
Psychiatric and Psychosocial Characteristics of a Cohort of Spanish Individuals Attending Genetic Counseling Due to Risk for Genetically Conditioned Dementia
Abstract
Background:
Predictive genetic tests are presently effective over several medical conditions, increasing the demand among patients and healthy individuals. Considering the psychological burden suspected familial dementia may carry on individuals, assessing personality, coping strategies, and mental health could aid clinicians in findings the appropriate time for delivering genetic test results and predict compliance regarding genetic counseling and expectations towards the genetic condition depending on the outcome.
Objective:
To describe the psychiatric, psychological, and coping characteristics of a sample of Spanish individuals at risk of familial dementia before genetic test results were given.
Methods:
We included 54 first degree relatives of patients diagnosed with Alzheimer’s disease, lobar frontotemporal degeneration, or prion diseases. The NEO-FFI-R, COPE, and HADS tests evaluated personality, coping strategies, and psychological distress, respectively.
Results:
Anxiety and depression were below the cut-off point for mild severity. Conscientiousness and Agreeableness were the most preponderant personality factors, while Neuroticism was the least. Positive reinterpretation and Acceptance were the most frequent coping strategies, and Denial and Alcohol and drug use were the least used. Ongoing medical pathologies increased depression, while psychiatric disorders worsened psychological distress.
Conclusion:
Contrary to our expectations, PICOGEN candidates showed psychological distress and personality traits within normative ranges, and the use of problem-focused coping strategies prevailed over avoidance coping strategies. Nevertheless, clinicians should pay particular attention to individuals attending genetic counseling who are women, aged, and present an ongoing psychiatric disorder and psychiatric history at inclusion to ensure their mental health and adherence throughout the process.
INTRODUCTION
Dementia is a severe and chronic neurodegenerative syndrome that constitutes impairment in memory and at least one other cognitive domain, including personality, praxis, abstract thinking, and visuospatial skills [1]. Altogether, the neurocognitive disparities associated with dementia interfere thoroughly with the daily functional living activities, entailing a major decrease from the previous level of functioning and leading to new psychiatric comorbidities while exacerbating the existing ones [2–4].
While most dementia cases manifest at a late age and are not genetically determined, genetic factors play a predisposing role in the onset of the neurodegenerative disorder [5]. Furthermore, in most age-related dementias, genetic factors are crucial to the onset of the disease [6]. In this regard, literature shows that nearly 1% of all neurodegenerative dementia cases are genetically determined due to a mutation in a gene involved in the pathogenesis of the disease and are inherited in an autosomal dominant pattern [7].
For instance, in the case of Alzheimer’s disease (AD), early-onset (before the age of 60) of this neurodegenerative disorder accounts for 1–6% of all cases, of which 60% are familial with an autosomal dominant inheritance of 13% [7, 8]. In this latter group, mutations in the genes for presenilin-1 (PSEN1), presenilin-2 (PSEN2), or amyloid protein precursor (APP) are known to be involved in the early onset of the disease, representing no more than 0.1% of the total clinical AD cases [8]. In the case of lobar frontotemporal degeneration (FTLD), considered the third cause of neurodegenerative dementia, between 5 and 10% of the cases are caused by mutations in the genes for tau (MAPT) or progranulin (PGRN) proteins [7, 9]. Similarly, 10 to 15% of human prion diseases, also named transmissible spongiform encephalopathies (TSEs), are due to mutations in the prion protein gene (PRNP), affecting approximately 1–2 persons per million worldwide annually [10–12].
The detection of a genetic cause in the development of familial early-onset dementia has, nevertheless, immediate repercussions [5]. On the one hand, it places individuals and their closest relatives at risk of developing the same disease in the future. Consequently, this might lead to unintended psychological and psychiatric disparities given the broad range of long-term implications associated with the neurodegenerative disorder [12–15]. On the other hand, detecting a genetic cause also offers the possibility of establishing a comprehensive advising plan to help individuals involved in the familial dementia scenario understand the nature of the neurodegenerative disorder, its transmission, and the appropriate management options. In this regard, genetic counseling is the process whereby reduce guilt, shame, and stigma associated with the neurodegenerative disorder, maintaining optimal mental health levels throughout the process, and guiding individuals through any decision-making regarding genetic testing or family planning, respecting at all times the autonomy of the individuals involved in the disease [13, 16].
Although genetic counseling could increase the individual’s distress regarding the neurodegenerative disorder [13], early research shows that assessing personality, anxiety, and depression (i.e., psychological distress) and coping strategies could help clinicians determine the most convenient timing for delivering genetic test results and predicting adherence to the program and expectations towards the genetic outcome [17–19]. In other words, the psychiatric and psychological evaluation, together with the fact of providing concise information regarding the neurodegenerative disorder and addressing psychological distress and other mental health comorbidities, especially in the event of being positive for the disease, places genetic counseling as a crucial process for dealing with the genetic condition while ensuring the better well-being of those affected and at risk of developing age-related dementia [17, 20].
The current study aimed to describe the psychiatric and psychological characteristics of a sample of Spanish individuals attending genetic counseling due to possible AD, FTLD, or prion diseases genetically determined to shed light on their personality, anxiety and depression levels, and coping strategies.
MATERIAL AND METHODS
Design
A cross-sectional and descriptive study with Spanish first-degree relatives of patients diagnosed with familial AD, FTLD, or prion diseases suspected of suffering from the same genetically determined neurodegenerative diseases.
All study procedures complied with the Helsinki declaration and received the approval of the Ethics Committee Board of the Hospital Clinic of Barcelona (HCP).
Setting and participants
This study was carried out at the Alzheimer’s and other cognitive disorders Unit (HCP), where a specific multidisciplinary (i.e., neurologists, psychiatrists, psychologists) genetic counseling consultation in the field of neurodegenerative dementias was set (PICOGEN program) between the years 2001 and 2008 [5].
Local media coverage of the PICOGEN program meant that most individuals requested a visit themselves. The rest of the individuals were recruited from the Alzheimer’s and other cognitive disorders Unit (HPC) or were referrals made by neurologists from other centers.
The inclusion criteria were to be 18 years of age or more and have at least one family member with early-onset AD (under 58 years of age) or a neuropathological study suggesting the genetic origin of the same condition, the DLFT phenotype suggesting genetic susceptibility or the prion disease phenotype. Instead, individuals who presented with any of the following criteria were excluded from the study: severe medical or psychiatric pathology and an intellectual disability that would prevent them from answering all questionnaires independently and confirmed diagnosis of dementia.
Individuals who were considered not eligible for the genetic screening study, either because they did not meet the inclusion criteria or there were no biological samples available from affected individuals, received a general explanation of the genetic risk in their particular case and the non-indication for a specific study.
All individuals included in the study gave informed consent to participate and were evaluated by the same specialists following the protocol established in the same hospital [5].
Clinical assessment
Individuals who requested to participate in the PICOGEN program received a neurological assessment prior to the psychiatric and psychological evaluations. The neurological assessment was performed by senior neurologists (JM Molinuevo & R. Sánchez-Valle) from the Alzheimer’s and other cognitive disorders Unit (HCP) following a strict multidisciplinary protocol based on the guidelines for pre-symptomatic testing in Huntington’s disease. That is, neurologists performed a specific clinical examination of the main cognitive areas while focusing on detecting symptoms related to cognitive impairment. The multidisciplinary protocol has been further described in previous studies from our group and approved by the ethics committee board (HCP) [5, 14, 21].
The collection of sociodemographic data and psychiatric interviews were conducted by a senior psychiatrist (L. Pintor) from the Consultation and Liaison Psychiatry Unit (HCP). The interviews consisted, firstly, of explaining the purpose of the psychiatric and psychological consultation within the PICOGEN program. Next, the psychiatrist carried out psycho-biographical questions and analyzed the individual’s baseline level of knowledge concerning genetic counseling. Then, the session continued with exploring past and current psychopathological aspects. Finally, an explanation was given of the need to administer psychometric questionnaires to analyze specific psychological characteristics. In addition, further clarification was given on the objectives of the follow-up, continued help throughout the process, and joint decision-making with the multidisciplinary team to make them aware of the genetic test results.
After the psychiatric interview, a senior clinical psychologist (JM. Peri) applied and supervised the administration of self-administered psychometric questionnaires.
Assessment instruments
Individual differences were evaluated using the sociodemographic form. The sociodemographic form included age, gender, marital status, psychiatric history, and current medical (any non-severe medical pathology consisting of infectious, cardiovascular, gastrointestinal, or metabolic diseases) and psychiatric pathology at baseline.
The psychiatric interview was conducted according to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition: Axis I Disorders Clinical Version and Axis II Personality Disorders of the American Psychiatry Association [22].
Anxiety and depression symptoms were examined using the HADS test Spanish adapted version [23]. The HADS test is a 14 items psychometric tool. Seven items evaluate depression (HADS-D subscale), and the other seven evaluate anxiety (HADS-A subscale). Each item scores 0 to 3, with a recommended cut-off point in both subscales (HAD-A and HAD-D) of 8–10 for doubtful cases and ≥11 for definite cases.
Personality was assessed using the Spanish-adapted version of the NEO Personality Inventory-Revised (NEO-FFI-R) [24]. The NEO-FFI-R is a self-administered questionnaire based on the comprehensive model of general personality traits: the Five-Factor Model [25]. The NEO-FFI-R is an abbreviated version of the NEO-PI-R questionnaire (240 items assessing 5 personality dimensions with 30 specific facets, i.e., 6 for each dimension) [26] comprised of 60 items with a five-point Likert scale response format ("Strongly disagree” to “Strongly agree") that assess five main personality dimensions: Neuroticism (N), the tendency to experience negative emotions and psychological distress; Extraversion (E), the degree of sociability, positive emotionality, and general activity; Openness to experience (O), the levels of curiosity, independent judgment, and conservativeness; Agreeableness (A), the tendency to altruistic, sympathetic and cooperative actions; Conscientiousness (C), the degree of self-control when planning and organizing. As with the original version, the NEO-PI-R, the NEO-FFI-R inventory has proven to have adequate psychometric properties (validity and reliability) for its use in the Spanish population [27].
Coping strategies were examined using the Coping Orientation to Problems Experience inventory (COPE) [28]. The COPE inventory is a multidimensional 60-item self-reported test that evaluates 15 theoretically-based coping strategies on a 4-point Likert scale (“I never do this” to “I do this very often). High COPE punctuations indicate greater use of the strategies. The COPE coping strategies can be meaningfully grouped into three factorially-based dimensions: Engagement [E], Disengagement [D], and Help-seeking [HS] [29, 30]. The COPE coping strategies are: Active-coping [E], to take action to eliminate or decrease the problem or its consequences; Planning [E], to deliberate on how to handle the problem; Seeking instrumental support [HS], to seek advice or help from others; Suppression of competing activities [E], to put aside other activities not connected to the problem to better deal with it; Restraint [E], to wait for the right time to act towards the problem; Seeking emotional support [HS], to seek sympathy or understanding from others; Positive reinterpretation [E], to reframe the stressor In favorable terms; Turning to religion [D]; to use faith as support; Acceptance [E], to learn to accept the problem; Humor [*], to use humor to minimize the importance of the problem; Focus on and venting emotions [HS], to be concerned about own emotions and tendency to express them; Denial [D], to refuse to acknowledge the problem; Mental disengagement [D], to distract one-self from thinking of the problem; Behavior disengagement [D], abandonment of efforts to deal with the problem; Alcohol and drug disengagement [*], to use alcohol or drugs to reduce emotional distress.
