Orthorexia prevalence among health care professionals involved in nutrition education: The ADI-O Study
Abstract
BACKGROUND:
Orthorexia Nervosa (ON) is defined as a pathological fixation about the consumption of healthy food. ON doesn’t yet appear in the Diagnostic and Statistical Manual of Mental Disorders-V (DSM-V) as a nosological category, so that it remains a new controversial concept that affects mostly health care professionals.
OBJECTIVE:
The aim of our study was to evaluate the prevalence of orthorexia in a large sample of health care professionals involved in nutrition education (1240 subjects).
METHODS:
A masked form of the Orto-15 questionnaire, the main validated test for the screening of orthorexic patients, was administrated to the ADI members by e-mail.
RESULTS:
The total score is significantly lower in divorced people (than in married or unmarried people, p = 0.005), biologists (rather than medical doctors, p = 0.002), free-lances (than government employees, p = 0.020), smokers (than no smokers, p = 0.011) and in professionals following a diet (p < 0.001). The main score predictors are the marital status (B =−0.464, CI95% =−0.727 – −0.134, p = 0.007, divorced vs. other categories), BMI (B = 0.882, CI95% = 0.819–0.976, p = 0.012) and adherence to a diet (B =−2.200, CI95% =−6.066 – −1.819, p < 0.001 versus subjects with free diet).
CONCLUSION:
In this large sample, orthorexia seems to be quite widespread, especially among biologists, free-lances, divorced, smokers, dieting and thin subjects.
1Introduction
Orthorexia Nervosa (ON) is a recent not yet codified entity [1], which can be defined as an obsession for healthy food [2].
ON has no diagnostic criteria [3], and it is not listed neither in DSM-V nor ICD-10, but it was debated on whether or not it should have a place in the recently published DSM V [4].
Million people follow particular nutritional restrictions or rules (vegans, vegetarians, fruitarians, raw foodists,...) for different motivations and reasons, but ON is a real fixation for healthy food and it isn’t only related to trends, religious feelings or philosophical customs [5]. Any obsessive idea can be a trigger: a health concern and a worry for the influence that nutrition has on it, can drive towards particular attitudes that evocate dietary restrictions.
The great attention and warning about the healthy nutrition is linked to the extreme importance that food is thought to have in maintaining a good state of health or in preventing illness, so that patients affected by ON spend most of their time making accurate selection of products to keep a correct dietary intake and this activity becomes the most important segment of their life [6].
Since the first published papers ON seems to be quite spread in the whole population [5–7] and most of all in particular groups like: athletes [8], artists [9] and nutritional medical figures [10–13].
In this context, the primary aim of our study was to estimate the prevalence of orthorexia in a large group of health care professionals involved in nutrition education, all members of the Italian Association of Dietology and Clinical Nutrition (ADI), by the mailing of a validated self-administered questionnaire, the ORTO-15 test [14]. The secondary aim was to evaluated the determinants of the ORTO-15 score in the studied population.
2Materials and methods
1240 ADI associated were recruited posting by e-mail a masked form of the Orto-15 questionnaire, the main validated test for the screening of orthorexic patients [5, 14]. The masking was made including the questions of the Orto-15 in the context of a more general explorative questionnaire with the apparent aim to define as best the general eating behavior among ADI professionals, depending on their anagraphic characteristics, cultural level and university degree, kind of work, life-style, and cardiovascular risk factors. Questions had multiple-choice answers associated to different scores with values from 1 to 4, “1” was the closest to orthorexia and “4” indicated a normal alimentary behaviour.
In the validation study [14], two different cut-off has been considered: 40 showed to have the most predictive power towards healthy nutrition behaviour (normality for values >40), but no specific power for orthorexia diagnosis, especially for the identification of obsessive traits. Cut-off of 35 has been analyzed in order to increase specificity and to improve diagnostic tendencies.
All the sampled data were included and encoded in a specific database by trained professionals. A full descriptive analysis was carried out of all sampled variables. Categorical data were compared by the chi-square test followed by the Fisher exact test. The Orto-15 test score was compared among groups with non-parametric tests (Kruskal-Wallis analysis of variance followed by the Mann-Whitney-U test). Then the factors associated to Orto-15 test scores were evaluated by a linear regression.
