
Efficacy of Therapy vs Surveillance in Patients with Resected Early-Stage Intermediate to High-Risk Renal Cell Carcinoma
Abstract
BACKGROUND:
The historical standard of care for locally advanced renal cell carcinoma (RCC) is nephrectomy + active surveillance. Despite a high recurrence rate ( 40%), adjuvant therapy was previously not included in the standard of care. This review of adjuvant pharmacotherapy reflects conflicting results from multiple trials.
OBJECTIVE:
The objective of this review is to summarize the efficacy of therapy vs surveillance in resected early-stage intermediate to high-risk renal cell carcinoma.
METHODS:
We performed a systematic literature search using PubMed, EMBASE, and SCOPUS. Keywords such as “renal cell carcinoma”, “adjuvant therapy” and “nephrectomy” were used. In the literature search, 2,711 studies were identified and screened.
RESULTS:
We included a total of 21 publications. The most common histology seen in trials was clear cell carcinoma. A variety of interventions were reviewed including immunotherapy, medroxyprogesterone acetate, interferon alfa, and tyrosine kinase inhibitors. Most trials did not demonstrate a benefit in relapse-free survival (RPS) or overall survival (OS). Pembrolizumab demonstrated a significant difference in disease recurrence in the KEYNOTE-564 trial although median data was not reached. Blinded independent reviewers identified a benefit in disease-free survival (DFS) with Sunitinib in the S-TRAC trial.
CONCLUSION:
There was not a clear benefit in using adjuvant therapy broadly for resected locoregional RCC; however, further investigation should be done in the highest-risk group to elucidate potential benefit.
INTRODUCTION
Renal cell carcinoma is the 6th most common cancer in men and the 9th most common cancer in women, representing 50,290 and 28,710 of projected cases for 2022 respectively [1]. This is an increase from last year for men and women, with 48,780 and 27,300 cases respectively [2].
Pembrolizumab has been accepted as a standard of care for adjuvant therapy for high-risk clear-cell renal cell carcinoma (RCC) in the United States and Europe [3], whereas surveillance remains an important option. Patients should be followed using history and physical, complete blood count, liver and kidney function, and chest and abdominal imaging either with computed tomography scan or magnetic resonance imaging. These guidelines are based on a systemic review from Donat et al in 2013 (3). Clear cell histology represents 75–80% of RCC [4]. In patients who undergo nephrectomy, disease recurrence can be as high as 40–50% [5]. Despite the encouraging data with the use of pembrolizumab, other trials studying adjuvant therapy have not yielded similar results. This warrants further investigation to ascertain the difference in patient selection, tumor types, etc.
Defining highest risk has been a challenge in selecting patients most suitable for adjuvant therapy. Stage, clinical activity, histology, and nuclear grade have all been studied to identify those patients at highest risk for recurrence. These features have also been combined into both preoperative and postoperative nomograms. Molecular features have not yet been applied prospectively to adjuvant clinical trials to hone risk.
The University of California LA Integrated Staging System (UISS system) is based on tumor, nodal disease, and metastatic disease (TMN), nuclear grade, and performance status [6]. Five-year survival predictions in this model range from 80.4% for moderate-risk disease to 54.7% for high-risk disease. Stage, size, necrosis, and grade (SSIGN) is a model used to predict 5-year metastatic-free survival [7]. In this model, intermediate and high-risk disease carry a 5-year metastases free survival of 73.8% and 31.2% respectively. The Karakiewicz preoperative nomogram utilizes age, gender, clinical stage, tumor size, presence of metastases, and classification of symptoms to predict survival with an >80% accuracy rate [8]. The Leibovich postoperative prognostic model was demonstrated to be able to accurately predict progression and death with c-indexes >0.75 [9]. The grade, age, nodes, and tumor stage (GRANT) score is a newer prognostic score that was validated both in the ASSURE trial and in a large population from the Surveillance, Epidemiology and End Results (SEER) database [10, 11].
Many drugs active in metastatic clear cell renal cancer have been investigated for adjuvant therapy in RCC, including vascular endothelial growth factor receptor tyrosine kinase inhibitors (VEGFR-TKIs) which target platelet-derived growth factor receptor and vascular endothelial growth factor receptor, two receptors which contribute to tumor growth and proliferation [12, 13], mammalian target of rapamycin inhibitors, vaccines, and immunotherapies. Given the variable results of adjuvant therapy in patients with completely resected early-stage intermediate to high-risk RCC, we aimed to systematically review the current body of evidence to provide updated data and guidance on the treatment of these patients.
METHODS
A systematic review of peer reviewed medical literature was searched in PubMed, Embase, and Scopus between October 16 and November 6, 2022, by the second author. The search was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [14]. The focus of the search was to identify studies in PubMed, EMBASE, and SCOPUS reporting on adjuvant therapy in resected early-stage intermediate to high-risk RCC. The PICO (Population, Intervention, Comparison, Outcome) question framework was utilized to structure the research question into a search strategy: (P) in patients, who are older than 18 years of age, diagnosed with RCC or early stage RCC, (I) that have only been treated with a partial or radical nephrectomy and are monitored, (C) when compared with RCC patients who have undergone a partial or radical nephrectomy and received adjuvant therapy, (O) is partial or radical nephrectomy, coupled with adjuvant therapy efficacious for patients with intermediate to high risk RCC. The search was limited to English language human studies, i.e., articles, conference papers, and conference abstracts, in which patients were older than 18 years of age and had been diagnosed with RCC or early stage RCC. The entire file for each database was searched, but the coverage for each database was different, i.e., Medline - 1946 – present; Embase – 1947-present, and Scopus, continuously, 1970 - present.
The key search concepts: “renal cell carcinoma,” “nephrectomy, i.e., full, radical, or whole,” “adjuvant therapy,” and specific drugs, “atezolizumab, axitinib, cabozantinib, durvalumab, everolimus, girentuximab, ipilimumab, nivolumab, pazopanib, pembrolizumab, sorafenib, sunitinib, and tremelimumab,” were mapped to controlled vocabulary and keywords, then combined with Boolean operators. Search results were downloaded into EndNote and duplicate references were removed. The refined search results were then uploaded into Covidence for further review. Complete search strategies are available in the Appendix.
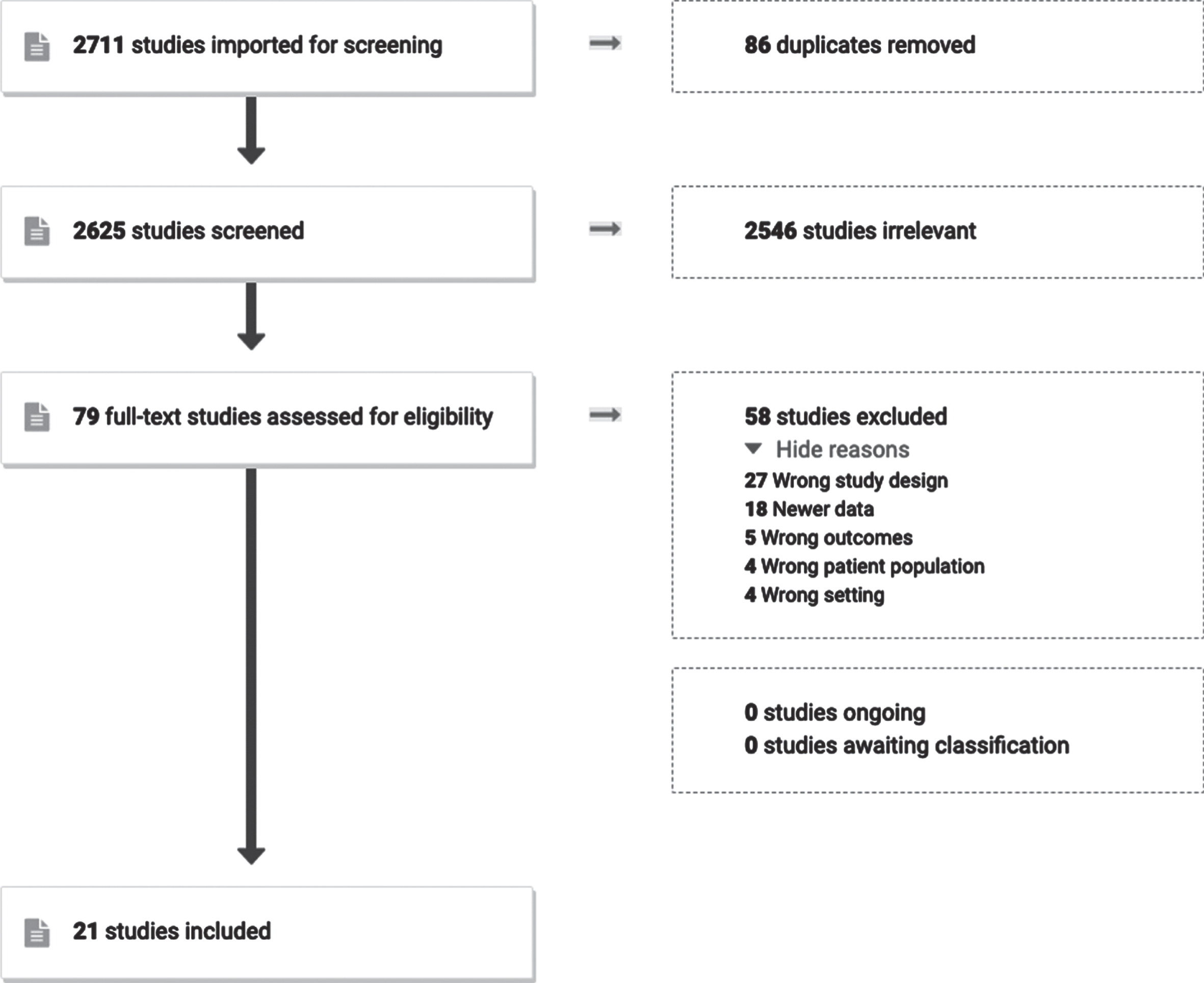
The selection process was conducted in multiple stages. The first author reviewed the title and abstract of all studies captured in the literature search to ascertain suitability. Once all articles had been screened, the first and last author discussed the studies that had been screened in during the first stage. There were no disagreements on which studies should be included. The first author manually searched the references of all included studies to search for potentially relevant studies that were not captured by the search strategy. Studies that were identified during this process also had their references searched until no more could be found. The first and last author then discussed these studies and compiled the final list for data extraction. The first author extracted the data from the articles and the last author reviewed the extracted data. Covidence, a web-based collaboration software platform, was used to screen studies and create the flow diagram of screened studies (Fig. 1).
