
Hidden in plain sight: A qualitative exploration of teachers and children’s perspectives on supporting developmental language disorder in school
Abstract
BACKGROUND:
Developmental language disorder (DLD) is a difficulty learning, understanding, and using spoken language with lifelong implications for education and well-being. Teachers play a key role in the identification of DLD, in referring children to speech and language therapy services, and in the delivery of supports in school. Research suggests that school staff may benefit from health promotion interventions to increase their awareness and understanding of the condition.
OBJECTIVE:
The aim of this study was to explore the awareness and understanding of teachers and children about DLD and how these needs can be met in school to inform the development of a locally- responsive health promotion DLD intervention.
METHODS:
Semi-structured interviews with children with DLD (n = 7), and focus groups were held with classroom teachers (n = 7) in schools serving populations of high socioeconomic need using a narrative inquiry approach. A framework analysis was undertaken using the International Classification of Functioning (ICF).
RESULTS:
Teachers reportedly continue to use a variety of diagnostic terms when describing DLD. All stakeholders discussed the importance of the teacher’s role in making the necessary classroom adjustments to enable children with DLD to achieve and participate. Children provided some practical suggestions regarding how their needs can be met in the classroom.
CONCLUSIONS:
The study findings highlight the important contextual insights that teachers and children can provide to inform the development of locally responsive, health promotion interventions aimed at increasing awareness, knowledge and actions related to DLD in school.
1Introduction
Developmental Language Disorder (DLD) is a neurodevelopmental condition that can affect the ability to learn, understand, and/or using spoken language (McGregor, 2020) despite otherwise typical development. DLD can be lifelong and has significant implications for literacy development, educational attainment, social-emotional development, employability, mental health, and quality of life (Beard, 2017; RCSLT, 2018; Adolf & Hogan, 2019). There is no known single cause, but biological, genetic, and environmental risk factors are considered to play a part (IASLT, 2017; RCSLT, 2018). Whilst limited prevalence data exists in the Irish context, robust population studies in other countries show a prevalence rate of over 7% (Tomblin, et al., 1997; Norbury, et al., 2016) with a higher incidence reported in socially disadvantaged communities (Law, et al., 2017).
DLD is most often diagnosed by a speech and language therapist (SLT) during the primary school years (IASLT, 2017; Bishop, Snowling, Thompson, Greenhalgh, and the CATALISE-2 consortium, 2017). In Ireland, majority of children with DLD attend a mainstream class in a mainstream school. For the additional needs of children in school to be addressed, three tiers of intervention need to be undertaken; interventions at a universal level (support for all); interventions at a targeted level (support for some); and interventions at a specialist level (support for few) (Rix, et al., 2013). SLTs work at all three levels, with children with DLD requiring input at the specialist level (Ebbels, et al., 2019). This tiered approach to the delivery of support in school is underpinned by public health principles (Greenwood, et al., 2017) including the need for: early and accurate identification of needs, more equitable access to appropriate support (Law, Reilly & Snow, 2013) and more efficient and cost-effective allocation of specialist resources (Ebbels, et al., 2019). A minority of children with DLD in Ireland may attend ‘special classes for pupils with specific speech and language disorder’ for two of their primary school years. These are small classes specifically for children with DLD situated in mainstream schools and are jointly funded by the Education and Health public systems.
Much has been written about the difficulties of identifying DLD (Bishop Snowling, Thompson, Greenhalgh, and the CATALISE consortium, 2016). It has been reported that communication disorders like DLD commonly go undetected by trainee nurses (Sudharshan Reddy, 2019), teachers and psychologists (Cohen, et al., 1998), the public (Sudharshan Reddy, et al., 2016), and parents (Adlof, et al., 2017) with poorer awareness among parents from a lower socio-economic status (SES) (Beard, 2017). Children with more visible difficulties i.e., speech difficulties, stuttering and/or dyslexia are more likely to be identified than children with DLD alone (Adlof, et al., 2017) with less than one third of children with DLD identified before they struggle to read (Adolf & Hogan, 2019).
Schools are an important setting to target in relation to the identification of risk factors, and for the introduction of prevention strategies for childhood neurodevelopmental difficulties (Bloch, et al., 2014). Educating teachers about speech, Language and Communication Needs (SLCN) in particular, has been shown to increase recognition and onward referral to services elsewhere (Johnson & VanHecke, 2015).
Understanding contextual and priority needs in relation to knowledge gaps and methods of engagement can increase the likelihood of successful outcomes in health promotion efforts (McKean, et al., 2015). Previous research has shown that such tailored and dynamic training approaches are an important element when aiming to implement practice change in schools (Lyon, et al., 2019; Fallon, et al., 2018).
