Definition of catheter jamming: A mechanical analysis of catheter fracture tension and fracture strain
Abstract
BACKGROUND:
Catheter jamming is an emerging and possibly underrated complication.
OBJECTIVE:
To find the criteria for determining if the catheter cannot be removed through the mechanical analysis of fracture tension and fracture strain (
METHOD:
We removed 30 pieces of PICC catheters from patients and recorded the indwelling time. Those with an indwelling time shorter than 12 weeks belonged to the short-term group. Those with an indwelling time longer than 12 weeks belonged to the long-term group. The first half of the same catheter is section A, and the second half is section B. The fraction tension and fracture strain of the catheter were measured, and statistical analysis was conducted.
RESULTS:
The fracture tension of catheter in sections A and B were 5.8917
CONCLUSION:
It is objective and consistent to take the catheter fracture tension as the standard. This standard would be able to accurately define the concept of catheter failure and reduce the risk of catheter fracture and the misdiagnosis of catheter failure. The catheter fracture tension and fracture strain was not affected by the catheter indwelling time. It is recommended to set the tensile force as 5 Newtons and carry it out at a speed of 100 mm/min for the catheter drawing of the PICC single-lumen silicone catheter (4.0F) from Budd Company.
1.Introduction
In 2005, Thein [1] reported the first case of hemodialysis catheter jamming, complicated with central venous catheter (CVC) fracture and residual indwelling in the vascular lumen. Recently, catheter jamming, also known as indwelling, imbedded, or tethered, has been reported as one of the mechanical complications. Given that the catheter is closely attached to the vessel wall at one or more sections of the vessel, removal of the catheter using standard techniques is difficult or even impossible [2]. Catheter jamming is an emerging and possibly underrated complication in literature [3]. Wilson et al. [4] found that 200 children had vascular access catheters made from polyurethane removed, and about 16 percent of cases experienced difficulty in surgical removal. The 2016 edition of intravenous therapy guidelines [5] states that “the catheter cannot be forcibly removed in the presence of resistance during the catheter removal process. Removing by force may result in catheter damage and even air embolism.” In the case of catheter removal by pulling, the concept of “forceful removal” is subjective. Too much pulling force leads to catheter fracture, and too little pulling force leads to pseudo-stalling of the catheter. Most previous studies on catheter jamming [1, 2, 3, 4, 5] are about central venous infusion devices, such as hemodialysis catheters, central venous catheters, and infusion ports. There have been few reports on Peripheral Inserted Central Catheters (PICC) jamming. In the 512 cases of PICC catheter drawing conducted by the authors from November 2015 to August 2020, three cases of catheter jamming occurred. In two cases, the catheter was pulled out forcibly after the catheter jamming. The catheter could not be removed in another patient after the catheter jamming, so a surgical incision was made to remove the catheter.
Current problem: How much tension is appropriate in a PICC catheter drawing operation? What are the objective criteria for determining catheter jamming?
We put forward the following hypothesis to solve the above problems: The PICC catheter fracture tension is taken as the upper limit of catheter drawing force. Catheter jamming refers to a failure to draw out the catheter when the catheter is pulled at a force close to the catheter’s fracture tension.
2.Materials and methods
2.1Experiment materials
The PICC silicone catheter was removed from the patient (single-lumen PICC 4.0F [1.40 mm OD]
Table 1
Statistical analysis of short- and long-term groups
| Group | Numbers | Average value | Mean | Sig | |
|---|---|---|---|---|---|
| Short-term group | 12 | 8.25 | 3.019 | 10.386 | 0.003 |
| Long-term group | 18 | 26.17 | 9.642 |
The PICC catheter is usually placed 35–45 cm in vivo and 5–6 cm in vitro. The in vivo part of the catheter was been selected as experimental material and was divided into two parts. The tip of the catheter is segment A and the rest is segment B. Mechanical test instrument: LLOYD (USA), model: EZ50, maximum speed: 100 mm/min.
2.2Methods
After placing the sample on the mechanical test machine, the following steps were sequentially proceeded. Supplementary Fig. 1 shows sections A and B. Complementarily, a picture describing the mechanical test is shown in Supplementary Fig. 2.
Step 1: pre-stretching the sample before the experiment. Applying tension to the sample at the loading speed of 10 mm/min make the sample stretch 10 times within the range of 2% of the initial length, and then unload and pause 5 min.
Step 2: stretching until the catheter is fractured according to the set stretching speed. Tension test velocity: section A 100 mm/min, section B 50 mm/min.
Step 3: save and analyze the data, including the initial length of the sample (marked on the catheter), the tension and length of the catheter when it fractures.
The experimental equipment and measurement data were completed by the Biomechanics Laboratory, School of Biomedical Engineering, Capital Medical University, China.