Fig. 1
PRISMA flow chart including exclusion criteria for screened studies.
Eligibility criteria
The literature search revealed 2,711 studies. When imported, 86 duplicates were removed which left 2,625 studies to be screened. Of those, 2,546 were screened out based on title and abstract alone. This left 79 full-text studies to be assessed, of which 21 were included for data extraction. All studies were trials, and many included a placebo group. The data was extracted by the first author and reviewed by the last author (Table 1).
Table 1
Results of trials studying adjuvant therapy in resected early-stage intermediate to high-risk renal cell carcinoma. *DFS and OS were reported in various ways in different studies and thus is reported in terms of 5 years percentages, probabilities, or median years unless otherwise stated
| Study ID | Year | Intervention | Patients (n) | Histology | Primary Endpoint | DFS* (Study vs control) | OS* (Study vs control) |
| Pizzocaro et al. [15] | 1987 | Medroxyprogesterone acetate | 136 | Unknown | Unspecified | 32.7% vs 33.9% | 67.1% vs 67.3% |
| Galligioni et al. [17] | 1996 | Autologous tumor cells + Bacillus Calmette-Guerin | 120 | Unknown | Unspecified | 63% vs 72% (p = 0.21) | 69% vs 78% (p = 0.28) |
| Pizzocaro et al. [19] | 2001 | Interferon alfa-2b | 247 | Unknown | Unspecified | 0.567 vs.671 (p = 0.107) | 0.660 vs.665 (p = 0.861) |
| Messing et al. [20] | 2003 | Interferon alfa-NL | 283 | Clear cell (69.3%) | Survival | 2.2 yrs vs 3.0 yrs (p = 0.33) | 5.1 yrs vs 7.4 yrs (p = 0.09) |
| Clark et al. [21] | 2003 | High-dose bolus IL-2 | 69 | Clear cell (46%) | DFS | Accrual halted due to futility | Accrual halted due to futility |
| Jocham et al. [23] | 2004 | Autologous renal tumor cell vaccine | 343 | Unknown | PFS | 77.4% vs 67.8% (p = 0.0204) | Not assessed |
| Aztpodien et al. [26] | 2005 | Interferon alfa-2a, IL-2, and fluorouracil | 203 | Clear cell (62%) | RFS | 42% vs 49% (p = 0.2398) | 58% vs 76% (p = 0.0278) |
| Wood et al. [24] | 2008 | Autologous renal tumor cell vaccine | 728 | Clear cell | RFS | 75% vs 72.7% (p = 0.390) [2 yr follow up] | 87.7% vs 86.8% (p = 0.586) [2 yr follow up] |
| Aitchison et al. [27] | 2014 | Alpha-interferon, IL-2, and fluorouracil | 309 | Not specified | DFS | 61.3% vs 50.4% (p = 0.233) for 3 yr DFS | 69.7% vs 62.8% (p = 0.428) |
| Passalacqua et al. [28] | 2014 | Interferon-alfa and lose-dose IL-2 | 303 | Clear cell (84%) | RFS | 76% vs 73% (p = 0.44) | 80% vs 81% (p = 0.79) |
| Haas et al. [30] | 2016 | Sunitinib vs sorafenib vs placebo | 1943 | Clear cell (79%) | DFS | 5.8 yrs (sunitinib) vs 6.1 yrs (sorafenib) vs 6.6 yrs | Sunitinib vs placebo: (HR 1.02; 97.5% CI, 0.85–1.23, p = 0.8038) Sorafenib vs placebo (HR 0.97; 97.5% CI, 0.80–1.17, p = 0.7184) |
| Ravaud et al. [35] | 2016 | Sunitinib vs placebo | 610 | Clear cell | DFS | 6.8 yrs vs 5.6 yrs (p = 0.03) | Not mature, p = 0.04 for the immature data |
| Chamie et al. [29] | 2017 | Girentuximab vs placebo | 864 | Clear cell (97%) | DFS and OS | 53.9% vs 51.6% (p = 0.74) | Not reached for either arm and no difference between arms with HR.99 |
| Motzer et al. [36] | 2017 | Pazopanib 800 mg vs placebo | 403 | Clear cell (>90%) | DFS | (HR, 0.69; 95% CI, 0.51 to 0.94; nominal P = 0.02) | |
| Motzer et al. [36] | 2017 | Pazopanib 600 mg vs placebo | 1135 | Clear cell (>90%) | DFS | (HR, 0.86; 95% CI, 0.70 to 1.06; P = 0.16 | |
| Gross-Goupil et al. [40] | 2018 | Axitinib vs placebo | 724 | Clear cell | DFS and OS | Not reached | 71.4 mo. (3-NR) vs NR |
| Eisen et al. [33] | 2020 | 3 yrs Sorafenib vs 1 yrs Sorafenib + 2 years placebo vs placebo | 1711 | Clear cell (84%) | DFS | Median DFS not reached in any arm. 3 years of sorafenib vs placebo (HR, 1.01; 95% CI, 0.82 to 1.23; P = 0.946). 1 year of sorafenib vs placebo (HR, 0.94; 95% CI, 0.77 to 1.14; P = 0.509). DFS in 3 years vs 1 year vs placebo (53% vs 55% vs 54%). | No difference in duration of OS was observed. 3 years of sorafenib vs placebo (HR, 1.06; 95% CI, 0.82 to 1.38; P = 0.638). OS for 1 year of sorafenib vs placebo: HR, 0.92; 95% CI, 0.71 to 1.20; P = 0.541). OS in 3 years vs 1 year vs placebo (70% vs 69% vs 69%). |
| Choueiri et al. [3] | 2021 | Pembrolizumab vs placebo | 994 | Clear cell | DFS | Median DFS not reached | Median OS not reached |
| Pal et al. [46] | 2022 | Atezolizumab vs placebo | 778 | Clear cell (93%) | DFS in intention to treat population | 57.2 mo. (95% CI 44.6 to NE) with atezolizumab and 49.5 mo. (47.4 to NE) with placebo (HR 0.93, 95% CI 0.75–1.15, p = 0.50). | 90.3% vs 89.8% |
| Allaf et al. [47] | 2022 | Nivolumab vs Observation | 819 | Clear cell (85%) | RFS | (HR, 0.97; 95 CI, 0.74–1.28, p = 0.43, median RFS not reached). Trial stopped due to futility. | (HR, 1.48; 95% CI, 0.89–2.48, p = 0.93) |
| Motzer et al. [50] | 2022 | Nivolumab + Ipilimumab vs placebo | 816 | Clear cell | DFS | 37 mo. Follow up: (HR, 0.92; 95% CI, 0.71–1.19; P = 0.5347) | Not assessed |
| Ryan et al. [41] | 2022 | Everolimus vs placebo | 1545 | Clear cell (83%) | RFS | 76 mo. Follow up (HR, 0.85, 95% CI, 0.72–1.00; p = 0.0246), prespecified significance level was 0.022 | Not assessed |
All full-text original articles reporting on adjuvant therapy in resected early-stage intermediate to high-risk RCC were included. Articles not in English, those that were not original work (review articles, case reports, editorials, etc.) were excluded. Abstracts during the years 2021-2022 were included due to the rapidly changing nature of this field. In situations where there were multiple publications for the same cohort, the publication with the newest data was selected. If the full text for the article was not available, the publication was excluded. Publications not reporting on adjuvant therapy in resected early-stage intermediate to high-risk RCC were excluded.
