
Fatal COVID-19 in a neonate after probable late intrauterine transmission
Abstract
We report the case of a 35-week gestation infant girl born by emergent cesarean section for fetal distress in a woman with recent coronavirus disease 2019 (COVID-19). Tests for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using polymerase chain reaction (PCR) on the infant at 24 and 48 hours of life were negative. However, at 72 hours of life, the infant’s respiratory status worsened, and a repeat SARS-CoV-2 PCR was positive. The infant developed leukopenia, thrombocytopenia, and progressive respiratory failure, and died on the ninth day of life. Pathologic examination of the placenta revealed findings consistent with COVID-19 placentitis, and SARS-CoV-2 RNA staining was positive, suggesting intrauterine transmission of the infection.
Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) resulting in coronavirus disease 2019 (COVID-19) is generally much less severe in children than in adults. However, little is known about the prevalence of COVID-19 in neonates. The rate of vertical transmission is approximately 5% [1], some of which is thought to be due to early postpartum acquisition. We present a case of fatal COVID-19 in a neonate who likely acquired the infection during the late intrauterine period.
1Case
A 2140 g female infant was born at 35 and 3/7 weeks’ gestational age to a 26-year-old gravida 1 para 1 woman by emergency cesarean section at a community hospital in the United States for decreased fetal movement and recurrent late decelerations on fetal monitoring. The infant’s mother was unvaccinated against COVID-19 and developed mild PCR-confirmed COVID-19 nine days before delivery. By the day of delivery, her symptoms had nearly resolved. Artificial rupture of the membranes occurred at the time of operative delivery, and the amniotic fluid was meconium-stained. Precautions for the delivery were in accordance with Centers for Disease Control and Prevention (CDC) recommendations, which included N95 respirators, gloves, gowns, and eye protection. No maternal-infant contact occurred after delivery. The neonate was limp and apneic, was given positive pressure ventilation by mask, and underwent deep suctioning with removal of thick meconium. Her Apgar scores were 4, 6, and 8 at 1, 5, and 10 minutes, respectively. A capillary blood gas obtained 2.5 hours after birth demonstrated a pH of 7.1, pCO2 49 mm Hg, pO2 48 mm Hg, HCO3 15.5 mmol/L, and a base deficit of 14 mmol/L. A blood culture was obtained, ampicillin, gentamicin, and intravenous fluids were administered, and she was transferred to a tertiary-care neonatal intensive care unit (NICU) while receiving noninvasive ventilation. Appropriate precautions for preventing SARS-CoV-2 transmission were observed during the transfer.
On admission to the NICU, the infant was immediately placed in a negative pressure isolation room, and precautions for a patient with possible SARS-CoV-2 infection were maintained throughout the hospitalization. The infant was tachycardic and tachypneic, with subcostal and intercostal retractions. The patient promptly underwent endotracheal intubation and was placed on conventional ventilation. Chest radiography performed shortly after intubation showed bilateral opacification of the lungs. Surfactant was administered via an endotracheal tube. Therapeutic hypothermia was not instituted as hypoxic ischemic encephalopathy was thought to be unlikely given the lack of prolonged resuscitation and a normal neurologic examination on admission.
At 24 and 48 hours of life, nasopharyngeal (NP) swabs were obtained to test for the presence of nucleic acids encoding the SARS-CoV-2 spike protein/ORF1. Both the tests yielded negative results. The infant’s respiratory status improved over the first 48 hours of life, but she remained on a ventilator. Chest radiographs obtained on days 2 and 3 were improved.
On day 4, the patient developed a fever of 38.8C. On the same day, her white blood cell count decreased to 2400/mcL, her absolute lymphocyte count decreased to 400/mcL, and her platelet count decreased to 99,000/mcL. Blood cultures were obtained, blood and surface swabs for herpes simplex virus were collected, and antibiotics were changed to ampicillin, ceftazidime, and acyclovir after an unsuccessful attempt at lumbar puncture. A repeat NP swab for SARS-CoV-2 nucleic acid targeting the spike protein/ORF1 was obtained and returned a positive result. On day 5, the infant developed tachycardia to 210 beats/min, C-reactive protein increased to 10.7 mg/dL, and platelet count decreased to 62,000/mcL. By day 6, her oxygen requirement had increased to 45% and pulmonary infiltrates had worsened. Surfactant was repeated without clinical improvement, and dexamethasone 0.15 mg/kg daily was begun.
