
Challenging Cases in Urothelial Cancer: Case 33
A 75 year old previously healthy woman was admitted to the hospital with a urinary tract infection which required one week admission. As part of the investigation, she had a CT scan of the abdomen and pelvis which revealed a mass in the anterior portion of the urinary bladder.
Her past medical history indicates only surgery for an ectopic pregnancy and a total abdominal hysterectomy for benign disease.
She smoked cigarettes for five years when she was in her 20 s.
She was seen as outpatient following recovery from the UTI and based upon the CT scan, she underwent flexible cystoscopy which revealed a solitary 3 cm tumor in the posterior portion of the bladder. It was thought to be confined to the surface. She was subsequently taken to the operating room where an uneventful transurethral resection of the bladder tumor was performed. The tumor was exophytic and papillary. It was thought to be confined to the urothelium. (Figs. 1-2). The impression was that this was a complete resection. (Fig. 3).
Figs. 1-2
Papillary solitary 3–4 cm tumor posterior wall.
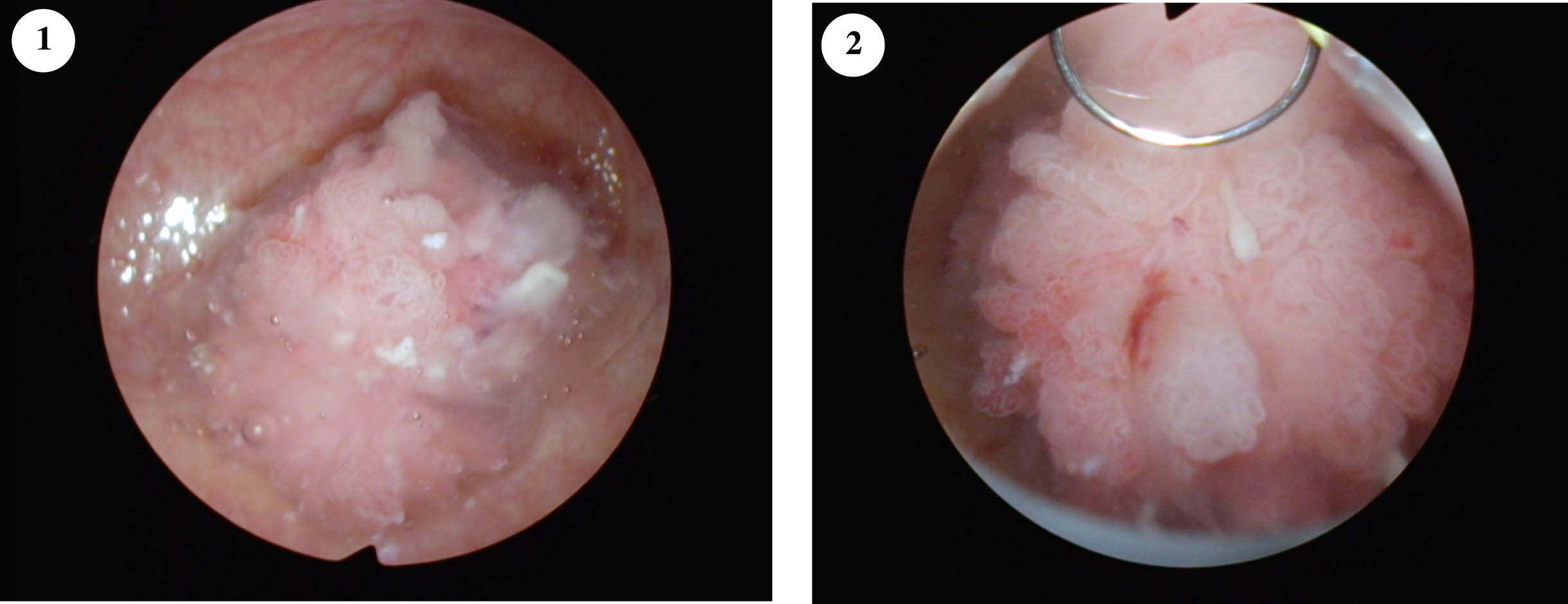
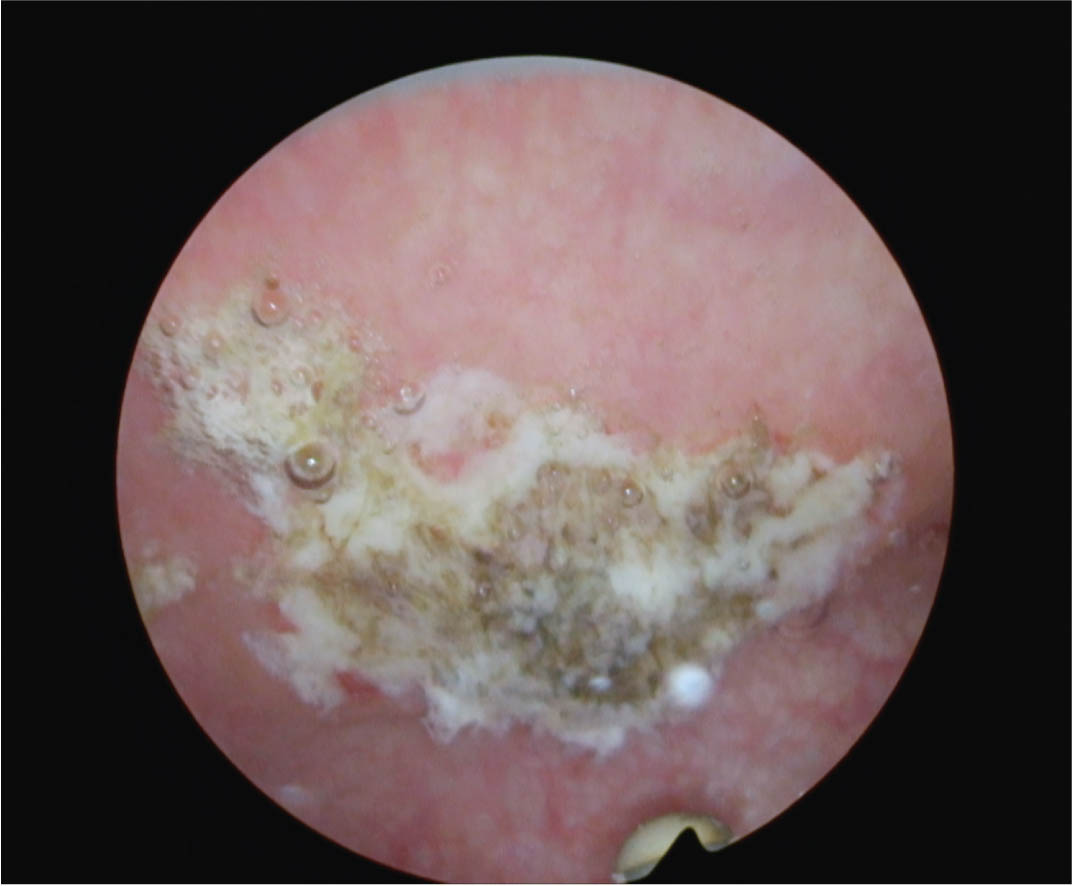
Fig. 3
Post TUR BT. Cauterized area post resection.
