
Adjuvant Treatment of Residual Disease Following Neoadjuvant Chemotherapy and Radical Cystectomy for Muscle Invasive Bladder Cancer
Abstract
BACKGROUND:
Cisplatin-based neoadjuvant chemotherapy (NAC) has shown overall survival benefit for patients with muscle invasive bladder cancer (MIBC). In contrast, there is limited data for adjuvant treatment options in patients with residual muscle invasive disease after NAC followed by radical cystectomy (RC).
OBJECTIVE:
This systematic review aims to give an overview of studies examining adjuvant treatment options for patients with residual MIBC at RC despite NAC.
METHODS:
We systematically searched the PubMed database and Clinicaltrials.gov (end point August 2019) for publications and registered trials combining NAC, RC, and adjuvant treatment options.
RESULTS:
After removal of duplicates, 659 articles and registered trials were further analyzed. Finally, 10 studies and 7 registered clinical trials met inclusion criteria. While 5 publications did not further characterize NAC and adjuvant regimens, the remaining 5 studies reported mainly platinum-based regimens. Altogether, the selected studies showed conflicting results regarding the potential role of adjuvant treatment strategies in the setting of residual disease after NAC and RC.
CONCLUSION:
Although there is an urgent need for adjuvant treatment options for patients with MIBC after NAC and residual muscle invasive disease at RC, there has been very limited evidence available. Inclusion of such patients into ongoing adjuvant clinical trials is urgently needed; active surveillance is strongly recommended in the absence of trials.
INTRODUCTION
Radical cystectomy (RC) with regional lymphadenectomy is the mainstay of treatment in patients with resectable muscle invasive bladder cancer (MIBC). Utilization of neoadjuvant cisplatin-based chemotherapy (NAC) has significantly improved overall survival, in patients with cT2-4a stage [1, 2]. In patients with clinical suspicion of N + disease who may receive chemotherapy before RC the term “induction or primary” chemotherapy is preferred and not the term NAC [3]. These chemotherapy protocols either consist of accelerated (dose dense) methotrexate, vinblastine, doxorubicin and cisplatin (MVAC) with G-CSF, or gemcitabine and cisplatin (GC) in usual practice. There is no evidence of benefit when using carboplatin instead of cisplatin both in the neoadjuvant and adjuvant setting. The main goal of NAC is to eradicate micro-metastasis which is the usual cause of death. Furthermore, NAC regimens offer the advantage of risk stratification – as patients with MIBC with pathologic complete response (CR) or, at least, downstaging to non-muscle invasive at the RC specimen belong to a favorable prognostic subgroup [4]. Downstaging can also help with RC in bulky tumors. Another important advantage of NAC is that the patients as opposed to adjuvant chemotherapy do not need to recover from RC. Nevertheless, NAC is markedly underutilized, regardless its advantages [5]. There are two main drawbacks of the neoadjuvant approach: First, there is the high rate of overtreatment as approximately 50% of all patients with MIBC remain recurrence-free after RC in the long-term without further systemic therapy, depending on pathologic stage [6, 7]. Second, pathologic downstaging or CR is observed in about 50% of the patients [8]. Conversely, the advantage of adjuvant chemotherapy could be that it may accurately select those patients at high risk of recurrence. In the adjuvant setting, cisplatin-based chemotherapy is considered based on advanced pathologic stage (pT3-4 and/or pN+), but these parameters do not accurately predict recurrence risk reduction after adjuvant chemotherapy in the individual level. In addition, up to 25% of all patients with RC may develop renal impairment or they may never reach an appropriate performance status, which can limit the use of cisplatin-based chemotherapy [9].
Conversely, patients with MIBC and residual disease after NAC and subsequent RC may benefit from further adjuvant treatment options. Potential therapeutic strategies could, in theory, include: re-challenge with chemotherapeutics previously used as NAC but also different chemotherapy protocols, targeted therapeutics like Tyrosine Kinase Inhibitors (TKI) and immunotherapies, such as checkpoint inhibitors. However, despite the distinct medical need in this subgroup, there is no clear evidence if and which adjuvant treatment might be effective. This systematic review aims to identify relevant articles in the PubMed database and Clinicaltrials.gov, thereby giving an overview of clinical studies evaluating adjuvant therapeutic options to patients with histopathologically confirmed residual muscle-invasive disease after NAC and RC.
METHODS
Our study was conducted according to the PRISMA (Reporting Items for Systematic Reviews and Meta-analyses) guidelines [10]. This study, as a literature review is exempt from any requirement for Institutional Review Board approval. No human or animal research was involved in the elaboration of this manuscript. In August 2019, we searched the PubMed database for relevant articles. We used the search term neoadjuvant AND cystectomy AND adjuvant. In a first step, appropriate PubMed articles were identified by title and abstract screening. Publications in languages other than English or German, animal studies as well as reviews and (editorial) comments were excluded from further analysis. Next, we screened the reference lists of appropriate publications and related review articles for studies previously not covered.