The tension at fracture was measured at each section and the fracture strain at fracture
3.Statistical results
3.1Statistical results of the paired t-test for section A and section B (Table 2)
Table 2
Statistical results of the paired
| Mean | Sig | |||
|---|---|---|---|---|
| Fracture tension of catheter (newtons) | Section A | 5.8917 | 0.393 | |
| Section B | 6.0670 | |||
| Fracture strain of catheter | Section A | 6.0611 | 0.343 | |
| Section B | 6.2543 |
Results analysis: Fracture tension of catheter: section A: 5.8917
3.2Statistical results of single sample t
Table 3
Statistical results of single sample
| Group | Case | Mean | Sig | ||
|---|---|---|---|---|---|
| Fracture tension of catheter (newtons) | Short-term group | 24 | 6.0696 | 0.624 | 0.535 |
| Long-term group | 36 | 5.9192 | |||
| Fracture strain of catheter | Short-term group | 24 | 6.0067 | 0.301 | |
| Long-term group | 36 | 6.2584 |
Results analysis: Fracture tension of catheter: short-term group: 6.0696
3.3Statistical description of fracture tension of all samples and 99.99% confidence interval (Table 4)
Table 4
Statistical description of fracture tension of all samples and 99.99% confidence interval
| Cases | Mean | 99.99% confidence interval | Max | Mix | |
| Lower limit | Upper limit | ||||
| 30 | 5.8917 | 5.0613 | 6.7221 | 7.94 | 3.61 |
Results analysis: The lower limit of 99.99% confidence interval of fracture tension of all samples is 5.0613 Newtons.
4.Discussion
Previous studies on the concept of catheter jamming seem to be consistent. However, these studies are unclear. Giacomo [2] held that due to the tight attachment of the catheter to the vessel wall, it is difficult or even impossible to remove the catheter using standard techniques. This is called catheter jamming. Lodi [3] believed that catheter jamming is a condition in which the catheter cannot be removed after the indwelling sleeve is removed. Ryan [6] defined catheter jamming as a catheter that cannot be removed after stripping and releasing the retaining cuff. These definitions define the concept of catheter jamming with the result of catheter drawing (the catheter cannot be removed) as the standard. Nonetheless, in practice, the operator determines whether the catheter can be effectively pulled out by maintaining the appropriate tension and speed. If the operator applies too much force, the catheter will rupture, requiring a further process to remove the catheter. If the operator is worried about the catheter fracture and applies too little tension, the catheter that could have been pulled out is wrongly classified as catheter jamming because of insufficient tension. Consequently, operators still need to go into the catheter room for catheter drawing. The process is complex, and the cost increases.
A PICC catheter is a 1.40 mm (4.0F) diameter catheter inserted through a peripheral vein. PICC catheters are finer than hemodialysis catheters, central venous catheters, infusion ports, and other central venous infusion devices. When the catheter drawing resistance is high, the patient would be more susceptible to the complications of catheter fracture or catheter jamming. This study shows that it is objective and consistent to take the catheter fracture tension as the upper limit of pulling tension, ensuring that the catheter drawing force is large enough to avoid catheter fracture. Based on this, failure to remove a tugged catheter by this standard can be defined as catheter jamming. This method of definition contributes to reducing both the risk of catheter fracture and the misdiagnosis of catheter jamming as well.
Idowu’s study [7] demonstrated that the amount of tension that could be safely applied in a CVC procedure for removal of the catheter without tearing the vascular wall in a child was unclear. Mahadeva [8] held that slow and gentle traction (up to 36 hours) has some success. However, Mahadeva did not specify the speed or pull of the pull. The mechanical properties and tissue reactivity of catheters differ with different materials. Wilson et al. [4] found that silicone-type catheters can also adhere to vascular walls and silicone catheters are less reactive than polycarbamates. They do not readily adhere to fibrous sheaths or vascular walls even after prolonged placement in situ. Idowu [7] argued that silicone catheters are more elastic than polyurethane catheters and, due to their elasticity, are more likely to break than polyurethane catheters.
The results of this study showed that the fracture tension of the proximal and distal PICC catheters was the same, and catheters can be removed with slow and gentle continuous traction. In this research, the lower limit of the 95% range of PICC 4.0F (1.40 mm OD)
What requires special attention is that different manufacturers, different types of catheters, and different materials may have different fracture tension limits. These limits need to be obtained by mechanical tests. The catheter used in this study is considered a viscoelastic material. Thus, pre-stretching is required. Whether there is a limit for the speed of catheter drawing can be considered as the content of the next study.