We applied as diagnostic cut-off the ones already indicated in literature: 35 or 40 [13].
Then, we applied the Alpha-Chronbach test to evaluate the more unspecific questions.
3Results
Our cohort counts 517 subjects: 46,2% (239) males and 53,8% (278) females.
The test was administrated to 203 medical doctors (39,3% ), 187 dieticians (36,2% ), 65 biologists (12,6% ) and other 62 health professionals (12% ). 53,8% work in national health system hospitals, 46,2% are free-lances.
Most of the subjects (61.1% ) were normoweight (mean BMI: 23,08±0,14), 15,9% underweight, 18,4% overweight and 3,9% obese, with a trend towards obesity and overweight among males and a trend towards underweight and normoweight among females (Fig. 1).
78% of the subjects spent less than 4 hours/week in physical activity, 17% 5–8 hours per week and less than 5% spent more than 8 hours per week. 53.6% led a light physical activity, moderate in 42.2% , intense just in 4.3% . Smoking habits were revealed in 21.5% of the subjects. 14.9% followed a specific diet in the last year (Figs. 2 and 3).
1.9% of the subjects were affected by diabetes, 5.2% by celiac disease/food intolerances, 11.6% by dyslipidemia and 10.1% by hypertension (Fig. 4).
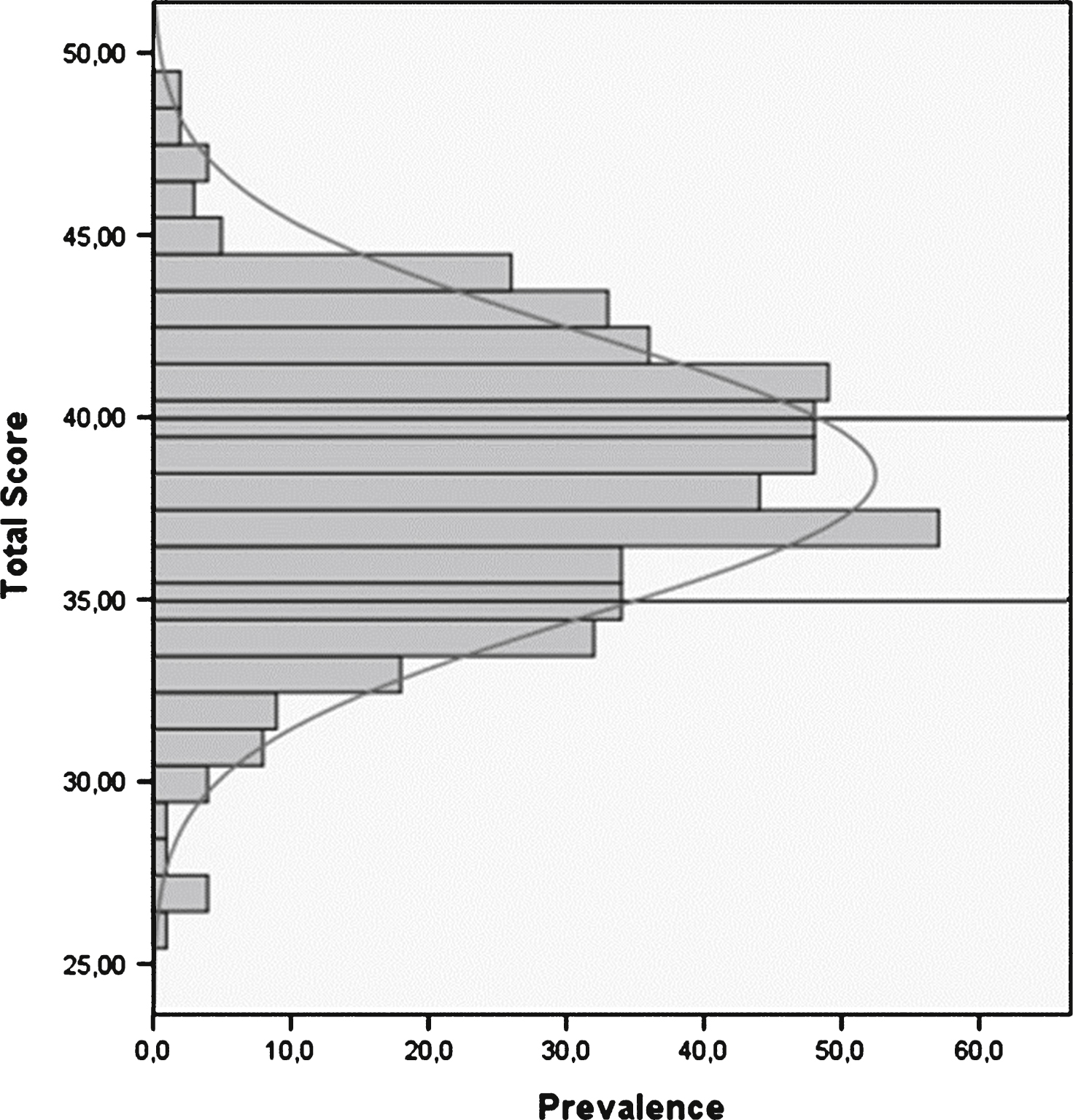
Our results of the 517 questionnaires show an high prevalence of patients with orthorexic attitude: the average score is 38.62 (SD) with 14.6% of the subjects with a score <35 and 55% with a score <40 (Fig. 5).
The total ORTO-15 score does not differ significantly between sex, professional figures, geographic areas, pathologies as diabetes or food intolerances, which should promote a different attention to diet.
On the other hand, the final (total) score is significantly lower in divorced people (than married or never married people, p = 0.005), biologists (rather than medical doctors, p = 0.002), free-lances (than government employees, p = 0.020), smokers (than never smokers, p = 0.011) and in dieting subjects (p < 0.001).
