 kDa C-terminal fragment of APP, the immediate precursor of Abeta. In Molecular Mechanisms of Dementia Wasco W, Tanzi R, eds. Springer Science+Business Media, New York, pp. 45–56 . |
[90] | Volloch V ((1997) ) Possible mechanism for resistance to Alzheimer’s disease (AD) in mice suggests new approach to generate a mouse model for sporadic AD and may explain familial resistance to AD in man. Exp Neurobiol 144: , 214–218. |
[91] | Almeida C , Takahashi , R , Gouras G ((2006) ) Beta-amyloid accumulation impairs multivesicular body sorting by inhibiting the ubiquitin–proteasome system. J Neurosci 26: , 4277–4288. |
[92] | Gregori L , Fuchs C , Figueiredo-Pereira M , Van Nostrand W , Goldgaber D ((1995) ) Amyloid-beta protein inhibits ubiquitin-dependent protein degradation in vitro. J Biol Chem 270: , 19702–19708. |
[93] | Oh S , Hong HS , Hwang E , Sim HJ , Lee W , Shin SJ , Mook-Jung I ((2005) ) Amyloid peptide attenuates the proteasome activity in neuronal cells. Mech Ageing Dev 126: , 1292–1299. |
[94] | Tseng B , Green K , Chan J , Blurton-Jones M , LaFerla F ((2008) ) Abeta inhibits the proteasome and enhances amyloid and tau accumulation. Neurobiol Aging 29: , 1607–1618. |
[95] | Egan MF , Kost J , Tariot PN , Aisen PS , Cummings JL , Vellas B , Sur C , Mukai Y , Voss T , Furtek C , Mahoney E , Harper Mozley L , Vandenberghe R , Mo Y , Michelson D ((2018) ) Randomized trials of verubecestat for mild-to-moderate Alzheimer’s disease. N Engl J Med 378: , 1691–1703. |
[96] | Egan MF , Kost J , Voss T , Mukai Y , Aisen PS , Cummings JL , Tariot PN , Vellas B , van Dyck CH , Boada M , Zhang Y , Li W , Furtek C , Mahoney E , Harper Mozley L , Mo Y , Sur C , Michelson D ((2019) ) Randomized trial of verubecestat for prodromal Alzheimer’s disease. N Engl J Med 380: , 1408–1420. |
[97] | Choi SH , Kim YH , Hebisch M , Sliwinski C , Lee S , D’Avanzo C , Chen H , Hooli B , Asselin C , Muffat J , Klee JB , Zhang C , Wainger BJ , Peitz M , Kovacs DM , Woolf CJ , Wagner SL , Tanzi RE , Kim DY ((2014) ) A three-dimensional human neural cell culture model of Alzheimer’s disease. Nature 515: , 274–278. |
[98] | Katzman R , Terry R , DeTeresa R , Brown T , Davies P , Fuld P , Rebing X , Peck A ((1988) ) Clinical, pathological, and neurochemical changes in dementia: A subgroup with preserved mental status and numerous neocortical plaques. Ann Neurol 23: , 138–144. |
[99] | Delaere P , Duyckaerts C , Masters C , Beyreuther K , Piette F , Hauw J ((1990) ) Large amounts of neocortical beta A4 deposits without neuritic plaques nor tangles in a psychometrically assessed, non-demented person. Neurosci Lett 116: , 87–93. |
[100] | Dickson D , Crystal H , Mattiace L , Masur D , Blau A , Davies P , Yen S , Aronson M ((1992) ) Identification of normal and pathological aging in prospectively studied nondemented elderly humans. Neurobiol Aging 13: , 178–189. |
[101] | Aizenstein H , Nebes R , Saxton J , Price J , Mathis C , Tsopelas N , Ziolko S , James J , Snitz B , Houck P , Bi W , Cohen A , Lopresti B , DeKosky S , Halligan E , Klunk W ((2008) ) Frequent amyloid deposition without significant cognitive impairment among the elderly. Arch Neurol 65: , 1509–1517. |
[102] | Klunk W , Mathis C , Price J , DeKosky S , Lopresti B , Tsopelas N , Saxton J , Nebes R ((2009) ) Amyloid imaging with PET in Alzheimer’s disease, mild cognitive impairment, and clinically unimpaired subjects. In PET in the Evaluation of Alzheimer’s Disease and Related Disorders ’ Silverman D, ed. Springer, New York pp. 119–147. |