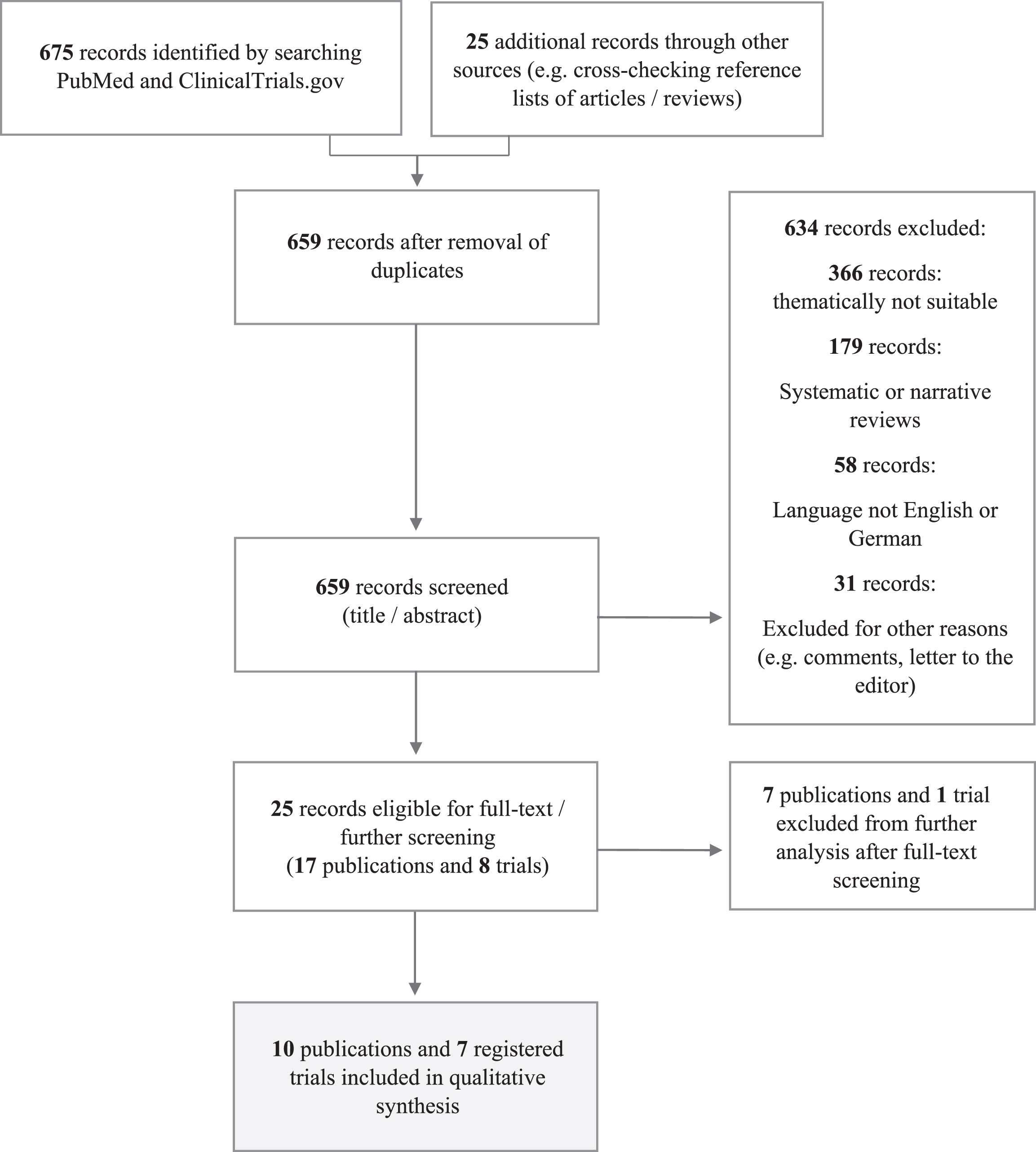
In a second approach, we searched for terminated, recruiting and projected trials registered at Clinicaltrials.gov by using the same search terms as in our PubMed search. Candidate studies were screened by checking their short descriptions. Figure 1 outlines the course of our study.
Fig. 1
Course of our study. Systematic search algorithms for relevant articles in PubMed and suitable registered clinical trials on Clinicaltrials.gov.
We included studies examining the impact of adjuvant treatment for patient populations with MIBC having residual muscle-invasive disease despite NAC and RC. Furthermore, we excluded clinical studies consisting of neoadjuvant treatment regimen other than chemotherapy (e.g. Erlotinib as targeted therapy [11]) and surgical procedures other than RC – e.g. bladder preserving techniques/partial cystectomy.
RESULTS
As illustrated in Fig. 1, searching the databases PubMed and ClinicalTrials.gov by applying the search term neoadjuvant AND cystectomy AND adjuvant yielded 659 potential records, we excluded 634 after title and abstract screening. In a next step, 25 records (17 publications and 8 registered trials) were selected for full text screening. As shown in Table 1, 10 publications were finally included in our qualitative synthesis.