In this paper, we report the findings of the first of a multi-phased study, in which we aimed to explore the views of stakeholders about the needs of children with DLD in school. We undertook the study as we wanted to gain insights into knowledge gaps related to DLD, to understand stakeholder intervention priorities, and to identify practical strategies that could inform the development of a locally responsive, acceptable health promotion intervention about DLD for schools.
The study addressed the following research questions:
1. How do teachers and children with DLD describe the condition?
2. What do stakeholders identify as priority areas for intervention to meet DLD needs in school?
3. What strategies do stakeholders identify as appropriate in relation to supporting DLD in school?
2Methodological considerations
The epistemological assumptions of this study are subjectivist in nature; that is, knowledge is socially constructed. Within this paradigm, the study is most closely aligned with subtle realism (Duncan & Nicol, 2004). Subtle realism accepts the possibility of multiple valid interpretations of a phenomenon under study but with the goal of striving for ‘objectivity.’ As a result, transparency, rigour, and credibility were of concern in planning the study. Techniques employed to address these concerns included adhering to the use of COREQ (Tong, Sainsbury & Craig, 2007) reporting guidelines in reporting the study (appendix 1), the use of critical reflection during analysis, systematic recording of analytical decisions, and member-checking (Birt, et al., 2016) of transcripts for accuracy.
3Methods
3.1Ethics
Ethical approval for this research was granted by the Health Service Executive (HSE), Galway University Hospital (GUH) Clinical Research Ethics Committee (Ref C.A. 2378) and approved by the Institute of Technology Sligo (IT Sligo) ethics committee.
3.2Sample and setting
A purposeful sampling strategy was employed (Creswell, 2007). We used this approach as it ensures the perspectives of individuals with unique knowledge and experience in the topic of interest are included. As previous studies have shown differences in perspectives in relation to DLD in both the literature and across stakeholder groups (Gallagher, et al., 2021; Gallagher, et al., 2019a; Gallagher, et al., 2019b), we aimed to include the perspective of both teachers and children in the study.
Children aged 9–12 years (n = 7) with a diagnosis of DLD who learn in a range of different classroom settings were sought to participate in the study. Teachers (n = 7) fulfilling a diverse range of school roles within the Irish education system also participated. Teachers and children were sought from both rural and urban schools.
3.3Data collection
Two focus groups were held with teachers in their place of work facilitated by the lead author. Three teachers attended focus group 1, held in a rural school, and the remaining four teachers attended a focus group in an urban school. Each group lasted 60 minutes. Focus groups were undertaken as they have the potential to facilitate rich, and thorough discussion and allow for an exploration of commonality and differences in views (Kitzinger 1995). Development of the topic guide was guided by principles of narrative inquiry (Clandinin & Connelly, 1994) (appendix 2). This approach allows the participants to share their experiences more openly with minimal prompting from the interviewer. The topic guides were piloted with teachers prior to the study. All groups were audio-recorded. The facilitator took field notes during focus groups and audio-recorded reflective memos immediately following each group. These notes were integrated with the transcripts to inform analysis. Transcripts were member checked prior to analysis.
Semi-structured interviews were held with the children. Most children attended face-to-face, and one interview was via a secure online platform as per ethics guidelines. One paired interview (n = 2) was held as the children were in the same class ‘pod.’ Two separate meetings with the children allowed for extra time to establish rapport, and to illustrate interview techniques. During the first meeting the facilitator introduced herself and demonstrated the planned activities. The children created a pseudonym for themselves. Children were given a red and green card to use during both interviews. The green card signalled a need for more language support in relation to the tasks. A red card signalled a withdrawal of assent. Individual interviews lasted approximately 15 minutes each and the paired interviews lasted 25 minutes each. The topic guides for the children’s interviews followed the same format as the teachers. A widely used method of ‘draw-and-tell’ was used during interviews with the children to reduce the pressure to communicate verbally (Lyons, et al., 2022).
3.4Data analysis
A framework method was employed. Framework analysis is a systematic, flexible, and efficient qualitative research method (Gale, et al., 2013). In contrast to thematic analysis, this approach involves first, generating open codes inductively, and then deductively categorising these into domains provided by a chosen conceptual framework. In this analytical approach, the term ‘theme’ is used to refer to the pre-determined domains of the framework rather than to descriptive or interpretive themes generated by the researcher inductively. The framework can be chosen apriori or during the analysis.
Framework analysis includes seven phases: (i) Transcription (data was transcribed verbatim post hoc by the researcher who facilitated the focus groups/interviews), (ii) Familiarity with the data (transcripts were read through several times), (iii) Coding (open codes were generated inductively within case transcripts), (iv) Identifying the ‘best fit’ analytical framework (v) Applying the framework (deductive charting of data for individual cases), (vi) Charting data into the framework matrix (refining of deductive charting of data within participant groups) and (vii) Interpreting the data (analysis across the participant groups to identify similarities and differences).
