
Evaluation of civil registration and vital statistics system in the Maldives: Focus on mortality statistics
Abstract
An efficient Civil Registration and Vital Statistics (CRVS) system is a development imperative. Data on death registration and causes of death are important for measuring health outcomes. This paper evaluates the completeness and quality of data on death registration and causes of death (CoD) based on analysis of the registration records on death and causes of death for the period 2009–2018.
Using established methods and approaches, we observed that CRVS system performed well on death registration completeness, quality of age and sex reporting. However, the quality of cause of death data was poor with 50% of the International Classification of Diseases (ICD) codes classified as “major garbage codes” and significant time lag was observed in the transmission and production of vital statistics.
The CRVS system in Maldives is complete with all deaths occurring within its territory registered and causes of death recorded. The two areas that require attention are the time taken for publication of vital statistics and quality of cause of death reporting. Appropriate re-engineering of the existing business process can build real-time mortality data, and regular quality assessment of death certificates with feedback to health facilities can bring sustained improvements in quality of vital statistics.
1.Introduction
Civil registration and vital statistics (CRVS) systems play an important role in generating data for good governance, measuring health outcomes and monitoring progress of sustainable development goals (SDGs). However, most low- and middle-income countries still have underdeveloped CRVS systems [1]. With a population of around 350 thousand spread across 187 islands [2] efficient implementation of a CRVS system in the Maldives poses a big challenge in terms of timely exchange of information and real-time analysis [3].
The CRVS system in the Maldives was introduced more than 50 years ago. As early as in 1960s, births and deaths were being reported to the Ministry of Health (MoH) through a registration system. This system was not properly enforced until the birth and death registration law was enacted in 1992 [4]. The new law mandated that a burial be permitted only after the death is compulsorily reported and cause(s) of death medically certified by a doctor or medical practitioner. This quickly and drastically improved death registration levels and cause of death reporting in the Maldives.
From 2003 onwards, a triplicate-copy system of reporting births and deaths through the birth form and the death certificate has been operational: the original copy is given to the parent or guardian in case of birth and the next of kin in case of deaths; the second copy is provided to the island administration; and the third copy is transmitted to the Department for National Registration (DNR), which inputs the data in the CRVS database. These forms are then coded in the CVRS database by the MoH [3].
This paper aims to evaluate the completeness and quality of data on death registration and cause(s) of death collected as part of the CRVS system. The CRVS is the single most important source of information on the aforesaid topics. The number of deaths and cause(s) of death as reported on the death certificate [5] are important to assess burden of diseases, the completeness and quality of vital statistics (VS) data [6]. The evaluation is mainly based on analysis of data obtained from the registration records on death and causes of death for the period 2009–2018.
2.Review of literature
Timely, quality, reliable and usable mortality data, trends and causes of death information are important to public health policies and interventions [7, 8]. Information on mortality in the Maldives is presented as the key mortality statistics in annual health statistics reports [9]. As of today, there is no published assessment or study on the CRVS of Maldives, although global estimates [10] show that the quality of VS with regard to completeness and recording of cause(s) of death is low in the Maldives.
Phillips and colleagues, developed in 2014 a procedure to combine six dimensions of VS in a composite Vital Statistics Performance Index (VSPI) [11]. ANACODA [12, 13] uses an adapted version of VSPI with 5 dimensions to assess the quality of death data as a matrix index (VSPI(Q)). The VSPI(Q) does not include data availability/timeliness dimension of the VSPI. The VSPI(Q) as an overall summary index of the quality of the mortality input data, combines the following five components of data quality into one measure [13]: (a) completeness of death registration, (b) amount and type of ‘garbage’ codes used to record the cause of death, including any non-ICD codes, (c) the degree of cause-specific detail included in the input data, (d) the frequency of biologically implausible causes of death in the dataset and (e) the fraction of deaths for which neither age nor sex was recorded.