On days 7 and 8, the infant continued to require increasing ventilator support with worsening pCO2 and increasing oxygen requirement. She developed hypothermia with a temperature of 35.2 C, and her platelet count decreased to 11,000/mcL, for which she received a platelet transfusion. On day 9, her platelet count was 26,000/mcL, and her serum fibrinogen level was < 50 mg/dL. The patient developed two posturing episodes that were concerning for seizures. She was treated with platelets, cryoprecipitate, and phenobarbital. Shortly thereafter, she developed bradycardia, agonal breathing with an oxygen saturation of 60% , and severe respiratory and metabolic acidosis with a venous pH < 6.8. Cardiopulmonary resuscitation was initiated, and the baby was placed on a high-frequency oscillatory ventilator without improvement in oxygenation or ventilation. Cranial ultrasound demonstrated effacement of the gray-white matter junction secondary to acute hypoxia or ischemia. The family was informed of the poor prognosis and opted for comfort care. An autopsy was not performed.
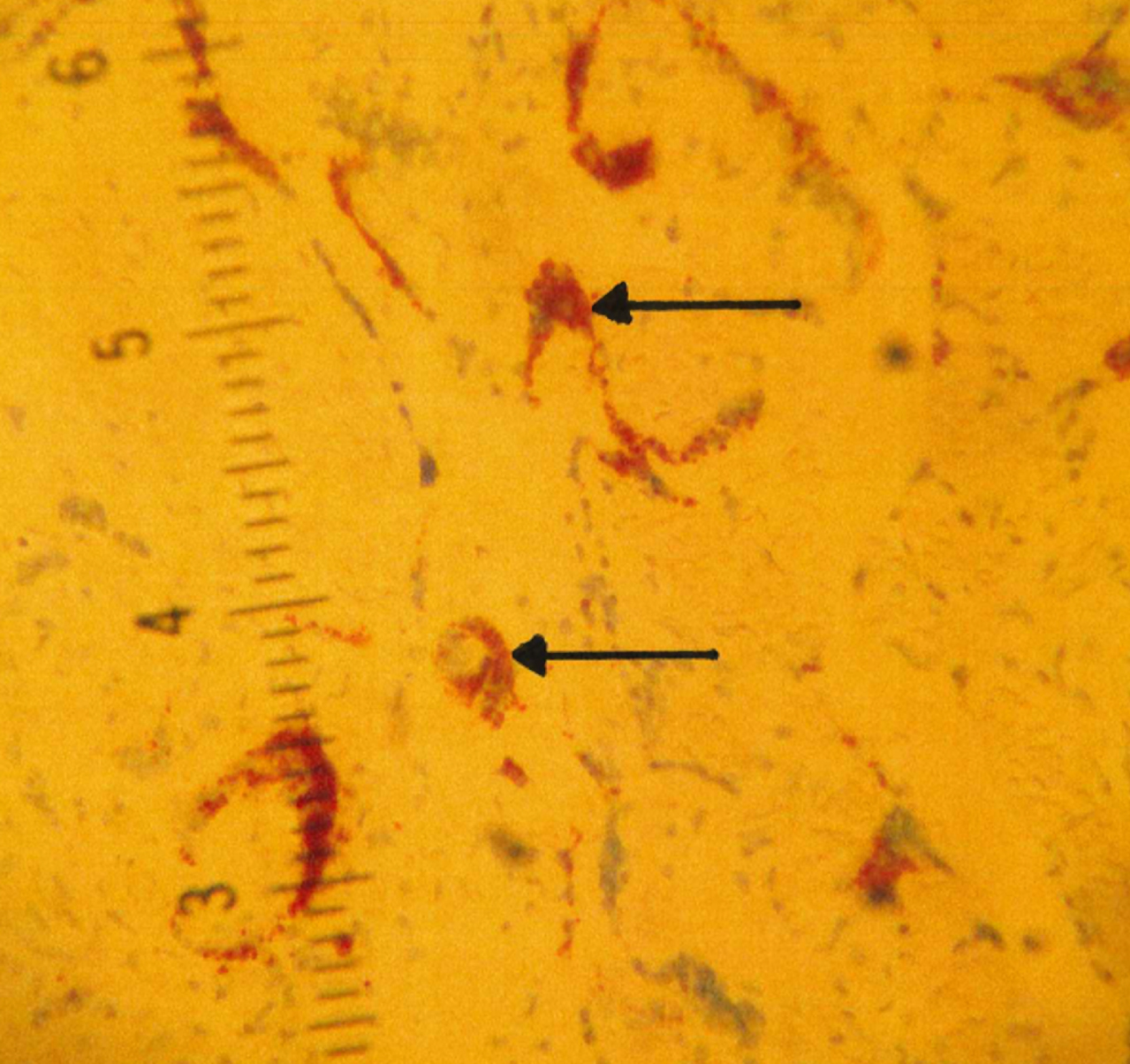
Results of the pathological examination of the placenta became available after the infant’s death. Histological examination revealed cystic areas with fresh hemorrhages throughout the placenta. Areas of