The International Classification of Functioning, Disability and Health (ICF) (WHO, 2001) framework ICF, a bio-psychosocial model widely used across health and education research was deemed the framework of ‘best fit’ as it incorporates concepts related to an individual’s health condition and functioning in addition to environmental influences in relation to participation. A sample of transcripts were coded independently by two researchers until consistency was achieved. Thereafter, coding was completed by MG.
4Findings
4.1Participant details
Fourteen participants from schools in the West of Ireland designated as serving populations of high socioeconomic need participated in the study. The sample included teachers (n = 7) and children with DLD (n = 7). Characteristics of participants presented in Tables 1 and 2.
Table 1
Participant details (adults)
| Participant reference | Gender M/F | Current role | Focus group (1 or 2) | School location Urban/Rural |
| T1 | F | Mainstream class teacher | 1 | Urban |
| T2 | F | Special education teacher (SET) | 1 | Urban |
| T3 | M | Special Education Needs (SEN) Coordinator &SET | 1 | Urban |
| T4 | F | Special education teacher (SET) | 2 | Rural |
| T5 | F | Special class teacher | 2 | Rural |
| T6 | F | Mainstream class teacher | 2 | Rural |
| T7 | F | Special class teacher | 2 | Rural |
Note: Mainstream class teachers have first-line responsibility for the education of all students in their class. Special education teachers (SETs) provide additional teaching to students with special educational needs. Special class teachers work with students with more complex special educational needs, in a smaller class, within their local mainstream school. A special education needs (SEN) coordinator is responsible for managing, organizing, and monitoring special education teaching in a school under the guidance of the principal.
Table 2
Participant details (children)
| Participant reference | Gender M/F | Age in years | School type Urban/Rural | Individual or paired interview | Setting | In-school / Virtual data capture |
| C1 | M | 9 | Rural | Paired | ‘Special’ classes for pupils with specific speech and language disorder | In-school |
| C2 | F | 10 | Rural | Paired | ‘Special’ classes for pupils with specific speech and language disorder | In-school |
| C3 | F | 11 | Rural | Individual | ‘Special’ classes for pupils with specific speech and language disorder | Virtual platform |
| C4 | M | 10 | Urban | Individual | Mainstream Classroom | In-school |
| C5 | M | 9 | Urban | Individual | Mainstream Classroom | In-school |
| C6 | F | 11 | Urban | Individual | Mainstream Classroom | In-school |
| C7 | F | 11 | Urban | Individual | Mainstream Classroom | In-school |
4.2Findings
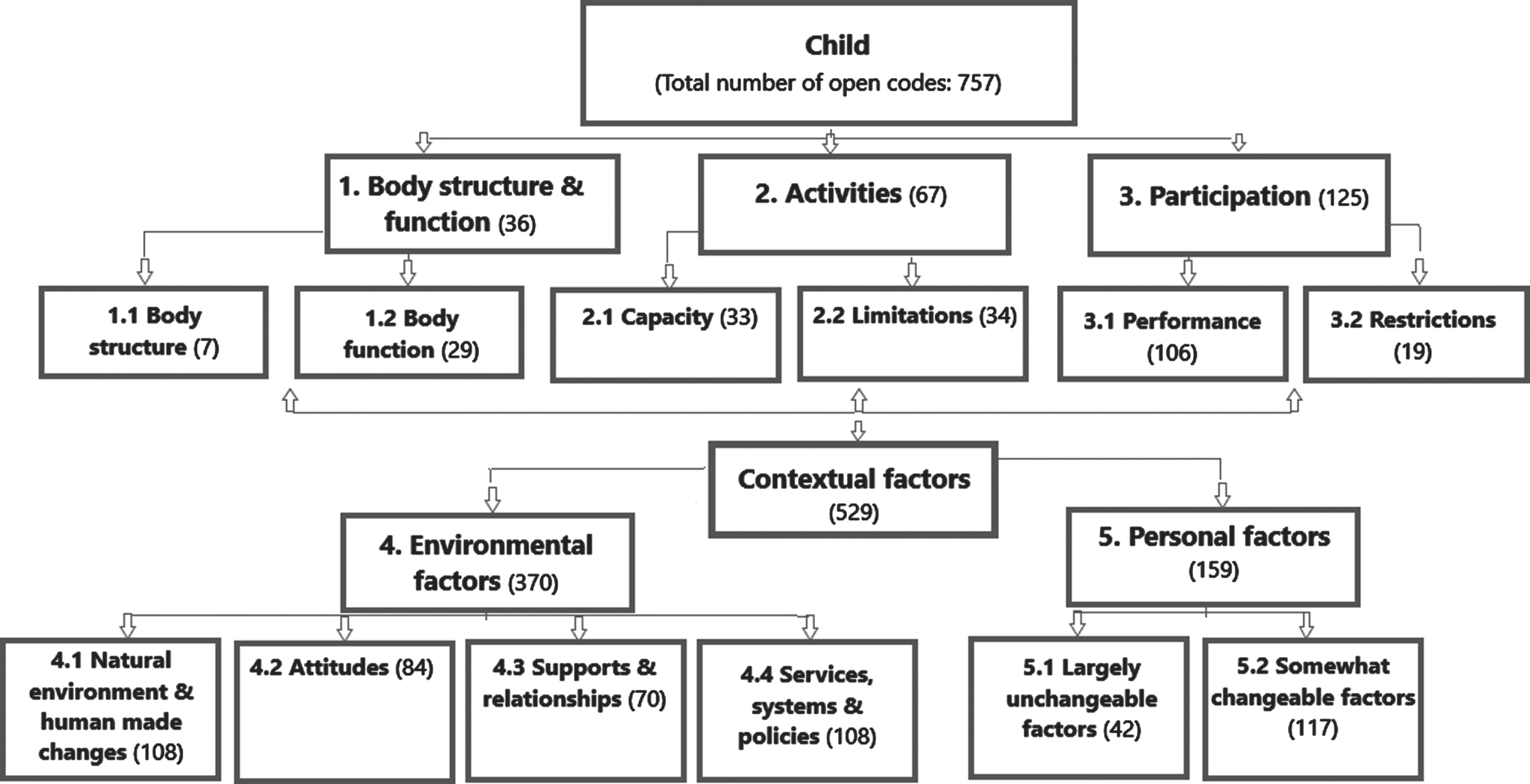
A descriptive summary of the findings under each ‘theme’ is provided below with illustrative quotes from across the dataset. The number of open codes mapped under each theme are presented in Fig. 1. Recall that ‘themes’ in this analytical process are the domains of the ICF framework. Under each theme, findings are further described in relation to the subcategories of the ICF.
Fig. 1
Number of open codes organized within each category under the five themes of the ICF.
4.3Theme 1: Body Structure and Function
Body structure and function (the physiological functions of body systems, including psychological functions) was the least discussed topic and was discussed primarily by teachers. They expressed a lack of clarity in relation to diagnostic terminology when referring to DLD and were noted to use a variety of terms in the focus group discussions. When describing the needs of children with DLD, teachers tended to discuss more observable non-linguistic rather than linguistic behaviours:
‘And you could nearly see it, like, in him, like if you’d say something, you could see him trying to process it in his head on his face’. [T7]
Several teachers described cognition as an area of strength in children with DLD and shared the belief that cognitive strengths were an identifying characteristic of this group, compared with other profiles of need in school. Children did not use diagnostic labels, instead referring to their language abilities in descriptive terms:
‘When I was younger, I didn’t really know how to talk that well’ [C5]
4.4Theme 2: Activity
Activity (the execution of a task or action by an individual) was discussed by both teachers and children. Both sets of participants reported that practical subjects were easier for children with DLD as they aid concentration:
‘he would lose himself in art and while he was doing anything with his hands’ [T5]
Mathematics was also noted as an area of strength from the perspective of the children with DLD when concentrating:
‘if my brain is turned on, I kind of get them (sums) all right’ [C1]
Limitations discussed related to aspects of speech, memory, and literacy skills. Teacher comments were related to directly observable behaviours such as poor speech intelligibility and when children use phrases to avoid responding:
“I don’t know’, that was his response to everything’ [T3]
whereas children commented more on difficulties related to listening and attention.
‘I very not concentrate. That my problem’. [C2]
4.5Theme 3: Participation
Participation (or involvement of people in all areas of life, and the participation restrictions they experience) was discussed by teachers and children. Children tended to report on their successes in participating in the classroom such as when actively engaged in tasks like explaining and describing ideas, when producing artefacts in practical activities and/or when they got something right. This contrasted with teachers who referred more to children’s restrictions, particularly in terms of social skills, taking turns, contributing to classroom discussions, and in having friends:
‘He finds it very hard to follow rules and wait for his turn . . . he has no friends’ [T2]
Both teachers and children noted difficulties or restrictions in relation to homework.
4.6Theme 4: Environmental factors
This was the most frequently discussed theme by both participant groups. The findings are described under four categories provided by the ICF under this domain including: (a) natural environment and human made changes, (b) attitudes, (c) supports and relationships, and (d) services, supports and policies.
In terms of ‘natural environment and human made changes,’ both stakeholder groups described the critical role that the classroom teacher plays in meeting the needs of the child with DLD in school. Both teachers and children described the optimal classroom as a ‘quiet’ space with a calm teacher, and one where the teacher makes the child with DLD feel like they belong. In terms of teacher strategies, the children noted the importance of the use of rewards, and the need to integrate breaks from learning with movement. Effective communication supports identified by the children included repeating instructions, being given time to talk, keeping instructions short, and agreeing ways of asking for clarification in the classroom:
‘Em, because when you don’t do what M says you ask her ‘can you please do that again’ [C1]
In terms of ineffective strategies, children stated that they did not like teachers drawing negative attention when they weren’t listening.