Due to the complexity and level of engagement by different institutions in the CRVS system, mapping of the vital registration process is useful to capture and identify the bottlenecks, time lags and areas where efficiencies are needed [14]. This in return can improve measurement of health outcomes through targeted investments for process efficiency. However, it must be noted that most of the CRVS systems around the world lacks the long-term public policy investments [15]. Thus, advocates are imperative to improve the CRVS system and work towards a greater political commitment for establishing effective processes and improving of systems [16].
3.Methodology
This study explores data on all the registered deaths from 2009 to 2018 in the CRVS system of the Maldives.
3.1Evaluating the Maldives CRVS system
For analytical purposes, we used two datasets: the population estimates of the Maldives obtained from the Global Burden of Diseases (GBD) Group [10]; and International Classification of Diseases (ICD) version 10 (ICD-10) coded death data obtained from the CRVS system for ten years from 2009 to 2018. In the Maldives, death registration and causes of death are recorded in one single document – the death certificate. This document also includes socio-demographic information of the deceased (e.g., age and sex) and the cause of death certified by a doctor. The MoH uses this information to determine the underlying Causes of Death (CoD) and code them using ICD-10 codes [17].
Ethical approval was obtained from the National Health Research Council in the Maldives to use the CRVS data for this study.
3.2ANACONDA
For analysing the quality of mortality and causes of death data, the Analyses of Causes of National Death for Action (ANACONDA) [18], developed by the Bloomberg Philanthropies Data for Health innovation program is applied. ANACONDA is a software application that assesses the accuracy and completeness of mortality, and cause of death data. It computes the vital statistics performance index (VSPI(Q)) which is a composite measure of the five dimensions of VS strength (a detailed discussion on ANACONDA and VSPI(Q) is available from Mikkelsen and colleagues) [12].
For the purpose of the study, VSPI(Q) and the separate scores for the five components were computed for five two-years periods, with the objective to analyse the progress of completeness and quality over this ten-year period.
Table 1
VSPI(Q) and its component scores, 2009–2018
| Particulars | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 |
|---|---|---|---|---|---|
| Vital Statistical Performance Index (VSPI(Q)) | 51.4 | 56.7 | 55.8 | 51.2 | 50.9 |
| Quality of age and sex reporting | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| Quality of cause of death reporting | 58.7 | 63.1 | 63.8 | 58.7 | 63.8 |
| Biologically plausible cause of death | 100.0 | 100 | 100 | 99.1 | 100.0 |
| Level of cause specific detail available | 81.5 | 81.5 | 81.0 | 79.4 | 82 |
| Completeness of death reporting | 95.4 | 97.5 | 97.2 | 97.9 | 97.2 |
Note: Generated from ANACONDA. Source: Authors estimate.
Table 2
Major GBD groups and garbage codes, 2009–2018
| Groups | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 |
| Total Usable Codes | 37.8 | 42.1 | 42.4 | 37.3 | 43.7 |
| Group 1: Communicable diseases | 6.7 | 5.3 | 3.7 | 4.5 | 4.8 |
| Group 2: Non-communicable diseases | 27.8 | 33.2 | 34.4 | 29.0 | 35.7 |
| Group 3: External causes | 3.3 | 3.6 | 4.3 | 3.8 | 3.2 |
| Garbage codes (including insufficiently specified causes with limited | 62.2 | 57.9 | 57.6 | 62.7 | 56.3 |
| impact and insufficiently specified causes) | |||||
| Very high | 26.9 | 36.0 | 34.1 | 32.4 | 28.0 |
| High | 24.4 | 9.3 | 8.4 | 15.7 | 13.1 |
| Medium | 4.2 | 3.1 | 3.2 | 5.5 | 6.4 |
| Low | 6.7 | 9.5 | 11.9 | 9.1 | 8.8 |
| Total causes | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
Note: Generated from ANACONDA. Source: Authors estimate.
3.3Business process mapping (BPM)
To understand the CRVS system of the Maldives, we mapped the system using BPM (see Fig. 1). The mapping used the ten CRVS milestone approach, described by Cubos and colleagues [19] that help understand the performance issues regarding the timeliness of death registration; processes; and time-lags at each step starting from the onset of a death to its certification, registration, coding, data analysis and dissemination of statistics. This BPM was shared and validated through different stakeholder consultations with MoH and DNR, both at national and field level.