Table 1
Further characteristics of selected publications included in our qualitative synthesis
| Publication | Design | Study population | Treatment | Control arm | Primary clinical endpoint | Significance | Comment |
| Kassouf W et al., 2009 | retrospective | Single-center database (1993-2003), pN+, n = 37 | AC, n = 11 | Observation, n = 24 | Recurrence-free survival (RFS), Disease-specific survival (DSS), Overall survival (OS) | YES | Significant effect of AC on RFS |
| Zargar-Shoshtari K et al., 2016 | retrospective | Single-center database (2001-2013), pT3-4 AND/OR pN+, n = 88 | AC, n = 29 | Observation, n = 59 | RFS, Cancer-specific survival (CSS) | NO | |
| Parker WP et al., 2017 | retrospective | National Cancer Database (NCDB, 2006-2012), pT3-4 OR pN1-3, n = 1361 | AC, n = 328 | Observation, n = 1033 | OS, Hazard Ratio (HR) | YES | Trend (p = 0.06) towards an association of AC and OS in multivariable analysis; significant association of AC and OS in pT4N0 patients |
| Sui W et al., 2017 | retrospective | NCDB (2004-2013), pT3-4 OR pN+, n = 705 | AC, n = 168 | Observation, n = 537 | OS | NO | |
| Seisen T et al., 2018 | retrospective | NCDB (2006-2012); T3-T4 AND/OR pN+, n = 788 | AC, n = 184 | Observation, n = 604 | OS | YES | OS benefit across all patients examined |
| Haque W et al., 2018 | retrospective | NCDB (2004-2013), pT3-4N0-3M0, n = 2592 | AC, n = 901 | Observation, n = 1691 | OS, HR | YES | OS benefit for pN2-3 AND patients with positive surgical margins |
| Lewis GD et al., 2018 | retrospective | NCDB (2004-2013), pT3-4N0-3M0, n = 1646 | Radiotherapy, n = 59 | Observation, n = 1587 | OS, HR | YES | OS benefit for patients with positive surgical margins |
| Bandini M et al., 2019 | retrospective | Multi-center database, cT2-4N0M0, n = 259 | AC, n = 17 | Observation, n = 242 | RFS | NO | NAC + AC as one subgroup within perioperative chemotherapy (total n = 950); no significant OS benefit for adding AC to NAC and RC |
| Pederzoli F et al., 2019 | retrospective | see Bandini M et al., 2019 | |||||
| Martinez Chanza N et al., 2019 | retrospective | Multi-center database,≥ypT3 AND/OR ypN+, n = 129 | AC, n = 23 | Observation, n = 106 | Time to recurrence (TTR) – primary OS – secondary | YES | In high-risk sub-group (ypT4b/ypN+): AC associated with significantly longer TTR |
Although we identified ten relevant publications on PubMed, these retrospective analyses did not derive from ten independent study cohorts – instead, we found two articles referring to independent single-center databases [12, 13]. Additionally, we identified two publications referring to the same multi-center database [14, 15] and a third study examining an independent multi-center database [16]. Moreover, five studies used data from the National Cancer Database (NCDB) with different time periods examined [17–21]. As we could not clearly separate the five NCDB-based study cohorts from each other and consecutively would have had to assume double counting of patients, we did not perform a quantitative meta-analysis.
In terms of comparing and meta-analyzing results, NCDB-based studies [17–21] also suffered from the limitation that NAC and AC specifications were not recorded within central data acquisition. The remaining independent studies mainly reported Platinum-based therapies. Table 2 outlines the available specifications of NAC and AC regimens within included studies.
Table 2
Specifications of NAC and AC regimens within identified studies
| Publication | NAC regimen | AC regimen |
| Kassouf W et al., 2009 | Treatment + Control, n = 37 | Platinum-based (mosty MVAC): |
| Platinum-based: n = 30(81%), | n = 8(73%), non-Platinum-based: | |
| non-Platinum-based: n = 7(19%) | n = 3(27%) | |
| Zargar-Shoshtari K et al., 2016 | Treatment, n = 29, | Carboplatin: n = 16(55%), |
| MVAC: n = 4(14%), GC: n = 19(65%) | Cisplatin: n = 8(28%), | |
| Carboplatin: n = 6(21%) Control, n = 51 | Other (mainly Taxane): n = 5(17%) | |
| MVAC: n = 4(7%), GC: n = 34(67%), Carboplatin: n = 13(26%) | ||
| Parker WP et al., 2017 | National Cancer Database (NCDB) study; no specific information about NAC and AC regimens | |
| Sui W et al., 2017 | NCDB study; no specific information about NAC and AC regimens; study cohort limited to | |
| “multi-agent” chemotherapy | ||
| Seisen T et al., 2018 | NCDB study; no specific information about NAC and AC regimens | |
| Haque W et al., 2018 | NCDB study; no specific information about NAC and AC regimens | |
| Lewis GD et al., 2018 | NCDB study; no specific information about NAC regimens; Radiotherapy instead of AC | |
| Bandini M et al., 2019 | Treatment, n = 17 | Carboplatin: n = 2(12%), |
| Carboplatin: n = 2(12%), Cisplatin: n = 11(65%), | Cisplatin: n = 10(59%), | |
| Unknown: n = 6(23%) | Unknown: n = 5(29%) | |
| Control, n = 242 Carboplatin: | ||
| n = 20(8%), Cisplatin: n = 203(84%), | ||
| Unknown: n = 19(8%) | ||
| Pederzoli F et al., 2019 | see Bandini M et al., 2019 | |
| Martinez Chanza N et al., 2019 | Treatment, n = 23 | MVAC (normal/dose-dense): n = 4(17%), |
| MVAC (normal/dose-dense): | GC: n = 7(30%), | |
| n = 7(30%), GC: n = 7(30%), Gemcitabin/Carboplatin/Paclitaxel: | Gemcitabin/Carboplatin/Paclitaxel: n = 2(9%), | |
| n = 6(21%), Cisplatin: n = 1(4%), Other: n = 4(17%) | Carboplatin/Paclitaxel: 3(13%), Other: n = 7(30%) | |
| Control, n = 106 MVAC (normal/dose-dense): | ||
| n = 20(19%), GC: n = 50(47%), | ||
| Gemcitabin/Carboplatin/Paclitaxel: n = 6(6%), | ||
| Gemcitabin/Carboplatin: n = 10(9%), | ||
| Cisplatin: n = 2(2%), Other: n = 18(17%) | ||
Overview of included publications
The earliest identified study dated from 2009 – searching their single-center database, Kassouf et al. [12] identified 37 nodal positive patients with MIBC after RC. Of them, 11 patients had received NAC (mostly MVAC) before RC. In their multivariate analysis, researchers discovered a significant association between AC and improved recurrence-free survival (RFS; Hazard Ratio (HR) 0.29, Confidence Interval (CI) 0.1–0.81, p = 0.02). Regarding further clinical endpoints, they found trends towards prolonged overall survival (OS, p = 0.08) and Disease-specific survival (DSS, p = 0.07) in AC-treated patients.