patchy villous edema, subchorionic thrombi, chorangiosis, and histiocytic intervillositis were observed (Fig 1). SARS-CoV-2 RNA immunohistochemistry staining was positive within the villous trophoblast (Fig 1).
Fig. 1
A. Placental histology shows histiocytic intervillositis highlighted by CD68 stain (arrows).
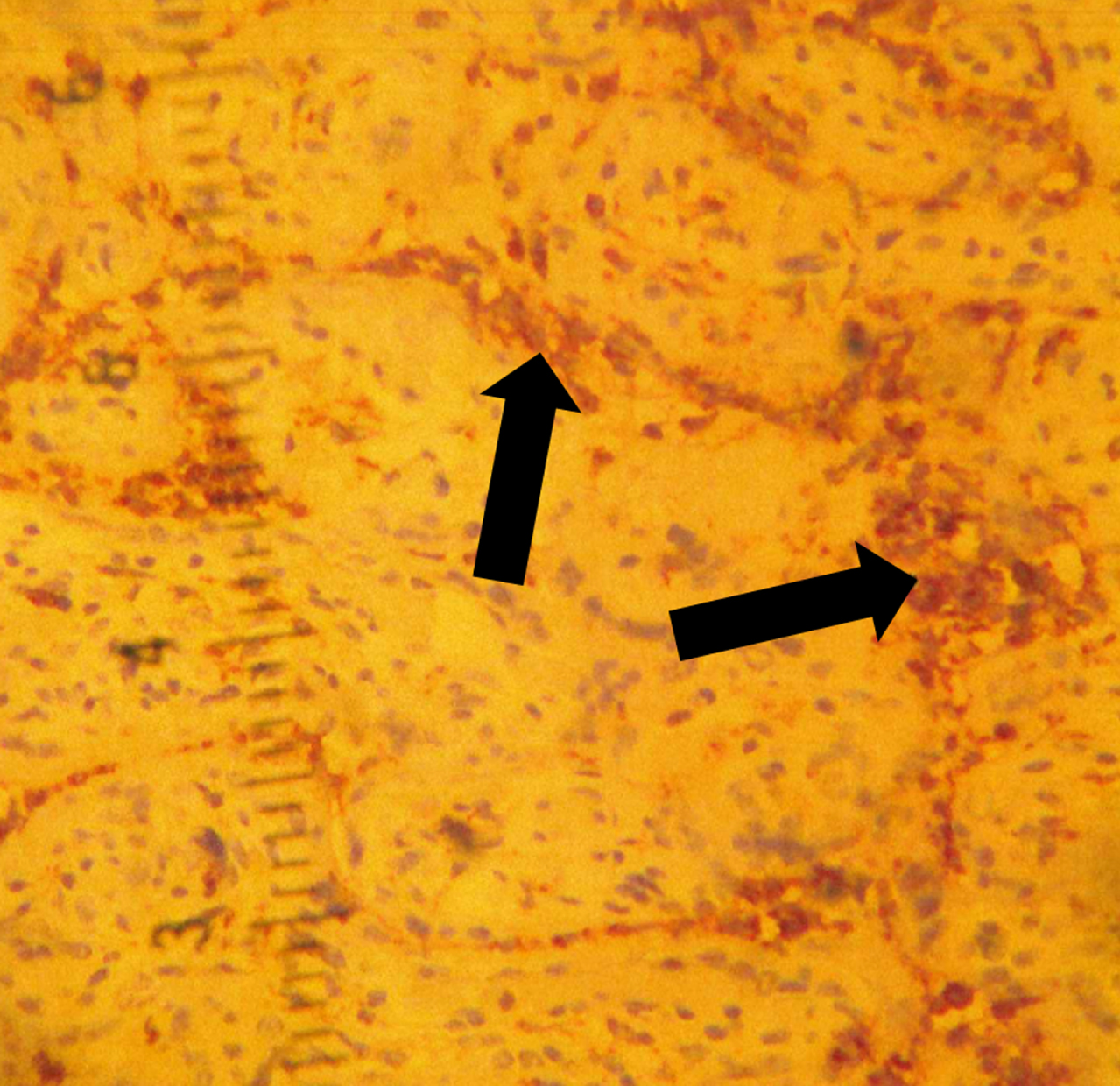
Fig. 1
B. Villous trophoblast involvement by COVID-19 demonstrated by SARS-CoV-2 immunohistochemistry staining (arrows).
2Discussion
COVID-19 is more severe in pregnant women than in nonpregnant women. Using data from the National Notifiable Diseases Surveillance System, Zambrano et al analyzed data from 409,462 women with laboratory-confirmed symptomatic COVID-19, of whom 23,434 (5.7%) were pregnant [2]. After adjusting for age, race/ethnicity, and underlying medical conditions, pregnant women were significantly more likely than nonpregnant women to be admitted to an intensive care unit (ICU), receive invasive mechanical ventilation, receive extracorporeal membrane oxygenation (ECMO), and die.
The effect of COVID-19 during pregnancy on the fetus is less clear, although the risk of premature delivery has been demonstrated in several studies. In a large meta-analysis, compared with pregnant women without COVID-19, pregnant women with COVID-19 had an increased odds of cesarean delivery, giving birth to a low-birth-weight infant, and delivering prematurely [1]. In that same study, the overall frequency of vertical transmission was 5.3%. However, the proportion of these cases that reflect early postnatal acquisition is difficult to assess.
In a study from the UK, the incidence of neonatal COVID-19 was 5.6 per 10,000 live births [3]. Two-thirds of cases were diagnosed at or after 7 days of life. The authors arbitrarily defined possible prenatal (intrauterine or intrapartum) transmission as the presence of a positive SARS-CoV-2 PCR in an infant within the first 12 hours of life, which occurred in only 2 (3%) of 66 infected neonates. This definition likely underestimates the rate of prenatal transmission as indicated by our infant, whose first positive SARS-CoV-2 PCR result occurred at 72 hours of life.
We cannot definitively exclude postnatal acquisition in our patient, but it seems unlikely for several reasons. There was no infant contact with the mother or other family members after delivery as the baby underwent immediate resuscitation by delivery room personnel. She was in isolation throughout her hospital stay with appropriate SARS-CoV-2 transmission precautions, and there were no other patients in our NICU with COVID-19 during her hospitalization.