According to Hassan [9], in case reports, catheter placement time was an important factor associated with catheter jamming. Liu [10] advised that CVC should be replaced every two years to prevent the catheter from jamming. Jones [11] showed that central IV devices staying in place for more than 20 months would be hard to remove. According to Andrew’s report [12], the mechanism by which the indwelling catheter adheres to the vessel wall is that after 90 days of prolonged indwelling, the venous wall in the endothelium injury is thickened and is closely bridged between the venous wall and the catheter. The mechanical properties of the catheter could change due to the long-term mechanical and chemical stimulation in vivo. A research carried out by Busch measured Young’s modulus (E), ultimate stress (
The novelty of this study is as follows: 1. the design and results of the study are closer to the clinic practice because of the use of catheters retained in vivo for a long time, 2. The subjective operation is investigated and assessed through a more objective criteria of the physical characteristics of the catheter, 3. Using an objective, simple and clear criteria define the seemingly subjective and vague clinical concepts. The difficulty of catheter pullout: it still cannot be pulled out at the maximum fracture force of the catheter.
The results of this study showed that the catheter fracture tension and fracture strain of the catheter was unrelated to the indwelling time of the catheter in vivo. There was no change in fracture tension and fracture strain for catheters up to and longer than 12 weeks. This means that, in catheter drawing, there is no need to consider the effect of the indwelling time on the fracture tension of the catheter. Hence, the operation can be carried out according to the uniform fracture tension standard.
Clinical significance of catheter fracture strain
The distance of catheter loosening can be judged by the fracture strain during catheter pulling operations, which provides a basis for the next operation. Specific operations: Marking points were selected in the outer part of the catheter before drawing. The distance from the marked point to the puncture point was measured as a. In cases of continuous tension (5 Newtons) and slow traction (100 mm/min), a stable state was reached without tension. The distance between the mark point and the puncture point was measured again as b. Length of catheter loosening in vivo
The sample size in this study is insufficient. Thus, it is necessary to increase the sample size for further research to enhance the persuasiveness. A brand of a type of catheter in this experiment was measured, showing a lack of universal significance. The mechanical data of other catheters need to be measured further.
5.Conclusion
It is objective and consistent to take the catheter fracture tension as the standard. This standard would be able to accurately define the concept of catheter failure and reduce the risk of catheter fracture and the misdiagnosis of catheter failure. The catheter fracture tension and fracture strain were not affected by catheter indwelling time. It is recommended to set the tensile force as 5 Newtons and carry it out at a speed of 100 mm/min for the catheter drawing of the PICC silicone catheter (4F size) from Budd Company.
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.
Funding
This work was supported by the Scientific research project of Beijing Shijingshan Hospital (sjsky-201814). The funding agency had no role in the study design, collection, analysis and interpretation of data, writing of the report, or decision to submit the article for publication.
References
[1] | Thein H, Ratanjee SK. Tethered hemodialysis catheter with retained portions in central vein and right atrium on attempted removal. Am J Kidney Dis. (2005) Sep; 46: (3): e35-9. |
[2] | Forneris G, Savio D, Quaretti P, Fiorina I, Cecere P, Pozzato M, Trogolo M, Roccatello D. Dealing with stuck hemodialysis catheter: state of the art and tips for the nephrologist. J Nephrol. (2014) Dec; 27: (6): 619-25. |
[3] | Lodi M, Ebrahimi RF, Pezzotti P, Carbonari L. The removal of a stuck catheter: An alternative to Hong’s technique. J Vasc Access. (2016) Nov 2; 17: (6): 548-551. |
[4] | Wilson GJ, van Noesel MM, Hop WC, van de Ven C. The catheter is stuck: complications experienced during removal of a totally implantable venous access device. A single-center study in 200 children. J Pediatr Surg. (2006) Oct; 41: (10): 1694-8. |
[5] | Gorski LA. The 2016 infusion therapy standards of practice. Home Healthc Now. (2017) Jan; 35: (1): 10-18. |
[6] | Ryan SE, Hadziomerovic A, Aquino J, Cunningham I, O’Kelly K, Rasuli P. Endoluminal dilation technique to remove “stuck” tunneled hemodialysis catheters. J Vasc Interv Radiol. (2012) Aug; 23: (8): 1089-93. |
[7] | Idowu O, Brown J, Kim S, Kim S. Mechanics of a stuck central venous catheter removal. J Pediatr Surg. (2016) May; 51: (5): 872-5. |
[8] | Mahadeva S, Cohen A, Bellamy M. The stuck central venous catheter: beware of potential hazards. Br J Anaesth. (2002) Oct; 89: (4): 650-2. |
[9] | Hassan A, Khalifa M, Al-Akraa M, Lord R, Davenport A. Six cases of retained central venous haemodialysis access catheters. Nephrol Dial Transplant. (2006) Jul; 21: (7): 2005-8. |
[10] | Liu T, Hanna N, Summers D. Retained central venous haemodialysis access catheters. Nephrol Dial Transplant. (2007) Mar; 22: (3): 960-1; author reply 961. |
[11] | Jones SA, Giacomantonio M. A complication associated with central line removal in the pediatric population: retained fixed catheter fragments. J Pediatr Surg. |
[12] | Forauer AR, Theoharis C. Histologic changes in the human vein wall adjacent to indwelling central venous catheters. J Vasc Interv Radiol. (2003) Sep; 14: (9 Pt 1): 1163-8. |
[13] | Busch JD, Schröder H, Sellenschloh K, Adam G, Ittrich H, Huber G. Test method for mechanical properties of implantable catheters according to DIN 10555-3. Journal of the mechanical behavior of biomedical materials. (2018) ; 82. |
Appendices
Supplementary
Supplementary Fig. 1.