Data Extraction
The following variables were extracted: study name, year, intervention, number of patients, histology, primary endpoint, disease-free survival (DFS), and overall survival (OS). Disease-free survival was used interchangeably with relapse-free survival (RFS) and recurrence-free survival (RFS) depending on how the studies addressed it.
Data Synthesis
Due to heterogeneity of studies with different classes of drugs and varying numbers of patients, outcome measures were not compared rather than combined. Data was organized in chronological order from oldest study to newest given the rapidly changing nature of the RCC environment. Each study was discussed independently although similar topics were grouped when feasible.
RESULTS
Medroxyprogesterone acetate
Medroxyprogesterone acetate was studied in the early 1980 s as a potential adjuvant treatment in patients with localized RCC who had undergone a radical nephrectomy [15]. This was based on responses seen in a small group of patients with renal cancer who expressed estrogen and/or progesterone receptors in primary kidney tumors [16]. Over a span of four years, 136 patients were recruited to medroxyprogesterone acetate vs a control group. Patients with Robson stages 1–3 were included in this study. Those with a Robson stage of 2 or 3 made up approximately half of the study. Robson stage describes the location of the tumor with stage 2 involving perinephric fat and stage 3 involving the renal vein and/or regional lymph nodes. The study group received 500 mg medroxyprogesterone acetate 3 times weekly for one year. Out of the 136 patients, 120 were deemed evaluable.
No difference was found in relapse rate between the study group and control group (32.7% vs 33.9%). The median interval to relapse was longer in the control group than in the study group (20 months vs 11 months); however, this difference was not significant. Five-year OS was not significantly different between the two groups with 67.1% still alive in the treatment group and 67.3% in the control group. A high number (56.9%) of patients in the medroxyprogesterone acetate group experienced complications related to the study drug.
Autologous tumor cells + Bacillus Calmette-Guerin
In the late 1990 s, the combination of an autologous tumor cell vaccine and bacillus Calmette-Guerin (BCG) was investigated as an adjuvant therapy in individuals with RCC who had undergone radical nephrectomy for RCC [17]. The rationale behind this design was to boost the individual’s own immune response against the tumor. This design demonstrated benefit in colon cancer patients thus the decision was made to study in RCC patients [18]. Over a four-year period, 120 patients were randomized to an autologous tumor cell vaccine and BCG vs surveillance. Five-year DFS was 63% for the study group and 72% for the control group with p = 0.21. Five-year OS was 69% for the study group and 78% for the control with p = 0.28. Neither DFS nor OS was considered statistically significant.
Interferon alfa
Interferon alfa was studied in the late 1990 s for use as adjuvant therapy in patients with Stages 2 and 3 RCC after radical nephrectomy [19]. Pizzocaro et al compared Interferon alfa with active surveillance. Eligible patients (n = 247) were those who had undergone radical nephrectomy and were found to have Robson stage 2 or 3 disease. Those randomized to adjuvant therapy received interferon-alfa three times weekly for 6 months. Disease-free survival was not statistically significant with probability of.567 for the study group and.671 for the control group with p-0.107. Overall survival was also not statistically significant between groups with OS probability.660 for the study group and.665 for the control group with p = 0.861. Univariate analysis did demonstrate statistical significance for N2 and N3 disease; however, the sample size was small, representing 10% of the study population.
SWOG-8792 trialed interferon-alfa vs observation in 283 patients [20]. Eligible patients were those with pT3-4a and/or node positive disease who had undergone a radical nephrectomy and lymphadenectomy. In this study, interferon alfa was given for 5 days every 3 weeks for a total of 12 cycles. DFS was not significant at 2.2 years in the study group and 3.0 years in the control group with p = 0.33. Median survival was 5.1 years in the study group and 7.4 years in the control group with a p = 0.09. The investigators stratified the results by tumor stage and nodal status, but still did not find significance.
High-Dose Bolus interleukin-2 (IL-2)
High-dose bolus IL-2 was investigated in the early 2000 s as adjuvant therapy for completely resected locally advanced high-risk RCC or M1 resected to NED [21]. At the time of the study, high-dose bolus IL-2 was the only therapy approved by the Food and Drug Administration for metastatic RCC [22]. Thirty-six percent of the study group had metastatic disease that was resected, and they showed no evidence of disease at the time of the study. This was a smaller study with 69 patients. Study patients were grouped according to disease stage and randomized 1:1 for high-dose IL-2 bolus vs control. The control group underwent active surveillance whereas the study received high-dose bolus IL-2 for a maximum of 28 doses (median of 20 doses) over 19 days. The primary endpoint was DFS. At the interim analysis, it was discovered that 72% of the expected events (disease progression or death) had occurred thus making it highly unlikely that high-dose bolus IL-2 would have the projected increase in DFS. Including only patients with locally advanced disease did not change this outcome therefore, accrual was halted. OS was also unchanged in this study.
Autologous vaccine trial
Autologous vaccination was studied as a possible adjuvant treatment for locally advanced completely resected RCC [23]. Thirty percent of the study group had pT3 disease. Patients were randomized to the vaccine group or to the control group which was active surveillance. A vaccine was created from the participant’s native tumor cells and 6 injections were given at 4 weeks intervals. The primary endpoint was progression-free survival. Five-year progression free survival for all eligible patients was 77.4% and 67.8% in the vaccine and control group respectively with p = 0.0204. When stratified by tumor stage, the significance disappeared for those with T2 tumors with 81.3% 5-year PFS in the vaccine group and 74.6% in the control group (p = 0.216). The significance was maintained, although the sample size was small at 11 patients, when looking at T3 tumors with 67.5% PFS in the vaccine group and 49.7% in the control group (p = 0.039). OS was not assessed in this cohort.
A study was conducted using an autologous, tumor derived heat shock protein (glycoprotein 96)-peptide complex known as Vitespen [24]. This was an open-label trial that randomized patients to vaccination vs observation. The primary endpoint was RFS. It was discovered that 124 of the patients in the intention-to-treat analysis had metastatic disease or recurrence disease prior to the start of the trial so RFS was calculated with and without those patients. Excluding the patients who had disease at the beginning of the trial, RFS over a span of two years was 75% for the study group and 72.7% for the control group with p = 0.390. OS was not mature but at the time of this study was 87.7% for the study group and 86.8% for the control group with p = 0.586.
Interleukin-2 and interferon-alpha2a based chemoimmunotherapy
Interferon alfa-2a, interleukin-2 (IL-2), and fluorouracil was studied as a treatment for progressive metastatic RCC, and a survival benefit was seen compared to interferon alfa-2a and vinblastine (Medizinische Hochschule Hannove as the coordinating center) [25]. The same group of investigators then trialed it in the adjuvant setting to assess efficacy [26]. Eligible patients were those with at least T3b disease who had undergone radical nephrectomy. Almost half of the patients (44%) had metastatic disease that was completely resected. Study patients received an 8-week treatment cycle of interferon alfa-2a, interleukin-2, and fluorouracil while control patients underwent observation. The primary endpoint was RFS. Five-year RFS was 42% for the study group and 49% for the control group with p = 0.2398. Stratified analysis by stage also did not reveal a survival benefit in the study group. Five-year OS was 58% for the study group and 76% for the control group, this was significant with p = 0.0278. While the investigators indicated that no toxicity-related death occurred, the study group had a significantly shorter OS than the control group.
Another study utilizing alpha-interferon, IL-2, and fluorouracil was conducted in patients at high risk of recurrence after nephrectomy (Clinical Trials number NCT00053807) [27]. Eligible patients had complete resection of their RCC with stage T3b and above or any pT stage with nodal disease or microscopic positive margins on pathology. The primary endpoint was DFS at 3 years and the secondary endpoint was OS at 5 years. Over a span of 9 years, 309 patients were randomized to treatment vs observation. Dose reductions, postponements. and premature halting of treatment occurred in 20–30% of the study group. Three-year DFS was 61.3% in the study group and 50.4% in the observation group with p = 0.233. Five-year OS was 69.7% in the study group and 62.8% in the observation group with p = 0.428. At 2 months, quality of life measures had decreased significantly for the treatment group, but these were no longer significant at 6 months. Overall, the treatment did not significantly change recurrence or survival but came at a cost of temporarily lowering of quality of life.
Interferon-alfa with low-dose IL-2 was also studied as an adjuvant therapy for resected RCC (Clinical Trials number NCT00502034) [28]. Eligible patients were those who had partial or radical nephrectomy for RCC and had pT2b stage and above. The primary endpoint was RPS, and then secondary endpoint was OS. Five-year RFS was 76% for the study group and 73% for the control group with p = 0.44. Five-year OS was 80% for the study group and 81% for the control group with p = 0.79. Neither of these were statistically significant, keeping in line with prior studies on this treatment.