In the study of Zargar-Shoshtari et al. [13], the authors examined a single-center cohort consisting of 88 patients with pT3-4 and/or pN+ stage receiving NAC and RC. Of them, 29 received AC – specifically carboplatin (n = 16), cisplatin (n = 8) and taxane-based regimens (n = 5) – whereas remaining 59 patients were observed. Regarding their clinical endpoints recurrence-free survival (RFS) and cancer-specific survival (CSS), the authors found no significant improvement of RFS or CSS associated with AC.
Parker et al. [17] analyzed patients with pT3-4 or pN1-3 stage from the NCDB (time period: 2006-2012). Of 1361 patients treated with NAC and RC, 328 received AC – remaining patients were observed. Regarding OS, the authors found no significant difference when comparing AC and observation group. However, multivariable analysis revealed a non-significant trend (p = 0.06) towards an association between AC and longer OS (HR 0.86; CI 0.74-1.01). Moreover, multivariable Cox proportional hazards regression revealed an association of AC and prolonged OS for patients with pT4N0 stage (p = 0.04).
Sui et al. examined patients with pT3-4 and/or pN+ stage from the NCDB (time period: 2004–2013) [18]. A total of 168 patients were treated with AC compared with 537 patients under observation. No significant difference in median OS between AC and observation group was reported. Neither multivariate nor subgroup analysis yielded significant survival advantages for AC.
In contrast, Seisen et al. found a significant association between AC and prolonged OS [19]. For their study, they also examined patients from NCDB (time period: 2006–2012) with pT3-4 and/or pN+ stage. The treatment arm consisted of 184 patients receiving AC, while 604 patients were observed in the control arm. Of note, the authors found a significant OS benefit in all subgroups examined, resulting in a 5-month OS benefit for patients in the AC treatment arm. The OS benefit significantly decreased with patient age, while no significant influence could be determined for variables such as pT/N classification or positive surgical margins.
The largest study cohort was analyzed by Haque et al. [20] – the authors examined a total of n = 2592 patients with pT3-4N0-3M0 MIBC from the NCDB (time period: 2004–2013). 901 patients were treated with AC, the control arm consisted of 1691 patients under observation. The researchers found no significant difference between AC and observation. However, patients with N2-3 stage (p = 0.005) and positive surgical margins had significant survival benefit from AC (p = 0.025).
The only publication addressing a potential impact of adjuvant radiotherapy (RT) after NAC and RC was performed by Lewis et al. [21]. Using the same underlying study cohort as Haque et al. [20] but excluding AC-treated patients from analysis, they examined 59 patients with MIBC treated with adjuvant RT versus 1587 patients in the control arm. The authors found no significant association of RT and OS across all patients, but an OS benefit for RT in case of positive surgical margins – with a median OS of 20.3 months vs. 13.1 months (p = 0.032).
Based on a multi-center database, Bandini et al. examined the 1-year RFS of 950 patients with cT2-4N0 MIBC receiving perioperative chemotherapy [14]. One small subgroup (n = 17) consisted of patients treated with NAC and AC. Although the NAC + AC combination showed the highest rate of 1-year RFS (58.8%), overall reception of AC was not significantly associated with RFS. Within another sub-analysis of this specific study cohort [15], the same group analyzed the additional role of AC. They found no significant difference between the NAC + AC and the NAC group. Of note, a 1-year RFS benefit for AC delivery was only significant when picking out patients with “high risk” features from their nomograms with a 1-year risk of recurrence >40%.
Finally, Martinez Chanza et al. searched their multi-institutional MIBC database and identified 129 patients with residual disease (≥ypT3 AND/OR ypN+) despite NAC followed by RC [16]. Although they only found a trend towards longer time to recurrence (TTR) in AC-treated versus patients under surveillance (18 vs. 10 months, p = 0.06), they identified a significant reduction in recurrence risk associated with AC (p = 0.01). In line with previous authors, they also reported significant effects of AC on TTR in high-risk sub-groups (ypT4b/ypN+).
Overview of registered clinical trials
We identified seven clinical trials registered at ClinicalTrials.gov at the time of our systematic search. One study (NCT01042795) was already terminated without published results. Two other trials were reported as “Active, not recruiting” (IMvigor010/NCT02450331 and CheckMate 274/NCT02632409). Four trials (AMBASSADOR/NCT03244384, NCT03406650, NCT03661320, NIAGARA/NCT03732677) were recruiting at time of our systematic search. While preparing this manuscript, the PROOF 302 study [22] (NCT04197986) and the PEGASUS trial (NCT04294277) were registered on ClinicalTrials.gov. After checking eligibility, we added both studies to our synthesis. Table 3 outlines the characteristics of all eligible clinical trials.
