
Using markerless motion capture and musculoskeletal models: An evaluation of joint kinematics
Abstract
BACKGROUND:
This study presents a comprehensive comparison between a marker-based motion capture system (MMC) and a video-based motion capture system (VMC) in the context of kinematic analysis using musculoskeletal models.
OBJECTIVE:
Focusing on joint angles, the study aimed to evaluate the accuracy of VMC as a viable alternative for biomechanical research.
METHODS:
Eighteen healthy subjects performed isolated movements with 17 joint degrees of freedom, and their kinematic data were collected using both an MMC and a VMC setup. The kinematic data were entered into the AnyBody Modelling System, which enables the calculation of joint angles. The mean absolute error (MAE) was calculated to quantify the deviations between the two systems.
RESULTS:
The results showed good agreement between VMC and MMC at several joint angles. In particular, the shoulder, hip and knee joints showed small deviations in kinematics with MAE values of 4.8∘, 6.8∘ and 3.5∘, respectively. However, the study revealed problems in tracking hand and elbow movements, resulting in higher MAE values of 13.7∘ and 27.7∘. Deviations were also higher for head and thoracic movements.
CONCLUSION:
Overall, VMC showed promising results for lower body and shoulder kinematics. However, the tracking of the wrist and pelvis still needs to be refined. The research results provide a basis for further investigations that promote the fusion of VMC and musculoskeletal models.
1.Introduction
Musculoskeletal models are a useful tool in biomechanics. The models allow the calculation of various internal and external body parameters such as muscle activities/forces, joint reaction forces (JRF) and moments, and ground reaction forces (GRF) and moments [1]. However, these models rely on accurate input from motion capture data to assess real life situations.
For many years, the gold standard for motion capture in biomechanics was and still is marker-based motion capture (MMC). These systems use active or passive markers attached to subjects and cameras to detect the marker positions in space. In recent years, however, other concepts of motion tracking (e.g. acceleration based IMU sensors) have emerged and markerless, video-based motion capture (VMC) systems are gaining importance in biomechanics [2, 3, 4]. These systems perform motion capture using synchronized video camera recordings and often artificial intelligence algorithms to analyze human motion. They range from small applications with one or two cameras (smartphones, action cameras) to large motion capture setups with ten or more video cameras (action cameras, machine vision cameras, professional video cameras).
VMC systems have many advantages over MMC systems. In addition to being easier for users to set up, they allow for more realistic capture, eliminating the need to attach sensors or markers to subjects. Consequently, scientists can perform measurements on subjects in normal clothing and without markers, which reduces the artificiality of movement patterns and discomfort [2]. With these advantages, they also become interesting for sophisticated biomechanical analysis with musculoskeletal models like OpenSim models [5] or the AnyBody Modeling System (AMS, AnyBody Technology, DK). As a result of their increasing popularity and use in biomechanical motion analysis, the accuracy of VMC systems has also come under scrutiny.
Van Hooren et al. [6] performed gait analyses with an MMC system and a VMC system using DeepLabCut [7] and OpenPose [8]. Running on a treadmill was recorded with one camera from the side at 50 Hz and the root mean squared error (RMSE) was calculated in relation to the MMC system. They determined an uncorrected RMSE for DeepLabCut of 9.1∘ for hip flexion, 11.5∘ for knee flexion and 7.3∘ for ankle flexion. With OpenPose, they calculated an uncorrected RMSE of 6.9∘, 9.2∘ and 5.6∘ respectively. OpenPose was also used in combination with 9 machine vision cameras recording running, walking and counter-movement-jumps [9]. To compare the VMC kinematics to MMC recorded kinematics, they performed a Bland-Altman analysis of the kinematics calculated with an OpenSim model. The mean bias for hip flexion ranged from
Musculoskeletal simulation models, which use the kinematic data from the motion measurement systems as input variables, are often used for further biomechanical analyses. Therefore, in this case, in addition to data acquisition, further data processing in the simulation software must also be taken into account as part of the process chain in order to be able to make statements about the accuracies. This study therefore aims to compare the resulting kinematics of a musculoskeletal simulation software for a VMC system with those of an MMC model. The joint kinematics of the main joints of the human body are analysed in Range of Motion (ROM) measurements in order to keep the significance as general as possible and without focusing on a specific everyday movement.
2.Methods
For this study, 18 healthy subjects (12 male, 6 female) with a mean age of 23.8
2.1Experimental protocol
The subjects performed 17 different movements that were selected to cover a wide ROM for each major joint represented in the musculoskeletal model. The participants started the movements in a neutral position (
Table 1
Matrix of the investigated joints and DOF for the performed motions
| Head | Shoulder | Elbow | Hand | Pelvis-thorax | Hip | Knee | Ankle | |
|---|---|---|---|---|---|---|---|---|
| Flexion/extension |
|
|
|
|
|
|
|
|
| Abduction/adduction |
|
|
|
|
|
| ||
| Axial rotation |
|
|
|
1) Lateral bending, 2) supination/pronation, 3) inversion/eversion.
