
Global COVID-19 childhood disability data coordination: A collaborative initiative of the International Alliance of Academies of Childhood Disability
Abstract
PURPOSE:
The International Alliance of Academies of Childhood Disability created a COVID-19 Task Force with the goal of understanding the global impact of COVID-19 on children with disabilities and their families. The aim of this paper is to synthesize existing evidence describing the impact of COVID-19 on people with disabilities, derived from surveys conducted across the globe.
METHODS:
A descriptive environmental scan of surveys was conducted. From June to November 2020, a global call for surveys addressing the impact of COVID-19 on disability was launched. To identify gaps and overlaps, the content of the surveys was compared to the Convention on the Rights of the Child and the International Classification of Functioning, Disability and Health.
RESULTS:
Forty-nine surveys, involving information from more than 17,230 participants around the world were collected. Overall, surveys identified that COVID-19 has negatively impacted several areas of functioning - including mental health, and human rights of people with disabilities and their families worldwide.
CONCLUSION:
Globally, the surveys highlight that impact of COVID-19 on mental health of people with disabilities, caregivers, and professionals continues to be a major issue. Rapid dissemination of collected information is essential for ameliorating the impact of COVID-19 across the globe.
Implication for rehabilitation
COVID-19 has negatively impacted several areas of functioning, overall well-being, and rights of people with disabilities and their families worldwide.
Impact on mental health of people with disabilities, caregivers, and professionals continues to be a major issue globally.
Providing support to families may help mitigate the negative effects of the pandemic on the health of people with disabilities.
1Introduction
At the time of this writing, the coronavirus disease (COVID-19) pandemic continues to cause major disruptions in service provision, participation, and overall well-being of children and young people with disabilities and their families worldwide [1– 5]. Due to social distancing restrictions, often implemented in the form of partial or complete lockdown [6], almost 90% of children around the world did not attend schools in person resulting in a lack of access to education, habilitation, and rehabilitation services [7, 8]. Stunningly, this equates to 1.5 billion children not receiving regular education during the early stages of the lockdown [9]. Understanding the impact of COVID-19 on people with disabilities provides the essential foundation to ameliorate the negative consequences during this ongoing global crisis and improve support and services.
In response to this global crisis, the International Alliance of Academies of Childhood Disability (IAACD) created a COVID-19 Task Force with the main goal of understanding the global impact of COVID-19. Detailed information about working groups is provided on the Task Force page (https://iaacd.net/iaacd-covid-19-task-force/). Despite the uncertainties about the short-/medium-/long-term global impact of the COVID-19 crisis, there was no global data available, especially on children with disabilities and their families. To fill this gap, in June 2020, the members of the COVID-19 Task Force Surveys working group launched the Global COVID-19 Childhood Disability Data Coordination project to identify and map out data collection initiatives worldwide.
In the context of global health crises like the ongoing COVID-19 pandemic, it is important to pay attention to the needs, rights, and contextual factors that influence everyday functioning of people with disabilities, in particular children and youth. The United Nations Convention on the Rights of the Child (CRC) [10] recognises the extent of impact of global inequalities on children and their development. More importantly, all of the articles of CRC define conditions for reducing inequalities and promoting children’s developmental potential, the rights to health and nutrition (Article 24), education (Articles 28 and 29), and articles ensuring that those rights are realized without discrimination of gender, ethnicity, and disability. It is therefore clear that a rights-based approach (i.e., one that considers the individual and collective human rights) is highly needed when studying the response to a global health emergency such as the COVID-19 pandemic [11]. The International Classification of Functionality, Disability and Health (ICF) [12] offers a dimensional model, well-suited to document the functional characteristics of the child, the environment where the child lives, plays, learns, and grows, and child-environment interactions. Hence, the ICF helps understand the impact of the pandemic – which affects many environmental factors – on the lives of children with disabilities.
The overarching purpose of the Global COVID-19 Childhood Disability Data Coordination project was to synthesize existing evidence derived from surveys conducted across the globe.
The guiding research question that was sought to answer was “What is the short-/medium-/long-term global impact of the COVID-19 crisis on physical health, mental health, participation, education, and financial status of children and adults with disabilities and their families?”.
The specific objectives were: 1) to facilitate knowledge sharing about the impact of COVID-19 on disability globally - based on survey data; 2) to identify key findings and gaps in knowledge based on content analysis of the surveys, by using the CRC and ICF frameworks and finally, 3) to describe lessons learned and highlight useful strategies for future health emergencies.
2Methods
2.1Study team
A descriptive environmental scan of surveys was conducted. The multicultural, international, and interdisciplinary Survey subgroup consisted of representatives of seven academies of childhood disabilities as follows: American Academy for Cerebral Palsy and Developmental Medicine (AACPDM), European Academy of Childhood Disability (EACD), Australasian Academy of Cerebral Palsy and Developmental Medicine (AusACPDM), Southern African Academy of Childhood Disability (SA-ChilD), Latin American Academy of Child Development and Disability (ALDID), Eastern African Academy of Childhood Disability (EAACD), and the Chinese Academy of Childhood Disability. The study team consisted of seven professionals and one trainee working in the field of childhood disability. Four members have medical backgrounds (two developmental pediatricians and two pediatricians), and four have physical and/or occupational therapy backgrounds. Five members conduct clinical and research activities, one is fully dedicated to research, the remaining two are clinicians. In addition, the team collaborated with people with disabilities and disability organizations in different countries to disseminate the initiative.
2.2Multi-step process: Quantitative and qualitative approaches
Overall, the purpose of this international initiative was to facilitate accessing and sharing information collected by surveys addressing the impact of COVID-19 on people experiencing a disability globally. Specifically, surveys were sought asking their respondents – individuals with a disability, caregivers, and/or professionals - to report directly on their own thoughts, feelings, and behaviours regarding the impact of COVID-19.
To answer the guiding research question, a mixed method study design was used, combining qualitative and quantitative research components [13]. The purpose of this sequential design was to complement the results from one method with the results from the other method. Overall, the theoretical drive was exploration-and-description, where the core component was the qualitative thematic analysis [14], and the quantitative component was supplemental.
