
The Impact of Physical Activity on Risk and Health-Related Quality of Life in Bladder Cancer
Abstract
BACKGROUND:
Sedentarism is an important modifiable risk factor in the struggle against cancer. In the last decades, the relationship between physical activity and different types of cancer has been investigated in depth.
OBJECTIVE:
To provide an overview of the literature on the effectiveness of physical activity in reducing the risk to develop bladder cancer and improving health-related quality of life in patients.
METHODS:
A systematic review was conducted through a search of the Embase, Cochrane, PubMed, Scopus, and Web of Science (WOS) databases to seek information and PRISMA system to delimitate the research. Outcomes included in searches were physical activity, tobacco consumption, obesity, body mass index, and metabolic syndrome, associated with bladder cancer and quality of life.
RESULTS:
Database searches identified 394 records, of which 75 were duplicated. A total of 280 articles were excluded based on abstract screening. An additional 16 full-text articles were excluded because they did not meet the eligibility criteria. Overall, 21 of the 23 studies included in the review reported beneficial effects of physical activity in bladder cancer. The majority of papers found that physical activity is a significant factor in reducing the risk of bladder cancer. Moreover, physical activity improves health-related quality of life in bladder cancer survivors, and diminishes both recurrence and mortality in those who engage in regular activity. Lastly, physical inactivity is associated with increased body mass index, obesity, metabolic syndrome, type 2 diabetes and unfavourable energy balance, which led to a greater probability of suffering from bladder cancer.
CONCLUSIONS:
These data reinforce the importance of promoting a healthy lifestyle to reduce the risk of bladder cancer and to improve survivorship and health-related quality of life of patients.
INTRODUCTION
Bladder cancer (BC) is among the top ten most prevalent cancers worldwide. Europe, North Africa, and the Middle East have the highest incidence rate, with 17 cases per 100,000 person-years. East Asia, including China, registers the least incidence rate with 6 cases per 100,000 person-years [1, 2]. The most common type of BC is urothelial carcinoma, and its mortality rate has increased in the last decades [2]. With such a high prevalence (at least 600,000 cases per year in the US alone) and the high cost of treatment programmes, this cancer is fast becoming one of the most expensive to treat [1, 3].
Two clinical phenotypes of BC have been established, depending on the tumour size, lymph node, and metastasis: non-muscle invasive BC (NMIBC) and muscle invasive BC (MIBC) [4]. Both have a different prognosis and, consequently, each one is managed in a very distinct way [5]. NMIBC has a high percentage of local recurrence [6], but a low risk of metastasis and death. Thus, the first priority with this type of cancer is its early detection with subsequent follow-up to treat local recurrences. This treatment requires regular hospitalisation which implies both very high medical costs and a decrease in patients quality of life [7, 8]. On the other hand, MIBC, with its higher risk of metastasis, requires invasive therapies such as radical cystectomy, radiotherapy in the bladder, and systemic chemotherapy, all of which have a major effect on quality of life [9].
Many different risk factors influence the development and recurrence of both BC clinical phenotypes. Of these, tobacco consumption is the most important, being responsible for a third of diagnoses [3, 10]. Industrial colorants [11], diesel fumes [11], body mass index (BMI) [8, 12–14], obesity [11], metabolic syndrome (MetS) [15, 16], and alcohol consumption [12, 16–18], are also associated with a higher risk of developing BC [11]. Finally, sedentarism is among the many modifiable risk factors for BC, with evidence suggesting that physical activity (PA) both improves survival rates and patient quality of life [11, 19].
The relationship between PA and risk for several different types of cancer has been investigated in depth [20, 21]. In recent years, it has become clear that PA reduces the risk for colorectal, mammary and endometrial cancers [18, 22]. However, regarding urological cancer data are limited and there seems to have been a less awareness of the importance of being adherent to PA [23, 24]. A systematic review on lifestyle factors and quality of life in BC survivors concluded that evidence of a positive association between quality of life and PA was small and that further studies were required [4]. Data now available suggest that moderate to intense PA has a positive effect on health, survivorship, and quality of life among BC patients [14, 25]. There is a growing recognition of how PA can influence the postoperative recovery of patients undergoing radical cystectomy [26–29], and that it has a role in reducing the mortality risk [10]. The results of some studies, however, are inconsistent with these findings, which may be due to inadequate adjustment for confounding lifestyle factors such as smoking [30].
The purpose of this systematic literature review is to explore the current knowledge about the relationship between PA and BC, and to identify whether available evidence supports the hypothesis that PA reduces the likelihood of developing BC and can improve health-related quality of life in BC survivors.
METHODS
Search strategy
The article search was conducted using the electronic databases Cochrane, Embase, PubMed, Scopus, and Web of Science (WOS) in July 2020. Mesh terms used were “bladder cancer AND physical activity” with the“[All fields]” tag in Embase search, the “[Title, Abstract, Keyword]” tag in Cochrane search, the “[All fields]” tag in PubMed search; the fields [Article title, Abstract, Keywords] in Scopus search and “[Topic]” in WOS search.