Ariser
The Ariser trial studied Girentuximab, an IgG1 κ light chain chimeric version of murine monoclonal antibody that recognizes carbonic anhydrase IX (CAIX), a cell surface glycoprotein that is expressed on the majority of clear cell RCC [29]. This study was a randomized, double-blind, placebo-controlled phase 3 clinical trial that involved weekly girentuximab for 24 weeks. Eligible patients (n = 864) were those who had undergone either a partial or full nephrectomy – the breakdown of partial vs full was not included in the manuscript. Most patients had T3 disease with Grade 2 or 3. Twelve percent were metastatic at baseline. The primary end points were DFS and OS.
Median follow-up time for both groups was 54 months. Five-year DFS for the girentuximab and placebo group were 53.9% and 51.6% respectively with HR 0.97; 95% CI, (0.79–1.18). Median DFS was 71.4 months for the girentuximab group and not reached for the placebo group with p = 0.74, demonstrating a lack of efficacy for girentuximab. Even when separating by pathologic risk group, there was no statistically significant difference in DFS. Serious adverse events (AE) were split evenly between the study drug and placebo and most AEs were deemed unlikely to be related to either the study drug or placebo. Given that Girentuximab targets CAIX, a sub-group analysis was performed which demonstrated a non-specific treatment benefit in patients with a CAIX score of 200 or greater (HR, 0.75; 95% CI, 0.55–1.04; P = 0.8).
Vascular endothelial growth factor tyrosine kinase inhibitors (VEGFR-TKIs)
ASSURE
The ASSURE trial was a randomized double-blind placebo-controlled phase 3 trial that involved a 1:1:1 randomization of sunitinib vs sorafenib vs placebo for prevention of recurrence with completely resected locoregional RCC [30]. Sunitinib and sorafenib are both VEGFR-TKIs, and both have shown effectiveness in advanced RCC [31–33]. Eligible patients (n = 1943) were those with completely resected clear cell or non-clear cell RCC. The primary endpoint was DFS. Median DFS was 5.8 years (1.6–8.2) for sunitinib, 6.1 years (1.7-not estimable) for sorafenib, and 6.6 years (1.4-not estimable) for placebo. The study groups were also compared against the placebo group. Disease-free survival also did not differ significantly between sunitinib vs placebo (HR, 1.02; 97.5% CI, 0.85–1.23) or sorafenib vs placebo (HR, 0.97; 97.5% CI, 0.80–1.17). Stratified log-rank p for both comparisons was 0.8038 and 0.7184 respectively. Overall survival did not differ significantly for any of the groups with 5-year survival 77.9%, 80.5%, and 80.3% for sunitinib, sorafenib, and placebo respectively.
The ASSURE trial also did a prespecified subset analysis of those with clear-cell RCC since it is commonly associated with a Von Hippel-Lindau (VHL) mutation and more likely to benefit from anti-angiogenic therapy [34]. No differences were seen with sunitinib vs placebo (HR, 1.02; 97.5% CI, 0.85–1.22, stratified log-rank p = 0.8931) or sorafenib vs placebo (HR, 0.99; 97.5% CI, 0.83–1.19, stratified log-rank p = 0.8734. Medium DFS in this subset was 5.6 years (1.6–8.2) for sunitinib, 5.6 years (1.8-not estimable) for sorafenib, and 6.6 (1.5–8.1) for placebo.
Due to adverse events, the starting doses of sunitinib (50 mg to 37.5 mg) and sorafenib (800 mg to 400 mg) were reduced mid-way through the study to decrease discontinuation rates. Dose escalations and reductions were allowed with the amended protocol. The effects of starting at a reduced dose were significant with treatment discontinuation decreasing to 34% from 44% in those on sunitinib (Gray’s test p = 0.0142) and 30% from 45% in those on sorafenib (p = 0.0001). Despite the dose reduction, grade 3 or worse adverse events were still seen in over half the study group for both therapies.
Due to concerns raised about lack of efficacy due to treatment discontinuation, a post-hoc analysis was done which demonstrated an absence of treatment effect in the group who start at the full dose and those who started at a reduced dose. Treatment effect was not seen in those who started at a full or reduced dose however, the hazard ratio (1.40) favored placebo over sorafenib in the reduced dose group.
S-TRAC
The S-TRAC trial investigated sunitinib for prevention of relapse in high-risk resected locoregional RCC [35]. This study was a randomized double-blind phase 3 trial that involved sunitinib vs placebo on a 4-weeks-on, 2-weeks-schedule for 1 year or until disease recurrence, consent withdrawal, or unacceptable toxicity. Eligible patients (n = 610) were those who had undergone nephrectomy for locoregional RCC and had not received any systemic treatment. The primary endpoint was DFS.
Blinded independent review and investigator review were done during the efficacy analysis. Based on blinded independent review, the median duration of DFS for sunitinib vs placebo was 6.8 years (95% CI, 5.8 to not reached) and 5.6 years (95% CI, 3.8 to 6.6) with a HR 0.76 and 95% CI, 0.59 to 0.98; P = 0.03. Based on investigator review, the median duration of DFS for sunitinib vs placebo was 6.5 years (95% CI, 4.7 to 7.0) and 4.5 years (95% CI, 3.8 to 5.9) with a HR 0.81; 95% CI, 0.64 to 1.02; P = 0.08. Some significance was seen in a select subgroup of patients who were deemed to be higher risk based on tumor stage, Fuhrman grade, nodal involvement, and ECOG score of 1 or more. Independent central review found a significant difference in DFS (HR, 0.74; 95% CI, 0.55 to 0.99; P = 0.04) but investigator review did not identify significance (HR, 0.76; 95% CI, 0.58 to 1.01; P = 0.06). It appears that investigators called relapse more quickly than independent central review for patients taking sunitinib.
Adverse events were seen in most patients with grade 3 or higher reported in 63.4% of the treatment group as opposed to 21.7% of the placebo group. Dose reductions or interruptions were also more common in the treatment group compared to placebo (34.3% and 46.4% vs 2.0% and 13.2%). Health-related quality of life was also assessed, with patients in the sunitinib group reporting lower scores than those in the placebo group. While most of the metrics did not meet the prespecified minimally important difference of 10 points between sunitinib and placebo, diarrhea (mean difference, 12.0 points; 95% CI, 9.6 to 14.4) and loss of appetite (mean difference, 10.0 points; 95% CI, 7.9 to 12.2) did with a P < 0.001 for both metrics. Based on this study, sunitinib was improved in the United States as an adjuvant treatment for resected locoregional RCC at high risk of recurrence.
PROTECT
The PROTECT trial similarly investigated the VEGFR-TKI pazopanib verses placebo in patients with locally advanced RCC at high risk (pT2 or higher) for relapse after nephrectomy [36, 37]. Eligible patients had resected clear cell RCC that was deemed high risk for recurrence. Most patients (>90%) underwent a full nephrectomy. The initial starting dose for pazopanib was 800 mg daily but was reduced to 600 mg daily due to a higher-than-expected rate of discontinuation.
The primary endpoint was investigator-assessed DFS, specifically with pazopanib 600 mg. In the 600 mg group, the primary DFS endpoint was not met (HR, 0.86; 95% CI, 0.70 to 1.06; P = 0.16) with a median follow-up of 30.4 months for pazopanib and 30.7 months for placebo. A benefit, however, was seen in the 800 mg group (HR, 0.69; 95% CI, 0.51 to 0.94; nominal p = 0.02) and when both groups were analyzed together (HR, 0.80; 95% CI, 0.68 to 0.95; nominal p = 0.01). This, however, was not the primary endpoint and the 800 mg group made up a smaller proportion of the study. Median follow-up was 47.9 months for pazopanib 800 mg and placebo. Overall survival was not mature during this analysis but did not show significance at that time. Final analysis of OS did not convey a survival benefit with HR 1.0, 95% CI 0.80–1.26; p > 0.9) [38]. During the study, levels of pazopanib (Ctrough) were drawn and higher early Ctrough quartiles were associated with longer DFS (HR, 0.58; 95% CI, 0.42–0.82; P = 0.002) [39].
ATLAS
The ATLAS trial tested axitinib, a selective inhibitor of vascular endothelial growth factor receptors 1, 2, and 3 [40] in the adjuvant setting. Axitinib had been approved in metastatic RCC. This study was a randomized, double-blind, placebo-controlled phase 3 clinical trial that involved twice-daily oral axitinib 5 mg vs placebo with a minimum treatment time of 1 year and a maximum of 3 years. Eligible patients (n = 724) were those who had underwent a nephrectomy and had not received any systematic treatment. Both lower risk and higher risk patients were included in this study. The primary end point was DFS. At a preplanned interim analysis, the trial was halted due to futility as 203 events had occurred (96 in the axitinib group and 107 in the placebo group). In subgroup analysis looking at patients in lower-risk group, a reduction in DFS was not seen. In the subgroup of patients with the highest risk of recurrence, both independent review (HR, 0.735 [95% CI = 0.525–1.028]; P = 0.0704) and investigator review (HR, 0.641 [95% CI = 0.468–0.879]; P = 0.0051) were observed but they were not significant.