A multi-step process was followed. Firstly, an inventory was started of surveys either under development, launched and in process, or already completed worldwide related to the impact of COVID-19 on people living with a disability and their families. Members of all the academies who collaborated with the IAACD were engaged to invite their members to share information regarding ongoing or completed surveys. To consider a survey for inclusion, a survey data collection form was posted on the IAACD COVID-19 Task Force website and survey developers were asked to complete the form. In this form (available as supplemental material S1), survey developers provided information such as the purpose and content of the surveys, a link to published results, and/or described ongoing or key findings. This call for surveys was disseminated using email distribution lists, social networking channels, and academic letters in different languages, including English, Spanish, Portuguese, and Chinese (Global COVID-19 Childhood Disability Data Coordination – IAACD). The collaboration of all Communication Committees of each participating academy was also sought to disseminate this initiative. Additionally, disability organizations in different countries were contacted, as well as the International Alliance of Disability and shared the call for surveys. Surveys that were not related to COVID-19 and disability were excluded. Surveys were collected from June 15th, 2020, to November 30th, 2020.
As surveys considered in this project were publicly available data, the study did not require Institutional Review Board review.
Secondly, to facilitate access to ongoing results, an open access Surveys repository was created, where surveys were sorted into ongoing and completed. When available, final reports and key findings of completed surveys were posted.
Thirdly, the content of each final report and/or key findings of completed surveys were reviewed and compared. To identify common themes and gaps, the CRC [10] and the ICF [12] frameworks were used.
2.3Mapping exercise
A mixed method inductive/deductive thematic analysis was used. Theme development was directed by the content of the data, specifically, the thematic analysis. Mapping methodology included the following steps: 1) Inductive analysis: Identifying the main themes described in the key findings of the survey, 2) Inductive analysis: Assigning the CRC article that best describes the theme, and 3) Deductive analysis: Assigning the ICF component that best describes the theme.
As a practice trial, each member of the team completed an independent mapping exercise, which included applying the proposed steps to the same survey. Following this exercise, the methodology was revised to improve clarity and practicality of the identification of themes. Specifically, to facilitate the identification of themes included in step 1, three raters (VS, AC, IS) identified from reading the full material a core list of themes that the remaining group members used as a guideline for their mapping exercise. This step was necessary to facilitate reliability. However, if raters identified additional themes based on their assigned reports, they could add those themes to the proposed core list of themes. In the mapping exercise, raters’ agreement against a the most experienced coder (VS) ranged from 66% to 93% for CRC items and from 87% to 100% for ICF. Disagreements were resolved by consensus during virtual working group meetings. Overall, the content of each survey was mapped out by two coders. The group meetings were also used for discussions about the meaning of the results, identification of gaps, and future directions.
Lastly, an essential part of the project was continuous dissemination of results. The Surveys page was updated on a weekly basis. Furthermore, monthly ‘Flash News’ were created, highlighting findings of completed surveys as well as promoting participation in ongoing surveys. (Supplemental Material S1)
3Results
In this section, the presentation of the results are organized based on the objectives as follows:
3.1Objective 1 to facilitate knowledge sharing about the impact of COVID-19 on disability globally - based on surveys data
From June to November 2020, the task force coordinated the participation and sharing of information collected using surveys around the world. Forty-nine surveys describing the impact of COVID-19 on people living with disabilities were identified. The completed surveys gathered information from 17,230 participants representing all continents. Detailed information about the distribution of respondents by regions of the world can be accessed in Supplemental Material S1. Table 1 shows the general characteristics of ongoing and completed surveys. Of note, only the content of 25 out of 49 surveys were created with active collaboration of people with disabilities.
Table 1
Summary of characteristics of ongoing and completed surveys (all collected surveys, n = 49)
| Countries where surveys data were collected (n, %) | |
| Argentina (n = 3, 6.12%) | |
| Australia (n = 5, 10.20%) | |
| Brazil (n = 4, 8.16%) | |
| Canada (n = 7, 14.29%) | |
| Chile (n = 1, 2.04%) | |
| China (n = 3, 6.12%) | |
| English speaking countries* (n = 1, 2.04%) | |
| European countries (n = 1, 2.04%) | |
| France (n = 2, 4.08%) | |
| Global (n = 6, 12.24%) | |
| India (n = 1, 2.04%) | |
| Kenya (n = 1, 2.04%) | |
| Mexico (n = 1, 2.04%) | |
| New Zealand (n = 1, 2.04%) | |
| Portugal (n = 1, 2.04%) | |
| Scotland (n = 1, 2.04%) | |
| South Africa (n = 3, 6.12%) | |
| Spain (n = 1, 2.04%) | |
| The Netherland (n = 1, 2.04%) | |
| United Kingdom (n = 3, 6.12%) | |
| United States of America (n = 3, 6.12%) | |
| Language (n, %) | Chinese (n = 3, 6.12%) |
| Dutch (n = 1, 2.04%) | |
| English (n = 29, 59.18%) | |
| French (n = 6, 12.24%) | |
| Portuguese (n = 5, 10.20%) | |
| Spanish (n = 7, 14.29%) | |
| Swahili (n = 1, 2.04%) | |
| Multiple languages (n = 3, 6.12%) | |
| Population of interest (%) | Children with disabilities (n = 26, 53.06%) |
| Youth with disabilities (n = 23, 46.94%) | |
| Adults with disabilities (n = 17, 34.69%) | |
| Carer of children and/or adults with disabilities (n = 34, 69.39 %) | |
| Professionals (n = 15, 30.61 %) | |
| Other (n = 6, 12.24 %) | |
| Survey developed in collaboration with people with disabilities (n, %) | Yes (n = 25, 51.02%) |
| No (n = 23, 46.94%) | |
| Unknown (n = 1, 2.04%) |
*As reported by surveys. #Only 1 survey collected self-report data.