All searches were performed using various inclusion criteria. After eliminating duplicate articles, the title of each article and its abstract were read, eliminating those that were not related to the descriptor used (bladder cancer and physical activity). Subsequently, the selected articles were analysed in full text, excluding those that met specific exclusion criteria.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: had been published in English between 2010 and July 2020, were a pilot studies or case studies, investigated the effects of PA or concerned quality of life improvement, and involved adult patients.
Studies were excluded if they were systematic reviews, animal studies, conference proceedings or congress communications, book chapters, or interviews.
Screening and data extraction
Titles were screened for inclusion according to the aforementioned criteria. After reading the abstracts of potentially eligible publications, some of them were removed following the inclusion and exclusion criteria, and the others were full–text read before selecting them. Finally, data were extracted from all eligible articles including the name of the first author, year of publication, experimental protocol, and outcomes (Table 1).
Table 1
Characteristics of studies and main findings
| Author (s), year, evidence level and quality rating | Type and number of subjects | Experimental protocol | Main findings |
| Blanchard, 2010 (35) Level III–C | 3,241 cancer survivors, including 201 BC | PA measured with the Godin Leisure-Time Exercise Questionnaire. QL using the RAND-36 | Aerobic exercise levels had a positive association with BMI in survivors of BC |
| Lin, 2010 (33) Level II–B | 803 BC patients, control group 803 subjects | Risk factor questionnaire, including PA through METs | High energy consumption and low PA were associated with a significantly increased risk of BC |
| Parent, 2011 (25) Level II–A | 3,549 cancer survivors, including 484 BC | Interview-questionnaire to calculate the average time worked and recreational PA with METs | The practice of recreational PA decreased the risk of developing BC |
| Fung, 2014 (36) Level III–B | 1,476 BC patients older than 65 years | QL measured by the PCS and MCS of the SF–36 or VR–12 | Higher risk for clinical QL differences in patients who had 4 or more comorbid medical conditions and 1 or more deficits in daily living activity |
| Porserud, 2014 (26) Level I–B | 18 BC patients with radical cystectomy | Exercise program for 12 weeks with group exercise training twice a week and daily walks. QL measured by the SF–36 | The training program increased physical function and positively affected the QL |
| Roswall, 2014 (12) Level III–B | 390,878 subjects, including 1,391 BC | Questionnaires about lifestyle habits and occupation (work) history | For men, there was a significant association between weight and BC |
| Wyszynski, 2014 (8) Level III–B | 726 BC patients, smokers, and overweight or obesity | Questionnaires covering sociodemographic, medical, and personal aspects, including PA | Interventions promoting weight reduction, such as practising PA, improve overall health and longevity. |
| Montella, 2015 (15) Level I–B | 690 BC patient, control group 665 healthy subjects | Questionnaire about healthy lifestyle habits, including daily PA | A positive relationship between smoking and metabolic syndrome with the risk of BC |
| Xu, 2015 (16) Level II–B | 972 BC patients, control group 1,098 healthy subjects | Dataset collected including lifestyle habits and serum samples | A remarkable correlation between higher BMI, MetS, diabetes, hy-pertriglyceridemia, and tobacco consumption with BC risk |
| Moore, 2016 (22) Level III–A | 1.44 million of participants with 186,932 types of cancer | Leisure time PA measured in METs by different validated questionnaires | A significant inverse correlation between the practice of PA and the reduction of the risk of 13 cancers, including BC. |
| Cannioto, 2017 (14) Level I–B | 208 BC patients, control group 766 subjects without cancer but with other illnesses | Questionnaire (PEDS) to evaluate factors related to QL, including PA | A positive correlation between the lack of recreational PA with the development of BC |
| Gopalakrishna, 2017 (4) Level III–A | 472 subjects with a mean age of 74 years | Questionnaires to measure QL (FACT-BI) and leisure time PA (IPAQ) | Physically active BC survivors at stage 0 to 2 in the long-term tend to have a health-related QL comparable to the rest of the population |