4.Results
4.1ANACONDA results
The VSPI(Q) showed no improvement from 2009 to 2018, beyond some marginal improvements in the intervening periods. For example, there was an improvement of VSPI(Q) in 2011 to 2014 compared to 2009–2010 which again declined in the recent years.
4.2Completeness of death reporting and quality of age and sex reporting
As shown in Table 1, the ‘Completeness of death reporting’ scores were consistently high for the entire 10-year period with small fluctuations. The ‘Quality of age and sex reporting’ scored 100 for the entire period.
4.3Quality of cause of death reporting
Over the period 2009–2018 the scores of ‘Qualities of cause of death reporting’ varied between 58 and 63 with a decline (58.7) during the period 2015–2016. ‘Biologically plausible cause of death’, scored 100 over the period 2009–2018 except for the years 2015–2016.
The usable codes (codes falling into category 1, 2 or 3 in Table 2) increased over the period from 37.3% in 2009–2010 to 42.4% in 2013–2014 to 43.5% in 2017–2018. The low quality of CoD reporting is attributed to the high proportion of ‘garbage codes’. Only a small reduction is seen in the extent of garbage codes in CoD during the period 2011–2014 but it increased again over the most recent periods (Table 2). Furthermore, garbage codes of “very high severity (level 1)” increased from 43.3% in 2009–2010 to 49.8% in 2017–2018. The garbage codes were more common in the age group of 70
Table 3
Top 10 causes of death in the Maldives, 2009–2010 and 2017–2018
| # | % of cause | ICD codes | Name of category | # | % of cause | ICD codes | Name of category |
| Leading ICD causes for Males 2017–2018 | Leading ICD causes for Females 2017–2018 | ||||||
| 1 | 8.8 | I46.9 | Cardiac arrest, unspecified | 1 | 9.0 | I46.9 | Cardiac arrest, unspecified |