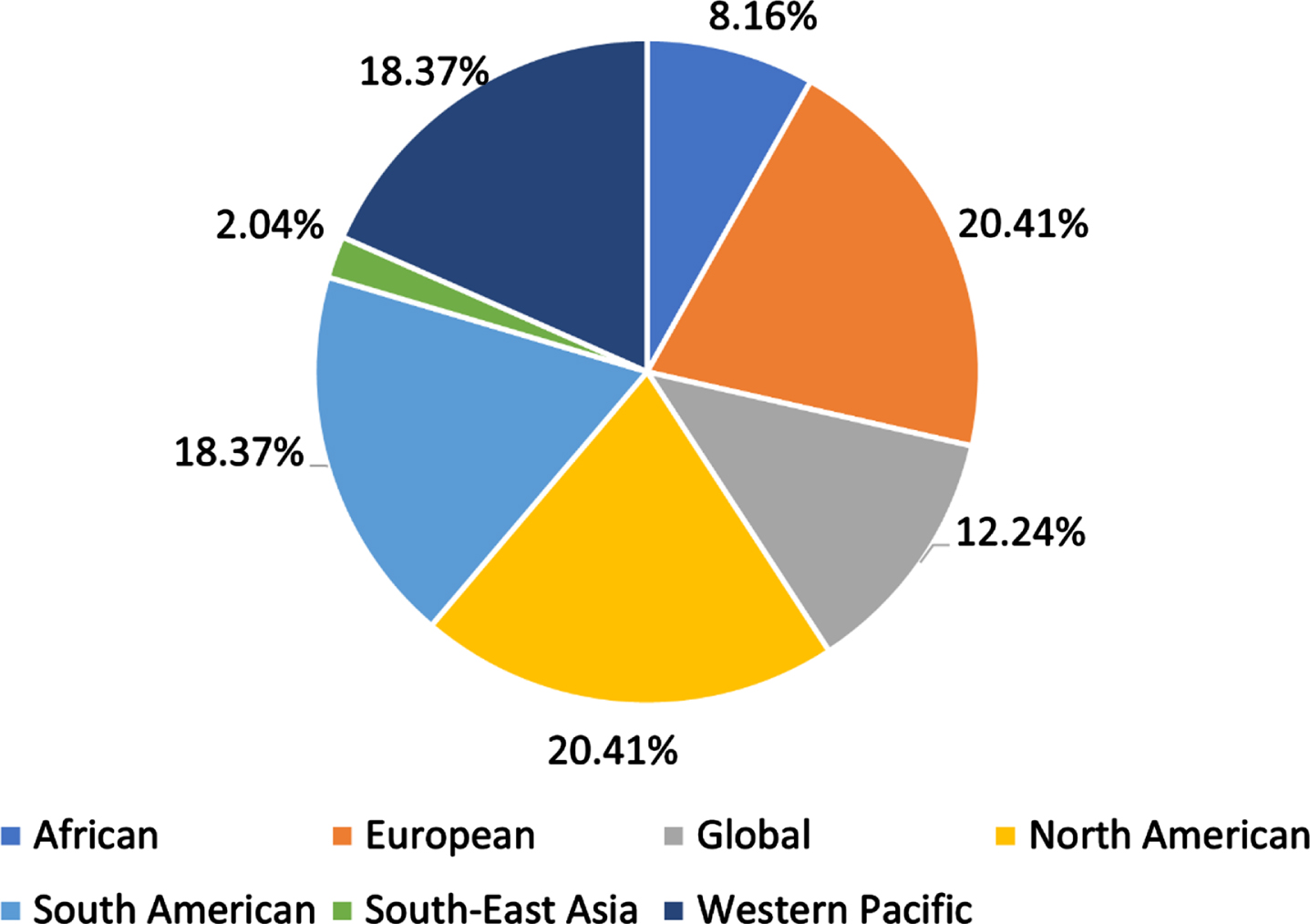
Figure 1 shows a representation of ongoing and completed surveys by regions of the world, as proposed by the WHO. Most surveys collected data representing The Americas, including North and South America, European, and Western-Pacific WHO’s health regions. The least represented WHO’s health regions were South-East Asian and African regions. Six of the 49 surveys addressed a global audience. Full distribution by country is shown in Table 1.
Fig. 1
Distribution of ongoing and completed surveys by world health regions.
The surveys varied in terms of target population, with the majority querying caregivers of people with disabilities and professionals working in rehabilitation settings. Caregivers were asked for opinions regarding the impact of COVID-19 on children and youth with disabilities. Healthcare professionals provided their views on aspects such as providing telehealth services (n = 2) and impact of the pandemic on rehabilitation services (n = 2), among others. Only one survey questioned the children directly in a pediatric sample of ages 7 to 10 years with and without disabilities. This was a survey from China with a focus on home programs for children with disabilities (Table 1).
Of the 49 surveys, 29 were constructed in English, followed by 7 in Spanish, 6 in French, 5 in Portuguese, and less than 3 in each of the following languages Chinese, Dutch, and Swahili. Three surveys were offered in multiple languages. (Table 1).
3.2Purpose and use of collected information
Surveys covered a great variety of purposes including describing and learning about the experience of lockdown due to COVID-19; impact on service provision; satisfaction with remote educational needs; satisfaction with remote support; documented lived experiences of caregivers; the impact of lockdown on children with autism spectrum disorder, brain injury, and/or cerebral palsy; perceived acceptability, effectiveness, and safety of telehealth services; professionals’ perception of delivering remote services, etc. A complete list describing aims and purpose of all surveys can be found on the Surveys subgroup page Global COVID-19 Childhood Disability Data Coordination – IAACD. Detailed information about the surveys can be accessed in Supplemental Material S1.
Regarding the intended use of the data collected, the answers were very broad. In general, survey developers reported variable uses such as: to inform future service provision, support policies, identify needs and priorities, compare impact of lockdown on overall well-being and mental health, identify barriers and facilitators of remote services, learn about COVID-19 response and reintegration of services, provide information for families and people with disabilities, improve response strategies, and inform governments and service providers.
3.3Objective 2 to identify key findings and gaps in knowledge based on content analysis of the surveys, by using the CRC and ICF frameworks
3.3.1Main themes and thematic categories
When reviewing the completed surveys (n = 24), on step 1 (inductive analysis) the core themes were identified and grouped in the following categories: accessibility of healthcare services, availability of healthcare services, family burden, satisfaction with remote services, continuity of care, access to information related to COVID-19, social isolation, special education, financial status, employment, participation, mental health, physical health, housing, personal values and experiences, communication, transportation, support, friendship, recreation, continued education, technology – accessibility of virtual platforms, and safety. Table 2 shows examples of core themes by category across surveys.