The marital status (B =−0.464, CI95% =−0.727 – −0.134, p = 0.007, divorced vs. other categories), BMI (B = 0.882, CI95% = 0.819–0.976, p = 0.012) and adherence to a diet (B =−2.200, CI95% =−6.066 – −1.819, p < 0.001 versus subject with free diet) are also the main score predictors, both in the univariate model and in a multivariate model.
No correlation has been found between the total score and continuous variables as age, physical activity hours and intensity, neither in univariate model nor in multivariate model.
Collecting answers from the ORTO-15 Test of our interviewed people some items resulted quite similar.
In the items number 2, 6 and 14 more than 80% of the people gave the answers 1 or 2; in items 3, 7 and 15 more than 80% answered 3 or 4: these items were therefore not specific for the orthorexia identification, as confirmed by the Cronbach alpha-test.
4Discussion
Our study, carried on in a large sample of health care professionals involved in nutrition education, shows that health care professionals are at high risk for Orthorexia Nervosa.
Our data do not agree with previous publications [9, 10, 15] because they don’t find any significant correlation between ORTO TEST score and BMI, conversely our findings show a negligible statistically significant association between ORTO-15 and BMI as in Varga study [3]. This correlation (thinnest members have lower score that can predict orthorectic behaviours) can be explained by general characteristics of ADI members, being mostly normoweight with a 15,9 % underweight and this can be explained by a greater attention for nutritional intake.
Differently from former studies [12] but in line with the most recent publication, in our sample, there is no difference in Ortho-Test score between sex [4, 5, 10, 14], metabolic disorders and diabetes that usually need a better care in feeding. However, as a limit of our study, the diagnosis of diabetes and metabolic disorders are self-reported and not based on objective data.
