
Evacuation safety effects of a lightweight elevator-type evacuation device using carbon material: Focus on plantar pressure and muscle strength
Abstract
BACKGROUND:
Elevator-type evacuation devices have proven to be feasible in high-rise buildings through studies on safety performance and evacuation time. However, there is a lack of research on safety using biosignal analysis in the elderly population.
OBJECTIVE:
A carbon material is used in this study to reduce the weight of an evacuation elevator. The impact on the human body is evaluated by conducting a satisfaction survey involving elderly and youth groups and quantitatively analyzing biological signals, including electromyography (EMG) and plantar pressure, during five repeated uses of the proposed device.
METHODS:
The study involves 12 healthy adults in their 20s and 20 elderly individuals with no experience in using an evacuation elevator. The EMG and left and right plantar pressures are analyzed to evaluate the physical factors affected by repeated use.
RESULTS:
The experiment results showed that the normalization of EMG to maximum voluntary contraction showed a significant decrease with repeated use, especially in the right tibialis anterior muscle. Moreover, plantar pressure shows a significant difference, which decreased with repetition, and the left and right balance gradually tilted to the left.
CONCLUSION:
This suggests that with more repeated use, muscle tension decreases owing to adaptation, resulting in lower muscle activity and plantar pressure. Particularly, the tibialis anterior muscle experiences significant muscle activity, indicating increased load, but without any apparent danger. In the future, it will be necessary to evaluate elevators for disabled individuals.
1.Introduction
In modern society, high-rise buildings are becoming increasingly prevalent owing to the rising population density caused by urbanization. The risk of disaster increases with an increase in the number of high-rise buildings. Unlike regular buildings, high-rise buildings can cause massive casualties in the event of a fire. To prevent casualties in disaster situations, it is imperative to ensure the ability of occupants to safely evacuate. This requires the development of design standards for securing evacuation safety and the provision of facilities and equipment that enable self-evacuation. The evacuation mechanisms specified in Article 3 of the Fire Safety Standards (NFSC 301) include evacuation ladders, turbines, simple turbines, rescue teams, air safety mats, evacuation equipment, top-down evacuation ladders, and evacuation elevators. Among them, an elevator-type evacuation device is designed to be universally adaptable for use in all high-rise buildings, with consideration for the specific installation requirements of each firefighting site [1].
Among these, descending lifelines and rescue sacks are the most commonly used because of their cost-effectiveness and minimal installation space requirements, but the structures of these evacuation devices are challenging to use for safely evacuating vulnerable groups (especially the elderly and disabled), whose physical activity is limited [2, 3]. In addition, they take a lot of preparation time before use during an emergency. Because of risk factors such as falls, fire-related laws mandate them to be used only up to the 10th floor, with installation restricted to the 11th floor or higher. Therefore, not all buildings with more than 11 floors have evacuation mechanisms, resulting in blind spots concerning disaster safety [1].
Introduced by the 2011 National Fire Safety Standards (NFSC 301), the lift evacuation device can be installed by connecting it to the inner balcony, outer wall, and balcony of the apartment; it is a fire evacuation device that descends by gravity without power. It is designed not only to replace direct (emergency) stairs under the Building and Fire Fighting Acts, but also to allow the disabled and the elderly to escape independently [4].
An elevator-type evacuation device is an unpowered structure that descends one floor at a time, under the weight of the occupants. When a rider gets on board and presses the start button, the descent begins. When a passenger leaves the elevator after descending one floor, the wire is wound around the wind-up box, and the elevator plate returns to the top using the energy stored when descending. The weight of the board depends on the driving force of the main spring box, which is the power unit. When the weight of the lifting plate is reduced, the size of the associated driving part is also reduced, thereby reducing risks during installation. In addition, reducing the weight of the lifting plate reduces the noise that can occur when the elevator board returns to the upper floor, thereby reducing psychological shock.