Table 2
Main themes retrieved from completed surveys, frequency, and examples
| Categories of themes | Number of surveys | Examples of themes mapped | Frequency themes in this category appeared* |
| COVID prevention | 1 | Access to protective personal equipment for themselves and/or carers; Access prevention measures to avoid exposure | 2 |
| Burden | 4 | Caregiver burden; Parents feel exhausted | 5 |
| Communication | 4 | Children’s communication negatively impacted | 4 |
| Education | 7 | Children’s learning negatively impacted; Low quality remote education; Disruption in special education; Parents concerned about return to school | 15 |
| Financial status | 7 | Financial pressure due to lockdown; Unemployment exacerbated | 8 |
| Friendship | 5 | Children’s friendships negatively impacted | 5 |
| Health services | 14 | Disruption in health services; Access to therapies, doctors, assessments and evaluations; Quality of health services | 27 |
| Home support | 6 | Disruption in home support for families; Lack of support from extended family and home support workers | 7 |
| Housing | 1 | Rent affordability; Home accommodations | 1 |
| Information | 7 | Need for information and guidance for disabled people; Need for information on accessing essential supplies and income; Better communication with agencies to learn about supports | 11 |
| Mental health | 13 | Declines in mental health; Behavioural problems | 22 |
| Participation | 2 | Disruption in recreational activities; Impact on participation and play | 2 |
| Personal values | 1 | Factors affecting intention to participate in virtual activities | 1 |
| Physical health | 7 | Declines in physical health of children as well as caregivers | 9 |
| Professionals | 3 | Professionals satisfaction and/or experiences delivering remote services; Reporting stress | 5 |
| Relationships | 3 | Positive family interactions; Positive aspects of lockdown – quality time with parents and getting to know children’s abilities | 4 |
| Remote support | 2 | Challenges and satisfaction with remote health services | 5 |
| Safety | 2 | Lack of resources to feel safe in the community; Consider safety when resuming research | 2 |
| Social isolation | 1 | Impact of social isolation; Family isolation | 2 |
| Stakeholders’ perspectives | 2 | Stakeholders’ perspectives on rehabilitation services | 1 |
| Stress | 5 | Children, parents/caregivers feel stressed out | 5 |
| Support | 7 | Inaccessibility or insufficiency of specific food and essential supplies; Flexibility from employers and schools to ensure extended family to provide support; Need for government support for people with disabilities | 16 |
| Technology | 2 | Access to assistive devices; Access to easy-to-use platforms for virtual visits | 2 |
* = Frequency of themes related to each category across all surveys. In some surveys, several themes related to a certain category were mapped.
As shown in Table 2, based on the distribution across surveys, the thematic categories that were most frequently included in the surveys were Health services (n = 14) and Mental health (n = 13), followed by Physical health, Information, Support, Education, and Financial status (n = 7 each). Values in brackets indicate how many surveys covered the core theme (note that one survey could mention several themes).
Following steps 2 and 3 on the methods, by deductive methods, all categories were matched to CRC and/or ICF components, except when not applicable, as shown on Table 3.
Table 3
Main categories of themes mapped to CRC articles and ICF components
| Categories mapped | CRC article | ICF components |
| COVID prevention | Article 24 | Environmental Factors – facilitator and barrier |
| Burden | Not applicable | Environmental Factors - barrier |
| Communication | Article 23 | Participation – restriction |
| Participation - facilitator | ||
| Education | Article 28 | Participation – restriction |
| Environmental Factors - facilitator and barrier | ||
| Financial status | Article 26 | Environmental Factors – facilitator and barrier |
| Friendship | Article 23 | Participation – restriction |
| Participation – facilitator | ||
| Health services | Article 24 | Environmental Factors - barrier |
| Home support | Article 24 | Environmental factors - barrier |
| Housing | Article 24 | Environmental factors - barrier |
| Information | Article 24 | Environmental Factors – facilitator and barrier |
| Article 26 | ||
| Mental Health | Not applicable | Body Function |
| Participation | Article 23 | Social Participation – virtual and in person |
| Article 31 | ||
| Personal values | Not applicable | Personal Factors |
| Physical health | Not applicable | Body Function |
| Professionals | Not applicable | Environmental Factors – barrier (professionals feel exhausted) |
| Relationship | Article 9 | Participation |
| Remote support | Not applicable | Personal Factors (satisfaction) |
| Safety | Article 26 | Environmental Factors – barrier |
| Social Isolation | Not applicable | Environmental Factors - barrier |
| Stakeholders’ perspectives | Not applicable | Personal Factors |
| Stress | Not applicable | Body Function |
| Support | Article 24 | Environmental Factors-barrier and facilitator |
| Article 23 | ||
| Article 26 | ||
| Technology | Article 24 | Environmental Factors – facilitator and barrier |
CRC: United Nations Convention on the Rights of the Child; ICF: International Classification of Functioning, Disability and Health.