Our study has also some other relevant limitations. The first one is the selection bias, because the sample was developed on the bases of spontaneous enrollment of the ADI professionals. However, the sample size is one of the largest reported in literature and it is representative of whole compound of ADI members. A second limitation is the clinical data that are self-reported and based on dichotomous (non quantitative) variables. This is in the nature of self-administered questionnaires, and clinical evaluation of the enrolled volunteers was outside the aim of this study. Moreover, health care professionals, interviewed could be influenced in their answer by the kind of questions and oriented to answer in the wrong way in order to avoid a diagnosis of orthorexia. In previous studies, in fact, the questionnaire was administered in an open fashion [5, 7, 8]. However, we are confident on our questions masking in the context of a more general questionnaire by the high prevalence we found. By the way, this is a large survey investigating study carried on to evaluate the prevalence of alleged new eating disorder in general population. Moreover, we evaluated a large number of health care professionals, considering many descriptive variables.
In conclusion, our survey shows that orthorexia could be a new largely undiagnosed eating disorder well represented among professionals involved in nutrition. However, the main validated diagnostic tool, the Orto-15, has to be improved because some items seem to be unspecific, especially among experts of nutrition.
5Conclusions
This first “ADI-O study” carried on health care professionals shows that the studied population has proper life-style habits even if it presents an high rate of orthorexia nervosa especially among biologists, free-lances, divorced, smokers, thin people and dieting subjects.
Conflict of interest
No one to be declared.
Appendix 1
The ED ADI Study Group: Fabrizio Malvaldi (Livorno), Annalisa Maghetti (Bologna), Valentina Culicchi (Grosseto), Irene Del Ciondolo (Siena), Elena D’Ignazio (Bologna), Barbara Paolini (Siena), Giuseppe Malfi (Cuneo), Daniela Vassallo (Torino), Francesca De Donà (Torino), Lorenza Caregaro (Padova), Roberta Situlin (Trieste), Pierandrea Vinci (Trieste), Simonetta Marucci (Terni), Massimo Vincenzi (Faenza) [Coordinator]
Acknowledgments
We are particularly grateful to Prof. L.M. Donini to have provided us the original validated Italian version of the ORTO 15 Test. We also thanks the regional ADI coordinators for their general support to the study.
References
1 | Bratman S, Knight D(2000) Health Food Junkies: Overcoming the obsession with heathfull eatingNew YorkBroadway Books |
2 | Dalla Ragione L, Scoppetta M(2009) Giganti d’argillaIl pensiero scientifico4046isbn 9788849002744 |
3 | Varga M, Thege SBK, Dukay-Szabò S, Tury F, Van Furth EF(2013) Evidence and gaps in the literature on orthorexia nervosaEat. Weight Disord18: 210311110.1007/s40519-013-0026-y |
4 | Fairburn Ch, Cooper Z(2011) Eating disorders, DSM-V and the clinical realityBr J Psych198: 81010.1192/bjb110.083881 |
5 | Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C(2004) Orthorexia nervosa: A preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenonEat Weight Disord9: 151157 |
6 | Ramacciotti CE, Perrone P, Coli E, Burgalassi A, Conversano C, Massimetti G, Dell’Osso L(2011) Orthorexia nervosa in the general population: A preliminary screening using a self-administred questionnaire (ORTO-15)Eat Weight Disord16: e127e130 |
7 | Barthels F, Pietrowsky R(2012) Orthorectic eating behaviour – nosology and prevalence ratesPsychother Psychosom Med Psychol62: 1244544910.1055/s-0032-1312630 |
8 | Segura-Garcia C, Papaianni MC, Caglioti F, Procopio L, Nisticò CG, Bombardiere L, Ammendolia A, De Fazio P, Capranica L(2012) Orthorexia nervosa: A frequent eating disordered behaviour in athletesEat Weight Disord10.3275/8272 |
9 | Aksoydan E, Camci N(2009) Prevalence of orthorexia nervosa among Turkish performance artistsEat Weight Disord14: 13337 |
10 | Kinzl JF, Hauer K, Trawegher CH, Chefer I(2006) Orthorexia nervosa in dietitiansPsychother Psychosom75: 39539610.1159/000095447 |
11 | Bagci Bosi AT, Camur D, Guler C(2007) Prevalence of orthorexia nervosa in resident medical doctors in the faculty of Medicine (Ankara, Turkey)Appetite49: 366166610.1016/j appet.2007.04.007 |
12 | Fidan T, Ertekin V, Isikay S, Kirpinar I(2010) Prevalence of orthorexia nervosa among medical students in Erzurum, TurkeyCompr Psychiatry51: 1495410.1016/j comppsych.2009.03.001 |
13 | Alvarenga MS, Martins MC, Sato KS, Vargas SV, Philippi ST, Scagliusi F(2012) Orthorexia nervosa behavior in a semple of Brazilian dietitians assessed by the Portoguese version of ORTO-15Eat Weight Disord17: 1e29e35 |
14 | Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C(2005) Orthorexia Nervosa: Validation of a diagnosis questionnaireEat Weight Disord10: e28e32 |
15 | Arusoglu G, Kabakci E, Koksal G, Kutluay Merdol T(2008) Orthorexia nervosa and adaptation of ORTO-11 in to TurkishTurk J Psych19: 3283291 |
Figures and Tables
Fig.1
BMI distribution per sex in the studied population.