| 2 | 6.6 | R99.- | Other ill-defined and unspecified causes of mortality | 2 | 6.4 | J44.9 | Chronic obstructive pulmonary disease, unspecified |
| 3 | 5.7 | I21.9 | Acute myocardial infarction, unspecified | 3 | 5.7 | R99.- | Other ill-defined and unspecified causes of mortality |
| 4 | 5.3 | R09.2 | Respiratory arrest | 4 | 5 | R09.2 | Respiratory arrest |
| 5 | 3.9 | I64.- | Stroke, not specified as hemorrhage or infarction | 5 | 4.5 | I10.- | Essential (primary) hypertension |
| 6 | 3.7 | I10.- | Essential (primary) hypertension | 6 | 3.8 | I21.9 | Acute myocardial infarction, unspecified |
| 7 | 3.2 | A41.9 | Septicemia, unspecified | 7 | 3.2 | A41.9 | Septicemia, unspecified |
| 8 | 2.8 | J44.9 | Chronic obstructive pulmonary disease, unspecified | 8 | 2.2 | I64.- | Stroke, not specified as hemorrhage or infarction |
| 9 | 2.2 | I25.9 | Chronic ischemic heart disease, unspecified | 9 | 2.1 | J18.9 | Pneumonia, unspecified |
| 10 | 1.9 | I25.1 | Atherosclerotic heart disease | 10 | 1.7 | I25.1 | Atherosclerotic heart disease |
| Leading ICD causes for Males 2009–2010 | Leading ICD causes for Females 2009–2010 | ||||||
| 1 | 18.1 | I10.- | Essential (primary) hypertension | 1 | 15.9 | I10.- | Essential (primary) hypertension |
| 2 | 7.7 | R99.- | Other ill-defined and unspecified causes of mortality | 2 | 7.6 | P96.4 | Termination of pregnancy, fetus and newborn |
| 3 | 5.1 | I46.9 | Cardiac arrest, unspecified | 3 | 7.2 | R99.- | Other ill-defined and unspecified causes of mortality |
| 4 | 4.2 | P96.4 | Termination of pregnancy, fetus and newborn | 4 | 5.3 | I46.9 | Cardiac arrest, unspecified |
| 5 | 3.9 | I21.9 | Acute myocardial infarction, unspecified | 5 | 5.1 | J44.9 | Chronic obstructive pulmonary disease, unspecified |