3.3.2Mapping to articles of the CRC
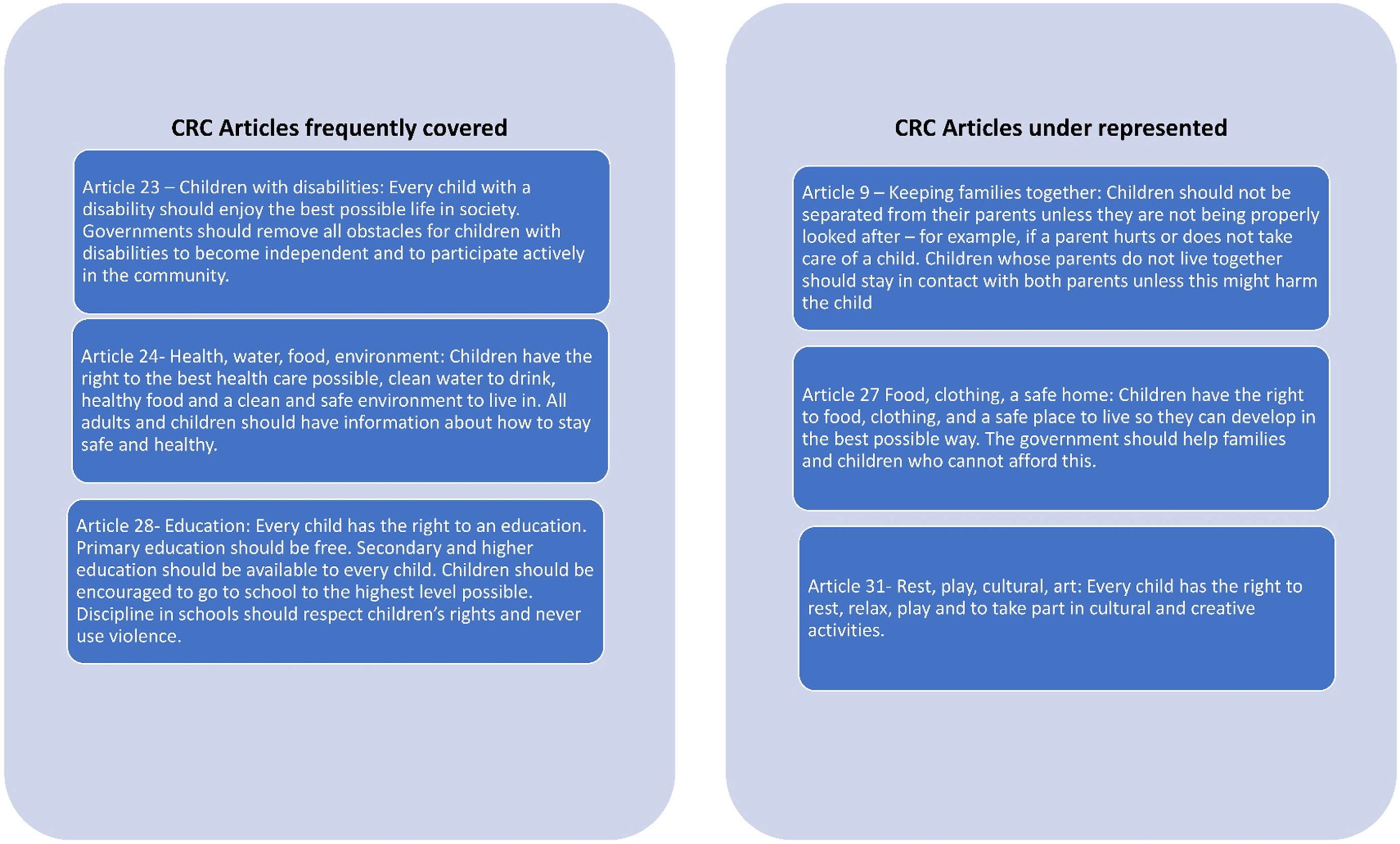
After identifying the themes represented by the findings of the surveys, a rights-based approach was used as a guiding framework to compare the themes with the content of the articles of the CRC. The articles frequently addressed were: Article 23- Children with disabilities have the right to actively participate in the community (n = 14), Article 24- All adults and children should have information about how to stay safe and healthy (n = 50). Article 26- Social and economic help (n = 12), and Article 28- Right to education (n = 12). Values in brackets indicate how many times a theme was related to this article (one survey could mention several themes). A few surveys covered the following CRC articles: Article 31- Right to participate in recreational activities (n = 3), Article 9- Keeping families together (n = 1), and Article 27- Food, clothing, and safe home (n = 1). Figure 2 highlights the description and frequency of distribution of these CRC articles. Specific themes that were not possible to map into CRC articles included: stakeholders’ perspectives, parents’ concerns, and professional education.
Fig. 2
Description of CRC articles covered by the surveys. CRC: United Nations Convention on the Rights of the Child.
3.3.3Mapping to ICF
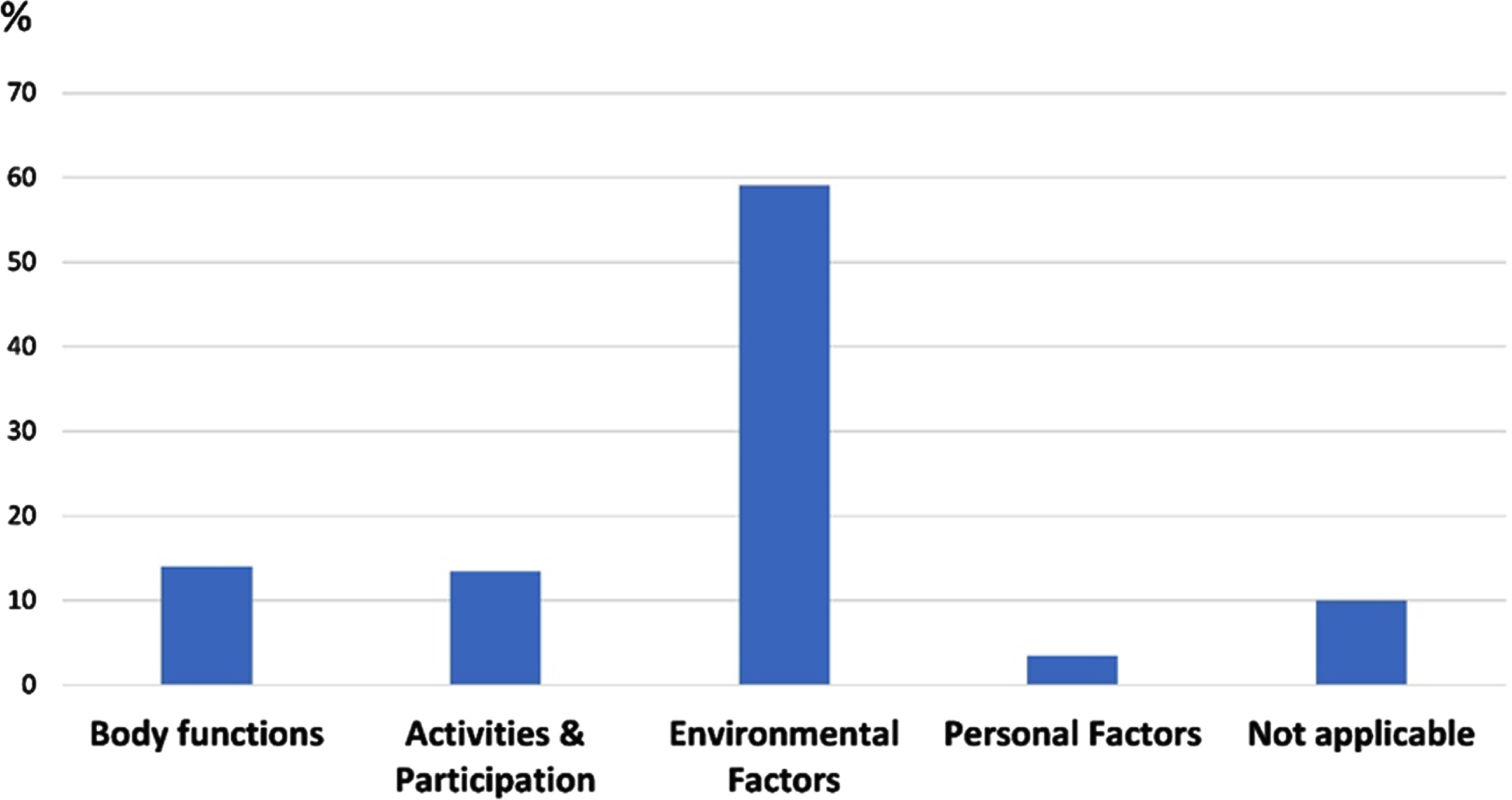
The themes were also mapped to the ICF components. Using a bio-psychosocial approach, the ICF components that were frequently addressed were: Body functions related to decline in mental health and physical fitness (n = 24 times themes were mapped into this component), Participation related to restrictions in socialization, recreation, education, and family interactions (n = 23), Environmental Factors described both as barriers and facilitators such as access and availability of health services, family support, financial support, caregivers’ health/stress/burden, access to technology, access and availability of special education, access to specific food and essential supplies (n = 101). Personal factors were represented by themes related to personal values, beliefs, and expectations (n = 7). Table 3 shows examples of themes mapped to the CRC and ICF. Figure 3 illustrates the distribution of themes by ICF components, showing that most themes covered by the surveys represented environmental factors (59% of total). Specific themes not matching any ICF component included professionals’ experiences with telehealth, overall physical health, and overall quality of life, among others, were coded as not covered by the ICF and/or non-applicable (n = 17).
Fig. 3
Distribution of themes covered by surveys representing ICF components. Footnote Figure 3: ICF; International Classification of Functioning, Disability and Health.
3.4Gaps in representation of CRC articles and ICF components
Based on their mapping frequency and/or identification by the study group, the following articles of the CRC and domains of the ICF were identified as content gaps: Article 2 – No discrimination, Article 12 – Respect for children’s views, and Article 19 – Protection from violence. In addition, some ICF domains related to Participation and Environmental factors were underrepresented by the surveys, as follows: lack of themes related to impact of lockdown on immediate family members beyond parents/carers (e.g., siblings); active involvement of people with disabilities or family members in planning and participating in inclusive emergency response; preferences regarding communication or sharing of information regarding COVID-19; challenges using digital information to express their needs; social attitudes and support from immediate community members (e.g., neighbours); affordability of medications; accessibility of emergency centers (e.g., discrimination).
3.5Objective 3 to describe lessons learned and highlight useful strategies for future health emergencies
3.5.1Positive changes and successful strategies