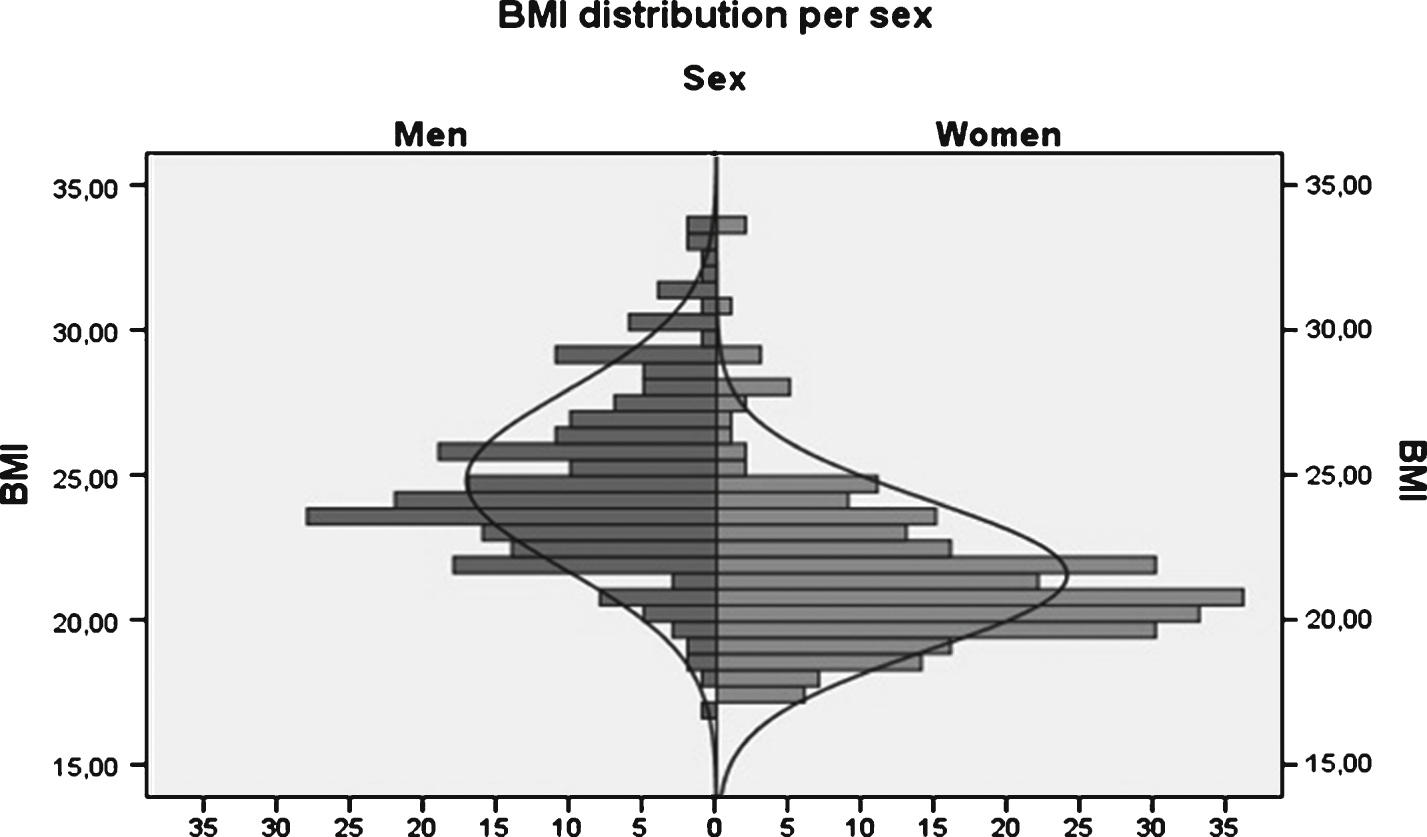
Fig.2
Hours/week spent in physical activity.