Procedures
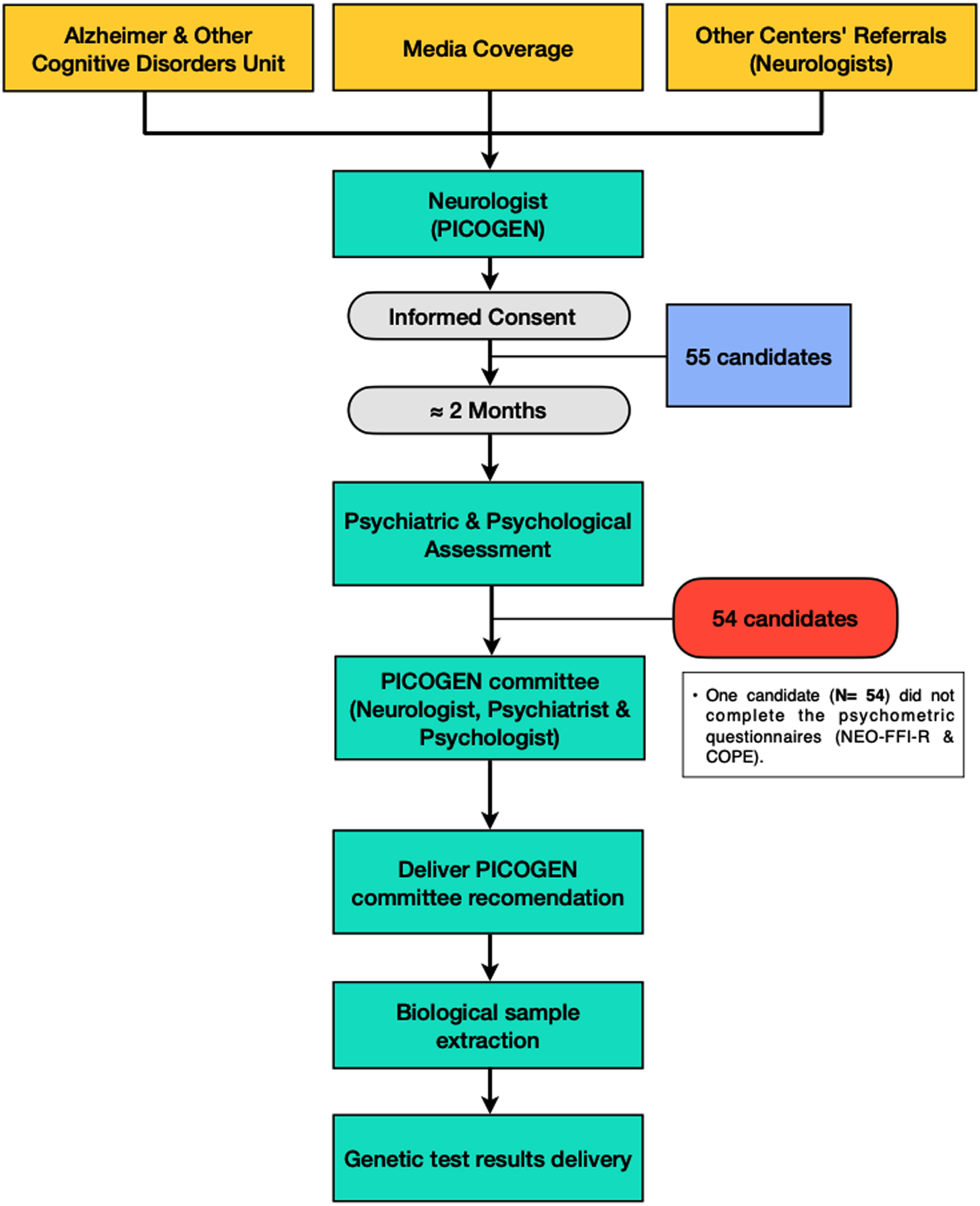
All PICOGEN candidates were recruited at the Alzheimer and other cognitive disorders Unit (HCP). The multidisciplinary research protocol consisted of the following stages (Fig. 1):
1. An initial visit with a neurologist to examine the clinical phenotype and familial transmission pattern, evaluate the presence or absence of symptoms, and inform the individual (asymptomatic or not) about the study protocol and risks of undergoing the genetic test. The first visit also included an in-depth explanation of the disease and its implications. According to the data collected during the first visit with the neurologist, individuals were invited to sign the informed consent to continue with the genetic study.
2. Individuals were given two months to consider the pros and cons of continuing the study. Then, whether individuals agreed to proceed with the study, they were scheduled with the psychiatrist for an interview. The psychiatric evaluation continued with a psychological assessment conducted by a clinical psychologist using anxiety, depression, personality, and coping strategies tests.
3. Following the psychiatric and psychological evaluation, the PICOGEN experts’ committee (i.e., neurologist, psychiatrist, and psychologist) evaluated the risk-benefit balance of the pre-symptomatic study in the individual. From the PICOGEN experts’ committee appraisal, a personalized recommendation on the safety of the genetic test and deliberation of the results was made to the individual. If an individual was not in optimal conditions (e.g., mental health impairment or high psychological distress) to be informed about the genetic test result, the psychiatric opinion prevailed to delay the results delivery until he or she showed better mental health after completing the recommended intervention. All this, respecting the autonomy and well-being of each PICOGEN candidate.
4. Hereafter, the PICOGEN expert’s committee recommendation was communicated to the individual, and only whether the individual finally agreed to proceed with the genetic study, a biological sample was taken. After approximately 14 days, or after accomplishing the recommended clinical intervention, individuals were already in optimal conditions, and unless they indicated otherwise, the genetic test results were communicated. Should the patient’s mental health condition require it after the genetic test results were delivered, referral to psychiatric outpatient services of the same hospital for further clinical intervention was advised.
Fig. 1
Flowchart of the PICOGEN study procedures.
Statistical analysis
Firstly, the variables’ distribution was analyzed, and a descriptive analysis was conducted. Then statistic tests were applied accordingly.
The Mann-Whitney U (non-parametric) test was used to compare differences between not normally distributed independent dichotomous variables. The non-parametric One-Way ANOVA (Kruskal-Wallis) was used instead when comparing multiple groups. Significance values were adjusted following the Bonferroni correction in the non-parametric pairwise comparisons (Dwass-Steel-Critchlow-Fligner: DSCF) to prevent Type I error.
The Pearson correlation coefficient (Pearson’s r) was also used to examine the correlation between anxiety and depression, personality factors and coping strategies, and anxiety and depression and personality factors and coping strategies.
Lastly, multiple regression models were fitted to examine the independent effects of several sociodemographic variables on PICOGEN candidates’ mental health based on the psychometric tests (i.e., HADS, NEO-FFI-R, and COPE) used in the quantitative psychiatric and psychological evaluation. Gender (women, men), age, marital status (married, not married), psychiatric history records (no, yes), medical pathology at baseline (no, yes), and psychiatric disorder at baseline (no, yes) were introduced in the initial model as predictors. The Backwards Elimination, in terms of the lowest AIC value, was used to fit the models.
Since some study variables had small subgroup sizes, for instance, psychiatric history and psychiatric pathology at baseline, these were unified to increase the statistical power and prevent Type I error in our analyses [31]. Furthermore, in group comparisons, the variable age was dichotomized according to whether the individuals’ age was far (22–44) or close (45–69) from the disease debut to analyze potential differences between these two groups [5, 32].
The RStudio version 1.3.1093 for Windows was used for all data analyses. All results were interpreted with a 95% confidence interval (CI) and a significance level (p-value) of 0.05.
RESULTS
Sociodemographic and clinical characteristics of the sample
A total of 55 individuals were recruited in the PICOGEN program. One individual with no psychiatric history nor psychiatric disorders at baseline was excluded from the analysis due to non-complete questionnaires. The clinical neurological screening did not reveal any PICOGEN candidate with cognitive impairment.
Table 1 shows the sociodemographic and clinical characteristics of the 54 individuals included in the final analysis. Almost 65% of the sample were women, married (61.1%) and without psychiatric history (74.1%), medical pathology (83.3%), and psychiatric disorder (68.52%) at baseline. The mean age was 41.40 (11.43) years.
Table 1
Sociodemographic and clinical characteristics of the sample
| N | Mean (S.D.) | |
| Age (y) | 54 | 41.4 (11.43) |
| % | ||
| Age (y, in groups) | ||
| 24–44 | 35 | 68.5 |
| 45–69 | 16 | 31.5 |
| Gender | ||
| Women | 35 | 64.8 |
| Men | 19 | 35.2 |
| Marital Status | ||
| Married | 33 | 61.1 |
| Not married | 21 | 38.9 |
| Psychiatric history records | ||
| None | 40 | 74.1 |
| Depression | 6 | 11.1 |
| Anxiety | 4 | 7.41 |
| Bipolar disorder | 2 | 3.7 |
| Psychosis | 1 | 1.85 |
| Drug addiction | 1 | 1.85 |
| Psychiatric history records | ||
| No | 40 | 74.1 |
| Yes | 14 | 25.9 |
| Medical pathology at baseline | ||
| No | 45 | 83.3 |
| Yes | 9 | 16.7 |
| Psychiatric disorder at baseline | ||
| None | 37 | 68.52 |
| Depression | 5 | 9.26 |
| Anxiety | 4 | 7.41 |
| Bipolar disorder | 3 | 5.56 |
| Psychosis | 2 | 3.70 |
| Drug addiction | 3 | 5.56 |
| Psychiatric disorder at baseline | ||
| No | 37 | 68.52 |
| Yes | 17 | 31.5 |
Anxiety and depression, coping strategies, and personality characteristics of the sample
Overall, the HAD-A and HAD-D subscale mean scores were below the cut-off point for doubtful cases (i.e., total subscale score from 8 to 10) of severe anxiety and depression, respectively. The most preponderant personality dimensions were Conscientiousness and Agreeableness, while Neuroticism was the least.
The coping strategies more frequent were Positive reinterpretation, Acceptance, and Planning. Instead, Behavioral disengagement, Denial, and Alcohol and drug use were the least prevalent. Engagement was the most distinctive coping dimension amongst PICOGEN candidates, while Disengagement was the least.