The results have also indicated positive aspects during the pandemic, such as: with remote health services and remote educational programs (n = 6 surveys), improved family interactions or support (n = 3), and child functioning (n = 2).
Importantly, the data from some surveys describe that the lockdown also brought creativity and new ideas and successful strategies. For example, rehabilitation professionals have been offering alternative methods of service provision, including remote consultations via video/phone/email, up to the development of collaborative home-based programs provided by caregivers. These creative ideas might further support parental empowerment and involvement in the habilitation and rehabilitation process in the future [15].
4Discussion
The Global COVID-19 Childhood Disability Data Coordination project identified that there are common needs and experiences reported by people living with disabilities and their families globally. From the early months of the COVID-19 pandemic, collaborative efforts ensured continuity of care. However, findings from the completed surveys highlight several challenges in the access to health services.
Some professionals and caregivers have reported that it was not possible to provide adequate rehabilitation and/or habilitation treatments to their patients, as virtual service provision does not replace assessments and/or interventions requiring in-person interactions and/or physical contact. These findings point to large variations in the quality of services around the world, which calls for continuing actions towards diminishing inequalities in access to health, as this represents violation of a fundamental right (Article 24).
The challenges in health service provision are presumably related to the frequent reports on the impact on the mental and physical health of individuals with disabilities and their families found in this study. Social isolation during the pandemic may be another factor negatively impacting children, possibly leading to anxiety and depression in children and adolescents [5], and potentially affecting those with previous vulnerabilities more critically [16, 17]. In addition to all the previously mentioned factors, increased sedentary behavior may further contribute to physical and mental health issues, thus affecting the health of children in a complex manner [18, 19].
Furthermore, the findings describe the immense burden being placed on families and caregivers of people with disabilities, due to several factors, for example: disruption in additional home/school support, impact on caregivers’ mental health - feelings of fear, frustration, stress, and anxiety. Plus some parents had to learn how to perform therapy at home. Financial challenges are another source of family stress that should be subject to appropriate measures that assure basic needs are met.
The access of children with disabilities to education has also been severely affected by the pandemic. Families reported concerns with safety - in terms of health protection - when going back to school. Additionally, families described several challenges related to the quality of special education services during the pandemic, including lack of support and information. Another possible source of rights violation resides in the fact that in vulnerable settings, schools provide food safety and protection against violence. In addition, the findings of negative impacts on learning, communication, and friendship suggest that not only during the pandemic, actions are needed to provide adequate support, but also after COVID-19 restrictions end, attention should be given to the gaps in education caused by this context [8, 20, 21].
Another concerning theme was related to lack of accessible information. Families and people with disabilities reported confusion over the appropriate safety protocols during COVID-19. This is a modifiable barrier that should be addressed in future health emergencies, for example, ensuring accessible information by including braille, sign language, and easy-to-read materials in different languages globally.