Elevator-type evacuation devices have proven to be feasible in high-rise buildings through studies on safety performance and evacuation time [5, 6]. However, there is a lack of research on safety using biosignal analysis in the elderly population.
Therefore, in this study, carbon was used as the lifting plate material to reduce the weight of the lifting plate, while achieving the same results as existing steel materials. In addition, to analyze the evacuation adaptability for safe evacuation, the distribution of the plantar pressure on the right foot when pressing the button and the electromyogram of the muscles involved in operating the elevating evacuation device were analyzed. This analysis was conducted through five consecutive usages of the elevating evacuation device by both elderly and young individuals.
2.Development of lightweight elevator-type evacuation device using carbon material
Figure 1.
Structure (left) and practical development (right) of the elevator-type evacuation device.
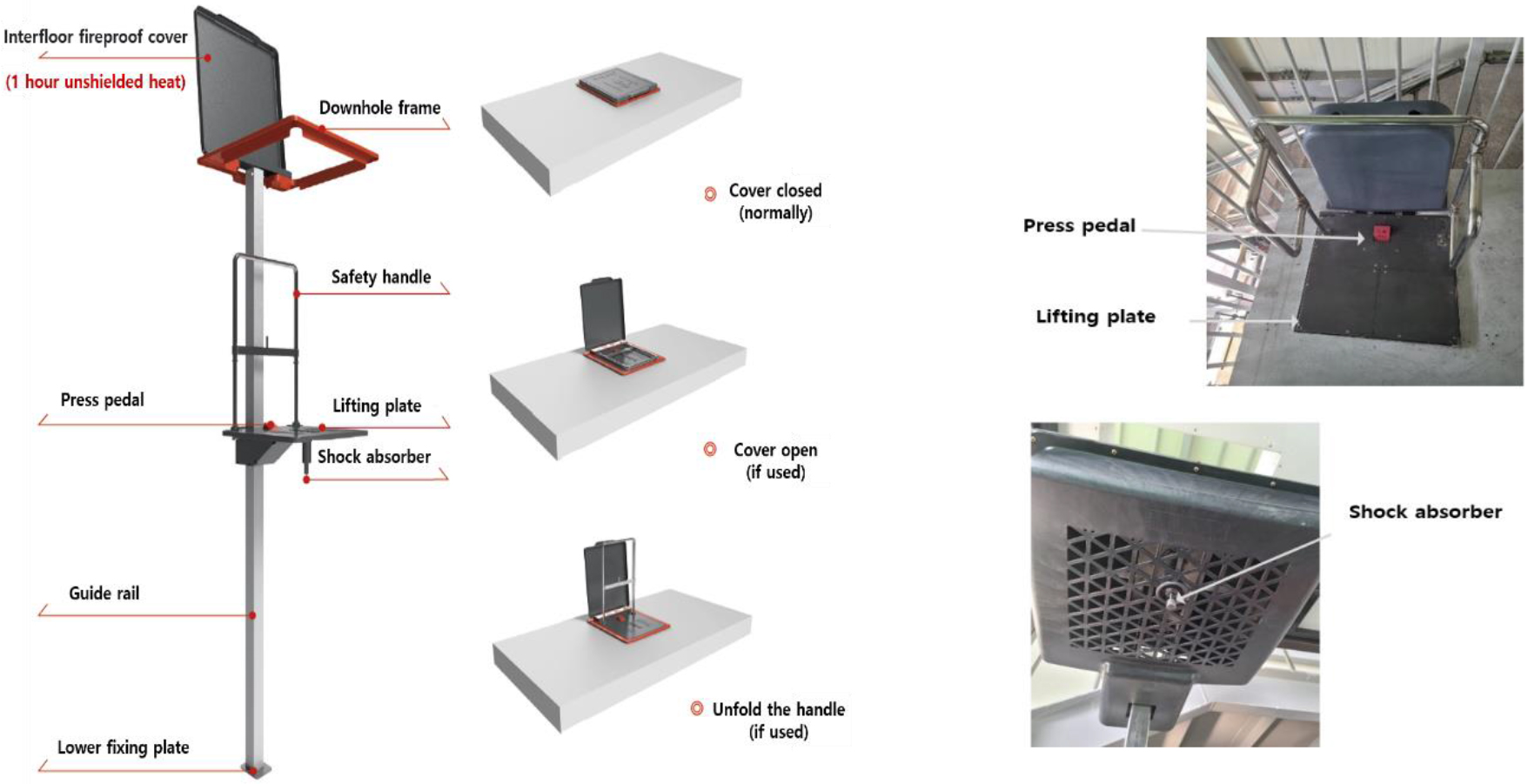
Figure 1 shows the elevator-type evacuation device used in this study by domestic company A, which consists of a cover applied through a fire-resistance test and an 83 cm-high folding handle connected to the lifting plate. The lifting plate was connected to a brake designed to withstand the load of the user, and the opening was 60 cm in diameter, which is sufficiently large for one adult male to pass through. The brake is released when the user stands on the platform, holds the safety handle, maintains balance, and then steps on the platform pedal button. At this time, the structure facilitates a single person to descend one floor at a time, via a guide rail connected to the