| Liss, 2017 (10) Level II–B | 222,163 participants with 83 cancer types | National Health Survey to collect lifestyle habits, including PA | A 47% decrease in BC deaths in individuals who engaged in some form of exercise compared to those who were inactive |
| Reulen, 2017 (34) Level II–B | 260 patients with prostate cancer, 438 with BC, control group of 427 people | Leisure time PA measured by the IPAQ | PA was associated with a decreased risk of prostate cancer, but not with BC |
| Robsahm, 2017 (32) Level I–B | 2,341 men 86 % healthy and 14 % with cancer, diabetes or cardiovascular, pulmonary, renal, or liver illnesses | Cardiorespiratory fitness measured by a 6 minutes bicycle test until exhaustion | High cardiorespiratory fitness was associated with a significant trend for lower risk of BC and cancer of the breast or pancreas |
| Bae, 2018 (13) Level III–A | 205,348 men: 35,7% normal weight and 35,1 % obese | Questionnaire about lifestyle, including PA | Men with a higher BMI, more likely to be physically inactive, are more likely to develop BC |
| Banerjee, 2018 (27) Level I–A | 60 BC patients with BC, control group 60 healthy subjects | Pre-operative vigorous intensity aerobic interval exercise 3–6 weeks | A very positive influence of the program on postoperative recovery |
| Banerjee, 2019 (28) Level III–B | 24 BC patients with radical cystectomy, control group 23 subjects | Pre-operative vigorous intensity aerobic interval exercise | Positive patient perspectives of exercise prehabilitation |
| Ihira, 2019 (37) Level III–A | 76,795 men with urological cancer, 373 with BC | Questionnaires to calculate the risk of urological cancer, including PA | People who practice PA in free time reduce non significantly the probability of developing BC and kidney cancer |
| Westhoff, 2019 (3) Level III–B | 969 patients with NMIBC | Questionnaire about awareness of risk factors and adherence to lifestyle recommendations | Patients who were aware of physical inactivity as a risk factor adhered in a greater percentage to recommendations for a healthy lifestyle |
| Chung, 2020 (17) Level II–B | 586 BC patients | PA measured by the Godin Leisure Time Exercise Questionnaire. QL using the Bladder Utility Symptom Scale (BUSS) | A lower weekly PA level, tobacco consumption, and a higher BMI associated with a higher recurrence or metastasis in BC |
| Hektoen, 2020 (30) Level III–A | 152,505 participants, 1,584 with NMIBC y 394 with MIBC | Analytic dataset and questionnaire data from the Janus Cohort. Leisure time PA measured by the IPAQ | PA decreases the risk of this cancer in non-smoking men and in non-smoking and ex-smoking women |
| Li, 2020 (18) Level I–A | 148,288 women, of whom 817 developed BC | Questionnaires to measure PA in METs | The amount of moderate to vigorous PA was inversely associated with the incidence of BC |
BC: bladder cancer; BMI: body mass index; METs: metabolic equivalents; PA: physical activity; QL: quality of life; level I: experimental study or randomized controlled trial (RCT); level II: quasi-experimental study; level III: non-experimental study; A: high quality; B: good quality; C: low quality.
Study quality assessment
Study quality was assessed using the Johns Hop-kins Hospital/The Johns Hopkins University Evidence Level and Quality Guide [31]. Articles were scored according to evidence levels based upon the type of article or research design. Six of the 23 publications (26%) were at level I: experimental study, randomized controlled trial (RCT), or systematic review of RCTs with or without meta-analysis [14, 15, 18, 26, 27, 32]. A further six studies (26%) were at level II: quasi-experimental studies, systematic review of a combination of RCTs and quasi-experimental studies, or quasi-experimental studies only, with or without meta-analysis [10, 19, 20, 30, 33, 34]. The remaining 11 publications (48%) were at level III: non-experimental study, and non-experimental studies only, with or without meta-analysis, or qualitative study or systematic review of qualitative studies with or without meta-synthesis [3, 4, 8, 12, 13, 22, 28, 30, 35–37]. Studies rated at levels IV (opinion of respected authorities, committees, and consensus panels) and V (quality improvement program evaluation, case reports) were not included in this review. According to the quality guides associated with evidence levels I to III, 8 articles were high quality (A), 14 articles were good quality (B) and 1 study was low quality or contained major flaws (C) due to the need of a larger sample size.