SORCE
The SORCE trial was an international, randomized, double-blind, three-arm trial of sorafenib vs placebo [33]. Patients were randomly assigned to 3 years of sorafenib vs 1 year of sorafenib + 2 years of placebo vs 3 years of placebo. Eligible patients had completely resected clear cell RCC or non-clear cell RCC that was deemed to be intermediate or high risk. The primary endpoint was DFS in either study arm. Disease-free survival was compared between 3 years of sorafenib vs placebo and did not show any significant difference (HR, 1.01; 95% CI, 0.82 to 1.23; P = 0.946). Disease-free survival was also compared between 1 year of sorafenib + 2 years of placebo vs placebo and no significant difference was observed (HR, 0.94; 95% CI, 0.77 to 1.14; P = 0.509). The ten-year DFS rate was 53% for 3 years of sorafenib, 55% for 1 year of sorafenib, and 54% for placebo, again demonstrating the lack of efficacy. No difference in OS was observed for 3 years of sorafenib vs placebo (HR, 1.06; 95% CI, 0.82 to 1.38; P = 0.638). Similar results were seen for 1 year of sorafenib vs placebo HR, 0.92; 95% CI, 0.71 to 1.20; P = 0.541). Adverse events were reported in most of the study population. Grade 3 and above adverse events were reported more frequently in the 1- and 3-year sorafenib group (58.6% vs 63.9%) than placebo (29.2%). Only a quarter of patients completed the 3-year arm of sorafenib, with 34% stopping treatment due to excessive toxicity.
EVEREST
The EVEREST trial investigated everolimus, an inhibitor of mammalian target of rapamycin (mTOR) vs placebo [41]. Everolimus has previously demonstrated efficacy in metastatic RCC [42]. Eligible patients (n = 1545) were those who had fully resected RCC at intermediate to high risk of recurrence. The primary endpoint was RFS. At the time of the analysis, the medium follow-up time was 76 months. The study group had a recurrence benefit, with HR 0.85, 95% CI, 0.72–1.00 with p = 0.0246. This missed the pre-specified one-sided significant level of 0.022. Median RFS was not reached in this study but the estimate for 6-year RFS was 64% for the study group and 61% for placebo. Those deemed high-risk for recurrence demonstrated benefit with HR 0.79, 95% CI 0.65–0.97; p = 0.011. Recurrence benefit was not seen in those at intermediate risk with HR 0.99, 95% CI 0.71–1.13 with p-0.48. Overall survival was similar between study group and placebo (HR 0.90, 95% CI, 0.71–1.13; p = 0.178). This study demonstrated benefit in those at high-risk for recurrence but not for those at intermediate risk.
Immune checkpoint inhibitor trials
KEYNOTE-564
Recently, the KEYNOTE-564 adjuvant trial tested pembrolizumab, a PDL-1 antibody with activity in metastatic RCC [3]. This study was a randomized, double-blind international trial that involved a 1:1 randomization of pembrolizumab vs placebo to be given once every 3 weeks for a maximum of 17 cycles or until disease recurrence. Eligible patients were those who had histologically confirmed locoregional RCC with a clear cell component and were high risk for recurrence (pT2 high grade or> = pT3 or pTxN1 or M1 resected within one year of nephrectomy). Nephrectomy (partial or radical –92.5% of the study group got a radical nephrectomy) was a prerequisite, and surgical margins had to be negative. The primary endpoint was DFS.
At the data-cutoff point for the KEYNOTE-564 trial, median DFS had not been reached; however, disease recurrence was 32% lower with pembrolizumab (HR, 0.68; 95% CI, 0.53–0.97; P = 0.002). The median OS was also not reached in either group, with 96.6% of patients alive in the pembrolizumab group and 93.5% in the placebo group at 24 months. Adverse events were seen in >90% of patients in both groups; however, 32.4% of patients in the pembrolizumab group experience a grade 3 to 5 adverse events compared to 17.7% in the placebo group.
A 30 month post-hoc analysis of the KEYNOTE-564 trial was done which showed that 75% of patients in the pembrolizumab group were disease-free compared to 65.5% in the placebo group. In terms of OS, at 30 months, 95.7% of patients in the pembrolizumab group were alive compared to 91.4% in the placebo group. This survival data, however, was not statistically significant. Further analysis demonstrated that pembrolizumab delayed time to first subsequent treatment or any-cause death compared to placebo (HR, 0.67; 95% CI, 0.50–0.90; medians not reached) [43]. Time from randomization to progress on next line of therapy or any-cause death was also delayed on pembrolizumab compared to placebo (HR, 0.57; 95% CI, 0.39–0.85; medians not reached) [43]. A post-hoc analysis of DFS and distant metastases free survival at 30.1 mo. across all risk subgroups participating in Keynote 564 was reported recently [44]. Most patients were enrolled in the UISS intermediate risk category (UCLA Integrated Staging System), and the benefit of pembrolizumab was seen across all risk groups consistent with the overall intent to treat group [45]. The FDA approved pembrolizumab for use as adjuvant therapy for resected locoregional RCC at high risk of recurrence based on the analysis at 24 mo, although the primary endpoint of DFS was not mature.
Thus, pembrolizumab can be used as adjuvant therapy in patients with pT2 (Grade 4) tumors and higher T stage with clear cell histology±sarcomatoid features and completely resected metastases within one year of nephrectomy; however, guidelines recommend surveillance as an equally efficacious option given that the data for Pembrolizumab is new [3].
IMmotion010
The IMmotion010 trial studied atezolizumab vs placebo in patients who had undergone nephrectomy and were at high risk of recurrence [46]. Atezolizumab is an anti-programmed death ligand 1 (PD-L1) antibody which preferentially bind to tumor cells rather than T cells. Eligible participants (n = 778) were those with resected RCC at increased risk of recurrence (65% were T2 or T3a, 21% were T3b-c or T4 or N+, and 14% were M1 with no evidence of disease). There was a proportion of patients (14%) who were M1 with no evidence of disease. Dose modifications of atezolizumab were not allowed in this study. The primary endpoint was investigator-assessed DFS. Median DFS was 57.2 months (95% CI 44.6 to not estimable) in the atezolizumab group and 49.5 months (47.4 to not estimable) in the placebo group (HR 0.93, 95% CI 0.75–1.15; p = 0.50) representing a non-significant difference. While survival data was not mature, there was no evidence that atezolizumab had a survival benefit compared to placebo (HR 0.97, 95% CI 0.67–1.42). Three-year survival was 90.3% for atezolizumab and 89.8% for placebo. The results of this study mirror other adjuvant studies revealing no RPS or OS benefit.
PROSPER
PROSPER (EA8143) was a phase 3 randomized cooperative group open label trial that enrolled patients planned for partial or radical nephrectomy who had clinical stage≥T2 or node positive disease who were deemed no evidence of disease post-nephrectomy. Three percent of patients had metastatic disease that was fully resected. This trial administered perioperative nivolumab for one cycle prior to resection of the primary tumor followed by 9 cycles of adjuvant nivolumab in one arm vs surgery and active surveillance in the comparator arm [47]. Nivolumab is a programmed cell death 1 immune checkpoint inhibitor that has demonstrated a survival advantage in metastatic RCC [48]. The rationale behind the perioperative nivolumab was to prime the immune system within the intact tumor in hopes that adjuvant therapy would be more effective. Over a period of 4 years, 819 patients were randomized to nivolumab or surgery alone. The primary endpoint was RFS. Due to futility, the trial was stopped prematurely with RFS similar between both arms (HR, 0.97; 95 CI, 0.74–1.28, p = 0.43, median RFS not reached). Although OS was not mature at the time of the analysis, no significant difference was seen for that endpoint (HR, 1.48; 95% CI, 0.89–2.48, p = 0.93). This was only available in abstract form and a subset analysis will be performed at a later time.
CHECKMATE 914
The CheckMate 914 trial investigated nivolumab + ipilimumab vs placebo or nivolumab vs nivolumab + ipilimumab vs placebo [49]. The current available analysis in abstract form is for nivolumab + ipilimumab vs placebo [50]. Eligible patients (n = 816) had undergone a radical or partial nephrectomy revealing predominant clear cell histology with high risk of relapse (T2a and greater). Patients with metastatic disease were not included in this trial. The primary endpoint was DFS. After a median follow-up of 37 months, DFS was not met (HR, 0.92; 95% CI, 0.71–1.19; P = 0.5347). At 24 months, DFS probabilities were 76.4% for the study group and 74% for the placebo group. Subgroup analysis revealed a potential benefit in patients with sarcomatoid features but this was not statistically significant. Thirty-three percent of patients discontinued the study drugs due to toxicities. Overall survival was not assessed at this time.
DISCUSSION
This review was comprised primarily of randomized control trials, most of which were placebo-controlled and blinded. Multiple agents with activity in metastatic renal cancer have been tested in the adjuvant setting. Medroxyprogesterone acetate did not have a disease-free or overall survival benefit and came with a high rate of toxicity. Autologous tumor cells were also trialed, again with no significant DFS or OS. Autologous vaccines were trialed again with a benefit in PFS seen in patients with T3 tumors, although the sample size was small (n = 11). A larger vaccination study did not demonstrate a significant benefit in RFS or OS. The ARISER trial investigated Girentuximab, a monoclonal antibody against carbonic anhydrase IX, overexpressed in poor prognosis renal cancer, with the trial demonstrating a lack of benefit in DFS and OS. It is important to note that 12% of the population was metastatic which could have shifted the results although separation by pathologic risk group did not demonstrate any difference. A non-specific treatment benefit was seen in individuals with a CAIX score of 200 or greater, indicating that this drug could be benefit solely in those with a high CIAX score.