Overall, increased parental involvement/empowerment was reported, along with increased recognition of the importance of parents and caregivers in the planning and treatment process. Finally, people with disabilities, caregivers, and professionals reported that access to technology and technological skills were essential to maintain communication with care teams and reduce social isolation. On the other hand, this finding raises concerns about service provision to families who do not have access to technologies.
4.1Importance of ongoing international collaboration
This project created an open-access platform summarizing meaningful information and connecting colleagues and families from different regions of the world. By creating a repository of ongoing and completed surveys and comparing the survey content, collaboration and coordination of useful information among professionals and individuals with disabilities and their families around the world was enhanced. This initiative was expected to advocate for support for accessing up-to-date information during health emergencies, and conducting and sharing survey studies for the benefit of people with disability globally.
The monthly ‘Flash News’ highlighted common themes identified by the surveys, encouraging colleagues to avoid duplications of efforts by asking the same questions and pointing out gaps in knowledge or methodological weakness. For example, 51% of the surveys were designed with active collaboration of people with disabilities or their families. This shows the need for improvement in the design of surveys, as end-users should participate in the development of questionnaire-collecting information about their experiences, needs, and everyday life. In addition, only one survey collected information directly from children with disabilities. Participatory research models have received increased support in the past few years as they improve the relevance and impact of the results [22]. Thus, it is hoped that more surveys in the future will address children’s opinions by asking children with disability to report on their experiences in a child-friendly manner.
4.2Lessons learned
By comparing the main themes covered by the surveys to the CRC and the ICF, commonalities and gaps in key areas impacting children’s rights and everyday functioning of people with disabilities were identified. Regarding the impact of the pandemic, by mapping the themes to the ICF components, it was identified that the pandemic has impacted functioning across the body functions and participation domains; modifiable environmental barriers and facilitators were relevant in many surveys. Environmental factors have been a major focus of attention, perhaps because of the dramatic changes in people’s lives due to lockdown and social distancing and to concerns raised regarding the impact of these measures in many groups and areas of functioning, especially for those with disabilities [5, 18, 19]. Nevertheless, some contextual aspects have been overlooked, particularly impact on family members other than main caregiver, preferences, attitudes, and supports. Future work should consider addressing the environment more broadly.
Under the CRC framework, several surveys collected information related to many rights of children with and without disabilities, including access to health, education, and social and economic help, which seem to be the more obviously affected areas during the COVID-19 crisis. However, there were some areas that were overlooked, including discrimination, recreation, respect for children’s views, and access to child-friendly information related to COVID-19 and how to stay safe. These are areas that future surveys or initiatives should consider. During a health crisis, the human rights of people with disabilities, specifically children and youths, are impacted [11, 23– 25]. Hence, it is important to adopt a rights-based approach to represent the areas that are frequently affected, and most importantly, those that are overlooked.
4.3Call for actions
Based on the analysis of the frequency of themes and their respective ICF components and CRC articles, it was noted several points where the surveys helped identify a set of actions needed to remediate the impact of COVID-19. For example, need for: accessible information and guidance for disabled people; flexibility and understanding during the transition back to school; flexibility from employers and schools to ensure extended family can provide support; information on accessing essential supplies; and flexibility in lockdown rules to allow support from extended family. Addressing these points would be important to inform policymakers in the future months when further surges of COVID-19 are anticipated.
4.4Positive experiences and positive changes
Many surveys collected positive experiences during the pandemic, such as, satisfaction with remote health services and remote educational programs. Children and families enjoyed spending more quality time together. Parents/caregivers appreciated their children’s abilities as they spent more time together, Some children showed a decrease levels of anxiety and behavioural problems. The use of technology facilitated connections between families and healthcare professionals providing positive support. In consonance with these positive findings, the literature has highlighted the opportunities revealed during the pandemic for professionals working with childhood disability to embrace a more family-centered approach [26], which may be a beneficial legacy from these challenging times.
4.5Limitations
It is important to acknowledge that there may be methodological challenges when mapping content of surveys that have been created for various purposes, such as different sampling strategies, response bias, timing of data collection - different phases of the pandemic in their contexts, etc. It is not possible to know which actions were taken in each area of the globe, so variations in response to the pandemic may therefore account for variability in the results. Another limitation is that, due to underrepresentation of world regions, the content analysis might not represent the needs and the impact of COVID-19 in certain regions, such as South East Asia and Africa. In addition, no data were collected on the methodological quality of the surveys, as the intention was to raise information rapidly to inform future actions. However, there are many benefits of facilitating data coordination and global collaboration, including avoiding duplication of efforts, maximizing resources, rapid dissemination of successful strategies, and planning for future phases of data collection.
5Conclusion
The findings from this study provided evidence that COVID-19 has negatively impacted several areas of functioning, overall well-being, and rights of people with disabilities and their families worldwide. Impact on mental health of people with disabilities, caregivers, and professionals continues to be a major issue globally, requiring immediate actions to mitigate the impact of COVID-19 measures and social restrictions.
In-person rehabilitation and habilitation services have been greatly impacted due to public health restrictions. However, the use of technology has facilitated alternative methods of service provision, and evidence of its effectiveness will need to be assessed in the aftermath of COVID-19. Inclusive responses to COVID-19 are crucial to ensure autonomy, respect, and to support independent living during the current global health emergency. Inclusive responses could be achieved by including people with disabilities – children, youths, and adults – in the planning stages and decision-making of emergency responses, particularly by collecting ongoing information directly from their perspectives during global health emergencies.
Acknowledgments
We would like to express our gratitude to all the developers and participants of the surveys for their contribution to our understanding of the ongoing impact of COVID-19. Special thanks to Danijela Grahovac who oversaw the design of the COVID-19 IAACD TASK FORCE website, generating and revising the web pages to facilitate rapid flow of information. In addition, we want to thank our colleagues from the Australasian Academy of Cerebral Palsy and Developmental Medicine for participating in some steps of the mapping exercise, special thanks to Christine Immis, Michelle Elmitt, and David Hobbs.
Conflict of interest
The authors have no conflicts of interest to declare. This project received no external funding.
Supplementary material
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/PRM-220035.