elevator plate, using the gravity generated by the person’s weight. After being lowered, the elevator plate rises again using the potential energy stored in the driving unit (wire box) and returns to its original position. There is a shock absorber on the floor to relieve shock at a height of approximately 20 cm above the ground, and the devices (floors) can be installed at a height of 3–6 m.
When comparing existing iron and carbon materials (size: 639
3.Materials and methods
3.1Participants
The subjects included 12 elderly and 12 young individuals with no record of mental, nervous, or cardiovascular disease and no experience of using the evacuation elevator (Table 2). This study was approved by the Institutional Review Board of Jeonbuk National University (IRB No: 2020-08-022-001).
Table 1
Comparison of the existing steel and carbon materials
| Material | Modulus of elasticity (Gpa) | Thickness (mm) | Weight (kg) | Sagging (weight of material |
|---|---|---|---|---|
| Carbon | 200 | 3.2 | 2.442 | 2.42 |
| SS400 | 200 | 3.2 | 11.761 | 3.13 |
Table 2
Subject information
| Category | Number of subjects ( | Age (years) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| Elderly | 12 | 25.3 | 176 | 78.2 |
| Youth | 20 | 77.6 | 168.7 | 66.1 |
Table 3
Sequence of experiment
| Phase | Waiting | Press-Button | Descending | Landing |
|---|---|---|---|---|
| Acting | Hold onto the handle and wait | Take the foot off and step | Descend while stepping | Place both feet on |
| on the lifting platform | on the button | on the button | the lifting platform |
3.2Experimental procedure
Figure 2.
Peak pressure for three parts of the plantar area depending on the number of times the elevator-type evacuation device was used.