Movements were recorded with MMC and VMC. The MMC setup consisted of 12 infrared cameras (Vicon Vero 2.2, Vicon Motion Systems Ltd, UK) recording infrared reflective motion capture markers at 240 Hz. The marker setup was adapted from the full body plug-in-gait marker set with additional markers to the extremities, resulting in a total of 53 markers. Post-processing was performed using Vicon Nexus (v. 2.11, Vicon Motion Systems Ltd, UK). A hardware trigger was used to synchronize the MMC and VMC recordings.
The videos for VMC were recorded with eight machine vision cameras (FLIR Blackfly S16S2C, Teledyne FLIR LLC, USA) at 60 Hz and 1440
2.2Musculoskeletal modelling
Kinematic data from MMC and VMC was each used as input for the AnyBody Modeling System (AMS, v. 7.3, AnyBody Technology, DK) along with the subjects’ anthropometrics to calculate the joint angles. The full body plug-in-gait model from the AnyBody Managed Model Repository (AMMR, v. 2.3.3) served as a basis for both the MMC and the VMC models. This model was chosen since the markerset of the MMC models was similar and these models often serve as base models for various applications. The joints in the models are modeled as ideal joints with the respective degrees of freedom shown in Table 1. For the VMC model, a markerset was created in the AMS as it is used in CapturyLive. Kinematic input data was filtered in the models using a second order lowpass Butterworth filter with a cut-off frequency of 5 Hz. Even so, the kinematic input had different sample rates, all kinematic analyses in the musculoskeletal models were performed at 60 Hz. The workflow has been adapted from Lund et al. [24].
2.3Data processing
All model output was processed using Python (v. 3.11.0) and the packages numpy (1.24.1), pandas (1.5.3) pyCompare (v.1.5.2), scipy (1.10.0) and seaborn (0.12.2). To compare the MMC and VMC kinematic output, a Bland-Altman analysis [25] was performed and the mean absolute error (MAE), the MAE in relation to the joints ROM (MAEROM) and the Pearson correlation (r) were calculated for all three repetitions and the whole ROM. With MMC being regarded as gold-standard in motion capture, all MAE(ROM) values reported should be interpreted as deviation of the VMC dataset from the MMC dataset. Since most of the datasets of MAE, MAEROM and r were not normally distributed, this work reports median values and the corresponding confidence interval (CI) with a level of significance of 0.95.
3.Results
A total of 612 musculoskeletal simulations were evaluated to compare VMC and MMC. For the upper extremities, the MAE ranged from 6.8∘ for elbow and shoulder flexion to 37.4∘ for elbow supination. In relation to the ROM, this means a deviation of 4.9% and 4.8% in elbow and shoulder flexion and 27.7% for elbow supination. Hand flexion and abduction MAE was at 15.0∘ (13.7%) and 26.3∘ (47.9%). All MAE values for the upper extremity including the 95% CI can be found in Fig. 1. Pearson correlation r was
Table 2
Bias of the Bland-Altman analysis including the 95% limits of agreement (LoA) as well as median absolute error in relation to the ROM (MAEROM) and Pearson correlation
| Parameter | Bias [LoA] (∘) | MAEROM [95% CI] (%) | |
|---|---|---|---|
| Head flexion | 13.0 [10.8, 15, 6] | 0.99 [0.99, 1.0] | |
| Head lateral bending | 11.5 [10.1, 12.5] | 1.0 [0.99, 1.0] | |
| Head rotation | 12.0 [ | 7.6 [5.0, 14.7] | 1.0 [1.0, 1.0] |
| Shoulder flexion | 4.8 [4.0, 6.4] | 0.99 [0.99, 0.99] | |
| Shoulder abduction | 5.1 [4.2, 6.7] | 1.0 [1.0, 1.0] | |
| Elbow flexion | 6.4 [ | 4.9 [3.6, 6.4] | 1.0 [1.0, 1.0] |
| Elbow supination | 15.4 [ | 27.7 [20.4, 37.1] | 0.71 [0.49, 0.86] |
| Hand flexion | 13.7 [11.1, 20.9] | 0.96 [0.61, 0.98] | |
| Hand abduction | 47.9 [41.8, 52.4] | 0.83 [0.62, 0.88] | |
| Pelvis-thorax flexion | 19.5 [15.0, 22.7] | 0.93 [0.86, 0.97] | |
| P-t lateral bending | 6.0 [5.1, 7.7] | 0.99 [0.98, 0.99] | |
| P-t rotation | 2.3 [ | 18.7 [16.9, 19.4] | 0.95 [0.92, 0.96] |
| Hip flexion | 6.8 [6.1, 8.3] | 1.0 [1.0, 1.0] | |
| Hip abduction | 5.8 [3.9, 7.1] | 1.0 [0.99, 1.0] | |
| Knee flexion | 3.5 [2.5, 5.3] | 1.0 [1.0, 1.0] | |
| Ankle flexion | 8.2 [ | 9.9 [6.5, 16.4] | 1.0 [1.0, 1.0] |
| Ankle inversion | 23.8 [19.6, 28.9] | 0.97 [0.93, 0.98] |
Figure 1.