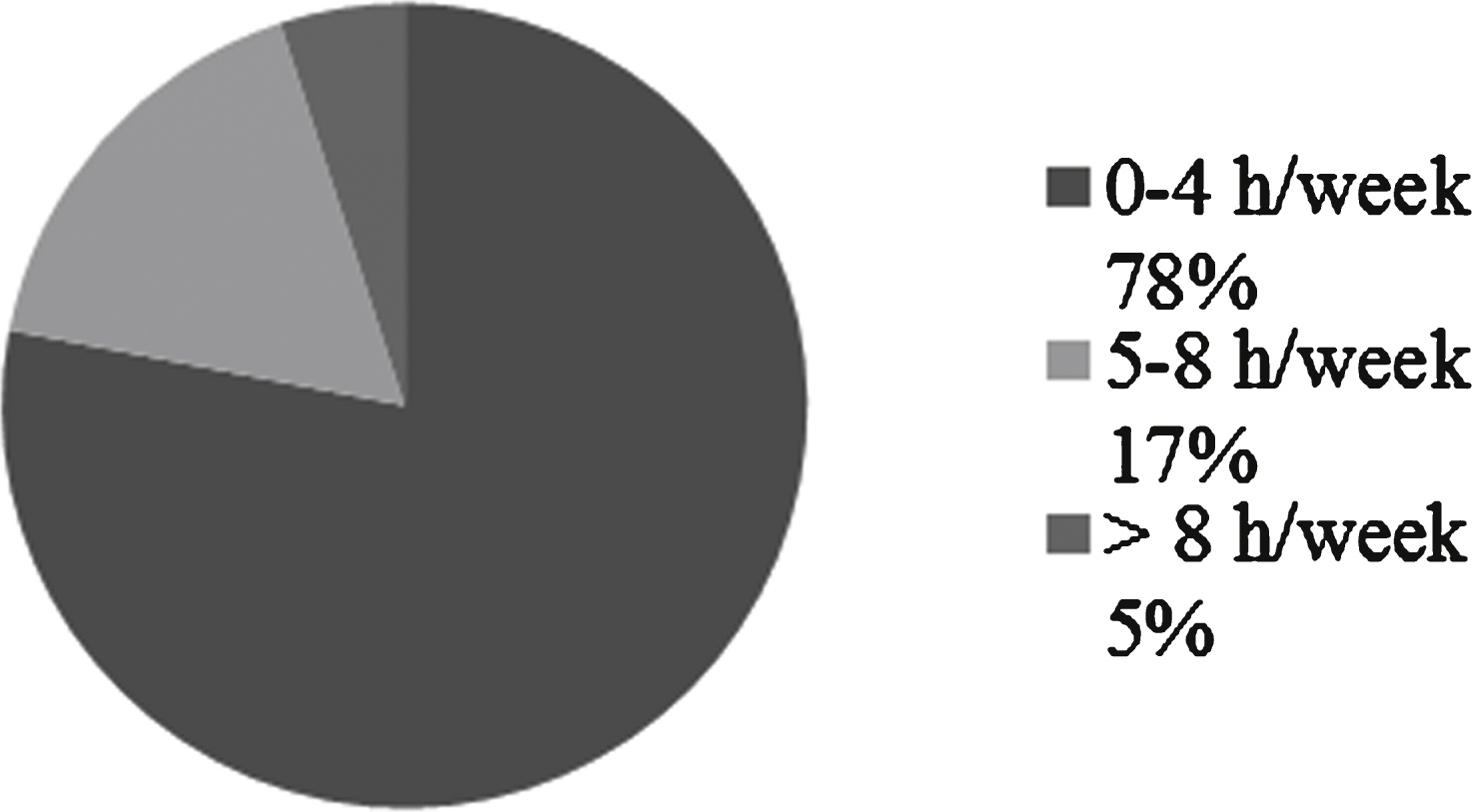
Fig.3
Type of physical activity exercised by the studied population, described as “light”, “moderate” and “intensive”.