| 6 | 2.5 | I64.- | Stroke, not specified as hemorrhage or infarction | 6 | 2.6 | P95.- | Fetal death of unspecified cause |
| 7 | 2.5 | J44.9 | Chronic obstructive pulmonary disease, unspecified | 7 | 2.3 | I64.- | Stroke, not specified as hemorrhage or infarction |
| 8 | 2 | P95.- | Fetal death of unspecified cause | 8 | 2.1 | R54.- | Senility |
| 9 | 1.8 | I25.9 | Chronic ischaemic heart disease, unspecified | 9 | 2 | P01.8 | Fetus and newborn affected by other maternal complications of pregnancy |
| 10 | 1.6 | A41.9 | Septicemia, unspecified | 10 | 1.3 | A41.9 | Septicemia, unspecified |
Note: Generated from ANACONDA. Source: Authors estimate.
4.4Level of cause specific details
The score on ‘Level of cause specific detail available’ mirrors the pattern of the ‘Quality of death reporting’ with a score of about 81, and a small drop in the period 2015–2016 to 79.4 (Table 1). The results show that the change in the top 10 leading causes of death over the ten-year period (2009–2018) is not significant; 6 (for males) and 7 (for females) out of the top 10 causes belong to the garbage (including insufficiently specified) category. The majority of the codes belong to group 2 according to GBD (Table 3).
In conclusion, the quality of death information beyond some minor fluctuations, has not improved over the past 10 years, making the data unusable for policy and programming purposes. Further, the ANACONDA results show that priority intervention areas for improving data quality were ‘Quality of cause of death reporting’ and the ‘Level of cause of specific details’ (Table 1)
Figure 1.
Business process map: Maldives CRVS system. Note: “
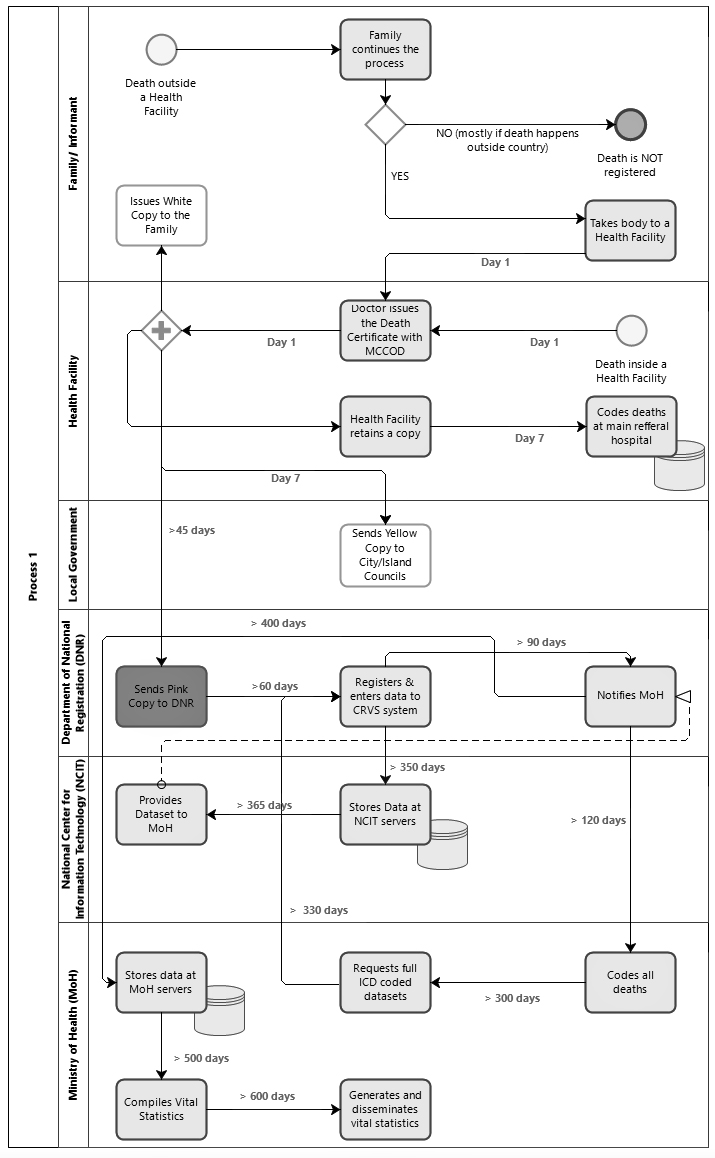
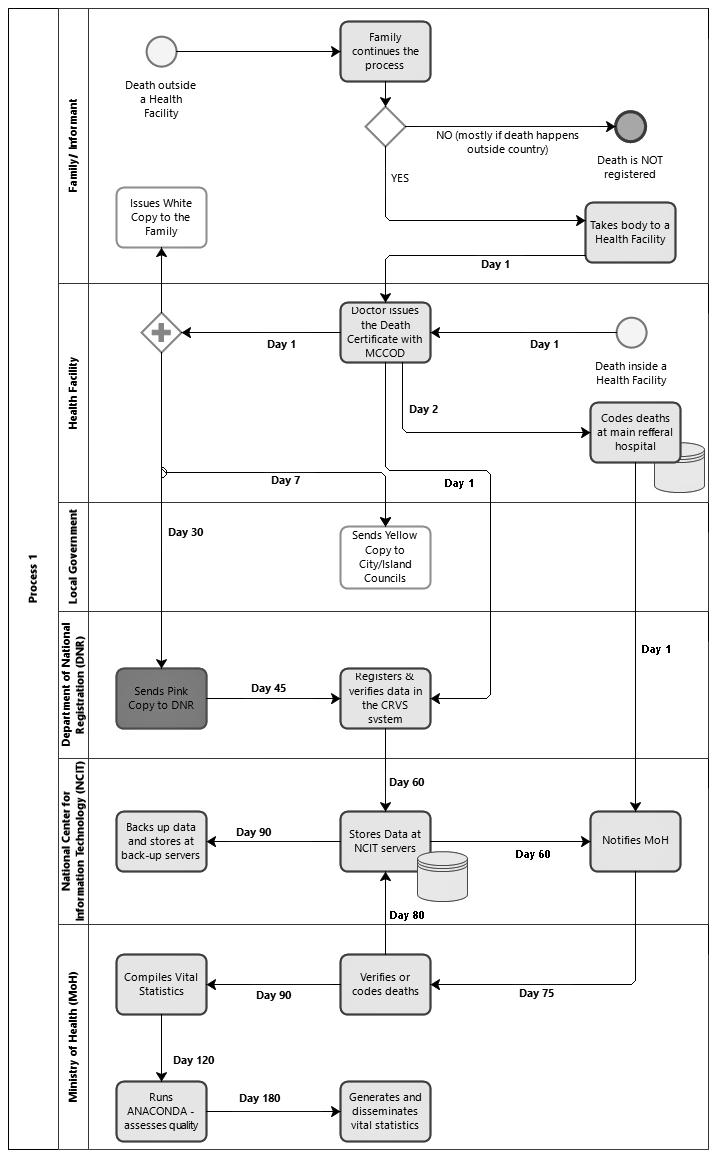
Figure 2.
Business process map: Maldives CRVS system with an online system. Note: Developed using Bizagi. Source: Authors findings.
