
First year impacts of the COVID-19 pandemic on pediatric physiatrists
Abstract
PURPOSE:
The objective of this study was to determine how the COVID-19 pandemic impacted the work and compensation of pediatric physiatrists during the first year of the pandemic.
METHODS:
Pediatric physiatrists were surveyed in the spring of 2021 about how the first year of the COVID-19 pandemic impacted their practices as a part of a larger survey examining pediatric rehabilitation medicine practices. The COVID-19 specific questions covered three topic areas: 1) personal experiences with COVID-19; 2) occupational workflow changes due to COVID-19, including telehealth; and 3) employment consequences of the COVID-19 pandemic.
RESULTS:
Thirteen of 259 pediatric physiatrists reported having a COVID-19 infection, of whom none required hospitalization. Nearly all (96.5%) of pediatric physiatrists reported using telehealth during the pandemic compared to 14% prior to the pandemic. They reported numerous changes to their clinical operations, and 50% reported not having adequate personal protective equipment available for themselves or their staff all of the time. Fifteen pediatric physiatrists (5.9%) reported being furloughed, and three reported job loss during the first year of the pandemic.
CONCLUSION:
While only a small percentage of pediatric physiatrists contracted COVID-19 during the first year of the pandemic, nearly all experienced workflow changes.
1Introduction
When the COVID-19 pandemic began in March of 2020 and most hospital systems and practices were relegated to providing only essential care, physiatrists were often deployed to offload or replace colleagues from other medical disciplines [1]. Physiatrists also implemented the role of telehealth into their practices [2]. Like other physicians, physiatrists are considered to be at higher risk of getting COVID-19 due to the likelihood of workplace exposures, but little data exists to determine the incidence of COVID-19 among practicing physicians. Although literature exists regarding the importance of physiatry in the rehabilitation of patients after SARS-CoV-2 infection and “ long COVID,” fewer studies examine the impact of COVID-19 on physiatrists and their practices and none conducted specifically on pediatric physiatrists [3–8]. The objectives of this study were to provide a nationally representative count of the number of pediatric physiatrists diagnosed with COVID-19 and determine how the pandemic impacted their work and compensation during the first year of the pandemic.
2Methods
Between March 18, 2021–June 30, 2021, all known United States-based pediatric rehabilitation medicine (PRM) physicians (N = 383) were surveyed via email. This email provided a link to a REDCap [9] survey about how the first year of the COVID-19 pandemic impacted their practices as a part of a larger survey examining PRM practices that was created by researchers with training in survey methodology and extensive experience surveying the field of PRM [10–14]. Prior to dissemination, three pediatric physiatrists-in-training read all of the questions for clarity to assure the questions were likely to be interpreted appropriately. The COVID-19 specific questions covered three topic areas: 1) personal experiences with COVID-19; 2) occupational workflow changes due to COVID-19, including telehealth; and 3) employment consequences of the COVID-19 pandemic (see Appendix 1). The survey also captured basic demographics and practice characteristics. Non-responses were case deleted and not included in the analysis. Descriptive statistics are presented, but when sample sizes were restrictively small, statistical comparisons were not generated. This study was approved by the University of Pittsburgh Institutional Review Board.
3Results
Of the 383 pediatric physiatrists who were invited to participate, 301 consented and participated with 259 continuing sequentially through the section pertaining to their experiences with COVID-19 (an 86% completion rate). The overall response rate for these analyses was 67.6%. Of the 259 who completed the survey, 76.7% reported never needing to quarantine due to a known or potential exposure to COVID-19, while 15.7% had to do so once and 7.6% more than once. Thirteen (5%) reported having a COVID-19 infection. Among those with a history of COVID-19, none required hospitalization resulting from infection. Those with a history of COVID-19 were on average (x = 50.7 years old, Standard Deviation [SD] = 11.8) similar to the sample in general (x = 47.0, SD = 11.2). Three (23.1%) of the 13 pediatric physiatrists with a history of COVID-19 reported having a disability in a survey population in which 8.5% were represented by persons self-identifying as having a disability; three (23.1%) identified as non-White or did not wish to disclose compared to 20.4% of the sample who identified as non-White; and six (46.2%) of those with a history of COVID-19 were men compared to 28.5% of the sample who identified as men (statistical comparisons not completed due to small sample sizes).