Teachers identified the importance of pace (giving the child time to answer), the use of role reversal (letting the child be the teacher), and the use of visual support systems. Asking the child to repeat back instructions immediately after hearing them to check understanding was also identified as effective. Teachers talked about the ways in which oracy and confidence building opportunities can be integrated across subjects. Unhelpful strategies from the teacher’s perspective included a high teacher workload, setting tasks with language heavy demands, and the physical constraints of the building such as ‘noisy’ classrooms.
In terms of ‘attitudes,’ children noted that they had experienced situations where teachers and peers were unsupportive, describing episodes when they were picked on or laughed at by peers:
‘And that when everyone making fun of me and I get laughed at’ [C1]
Teachers also noted that there can be negative attitudes towards children with SEN in schools on the part of teachers, but that this was mainly where a teacher does not have additional training in how to support a child’s needs.
In terms of ‘supports and relationships,’ teachers discussed the importance of a trusting professional relationship with an SLT. Regular communication between the teacher and the SLT such as scheduled check-in phone calls between visits, and opportunities for collaborative planning and problem solving together were identified as essential to optimising the classroom for children with DLD:
‘I think it’s important that there is somebody at the end of the phone that can say ‘that’s great stuff, that will be normal for at child at that level, keep doing it and come back to me in another couple of weeks” [T3]
Conversely, having limited or no contact from an SLT was identified as a significant barrier to meeting the needs of children with DLD in school. Where the SLT service provided programmes of activities for individual children to carry out without therapy techniques being modelled, it was not always feasible for the teacher to implement these in the classroom setting.
With regards to ‘supports, services and policies,’ teachers described the role of the special education teacher as particularly important as these teachers have the time to fully understand a child’s language profile, and to deliver individualised supports. Teachers also stated a preference for school based SLT services. The advantages of ‘special’ classes for pupils with specific speech and language disorder’ were described by teachers as a setting where children make progress because they get access to an SLT:
‘the children were brought on so much because they had access to a speech and language therapist every single day’ [T1]
A variety of issues in relation to SLT services were discussed by teachers. These included inappropriate or unrealistic service access criteria, long gaps in service delivery due to minimal staffing, and logistical barriers for parents where SLT services were only provided in health clinics.
Children also discussed SLT services. They described having to leave school to go to their local health centre as inconvenient. They also described unpleasant smells they encountered in the clinic building, and the inappropriately small furniture they were made to sit on in the clinic room. In relation to ‘special’ classes for pupils with specific speech and language disorder’, one child noted that attending a such class disrupted his friendships:
‘Except for first and second (class). I go to a different classroom . . . so I had to wait two years to meet them (friends) again in third class’ [C4]
4.7Theme 4: Personal factors
Personal factors were the second most discussed theme. Two categories are provided by the ICF under this domain. The categories include: (a) somewhat changeable factors and (b) largely unchangeable factors.
Children discussed feelings about school as important and that positive feelings could be enhanced where teachers knew and actively sought to tap into the child’s hobbies and interests. Common activities discussed by children as promoting positive feelings included reading, playing with Lego, drawing, and time in the outdoors. A supportive family and home life where they could relax and be themselves was valued by the children.
Teachers reported that parents’ understanding of how services work was an important factor which could be supported to help secure supports for the child in the school. Teachers also discussed the resilience of the child as an important mutable factor which could be improved.
Teachers discussed some factors related to some children’s home life as largely unchangeable and as being problematic. Some teachers discussed having another language at home as being a disadvantage for children with DLD, as well as presenting barriers to communication with parents:
‘it’s very hard to get to the bottom between the parents . . . are saying that they’re OK in their own language or the parents, I don’t know’ [T2]
Some children experienced differences between their first language to that of the school language as negative:
‘No, I never knew how to speak English until I started going to school . . . really weirdly, a weird feeling’ [C4]
5Discussion
Understanding contextual and priority needs can increase the likelihood of successful outcomes in health promotion efforts. We engaged teachers and children with experience of a range of school settings from schools in the West of Ireland to inform the development of a locally responsive health promotion intervention about DLD. A narrative inquiry approach was employed and ‘draw and tell’ techniques were used in semi-structured interviews with children with DLD.
As per previous studies, children described their optimal classroom as a calm space where they have a sense of belonging, and where their interests are taken into consideration. In terms of participation, children spoke more about what enables their success when contributing in class as opposed to their failures. This is also consistent with findings from identity research, where children could have positive self-perceptions in a context of poor academic progress (Lyons & Roulstone, 2017). These findings add to a growing body of research in the field of SLT literature of the importance of gaining children’s views about what practical, facilitative communication strategies are, and are not acceptable to them in the classroom in relation to their language needs (Gallagher, et al., 2020, Lyons & Roulstone, 2018).