Further description of the sample’s anxiety and depression, personality, and coping characteristics is provided in Table 2.
Table 2
Anxiety, depression, coping, and personality characteristics of the sample
| Mean (S.D.) | Min | Max | |
| HADS scale | |||
| HAD-Anxiety | 6.29 (3.83) | 1.0 | 17.0 |
| HAD-Depression | 2.92 (3.92) | 0.0 | 18.0 |
| NEO-FFI-R inventory | |||
| Neuroticism | 18.9 (8.19) | 3.0 | 36.0 |
| Extraversion | 29.73 (6.11) | 16.0 | 44.0 |
| Openness to experience | 30.46 (6.45) | 16.0 | 46.0 |
| Agreeableness | 34.88 (6.66) | 19.0 | 46.0 |
| Conscientiousness | 36.02 (7.02) | 17.0 | 47.0 |
| COPE inventory - Subscales | |||
| Active coping [E] | 60.77 (17.73) | 0.0 | 83.0 |
| Planning [E] | 69.29 (19.62) | 17.0 | 100.0 |
| Seeking instrumental support [HS] | 64.6 (17.66) | 17.0 | 100.0 |
| Suppression of competing activities [E] | 43.73(17.39) | 0.0 | 83.0 |
| Restraint [E] | 55.35 (17.26) | 17.0 | 92.0 |
| Seeking emotional support [HS] | 58.02 (22.49) | 8.0 | 100.0 |
| Positive reinterpretation [E] | 73.9 (16.65) | 25.0 | 100.0 |
| Turning to religion [D] | 11.65 (20.41) | 0.0 | 100.0 |
| Acceptance [E] | 69.46 (18.78) | 17.0 | 100.0 |
| Humor [*] | 39.19 (27.93) | 0.0 | 100.0 |
| Focus on &venting emotions [HS] | 40.13 (23.91) | 0.0 | 92.0 |
| Denial [D] | 14.17 (13.77) | 0.0 | 50.0 |
| Mental disengagement [D] | 32.63 (20.5) | 0.0 | 75.0 |
| Behavioral disengagement [D] | 19.81 (16.75) | 0.0 | 67.0 |
| Alcohol &drug use [*] | 6.75 (18.8) | 0.0 | 100.0 |
| COPE inventory - Dimensions | |||
| Engagement [E] | 62.94 (13.37) | 21.0 | 99.5 |
| Disengagement [D] | 19.59 (10.92) | 0.0 | 48.0 |
| Help-seeking [HS] | 54.04 (16.33) | 11.0 | 94.3 |
Factors contributing to anxiety and depression, and personality differences across the sample
There were significant differences in psychological distress and personality characteristics depending on different study variables. Differences in anxiety, depression, and personality characteristics across the sample and level of significance are shown in Tables 3 and 4, respectively.
Regarding the HADS test, statistically significant differences were found in the HAD-D subscale according to the age group individuals were classified in and whether individuals had an ongoing medical pathology when recruited for the study (Table 3). Individuals aged 45 to 69 (U = 176.5, p = 0.032) and those with a medical illness (U = 98.00, p = 0.049) had statically significant more depression than those aged 22 to 44 and without a medical illness. Despite noticing the same trend for the HAD-A subscale, no statistically significant differences were found in anxiety between the age (U = 194.5, p = 0.083) or medical pathology (U = 236.5, p = 0.095) groups. When comparisons were performed depending on whether individuals presented a psychiatric disorder at baseline, results showed that those with a psychiatric disorder had statistically higher mean scores in the HAD-A (U = 143.5, p = 0.005) and HAD-D (U = 161, p = 0.013) subscales than those without a psychiatric disorder.
Table 3
Anxiety and depression differences across the sample
| HAD-Anxiety | HAD-Depression | |
| Mean (S.D.) | ||
| Gender | ||
| Women | 6.81 (3.95) | 3.03 (3.59) |
| Men | 5.42 (3.55) | 2.74 (4.53) |
| p | 0.200 | 0.259 |
| Age | ||
| 24 to 44 | 5.69 (3.64) | 1.91 (2.39) |
| 45 to 69 | 7.63 (4.01) | 5.13 (5.59) |
| p | 0.083 | 0.032 |
| Marital status | ||
| Married | 6.32 (3.66) | 3.10 (4.32) |
| Not married | 6.25 (4.17) | 2.65 (3.31) |
| p | 0.831 | 0.882 |
| Psychiatric history records | ||
| No | 6.05 (4.18) | 2.84 (3.72) |
| Yes | 6.93 (2.73) | 3.14 (4.57) |
| p | 0.143 | 0.649 |
| Medical pathology at baseline | ||
| No | 5.91 (3.68) | 2.61 (3.85) |
| Yes | 8.38 (4.21) | 4.63 (4.14) |
| p | 0.095 | 0.049 |
| Psychiatric disorder at baseline | ||
| No | 5.11 (2.62) | 1.63 (1.77) |
| Yes | 8.88 (4.79) | 5.75 (5.64) |
| p | 0.005 | 0.013 |
When it comes to the NEO-FFI-R results (Table 4), women had significantly higher mean scores in Neuroticism (U = 179, p = 0.014) than men (M = 15.33, 7.25). Women also had higher overall mean scores in Agreeableness (U = 215.5, p = 0.083) and Conscientiousness (U = 219, p = 0.095) than men, without finding statistical significance between the two groups.
Table 4
Personality differences across the sample
| Neuroticism | Extraversion | Openness to experience | Agreeableness | Conscientiousness | ||
| Mean (S.D.) | ||||||
| Gender | ||||||
| Women | 20.79 (8.12) | 29.68 (6.04) | 30.24 (6.16) | 36.03 (6.32) | 37.41 (6.17) | |
| Men | 15.33 (7.25) | 29.83 (6.41) | 30.89 (7.14) | 32.72 (6.94) | 33.39 (7.93) | |
| p | 0.014 | 0.977 | 0.931 | 0.83 | 0.095 | |
| Age | ||||||
| 24 to 44 | 17.70 (7.78) | 30.08 (6.53) | 30.05 (6.62) | 33.86 (6.98) | 35.30 (7.48) | |
| 45 to 69 | 21.87 (8.68) | 28.87 (5.03) | 31.47 (6.13) | 37.40 (5.21) | 37.80 (5.58) | |
| p | 0.060 | 0.517 | 0.270 | 0.097 | 0.352 | |
| Marital status | ||||||
| Married | 19.50 (8.77) | 30.53 (6.23) | 31.06 (6.78) | 35.00 (7.09) | 37.03 (6.77) | |
| Not married | 17.95 (7.27) | 28.45 (5.84) | 29.50 (5.93) | 34.70 (6.10) | 34.40 (7.29) | |
| p | 0.651 | 0.429 | 0.346 | 0.699 | 0.184 | |
| Psychiatric history records | ||||||
| No | 18.51 (8.45) | 30.15 (5.76) | 30.49 (6.55) | 35.28 (6.70) | 36.08 (7.12) | |
| Yes | 20.08 (7.55) | 28.46 (7.17) | 30.38 (6.41) | 33.69 (6.68) | 35.85 (6.99) | |
| p | 0.604 | 0.409 | 0.672 | 0.511 | 0.890 | |
| Medical pathology at baseline | ||||||
| No | 18.61 (8.16) | 29.57 (6.23) | 30.39 (6.68) | 34.80 (6.84) | 35.66 (7.17) | |
| Yes | 20.50 (8.80) | 30.63 (5.73) | 30.88 (5.44) | 35.38 (6.02) | 38.00 (5.19) | |
| p | 0.685 | 0.713 | 0.829 | 0.959 | 0.476 | |
| Psychiatric disorder at baseline | ||||||
| No | 18.05 (7.83) | 30.41 (5.46) | 30.51 (5.88) | 34.19 (6.70) | 35.89 (6.69) | |
| Yes | 21.00 (8.94) | 28.07 (7.43) | 30.33 (7.93) | 36.60 (6.49) | 36.33 (8.02) | |
| p | 0.384 | 0.148 | 0.585 | 0.198 | 0.769 | |
No other significant differences were found in the quantitative psychological analysis.
3.4Factors contributing to coping strategies differences across the sample
The analysis conducted on the COPE inventory data also revealed significant differences in some coping strategies across different study groups. Table 5 shows the mean scores and differences within groups for the COPE inventory.