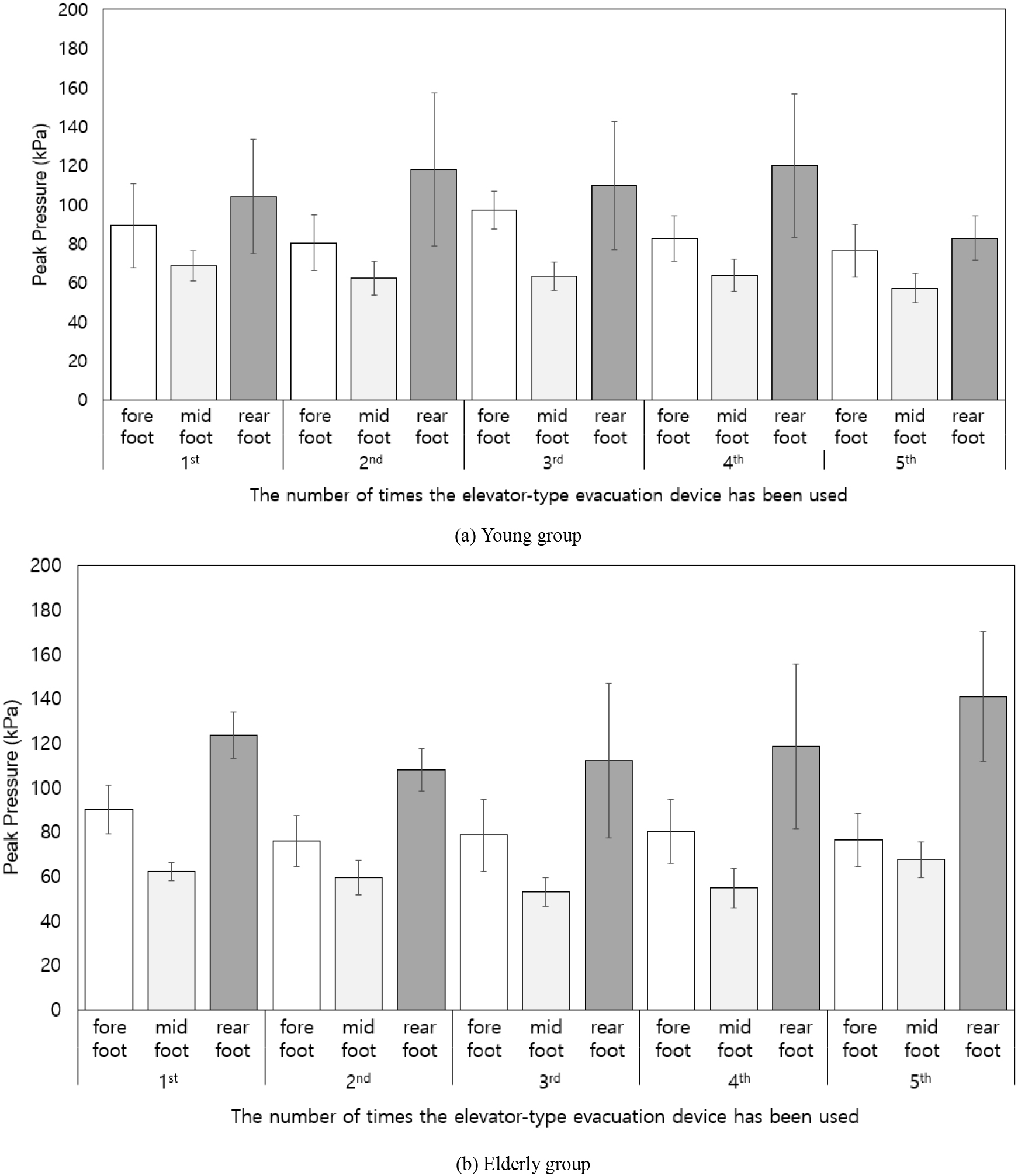
The experimental procedure is illustrated in Fig. 2. The subject got on the elevator, held the handle, and stood by. The subject was verbally instructed to step on the pedal button with their right foot to descend. Simultaneously, the muscle activity and plantar pressure were measured in real-time when the instrument was operated, and the measurements were completed after landing. This process was repeated five times.
In the case of electromyography (EMG), a surface EMG system (TeleMyo Desktop DT, Noraxon Inc., USA) was used to measure the muscle activity. Eight measurement areas were used: the right trapezius, brachioradialis, erector spinae, gluteus maximus, biceps femoris, vastus lateralis, gastrocnemius, and tibialis anterior. The sampling rate was 1,024 Hz. Bandpass filtering was performed on the raw EMG at 50–500 Hz. After a rectification process, the EMG data was analyzed to obtain its root-mean-square (RMS) value with a 50 ms overlapping window. A normalization process was necessary to minimize the differences in individual strengths. The normalized value was the maximum voluntary contraction ratio (MVC). The %MVC was analyzed by comparing the percentage with the EMG measured at a specific point using the EMG under maximal strength [7].