In contrast to previous studies, and aligned with inclusive education policy, we identified agreement between teachers and children on the many practical classroom strategies that can support the inclusion of the child with DLD in the classroom. Combined, the stakeholders produced a list of actionable techniques to make their classroom more communication friendly, the efficacy of which have been previously established (Dockrell et al., 2014). These strategies included pacing, reducing language load, the use of visual supports, increased opportunities for reciprocal teaching amongst others. These findings show that engaging stakeholders in the development of health promotion interventions can ensure acceptable, universal level techniques that advance the inclusion of the children with DLD in the classroom.
Despite efforts to increase awareness of the condition since the publication of CATALISE recommendations (Bishop et al., 2016; Bishop et al., 2017), our study highlights the continued need for health promotion efforts to address knowledge gaps if we are to support the accurate identification of DLD in schools (Bishop, et al., 2017; Mc Gregor 2020). Of particular concern were the negative views of being exposed to more than one language at home, and the continued belief that cognitive referencing is a valid means of identifying children with DLD. Without education and training, teachers may continue to over or under diagnose the condition as is reported currently in the literature or, at best, to focus solely on observable linguistic elements, resulting in an exclusive focus on oracy. Whilst an important element of supporting the needs of children with DLD is building vocabulary and grammar use, it means that the needs of children with comprehension difficulties are likely to go unaddressed.
Engaging with stakeholders has highlighted the continued need for health promotion efforts to increase understanding of the nature and characteristics of DLD in Irish schools in the West of Ireland. It has also provided important insights into the priorities of children and teachers in these schools providing clear guidance as to the priority concerns of these stakeholders. Practical ideas mainly focused on the classroom setting have been identified as important content for a health promotion intervention. It is sobering to note that teachers in this study valued and sought collaborative working relationships with SLTs to meet the needs of children with DLD but spoke of many barriers to accessing and navigating local SLT services. The need to include very basic practical steps to help teachers to reach out to local SLT services is also highlighted as is the need for health services to ensure systems are in place to respond to these communicative efforts from schools about SLT supports.
6Strengths and limitations
The use of narrative inquiry (Lyons, et al., 2022) is a strength of the study as it allowed the participants share their experiences more openly with minimal prompting from the interviewer. Use of the COREQ (Tong, et al., 2007) reporting guidelines enhanced credibility. The transferability of the findings would have been further enhanced had we recruited non-DEIS as well as DEIS schools. We acknowledge the aims of qualitative inquiry are such that the findings should not be viewed as representative of the views of all teachers and children with DLD. The ICF framework (WHO, 2001) was determined to be ‘best fit’ however we acknowledge that the domains of body structure and function do not necessarily fully encapsulate the characteristics of neurodevelopmental conditions.
7Conclusions
Understanding contextual and priority needs can increase the likelihood of successful outcomes in health promotion efforts. We explored the views of teachers and children about DLD to provide insights to guide the development of a locally responsive health promotion intervention. Findings show the need to focus on the use of up-to-date terminology and evidence-informed markers of the DLD as well as the need to include practical tools and techniques to optimise classroom communication for children with DLD. Myth busting about DLD in the context of bilingualism is also warranted. The importance of cross-sectoral partnerships between health and education is highlighted.
Acknowledgments
The authors acknowledge the children and teachers for their time and input.
Conflict of interest
The authors have no conflict of interest to report.