Table 5
Coping strategies differences across the sample
| Gender | Age (in groups) | Marital status | Psychiatric history records | Medical pathology at baseline | Psychiatric disorder at baseline | ||||||||
| Women | Men | 24 to 44 | 45 to 69 | Married | Not married | No | Yes | No | Yes | No | Yes | ||
| Mean (S.D.) | |||||||||||||
| Active coping [E] | 60.07 (18.56) | 61.94 (16.7) | 60.67 (18.62) | 61.08 (15.45) | 62.8 (14.87) | 57.39 (21.73) | 64.54 (15.49) | 50.62 (19.94) | 60.37 (18.65) | 63.14 (11.63) | 63.67 (14.74) | 52.08 (23.27) | |
| p | 0.821 | 0.726 | 0.524 | 0.15 | 0.988 | 0.131 | |||||||
| Planning [E] | 69.47 (22.39) | 69.0 (14.45) | 67.67 (20.51) | 74.17 (16.49) | 71.4 (18.82) | 65.78 (20.95) | 72.89 (18.22) | 59.62 (20.67) | 67.32 (19.94) | 80.86 (13.48) | 70.83 (18.42) | 64.67 (23.09) | |
| p | 0.690 | 0.373 | 0.413 | 0.036 | 0.067 | 0.508 | |||||||
| Seeking instrumental support [HS] | 67.2 (16.64) | 60.28 (18.92) | 66.06 (18.71) | 60.25 (13.83) | 62.73 (17.36) | 67.72 (18.2) | 67.4 (15.21) | 57.08 (21.94) | 63.46 (18.05) | 71.29 (14.44) | 66.0 (16.7) | 60.42 (20.48) | |
| p | 0.189 | 0.156 | 0.246 | 0.100 | 0.421 | 0.314 | |||||||
| Suppression of competing activities [E] | 43.3 (19.11) | 44.44 (14.58) | 43.47 (16.6) | 44.5 (20.38) | 42.5 (16.83) | 45.78 (18.6) | 45.69 (18.88) | 38.46 (11.56) | 41.05 (16.18) | 59.43 (17.0) | 44.47 (16.08) | 41.5 (21.52) | |
| p | 0.713 | 0.904 | 0.352 | 0.239 | 0.053 | 0.809 | |||||||
| Restraint [E] | 55.23 (18.25) | 55.56 (15.97) | 57.61 (17.0) | 48.58 (16.92) | 54.13 (17.5) | 57.39 (17.14) | 56.11 (16.02) | 53.31 (20.81) | 54.05 (17.73) | 63.0 (12.57) | 57.39 (17.0) | 49.25 (17.27) | |
| p | 0.779 | 0.078 | 0.532 | 0.860 | 0.237 | 0.210 | |||||||
| Seeking emotional support [HS] | 62.27 (21.41) | 50.94 (23.06) | 58.39 (25.16) | 56.92 (12.08) | 58.6 (20.72) | 57.06 (25.79) | 58.37 (21.46) | 57.08 (25.98) | 58.98 (23.09) | 52.43 (19.16) | 58.58 (22.26) | 56.33 (24.11) | |
| p | 0.205 | 0.857 | 0.691 | 0.833 | 0.250 | 0.622 | |||||||
| Positive reinterpretation [E] | 74.97 (18.04) | 72.11 (14.33) | 73.58 (17.42) | 74.83 (14.74) | 73.53 (14.74) | 74.5 (19.87) | 77.54 (16.16) | 64.08 (14.22) | 72.9 (17.38) | 79.71 (10.5) | 76.56 (14.13) | 65.92 (21.36) | |
| p | 0.369 | 0.726 | 0.689 | 0.006 | 0.458 | 0.119 | |||||||
| Turning to religion [D] | 15.27 (23.59) | 5.61 (11.88) | 9.06 (19.89) | 19.42 (20.83) | 16.97 (23.84) | 2.78 (7.03) | 9.77 (15.89) | 16.69 (29.64) | 11.41 (21.58) | 13.0 (12.57) | 12.5 (22.61) | 9.08 (12.03) | |
| p | 0.088 | 0.064 | 0.012 | 0.738 | 0.178 | 0.956 | |||||||
| Acceptance [E] | 68.87 (19.96) | 70.44 (17.14) | 71.11 (19.95) | 64.5 (14.31) | 69.17 (15.79) | 69.94 (23.43) | 71.66 (18.03) | 63.54 (20.19) | 68.73 (19.32) | 73.71 (15.8) | 71.08 (15.91) | 64.58 (25.82) | |
| p | 0.889 | 0.159 | 0.533 | 0.271 | 0.595 | 0.665 | |||||||
| Humor [*] | 31.2 (25.24) | 52.5 (27.74) | 42.56 (28.07) | 29.08 (26.02) | 33.13 (25.38) | 49.28 (29.74) | 39.43 (26.72) | 38.54 (32.1) | 42.73 (28.06) | 28.43 (16.45) | 37.86 (27.34) | 43.17 (30.5) | |
| p | 0.008 | 0.113 | 0.057 | 0.824 | 0.059 | 0.564 | |||||||
| Focus on &venting emotions [HS] | 45.0 (23.84) | 32.0 (22.33) | 37.25 (23.35) | 48.75 (24.46) | 40.57 (24.79) | 39.39 (23.03) | 37.63 (25.19) | 46.85 (19.33) | 38.83 (24.05) | 47.71 (23.26) | 36.83 (23.51) | 50.0 (23.28) | |
| p | 0.068 | 0.098 | 0.838 | 0.164 | 0.346 | 0.063 | |||||||
| Denial [D] | 18.53 (15.12) | 6.89 (6.64) | 12.44 (13.74) | 19.33 (13.06) | 11.87 (11.95) | 18.0 (15.99) | 14.2 (14.28) | 14.08 (12.83) | 14.37 (13.85) | 13.0 (14.26) | 13.83 (13.25) | 15.17 (15.82) | |
| p | 0.010 | 0.083 | 0.234 | 0.905 | 0.730 | 0.855 | |||||||
| Mental disengagement [D] | 34.73 (20.91) | 29.11 (19.89) | 33.75 (21.23) | 29.25 (18.6) | 28.07 (18.49) | 40.22 (21.94) | 30.71 (18.33) | 37.77 (25.6) | 33.56 (20.06) | 27.14 (23.85) | 29.86 (19.19) | 40.92 (22.91) | |
| p | 0.443 | 0.548 | 0.060 | 0.331 | 0.452 | 0.136 | |||||||
| Behavioral disengagement [D] | 19.23 (17.32) | 20.78 (16.19) | 20.64 (17.56) | 17.33 (14.44) | 15.87 (13.4) | 26.39 (19.9) | 19.77 (15.42) | 19.92 (20.61) | 19.76 (17.46) | 20.14 (12.85) | 19.44 (15.94) | 20.92 (19.71) | |
| p | 0.619 | 0.611 | 0.057 | 0.814 | 0.744 | 0.990 | |||||||
| Alcohol &drug use [*] | 4.43 (13.99) | 10.61 (24.86) | 8.78 (21.35) | 0.67 (2.31) | 5.8 (19.68) | 8.33 (17.67) | 8.06 (21.43) | 3.23 (8.05) | 7.1 (19.78) | 4.71 (12.47) | 5.06 (14.11) | 11.83 (28.97) | |
| p | 0.217 | 0.241 | 0.254 | 0.645 | 0.780 | 0.506 | |||||||
| Engagement [E] | 63.38 (15.37) | 62.21 (9.5) | 63.35 (14.09) | 61.73 (11.38) | 63.65 (11.94) | 61.76 (15.77) | 65.93 (12.83) | 54.9 (11.73) | 61.75 (13.75) | 69.94 (8.58) | 65.16 (11.2) | 56.3 (17.34) | |
| p | 0.670 | 0.453 | 0.924 | 0.006 | 0.121 | 0.190 | |||||||
| Disengagement [D] | 22.0 (11.71) | 15.58 (8.28) | 18.95 (11.3) | 21.53 (9.92) | 18.26 (9.86) | 21.83 (12.48) | 18.66 (10.09) | 22.1 (13.01) | 19.82 (11.27) | 18.29 (9.26) | 18.96 (10.16) | 21.51 (13.27) | |
| p | 0.062 | 0.446 | 0.327 | 0.403 | 0.672 | 0.651 | |||||||
| Help-seeking [*] | 57.84 (14.65) | 47.71 (17.41) | 53.63 (17.1) | 55.27 (14.36) | 53.93 (17.05) | 54.22 (15.52) | 54.19 (16.06) | 53.63 (17.69) | 53.51 (16.92) | 57.11 (12.91) | 53.54 (16.5) | 55.54 (16.42) | |
| p | 0.050 | 0.839 | 0.941 | 0.754 | 0.748 | 0.858 | |||||||
Women had significantly higher mean scores in Denial (U = 152.5, p = 0.010) and Help-seeking (U = 178, p = 0.050) than men. Instead, men had higher means scores than women in Humor (U =146.5, p = 0.008).
Individuals with no psychiatric history at baseline showed significantly higher mean scores in Active coping (U = 124.5, p = 0.015), Planning (U = 138, p = 0.036), Positive reinterpretation (U =111.5, p = 0.006), and Engagement (U = 108, p =0.006) than those with a history of previous psychiatric disorders.
Married individuals had significantly higher mean scores in Religion than those not married (U = 167.5, p = 0.012).
No other significant differences were found regarding coping characteristics.
Association between anxiety and depression, personality and coping strategies, and psychological distress and personality and coping strategies
Pearson’s r correlation was used to examine the association between depression and anxiety, personality traits and coping strategies, and depression and anxiety and personality and coping strategies (Table 6).
In the first instance, depression and anxiety were found to be strongly positively correlated (r = 0.74, p < 0.001) with one another.
Table 6
Correlations coefficients between anxiety and depression, coping strategies and personality dimensions, and anxiety and depression with personality dimensions and coping strategies
| HADS scale | NEO-FFI-R inventory | |||||||
| HAD-Anxiety | HAD-Depression | Neuroti-cism | Extraver-sion | Openness to experience | Agree-ableness | Conscient-iousness | ||
| HADS scale | ||||||||
| HAD-Anxiety | Pearson’s r | – | – | 0.72 | –0.12 | 0.07 | –0.20 | –0.06 |
| p | – | – | < 0.001 | 0.414 | 0.651 | 0.166 | 0.688 | |
| HAD-Depression | Pearson’s r | 0.74 | – | 0.058 | –0.11 | 0.18 | –0.20 | –0.15 |
| p | < 0.001 | – | < 0.001 | 0.436 | 0.222 | 0.979 | 0.297 | |
| COPE inventory –Subscales | ||||||||
| Active coping [E] | Pearson’s r | –0.15 | –0.05 | –0.02 | 0.41 | 0.24 | 0.02 | 0.14 |
| p | 0.338 | –0.749 | 0.907 | 0.004 | 0.106 | 0.887 | 0.340 | |
| Planning [E] | Pearson’s r | –0.11 | –0.02 | –0.07 | 0.19 | 0.18 | –0.01 | 0.21 |
| p | 0.489 | 0.878 | 0.642 | 0.201 | 0.223 | 0.960 | 0.157 | |
| Seeking instrumental support [HS] | Pearson’s r | 0.07 | –0.04 | 0.18 | 0.30 | 0.25 | –0.08 | 0.18 |
| p | 0.631 | 0.809 | 0.226 | 0.041 | 0.081 | 0.574 | 0.220 | |
| Suppression of competing activities [E] | Pearson’s r | 0.20 | 0.05 | 0.20 | 0.20 | 0.32 | –0.22 | 0.23 |
| p | 0.188 | 0.725 | 0.167 | 0.177 | 0.028 | 0.131 | 0.122 | |
| Restraint [E] | Pearson’s r | –0.29 | –0.22 | –0.23 | –0.02 | –0.17 | 0.15 | 0.09 |
| p | 0.055 | 0.155 | 0.123 | 0.886 | 0.260 | 0.301 | 0.526 | |
| Seeking emotional support [HS] | Pearson’s r | –0.04 | 0.06 | 0.23 | 0.46 | 0.42 | 0.11 | –0.05 |
| p | 0.789 | 0.708 | 0.120 | < 0.001 | 0.003 | 0.451 | 0.734 | |
| Positive reinterpretation [E] | Pearson’s r | –0.30 | –0.28 | –0.21 | 0.09 | 0.12 | 0.21 | 0.15 |
| p | 0.044 | 0.062 | 0.144 | 0.539 | 0.435 | 0.147 | 0.305 | |
| Turning to religion [D] | Pearson’s r | 0.02 | 0.04 | 0.27 | 0.09 | 0.20 | 0.05 | 0.29 |
| p | 0.881 | 0.781 | 0.061 | 0.557 | 0.184 | 0.715 | 0.044 | |
| Acceptance [E] | Pearson’s r | –0.28 | –0.18 | –0.22 | 0.13 | 0.10 | 0.29 | –0.13 |
| p | 0.059 | 0.226 | 0.137 | 0.358 | 0.518 | 0.046 | 0.372 | |
| Humor [*] | Pearson’s r | –0.04 | 0.08 | –0.003 | 0.04 | 0.25 | –0.08 | –0.5 |
| p | 0.805 | 0.587 | 0.848 | 0.796 | 0.085 | 0.573 | < 0.001 | |
| Focus on &venting emotions [HS] | Pearson’s r | 0.42 | 0.28 | 0.68 | 0.08 | 0.51 | –0.11 | –0.14 |
| p | 0.004 | 0.062 | < 0.001 | 0.572 | < 0.001 | 0.465 | 0.346 | |
| Denial [D] | Pearson’s r | 0.22 | 0.15 | 0.42 | 0.07 | 0.01 | 0.15 | 0.21 |
| p | 0.143 | 0.324 | 0.003 | 0.659 | 0.971 | 0.306 | 0.146 | |
| Mental disengagement [D] | Pearson’s r | 0.29 | 0.18 | 0.46 | –0.18 | 0.28 | –0.05 | –0.24 |
| p | 0.052 | 0.242 | < 0.001 | 0.213 | 0.053 | 0.747 | 0.096 | |
| Behavior disengagement [D] | Pearson’s r | 0.01 | 0.11 | 0.12 | –0.28 | –0.02 | 0.06 | –0.14 |
| p | 0.946 | 0.478 | 0.406 | 0.056 | 0.892 | 0.661 | 0.335 | |
| Alcohol &drug disengagement [D] | Pearson’s r | 0.22 | 0.32 | 0.35 | –0.11 | 0.4 | –0.37 | –0.5 |
| p | 0.145 | 0.029 | 0.014 | 0.460 | 0.005 | 0.011 | < 0.001 | |
| COPE inventory –Dimensions | ||||||||
| Engagement [E] | Pearson’s r | –0.20 | –0.11 | –0.11 | 0.28 | 0.24 | 0.11 | 0.10 |
| p | 0.178 | 0.463 | 0.438 | 0.056 | 0.100 | 0.447 | 0.479 | |
| Disengagement [D] | Pearson’s r | 0.21 | 0.19 | 0.51 | –0.14 | 0.22 | 0.08 | 0.04 |
| p | 0.156 | 0.217 | < 0.001 | 0.356 | 0.136 | 0.581 | 0.803 | |
| Help-seeking [HS] | Pearson’s r | 0.21 | 0.16 | 0.49 | 0.36 | 0.53 | –0.02 | –0.04 |
| p | 0.172 | 0.308 | < 0.001 | 0.011 | < 0.001 | 0.915 | 0.796 | |
Values expressed in the table are Pearson’s Correlation Coefficients (r statistic).