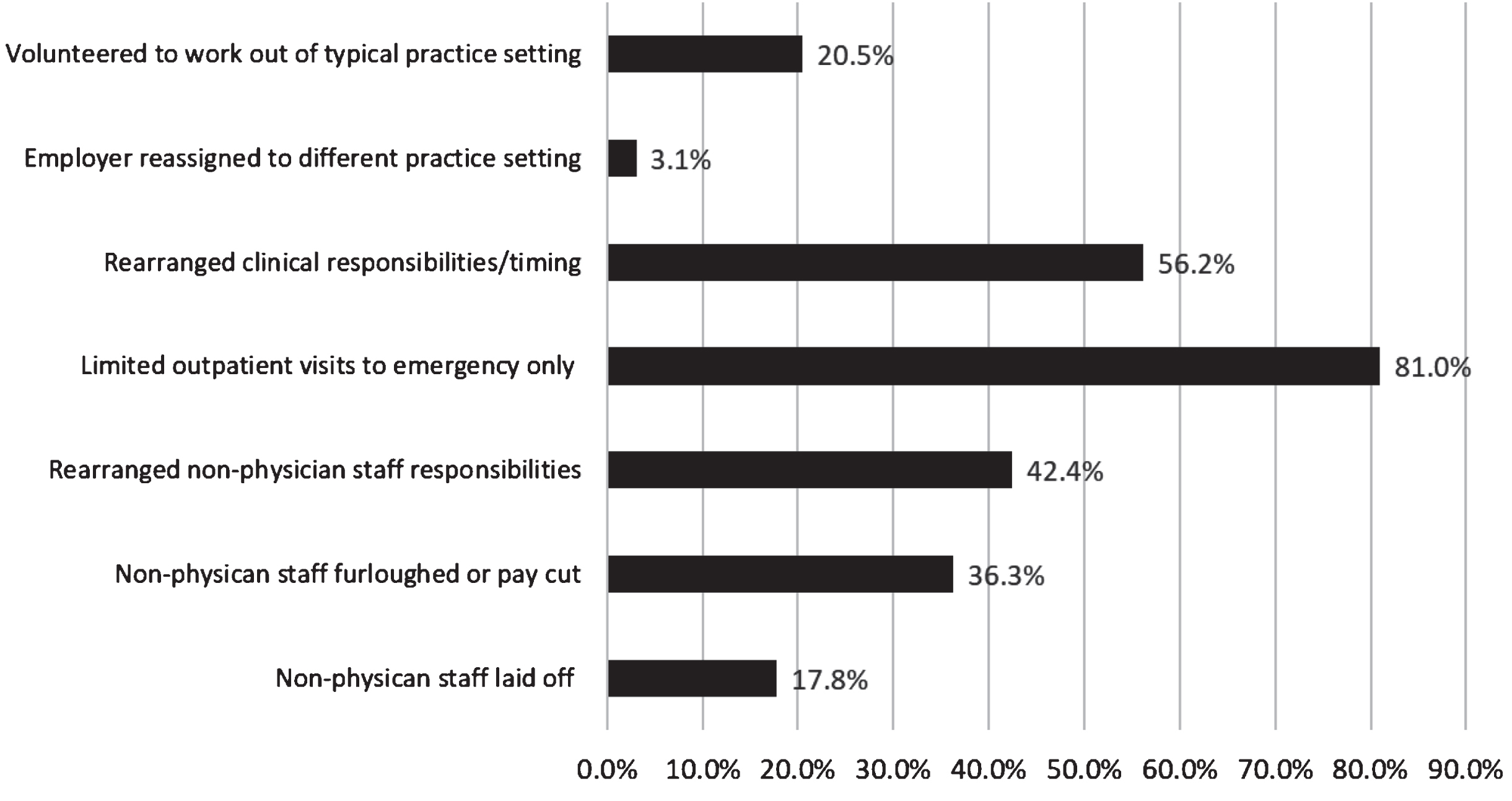
The impact on workflow varied among respondents. Nearly all (96.5%) of pediatric physiatrists reported using telehealth during the pandemic compared to 14% prior to the pandemic. Figure 1 shows that the types of services offered via telehealth varied, with single provider outpatient appointments being the most common. Pediatric physiatrists reported numerous changes to their clinical operations ranging in frequency from 3.1% being reassigned by their employer to a different practice to 81% reporting limiting outpatients to emergency visits only for a time during the pandemic (see Figure 2). Fifty percent reported not having adequate personal protective equipment available for themselves or their staff all of the time.