Sections A and B.

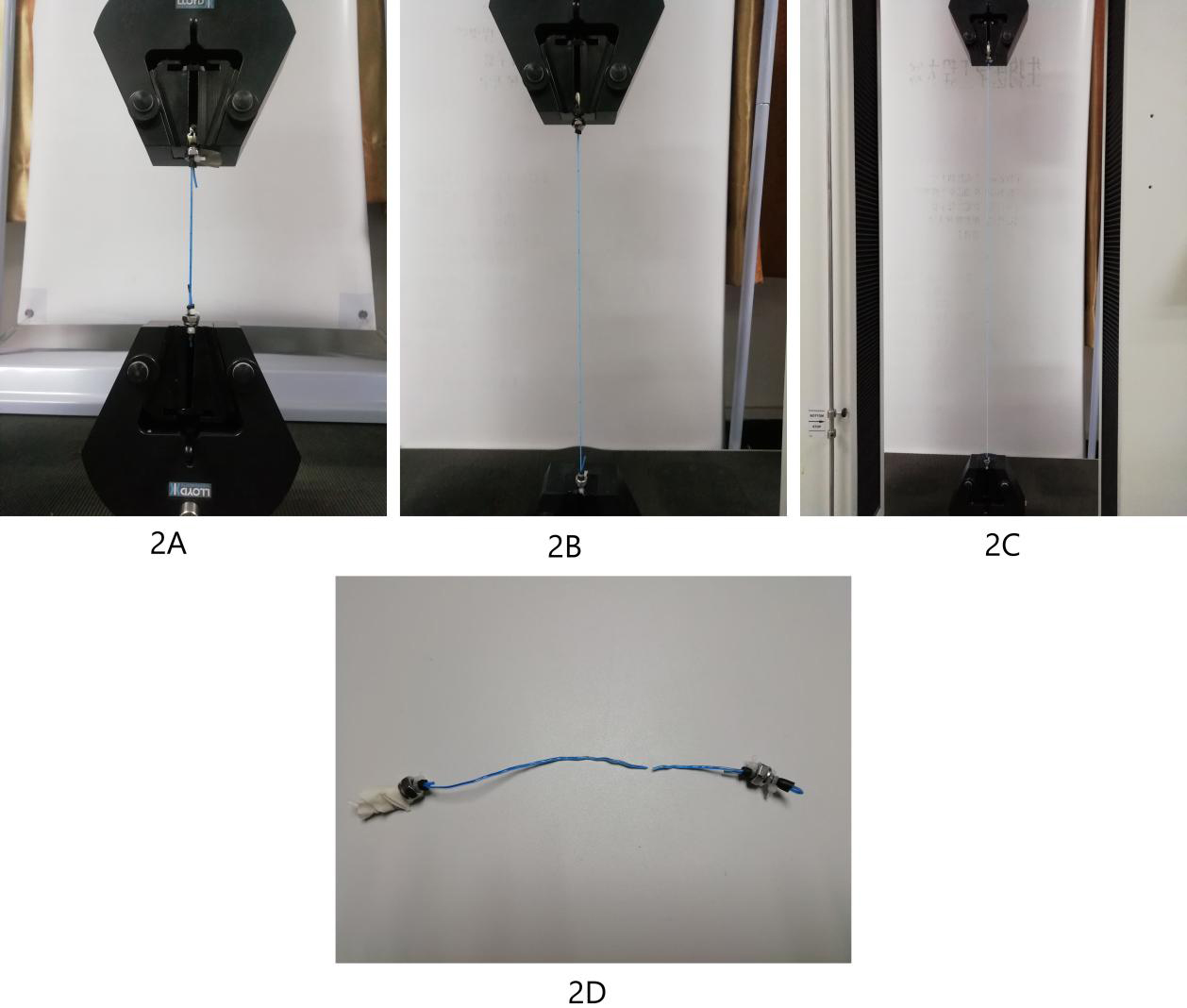
Supplementary Fig. 2.
Mechanical test process. 2A: Conduit ready for stretching; 2B: Conduit stretching in progress; 2C: Conduit tension near limit state; 2D: Status after conduit fracture.