The right plantar pressure was measured in real time at the same time as the electromyogram measurement for the analysis of the subject’s left and right centers of pressure and contact pressure, and the measurement was completed after landing. The equipment used for the plantar pressure measurement was the Pedar-X System (Novel Gmbh, Germany), and to maximize the foot contact with the leading sensor of the equipment, flat-soled shoes were provided to increase reliability. The measured plantar pressure data analyzed the peak plantar pressure (kPa) of the right foot during button pressing when using the elevator evacuation machine, as in the EMG. In addition, the measured plantar pressure was analyzed by categorizing it into the forefoot, midfoot, and rearfoot regions.
4.Results
Figure 2 shows the peak pressure of the plantar area for each part of the foot according to the repeated use of the elevator-type evacuation machines by each group. The plantar pressure was analyzed based on the maximum pressure recorded at the moment of stepping on the working pedal of the elevator-type evacuation machine at each foot region (fore, mid, and rear). The peak plantar pressure in the forefoot area of young adults decreased from 90 kPa to 76 kPa (approximately 15.6%), from the first to fifth ride. There was a slight change in the midfoot area; however, in the hindfoot area, contrary to the forefoot, there was a 14.1% increase in the fifth ride compared with the first ride. The peak pressure of the plantar pressure in the forefoot area of the elderly decreased from 89 to 76 kPa (approximately 14%), from the first to fifth ride. In the midfoot area, it decreased by approximately 16.1% from 68 kPa to 57 kPa, and in the rearfoot area, unlike for the young population, it decreased by 20.2% during the fifth ride compared to the first ride.
Figure 3.
MVC (%) for the eight muscles in the young and elderly groups, based on the number of times the elevator-type evacuation device was used.
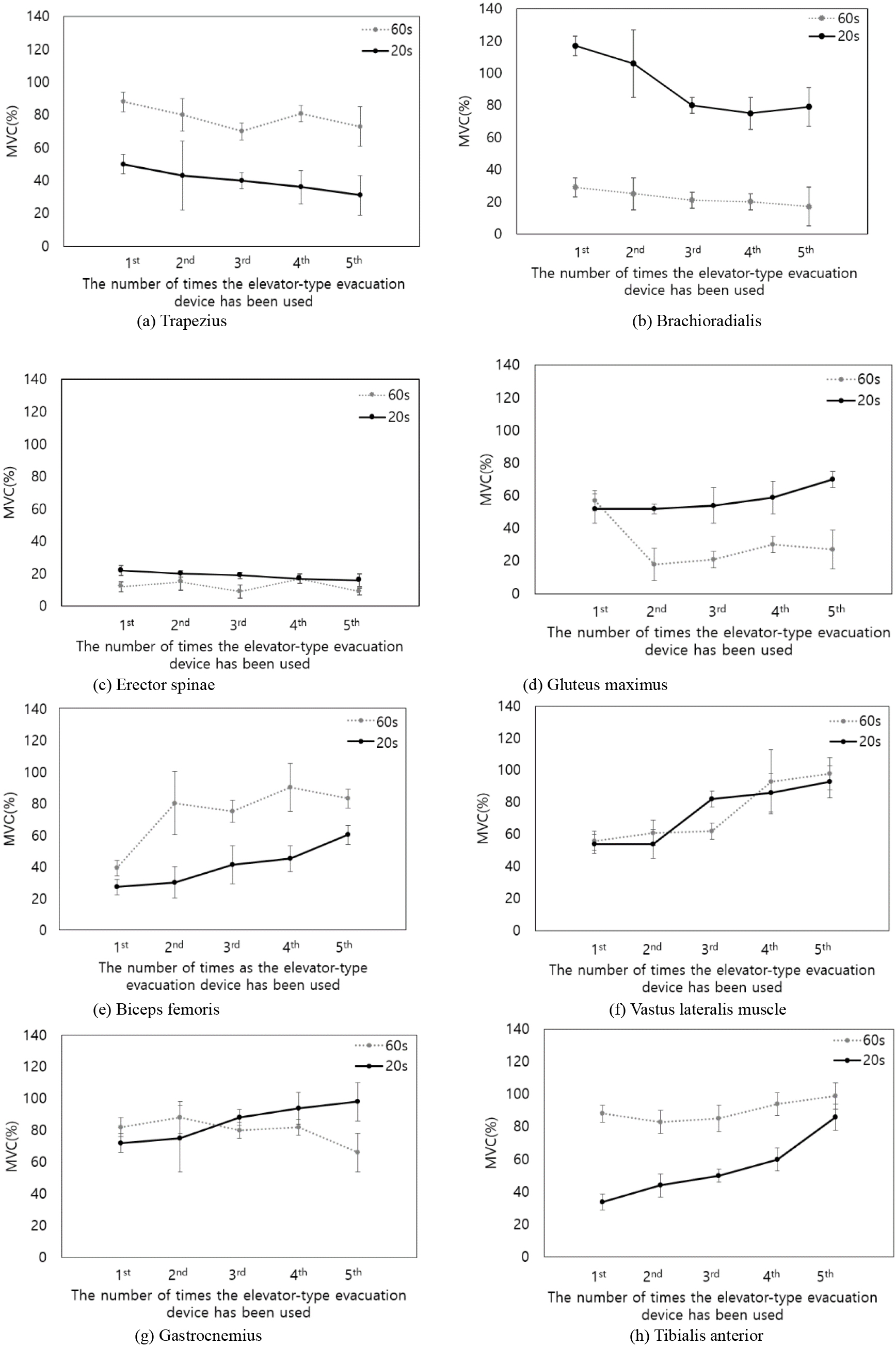
Figure 3 shows the muscle activity of each part when the elevator-type evacuation machines were used by the elderly and youth groups. The EMG was analyzed mainly for muscle activity during the stepping operation of the evacuation elevator, and standardization was performed using the MVC (%) of each subject for reliability according to the EMG characteristics due to physical differences. The measured MVC (%) is the maximum muscle force that each subject can produce during isometric contraction, and the raw EMG data measured when using the evacuation elevator was expressed as a ratio with respect to the MVC (%).