After activity of VEGFR-TKI therapy was seen in metastatic disease, these drugs were heavily tested in the adjuvant setting. Patient selection, dose intensity, and duration of therapy were all investigated. As mentioned earlier, there was no statistical benefit in DFS in any of the adjuvant VEGFR-TKI trials (ASSURE, SORCE, PROTECT, ATLAS) except S-TRAC despite further analyses of pharmacokinetics, dosing strategies, duration of therapy, or by analyses of stage or nomogram. The S-TRAC trial demonstrated an improvement in DFS of approximately one year in most of the subgroups analyzed [51]. The S-TRAC trial analyzed their results by investigator review and blinded independent review. While investigator review did not reveal significance, blinded independent review did reveal a significant difference in DFS, both broadly and in higher-risk subgroups. After the results of S-TRAC were reported, the ASSURE trial published an ad hoc analysis of pT3/4 or node positive and clear cell histology that did not demonstrate a benefit with adjuvant sunitinib or sorafenib, even when broken down by dose quartiles [52]. Discussion regarding these conflicting trials has pointed towards patient selection and/or dose range as being the different in outcomes with only high-risk disease per UISS criteria allowed in S-TRAC [53]. However, S-TRAC only saw benefit with blinded independent review, raising the question of how applicable these results are to the population given that relapse is not generally detected by blinded independent review, rather by the patient’s team of physicians. Further, all VEGFR-TKI trials reported high rates of toxicity or intolerance in the adjuvant setting [30, 33, 35–37, 40].
The activity of immune checkpoint and CTLA4 inhibitors seen in advanced RCC as well as low albeit permanent side effect profile led to testing in the perioperative setting. As KEYNOTE-564 using a PD-1 inhibitor was the only trial demonstrating a difference in outcome, discussion is warranted to pose reasons for the differences in outcome among these trials. KEYNOTE-564 results are limited in that median DFS is not mature in either group, and an OS benefit has yet to be elucidated. The IMmotion-010 trial using a PDL-1 inhibitor versus placebo did not reveal a benefit in DFS or OS. A notable difference between the IMmotion-010 and KEYNOTE-564 trials was that 14% of the patients in the IMmotion-010 trial were M1 NED compared to 5.8% in KEYNOTE-564. Sarcomatoid features, which are known to have a worse prognosis, were similar between trials at 9% vs 10%. Duration of therapy was also similar between trials, with 61.1% of Pembrolizumab group completing 1 year of therapy compared with 65% of the Atezolizumab group.
PROSPER EA8143 tested nivolumab, a PD-1 immune checkpoint inhibitor, given prior to surgery and for 9 months following surgery might result in benefit over surgery alone. Both clear cell RCC and non-clear cell RCC patients were enrolled in this trial. Patient selection, duration of preoperative nivolumab and use of a non-placebo comparator are all under scrutiny. CHECKMATE 914 is questioned for its use of a shorter 6-month duration of adjuvant PD-1 inhibitor with a CTLA4 inhibitor, nivolumab + ipilimumab respectively, in a unique dosing schema spaced apart by 6 weeks (as opposed to the usual 3-week interval. The short duration 6-month nivolumab monotherapy comparator arm is not yet mature. After three years, DFS for the ipilimumab/nivolumab versus placebo arms was not significant and overall survival was not assessed. Critical differences between these immunotherapy trials that confound interpretation, are the type of drug (pdL1inhibitor versus PD-1inhibitor±CTLA-4 inhibitor), the duration of drug (1 year versus 6 months), and composition of the patients (only clear cell predominant or all comers, oligometastatic disease resected < or >12 months from the primary tumor, and the patient assessment in the middle of a pandemic which may have interrupted in person assessments. Additionally, the duration of neoadjuvant therapy in PROSPER may be important, based on recent studies performed in melanoma and colorectal cancer [54–56].
Treatment tolerability and reversible versus permanent side effects are important factors in the consideration of adjuvant therapy. Participants in the CHECKMATE 914 trial experienced a relatively high discontinuation rate, with a 32% discontinuation rate in the treatment group related to adverse events and four deaths attributed to the study drugs. PROSPER, on the other hand, exhibited a 14% discontinuation rate due to adverse effects. The S-TRAC trial also experienced a sizeable discontinuation rate of 28% in the treatment group. SORCE also struggled with patient tolerance and toxicity, with only a quarter of patients completing the 3-year arm. The balance of identifying efficacious and tolerable treatment is ongoing with more research needed.
Mutational burden may also play a role in the level of response towards immunotherapy. A recent study using neoadjuvant nivolumab in resectable early non-small cell lung cancer revealed that tumor mutational burden was predictive of response towards nivolumab [57]. Identifying a potential molecular target is another aspect of developing effective adjuvant therapy. A comprehensive genomic and transcriptomic analysis from the S-TRAC trial identified Mer proto-oncogene tyrosine kinase (MERTK) and Tryptophan 2,3 dioxygenase (TDO2) but further research is required [58].
Determining high-risk for recurrence is not always straightforward with nomograms varying, sometimes dramatically, in terms of projected 5-year DFS [59]. While nodal disease certainly has a poorer 5-year DFS, elucidating DFS among the different tumor stages can be challenging. It is likely, however, that these nomograms will be expanded significantly to include biomarkers in the near future. Similar to other cancers, biomarkers are being heavily investigated in RCC. Higher levels of kidney injury molecule-1 (KIM-1) post nephrectomy have shown worse DFS even when adjusting for grade, stage, and histology [60].
There are ongoing trials investigating the efficacy of adjuvant therapy in locally advanced RCC in patients who have undergone nephrectomy. The LITESPARK-022 (NCT05239728) trial aims to investigate belzutifan + pembrolizumab vs placebo + pembrolizumab with a primary endpoint of DFS [61]. Belzutifan is an inhibitor of HIF-2α, a transcription factor that has been implicated in tumorigenesis [62]. The RAMPART trial is a multi-arm trial for patients with fully resected RCC [63]. This trial investigates active surveillance vs durvalumamb vs tremelimumab in the adjuvant setting with a primary endpoint of DFS and OS.
A large cohort study from the National Cancer Database investigated the use of off-label adjuvant therapy in over 40,000 patients [64]. This study was conducted from 2006–2015 and considered high risk according to the University of California Los Angeles Integrated Staging System criteria, the same criteria used in the S-TRAC trial. Those who received adjuvant therapy had a statistically significant decrease in OS compared to those who did not receive it (p < 0.001). Subgroup analysis of those with and without nodal disease demonstrated decreased OS. Given that this was a cohort study, selection bias is a potential confounding factor in the results of this study, Additionally, it does not include a breakdown of the agents given as this review has demonstrated that some agents have more promise than others. It is clear, however, that further research is imperative in those with high-risk disease in conjunction with relevant biomarkers.
CONCLUSIONS
Adjuvant therapy for resected locoregional RCC does not have strong evidence supporting its use. Despite encouraging results from S-TRAC and Keynote –564, these remain outliers in this analysis and in our analysis, application to the general population does not currently favor adjuvant therapy. Potential areas of benefit include those with very-high risk disease and/or resected metastatic disease; however, further studies should be done in those populations. Furthermore, exploring biomarkers to predict the efficacy of adjuvant therapy is another area that should be investigated.
ACKNOWLEDGMENTS
The authors have no acknowledgements.
FUNDING
CKM and CIR and NBH report no funding.
AUTHOR CONTRIBUTIONS
CKM and NBH reviewed the literature, extracted the data, drafted, and finalized the manuscript. CIR designed and performed the search strategy and wrote portions of the methods section.
CONFLICT OF INTEREST
CKM has no conflict of interest to disclose. CR has no conflict of interest to disclose. NBH participated in advisory boards for MERCK, AVEO, EISAI, BMS. NBH is a study chair for E2805 ASSURE. NBH contributed to the study design for PROTECT, EA8143 PROSPER, KEYNOTE-564 and EVEREST. NBH was on the steering committee for PROTECT. NBH is a consultant for Roche Genentech.
NBH is an Editorial Board Member of this journal, but was not involved in the peer-review process of this paper, nor had access to any information regarding its peer-review.
SUPPLEMENTARY MATERIAL
[1] The Appendix is available in the electronic version of this article: https://dx.doi.org/10.3233/KCA-220018.