Table 3
Further characteristics of registered clinical trials included in our qualitative synthesis
| Trial Identifier | Status | Title/Study characteristics | Treatment | Control arm | Primary clinical endpoint | Significance | Comment |
| NCT01042795 | Terminated | Phase II, single-center | Adjuvant Sunitinib, n = 7 | Observation | Disease-free survival (DFS) | / | Study terminated due to poor accrual |
| NCT02450331 | Active, not recruiting | IMvigor010/Phase III, multi-center, randomized, enrollment n = 809 (04/2020) | Adjuvant Atezolizumab | Observation | DFS | Results pending | NAC-treated MIBC patients ypT2-4a or ypN + as eligible subgroup |
| NCT02632409 | Active, not recruiting | CheckMate 274/Phase III, multi-center, randomized, estimated enrollment n = 700 | Nivolumab | Placebo | DFS | Results pending | |
| NCT03244384 | Recruiting | AMBASSADOR/Phase III, multi-center, randomized, estimated enrollment n = 739; | Adjuvant Pembrolizumab | Placebo | OS, DFS | Results pending | NAC-treated MIBC patients≥ypT2 or ypN + as eligible subgroup |
| NCT03406650 | Recruiting | Phase II, multi-center, single-arm | Neoadjuvant: GC + Durvalumab, Adjuvant: Durvalumab | Observation | Event-free survival (EFS, 2 years) | Results pending | |
| NCT03661320 | Recruiting | Phase III, multi-center, randomized, estimated enrollment n = 1200 | Neoadjuvant: GC + Nivolumab±BMS-986205 (IDO1 inhibitor), Adjuvant: Nivolumab±BMS-986205 | Chemotherapy alone (NAC) | Pathologic complete response (pCR) rates at time of cystectomy, EFS | Results pending | Patients with T2N0M0-T4aN0M0 eligible |
| NCT03732677 | Recruiting | NIAGARA/Phase III, multi-center, estimated enrollment n = 1050 | Neoadjuvant: GC + Durvalumab, Adjuvant: Durvalumab | Chemotherapy alone (NAC) | pCR, EFS | Results pending | Patients with T2N0M0-T4aN0M0 eligible |
| (Continued) | |||||||
| NCT04197986 | Recruiting | PROOF 302/Phase III, multi-center, randomized, Placebo-controlled, estimated enrollment n = 218 | Infigratinib | Placebo | DFS | Results pending | NAC-treated MIBC patients≥ypT2 or ypN + as eligible subgroup - in case of FGFR3 alterations |
| NCT04294277 | Not yet recruiting | PEGASUS/Phase II, single-arm, open label, estimated enrollment n = 56 | Pemigatinib | / | Relapse-free survival rate (time frame up to 2 years) | Recruting not started | Patients with MIBC and FGFR alterations after NAC (for Pt-eligible patients) and RC |
The terminated study (NCT01042795) examined the potential benefit of TKI Sunitinib after NAC and RC. However, only two of seven patients completed the dosing period (37.5 mg Sunitinib per day for 16 weeks), three presented serious adverse events during the study period. Consequently, disease-free survival as the clinical endpoint initially planned could not be addressed and the study was ultimately terminated due to poor accrual.
Six further clinical trials currently examine the effects of immune checkpoint inhibition, thereby using four different compounds – the PD-L1 inhibitors Atezolizumab and Durvalumab as well as the PD-1 inhibitors Nivolumab and Pembrolizumab. Regarding Atezolizumab (IMvigor010), Hussain et al. presented results at the ASCO 2020 meeting. In this phase III, open-label, multicenter, randomized study of Atezolizumab (anti-PD-L1 antibody) versus observation as adjuvant therapy in patients with high-risk muscle-invasive urothelial carcinoma after surgical resection. They stated that the trial missed its primary clinical endpoint, with a median DFS of 19.4 months in the Atezolizumab group vs. 16.6 months in the observation cohort (p = 0.245) [23]. The study included a subgroup of 385 patients that were previously treated in the neoadjuvant setting with cisplatin-based chemotherapy. Within this subgroup, the study not only failed to reach its primary endpoint (DFS) but also failed to show an OS advantage.
For patients with MIBC harboring genomic alterations (activating mutations or fusions) within the FGFR family (fibroblast growth factor receptor), PROOF 302 (NCT04197986) is investigating the role of the FGFR inhibitor Infigratinib in the adjuvant setting. Moreover, PEGASUS (NCT04294277) plans to investigate the impact of Pemigatinib, another FGFR inhibitor, after NAC and RC.
Of note, apart from the terminated Sunitinib trial and negative results from IMvigor010, all identified clinical trials had no published results at time of search and manuscript preparation.
DISCUSSION
Although further adjuvant treatment options for patients with residual disease after NAC and RC are urgently needed, there is a substantial lack of high-level evidence for this patient subgroup. Systematically searching PubMed and Clinicaltrials.gov, we did not find any published results from prospective clinical trials. Moreover, the 10 retrospective analyses included in our study offered a mixed picture regarding potential benefits and risks of adjuvant treatment approaches – while Seisen et al. found an OS survival benefit for AC across all subgroups [19], other publications could not identify a significant association between AC and survival [13–15, 18].
However, the remaining studies suggested a potential benefit of AC [16, 17, 20] and adjuvant RT [21] in “high risk” subgroups, such as pN+ and those with positive surgical margins in RC. Yet, all these studies do not provide adequate evidence and the role of any adjuvant therapy after NAC and RC remains inconclusive and is not recommended. Further prospective clinical trials are required to evaluate the potential role of immunotherapy or targeted therapies for this specific subgroup.