Hereafter, Neuroticism was moderate to strongly positively correlated with Focus on and venting emotions (r = 0.68, p < 0.001), moderately positively associated with Mental disengagement (r = 0.46, p < 0.001) and Denial (p = 0.042, p = 0.003), and weak to moderately positively correlated with Alcohol and drug use (r = 0.49, p < 0.001). Neuroticism was also moderately positively correlated with Disengagement (r = 0.51, p < 0.001) and Help-seeking (r = 0.49, p < 0.001). Extraversion was moderately positively associated with Seeking emotional support (r = 0.46, p < 0.001) and Active coping (r = 0.46, p < 0.001). Extraversion also weakly positively correlated with Help-seeking (r = 0.36, p = 0.011) and Seeking instrumental support (r = 0.30, p = 0.041). Pearson’s r also showed that Openness to experience was strongly positively correlated with Help-seeking (r = 0.53, p < 0.001), Focus on and venting emotions (r = 0.51, p < 0.001), Seeking emotional support (r = 0.42, p = 0.003), and Alcohol and drug use (r = 0.40, p = 0.005). The association between Openness to experience and Suppression of competing activities was positively weak (r = 0.32, p = 0.028). Agreeableness was weakly positively correlated with Acceptance (r = 0.29, p = 0.046) but weakly to moderately negatively associated with Alcohol and drug disengagement (r = –0.37, p = 0.011). Lastly, Conscientiousness was weakly positively correlated with Turning to religion (r = 0.29, p = 0.044) but moderately negatively correlated with Alcohol and drug use (r = –0.50, p < 0.010) and Humor (r = –0.50, p < 0.001).
At last, Neuroticism was strongly positively correlated (r = 0.72. p < 0.001) with anxiety and moderately positively correlated with depression (r = 0.58, p≤0.001). Positive interpretation and growth were weak to moderately negatively correlated (r = –0.30, p = 0.044) with anxiety, while Focus on and venting emotions were moderately positively correlated (r = 0.42, p = 0.004) with anxiety. Alcohol and drug use was weak to moderately positively associated (r = 0.32, p = 0.029) with depression.
Predictors of psychological distress, personality traits, and coping strategies based on sociodemographic background
Lastly, after adjusting for age and gender, it was found that having a psychiatric disorder at baseline was associated with greater anxiety (β= 3.662, p < 0.001) and depression (β= 3.47, p < 0.001). Age was also significantly associated with depression, with an increase in depressive symptomatology the older the individual was (β= 0.96, p = 0.022). A psychiatric history record was associated with lower Engagement (β= –11.024, p = 0.010). On the contrary, being a woman was associated with higher Neuroticism (β= 5.461, p = 0.021) and greater Disengagement (β= 6.427, p = 0.047). Further details of the regression coefficients and results are shown in Table 7.
Table 7
Regression coefficients for the significant predictors of psychological distress, personality traits, and coping strategies based on sociodemographic background
| HADS scale | B | 95% CI | β | t | p | |||
| HAD-Anxietya | Psychiatric disorder at baseline, Yes | 3.662 | 1.615–5.710 | 0.448 | 3.597 | < 0.001 | ||
| HAD-Depressionb | Psychiatric disorder at baseline, Yes | 3.847 | 1.833–5.862 | 4.60 | 3.840 | < 0.001 | ||
| Age (y) | 0.096 | 0.015–0.178 | 0.284 | 2.371 | 0.022 | |||
| NEO-FFI-R inventory | ||||||||
| Neuroticismc | Gender, Men | –5.461 | –10.048––0.873 | –0.320 | –2.391 | 0.021 | ||
| COPE inventory | ||||||||
| Engagementd | Psychiatric history records, Yes | –11.024 | –19.232––2.816 | –0.370 | –2.704 | 0.010 | ||
| Disengagemente | Gender, Men | –6.427 | –12.773––0.081 | –0.288 | –2.039 | 0.047 |
CI, confidence interval for B. a[F(2, 48) = 8.279, p < 0.001; R2 = 0.256]. b[F(2, 48) = 11.385, p < 0.001; R2 = 0.322]. c[F(1, 50) = 5.717, p = 0.021; R2 = 0.120]. d[F(1, 46) = 7.309, p = 0.10; R2 = 0.137]. e[F(1, 46) = 4.156, p = 0.047; R2 = 0.083].
DISCUSSION
To the best of our knowledge, our study is the first to provide consistent data on the psychiatric, psychological, and coping characteristics of first-degree individuals who requested genetic counseling due to possible familial dementia. While we acknowledge that factors such as predisposition and willingness of individuals to attend genetic counseling may have a meaningful effect on our results, we encountered personality factors, coping strategies, and depression and anxiety levels comparable with the general population.
In further detail, our study showed that women had higher Conscientiousness, Agreeableness, and Neuroticism than men, observing significant differences in this last personality factor. Despite these differences across genders, results were in line with the Spanish normative data for the NEO-FFI inventory. That is, gender differences were significantly different in Neuroticism and Agreeableness, with women presenting higher levels than men in both cases [33]. Our results also partially supported early research conducted in the general population, where women showed not only significantly higher Neuroticism and Agreeableness than men but also in Openness to experience and Extraversion [34–36].
When taken as a whole, the NEO-FFI-R inventory outcome for the sample revealed that Conscientiousness and Agreeableness were the most preponderant personality dimensions while Neuroticism was the least. These results were similar to those observed in heart transplantation recipients, who were expected to have high psychological distress due to the severity of the surgery they were subjected to [37, 38]. To our surprise, the personality outcome for the sample, hence of heart transplantation recipients, appeared to be within the range of results obtained in the Spanish validation of the scale [39].
Regarding the NEO-FFI-R inventory, previous research has shown that personality traits are strongly related to mental health [40–43]. High Neuroticism and low Conscientiousness, Extraversion, and Agreeableness have been defined as the typical pattern linked to mental disorders [40, 43]. On the contrary, high Openness to experience has been largely unrelated to psychiatric symptoms [40]. Similarly, research has also unfolded the relationship between personality traits and therapy results and all this entails [37, 38]. For instance, a study conducted with 65 patients attending interdisciplinary genetic counseling for hereditary non-polyposis colorectal cancer concluded that high levels of Openness to experience and Agreeableness were strongly associated with positive therapy outcomes [44, 45]. Therefore, and bearing the previous literature in mind, the personality outcome for the sample suggested a low correlation between personality traits across PICOGEN candidates and mental health impairment. A low correlation between personality traits and mental health impairment and high levels of Openness to experience and Conscientiousness could infer better compliance and outcome regarding genetic counseling, as other authors have already suggested [42].
Despite not finding any other study to compare our personality results with a similar cohort of individuals attending genetic counseling for familial dementia, study factors such as psychiatric history, ongoing medical illness, or psychiatric disorder at baseline did not involve significant differences in personality traits. Contrary to what we expected, personality traits across study groups were much alike and close to normative data [33]. The lack of statistical differences in personality across groups may be due to the low occurrence of these factors in our sample. In other words, although psychiatric disorders increase the probability of future psychiatric conditions and other comorbidities [46], thereby impairing life quality and inducing fluctuations in behavior, personality, and psychological distress [47, 48], psychiatric history and psychiatric disorders were somewhat anecdotal in our sample. The same applies to medical illnesses [49, 50], being this group a minority in our study.
Regarding the HADS test, comparisons between men and women appeared to be consistent with the results observed in the general population [23, 51] and individuals testing for Huntington’s disease and other neurodegenerative disorders [52, 53]. Women had overall greater emotional distress than men. Moreover, both men and women in our study scored below the threshold for clinical relevance in anxiety and depression [37, 38, 54]. Having a psychiatric history did not involve a significant difference in the HADS test, being the levels of anxiety and depression between individuals with and without psychiatric history closely alike, similar to those observed in the general population [23], and below the cut-off point for mild severity [55, 56]. A reasonable explanation for the latter results could be that previous psychiatric disorders were already resolved when conducting the psychiatric assessment at baseline, thus not interfering with the basal anxiety and depression levels. On the contrary, aging involved a significant increase in depression and, to some extent, anxiety [57–59]. These results are reasonable if one takes into consideration that the older the individual, the closer to the age of debut of the disease. Thus, the more intense the feelings of threat of developing early-onset dementia may be [52, 60].
In line with aging, having an ongoing medical illness implied significantly greater depression than having no medical illness. On this matter, the HAD-D mean scores indicated mild severity of the depression symptoms. Individuals with an ongoing medical illness also appeared to have greater anxiety than those without any medical pathology. Nevertheless, anxiety differences between the two groups were not significant. As previously discussed in this section, presenting a medical illness can significantly increase psychological distress, especially when chronic [50, 61]. This latter, together with the psychological burden associated with the familial dementia consultation, highlights the importance of genetic counseling to ensure the best well-being of individuals. Otherwise, the psychological distress resulting from the medical illness and the genetic consultation could negatively affect the patient’s quality of life and thus interfere meaningfully with adherence to genetic counseling and coping with the results, as some authors assert [49, 50].