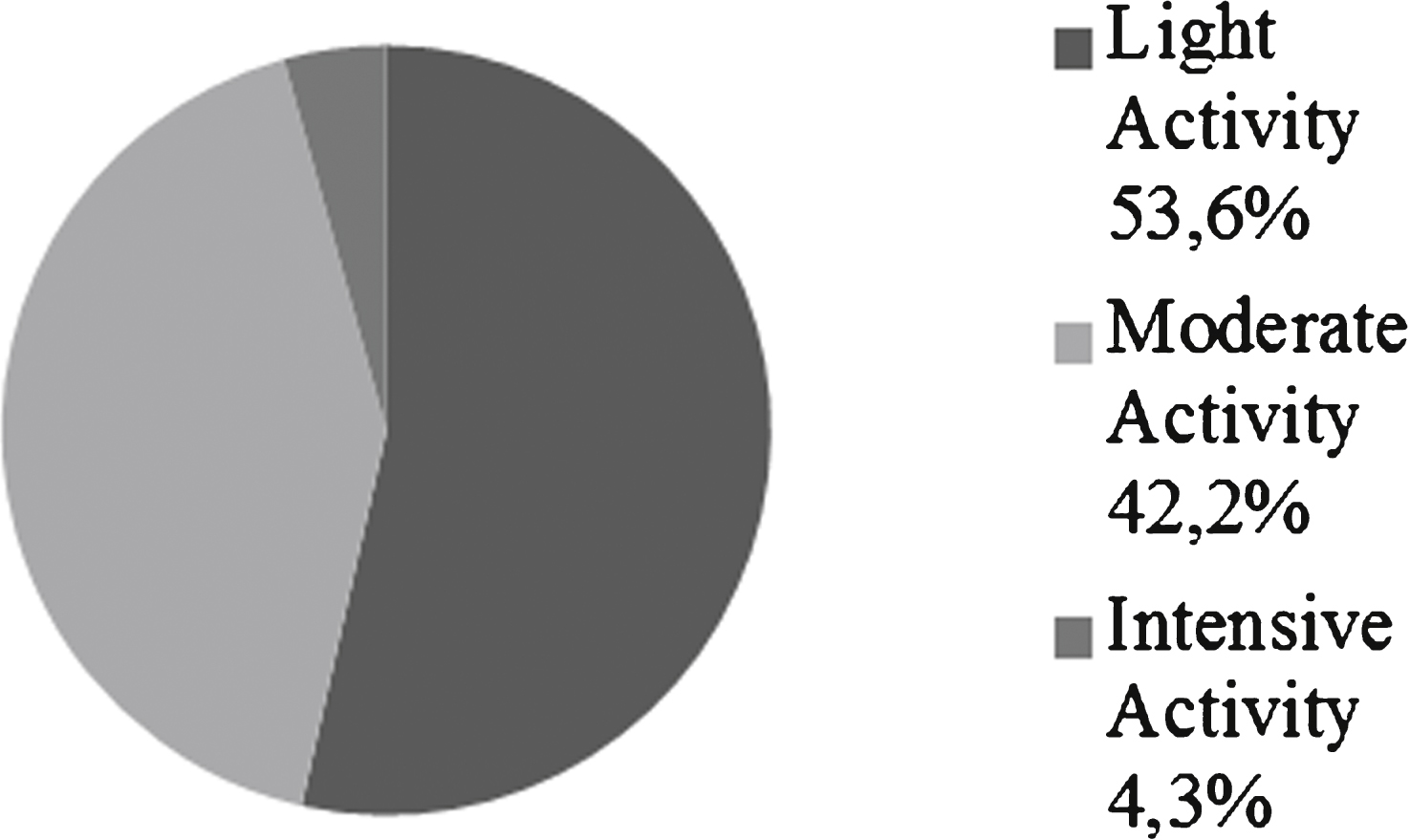
Fig.4
Health disorders distribution.