Although only one study reported results of radiotherapy as adjuvant treatment in patients with previous NAC and RC, this therapeutic approach seems promising in the adjuvant setting – especially for patients at risk for local recurrence [24]. In the study from Bateni et al., the results showed a benefit for adjuvant radiotherapy in patients with positive surgical margins regarding OS – independent from NAC reception [25]. A recent phase II randomized trial of patients with locally advanced bladder cancer after RC and pelvic lymph node dissection with negative margins reported significantly improved local control with the addition of AC+ radiotherapy versus AC alone, with a 2-year local control of 96% for sequential chemotherapy plus RT vs. 69% for chemotherapy alone (P < 0.01) [26]. Accordingly, this could be an attractive concept for combining RT and immune checkpoint inhibitors. There are ongoing studies with this combination regarding local recurrence of bladder cancer after RC, but also in the neoadjuvant setting [27].
For immune checkpoint inhibitors, we currently have limited and conflicting data for the use of these agents in the adjuvant setting. First results from the IMvigor010 study (NCT02450331) using Atezolizumab as adjuvant therapy in high risk urothelial cancer were rather discouraging. The study also included a large subgroup (47%, n = 385) of patients after cisplatin-based NAC. The study failed to reach its primary endpoint of DFS in the total population but also in this patient subgroup. Potentially, these early results indicate that a certain tumor load is required for immune checkpoint inhibitors to work properly [28], and that AC will remain the dominant concept to fight systemic disease (micro-metastases). Therefore, immune checkpoint inhibitors could be more effective either at earlier stages of the disease (e.g. in the neoadjuvant setting) or in patients with metastatic disease – alone or as a maintenance therapy as shown within the JAVELIN100 study [29]. In contrast, a very recent press release from September 2020 [30] stated that CheckMate 274 (NCT02632409) reached its primary endpoint DFS in an interim analysis – with Nivolumab showing a benefit in all patients as well as in patients whose tumor cells express PD-L1 ≥1%. Of note, the AMBASSADOR trial (NCT03244384) examining Pembrolizumab in an adjuvant setting is still accruing, as is PROOF 302 (NCT04197986) for the FGFR1-3 inhibitor Infigratinib.
Regarding the variety of adjuvant treatment options, nine out of ten PubMed publications analyzed the influence of AC, whereas only one study [21] examined the potential added value of adjuvant RT. Apart from the small number of relevant studies identified in this systematic review, lack of specific information about NAC and AC regimens, especially in NCDB-based studies, were a serious limitation and a reason for deciding against a quantitative meta-analysis. Moreover, missing data, several selection and confounding biases inherent to retrospective studies, lack of central radiology review and of randomized trial data, are important limitations in this particular treatment setting.
In conclusion, patients with residual disease following NAC and RC must be included in adjuvant clinical trials in order to assess the potential role of additional therapy. If there is no trial available, we strongly recommend active surveillance as per NCCN guidelines. Apart from gathering new clinical trial data, we should learn about the prognostic implications and the biological mechanisms of resistance to NAC. Previously, researchers showed that NAC-induced tumor regression grades (TRGs) of patients with MIBC added substantial prognostic value to classical TNM staging [31, 32]. Moreover, different TRGs were associated with biologically distinct tumor subgroups [33]. A deeper understanding of the biology of non-response to NAC will help identify therapeutic targets and biomarkers to be tested in prospective trials.
ACKNOWLEDGMENTS
The authors have no acknowledgments.
FUNDING
A personal grant from Else-Kröner-Foundation to Markus Krebs (Else Kröner Integrative Clinician Scientist College for Translational Immunology, University Hospital Würzburg, Würzburg, Germany) supported this work.
AUTHORS CONTRIBUTIONS
Markus Krebs and Ioannis Sokolakis: performance of work; interpretation or analysis of data; writing the article.
Roland Seiler, Siamak Daneshmand and Petros Grivas: interpretation or analysis of data; writing the article
Georgios Gakis: conception; interpretation or analysis of data; writing the article.
ETHICAL CONSIDERATIONS
This study, as a literature review is exempt from any requirement for Institutional Review Board approval. No human or animal research was involved in the elaboration of this manuscript.
CONFLICT OF INTEREST
Markus Krebs: Clinical investigator for the NIAGARA trial (NCT03732677) at study site Würzburg, Germany. Advisory Board: GlaxoSmithKline.
Ioannis Sokolakis: no conflicts of interest to declare.
Roland Seiler: no conflicts of interest to declare.
Siamak Daneshmand: Advisory Board: Janssen, Ferring, Photocure, Taris, Spectrum, Pacific Edge, QED, Abbvie, Johnson & Johnson, Seattle Genetics, Nucleix, Aduro, BMS. Payments from commercial organizations: Janssen, Ferring, Photocure, Taris, Spectrum, Pacific Edge, QED, Abbvie, Johnson & Johnson, Seattle Genetics, Nucleix, Aduro, BMS. Grants: Photocure, Janssen, Ferring, Taris, Pacific Edge, Johnson & Johnson, BMS. Investments: Taris. Clinical trial participation (last 2 years): Photocure, Janssen, Ferring, Taris, Pacific Edge, Johnson & Johnson, BMS.
Petros Grivas (COI in the last 3 years): consulting for AstraZeneca, Bayer, Bristol-Myers Squibb, Clovis Oncology, Driver, EMD Serono, Exelixis, Foundation Medicine, GlaxoSmithKline, Genentech, Genzyme, Heron Therapeutics, Janssen, Merck, Mirati Therapeutics, Pfizer, Roche, Seattle Genetics, QED Therapeutics; participation in educational program for Bristol-Myers Squibb; and institutional research funding from AstraZeneca, Bavarian Nordic, Bayer, Bristol-Myers Squibb, Clovis Oncology, Debiopharm, Genentech, Immunomedics, Kure It Cancer Research, Merck, Mirati Therapeutics, Oncogenex, Pfizer, QED Therapeutics, GlaxoSmithKline.