In the case of the young group, the MVC ratio of the trapezius and brachioradialis muscles, which are involved in holding the handle of the elevator-type evacuation device, decreased depending on the number of times the elevator-type evacuation device was used (trapezius:
In the elderly, the trapezius and brachioradialis muscles exhibited a slight decrease (trapezius:
5.Discussion
In this study, evacuation behavior was analyzed repeatedly using the EMG and plantar pressure obtained during the use of an elevator-type evacuation device. The EMG measured when pressing the pedal button of the elevator-type evacuation device was showed that the muscle activity gradually decreased with the repeated use of all muscles. The lack of experience in using the elevator-type evacuation device led to physical stiffness and heightened muscle activity in the user due to anxiety. This is analogous to the higher muscle activity observed during exercise and increased response rate due to the influence of stress on the central and peripheral nervous systems [1]. Accordingly, it was deduced that the anxiety decreased with repeated use, leading to an overall decrease in both the muscle activity and plantar pressure. This suggests that the stiffness caused by anxiety can be a risk factor during disaster situations. However, the use of an elevator is considered physically safe because the muscle activity shown in this study does not appear to have excessive activation or load factors.
In addition, the changes in the left and right pressure distributions, which shifted to the left, were compared with changes in the vastus lateralis, biceps femoris, and gastrocnemius muscles, which are involved in balance; the activity of all these muscles increased gradually. In this study, there was no relationship between the left and right pressure distributions and muscle activity, and it was inferred that there was no muscle load risk due to central movement. In particular, it can be interpreted that the load increased in the case of the tibialis anterior muscle, which has a large muscle activity, but there seemed to be no dangerous load factor because it was the primary muscle involved in the operation.