Fig. 1
Types of Telehealth Services Offered by Pediatric Physiatrists During the First Year of the COVID-19 Pandemic. *Total percentages exceed 100% as respondents could answer more than one type of telehealth service employed in their practice.
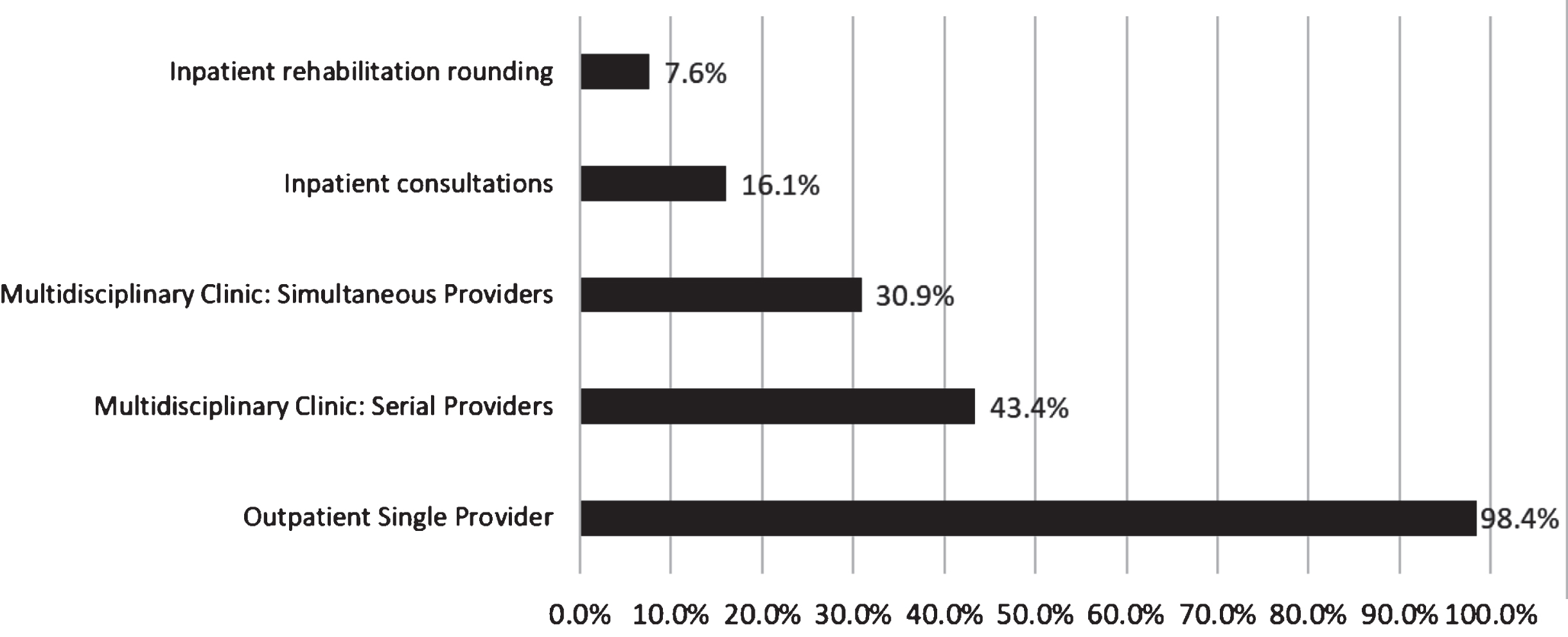
Fig. 2
Percentage of Pediatric Physiatrists Reporting Changes to Their Clinical Operations. *Total percentages add up to greater than 100% as respondents could answer more than one type of operational change impacting their practice, duties or salary.
Nearly all (93.1%) medical directors of comprehensive rehabilitation programs reported making changes to their treatment strategies for physical distancing including limiting the number of children in the treatment gym (93.1%), reducing or eliminating group therapies (58.6%), and/or reducing or eliminating co-treatments (31%). No medical directors reported providing therapies only in patient rooms or reducing therapy hours. Patients with an active COVID-19 infection could be admitted to inpatient rehabilitation by 24.1% of all respondents. Most (62.1%) medical directors reported all admitted patients were tested for COVID-19 prior to admission, while 27.6% reported only certain patients were tested and 10.3% reported no patient required testing before admission for inpatient rehabilitation.