REFERENCES
[1] | Siegel RL , Miller KD , Fuchs HE , Jemal A Cancer statistics 2022, CA Cancer J Clin. (2022) ;72: (1):7–33. |
[2] | Siegel RL , Miller KD , Fuchs HE , Jemal A Cancer statistics, 2022 CA Cancer J Clin. (2021) ;71: (1):7–33. |
[3] | Choueiri TK , Tomczak P , Park SH , Venugopal B , Ferguson T , Chang YH , et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med. (2021) ;385: (8):683–94. |
[4] | Cairns P Renal cell carcinoma. Cancer Biomark. (2010) ;9: (1-6):461–73. |
[5] | Janzen NK , Kim HL , Figlin RA , Belldegrun AS Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease. Urol Clin North Am. (2003) ;30: (4):843–52. |
[6] | Zisman A , Pantuck AJ , Dorey F , Said JW , Shvarts O , Quintana D , et al. Improved prognostication of renal cell carcinoma using an integrated staging system. J Clin Oncol. (2001) ;19: (6):1649–57. |
[7] | Frank I , Blute ML , Cheville JC , Lohse CM , Weaver AL , Zincke H An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J Urol. (2002) ;168: (6):2395–400. |
[8] | Karakiewicz PI , Suardi N , Capitanio U , Jeldres C , Ficarra V , Cindolo L , et al. A preoperative prognostic model for patients treated with nephrectomy for renal cell carcinoma. Eur Urol. (2009) ;55: (2):287–95. |
[9] | Leibovich BC , Lohse CM , Cheville JC , Zaid HB , Boorjian SA , Frank I , et al. Predicting oncologic outcomes in renal cell carcinoma after surgery. Eur Urol. (2018) ;73: (5):772–80. |
[10] | Buti S , Puligandla M , Bersanelli M , DiPaola RS , Manola J , Taguchi S , et al. Validation of a new prognostic model to easily predict outcome in renal cell carcinoma: The GRANT score applied to the ASSURE trial population. Ann Oncol. (2017) ;28: (11):2747–53. |
[11] | Buti S , Karakiewicz PI , Bersanelli M , Capitanio U , Tian Z , Cortellini A , et al. Validation of the GRade, Age, Nodes and Tumor (GRANT) score within the Surveillance Epidemiology and End Results (SEER) database: A new tool to predict survival in surgically treated renal cell carcinoma patients. Sci Re. (2019) ;9: (1):13218. |
[12] | Nathan P , Chao D , Brock C , Savage P , Harries M , Gore M , et al. The place of VEGF inhibition in the current management of renal cell carcinoma. Br J Cancer. (2006) ;94: (9):1217–20. |
[13] | Sulzbacher I , Birner P , Traxler M , Marberger M , Haitel A Expression of platelet-derived growth factor-alpha alpha receptor is associated with tumor progression in clear cell renal cell carcinoma. Am J Clin Pathol. (2003) ;120: (1):107–12. |
[14] | Page MJ , McKenzie JE , Bossuyt PM , Boutron I , Hoffmann TC , Mulrow CD , et al. The PRISMA statement: An updated guideline for reporting systematic reviews. BMJ. (2021) ;372: :n71. |
[15] | Pizzocaro G , Piva L , Di Fronzo G , Giongo A , Cozzoli A , Dormia E , et al. Adjuvant medroxyprogesterone acetate to radical nephrectomy in renal cancer: 5-year results of a prospective randomized study. J Urol. (1987) ;138: (6):1379–81. |
[16] | Concolino G , Di Silverio F , Marocchi A , Bracci U Renal cancer steroid receptors: Biochemical basis for endocrine therapy. Eur Urol. (1979) ;5: (2):90–3. |
[17] | Galligioni E , Quaia M , Merlo A , Carbone A , Spada A , Favaro D , et al. Adjuvant immunotherapy treatment of renal carcinoma patients with autologous tumor cells and bacillus Calmette-Guerin: Five-year results of a prospective randomized study. Cancer. (1996) ;77: (12):2560–6. |
[18] | Hoover HC Jr , Brandhorst JS , Peters LC , Surdyke MG , Takeshita Y , Madariaga J , et al. Adjuvant active specific immunotherapy for human colorectal cancer: 6.5-year median follow-up of a phase III prospectively randomized trial. J Clin Oncol. (1993) ;11: (3):390–9. |
[19] | Pizzocaro G , Piva L , Colavita M , Ferri S , Artusi R , Boracchi P , et al. Interferon adjuvant to radical nephrectomy in Robson stages II and III renal cell carcinoma: A multicentric randomized study. J Clin Oncol. (2001) ;19: (2):425–31. |
[20] | Messing EM , Manola J , Wilding G , Propert K , Fleischmann J , Crawford ED , et al. Phase III study of interferon alfa-NL as adjuvant treatment for resectable renal cell carcinoma: An Eastern Cooperative Oncology Group/Intergroup trial. J Clin Oncol. (2003) ;21: (7):1214–22. |
[21] | Clark JI , Atkins MB , Urba WJ , Creech S , Figlin RA , Dutcher JP , et al. Adjuvant high-dose bolus interleukin-2 for patients with high-risk renal cell carcinoma: A cytokine working group randomized trial. J Clin Oncol. (2003) ;21: (16):3133–40. |
[22] | Yang JC , Topalian SL , Parkinson D , Schwartzentruber DJ , Weber JS , Ettinghausen SE , et al. Randomized comparison of high-dose and low-dose intravenous interleukin-2 for the therapy of metastatic renal cell carcinoma: An interim report. J Clin Oncol. (1994) ;12: (8):1572–6. |
[23] | Jocham D , Richter A , Hoffmann L , Iwig K , Fahlenkamp D , Zakrzewski G , et al. Adjuvant autologous renal tumour cell vaccine and risk of tumour progression in patients with renal-cell carcinoma after radical nephrectomy: Phase III, randomised controlled trial. Lancet. (2004) ;363: (9409):594–9. |
[24] | Wood C , Srivastava P , Bukowski R , Lacombe L , Gorelov AI , Gorelov S , et al. An adjuvant autologous therapeutic vaccine (HSPPC-96; vitespen) versus observation alone for patients at high risk of recurrence after nephrectomy for renal cell carcinoma: A multicentre, open-label, randomised phase III trial. Lancet. (2008) ;372: (9633):145–54. |
[25] | Atzpodien J , Kirchner H , Jonas U , Bergmann L , Schott H , Heynemann H , et al. Interleukin-2- and interferon alfa-2a-based immunochemotherapy in advanced renal cell carcinoma: A Prospectively Randomized Trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). J Clin Oncol. (2004) ;22: (7):1188–94. |
[26] | Atzpodien J , Schmitt E , Gertenbach U , Fornara P , Heynemann H , Maskow A , et al. Adjuvant treatment with interleukin-2- and interferon-alpha2a-based chemoimmunotherapy in renal cell carcinoma post tumour nephrectomy: Results of a prospectively randomised trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). Br J Cancer. (2005) ;92: (5):843–6. |
[27] | Aitchison M , Bray CA , Van Poppel H , Sylvester R , Graham J , Innes C , et al. Adjuvant 5-flurouracil, alpha-interferon and interleukin-2 versus observation in patients at high risk of recurrence after nephrectomy for renal cell carcinoma: Results of a phase III randomised European Organisation for Research and Treatment of Cancer (Genito-Urinary Cancers Group)/National Cancer Research Institute trial. Eur J Cancer. (2014) ;50: (1):70–7. |
[28] | Passalacqua R , Caminiti C , Buti S , Porta C , Camisa R , Braglia L , et al. Adjuvant low-dose interleukin-2 (IL-2) plus interferon-alpha (IFN-alpha) in operable renal cell carcinoma (RCC): A phase III, randomized, multicentre trial of the Italian Oncology Group for Clinical Research (GOIRC). J Immunother. (2014) ;37: (9):440–7. |
[29] | Chamie K , Donin NM , Klopfer P , Bevan P , Fall B , Wilhelm O , et al. Adjuvant weekly girentuximab following nephrectomy for high-riskrenal cell carcinoma: The ARISER randomized clinical trial. JAMAOncol. (2017) ;3: (7):913–20. |
[30] | Haas NB , Manola J , Uzzo RG , Flaherty KT , Wood CG , Kane C , et al. Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN EA double-blind, placebo-controlled, randomised, phase 3 trial. Lancet. (2016) ;387: (10032):2008–16. |
[31] | Motzer RJ , Hutson TE , Tomczak P , Michaelson MD , Bukowski RM , Rixe O , et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. (2007) ;356: (2):115–24. |
[32] | Escudier B , Eisen T , Stadler WM , Szczylik C , Oudard S , Siebels M , et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. (2007) ;356: (2):125–34. |
[33] | Eisen T , Frangou E , Oza B , Ritchie AWS , Smith B , Kaplan R , et al. Adjuvant sorafenib for renal cell carcinoma at intermediate or high risk of relapse: Results from the SORCE randomized phase III intergroup trial. J Clin Oncol. (2020) ;38: (34):4064–75. |