RESULTS
Literature search
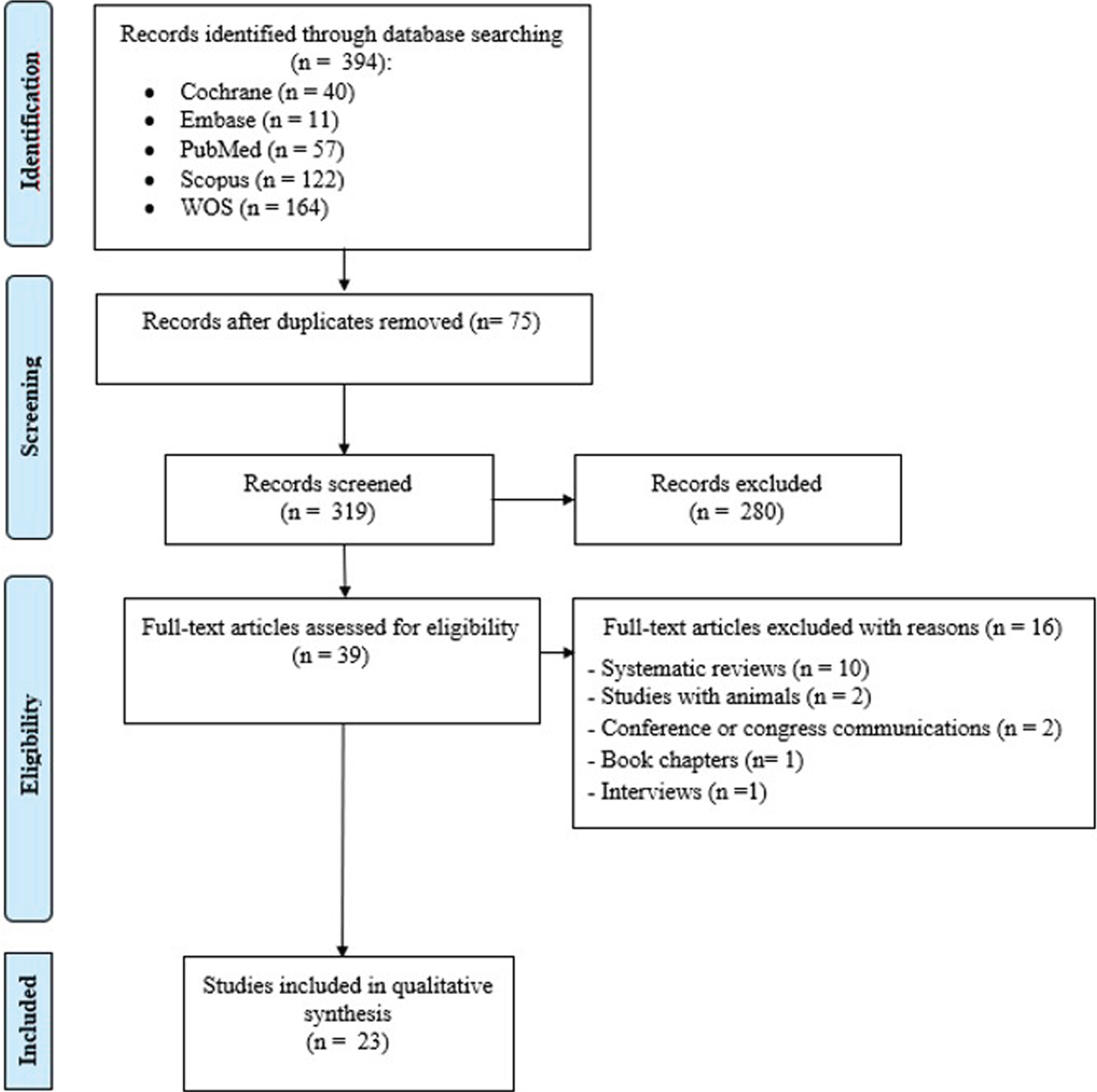
Study selection was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) system, as it is described in Fig. 1. A total of 394 articles were obtained in the database search, of which 40 articles were from Cochrane, 11 from Embase, 57 from PubMed, 122 from Scopus, and 164 from WOS. After identifying and removing duplicates, 319 underwent title and abstract screening, leading to the decision to exclude 280 articles as they did not meet our inclusion criteria. The remaining 39 articles were full text screened with the result that 16 were discarded due to the following reasons: 10 were systematic reviews, 2 were animal studies, 2 were conference communications, 1 was a book chapter and the last was an interview. In total, 23 studies met the eligibility criteria and were included in this systematic review.
Fig. 1
Flow diagram of the study selection process following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Description of studies
Table 1 summarizes the main characteristics of the articles included in this review. Of the 23 studies analysed, 13 were published in the last 5 years. In 3 of these studies, the primary focus is on tobacco as a risk factor for BC. 5 studies involved patients with MIBC (radical cystectomy), and another 5 focused on NMIBC. The hypothesis that high BMC is a risk factor for BC is presented and confirmed in 5 studies. 7 investigations focused on obesity as a risk factor for BC. 3 studies confirm the positive correlation between MetS and BC. In 2 investigations the object of study were modifiable risk factors for BC. One study involved an analysis of the effects of PA in postmenopausal women with BC. All studies, directly or indirectly, investigate PA and its role in the prevention of BC.
Summary of findings
Quality of life, measured using the SF-36 ort the VR-12, differed between MIBC and NIMBC patients, with a better physical function, a higher vitality, and lower corporal pain in the second [36]. Using the FACT-BI questionnaire findings show that NMIBC patients in stages 0 to 2 report a quality of life similar to that of the rest of the population [4]. In addition, adherence to a PA program is found to be higher (70 %) among NMIBC patients aware that sedentarism is a BC risk factor [3].
The results of two randomized controlled trials prove the potential benefits of exercise training programs for MIBC patients. The first of these, a study with 60 BC patients awaiting a radical cystectomy shows improvements in cardiovascular function for pre-operative patients attending a supervised twice-weekly, vigorous intensity aerobic interval exercise for 3–6 weeks. These results could have important implications for post-operative recovery [27]. The second, involving 18 MIBC patients who had recently undergone radical cystectomy, looks at the effects of a 12-week program of lower extremities strength and endurance training. Although the training programme was not a feasible option for all patients due to poor post-operative health status, compared to controls patients in the intervention group (n = 5) reported both long and short term increases in functional capacity and in the SF36 role physical domain [26].
According to many studies, PA is a factor in preventing BC. Based in self-reported data, individuals with a high energy intake and low PA levels have 22-fold increase in their risk of developing BC compared to individuals with a balanced energy intake and high PA levels [33]. Indeed, active people who recognize to practice recreative PA reduce the risk of BC from 20 to 40 % [25] and the risk is also low in people who have a high cardiorespiratory condition measured by a maximal exercise bicycle test [32]. Furthermore, engaging in recreational PA is also linked to lower BC risk [15]. Higher levels of PA are correlated with lower levels of BC recurrence and metastasis [17], and in a study carried out in a group of postmenopausal women, it was demonstrated that those patients recognizing to practice moderate to vigorous PA had the lowest level of BC recurrence [18]. Furthermore, individuals who self-report any form of exercise are found to be 47% less likely to die from BC than those who do not exercise [10].