References
1 | Adlof, S. M. , Hogan, T. P. ((2019) ) If we don’t look, we won’t see: Measuring language development to inform literacy instruction, Policy Insights from the Behavioral and Brain Sciences 6: (2), 210–217. https://doi.org/10.1177/2372732219839075 |
2 | Adlof, S. M. , Scoggins, J. , Brazendale, A. , Babb, S. , Petscher, Y. ((2017) ) Identifying children at risk for language impairment or dyslexia with group administered measures, Journal of Speech, Language, and Hearing Research: JSLHR 60: , 3507–3522. https://doi.org/10.1044/2017_JSLHR-L-16-0473 |
3 | Beard, A. ((2017) ) Speech, language, and communication: A public health issue across the lifecourse, Paediatrics and Child Health (Oxford) 28: (3), 126–131. https://doi.org/10.1016/j.paed.2017.12.004 |
4 | Birt, L. , Scott, S. , Cavers, D. , Campbell, C. , Walter, F. ((2016) ) Member checking: A tool to enhance trustworthiness or merely a nod to validation? Qualitative Health Research 26: (13), 1802–1811 https://doi.org/10.1177/1049732316654870 |
5 | Bishop, D. V. M. , Snowling, M. J. , Thompson, P. A. , Greenhalgh, T. the CATALISE consortium ((2016) ) CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children, PLoS One 11: (7), e0158753. https://doi.org/10.1371/journal.pone.0158753 |
6 | Bishop, D. V. M. , Snowling, M. J. , Thompson, P. A. , Greenhalgh, T. the CATALISE-2 consortium. ((2017) ) Phase of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology, Journal of Child Psychology and Psychiatry, and Allied Disciplines 58: (10), 1068–1080. https://doi.org/10.1111/jc12721 |
7 | Bloch, P. , Toft, U. , Reinbach, H. C. , Clausen, L. T. , Mikkelsen, B. E. , Poulsen, K. , Jensen, B. B. ((2014) ) Revitalizing the setting approach - supersettings for sustainable impact in community health promotion, The International Journal of Behavioral Nutrition and Physical Activity 11: , 118. https://doi.org/10.1186/s12966-014-0118-8 |
8 | Clandinin, J. , Connelly, F. M. (1994). Personal experience methods. In N. Denzin&Y. Lincoln (Eds.), Handbook of Qualitative Research. Sage. |
9 | Cohen, N. J. , Menna, R. , Vallance, D. D. , Barwick, M. A. , Im, N. , Horodezky, N. B. ((1998) ) Language, social cognitive processing, and behavioral characteristics of psychiatrically disturbed children with previously identified and unsuspected language impairments, Journal of Child Psychology and Psychiatry, and Allied Disciplines 39: (6), 853–864. https://doi.org/10.1111/1469-7610.00286 |
10 | Creswell, J. W. (2007). Qualitative Inquiry and Research Design: Choosing among Five Traditions (2nd ed.). Sage. |
11 | Dockrell, J. , Lindsay, G. , Roulstonw, S. , Law J. , ((2014) ) Supporting children with speech, language and communication needs: an overview of the results of the Better Communication Research Programme, International Journal of Language & Communication Disorders 49: (5), 543–547. https://doi.org/10.1111/1460-6984.12089 |
12 | Duncan, E. A. S. , Nicol, M. M. ((2004) ) Subtle Realism and Occupational Therapy: An Alternative Approach to Knowledge Generation and Evaluation, British Journal of Occupational Therapy 67: (10), 453–456. https://doi.org/10.1177/030802260406701006 |
13 | Ebbels, S. H. , McCartney, E. , Slonims, V. , Dockrell, J. E. , Norbury, C. F. ((2019) ) Evidence-based pathways to intervention for children with language disorders, International Journal of Language & Communication Disorders 54: (1), 3–19 https://doi.org/10.1111/1460-6984.12387 |
14 | Fallon, L. M. , Cathcart, S. C. , DeFouw, E. R. , O’Keeffe, B. V. , Sugai, G. ((2018) ) Promoting teachers’ implementation of culturally and contextually relevant class-wide behavior plans, Psychology in the Schools 55: (3), 278–94. https://doi.org/10.1002/pits.22107 |
15 | Gale, N. K. , Heath, G. , Cameron, E. , Rashid, S. , Redwood, S. ((2013) ) Using the framework method for the analysis of qualitative data in multi-disciplinary health research, BMC Medical Research Methodology 13: (117), 117. https://doi.org/10.1186/1471-2288-13-117 |
16 | Gallagher, A. L. , Murphy, C. A. , Conway, P. F. , Perry, A. ((2021) ) Establishing premises for inter-professional collaborative practice in school: inclusion, difference and influence, Disability and Rehabilitation 43: (20), 2909–2918 https://doi.org/10.1080/09638288.2020.1725154 |
17 | Gallagher, A. L. , Murphy, C. A. , Conway, P. F. , Perry, A. (2021a). Consequential differences in perspectives and practices concerning children with developmental language disorders: An integrative review, International Journal of Language & Communication Disorders 54: (4), 529–552 https://doi.org/10.1111/1460-6984.12469 |
18 | Gallagher, A. L. , Murphy, C. A. , Conway, P. F. , Perry, A. (2021b). Engaging multiple stakeholders to improve speech and language therapy services in schools: An appreciative inquiry-based study, BMC Health Services Research 19: (1), 226–https://doi.org/10.1186/s12913-019-4051-z |