4.5Garbage codes
Garbage codes refer to anything that is marked as a cause of death on a death certificate considered impossible be an underlying specific cause of death [20, 21]. The rate of garbage codes is an indicator of quality of causes of death: the higher the proportion of garbage codes the worse is the quality of the recording of causes of death. These are mainly attributed to poor and incomplete recording of causes of death by doctors and/or poor-quality coding of causes of death. Table 2 shows that although the proportion of garbage codes (including insufficiently specified causes) declined from 62% to 56% over the 10-year period, they remain unacceptably high. On the positive side, this also means that the rate of usable codes has slightly increased over the period from 37.3% in 2009–2010 to 43.5% in 2017–2018 (Table 2). Contributing to the negative conclusion is that the rate of garbage codes of “very high severity (level 1)” increased from 43% in 2009–2010 to 50% in 2017–2018. These garbage codes were consistently higher in the age-category 70 years and above and among males over the 10-year period. The ‘percentage of deaths with unspecified age or sex’, and the ‘percentage of deaths with causes of deaths considered impossible’ in some age-sex combinations were very low with 1–2 deaths in each period.
4.6Business process mapping (BPM)
In addition to assessing the completeness and quality of causes of death statistics, we evaluated the efficiency of the existing certification and registration processes to understand causes of delay in data release. It can be seen from the BPM in Fig. 1, that there is duplication in death coding, as it is done both at the main referral facility and at the national level by the MoH. A critical aspect observed is the inordinate delay from the time of notification of death to the island council to the time for that information to reach the DNR. This is mainly due to the geographic dispersion of the Maldives islands, use of paper records, lack of prescribed time limits in the operating procedures, and use of outdated technology. Another cause of delay in production and dissemination is the bureaucratic processes at MOH and DNR. Although CoD is coded by MoH, they must always make a request for data from the DNR who in turn requests the national centre for information technology to provide the data to MoH for analysis.
The Maldives has initiated the work on a new online system which is currently being piloted in the field. The redesigned BPM in Fig. 2 is expected to considerably reduce the time required for ICD-10 coding, cleaning and compilation of VS, as this would allow initiation of death coding without having to wait for physical forms to be sent from islands to DNR and onward to MoH. This, if implemented, can help produce snapshots of VS data bi-annually and facilitate a more timely sharing of data with national planning agencies and/or international parties for better-informed policy and programming. Furthermore, the system will be able to respond to the VS data requirements in emergencies such as that of the COVID-19 pandemic.
5.Discussion, conclusion and recommendations
It is widely recognized that a well-functioning CRVS systems and investment into strengthening the system are not only vital for individuals and societies, but also a development imperative that is critical for national health [15]. The Maldives is among the very few countries in the World Health Organisation (WHO) South East Asia Region (SEAR) [22] that has been able to register almost all deaths in its territory with information on causes of death. However, when compared to other small island countries Maldives performs poorer than Mauritius but better than Seychelles [23]. The reporting and quality of age and sex for all registered deaths have consistently been complete over the last ten years. However, the quality of reporting causes of death remains a major concern. Similar to what is reported in global studies [23], there has been little improvement in the VSPI(Q) from 2009 to 2018 in the Maldives. The proportion of garbage codes remains very high with more than half of them in the category of very high severity. This includes a handful of causes such as cardiac arrest, shock and deaths reflected with impossible causes, coded as such as a minor injury. There are only a few ICD codes that contribute to most of the garbage codes; these include cardiac arrest, unspecified, essential (primary) hypertension, other ill-defined and unspecified causes of mortality and septicemia, unspecified, and respiratory arrest. This makes the overall quality of the data poor and of little use to policy makers.
The assessment of death certificates based on the Medical Certification of Cause of Death (MCCOD) tool [24], showed that in addition to illegible hand-writing, there were weaknesses in other aspects of quality cause of death recording [25]. This observation raised questions about whether the current practices to equip doctors with skills for MCCOD are appropriate and adequate. Improving the quality of MCCOD solely rest within the mandate of the MoH in the Maldives and flows downstream to the health care providers. Since the CoD certification is completed by a medical doctor in the Maldives, there is a unique opportunity to improve the quality of CoD data. This can be achieved through training of doctors in standard death certification practices, which has proven to reduce the errors in other countries [26]. This can be supplemented with strategies such as hospital based committees that can oversee cause of death quality assessments [27].