However, 2 of 23 studies analysed, both carried out in Asia, are the cause of some controversy with regards to correlations between BC and PA levels. One, a long corpus Japanese study, used a self-administered questionnaire and found that, although recreational PA appears to reduce the risk for both bladder and kidney cancer, results are not statistically significant [37]. The other is a Chinese hospital-based case-control study that used the IPAQ to assess PA levels, and came to the conclusion that there is no relationship between PA and the development of BC [34].
DISCUSSION
The studies analysed show a great heterogeneity regarding subjects and hypotheses. In many cases, a comparison was made between the group of patients to be evaluated (cases) and a control group [14–16, 26–28, 30, 33, 34]. Most, performed in hospitals, investigated patients with common cancers, including BC. The vast majority of subjects were men. The age of participants varied greatly from study to study: from 18 years upwards [17, 22], between 40 and 59 years old [32], between 45 and 74 years old [37] and between 64 and 78 years old [26]. In addition to the BC, studies included other evaluable criteria, such as obesity, BMI, tobacco consumption, frequency and intensity of PA, type of BC, MetS, energetic balance, and race. In some cases, the objective of the study was to analyze BC risk factors, including: obesity [10, 13, 14, 16, 33], BMI [8, 12-14, 17, 35], tobacco consumption [8, 10, 14, 13–18, 30, 37], physical inactivity [14, 17, 18, 30], MetS [15, 16], and energy balance [33]. In other cases research was aimed at showing the benefits of PA in different categories of patients, such as those with NMIBC at stages 0 and 1, or those with a better prognosis and physical condition [3, 4, 16, 30, 36]. Lastly, in one study the purpose was to compare the benefits of PA programs [27] in MIBC patients undergoing a radical cystectomy, reporting improvements in their physical function and quality of life.
Concerning different categories of PA, several types were analysed: occupational, recreational, domestic or active transport, and intensities also varied: low, moderate, high, and vigorous [4]. In most cases, with studies carried out with patient groups in different countries (Table 2), validated questionnaires were used to assess levels of PA among participants [3, 4, 8, 10, 12, 113–15, 22, 28, 30, 33–37] (Table 2). In general, studies saw a significant correlation between engaging in PA and decreased risk of BC. However, there were two exceptions involving investigations carried out with Asian patients. One showed that there is no relationship between self-reported PA and the risk of developing BC [34]. The other revealed that the decrease in BC risk for people who engaged in sports or recreational PA was not statistically significant either [37] (Table 2). These two studies apart, findings show that PA not only helps to prevent cancer in active subjects, but also improves the quality of life in subjects suffering from BC, both MIBC [26–28, 36] and NMIBC [3, 4, 16, 30, 36]. Three studies, carried out in Sweden [26], South Korea [27], and Norway [32], involved specific training programs with both control and experimental groups, measuring physical condition before, during and after each program. Although the objectives of each study were slightly different, their conclusions confirmed the benefits of PA, showing that high levels of PA can reduce the risk of BC [32]; and that PA can improve the health-related quality of life of BC patients, increase their physical function [26] and contribute to a better postoperative recovery [27].
Table 2
Relationship between PA and effects on BC, according to the origin of participants and study design
| Author (s), year | Origin of participants | Study design | Correlation between PA and reducing BC |
| Blanchard, 2010 (35) | United States | A national cross-sectional study |  |
| Lin, 2010 (33) | United States | A case-control study | |
| Parent, 2011 (25) | Canada | A multi-cancer population-based case-control | |
| Fung, 2014 (36) | United States | A cross-sectional study | |
| Porserud, 2014 (26) | Sweden | A pilot randomized controlled trial | |
| Roswall, 2014 (12) | Denmark, France, Germany, Greece, Italy, Netherlands, Norway, Spain, Sweden and United Kingdom | A prospective study | |
| Wyszynski, 2014 (8) | United States | A prospective cohort study | |
| Montella, 2015 (15) | Italy | A hospital-based case-control study | |
| Xu, 2015 (16) | China | A case-control study | |
| Moore, 2016 (22) | United States and Europe | A prospective cohort | |
| Cannioto, 2017 (14) | United States | A hospital-based case-control study | |
| Gopalakrishna, 2017 (4) | United States | A cross-sectional study | |
| Liss, 2017 (10) | United States | A cross-sectional study | |
| Reulen, 2017 (34) | China | A case-control study |  |
| Robsahm, 2017 (32) | Norway | A long-term prospective cohort study | |
| Bae, 2018 (13) | South Korea | A 10-year nationwide population-based observational study | |
| Banerjee, 2018 (27) | South Korea | A randomized controlled trial | |
| Banerjee, 2019 (28) | Sweden | A qualitative focus group study | |
| Ihira, 2019 (37) | Japan | A prospective study | |
| Westhoff, 2019 (3) | Netherlands | A cohort study | |
| Chung, 2020 (17) | United States, Canada | A cross-sectional study | |
| Hektoen, 2020 (30) | Norway | A prospective cohort study | |
| Li, 2020 (18) | United States | A prospective study of 3 clinical trials and an observational study | |
BC: bladder cancer; PA: Physical activity.
