Challenging Cases in Urothelial Cancer
INTRODUCTION
Urothelial cancer of the urinary tract is common and affects a large number of men and women, resulting in a reasonably large part of the work effort of urologists who take care of adults. Most of the urothelial tumors arise in the bladder but the same causative factors can lead similar tumors of the upper urinary tract and prostatic urethra. Due to the heterogeneous nature of these tumors as well as their propensity for “recurring” in time and location over the patient’s life the clinician is often in the position of deciding among often challenging treatment choices for his/her patient. Although there are published guidelines many cases do not readily fit into a typical scenario, thus leaving ample room for decision making for the individual patient. We invite our readers to review and comment on the case and management by email to: .
Case 1. T1 high-grade urothelial bladder cancer
The patient is a 56 year old male practicing urologist. He had the acute onset of gross hematuria and a CT scan of the abdomen and pelvis was normal except for a possible small bladder tumor. An office cystoscopy indicated a solitary 3 cm papillary tumor at the right lateral wall. A TURBT was performed and the pathology revealed a high-grade focally invasive T1 urothelial carcinoma. Muscle was present and not involved. There was a focus of CIS adjacent to the tumor. The rest of the bladder and the prostatic urethra were visually normal but not biopsied.
His general health has been excellent with the exception of type 2 diabetes.
He has never had surgery and he never smoked cigarettes.
The patient sought a second opinion and 6 weeks later he was taken to the operating room. The bladder was normal except for a 1 cm slightly raised flat lesion on the posterior wall. The prior resection site was healed and no other areas suggested CIS. A combination of cold cup biopsy and loop resection was performed from the prior biopsy site and the small suspected tumor.
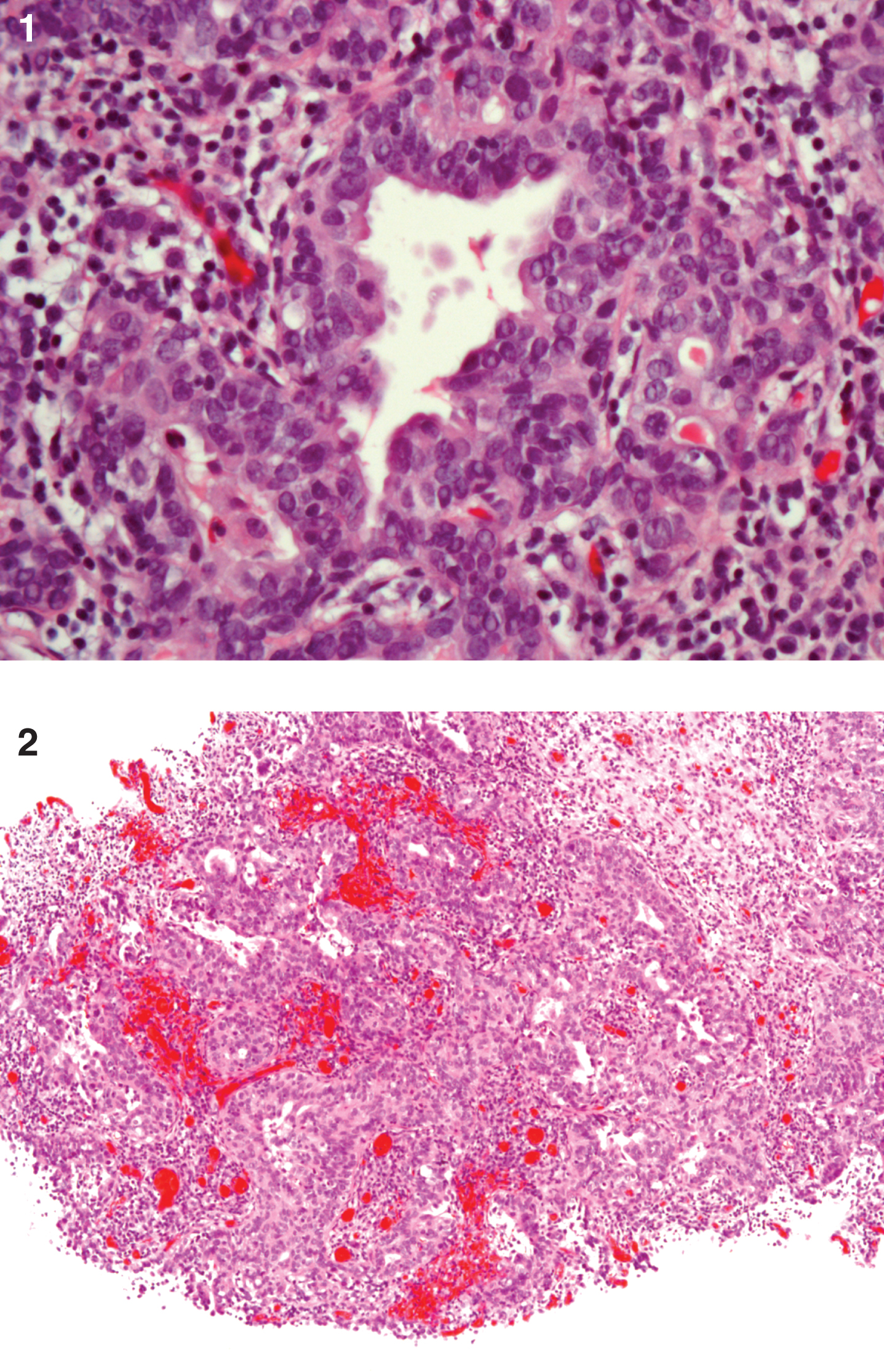
The pathology revealed no tumor at the initial tumor site. The small lesion in the posterior wall was a mixed urothelial and adenocarcinoma with focal invasion into the lamina propria. Muscle was scantbut was free of tumor. The patient has not had any intravesical therapy and not surprisingly the patient would prefer to avoid removal of his bladder (Figs. 1 and 2). Next steps may include:
1) Intravesical BCG
2) Radical cystectomy
3) Bladder sparing chemo-radiation therapy
4) Cystoscopy with Cysview and re-resection of posterior wall tumor with mapping biopsies of the rest of the bladder and prostatic urethra
5) Other ----------------------------------------
Please indicate recommendation and provide a short description of justification.
Figures and Tables
Figs.1 and 2
This is a high grade urothelial carcinoma (UC) with adenocarcinoma which is invasive into the lamina propria. Muscularis propria is present and not involved with cancer. There is an in situ component as well as an invasive component which is gland forming without mucin production. The tumor is GATA 3 positive (for UC). The tumor is >50% positive for Ki67.