The functions of the CRVS system in the Maldives, as in many other countries, is handled by multiple stakeholders. This arrangement introduces an inherent risk of fragmentation that requires each party to play an important role to improve its functioning. Experiences from other countries show that no single agency can be expected to tackle the weaknesses of CRVS system [28].
The CRVS system in the Maldives is complete from the perspective of the level of registration and the process is fairly well-functioning though there are time delays in transmission of information due to geographic dispersion of population. The country has initiated action for implementing an online CRVS system, which is expected to cut down on the delay in transmission, processing and compilation of mortality data and has the potential to provide mortality data in real-time. It must be, however, recognized that a real-time CRVS system neither automatically improves quality of data nor brings efficiencies in the processes. Efforts must be made to systematically enhance the organizational capabilities such as policies, legal framework, human resources, management and coordination in order to implement a CRVS system that is able to provide data in real time with the desired quality. It would be crucial to systematically assess the current status of death registration and CoD [29] identify bottlenecks and develop, based on analysis, a strategic action plan with indicators for monitoring and timelines for implementation. A significant and sustained government commitment and investment in strengthening the CRVS in the Maldives is recommended in response to monitoring mortalities as mandated by the SDGs [30].
Acknowledgments
The paper was prepared under the kind mentorship of Raj Gautam Mitra, Country Advisor Vital Strategies (Cambodia, Vietnam and Sri Lanka), Data for Health. We also thank Eileen P. Capilit, Matthew Shearing and Gemma Van Halderen from UNESCAP for guidance and support provided during the stages of this paper preparation.
References
[1] | Suthar AB, Khalifa A, Yin S, Wenz K, Ma Fat D, Mills SL, et al. Evaluation of approaches to strengthen civil registration and vital statistics systems: a systematic review and synthesis of policies in 25 countries. PLOS Medicine. (2019) ; 16: (9): e1002929. |
[2] | National Bureau of Statistics. Statistical Yearbook of Maldives 2018 http://statisticsmaldives.gov.mv: Govermnet of Maldives; (2019) [Available from: http://statisticsmaldives.gov.mv/yearbook/2018/geography/. |
[3] | Mohamed M, Razzag UA. Health statistics reporting in Maldives. In: Ministry of Health and Gender, editor. Third regional conference on production and use of Vital Statistics; 1 July; Daejeon, Korea. US stats website (2014) . p. 28. |
[4] | Law on birth and death registration of Maldives, 7/92 ((1992) ). |
[5] | Sirken MG, Rosenberg HM, Chevarley FM, Curtin LR. The quality of cause-of-death statistics. American Journal of Public Health. (1987) ; 77: (2): 137-9. |
[6] | Patterson JE. Assessing the quality of vital statistics. American Journal of Public Health. (1980) ; 70: (9): 944-5. |
[7] | Masquelier B, Pison G, Rakotonirina J, Rasoanomenjanahary A. Estimating cause-specific mortality in Madagascar: an evaluation of death notification data from the capital city. Population Health Metrics. (2019) ; 17: (1): N.PAG-N.PAG. |
[8] | Hasanpour-Heidari S, Jafari-Delouei N, Shokoohifar N, Sedaghat SM, Moghaddami A, Hosseinpour R, et al. Completeness and accuracy of death registry data in Golestan, Iran. Archives of Iranian Medicine (AIM). (2019) ; 22: (1): 1-6. |
[9] | Usman SK. Maldives Health Statistics 2015–16. Maldives: Ministry of Health; 2019 May 2019. 198. |
[10] | GBD 2017 Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392 North American Edition (10159): 1684-735. |
[11] | Phillips DE, Lozano R, Naghavi M, Atkinson C, Gonzalez-Medina D, Mikkelsen L, et al. A composite metric for assessing data on mortality and causes of death: the vital statistics performance index. Population Health Metrics. (2014) ; 12: : 2-30. |