Most research, apart from the two Asian studies mentioned above [34, 37], shows that engaging in PA can decrease rates of BC recurrence [17]. The percentage risk reduction varies between studies from 20% to 60% [25, 32]. Additionally, in patients who have already developed the disease, those who engage in PA have a lower recurrence and mortality [10]. What is more, for NMIBC patients, engaging in PA correlates with an improved health-related quality of life in the short and medium terms, comparable to that reported by general population [3, 4]. MIBC patients who completed a preoperative training program, show better post-operative recovery than those who did not and also subsequently report better quality of life [26–28, 36].
An awareness of the benefits of PA appears encourage people to have healthy lifestyle habits [17, 30]. Indeed, the more frequently people engage in PA, better their lifestyle habits will be acquired. Thus, inactive people are more likely to have unhealthy lifestyle habits, such as sedentarism, unbalanced energy intake, or tobacco consumption. These lifestyle habits are in turn linked to a higher than recommended BMI, obesity, conditions such as MetS and ultimately BC, as a great deal of research now shows. Inactivity results in low caloric expenditure and thus an imbalance between energy intake and expenditure. Having such an energy imbalance has been shown to increase a person’s risk of developing BC [32]. Current and former smokers appear to have a higher risk of developing BC [3, 10, 15, 18, 30]; specifically, they are 7 times more likely to develop BC than individuals who have never smoked [15]. Concerning BMI, although a research found no connection between BMI and risk of developing BC [35], most studies conclude that people with a higher than recommended BMI are at a high risk of suffering from BC [14], and that there is a positive correlation between BMI, physical inactivity, and BC risk [8, 12-14]. In turn, BMI is closely related to obesity, factor that is also implicated in the appearance and recurrence of BC [8, 10, 13–16, 35]. Obesity can also lead to the development of MetS, which in diabetes sufferers considerably increases the risk of BC [15, 16, 30].
The present review has several limitations affecting the generalizability of results. The heterogeneity of the studies included here means that it was only possible to evaluate study outcomes in a narrative synthesis rather than by performing a meta-analysis. Thus, different components of effective interventions could not be compared. Moreover, several included studies imply a follow-up lasting for decades, with ongoing research as further data are recollected, patients progress or results are assessed. Nevertheless, and notwithstanding the need for further research, despite its shortcomings, this research supports the hypothesis that PA has beneficial effects in the prevention and treatment of BC.
CONCLUSION
Most studies suggest that PA is a factor in the prevention of BC in healthy subjects. In patients already suffering BC, both NMIBC and MIBC, leisure-time, occupational and recreational PA, and exercise training programs improve their health-related quality of life. Furthermore, in subjects awaiting radical cystectomy, a 12-week training program has been shown to aid postoperative recovery and short, medium, and long-term quality of life. Lower recurrence and mortality rates have also been reported. Lastly, physical inactivity causes collateral damage such as increased BMI, obesity, MetS, diabetes or an unfavourable energy balance, all of which lead to a greater probability of suffering from BC. However, further work is still necessary before it is possible to draw definitive conclusions concerning several of the above findings. Thus, follow-up work with large representative samples of BC survivors is required to a full evaluation of lifestyle factors as predictors of clinical outcomes in BC and to better establish independent and interactive associations between PA and other BC risk factors. This would enable better identification of target groups suitable for PA interventions. The use of standardized methods to measure PA and quality of life is also important to improve outcomes. Moreover, adequate powered clinical trials are required to confirm the benefits of pre-operative exercise for radical cystectomy. As a final point, appropriate forms of exercise which can lead to broad health benefits and feasible for all BC patients should be explored.
ACKNOWLEDGMENTS
M.R.C. was postgraduate student at the Universidad Internacional de Andalucía, Spain.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
Conception: MRC and JGG. Performance: MRC. Interpretation of data and drafting of manuscript: MRC, SMR and JGG.
ETHICAL CONSIDERATIONS
This study, as a literature review, is exempt from any requirement for Institutional Review Board approval. No human or animal research was involved in the elaboration of this manuscript.
CONFLICT OF INTEREST
MRC, SM and JGG have no conflicts of interest to report.