Point plot of median mean absolute error (MAE) of the arm joints including the 95% CI.
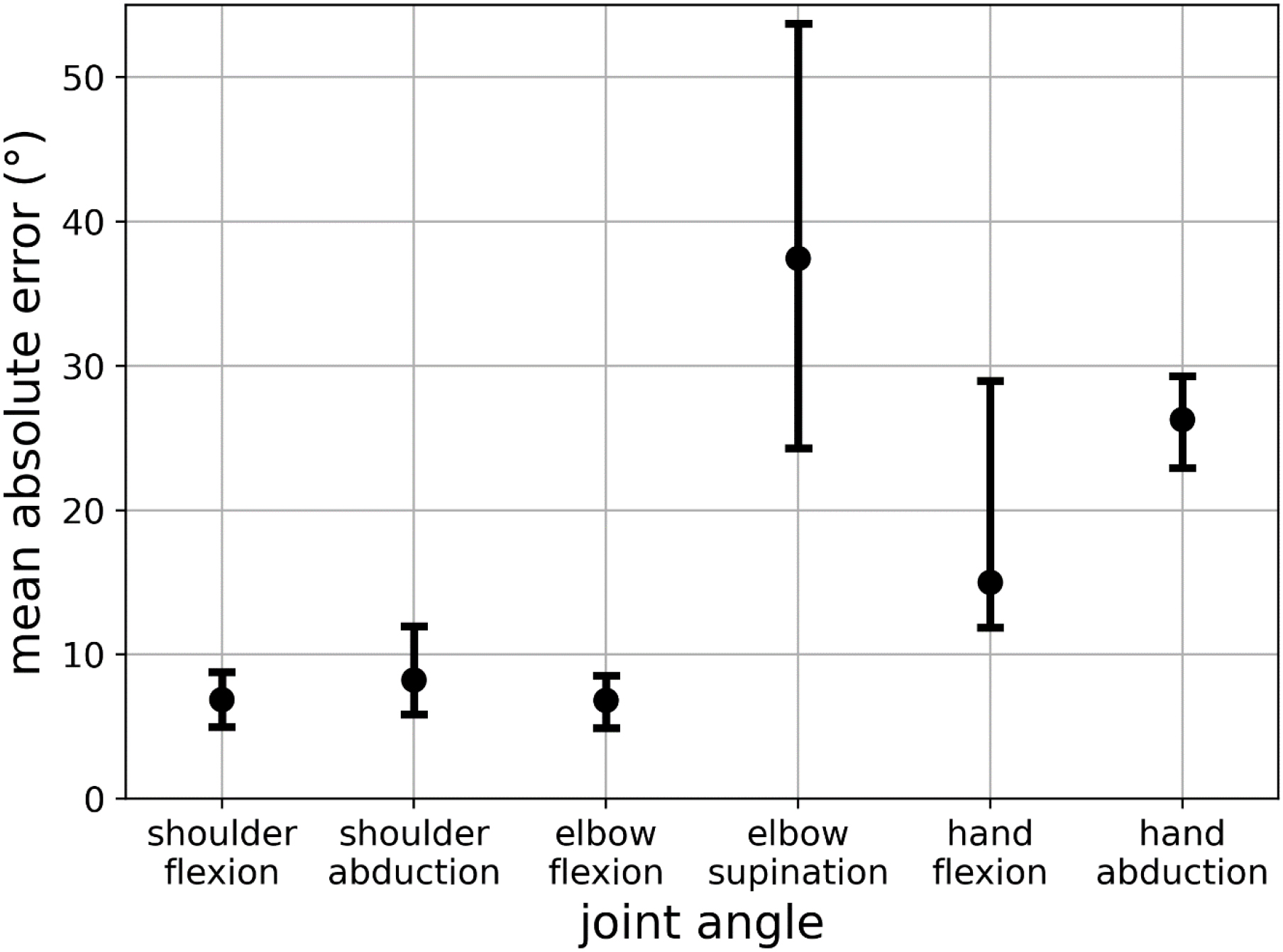
Figure 2.
Point plot of median mean absolute error (MAE) of the head and pelvis thorax joints including the 95% CI.