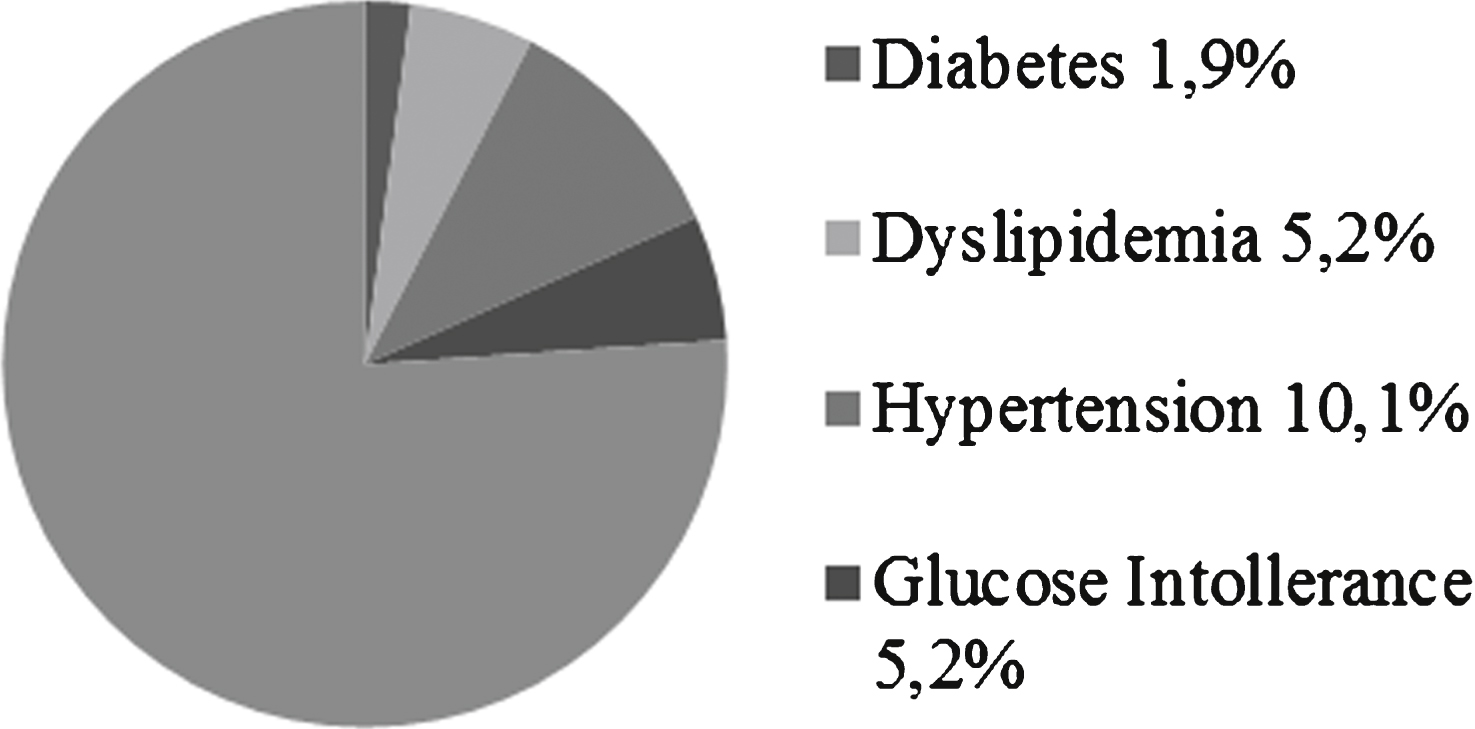
Fig.5
Questionnaires results and their distribution: 55% of the subjects reach a score <40, 14,6% a score <35.