Presenting a psychiatric disorder at baseline led to greater anxiety and depression than not having any. Apart from being statistically significant, these differences between groups revealed that individuals with a psychiatric disorder presented mild anxiety levels [62]. A psychiatric disorder in the uncertainty of the genetic test results may exacerbate the baseline psychological distress and foster new psychiatric comorbidities [46, 47]. As previously discussed in this manuscript, the worsening of mental health could drastically diminish the individual’s life quality, thus interfering with genetic counseling and the management of the clinical implications of the disease [49, 50]. Nevertheless, note that the anxiety and depression levels across individuals with psychiatric disorders were close to the general population [55].
As for the sample, anxiety and depression levels were below the threshold for mild severity [44] and similar to those observed across individuals at risk of hereditary non-polyposis colorectal cancer [17, 44] and referred to genetic counseling for breast and ovarian cancer [63]. Furthermore, albeit PICOGEN candidates had slightly higher mean scores, anxiety and depression levels encountered in the psychological evaluation were within the range of the HADS test normative data [55]. All in all, these results accentuate the sample’s low clinical levels of psychological distress before undertaking the genetic test.
Regarding the COPE inventory, and although the literature contemplates different groups of coping strategies [64], our sample emphasized the use of Engagement and Help-seeking coping strategies over those grouped within the Disengagement dimension. These findings align with previous research on individuals from the general population [65] and testing for breast cancer [66]. The same tendency was observed across the other study groups analyzed in our study. Overall, Engagement coping strategies were the most frequently used, whereas Disengagement strategies were the least adopted. The combined use of problem- and emotion-focused coping mechanisms, in other words, Engagement and Help-seeking strategies, respectively, have shown to predict higher perceived efficacy in handling the illness, as well as greater compliance with the medical process involved with the same illness amongst transplant recipients [37, 67–69]. In contrast, maladaptive coping strategies, also known as Disengagement strategies, have been related to higher emotional distress, lower resilience, worse course of the illness, and poorer quality of life [70, 71].
It is noteworthy that men and women showed fair homogeneity across the coping strategies assessed, except for Humor, Denial, and Help-seeking. Despite the latter differences, the COPE results across gender were within normality ranges [39]. A reason for this similarity between men and women in coping strategies could be the context [66, 72]. Essentially, our study aimed to evaluate individuals who voluntarily joined the PICOGEN program to receive genetic counseling. Not surprisingly, we expected to encounter men and women who were, to some extent, willing to know about their genetic condition, despite the consequences this may involve in both the short- and long-term after the genetic test results are given.
Individuals married at baseline reported using more religious coping strategies than those not married. Beyond the relationship between traditional marriage and religion, these results are interesting. Research has demonstrated that religiousness, based on beliefs and practices, helps cope with difficult situations such as illnesses or psychological distress [73, 74]. That is, individuals who use religious coping appear to handle their conditions more effectively than those who do not [74], which would greatly benefit when addressing the familial dementia implications.
Our study also revealed poorer Active coping, Planning, Positive reinterpretation, and Engagement coping strategies across individuals with a psychiatric history [75, 76]. Accordingly, these results would indicate that individuals with a previous psychiatric disorder at baseline would show reduced commitment to cope with a stressor, ability to plan on how to handle the problem and see events in a more positive light to reduce the stressor or its consequences. Once again, these results emphasize the relevance of genetic counseling as a key procedure to effectively deliver accurate information regarding the neurodegenerative disorder while offering professional accompaniment and follow-up to individuals. By doing so, genetic counseling would contribute to strengthening the individuals’ competencies to organize and take action to effectively cope with the genetic test results and be proactive in dealing with its clinical implications, especially in the event of being positive for the disease [13, 16, 60].
Our correlation analysis confirmed what other studies have already yielded regarding psychological distress: a positive relationship between anxiety and depression. As anxiety increased, depression also increased, and vice versa [77, 78]. The correlation analysis additionally revealed that adaptive personality traits were positively associated with Active coping strategies and negatively associated with Disengagement strategies. Likewise, maladaptive personality traits were positively associated with Disengagement coping strategies and negatively correlated with adaptive coping strategies [79, 80]. The correlation between anxiety and depression with personality and coping strategies also aligned with early investigations [80, 81]. On the one hand, Neuroticism positively correlated with depression and anxiety, with the latter association being significant in our study. On the other hand, Focus on and venting emotions was positively correlated with anxiety and Alcohol and drug use with depression, and Positive reinterpretation was negatively correlated with anxiety. In short, the correlation analysis evidenced the positive association between problem-focused coping strategies and adaptive personality traits, with these latter two outweighing the use of avoidance coping strategies and maladaptive personality traits among PICOGEN candidates.
Lastly, the regression models also confirmed the findings already discussed in our study. At baseline, an ongoing psychiatric disorder predicted worse psychological distress [47], with aging specifically aggravating depressive symptoms [82, 83]. Psychiatric history was a predictor of lower Engagement [75], which would foster the avoidance of confronting the situation related to familial dementia [28]. Likewise, being a woman was related to an increase in Neuroticism [30], which in our study also correlated with increased depression and anxiety. The regression models also showed that women were related to increased Disengagement. Disengagement has been widely documented to negatively interfere with the coping process, thus resulting in greater psychological distress, lower resilience, worse course of the illness, and poorer quality of life [59, 60]. Nevertheless, it is important to underline that some forms of Disengagement, such as positive distraction (e.g., leisure coping, positive emotionally), may also be adaptive in contexts of extreme uncertainty, as other studies have indicated [84–87]. That is, positive distraction (as opposed to avoidance), which is defined as thinking or engaging oneself in activities that trigger positive emotions to distract from a stressor, has proven to be a strong predictor of positive outcomes when dealing with chronic stressors. Namely, higher well-being and positive emotions, and fewer depressive symptoms and negative emotions [88].
This study, though, presents a few limitations. In the first instance, the number of participants recruited for the study was relatively small, which can be explained by different reasons. To begin with, and despite the local media coverage, genetic counseling is an event that, if not new, was and still is largely unknown to most of the general population. This latter fact, together with the fear of being aware of the possibility of suffering from an inevitably terminal disease, we believe negatively impacted the decision to participate, even when neurologists from our and other hospitals referred individuals to the PICOGEN program. The inability to assess first-grade individuals of patients diagnosed with familial dementia who decided not to participate in the PICOGEN program also directly impacted the sample size. Furthermore, first-grade individuals of patients diagnosed with familial dementia who decided not to participate were expected to differ in psychological and psychiatric characteristics and coping strategies compared to PICOGEN candidates who volunteered to participate [72, 89]. Taken together, the sample size-related limitations could have led us to mistakenly reject a true null hypothesis (i.e., false positive) in the analyses conducted. Likewise, the lack of a control group prevented determining whether the measured features were actual characteristics of PICOGEN candidates. The nature of cross-sectional study designs also prevented generalizing the findings while reducing the statistical power of the results [90]. The assessment of the psychiatric and psychological characteristics of PICOGEN candidates was solely based on three different psychometric instruments (HADS, NEO-FFI-R, COPE) selected upon the following criteria: to be a gold-standard in their clinical area, hold strong psychometric properties, and be widely used in research [24, 28, 51]. In addition, we also considered the limited time to conduct the research, the high healthcare pressure to which our group is exposed daily (and which is combined with the research activity), the small size of our research group, and, above all, ensuring that PICOGEN candidates were not overwhelmed with long and numerous assessment tools. Nevertheless, we acknowledge that adding a broader range of standardized psychometric instruments to the clinical assessment, especially for what concerns anxiety and depression (e.g., Hamilton Anxiety Rating Scale [91] & Hamilton Depression Rating Scale [92])— evaluated using a single assessment instrument (i.e., HADS)— would have brought more consistency to the study results. Similarly, although it was not the object of our research, the clinical neurological assessment was based exclusively on observational methods (i.e., clinical interview). The quantification of the mental state of PICOGEN candidates would have provided objectivity and solidity to the recruitment process and thus to the results.
In short, genetic counseling is a crucial resource by which empower affected individuals and relatives at risk to make autonomous decisions regarding familial dementia. That is, to help those involved in the illness understand, adapt, and adjust to the medical, social, and psychological consequences of genetic contributions to illness [16, 60, 93]. Despite the central role of genetic counseling in the acceptance and management of the illness, data on this topic are still narrow and relatively controversial. What is worse, the data available highlight access limitations [72, 89, 94]. While we acknowledge the uniqueness of our sampling, which may limit the interpretation of the results and prevent their generalization to other cohorts under similar characteristics, we believe our study findings provide valuable data to experts from all related areas. More importantly, our study findings enhance the overall knowledge related to genetic counseling, especially concerning the psychiatric and psychological characteristics of the attendees. Taken together, our study will allow future research projects to be more tailored to the reality of the processes involved in the disease.
We, therefore, encourage future research to recruit a more generous cohort and include a follow-up to examine the differences in psychological, psychiatric, and coping characteristics throughout the genetic counseling program. We also recommend including a control group, which would allow further comparisons. Likewise, we strongly suggest using a wider selection of psychometric instruments in the clinical assessment to quantify the neurocognitive evaluation and provide robustness to the results of the psychiatric and psychological evaluations.
Conclusions
Contrary to our expectations, the current research illustrates that the overall levels of anxiety and depression, personality traits, and coping strategies among PICOGEN candidates were compatible with those encountered within the general population. In other words, the levels of psychological distress were predominantly below the cut-off point for clinical relevance, and adaptive personality traits and problem-focused coping strategies prevailed over avoidance coping strategies and maladaptive personality traits. Nevertheless, clinicians should pay particular attention to individuals attending genetic counseling who are women, aged, and present an ongoing psychiatric disorder and psychiatric history at inclusion to ensure their mental health and adherence throughout the genetic counseling program.