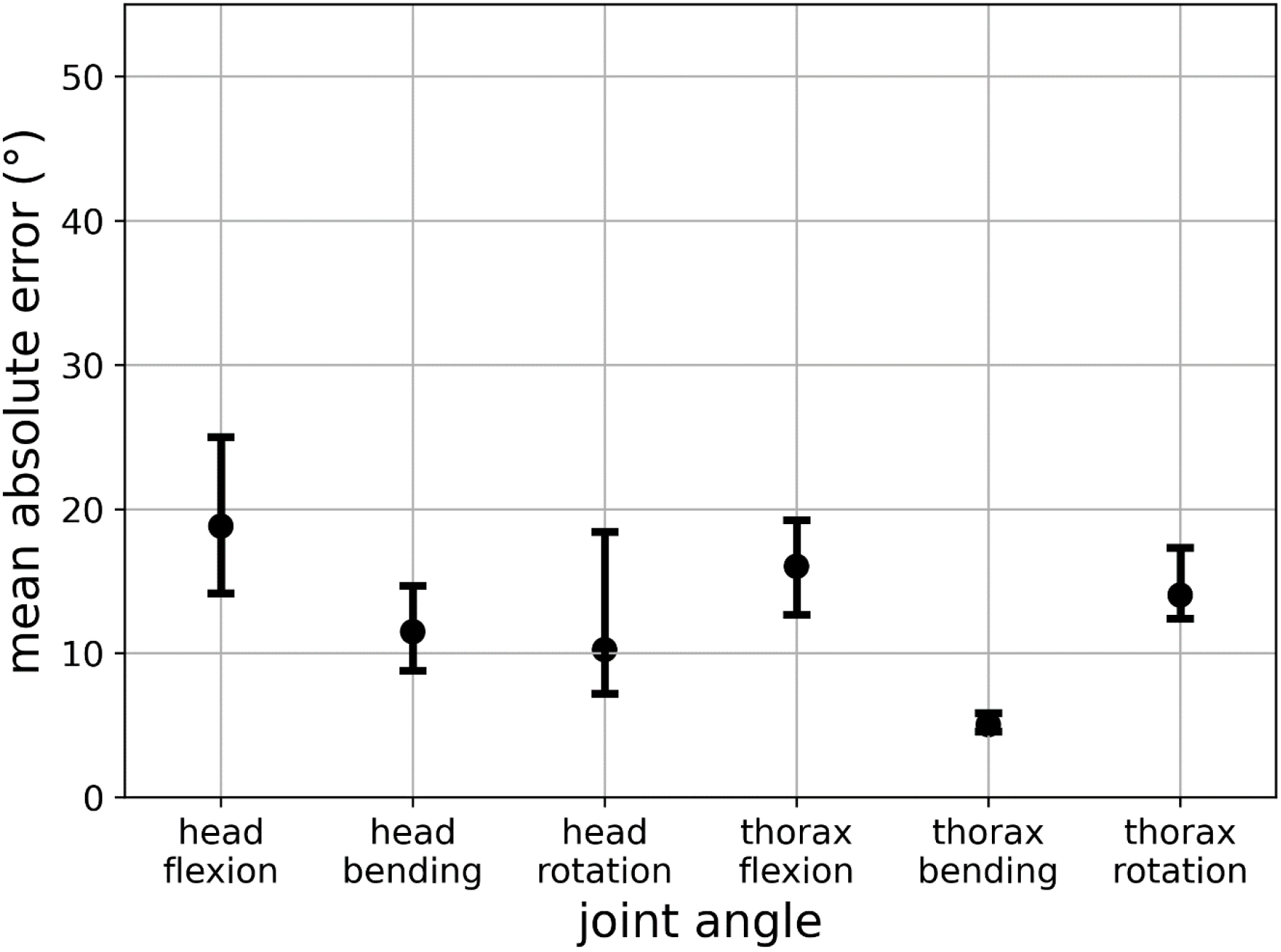
In the head and thorax joints, the MAE was lowest for lateral bending of the thorax at 5.1∘ (6.0%) and highest for head flexion at 18.9∘ (13.0%) (Fig. 2). r ranged from 0.93 for pelvis-thorax flexion up to 1.0 for head rotation and lateral bending. The bias was lowest for the lateral bending of the head and thorax with
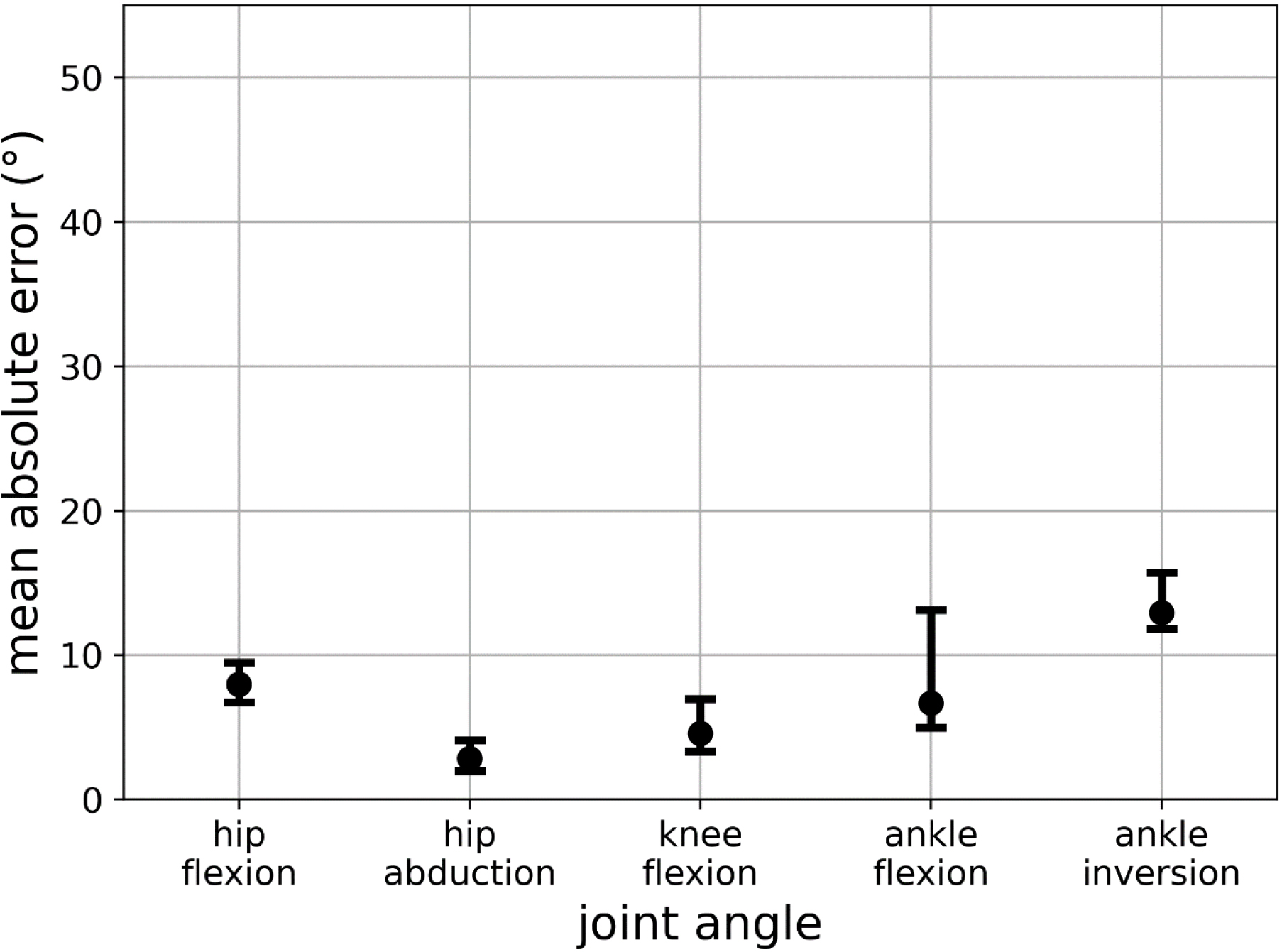
The lower extremity showed the lowest MAE for hip abduction with 2.9∘ (5.8%) and the highest for ankle inversion with 12.9∘ (23.8%) (Fig. 3). Correlation was excellent for all joints with r
Figure 3.
Point plot of median mean absolute error (MAE) of the leg joints including the 95% CI.
4.Discussion
This work aimed to compare MMC and a commercial VMC system when used as kinematic input for musculoskeletal models and the joint angles calculated in those models. The evaluation showed overall low deviations of VMC joint angles for shoulder, hip and knee joints as well as for elbow and ankle flexion. The joint kinematics’ errors of head and thorax were higher than those of the extremities although the highest errors were found in elbow pronation and hand abduction.