[34] | Kim H , Shim BY , Lee SJ , Lee JY , Lee HJ , Kim IH Loss of Von Hippel-Lindau (VHL) tumor suppressor gene function: VHL-HIF pathway and advances in treatments for metastatic Renal Cell Carcinoma (RCC). Int J Mol Sci. (2021) ;22: (18). |
[35] | Ravaud A , Motzer RJ , Pandha HS , George DJ , Pantuck AJ , Patel A , et al. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N Engl J Med. (2016) ;375: (23):2246–54. |
[36] | Motzer RJ , Haas NB , Donskov F , Gross-Goupil M , Varlamov S , Kopyltsov E , et al. Randomized phase III trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma. J Clin Oncol. (2017) ;35: (35):3916–23. |
[37] | Motzer RJ , Hutson TE , Cella D , Reeves J , Hawkins R , Guo J , et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. (2013) ;369: (8):722–31. |
[38] | Motzer RJ , Russo P , Haas N , Doehn C , Donskov F , Gross-Goupil M , et al. Adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma: Final overall survival analysis of the phase 3 PROTECT trial. Eur Urol. (2021) ;79: (3):334–8. |
[39] | Sternberg CN , Donskov F , Haas NB , Doehn C , Russo P , Elmeliegy M , et al. Pazopanib exposure relationship with clinical efficacy and safety in the adjuvant treatment of advanced renal cell carcinoma. Clin Cancer Res. (2018) ;24: (13):3005–13. |
[40] | Gross-Goupil M , Kwon TG , Eto M , Ye D , Miyake H , Seo SI , et al. Axitinib versus placebo as an adjuvant treatment of renal cell carcinoma: Results from the phase III, randomized ATLAS trial. Ann Oncol. (2018) ;29: (12):2371–8. |
[41] | Ryan CW , Tangen C , Heath EI , Stein MN , Meng M , Alva AS , et al. EVEREST: Everolimus for renal cancer ensuing surgical therapy — A phase III study (SWOG SNCT S0931, NCT01120249). Journal of Clinical Oncology. (2022) ;40: (17_suppl):LBA4500-LBA. |
[42] | Motzer RJ , Escudier B , Oudard S , Hutson TE , Porta C , Bracarda S , et al. Efficacy of everolimus in advanced renal cell carcinoma: A double-blind, randomised, placebo-controlled phase III trial. Lancet. (2008) ;372: (9637):449–56. |
[43] | Choueiri TK , Tomczak P , Park SH , Venugopal B , Ferguson T , Symeonides SN , et al. Adjuvant pembrolizumab for postnephrectomy renal cell carcinoma (RCC): Expanded efficacy analyses from KEYNOTE-564. Journal of Clinical Oncology. (2022) ;40: (16_suppl):4512. |
[44] | Choueiri TK , Tomczak P , Park SH , Venugopal B , Ferguson T , Symeonides SN , et al. Adjuvant pembrolizumab (pembro) for renal cell carcinoma (RCC) across UCLA Integrated Staging System (UISS) risk groups and disease stage: Subgroup analyses from the KEYNOTE-564 study. Journal of Clinical Oncology. (2023) ;41: (6_suppl):679. |
[45] | Zisman A , Pantuck AJ , Wieder J , Chao DH , Dorey F , Said JW , et al. Risk group assessment and clinical outcome algorithm to predict the natural history of patients with surgically resected renal cell carcinoma. J Clin Oncol. (2002) ;20: (23):4559–66. |
[46] | Pal SK , Uzzo R , Karam JA , Master VA , Donskov F , Suarez C , et al. Adjuvant atezolizumab versus placebo for patients with renal cell carcinoma at increased risk of recurrence following resection (IMmotion010): A multicentre, randomised, double-blind, phase 3 trial. Lancet. (2022) ;400: (10358):1103–16. |
[47] | Allaf M KS , Harshman LC , McDermott DF , Master VA , Signoretti S , Cole S , Moon H , Adra N , Singer EA , Gills J , Choueiri TK , Leibovich B , Michaelson MD , Shuch B , Lara PN , Heng DYC , Kapoor A , Carducci MA , Haas NB LBA67 - Phase III randomized study comparing perioperative nivolumab (nivo) versus observation in patients (Pts) with renal cell carcinoma (RCC) undergoing nephrectomy (PROSPER, ECOG-ACRIN EAa National Clinical Trials Network trial. Annals of Oncology. (2022) ;33: :S808–S69. |
[48] | Motzer RJ , Escudier B , McDermott DF , George S , Hammers HJ , Srinivas S , et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. (2015) ;373: (19):1803–13. |
[49] | Motzer RJ , Russo P , Grunwald V , Tomita Y , Zurawski B , Parikh O , et al. Adjuvant nivolumab plus ipilimumab versus placebo for localised renal cell carcinoma after nephrectomy (CheckMate 914): A double-blind, randomised, phase 3 trial. Lancet. (2023) . |
[50] | Motzer RJ RP , Gruenwald V , Tomita Y , Zurawski B , Parikh OA , Buti S , Bathelemy P , Goh JCH , Ye D , Lingua A , Lattouf J , Escudier B , George S , Shuch B , Simsek B , Spiridigliozzi , Chudnovsky A , Bex A LBA4 - Adjuvant nivolumab plus ipilimumab (NIVO+IPI) vs placebo (PBO) for localized renal cell carcinoma (RCC) at high risk of relapse after nephrectomy: Results from the randomized, phase III CheckMate 914 trial. Annals of Oncology. (2022) ;33: :S808–S69. |
[51] | Motzer RJ , Ravaud A , Patard JJ , Pandha HS , George DJ , Patel A , et al. Adjuvant sunitinib for high-risk renal cell carcinoma after nephrectomy: Subgroup analyses and updated overall survival results. Eur Urol. (2018) ;73: (1):62–8. |
[52] | Haas NB , Manola J , Dutcher JP , Flaherty KT , Uzzo RG , Atkins MB , et al. Adjuvant treatment for high-risk clear cell renal cancer: Updated results of a high-risk subset of the ASSURE randomized trial. JAMA Oncol. (2017) ;3: (9):1249–52. |
[53] | Porta C , Chiellino S ASSURE vs. S-TRAC: Conflicting results of adjuvant treatments for kidney cancer in the era of targeted agents and genomics. Ann Transl Med. (2016) ;4: (Suppl 1):S14. |
[54] | Patel SP , Othus M , Chen Y , Wright GP Jr , Yost KJ , Hyngstrom JR , et al. Neoadjuvant-adjuvant or adjuvant-only pembrolizumab in advanced melanoma. N Engl J Med. (2023) ;388: (9):813–23. |
[55] | Chalabi M , Fanchi LF , Dijkstra KK , Van den Berg JG , Aalbers AG , Sikorska K , et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. (2020) ;26: (4):566–76. |
[56] | Andre T , Lonardi S , Wong KYM , Lenz HJ , Gelsomino F , Aglietta M , et al. Nivolumab plus low-dose ipilimumab in previously treated patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: 4-year follow-up from CheckMate 142. Ann Oncol. (2022) ;33: (10):1052–60. |
[57] | Forde PM , Chaft JE , Smith KN , Anagnostou V , Cottrell TR , Hellmann MD , et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med. (2018) ;378: (21):1976–86. |
[58] | Motzer RJ , Martini JF , Mu XJ , Staehler M , George DJ , Valota O , et al. Molecular characterization of renal cell carcinoma tumors from a phase III anti-angiogenic adjuvant therapy trial. Nat Commun. (2022) ;13: (1):5959. |
[59] | Pal SK , Haas NB Adjuvant therapy for renal cell carcinoma: Past, present, and future. Oncologist. (2014) ;19: (8):851–9. |
[60] | Xu W , Puligandla M , Halbert B , Haas NB , Flaherty KT , Uzzo RG , et al. Plasma KIM-1 is associated with recurrence risk after nephrectomy for localized renal cell carcinoma: A trial of the ECOG-ACRIN research group (E2805) Clin Cancer Res. (2021) ;27: (12);3397–403. |
[61] | Choueiri TK , Bedke J , Karam JA , McKay RR , Motzer RJ , Pal SK , et al. LITESPARK- A phase 3 study of pembrolizumab + belzutifan as adjuvant treatment of clear cell renal cell carcinoma (ccRCC). Journal of Clinical Oncology. (2022) ;40: (16_suppl):TPS4602-TPS. |
[62] | Choi WSW , Boland J , Lin J Hypoxia-inducible factor-2alpha as a novel target in renal cell carcinoma. J Kidney Cancer VHL. (2021) ;8: (2):1–7. |
[63] | Oza B , Frangou E , Smith B , Bryant H , Kaplan R , Choodari-Oskooei B , et al. RAMPART: A phase III multi-arm multi-stage trial of adjuvant checkpoint inhibitors in patients with resected primary renal cell carcinoma (RCC) at high or intermediate risk of relapse. Contemp Clin Trials. (2021) ;108: :106482. |
[64] | Chakiryan NH , Acevedo AM , Garzotto MA , Chen Y , Liu JJ , Isharwal S , et al. Survival outcomes and practice trends for off-label use of adjuvant targeted therapy in high-risk locoregional renal cell carcinoma. Urol Oncol. (2020) ;38: (6):604 e1–e7. |