19 | Greenwood, C. R. , Carta, J. J. , Walker, D. , Watson-Thompson, J. , Gilkerson, J. , Larson, A. L. , Schnitz, A. ((2017) ) Conceptualizing a Public Health Prevention Intervention for Bridging the Million Word Ga, Clinical Child and Family Psychology Review 20: (1), 3–24. https://doi.org/10.1007/s10567-017-0223-8 |
20 | Irish Association of Speech and Language Therapists (IASLT). (2017). Supporting Children with Developmental Language Disorder in Ireland: IASLT Position Paper and Guidance Document. |
21 | Johnson, N. , Van Hecke, A. ((2015) ) Increasing awareness in inner-city churches: A brief report, Pediatric Nursing 30: , e63–e69. https://doi.org/10.1016/j.pedn.2015.04.008 |
22 | Kitzinger, J. ((1995) ) Qualitative Research: Introducing focus groups, BMJ 311: (7000), 299–302. https://doi.org/10.1136/bmj.311.7000.299 |
23 | Law, J. , Levickis, P. , McKean, C. , Goldfield, S. (2017). Child Language in Public Health Context. Policy Brief Synthesising research evidence to inform policy. Murdoch Childrens Research Institute. |
24 | Law, J. , Reilly, S. , Snow, P. C. ((2013) ) Child speech, language and communication need re-examined in a public health context: A new direction for the speech and language therapy profession, International Journal of Language & Communication Disorders 48: (5), 486–496. https://doi.org/10.1111/1460-6984.12027 |
25 | Lyon, A. R. , Cook, C. R. , Locke, J. , Davis, C. , Powell, B. J. , Waltz, T. J. ((2019) ) Importance and feasibility of an adapted set of implementation strategies in schools, Journal of School Psychology 76: , 66–77. https://doi.org/10.1016/j.js2019.07.014 |
26 | Lyons, R. , Carroll, C. , Gallagher, A. , Merrick, R. , Tancredi, H. ((2022) ) Understanding the perspectives of children and young people with speech, language, and communication needs: How qualitative research can inform practice, International Journal of Speech-Language Pathology 24: (5), 547–557. https://doi.org/10.1080/17549507.2022.2038669 |
27 | Lyons, R. , Roulstone, S. ((2017) ) Labels, identity, and narratives in children with primary speech and language impairments, International Journal of Speech-Language Pathology 19: (5), 503–518. https://doi.org/10.1080/17549507.2016.1221455 |
28 | Lyons, R. , Roulstone, S. ((2018) ) Listening to the voice of children with developmental speech and language disorders using narrative inquiry: Methodological considerations, International Journal of Language & Communication Disorders 72: , 16–25 https://doi.org/10.1016/j.jcomdis.2018.02.006 |
29 | McKean, C. , Reilly, S. , Bavin, E. L. , Bretherton, L. , Cini, E. , Conway, L. , Cook, F. , Eadie, P. , Prior, M. , Wake, M. , Mensah, F. (2017, March). Language Outcomes at Years: Early Predictors and Co-Occurring Difficulties, Pediatrics 139: (3), e20161684. https://doi.org/10.1542/peds.2016-1684 |
30 | McGregor, K. K. ((2020) ) How we fail children with developmental language disorder, Language, Speech, and Hearing Services in Schools 51: , 981–992 https://doi.org/10.1044/2020_LSHSS-20-00003 |
31 | Norbury, C. F. , Gooch, D. , Wray, C. , Baird, G. , Charman, T. , Simonoff, E. , Vamvakas, G. , Pickles, A. ((2016) ) The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study, Journal of Child Psychology and Psychiatry, and Allied Disciplines 57: , 1247–1257 https://doi.org/10.1111/jc12573 |
32 | Royal College of Speech and Language Therapists (RCSLT). (2018). Giving voice to people with developmental language disorder. |
33 | Rix, J. , Sheehy, K. , Fletcher-Campbell, F. , Crisp, M. , Harper, A. ((2013) ) Exploring provision for children identified with special educational needs: An international review of policy and practice, European Journal of Special Needs Education 28: (4), 375–391. https://doi.org/10.1080/08856257.2013.812403 |
34 | Sudharshan Reddy, M. ((2019) ) A preliminary report on awareness of communication disorders among nursing trainees and primary school teachers, Indian Journal of Pediatrics 19: , 500–508. |
35 | Sudharshan Reddy, M. , Shanbal, J. C. , Arunraj, K. ((2016) ) Awareness of communication disorders in Hospet Taluk of Karnataka: A preliminary survey report, Indian Journal of Pediatrics 16: , 132–144. |
36 | Tomblin, J. B. , Records, N. L. , Buckwalter, P. , Zhang, X. , Smith, E. , O’Brien, M. ((1997) ) Prevalence of specific language impairment in kindergarten children, Journal of Speech, Language, and Hearing Research: JSLHR 40: , 1245–1260 https://doi.org/10.1044/jslhr.4006.1245 |
37 | Tong, A. , Sainsbury, P. , Craig, J. ((2007) ) Consolidated criteria for reporting qualitative research COREQ): a item checklist for interviews and focus groups, International Journal for Quality in Health Care 19: (6), 349–357 https://doi.org/10.1093/intqhc/mzm042 |
38 | World Health Organisation (WHO) (2001) International Classification of Functioning, Disability, and Health (ICF). http://www.who.int/classifications/icf/en/ |