The vastus lateralis descends along the outer side of the thigh and is involved in knee joint movement [8]. The tibialis anterior extends from the shin to the soles of the feet and is involved in bending the back of the ankle joint and the extracorporeal action inside the soles [9]. The activity of the tibialis anterior was the highest compared to other muscles, and it exhibited the highest rate of increase and muscle activity (especially in the elderly group). This is attributed to it being the main muscle used in the process of pedaling with the right ankle.
The femoral bicep comprises the hamstring and is involved in the extension of the hip joint, flexion of the knee joint, and outer rotation of the calf. Alternatively, it prevents excessive knee elongation and stabilizes the knee and pelvis as soon as the foot touches the ground [10], to support the weight and stabilize the knee joint. When using the evacuation elevator, the right foot stepped on the pedal button, sole of the foot touched the ground, and right femoral biceps were initially more activated, and this seemed to increase with repetition.
The elevator-type evacuation device should descend at 11–130 cm/s, with a maximum load of 150 kg. When ascending, it returns at 40 cm/s carrying the weight of the empty platform [5]. Therefore, lightweight platforms can reduce the load on the accessories that lower the platform and allow them to return at a faster speed to facilitate faster evacuation. Thus, elevator-type evacuation devices can be used to evacuate one floor at a time from the upper floor to the lower floor in the form of vertical evacuation, making it easier for the elderly to evacuate compared with lifelines and rescue sacks.
The elderly not only need the help of others to evacuate safely in disaster situations but also interfere with the evacuation of others [11]. Owing to mobility issues caused by the weakening of musculoskeletal and cognitive functions, it is very difficult for the elderly to evacuate using stairs [12]. Therefore, when introducing evacuation devices, such as elevator-type evacuation devices, it is necessary to analyze how many times they can be used most effectively by the elderly. Therefore, in this study, we compared young and elderly groups to determine whether an elevator-type evacuation device could be used without harming the human body, by measuring the plantar pressure and EMG during five repeated uses of the device. The plantar pressure gradually increased in rear foot area of the young group and suddenly decreased in rear foot area of the elderly group at the fifth use, indicating that postural balance was disturbed during the fifth use. In the case of MVC (%), the increase in the tibialis anterior and gastrocnemius muscles, which directly affect pedaling, and vastus lateralis and biceps femoris muscles, which affect the balance of the lower limbs and right knee, suggests that repetitive use more than five uses is unreasonable for the elderly group. In a similar study, Joung and Yoon [13] deduced that the total evacuation time was reduced when the evacuation was guided in stages of five floors from the top floor after the immediate fire floor, compared to the simultaneous evacuation of all floors. This suggests that designing a five-story evacuation in increments of five floors can lead to a safe and efficient evacuation when elevator-type evacuation devices are used in high-rise buildings.
In this study, the elevated evacuation system was used repeatedly on one floor instead of being installed on each floor; therefore, there may be differences in its actual use. To compensate for this limitation, it is necessary to conduct research on the use of elevated evacuation systems on multiple floors. Future follow-up studies, such as surveys that include psychological variables of evacuees, are necessary.
6.Conclusion
In this study, a usability evaluation was conducted using a lightweight elevator, and human loads that can affect the evacuation behavior were evaluated using EMG and plantar pressure analysis.
The evaluation of the EMG and pressure of the elderly and young groups following repeated use shows that the muscle activity gradually decreased with the repeated use of all muscles in pressing the pedal button of the elevator-type evacuation machine. This suggests that high muscle activity and plantar pressure occur in the users when using the device for the first time. However, with repeated use, the anxiety decreased as the individuals adapted, resulting in an overall decrease in muscle activity and plantar pressure. In addition, there was no relationship between the left and right pressure distributions and muscle activity. Hence, there is no muscle load risk due to central movement. In particular, the load increased in the case of the tibialis anterior muscle, which showed significant muscle activity, but there was no dangerous load factor.