Job loss was experienced by three (1.2%) of the surveyed pediatric physiatrists, and an additional 33 (12.9%) reported having missed out or potentially missing out on a job opportunity due to the pandemic, as shown in Table 1. Disability was over-represented among those who reported having missed or maybe having missed a job opportunity; 18.6% of those who reported having missed or maybe having missed a job opportunity indicated that they have a disability compared to only 7.7% of those without a missed job opportunity (p < 0.05). Fifteen pediatric physiatrists (5.9%) reported being furloughed during the first year of the pandemic. Twelve of them worked at academic health centers. Those who were furloughed had been in practice longer (19.3 years, SD = 11.0) than those who were not furloughed (12.9 years, SD = 10.1, p < 0.05). Pay cuts were more common than furloughs with 64 pediatric physiatrists (25.1%) reporting a pay cut due to the pandemic. Of those with a pay cut, 39.1% worked in non-academic university medical centers compared to 28.3% of those without a pay cut (p < 0.5). Among the 64 pediatric physiatrists with a pay cut, 53 (82.8%) had returned to their regular salaries by the time of the survey. Childcare was a problem for 27.8% with no statistical difference by gender, minoritized race or practice in an academic university medical center. Pediatric physiatrists with childcare challenges had fewer years in practice (9.2, SD = 6.3) than those without childcare challenges (14.9, SD = 11.0, p < 0.05).
Table 1
Compensation and workforce impacts of the COVID-19 pandemic
| Sample n, (%) | Women and gender minorities sample n, (%) | Minoritized race (non-white or did not disclose) sample n, (%) | Disclosed disability sample n, (%) | Average years in practice (Standard Deviation [SD]) | Not practicing at an academic university medical center | |
| Lost job | 3, (1.2%) | |||||
| Have or may have missed job opportunity | 33, (12.9%) | 22, (66.7%) | 10, (31.3%) | 6, (18.8%)* | 11.0 (SD = 9.3) | 6, (18.8%) |
| No missed job opportunity | 162, (73.0%) | 41, (18.6%) | 17, (7.7%) | 13.6 (SD = 10.3) | 75, (33.6%) | |
| Furloughed | 15, (5.9%) | 12, (75%) | 4, (26.7%) | 4, (26.7%) | 19.3 (SD = 11.0)* | 3, (20%) |
| Not Furloughed | 138, (72.6%) | – | –- | 12.9 (SD = 10.1) | – | |
| Pay cut | 64, (25.1%) | 46, (71.9%) | 11, (17.2%) | 5, (7.8%) | 14.2 (SD = 10.3) | 25, (39.1%)* |
| No pay cut | 139, (73.0%) | 41, (21.5%) | 17, (8.9%) | 12.9 (SD = 10.2) | 54, (28.3%) | |
| Childcare challenges | 72, (27.8%) | 51, (70.8%) | 14, (19.4%) | 3, (4.2%) | 9.2 (SD = 6.3)* | 17, (23.6%) |
| No challenges/no children | 175, (72.2%) | 38, (20.3%) | – | 14.9 (SD = 11.0) | 64, (34.2%) |
*p-value < 0.05 for distribution comparisons, –data withheld because statistical comparisons were not made.
4Discussion
This nationally representative study of the impacts of COVID-19 on pediatric physiatrists and their practices found that, while only a small percentage of pediatric physiatrists contracted COVID-19 during the first year of the pandemic, nearly everyone surveyed experienced workflow changes. Unfortunately, there was no reliable data about infection rates during the first year of the pandemic from other specialties to compare to pediatric physiatrists to determine if they were at higher or lower risk than other physicians. Additionally, there were insufficient data regarding regional variations for infection incidence, although pediatric physiatrists are over-represented in the Midwest region [11], which could indicate that they were at lower risk of COVID-19 because they were not disproportionately practicing in COVID-19 epicenters. The vast majority of pediatric physiatrists used telehealth and limited outpatient visits to emergencies for a time. The rates of telehealth use prior to and during the pandemic were similar to the rates found in a recently published smaller non-representative survey of pediatric physiatrists [6]. How telehealth is utilized long-term is yet to be determined, but many providers and patients find it a valuable adjunct to in-person visits [2, 6]. Due to the variable success and satisfaction with telehealth services for people with disabilities, pediatric physiatrists may consider how to equitably provide telehealth services and assure high quality [15, 16].