The deviations from CapturyLive to MMC are within the range of other VMC systems compared to MMC. Kanko et al. [4] evaluated the gait kinematics of Theia3D versus a Qualysis MMC setup. They determined deviations for hip flexion of (11∘), lower values for ankle inversion (8∘) and similar errors for hip abduction (2.6∘), knee flexion (3.3∘) and ankle flexion (6.7∘). Although one must mention that they determined an RMSE instead of the MAE and these two metrics are not entirely the same. However, they both give an estimation of accuracy, but MAE is more stable to outliers. Van Hooren et al. [6] also determined the RMSE for treadmill gait with a VMC setup. Although they only used one video camera with DeepLabCut and OpenPose they determined only slightly higher or similar errors for hip flexion (9.1∘/6.9∘), knee flexion (11.5∘/9.2∘) and ankle flexion (7.3∘/5.6∘). With OpenCap [10], an overall MAE for lower limb kinematics during various activities of 4.5∘ was determined, which is lower than the reported values of this study. However, they also reported higher deviations from MMC in pelvis-thorax flexion or hip abduction compared to other DOF. Needham et al. [9] used nine machine vision cameras, OpenPose and OpenSim to determine lower body kinematics for gait, running and jumping. The mean bias of their Bland-Altman analysis was slightly lower than the values determined in this study. They found a mean bias for hip flexion of
The variations in MAE and MAEROM show that not all joints are tracked equally by the VMC system. Especially the hand flexion/abduction and elbow flexion yield a high deviation from the gold standard. The hand flexion movements were sometimes tracked very well with a low error but most of the time, the tracking resulted in an overall high deviation. This is probably caused by a combination of a relatively low resolution of 1 px/cm, where 2 px/cm would be recommended by the software and lighting conditions for finger/hand tracking. These circumstances arise from the fact that the measurement setup was set up for a whole-body recording, as would be the case in a general study. They may also play a role in the high errors in hand abduction and elbow pronation. However, for these movements, the VMC system did not track any movements at all or only in one direction for most of the trials. The large error for the elbow pronation can be explained by deficiencies in hand tracking since visually, the elbow pronation can mainly only be tracked by the movement of the palm. In combination with a large ROM, this leads to high MAE values. Despite the insufficient tracking of these joints, the shoulder joint as well as the elbow flexion was tracked quite well with the MAEROM below 8% despite a large ROM (
The relatively high deviations in the head joint can be explained by the headband worn for the head markers of the MMC system. This headband was worn differently by all subjects to fit conveniently leading to a marker offset in the AMS. Since the actual offset could not be determined objectively for all subjects and trials, no correction was done to uphold data integrity. Nonetheless, the high r values of these joints (r
For the pelvis-thorax flexion and rotation and the ankle inversion, in the VMC system, some transfer of motion to the hip joint could be determined, leading to larger MAE and MAEROM values. For the flexion/rotation of the thorax, it was already noticeable in the visual inspection of the tracking that the virtual pelvis of the VMC system did move more than the real pelvis of the subject. Since the MMC setup has actual markers attached at the height of the anterior and posterior superior iliac spine, the pelvis movement could be tracked more accurately. By adding the hip flexion/rotation to the thorax flexion/rotation angle the overall deviation between VMC and MMC was considerably lower. In ankle inversion, a similar effect could be recognized. On the one hand, the VMC system tracked more whole-leg movement (
The remaining joints of the lower extremity, hip, knee and ankle flexion as well as hip abduction, were tracked by the VMC system with a low overall deviation and high correlation. Their MAE, MAEROM and bias were within the margin of error of MMC setups [16, 17]. Usually, the margin of error for an MMC setup’s joint angles is roughly
4.1Limitations
It must be noted that the experimental setup does not correspond to the actual application of a VMC system, since the subjects were not recorded in everyday clothing but lightly clothed and equipped with markers. Since the AI models of the VMC systems are usually trained on clothed subjects, though, this can lead to divergences. Nevertheless, this also means that the experiments conducted are more likely to correspond to a worst-case scenario and that improved tracking can be expected in regular experiments with normal clothing. Also, it should be noted that due the VMC accuracy might be influenced by different anthropometrics, which are not addressed in the present study. In addition, abstract motions were chosen for the comparison of VMC and MMC, which do not correspond to any usual motion sequences. Everyday movements are considerably more complex due to the interaction of several joints and can rarely be broken down to DOF. However, the choice of isolated movements has the advantage that the largest possible ROM can be achieved and the influence of individual DOFs of a joint can also be investigated allowing conclusions for more complex movements. We have tried to isolate these motions at much as possible, however for real single plane motions more constrained movements might be used. The use of musculoskeletal models introduces further imprecision into the evaluation, as these over-determined systems use optimization algorithms to calculate kinematics and kinetics and do not yield exact solutions. In addition, there is an adjustment of the kinematic input data to the musculoskeletal model due to the different DOFs in the joints of the subject, VMC/MMC, and the musculoskeletal model. This means that the results from the models cannot be directly transferred to the motion capture systems, so the results are only valid for an application with musculoskeletal models. Nevertheless, musculoskeletal models themselves have often been the subject of investigations in the past and future, so their use is now considered standard and valid [1, 26, 27], and combination of VMC and model will simplify the collection of biomechanical quantities.