The results of this study appear to have no load factors in the evacuation behavior. Hence, the use of lightweight evacuation elevators is physically safe, and the data obtained can be used as basic biomechanical data for ergonomic instrument design and performance evaluation of existing elevator-type evacuation machines. For a more reliable evaluation in the future, it is necessary to conduct a performance evaluation that gathers feedback on discomfort, evaluates posture shaking using a tilt sensor, and makes comparisons with elderly and disabled individuals.
Acknowledgments
This research was supported by a grant (20022159) of the Regional Customized Disaster-Safety R&D Program, funded by the Ministry of Interior and Safety (MOIS, Korea).
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Ra PJ, Seul YM. A study on the necessity of introducing evacuation instrument in high-rise buildings-focusing on elevator type evacuation instrument. Fire Science and Engineering. (2014) ; 28: (3): 10-19. |
[2] | Jeon JI, Kong HS.Safe arm posture when using vertical rescue sack. The Journal of the Convergence on Culture Technology. (2020) ; 6: (1): 1-6. |
[3] | Lee SW. A study of the structural improvement in descending life lines for the fire emergency escaping purpose (DLL-FEEP) for the safety of the old and the infirm. Korean Journal of Safety Culture. (2021) ; 12: : 75-86. |
[4] | Choi KC, Park YJ. study on the improvement method of the performance technical standard of the elevator type evacuation device. Proceedings of the Korea Institute of Fire Science and Engineering Conference. Korean Institute of Fire Science & Engineering. (2022) . p. 72. |
[5] | Choi KC, Ra PJ, Bae HE, Park YJ. Analysis of the evacuation effect of entry-level elevator evacuation mechanism for high-rise communal houses. Korean Journal of Hazardous Materials. (2022) ; 10: (2): 18-24. |
[6] | Liu Y, Kim SK, Kim KH, Lee DH. Economic and evacuation time analysis of horizontally-installed indoor emergency exit. Journal of the Korea Institute of Building Construction. (2018) ; 18: (4): 363-373. |
[7] | Kim TY. Electromyographic Analysis: Theory and Application. Seoul (Korea): Hanmibook; (2014) . |
[8] | Grob K, Manestar M, Filgueira L, Kuster MS, Gilbey H, Ackland T. The interaction between the vastus medialis and vastus intermedius and its influence on the extensor apparatus of the knee joint. Knee Surgery, Sports Traumatology, Arthroscopy. (2018) ; 26: : 727-738. |
[9] | Wang R, GUTIERREZ-FAREWIK, Elena M. The effect of subtalar inversion/eversion on the dynamic function of the tibialis anterior, soleus, and gastrocnemius during the stance phase of gait. Gait & Posture. (2011) ; 34: (1): 29-35. |
[10] | Chevalier A, Van Overmeire A, Vermue H, Pringels L, Herregodts S, Victor J, Loccufier M. Effect of iliotibial band and gastrocnemius activation on knee kinematics. The Knee. (2023) ; 40: : 238-244. |
[11] | Willoughby M, Kipsaina C, Ferrah N, Blau S. Mortality in nursing homes following emergency evacuation: A systematic review. Journal of the American Medical Directors Association. (2017) ; 18: (8): 664-670. |
[12] | Ma J, Lo SM, Song WG. Cellular automaton modeling approach for optimum ultra high-rise building evacuation design. Fire Safety Journal. (2012) ; 54: : 57-66. |
[13] | Joung SH, Yoon MO. Vertical Evacuation Speed in Stairwell of a High-rise Office Building. Fire Science and Engineering. (2015) ; 29: (3): 13-20. |