Job security in health care had been a major concern, especially early in the pandemic [17]. These analyses demonstrate that pediatric physiatrists were not immune to the financial shifts that occurred. While only three lost their jobs, over 10% reported that they missed out or potentially missed out on job opportunities. Those who missed out disproportionally reported disabilities. This finding may relate to the extensively acknowledged discrimination that people with disabilities experience generally in the workforce and specifically in hiring [18]. While under 10% were furloughed, those who were furloughed were older than those who were not. Pay cuts were common with a quarter of pediatric physiatrists reporting them. This is notably different than the 49% of physicians who noted this adverse economic impact in a national non-representative sample, although a direct comparison is not possible due to differences in how the questions were asked [19]. Working in an academic university medical center was associated with not having a pay cut (protective), a finding also noted by Long et al. [19]. Male gender was not associated with protection from a pay cut unlike in an analysis of pediatric cardiologists, the only comparable study [20]. Similarly, gender differences in childcare challenges were not reported, unlike in the analysis of pediatric cardiologists [20]. The reasons for these observed differences are unknown but worthy of future investigation because ample evidence indicates a differential burden between mothers and fathers [21–23]. As might be expected, there were differences in the average years in practice for those with and without childcare challenges such that those with childcare challenges were approximately five years younger and thus more likely to have children of an age needing childcare.
This survey was not without limitations and was not immune to bias. It did not achieve as high of a completion rate by eligible subjects compared to prior administrations of surveys of the field [11], which introduces the possibility of nonresponse bias and subsequent inaccurate conclusions. However, response rates above 50–60% are generally considered optimal because nonresponse bias is minimal [24]. Data about inpatient rehabilitation was gathered from medical directors of whom only 29 completed the section on COVID-19, limiting the generalizability of this data. Further, timing of when COVID-19 impacts occurred was not collected, and the potential of recall bias from self-report of one year of information is a limitation. Conversely, this survey captured information from only the first year of the pandemic. As the impacts on health care delivery evolve over time, additional research is warranted to identify how pediatric physiatry has changed and how pediatric physiatrists have been impacted.
5Conflict of interest
The authors have no conflicts of interest to report.
6Funding
The authors have no funding to report.
Appendices
Appendix 1: COVID-19 Survey Questions
| Question | Possible response |
| Have you tested positive for SARS-CoV-2/COVID-19? | Yes |
| No | |
| Did you require hospitalization? * | Yes |
| No | |
| Did you require ICU care? * | Yes |
| No | |
| Did you require mechanical ventilation? * | Yes |
| No | |
| Have you been quarantined due to exposure or potential exposure to SARS-CoV-2/COVID-19? | Yes, once |
| Yes, more than once | |
| No | |
| Have you volunteered to work as a physician outside of your typical practice setting (such as in the ED) during the SARS-CoV-2/COVID-19 pandemic? | Yes |
| No | |
| Has your employer reassigned you to work outside of your typical practice setting (such as in the ED) during the pandemic? | Yes |
| No | |
| Has your physician group rearranged clinical responsibilities (such as having you work two weeks in person and then two weeks remote) during the SARS-CoV-2/COVID-19 pandemic? | Yes |
| No | |
| At any time during the SARS-CoV-2/COVID-19 pandemic has your practice limited in-person outpatient visits to emergency only visits? | Yes |
| No | |
| Prior to the SARS-CoV-2/COVID-19 pandemic did you personally offer telehealth visits? | Yes |
| No | |
| During the SARS-CoV-2/COVID-19 pandemic have you personally offered telehealth visits? | Yes |