REFERENCES
[1] | Botteman MF , Pashos CL , Redaelli A , Laskin B , Hauser R . The health economics of bladder cancer. Pharmacoeconomics. (2003) ;21: (18):1315–30. doi: 10.1007/BF03262330. |
[2] | Siegel R , Ma J , Zou Z , Jemal A . Cancer statistics, 2014. Ca Cancer J Clin. (2014) ;64: (1):9–29. doi: 10.3322/caac.21208. |
[3] | Westhoff E , Kampman E , Aben KK , Hendriks IG , Witjes JA , Kiemeney LA , et al. Low awareness, adherence, and practice but positive attitudes regarding lifestyle recommendations among non-muscle-invasive bladder cancer patients. Urol Oncol. (2019) ;37: (9):573.e1–573.e8. doi: 10.1016/j.urolonc.2019.04.016. |
[4] | Gopalakrishna A , Longo TA , Fantony JJ , Harrison MR , Inman BA . Physical activity patterns and associations with health-related quality of life in bladder cancer survivors. Urol Oncol. (2017) ;35: (9):540.e1.–1540.e6. doi: 10.1016/j.urolonc.2017.04.016. |
[5] | Harshman LC , Preston MA , Bellmunt J , Beard C . Diagnosis of bladder carcinoma: A clinician’s perspective. Surg Pathol Clin. (2015) ;8: (4):677–85. doi: 10.1016/j.path.2015.07.004. |
[6] | Konety B , Isharwal S . Non-muscle invasive bladder cancer risk stratification. Indian J Urol. (2015) ;31: (4):289. doi: 10.4103/0970-1591.166445. |
[7] | Mossanen M , Gore JL . The burden of bladder cancer care: direct and indirect costs. Curr Opin Urol. (2014) ;24: (5):487–91. doi: 10.1097/MOU.0000000000000078. |
[8] | Wyszynski A , Tanyos SA , Rees JR , Marsit CJ , Kelsey KT , Schned AR , et al. Body mass and smoking are modifiable risk factors for recurrent bladder cancer. Cancer. (2014) ;120: (3):408–14. doi: 10.1002/cncr.28394. |
[9] | Sancho G , Maroto P , Palou J . Current management of muscle-invasive bladder cancer. Clin Transl Oncol. . (2011) ;13: (12):855–61. doi: 10.1007/s12094-011-0746-2. |
[10] | Liss MA , White M , Natarajan L , Parsons JK . Exercise decreases and smoking increases bladder cancer mortality. Clin Genitourin Cancer. (2017) ;15: (3):391–5. doi: 10.1016/j.clgc.2016.11.006. |
[11] | Freedman ND , Silverman DT , Hollenbeck AR , Schatzkin A , Abnet CC . Association between smoking and risk of bladder cancer among men and women. JAMA. (2011) ;306: (7):737–45. doi: 10.1001/jama.2011.1142. |
[12] | Roswall N , Freisling H , Bueno-de-Mesquita HB , Ros M , Christensen J , Overvad K , et al. Anthropometric measures and bladder cancer risk: A prospective study in the EPIC cohort. Int J Cancer. (2014) ;135: (12):2918–29. doi: 10.1002/ijc.28936. |
[13] | Bae WJ , Choi JB , Moon HW , Park YH , Cho HJ , Hong S-H , et al. Influence of diabetes on the risk of urothelial cancer according to body mass index: A 10-year nationwide population-based observational study. J Cancer.. (2018) ;9: (3):488–93. doi: 10.7150/jca.22107. |
[14] | Cannioto R , Etter JL , Guterman LB , Joseph JM , Gulati NR , Schmitt KL , et al. The association of lifetime physical inactivity with bladder and renal cancer risk: A hospital-based case-control analysis. Cancer Epidemiol. (2017) ;49: :24–9. doi: 10.1016/j.canep.2017.04.017. |
[15] | Montella M , Di Maso M , Crispo A , Grimaldi M , Bosetti C , Turati F , et al. Metabolic syndrome and the risk of urothelial carcinoma of the bladder: A case-control study. BMC Cancer. (2015) ;15: (1):720. doi: 10.1186/s12885-015-1769-9. |
[16] | Xu S , Zhang G-M , Guan F-J , Dong D-H , Luo L , Li B , et al. The association between metabolic syndrome and the risk of urothelial carcinoma of the bladder: A case-control study in China. World J Surg Oncol. (2015) ;13: (1):236. doi: 10.1186/s12957-015-0631-5. |
[17] | Chung J , Kulkarni GS , Bender J , Breau RH , Guttman D , Maganti M , et al. Modifiable lifestyle behaviours impact the health-related quality of life of bladder cancer survivors. BJU Int. (2020) ;125: :836–42. doi: 10.1111/bju.15007. |
[18] | Li Y , Hendryx MS , Xun P , He K , Shadyab AH , Lane DS , et al. Physical activity and risk of bladder cancer among postmenopausal women. Int J Cancer. 2020; doi: 10.1002/ijc.33042. |
[19] | Campbell PT , Newton CC , Dehal AN , Jacobs EJ , Patel AV , Gapstur SM . Impact of body mass index on survival after colorectal cancer diagnosis: The Cancer Prevention Study-II Nutrition Cohort. J Clin Oncol. (2012) ;30: (1):42–52. doi: 0.1200/JCO.2011.38.0287. |