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCES
[1] | Buffington ALH , Lipski DM , Westfall E ((2013) ) Dementia: An evidence-based review of common presentations and family-based interventions. J Am Osteopath Assoc 113: , 768–775. |
[2] | Onyike CU ((2016) ) Psychiatric aspects of dementia. Continuum (Minneap Minn) 22: , 600–614. |
[3] | Lyketsos CG ((2015) ) Neuropsychiatric symptoms in dementia: Overview and measurement challenges. J Prev Alzheimers Dis 2: , 155–156. |
[4] | Gottesman RT , Stern Y ((2019) ) Behavioral and psychiatric symptoms of dementia and rate of decline in Alzheimer’s disease. Front Pharmacol 10: , 1062. |
[5] | Fortea J , Lladó A , Clarimón J , Lleó A , Oliva R , Peri J , Pintor L , Yagüe J , Blesa R , Molinuevo JL , Sánchez-Valle R ((2011) ) PICOGEN: Experiencia de 5 años de un programa de asesoramiento genético en demencia.. Neurologia 26: , 143–149. |
[6] | Paulson HL , Igo I ((2011) ) Genetics of dementia. Semin Neurol 31: , 449–460. |
[7] | Lladó A , Gaig C , Molinuevo JL ((2006) ) Genética de las enfermedades neurodegenerativas más prevalentes [Genetics of prevalent neurodegenerative disorders]. Med Clin 126: , 662–670. |
[8] | Lleó A , Blesa R , Queralt R , Ezquerra M , Molinuevo JL , Peña-Casanova J , Rojo A , Oliva R ((2002) ) Frequency of mutations in the presenilin and amyloid precursor protein genes in early-onset Alzheimer disease in Spain. Arch Neurol 59: , 1759–1763. |
[9] | Hogan DB , Jetté N , Fiest KM , Roberts JI , Pearson D , Smith EE , Roach P , Kirk A , Pringsheim T , Maxwell CJ ((2016) ) The prevalence and incidence of frontotemporal dementia: A systematic review. Can J Neurol Sci 43: , S96–S109. |
[10] | Sanchez-Valle R , Nos C , Yagüe J , Graus F , Domínguez A , Saiz A ((2004) ) Clinical and genetic features of human prion diseases in Catalonia: 1993-2002. Eur J Neurol 11: , 649–655. |
[11] | Collins SJ , Lawson VA , Masters CL ((2004) ) Transmissible spongiform encephalopathies. Lancet 363: , 51–61. |
[12] | Kovács GG , Puopolo M , Ladogana A , Pocchiari M , Budka H , van Duijn C , Collins SJ , Boyd A , Giulivi A , Coulthart M , Delasnerie-Laupretre N , Brandel JP , Zerr I , Kretzschmar HA , de Pedro-Cuesta J , Calero-Lara M , Glatzel M , Aguzzi A , Bishop M , Knight R , Belay G , Will R , Mitrova E ((2005) ) Genetic prion disease: The EUROCJD experience. Hum Genet 118: , 166–174. |
[13] | Austin J , Honer W ((2004) ) The potential impact of genetic counseling for mental illness. Clin Genet 67: , 134–142. |
[14] | Molinuevo JL , Pintor L , Peri J , Lleó A , Oliva R , Marcos T , Blesa R ((2005) ) Emotional reactions to predictive testing in Alzheimer’s disease and other inherited dementias. Am J Alzheimers Dis Other Demen 20: , 233–238. |
[15] | Chen C , Dong XP ((2016) ) Epidemiological characteristics of human prion diseases. Infect Dis Poverty 5: , 47. |
[16] | Resta R , Bowles Biesecker B , Bennett RL , Blum S , Hahn SE , Strecker MN , Williams JL ((2006) ) A new definition of Genetic Counseling: National Society of Genetic Counselors’ Task Force report. J Genet Couns 15: , 77–83. |
[17] | Nordin K , Lidén A , Hansson M , Rosenquist R , Berglund G ((2002) ) Coping style, psychological distress, risk perception, and satisfaction in subjects attending genetic counselling for hereditary cancer. J Med Genet 39: , 689–694. |
[18] | Tibben A , Frets PG , van de Kamp JJ , Niermeijer MF , Vegter-van der Vlis M , Roos RA , van Ommen GJ , Duivenvoorden HJ , Verhage F ((1993) ) Presymptomatic DNA-testing for Huntington disease: Pretest attitudes and expectations of applicants and their partners in the Dutch program. Am J Med Genet 48: , 10–16. |
[19] | Decruyenaere M , Evers-Kiebooms G , Boogaerts A , Cassiman JJ , Cloostermans T , Demyttenaere K , Dom R , Fryns JP , Van den Berghe H ((1996) ) Prediction of psychological functioning one year after the predictive test for Huntington’s disease and impact of the test result on reproductive decision making. J Med Genet 33: , 737–743. |
[20] | Mohamed S , Sabki ZA , Zainal NZ ((2014) ) Depression and psychosocial correlates of liver transplant candidates: A systematic review. Asia Pac Psychiatry 6: , 447–453. |
[21] | Fox S , Bloch M , Fahy M , Hayden MR ((1989) ) Predictive testing for Huntington disease: I. Description of a pilot project in British Columbia. Am J Med Genet 32: , 211–6. |
[22] | First MB , Spitzer RL , Gibbon M , Williams JB ((1996) ) Structured clinical interview for DSM-IV Axis I Disorders, clinician version (SCID-CV), American Psychiatric Press, Washington, DC. |
[23] | Zigmond AS , Snaith RP ((1983) ) The hospital anxiety and depression scale. Acta Psychiatr Scand 67: , 361–370. |
[24] | Costa PT Jr , McCrae RR (1992) Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) professional manual, Psychological Assessment Resources, Odessa, FL. |
[25] | Digman JM ((1990) ) Personality structure: Emergence of the five-factor model. Annu Rev Psychol 41: , 417–440. |
[26] | Costa PT , McCrae RR (1992) NEO-PI-R Professional Manual. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five Factor Inventory (NEO-FFI), Psychol Assess Resources, Odessa, FL. |
[27] | Aluja A , Blanch A , Solé D , Dolcet J-M , Gallart S ((2009) ) Versiones cortas del NEO-PI-R: El NEO-FFI frente al NEO-FFI-R. Behav Psychol 17: , 335–350. |
[28] | Martínez Ortega Y , Gomà-i-Freixanet M , Fornieles Deu A ((2016) ) The COPE-48: An adapted version of the COPE inventory for use in clinical settings. Psychiatry Res 246: , 808–814. |
[29] | Gutiérrez F , Peri JM , Torres X , Caseras X , Valdés M ((2007) ) Three dimensions of coping and a look at their evolutionary origin. J Res Pers 41: , 1032–1053. |
[30] | Gárriz M , Gutiérrez F , Peri JM , Baillés E , Torrubia R ((2015) ) Coping strategies within a personality space. Pers Individ 80: , 96–100. |
[31] | Kim H-Y ((2015) ) Statistical notes for clinical researchers: Type I and type II errors in statistical decision. Restor Dent Endod 40: , 249–252. |
[32] | Pilotto A , Padovani A , Borroni B ((2013) ) Clinical, biological, and imaging features of monogenic Alzheimer’s disease. Biomed Res Int 2013: , 689591. |
[33] | Manga D , Ramos F , Morán C ((2004) ) The spanish norms of the NEO five-factor inventory: New data and analyses for its improvement. Rev Int Psico Ter Psicol 4: , 639–648. |
[34] | Balluerka N , Gorostiaga A , Alonso-Arbiol I , Haranburu M ((2007) ) La adaptación de instrumentos de medida de unas culturas a otras: Una perspectiva práctica. Psicothema 19: , 123–133. |
[35] | Costa PT , Terracciano A , McCrae RR ((2001) ) Gender differences in personality traits across cultures: Robust and surprising findings. J Pers Soc Psychol 81: , 322–331. |
[36] | Jonassaint CR , Siegler IC , Barefoot JC , Edwards CL , Williams RB ((2011) ) Low life course socioeconomic status (SES) is associated with negative NEO PI-R personality patterns. Int J Behav Med 18: , 13–21. |
[37] | Sánchez R , Baillès E , Peri JM , Bastidas A , Pérez-Villa F , Bulbena A , Pintor L ((2016) ) Assessment of psychosocial factors and predictors of psychopathology in a sample of heart transplantation recipients: A prospective 12-month follow-up. Gen Hosp Psychiatry 38: , 59–64. |
[38] | Sánchez R , Baillés E , Peri JM , Bastidas A , Pérez-Villa F , Bulbena A , Pintor L ((2014) ) Cross-sectional psychosocial evaluation of heart transplantation candidates. Gen Hosp Psychiatry 36: , 680–685. |
[39] | Aluja A , García O , Rossier J , García LF ((2005) ) Comparison of the NEO-FFI, the NEO-FFI-R and an alternative short version of the NEO-PI-R (NEO-60) in Swiss and Spanish samples. Pers Individ Dif 38: , 591–604. |
[40] | Kotov R , Gamez W , Schmidt F , Watson D ((2010) ) Linking “Big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychol Bull 136: , 768–821. |
[41] | Canuto A , Meiler-Mititelu C , Herrmann F , Giannakopoulos P , Weber K ((2008) ) Impact of personality on termination of short-term group psychotherapy in depressed elderly outpatients. Int J Geriatr Psychiatry 23: , 22–26. |
[42] | Hayward RD , Taylor WD , Smoski MJ , Steffens DC , Payne ME ((2013) ) Association of five-factor model personality domains and facets with presence, onset, and treatment outcomes of major depression in older adults. Am J Geriatr Psychiatry 21: , 88–96. |
[43] | Malouff JM , Thorsteinsson EB , Schutte NS ((2005) ) The relationship between the five-factor model of personality and symptoms of clinical disorders: A meta-analysis. J Psychopathol Behav 27: , 101–114. |
[44] | Keller M , Jost R , Mastromarino Haunstetter C , Kienle P , Knaebel H-P , Gebert J , Sutter C , Knebel-Doeberitz M v , Cremer F , Mazitschek U ((2002) ) Comprehensive genetic counseling for families at risk for HNPCC: Impact on distress and perceptions. Genet Test 6: , 291–302. |
[45] | Dale RM , Bryant KA , Finnegan N , Cromer K , Thompson NR , Altinay M , Anand A ((2020) ) The NEO-FFI domain of openness to experience moderates ketamine response in treatment resistant depression. J Affect Disord 260: , 323–328. |
[46] | Sobregrau P , Andreu C , Carreño M , Donaire A , Rumià J , Boget T , Bargalló N , Setoain X , Roldan P , Conde-Blanco E , Centeno M , Pintor L ((2021) ) Psychiatric disorders in patients with resistant temporal lobe epilepsy two years after undergoing elective surgery. A longitudinal study. Epilepsy Behav 118: , 107921. |
[47] | Berghöfer A , Martin L , Hense S , Weinmann S , Roll S ((2020) ) Quality of life in patients with severe mental illness: A cross-sectional survey in an integrated outpatient health care model. Qual Life Res 29: , 2073–2087. |
[48] | Widiger TA ((2011) ) Personality and psychopathology. World Psychiatry 10: , 103–106. |