| No | |
| Which services are you offering via telehealth (check all that apply)? | Outpatient appointments as part of a multidisciplinary clinic in which patients are seen serially by providers of different disciplines |
| Outpatient appointments as part of a multidisciplinary clinic in which multiple providers of different disciplines see patients at the same time | |
| Outpatient appointments as a single provider | |
| Outpatient appointments as a single provider | |
| Rounding on rehabilitation patients as an attending | |
| Have you missed out on a job opportunity due to the SARS-CoV- 2/COVID-19 pandemic? | Yes |
| No | |
| I do not know | |
| Have you lost your job due to the SARS-CoV-2/COVID-19 pandemic? | Yes |
| No | |
| Have you experienced a pay-cut (reduced pay with the same hours) during the pandemic SARS-CoV-2/COVID-19 with no reduction in work expectations? | Yes |
| No | |
| Have you been furloughed (reduced pay and reduced hours) for any amount of time during the SARS-CoV-2/COVID-19 pandemic? | Yes |
| No | |
| Has your family experienced child care issues during the SARS-CoV- 2/COVID-19 pandemic? | Yes |
| No | |
| I have no children living at home | |
| As a result of the SARS-CoV-2/COVID-19 pandemic, have any non-physician staff in your practice been laid off? | Yes |
| No | |
| I do not know | |
| As a result of the SARS-CoV-2/COVID-19 pandemic, have any non-physician staff in your practice been furloughed or taken a pay cut? | Yes |
| No | |
| I do not know | |
| In your opinion, have you and your staff had adequate access to PPE? | All of the time |
| Most of the time | |
| Some of the time | |
| Rarely | |
| Never | |
| I do not know | |
| Do you admit patients with active SARS-CoV-2/COVID-19 infections to your rehabilitation program?** | Yes |
| No | |
| Prior to admission to your rehabilitation program, do you require testing for SARS-CoV-2/COVID-19?** | Yes for everyone |
| Yes for certain patients | |
| No | |
| To facilitate physical distancing, how has your program altered how therapies are provided (check all that apply)?** | We now provide therapy only in the patient’s room |
| We limit the number of patients in the gym at one time | |
| Reduced or eliminated group therapies | |
| Therapy hours per patient have been reduced | |
| Reduced or eliminated the number of co-treatments available | |
| No changes |
*Questions branched off of positive responses such that if a respondent said ‘No’ to having tested positive, they would not be asked about hospitalization. **Only asked of inpatient rehabilitation medical directors. ICU = intensive care unit, ED = emergency department.
Acknowledgments
The authors would like to thank Kristyn Felman for her assistance managing the dataset and Matt Haas, MD, Caitlin Chicoine, MD, and Jasmin Ng, MD, for reviewing the survey draft for clarity.
References
[1] | Weinstein SM . How COVID-19 informed the future impact of the specialty of physical medicine and rehabilitation across the health care continuum. PM R. (2021) ;13: (6):551–3. doi: 10.1002/pmrj.12620 |
[2] | Sukhov R , Asante A , Ilizarov G . Telemedicine for pediatric physiatry: How social distancing can bring physicians and families closer together. J Pediatr Rehabil Med. (2020) ;13: (3):329–38. doi: 10.3233/PRM-200747 |
[3] | Stein J , Visco CJ , Barbuto S . Rehabilitation Medicine Response to the COVID-19 Pandemic. Am J Phys Med Rehabil. (2020) ;99: (7):573–9. doi: 10.1097/PHM.0000000000001470 |
[4] | Negrini S , Arienti C , Iannicelli V , Lazzarini SG , Patrini M , Kiekens C . Importance for Our Field of the Newly Published Cochrane Special Collection on “Coronavirus (COVID-19): Evidence Relevant to Clinical Rehabilitation”. Am J Phys Med Rehabil. (2021) ;100: (2):110–1. doi: 10.1097/PHM.0000000000001638 |
[5] | Verduzco-Gutierrez M , Estores IM , Graf MJP , et al. Models of Care for Postacute COVID-19 Clinics: Experiences and a Practical Framework for Outpatient Physiatry Settings. Am J Phys Med Rehabil. (2021) ;100: (12):1133–9. doi: 10.1097/PHM.0000000000001892 |
[6] | Dietzen A , Ide W , Pavone L . Telehealth in pediatric rehabilitation medicine: A survey of clinician reported utilization and experience. J Pediatr Rehabil Med. (2020) ;13: (3):281–8. doi: 10.3233/PRM-200762 |