Georgios Gakis: Advisory Board: MSD, Bayer, LEO Pharma. Receipt of speaker honoraria/travel grants: IPSEN, medac, Pierre Fabre, Erbe Elektromedizin.
REFERENCES
[1] | Grossman HB , Natale RB , Tangen CM , Speights VO , Vogelzang NJ , Trump DL , et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. (2003) ;349: (9):859–66. |
[2] | Sternberg CN , Skoneczna I , Kerst JM , Albers P , Fossa SD , Agerbaek M , et al. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+M0 urothelial carcinoma of the bladder (EORTC 30994): an intergroup, open-label, randomised phase 3 trial. Lancet Oncol. (2015) ;16: (1):76–86. |
[3] | Zargar-Shoshtari K , Zargar H , Lotan Y , Shah JB , Van Rhijn BW , Daneshmand S , et al. A multi-institutional analysis of outcomes of patients with clinically node positive urothelial bladder cancer treated with induction chemotherapy and radical cystectomy. The Journal of Urology. (2016) ;195: (1):53–9. |
[4] | Zargar H , Zargar-Shoshtari K , Lotan Y , Shah JB , van Rhijn BW , Daneshmand S , et al. Final Pathological Stage after Neoadjuvant Chemotherapy and Radical Cystectomy for Bladder Cancer-Does pT0 Predict Better Survival than pTa/Tis/T1? J Urol. (2016) ;195: (4 Pt 1):886–93. |
[5] | Patafio FM , Mackillop WJ , Feldman-Stewart D , Siemens DR , Booth CM . Why is perioperative chemotherapy for bladder cancer underutilized? In: Urologic Oncology: Seminars and Original Investigations. Elsevier; 2014. pp. 391-395. |
[6] | Stein JP , Lieskovsky G , Cote R , Groshen S , Feng AC , Boyd S , et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. (2001) ;19: (3):666–75. |
[7] | Madersbacher S , Hochreiter W , Burkhard F , Thalmann GN , Danuser H , Markwalder R , et al. Radical cystectomy for bladder cancer today–a homogeneous series without neoadjuvant therapy. J Clin Oncol. (2003) ;21: (4):690–6. |
[8] | Peyton CC , Tang D , Reich RR , Azizi M , Chipollini J , Pow-Sang JM , et al. Downstaging and Survival Outcomes Associated With Neoadjuvant Chemotherapy Regimens Among Patients Treated With Cystectomy for Muscle-Invasive Bladder Cancer. JAMA Oncol. (2018) 01;4: (11):1535–42. |
[9] | Eisenberg MS , Thompson RH , Frank I , Kim SP , Cotter KJ , Tollefson MK , et al. Long-term renal function outcomes after radical cystectomy. J Urol. (2014) ;191: (3):619–25. |
[10] | Liberati A , Altman DG , Tetzlaff J , Mulrow C , Gøtzsche PC , Ioannidis JPA , et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) ;339: :b2700. |
[11] | Pruthi RS , Nielsen M , Heathcote S , Wallen EM , Rathmell WK , Godley P , et al. A phase II trial of neoadjuvant erlotinib in patients with muscle-invasive bladder cancer undergoing radical cystectomy: clinical and pathological results: ERLOTINIB IN BLADDER CANCER. BJU International.349-54. (2010) ;106: (3). |
[12] | Kassouf W , Agarwal PK , Grossman HB , Leibovici D , Munsell MF , Siefker-Radtke A , et al. Outcome of Patients With Bladder Cancer With pN+ Disease After Preoperative Chemotherapy and Radical Cystectomy. Urology. (2009) ;73: (1):147–52. |
[13] | Zargar-Shoshtari K , Kongnyuy M , Sharma P , Fishman MN , Gilbert SM , Poch MA , et al. Clinical role of additional adjuvant chemotherapy in patients with locally advanced urothelial carcinoma following neoadjuvant chemotherapy and cystectomy. World J Urol. (2016) ;34: (11):1567–73. |
[14] | Bandini M , Briganti A , Plimack ER , Niegisch G , Yu EY , Bamias A , et al. Modeling 1-year Relapse-free Survival After Neoadjuvant Chemotherapy and Radical Cystectomy in Patients with Clinical T2-4N0M0 Urothelial Bladder Carcinoma: Endpoints for Phase 2 Trials. Eur Urol Oncol. (2019) ;2: (3):248–56. |
[15] | Pederzoli F , Bandini M , Briganti A , Plimack ER , Niegisch G , Yu EY , et al. Incremental Utility of Adjuvant Chemotherapy in Muscle-invasive Bladder Cancer: Quantifying the Relapse Risk Associated with Therapeutic Effect. Eur Urol. (2019) ;76: (4):425–9. |
[16] | Martinez Chanza N , Werner L , Plimack E , Yu EY , Alva AS , Crabb SJ , et al. Incidence, Patterns, and Outcomes with Adjuvant Chemotherapy for Residual Disease After Neoadjuvant Chemotherapy in Muscle-invasive Urinary Tract Cancers. Eur Urol Oncol. 2019 Jan 30; |
[17] | Parker WP , Habermann EB , Day CN , Zaid HB , Frank I , Thompson RH , et al. Adverse Pathology After Neoadjuvant Chemotherapy and Radical Cystectomy: The Role of Adjuvant Chemotherapy. Clin Genitourin Cancer. 2017 Jul 22; |