4.2Outlook
These results suggest that VMC systems can be used for biomechanical analyses with musculoskeletal models, although not all applications are suitable. As of now hand motions or elbow pronation aren’t tracked sufficiently and VMC consequently can’t be used for such applications. Also, investigations regarding pelvis-thorax movements must take into consideration that pelvis movement cannot be depicted with VMC as it can be with MMC. Nonetheless, the low deviations with the margin of error of the MMC system in the lower extremities are a promising first step for whole-body musculoskeletal analysis with VMC input. VMC offers several advantages over MMC systems. An obvious advantage is the reduced preparation time for researchers and subjects. Even though VMC systems also require cameras to be installed and set up, their configuration is less complex and error-prone. In addition, subjects do not need to be specially prepared but can usually be measured as they come into the lab, leaving aside other measurement systems such as electromyography or the like. On the one hand, this reduces human errors such as the inaccurate sticking of markers, and on the other hand, it allows the subjects to perform the tests more comfortably and more familiarly since they are not additionally stuck with markers and can also wear clothing that is customary for the individual task. However, even though the accuracy of lower limb and shoulder joint angles is promising, there is still a long way to go for the widespread application of VMC input in musculoskeletal models. To make the combination of VMC input and musculoskeletal models broadly useful, the accuracy of the used VMC system should improve. The wrist and elbow pronation need considerable improvement in tracking. Hip positioning/rotation and the ankle will also require further attention. Considering the ever-advancing development of artificial intelligence and the associated increase in performance of such AI-based VMC systems, however, these challenges appear to be solvable. Hence, the results of this study provide an initial basis for further investigations in terms of methodology and target parameters.
5.Conclusion
This study examined the application of a commercial VMC system as a kinematic input for musculoskeletal models, comparing its performance to the gold standard MMC. The results showed generally small deviations in joint angles, especially for major joints in the upper and lower extremities. However, challenges were identified in accurately tracking hand and elbow movements, highlighting specific areas where improvements in VMC system accuracy are needed. The study highlights the promising potential of VMC systems for biomechanical analyses with musculoskeletal models, especially in the context of lower extremity joint tracking. Acknowledging the limitations and considering the experimental setup as a worst-case scenario, the results provide a foundation for future research and development in refining VMC technologies to enhance their accuracy and broaden their application in real-world biomechanical studies. The findings of the study contribute to advancing the field of motion capture and musculoskeletal modeling and provide valuable considerations for researchers and clinicians seeking to utilize innovative technologies in their analyses.
Funding
This work is part of a project sponsored by the German Federal Ministry of Education and Research under number 01|S21025B. Gold Open Access was enabled by the library of the OTH Regensburg.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/THC-240202.
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
TheCaptury provided the hard- and software as well as technical support for the recordings of the kinematic data. Nevertheless, TheCaptury was not involved in the processing and evaluation of the kinematic data.
References
[1] | Fluit R, Andersen MS, Kolk S, et al. Prediction of ground reaction forces and moments during various activities of daily living. J Biomech (2014) ; 47: : 2321-9. doi: 10.1016/j.jbiomech.2014.04.030. |
[2] | Colyer SL, Evans M, Cosker DP, et al. A review of the evolution of vision-based motion analysis and the integration of advanced computer vision methods towards developing a markerless system. Sports Med – Open (2018) ; 4: : 24. doi: 10.1186/s40798-018-0139-y. |
[3] | Moro M, Marchesi G, Hesse F, et al. Markerless vs. Marker-Based Gait Analysis: A Proof of Concept Study. Sensors; 22. doi: 10.3390/s22052011. Epub ahead of print 1 January 2022. doi: 10.3390/s22052011. |
[4] | Kanko RM, Laende EK, Davis EM, et al. Concurrent assessment of gait kinematics using marker-based and markerless motion capture. J Biomech (2021) ; 127: : 110665. doi: 10.1016/j.jbiomech.2021.110665. |