[7] | Escalon MX , Raum G , Tieppo Francio V , Eubanks JE , Verduzco-Gutierrez M . The Immediate Impact of the Coronavirus Pandemic and Resulting Adaptations in Physical Medicine and Rehabilitation Medical Education and Practice. PM R. (2020) ;12: (10):1015–23. doi: 10.1002/pmrj.12455 |
[8] | McLaughlin M . Safe and effective medication utilization in pediatric patients requiring rehabilitation services during the Coronavirus pandemic of 2019. J Pediatr Rehabil Med. (2020) ;13: (3):221–3. doi: 10.3233/PRM-200026 |
[9] | Harris PA , Taylor R , Thielke R , Payne J , Gonzalez N , Conde JG . Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) ;42: (2):377–81. doi: 10.1016/j.jbi.2008.08.010 |
[10] | Houtrow AJ , Pruitt DW , Zigler CK . Gender-Based Salary Inequities Among Pediatric Rehabilitation Medicine Physicians in the United States. Arch Phys Med Rehabil. (2020) ;101: (5):741–9. doi: 10.1016/j.apmr.2019.11.007 |
[11] | Houtrow AJ , Zigler CK , Pruitt DW . The State of the Field: Results from the 2014 and 2017 Pediatric Rehabilitation Medicine Practice Surveys. PM R. (2020) ;12: (2):168–79. doi: 10.1002/pmrj.12235 |
[12] | Paulson A , Zigler CK , Houtrow A , Pruitt D . Botulinum Toxin: Techniques Within Pediatric Physiatry. PM R. (2019) ;11: (1):38–44. doi: 10.1016/j.pmrj.2018.06.004 |
[13] | Pruitt DW , Zigler CK , Massagli TL , Houtrow AJ . Assessing the Field of Pediatric Rehabilitation Medicine’s Interest in Expanding Fellowship Training to Pediatricians. PM R. (2021) ;13: (10):1136–47. doi: 10.1002/pmrj.12549 |
[14] | Houtrow A . Results from the 2009 Pediatric Rehabilitation Practice survey of the AAPM&R Pediatric Rehabilitation/Developmental Disabilities Council. PM R. (2011) ;3: (1):45–52. doi: 10.1016/j.pmrj.2010.08.013 |
[15] | Murphy A , Pinkerton LM , Bruckner E , Risser HJ . The Impact of the Novel Coronavirus Disease 2019 on Therapy Service Delivery for Children with Disabilities. J Pediatr. (2021) ;231: :168–77.e1. doi: 10.1016/j.jpeds.2020.12.060 |
[16] | Van Kessel R , Hrzic R , O’Nuallain E , et al. Digital Health Paradox: International Policy Perspectives to Address Increased Health Inequalities for People Living With Disabilities. J Med Internet Res. (2022) ;24: (2):e33819. doi: 10.2196/33819 |
[17] | Cutler DM , Nikpay S , Huckman RS . The Business of Medicine in the Era of COVID-19. JAMA. (2020) ;323: (20):2003–4. doi: 10.1001/jama.2020.7242 |
[18] | McMahon BT , Roessler R , Rumrill PD , et al., Hiring Discrimination Against People with Disabilities Under the ADA: Characteristics of Charging Parties. J Occup Rehabil. (2008) ;18: (2):122–32. doi: 10.1007/s10926-008-9133-4 |
[19] | Long D , Long D , Turner W , et al., LB-13. Economic and workload impact of COVID-19 pandemic on physicians in the United States: results of a national survey. Open Forum Infect Dis. (2020) ;7: (Suppl 1):S850. doi: 10.1093/ofid/ofaa515.1910 |
[20] | Ferns SJ , Gautam S , Hudak ML . COVID-19 and Gender Disparities in Pediatric Cardiologists with Dependent Care Responsibilities. Am J Cardiol. (2021) ;147:137–42. doi: 10.1016/j.amjcard.2021.02.017 |
[21] | Nishida S , Nagaishi K , Motoya M , et al. Dilemma of physician-mothers faced with an increased home burden and clinical duties in the hospital during the COVID-19 pandemic. PLoS One. (2021) ;16: (6):e0253646. doi: 10.1371/journal.pone.0253646 |
[22] | Delaney RK , Locke A , Pershing ML , et al. Experiences of a health system’s faculty, staff, and trainees’ career development, work culture, and childcare needs during the COVID-19 pandemic. JAMA Netw Open. (2021) ;4: (4):e213997. doi: 10.1001/jamanetworkopen.2021.3997 |
[23] | Frank E , Zhao Z , Fang Y , Rotenstein LS , Sen S , Guille C . Experiences of Work-Family Conflict and Mental Health Symptoms by Gender Among Physician Parents During the COVID-19 Pandemic. JAMA Netw Open. (2021) ;4: (11):e2134315. doi: 10.1001/jamanet-workopen.2021.34315 |
[24] | Draugalis JR , Plaza CM . Best practices for survey research reports revisited: implications of target population, probability sampling, and response rate. Am J Pharm Educ. (2009) ;73: (8):142. doi: 10.5688/aj7308142 |