[12] | Mikkelsen L, Moesgaard K, Hegnauer M, Lopez AD. ANACONDA: a new tool to improve mortality and cause of death data. BMC Medicine. (2020) ; 18: (1): 61. |
[13] | University of Melbourne. Tools specifically to assess mortality data quality – ANACONDA: University of Melbourne; (2019) [Available from: https://crvsgateway.info/Tools-specifically-to-assess-mortality-data-quality-ANACONDA∼341. |
[14] | University of Melbourne. Understanding CRVS systems: The importance of process mapping: University of Melbourne; (2018) [Available from: https://crvsgateway.info/file/9847/46. |
[15] | Phillips DE, AbouZahr C, Lopez AD, Mikkelsen L, de Savigny D, Lozano R, et al. Are well functioning civil registration and vital statistics systems associated with better health outcomes? Lancet. 2015; 386 North American Edition (10001): 1386-94. |
[16] | Upham S, Mikkelsen L. Advocacy for strengthening civil registration and vital statistics. Pacific Health Dialog. (2012) ; 18: (1): 41-52. |
[17] | World Health Organisation. International statistical classification of diseases and related health problems: World Health Organisation, (2007) [10th revision: [Available from: http://apps.who.int/classifications/apps/icd/icd10online. |
[18] | Mikkelsen L, Moegaard K, Hegnauer M, Lopez AD. ANACONDA: A new tool to improve mortality and cause of death data. BMC Medicine. (2020) . |
[19] | Cobos Muñoz D, Abouzahr C, de Savigny D. The ’Ten CRVS Milestones’ framework for understanding Civil Registration and Vital Statistics systems. BMJ Glob Health. (2018) ; 3: (2): e000673-e. |
[20] | Alexander L. Determining causes of death: How we reclassify miscoded deaths. IHME Foundations; (2018) . |
[21] | Murray CJ, Lopez AD, Organization WH. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020: summary: World Health Organization; (1996) . |
[22] | WHO. About WHO South-East Asia Region WHO website: WHO; (2020) [cited 2020. Available from: https://www.who.int/southeastasia/about. |
[23] | Mikkelsen L, Phillips DE, AbouZahr C, Setel PW, de Savigny D, Lozano R, et al. A global assessment of civil registration and vital statistics systems: monitoring data quality and progress. The Lancet. (2015) ; 386: (10001): 1395-406. |
[24] | Rampatige R, Saman G, Nicola R, Ian R, Nandalal W. Assessing the quality of death certificates: Guidance for the rapid tool: Civil Registration and Vital Statistics Improvement Group, Bloomberg Philanthropies Data for Health Initiative; (2019) [Available from: https://crvsgateway.info/file/9587/62. |
[25] | Usman SK. Assessing the quality of mortality data in the Maldives. Bloomberg Philanthropies Data for Health Initiative: The University of Melbourne, (2020) Contract No.: 20 April. |
[26] | Miki J, Rampatige R, Richards N, Adair T, Cortez-Escalante J, Vargas-Herrera J. Saving lives through certifying deaths: assessing the impact of two interventions to improve cause of death data in Per? BMC Public Health. (2018) ; 18: (1): N.PAG-N.PAG. |
[27] | Hart JD, Sorchik R, Bo KS, Chowdhury HR, Gamage S, Joshi R, et al. Improving medical certification of cause of death: effective strategies and approaches based on experiences from the data for health initiative. BMC Medicine. (2020) ; 18: (1): 1-11. |
[28] | AbouZahr C, de Savigny D, Mikkelsen L, Setel PW, Lozano R, Nichols E, et al. Civil registration and vital statistics: progress in the data revolution for counting and accountability. The Lancet. (2015) ; 386: (10001): 1373-85. |
[29] | Rampatige R, Gamage S, Peiris S, Lopez AD. Assessing the reliability of causes of death reported by the vital registration system in sri lanka: medical records review in colombo. Health Information Management Journal. (2013) ; 42: (3): 20-8. |
[30] | Collaborators GS. Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals for 195 countries and territories: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) ; 392: (10159): 2091-138. |