[20] | Friedenreich CM , Neilson HK , Lynch BM . State of the epidemiological evidence on physical activity and cancer prevention. Eur J Cancer. (2010) ;46: (14):2593–604. doi: 10.1016/j.ejca.2010.07.028. |
[21] | Leitzmann MF . Physical activity and genitourinary cancer prevention. Recent Results Cancer Res. (2011) ;186: :43–71. doi: 10.1007/978-3-642-04231-7_3. |
[22] | Moore SC , Lee IM , Weiderpass E , Campbell PT , Sampson JN , Kitahara CM , et al. Association of leisure-time physical activity with risk of 26 types of cancer in 1. 44 million adults. JAMA Intern Med. (2016) ;176: (6):816–25. doi: 10.1001/jamainternmed.2016.1548. |
[23] | Wolin KY , Stoll C . Physical activity and urologic cancers. Urol Oncol. (2012) ;30: (5):729–34. doi: 10.1016/j.urolonc.2012.07.009. |
[24] | Jones LW , Courneya KS . Exercise discussions during cancer treatment consultations. Cancer Pract. (2002) ;10: (2):66–74. doi: 10.1046/j.1523-5394.2002.102004.x. |
[25] | Parent M-É , Rousseau M-C , El-Zein M , Latreille B , Désy M , Siemiatycki J . Occupational and recreational physical activity during adult life and the risk of cancer among men. Cancer Epidemiol. (2011) ;35: (2):151–9. doi: 10.1016/j.canep.2010.09.004. |
[26] | Porserud A , Sherif A , Tollbäck A . The effects of a physical exercise programme after radical cystectomy for urinary bladder cancer. A pilot randomized controlled trial. Clin Rehabil. (2014) ;28: (5):451–9. doi: 10.1177/0269215513506230. |
[27] | Banerjee S , Manley K , Shaw B , Lewis L , Cucato G , Mills R , et al. Vigorous intensity aerobic interval exercise in bladder cancer patients prior to radical cystectomy: A feasibility randomised controlled trial. Support Care Cancer. . (2018) ;26: (5):1515–23. doi: 10.1007/s00520-017-3991-2. |
[28] | Banerjee S , Semper K , Skarparis K , Naisby J , Lewis L , Cucato G , et al. Patient perspectives of vigorous intensity aerobic interval exercise prehabilitation prior to radical cystectomy: a qualitative focus group study. Disabil Rehabil. (2019) ;14: ;1–8. doi: 10.1080/09638288.2019.1651907. |
[29] | Jensen BT , Petersen AK , Jensen JB , Laustsen S , Borre M . Efficacy of a multiprofessional rehabilitation programme in radical cystectomy pathways: A prospective randomized controlled trial. Scand J Urol. 4. (2015) ;49: (2):133–41. doi: 10.3109/21681805.2014.967810. |
[30] | Hektoen HH , Robsahm TE , Andreassen BK , Stenehjem JS , Axcrona K , Mondul A , et al. Lifestyle associated factors and risk of urinary bladder cancer: A prospective cohort study from Norway. Cancer Med. (2020) ;9: (12):4420–32. doi: 10.1002/cam4.3060. |
[31] | Dang D , Dearholt SL . Johns Hopkins nursing evidence-based practice: Model and guidelines. 3rd ed. Sigma Theta Tau International; 2017. |
[32] | Robsahm TE , Falk RS , Heir T , Sandvik L , Vos L , Erikssen J , et al. Cardiorespiratory fitness and risk of site-specific cancers: A long-term prospective cohort study. Cancer Med. (2017) ;6: (4):865–73. doi: 10.1002/cam4.1043. |
[33] | Lin J , Wang J , Greisinger AJ , Grossman HB , Forman MR , Dinney CP , et al. Energy balance, the PI3K-AKT-mTOR pathway genes, and the risk of bladder cancer. Cancer Prev Res. (2010) ;3: (4):505–17. doi: 10.1158/1940-6207.CAPR-09-0263. |
[34] | Reulen RC , De Vogel S , Zhong W , Zhong Z , Xie L-P , Hu Z , et al. Physical activity and risk of prostate and bladder cancer in China: The South and East China case-control study on prostate and bladder cancer. PLoS One. (2017) ;12: (6):e0178613. doi: 10.1371/journal.pone.0178613. |
[35] | Blanchard CM , Stein K , Courneya KS . Body mass index, physical activity, and health-related quality of life in cancer survivors. Med Sci Sports Exerc. (2010) ;42: (4):665–71. doi: 10.1249/MSS.0b013e3181bdc685. |
[36] | Fung C , Pandya C , Guancial E , Noyes K , Sahasrabudhe DM , Messing EM , et al. Impact of bladder cancer on health related quality of life in 1,476 older Americans: A cross-sectional study. J Urol. (2014) ;192: (3):690–5. doi: 10.1016/j.juro.2014.03.098.g. |
[37] | Ihira H , Sawada N , Yamaji T , Goto A , Shimazu T , Inoue M , et al. Physical activity and subsequent risk of kidney, bladder and upper urinary tract cancer in the Japanese population: the Japan Public Health Centre-based Prospective Study. Br J Cancer. (2019) ;120: (5):571–4. doi: 10.1038/s41416-019-0392-y. |