References
[1] | Dhiman S , Sahu PK , Reed WR , Ganesh GS , Goyal RK , Jain S . Impact of COVID-19 outbreak on mental health and perceived strain among caregivers tending children with special needs. Res Dev Disabil. (2020) ;107: :103790. doi: 10.1016/j.ridd.2020.103790 |
[2] | Grumi S , Provenzi L , Gardani A , et al. Engaging with Families through On-line Rehabilitation for Children during the Emergency (EnFORCE) Group. Rehabilitation services lockdown during the COVID-19 emergency: The mental health response of caregivers of children with neurodevelopmental disabilities. Disabil Rehabil. (2020) ;43: (1):27–32. doi: 10.1080/09638288.2020.1842520 |
[3] | Houtrow A , Harris D , Molinero A , Levin-Decanini T , Robichaud C . Children with disabilities in the United States and the COVID-19 pandemic. J Pediatr Rehabil Med. (2020) ;13: (3):415–24. doi: 10.3233/PRM-200769 |
[4] | Jiao WY , Wang LN , Liu J , et al. Behavioral and emotional disorders in children during the COVID-19 epidemic. J Pediatr. (2020) ;221: :264–6.e1. doi: 10.1016/j.jpeds.2020.03.013 |
[5] | Loades ME , Chatburn E , Higson-Sweeney N , et al. Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. (2020) ;59: (11):1218–39.e3. doi: 10.1016/j.jaac.2020.05.009 |
[6] | Askitas N , Tatsiramos K , Verheyden B . Lockdown strategies, mobility patterns and covid-19. CESifo Working Paper No. 8338. SSRN; 2020. Available from: https://ssrn.com/abstract=3619687 |
[7] | Lee J . Mental health effects of school closures during COVID-19. Lancet Child Adolesc Health. (2020) ;4: (6):421s. doi: 10.1016/S2352-4642(20)30109-7 |
[8] | Van Lancker W , Parolin Z . COVID-19, school closures, and child poverty: A social crisis in the making. Lancet Public Health. (2020) ;5: (5):e243–e244. doi: 10.1016/S2468-2667(20)30084-0 |
[9] | World Health Organization. Coronavirus disease 2019 (COVID-19): Situation report, 77. World Health Organization; 2020. |
[10] | UN General Assembly. Convention on the Rights of the Child. United Nations, Treaty Series, vol. 1577, p. 3. United Nations; 1989. Available from: https://www.refworld.org/docid/3ae6b38f0.html |
[11] | Schiariti V . The human rights of children with disabilities during health emergencies: The challenge of COVID-19. Dev Med Child Neurol. (2020) ;62: (6):661. doi: 10.1111/dmcn.14526 |
[12] | World Health Organization. International Classification of Functioning, Disability and Health. Geneva: Worth Health Organization; (2001) . |
[13] | Schoonenboom J , Johnson RB . How to construct a mixed methods research design. Kolner Z Soz Sozpsychol. (2017) ;69: (Suppl 2):107–31. doi: 10.1007/s11577-017-0454-1 |
[14] | Braun V , Clarke V . Using thematic analysis in psychology. Qual Res Psych. (2006) ;3: (2):77–101. doi: 10.1191/1478088706qp063oa |
[15] | Schiariti V , McWilliam RA . Crisis brings innovative strategies: Collaborative empathic teleintervention for children with disabilities during the COVID-19 lockdown. Int J Environ Res Public Health. (2021) ;18: (4):1749. doi: 10.3390/ijerph18041749 |
[16] | Araújo LA , Veloso CF , Souza MC , Azevedo JMC , Tarro G . The potential impact of the COVID-19 pandemic on child growth and development: A systematic review. J Pediatr (Rio J). (2021) ;97: (4):369–77. doi: 10.1016/j.jped.2020.08.008 |
[17] | Patel K . Mental health implications of COVID-19 on children with disabilities. Asian J Psychiatr. (2020) ;54: :102273. doi: 10.1016/j.ajp.2020.102273 |
[18] | Bates LC , Zieff G , Stanford K , et al. COVID-19 impact on behaviors across the 24-hour day in children and adolescents: Physical activity, sedentary behavior, and sleep. Children (Basel). (2020) ;7: (9):138. doi: 10.3390/children7090138 |
[19] | Longo E , de Campos AC , Schiariti V . COVID-19 pandemic: Is this a good time for implementation of home programs for children’s rehabilitation in low- and middle-income countries? Phys Occup Ther Pediatr. (2020) ;40: (4):361–4. doi: 10.1080/01942638.2020.1759947 |
[20] | Sholas MG , Apkon SD , Houtrow AJ . Children with disabilities must be more than an afterthought in school reopening. JAMA Pediatr. (2021) ;175: (4):423–4. doi: 10.1001/jamapediatrics.2020.5308 |
[21] | Meyerowitz EA , Vannier AGL , Friesen MGN , et al. Rethinking the role of hydroxychloroquine in the treatment of COVID-19. FASEB J. (2020) ;34: (5):6027–37. doi: 10.1096/fj.202000919 |
[22] | Smits DW , van Meeteren K , Klem M , Alsem M , Ketelaar M . Designing a tool to support patient and public involvement in research projects: The Involvement Matrix. Res Involv Engagem. (2020) ;6: (1):1–7. doi: 10.1186/s40900-020-00188-4 |
[23] | The State of the World’s Children 2013. Children with disabilities. UNICEF; 2013 [cited 4 February 2020]. Available from: https://www.unicef.org/sowc2013/files/SWCR2013_ENG_Lo_res_24_Apr_2013.pdf |
[24] | Disability-Inclusive Disaster Risk Reduction and Emergency Situations. UN Department of Economic and Social Affairs; 2013 [cited 30 March 2020]. Available from: https://www.un.org/development/desa/disabilities/issues/disability-inclusive-disaster-risk-reduction-and-emergency-situations.html |
[25] | World Report on Disability: Summary. UN World Health Organization (WHO); 2011 [cited 6 February 2020]. Available from: https://www.refworld.org/docid/50854a322.html |
[26] | Rosenbaum PL , Silva M , Camden C . Let’s not go back to ‘normal’! Lessons from COVID-19 for professionals working in childhood disability. Disabil Rehabil. (2021) ;43: (7):1022–8. doi: 10.1080/09638288.2020.1862925 |