[49] | Feingold D , Brill S , Goor-Aryeh I , Delayahu Y , Lev-Ran S ((2017) ) Depression and anxiety among chronic pain patients receiving prescription opioids and medical marijuana. J Affect Disord 218: , 1–7. |
[50] | Pengpid S , Peltzer K ((2018) ) The impact of chronic diseases on the quality of life of primary care patients in Cambodia, Myanmar and Vietnam. Iran J Public Health 47: , 1308–1316. |
[51] | Herrero MJ , Blanch J , Peri JM , de Pablo J , Pintor L , Bulbena A ((2003) ) A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen Hosp Psychiatry 25: , 277–283. |
[52] | Susana L , Ângela L , Sequeiros J ((2013) ) Anxiety and pre-symptomatic testing for neurodegenerative disorders. Open J Genet 3: , 14–26. |
[53] | Gargiulo M , Lejeune S , Tanguy ML , Lahlou-Laforêt K , Faudet A , Cohen D , Feingold J , Durr A ((2009) ) Long-term outcome of presymptomatic testing in Huntington disease. Eur J Hum Genet 17: , 165–171. |
[54] | Hinz A , Herzberg PY , Lordick F , Weis J , Faller H , Brähler E , Härter M , Wegscheider K , Geue K , Mehnert A ((2019) ) Age and gender differences in anxiety and depression in cancer patients compared with the general population. Eur J Cancer Care 28: , e13129. |
[55] | Hinz A , Brähler E ((2011) ) Normative values for the hospital anxiety and depression scale (hads) in the general German population. J Psychosom Res 71: , 74–78. |
[56] | Michopoulos I , Douzenis A , Kalkavoura C , Christodoulou C , Michalopoulou P , Kalemi G , Fineti K , Patapis P , Protopapas K , Lykouras L ((2008) ) Hospital Anxiety and Depression Scale (HADS): Validation in a Greek general hospital sample. Ann Gen Psychiatry 7: , 4. |
[57] | Arias de la Torre J , Vilagut G , Ronaldson A , Dregan A , Ricci-Cabello I , Hatch SL , Serrano-Blanco A , Valderas JM , Hotopf M , Alonso J ((2021) ) Prevalence and age patterns of depression in the United Kingdom. A population-based study. J Affect Disord 279: , 164–172. |
[58] | Luppa M , Sikorski C , Luck T , Ehreke L , Konnopka A , Wiese B , Weyerer S , König HH , Riedel-Heller SG ((2012) ) Age- and gender-specific prevalence of depression in latest-life–systematic review and meta-analysis. J Affect Disord 136: , 212–221. |
[59] | Gallo JJ , Lebowitz BD ((1999) ) The epidemiology of common late-life mental disorders in the community: Themes for the new century. Psychiatr Serv 50: , 1158–1166. |
[60] | Neilson J ((1999) ) A patient’s perspective on genetic counseling and predictive testing for Alzheimer’s disease. J Genet Couns 8: , 37–46. |
[61] | Gerontoukou E-I , Michaelidoy S , Rekleiti M , Saridi M , Souliotis K ((2015) ) Investigation of anxiety and depression in patients with chronic diseases. Health Psychol Res 3: , 2123. |
[62] | Ramos-Perdigués S , Baillés E , Mané A , Carreño M , Donaire A , Rumià J , Bargalló N , Boget T , Setoain X , Valdés M , Pintor L ((2018) ) Psychiatric symptoms in refractory epilepsy during the first year after surgery. Neurotherapeutics 15: , 1082–1092. |
[63] | Reichelt JG , Heimdal K , Møller P , Dahl AA ((2004) ) BRCA1 testing with definitive results: A prospective study of psychological distress in a large clinic-based sample. Fam Caner 3: , 21–28. |
[64] | García FE , Barraza-Peña CG , Wlodarczyk A , Alvear-Carrasco M , Reyes-Reyes A ((2018) ) Psychometric properties of the Brief-COPE for the evaluation of coping strategies in the Chilean population. Psicol Reflex Crit 31: , 22. |
[65] | Amoyal N , Fernandez AC , Ng R , Fehon DC ((2016) ) Measuring coping behavior in liver transplant candidates: A psychometric analysis of the brief cope. Prog Transplant 26: , 277–285. |
[66] | di Mattei VE , Carnelli L , Bernardi M , Bienati R , Brombin C , Cugnata F , Rabaiotti E , Zambetti M , Sarno L , Candiani M , Gentilini O ((2018) ) Coping mechanisms, psychological distress, and quality of life prior to cancer genetic counseling. Front Psychol 9: , 1218. |
[67] | Telles-Correia D , Barbosa A , Mega I , Mateus E , Monteiro E ((2009) ) Psychosocial determinants of quality of life 6 months after transplantation: Longitudinal prospective study. Transplant Porc 41: , 898–900. |
[68] | Golfieri L , Lauro A , Tossani E , Sirri L , Dazzi A , Zanfi C , Vignudelli A , Amaduzzi A , Cucchetti A , la Barba G , Pezzoli F , Ercolani G , Vivarelli M , del Gaudio M , Ravaioli M , Cescon M , Grazi GL , Grandi S , Pinna AD ((2007) ) Coping strategies in intestinal transplantation. Transplant Proc 39: , 1992–1994. |
[69] | Burker EJ , Madan A , Evon D , Finkel JB , Mill MR ((2009) ) Educational level, coping, and psychological and physical aspects of quality of life in heart transplant candidates. Clin Transplant 23: , 233–240. |
[70] | Matud MP ((2004) ) Gender differences in stress and coping styles. Pers Individ Dif 37: , 1401–1415. |
[71] | Emslie C , Fuhrer R , Hunt K , MacIntyre S , Shipley M , Stansfeld S ((2002) ) Gender differences in mental health: Evidence from three organisations. Soc Sci Med 54: , 621–624. |
[72] | Broadstock M , Michie S , Marteau T ((2000) ) Psychological consequences of predictive genetic testing: A systematic review. Eur J Hum Genet 8: , 731–738. |
[73] | Brown A ((2003) ) Handbook of religion and health. Harold G. Koenig, Michael E. McCullough, David B. Larson 2001. Oxford University Press. Oxford: ISBN 019511866-9. Spiritual Health Int 4: , 55. |
[74] | Smith TB , McCullough ME , Poll J ((2003) ) Religiousness and depression: Evidence for a main effect and the moderating influence of stressful life events. Psychol Bull 129: , 614–636. |
[75] | Henderson M , Harvey SB , Øverland S , Mykletun A , Hotopf M ((2012) ) Work and common psychiatric disorders. J R Soc Med 105: , 198–207. |
[76] | Holubova M , Prasko J , Hruby R , Latalova K , Kamaradova D , Marackova M , Slepecky M , Gubova T ((2016) ) Coping strategies and self-stigma in patients with schizophrenia-spectrum disorders. Patient Prefer Adherence 10: , 1151–1158. |
[77] | Li Q , Lin Y , Xu Y , Zhou H ((2018) ) The impact of depression and anxiety on quality of life in Chinese cancer patient-family caregiver dyads, a cross-sectional study. Health Qual Life Outcomes 16: , 230. |
[78] | Hu P , Yang Q , Kong L , Hu L , Zeng L ((2018) ) Relationship between the anxiety/depression and care burden of the major caregiver of stroke patients. Medicine 97: , e12638. |
[79] | Carver CS , Scheier MF , Weintraub KJ ((1989) ) Assessing coping strategies: A theoretically based approach. J Pers Soc Psychol 56: , 267–283. |
[80] | Afshar H , Roohafza HR , Keshteli AH , Mazaheri M , Feizi A , Adibi P ((2015) ) The association of personality traits and coping styles according to stress level. J Res Med Sci 20: , 353–358. |
[81] | Orzechowska A , Zajaczkowska M , Talarowska M , Gałecki P ((2013) ) Depression and ways of coping with stress: A preliminary study. Med Sci Monit 19: , 1050–1056. |
[82] | Hussenoeder FS , Jentzsch D , Matschinger H , Hinz A , Kilian R , Riedel-Heller SG , Conrad I ((2021) ) Depression and quality of life in old age: A closer look. Eur J Ageing 18: , 75–83. |
[83] | Geldsetzer P , Vaikath M , Wagner R , Rohr JK , Montana L , Gómez-Olivé FX , Rosenberg MS , Manne-Goehler J , Mateen FJ , Payne CF , Kahn K , Tollman SM , Salomon JA , Gaziano TA , Bärnighausen T , Berkman LF ((2019) ) Depressive symptoms and their relation to age and chronic diseases among middle-aged and older adults in rural South Africa. J Gerontol A Biol Sci Med Sc 74: , 957–963. |
[84] | Tsaur SH , Tang YY ((2012) ) Job stress and well-being of female employees in hospitality: The role of regulatory leisure coping styles. Int J Hosp Manag 31: , 1038–1044. |
[85] | Iwasaki Y ((2001) ) Contributions of leisure to coping with daily hassles in university students’ lives. Can J Behav Sci 33: , 128–141. |
[86] | Hamilton NA , Ingram RE ((2015) ) Self-Focused Attention and Coping: Attending to the right things. In Coping with stress: Effective people and processes, Snyder CR, ed. Oxford University Press, New York, pp. 178–195. |
[87] | Quoidbach J , Mikolajczak M , Gross JJ ((2015) ) Positive interventions: An emotion regulation perspective. Psychol Bull 141: , 655–693. |
[88] | Waugh CE , Shing EZ , Furr RM ((2020) ) Not all disengagement coping strategies are created equal: Positive distraction, but not avoidance, can be an adaptive coping strategy for chronic life stressors. Anxiety Stress Coping 33: , 511–529. |
[89] | Steinbart EJ , Smith CO , Poorkaj P , Bird TD ((2001) ) Impact of DNA testing for early-onset familial Alzheimer disease and frontotemporal dementia. Arch Neurol 58: , 1828–1831. |
[90] | Carlson MDA , Morrison RS ((2009) ) Study design, precision, and validity in observational studies. ,. J Palliat Med 12: , 77–82. |
[91] | Hamilton M ((1960) ) A rating scale for depression. J Neurol Neurosurg Psychiatry 23: , 56–62. |
[92] | Hamilton M ((1959) ) The assessment of anxiety states by rating. Br J Med Psychol 32: , 50–56. |
[93] | Patch C , Middleton A ((2018) ) Genetic counselling in the era of genomic medicine. Br Med Bull 126: , 27–36. |
[94] | Abacan MA , Alsubaie L , Barlow-Stewart K , Caanen B , Cordier C , Courtney E , Davoine E , Edwards J , Elackatt NJ , Gardiner K , Guan Y , Huang LH , Malmgren CI , Kejriwal S , Kim HJ , Lambert D , Lantigua-Cruz PA , Lee JMH , Lodahl M , Lunde Å , Macaulay S , Macciocca I , Margarit S , Middleton A , Moldovan R , Ngeow J , Obregon-Tito AJ , Ormond KE , Paneque M , Powell K , Sanghavi K , Scotcher D , Scott J , Juhé CS , Shkedi-Rafid S , Wessels TM , Yoon SY , Wicklund C ((2019) ) The global state of the genetic counseling profession. Eur J Hum Genet 27: , 183–197. |