[18] | Sui W , Lim EA , Joel Decastro G , McKiernan JM , Anderson CB . Use of Adjuvant Chemotherapy in Patients with Advanced Bladder Cancer after Neoadjuvant Chemotherapy. Bladder Cancer. (2017) ;3: (3):181–9. |
[19] | Seisen T , Jamzadeh A , Leow JJ , Rouprêt M , Cole AP , Lipsitz SR , et al. Adjuvant Chemotherapy vs Observation for Patients With Adverse Pathologic Features at Radical Cystectomy Previously Treated With Neoadjuvant Chemotherapy. JAMA Oncol. (2018) ;4: (2):225–9. |
[20] | Haque W , Lewis GD , Verma V , Darcourt JG , Butler EB , Teh BS . The role of adjuvant chemotherapy in locally advanced bladder cancer. Acta Oncol. (2018) ;57: (4):509–15. |
[21] | Lewis GD , Haque W , Verma V , Butler EB , Teh BS . The Role of Adjuvant Radiation Therapy in Locally Advanced Bladder Cancer. Bladder Cancer. (2018) ;4: (2):205–13. |
[22] | Pal SK , Daneshmand S , Matin SF , Loriot Y , Sridhar SS , Grivas P , et al. PROOF A randomized, double-blind, placebo-controlled, phase III trial of infigratinib as adjuvant therapy in patients with invasive urothelial carcinoma harboring FGFR3 alterations. JCO. (2020) ;38: (6_suppl):TPS600–TPS600. |
[23] | Hussain MHA , Powles T , Albers P , Castellano D , Daneshmand S , Gschwend J , et al. IMvigor Primary analysis from a phase III randomized study of adjuvant atezolizumab (atezo) versus observation (obs) in high-risk muscle-invasive urothelial carcinoma (MIUC). JCO. (2020) ;38: (15_suppl):5000–5000. |
[24] | Fischer-Valuck BW , Michalski JM , Mitra N , Christodouleas JP , DeWees TA , Kim E , et al. Effectiveness of postoperative radiotherapy after radical cystectomy for locally advanced bladder cancer. Cancer Med. (2019) ;8: (8):3698–709. |
[25] | Bateni ZH , Pearce SM , Zainfeld D , Ballas L , Djaladat H , Schuckman AK , et al. National Practice Patterns and Overall Survival After Adjuvant Radiotherapy Following Radical Cystectomy for Urothelial Bladder Cancer in the USA, 2004-2013. Eur Urol Oncol. 2018 Dec 19; |
[26] | Zaghloul MS , Christodouleas JP , Smith A , Abdallah A , William H , Khaled HM , et al. Adjuvant Sandwich Chemotherapy Plus Radiotherapy vs Adjuvant Chemotherapy Alone for Locally Advanced Bladder Cancer After Radical Cystectomy: A Randomized Phase 2 Trial. JAMA Surg. (2018) 17;153: (1):e174591. |
[27] | Schmid SC , Koll FJ , Rödel C , Maisch P , Sauter A , Beckert F , et al. Radiation therapy before radical cystectomy combined with immunotherapy in locally advanced bladder cancer - study protocol of a prospective, single arm, multicenter phase II trial (RACE IT). BMC Cancer. (2020) ;20: (1):8. |
[28] | Gopalakrishnan D , Koshkin VS , Ornstein MC , Papatsoris A , Grivas P . Immune checkpoint inhibitors in urothelial cancer: recent updates and future outlook. Ther Clin Risk Manag. (2018) ;14: :1019–40. |
[29] | Powles T , Park SH , Voog E , Caserta C , Valderrama BP , Gurney H , et al. Maintenance avelumab+best supportive care (BSC) versus BSC alone after platinum-based first-line (1L) chemotherapy in advanced urothelial carcinoma (UC): JAVELIN Bladder 100 phase III interim analysis. JCO. (2020) ;38: (18 suppl):LBA1–LBA1. |
[30] | Opdivo (nivolumab) Significantly Improves Disease Free-Survival vs. Placebo as Adjuvant Therapy for Patients with High-Risk, Muscle-Invasive Urothelial Carcinoma in Phase 3 CheckMate -274 Trial [Internet]. 2020 [cited 2020 Sep 27]. Available from: https://news.bms.com/news/corporate-financial/2020/Opdivo-nivolumab-Significantly-Improves-Disease-Free-Survival-vs.-Placebo-as-Adjuvant-Therapy-for-Patients-with-High-Risk-Muscle-Invasive-Urothelial-Carcinoma-in-Phase-3-CheckMate–274-Trial/default.aspx |
[31] | Fleischmann A , Thalmann GN , Perren A , Seiler R . Tumor regression grade of urothelial bladder cancer after neoadjuvant chemotherapy: a novel and successful strategy to predict survival. Am J Surg Pathol. (2014) ;38: (3):325–32. |
[32] | Voskuilen CS , Oo HZ , Genitsch V , Smit LA , Vidal A , Meneses M , et al. Multicenter Validation of Histopathologic Tumor Regression Grade After Neoadjuvant Chemotherapy in Muscle-invasive Bladder Carcinoma. Am J Surg Pathol. (2019) ;43: (12):1600–10. |
[33] | Seiler R , Gibb EA , Wang NQ , Oo HZ , Lam H-M , van Kessel KE , et al. Divergent Biological Response to Neoadjuvant Chemotherapy in Muscle-invasive Bladder Cancer. Clin Cancer Res (2019) 15;25: (16):5082–93. |