[103] | Villemagne V , Pike K , Chetelat G , Ellis K , Mulligan R , Bourgeat P , Ackermann U , Jones G , Szoeke C , Salvado O , Martins R , O’Keefe G , Mathis C.A , Klunk W , Ames D , Masters C , Rowe C ((2011) ) Longitudinal assessment of Abeta and cognition in aging and Alzheimer disease. Ann Neurol 69: , 181–192. |
[104] | Seto M , Weiner RL , Dumitrescu L , Hohman TJ ((2021) ) Protective genes and pathways in Alzheimer’s disease: Moving towards precision interventions. Mol Neurodegen 16: , 29. |
[105] | Makin S ((2018) ) The amyloid hypothesis on trial. Nature 559: , S4–S7. |
[106] | Farzan M , Schnitzler CE , Vasilieva N , Leung D , Choe H ((2000) ) BACE2, a beta-secretase homolog, cleaves at the site and within the amyloid- region of the amyloid- precursor protein. Proc Natl Acad Sci U S A 97: , 9712–9717. |
[107] | Jonsson T , Atwal JK , Steinberg S , Snaedal J , Jonsson PV , Bjornsson S , Stefansson H , Sulem P , Gudbjartsson D , Maloney J , Hoyte K , Gustafson A , Liu Y , Lu Y , Bhangale T , Graham RR , Huttenlocher J , Bjornsdottir G , Andreassen OA , Jonsson EG , Palotie A , Behrens TW , Magnusson OT , Kong A , Thorsteinsdottir U , Watts RJ , Stefansson K ((2012) ) A mutation in APP protects against Alzheimer’s disease and age-related cognitive decline. Nature 488: , 96–99. |
[108] | Harper AR , Nayee S , Topol EJ ((2015) ) Protective alleles and modifier variants in human health and disease. Nat Rev Genet 16: , 689–701. |
[109] | Huse J , Liu K , Pijak D , Carlin D , Lee V Doms R ((2002) ) Beta-secretase processing in the trans-Golgi network preferentially generates truncated amyloid species that accumulate in Alzheimer’s disease brain. J Biol Chem 277: , 16278–16284. |
[110] | Liu K , Doms R , Lee M ((2002) ) Glu11 site cleavage and N-terminally truncated Abeta production upon BACE overexpression. Biochemistry 41: , 3128–3136. |
[111] | Lee EB , Zhang B , Liu K , Greenbaum EA , Doms RW , Trojanowski JQ , Lee VM ((2005) ) BACE overexpression alters the subcellular processing of APP and inhibits Abeta deposition in vivo. J Cell Biol 168: , 291–302. |
[112] | Kimura A , Hata S , Suzuki T ((2016) ) Alternative selection of beta-site APP-cleaving enzyme 1 (BACE1) cleavage sites in amyloid beta-protein precursor (APP) harboring protective and pathogenic mutations within the Abeta sequence. J Biol Chem 291: , 24041–24053. |
[113] | Wingfield P ((2017) ) N-terminal methionine processing. Curr Protoc Protein Sci 88: , 6.14.1-6.14.3. |
[114] | Sturchio A , Dwivedi AK , Young CB , Malm T , Marsili L , Sharma JS , Mahajan A , Hill EJ , Andaloussi SE , Poston KL , Manfredsson FP , Schneider LS , Ezzat K , Espay AJ ((2021) ) High cerebrospinal amyloid-β 42 is associated with normal cognition in individuals with brain amyloidosis. EClinicalMedicine 38: , 100988. |
[115] | Espay AJ , Sturchio A , Schneider LS , Ezzat K ((2021) ) Soluble amyloid-β consumption in Alzheimer’s disease. J Alzheimers Dis 82: , 1403–1415. |
[116] | Brewer G , Herrera R , Philipp S , Sosna J , Reyes-Ruiz J , Glabe C ((2020) ) Age-related intraneuronal aggregation of amyloid-β in endosomes, mitochondria, autophagosomes, and lysosomes. J Alzheimers Dis 73: , 229–246. |