[5] | Seth A, Hicks JL, Uchida TK, et al. OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS Comput Biol (2018) ; 14: : 1006223. doi: 10.1371/journal.pcbi.1006223. |
[6] | Van Hooren B, Pecasse N, Meijer K, et al. The accuracy of markerless motion capture combined with computer vision techniques for measuring running kinematics. Scand J Med Sci Sports (2023) ; 33: : 966-978. doi: 10.1111/sms.14319. |
[7] | Mathis A, Mamidanna P, Cury KM, et al. DeepLabCut: Markerless pose estimation of user-defined body parts with deep learning. Nat Neurosci (2018) ; 21: : 1281-1289. doi: 10.1038/s41593-018-0209-y. |
[8] | Cao Z, Hidalgo G, Simon T, et al. OpenPose: Realtime Multi-Person 2D Pose Estimation using Part Affinity Fields. doi: 10.48550/ARXIV.1812.08008. Epub ahead of print 2018. doi: 10.48550/ARXIV.1812.08008. |
[9] | Needham L, Evans M, Wade L, et al. The development and evaluation of a fully automated markerless motion capture workflow. J Biomech (2022) ; 144: : 111338. doi: 10.1016/j.jbiomech.2022.111338. |
[10] | Uhlrich SD, Falisse A, Kidziński Ł, et al. OpenCap: Human movement dynamics from smartphone videos. PLOS Comput Biol (2023) ; 19: : e1011462. doi: 10.1371/journal.pcbi.1011462. |
[11] | Fleisig GS, Slowik JS, Wassom D, et al. Comparison of marker-less and marker-based motion capture for baseball pitching kinematics. Sports Biomech (2022) ; 1-10. doi: 10.1080/14763141.2022.2076608. |
[12] | Kanko RM, Laende EK, Strutzenberger G, et al. Assessment of spatiotemporal gait parameters using a deep learning algorithm-based markerless motion capture system. J Biomech (2021) ; 122: : 110414. doi: 10.1016/j.jbiomech.2021.110414. |
[13] | Ripic Z, Theodorakos I, Andersen MS, et al. Prediction of gait kinetics using Markerless-driven musculoskeletal modeling. J Biomech (2023) ; 157: : 111712. doi: 10.1016/j.jbiomech.2023.111712. |
[14] | Benoit DL, Ramsey DK, Lamontagne M, et al. Effect of skin movement artifact on knee kinematics during gait and cutting motions measured in vivo. Gait Posture (2006) ; 24: : 152-164. doi: 10.1016/j.gaitpost.2005.04.012. |
[15] | Kessler SE, Rainbow MJ, Lichtwark GA, et al. A Direct Comparison of Biplanar Videoradiography and Optical Motion Capture for Foot and Ankle Kinematics. Front Bioeng Biotechnol. 7. https://www.frontiersin.org/articles/10.3389/fbioe.2019.00199 (2019, accessed 24 July 2023). |
[16] | Miranda DL, Rainbow MJ, Crisco JJ, et al. Kinematic differences between optical motion capture and biplanar videoradiography during a jump-cut maneuver. J Biomech (2013) ; 46: : 567-573. doi: 10.1016/j.jbiomech.2012.09.023. |
[17] | Windolf M, Götzen N, Morlock M. Systematic accuracy and precision analysis of video motion capturing systems-exemplified on the Vicon-460 system. J Biomech (2008) ; 41: : 2776-80. doi: 10.1016/j.jbiomech.2008.06.024. |
[18] | Howard C, Kahnt A, Volberding JL, et al. Assessment of bilateral shoulder range of motion in firefighter trainees using a markerless motion capture system. Int J Athl Ther Train (2023) ; 28: : 263-268. doi: 10.1123/ijatt.2022-0039. |
[19] | Mündermann L, Corazza S, Andriacchi TP. The evolution of methods for the capture of human movement leading to markerless motion capture for biomechanical applications. J NeuroEngineering Rehabil (2006) ; 3: : 6. doi: 10.1186/1743-0003-3-6. |
[20] | Bottino A, Laurentini A. The visual hull of smooth curved objects. IEEE Trans Pattern Anal Mach Intell (2004) ; 26: : 1622-1632. doi: 10.1109/TPAMI.2004.130. |
[21] | Piccardi M. Background subtraction techniques: a review. In: 2004 IEEE International Conference on Systems, Man and Cybernetics (IEEE Cat. No.04CH37583). The Hague, Netherlands: IEEE. pp. 3099-3104. |
[22] | Stoll C, Hasler N, Gall J, et al. Fast articulated motion tracking using a sums of Gaussians body model. In: 2011 International Conference on Computer Vision. Barcelona, Spain: IEEE. pp. 951-958. |
[23] | Harsted S, Holsgaard-Larsen A, Hestbæk L, et al. Concurrent validity of lower extremity kinematics and jump characteristics captured in pre-school children by a markerless 3D motion capture system. Chiropr Man Ther (2019) ; 27: : 39. doi: 10.1186/s12998-019-0261-z. |
[24] | Lund ME, Andersen MS, de Zee M, et al. Scaling of musculoskeletal models from static and dynamic trials. Int Biomech (2015) ; 2: : 1-11. doi: 10.1080/23335432.2014.993706. |
[25] | Bland M, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. The Lancet (1986) ; 327: : 307-310. doi: 10.1016/S0140-6736(86)90837-8. |
[26] | Damsgaard M, Rasmussen J, Christensen ST, et al. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul Model Pract Theory (2006) ; 14: : 1100-1111. doi: 10.1016/j.simpat.2006.09.001. |
[27] | Skals S, Jung MK, Damsgaard M, et al. Prediction of ground reaction forces and moments during sports-related movements. Multibody Syst Dyn (2017) ; 39: : 175-195. doi: 10.1007/s11044-016-9537-4. |