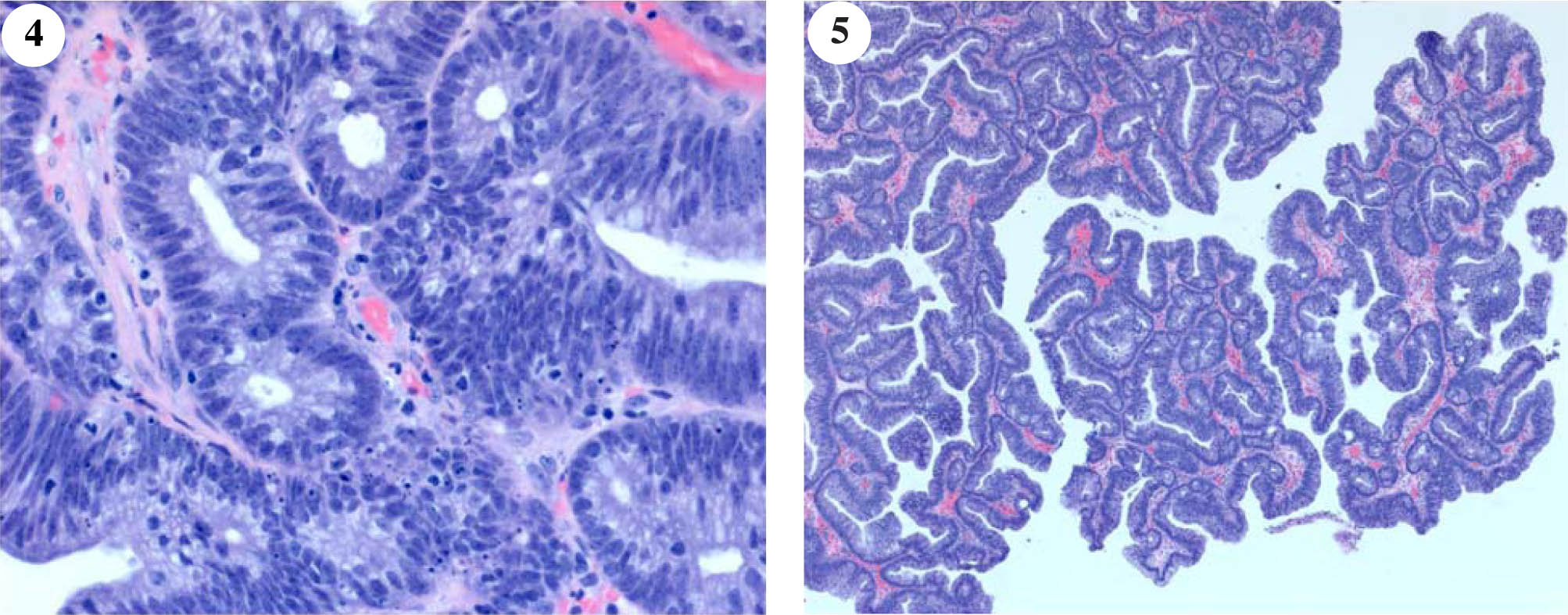
At the time of cystoscopy urine was obtained for cytology and was negative for high-grade tumor cells. The resection specimen from the tumor indicated this to be a tubulovillous adenoma with high-grade dysplasia. (Figs. 4-5). There was no invasion.
Figs. 4-5
Histology of the tubulovillous adenoma of the bladder. Description in the text.
There was no muscle in the specimen.
Tubulovillous adenoma of the urinary bladder is similar to colorectal tubulovillous adenoma. A tubular/villous microscopic architecture is noted, with dysplastic epithelium showing nuclear pleomorphism, hyperchromasia, and elongated nuclei arranged in a pseudo stratified columnar fashion. Dysplasia maybe high-grade with the circular nuclei, nucleoli, loss of polarity, cribiform architecture and necrosis. Immunohistochemical staining demonstrates an intestinal-type phenotype. Thus, this lesion was positive for CDX2, CK20 and Villin-1.
One month after the initial TUR BT the patient had a flexible cystoscopy which indicated that there was tumor present at the previous site in the posterior wall of the bladder. An MRI confirmed a small 1.4 cm mass which suggested that this was a urachal tumor. (Figs. 6-8).
Figs. 6-8
Post initial TUR BT imaging indicating mass involving the urachus.

The patient subsequently underwent a robot assisted partial cystectomy with the resultant pathology once again indicating a tubulovillous adenoma with high-grade dysplasia and no invasive carcinoma. Margins were negative.
This is a very rare neoplasm and should be differentiated from an adenocarcinoma.
AUTHOR CONTRIBUTIONS
MSS contributed to the work conception, performance, analysis of data and writing; NAA and NP supplied the histology description and the photos of the pathology.
INFORMED CONSENT
Written informed consent for publication was obtained from the patients.
ETHICAL CONSIDERATIONS
The author has institutional review board approval for reviewing bladder cancer cases for outcome (MHS.2020.026).
CONFLICT OF INTEREST
MSS, NAA and NP have nothing to disclose.