There are multiple causes of fetal distress and hypoxia, including umbilical cord compression, cord prolapse, cord entanglement, placental abruption, infection, uterine rupture, and other events that result in compromised perfusion to the fetus. However, based on the newborn records, there were no concerns for bleeding or abruption around delivery, nor was there evidence of another inciting event. Although the infant’s initial NP swabs were negative for COVID-19, her non-reassuring fetal heart rate variability and subsequent meconium aspiration were likely a result of intrauterine infection with COVID-19, given the placental histology and the presence of SARS-CoV-2 within the placental tissue. In a study of women with COVID-19 during the third trimester of pregnancy, common placental findings included evidence of maternal vascular malperfusion (MVM) [4], manifested as injured maternal vessels, intervillous thrombi, and histiocytic intervillositis, features that were also observed in our case (Fig 1).
The reason that our patient had negative SARS-CoV-2 PCR tests at 24 and 48 hours of life is unclear. The portal(s) of entry for intrauterine transmission of COVID-19 have not been identified, and it is possible that sampling an area other than the nasopharynx, such as the blood, would have enabled viral detection sooner. Unfortunately, most SARS-CoV-2 PCR tests are only authorized for use with NP swabs. Interestingly, in one of the first reports of confirmed placental infection with COVID-19, the neonate tested negative for SARS-CoV-2 despite developing severe multi-organ inflammatory symptoms [5].
There are relatively few reports of neonatal COVID-19 in which placental infection is confirmed by histological testing and SARS-CoV-2 staining, thus suggesting intrauterine transmission [6–8]. Placental histology typically shows chronic histiocytic intervillositis and syncytiotrophoblast necrosis. Neonatal outcomes range from asymptomatic infection to severe multisystem inflammatory disease to stillbirth.
Both CDC and the American Academy of Pediatrics recommend that infants born to mothers with confirmed or suspected COVID-19 be tested for COVID-19 at 24 hours of life and, if negative, again at 48 hours of life. This practice is likely sufficient for asymptomatic infants. However, this might not be sufficient in the neonate for whom previous testing was negative but in whom symptoms persist. Based on our case, we suggest that infants born to mothers with COVID-19 who develop non-reassuring fetal status and/or neonatal respiratory distress should be tested beyond the 48-hour mark, particularly if leukopenia or thrombocytopenia develops. The age at which testing can safely be stopped in a maternally exposed, symptomatic newborn is not yet clear.
COVID-19 vaccines during pregnancy are safe for the mother [9] and developing fetus [10], and both CDC and the American College of Obstetricians and Gynecologists recommend that all pregnant and lactating women receive vaccination against COVID-19. Despite this recommendation, COVID-19 vaccination completion is lower in pregnant women than in non-pregnant women of reproductive age [11]. As of the date of our patient’s delivery, only 35% of pregnant women in the US were fully vaccinated against COVID-19 either before or during their pregnancy.
In summary, we report a fatal case of a 9-day old infant born to a mother with recent COVID-19, which likely occurred from late intrauterine transmission. While such outcomes appear to be rare, they are also unpredictable. Therefore, all pregnant women should be counseled to receive COVID-19 vaccination, which is safe and effective in preventing illness in both pregnant women and their infants [12]. In symptomatic infants born to women with COVID-19, a high index of suspicion for neonatal COVID-19 should be maintained, even if the initial testing is negative.
Contributions statement
All authors have seen and approved the manuscript, have contributed significantly to the work, and attest that the manuscript has not been previously published nor is it being considered for publication elsewhere.
Conflict of interest statement
None of the authors have any competing interests to declare.
Ethics statement
The case report has no identifiers and was considered exempt by our Institutional Review Board.
Funding
None.
References
[1] | Jafari M , Pormohammad A , Sheikh Neshin SA , Ghorbani S , Bose D , Alimohammadi S , et al., Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: a systematic review and meta-analysis, Rev Med Virol (2021) ;31: :1–16. |
[2] | Zambrano LD , Ellington S , Strid P , Galang RR , Oduyebo T , Tong VT , et al., Update: Characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status - United States, January 22-October 3, MMWR Morb Mortal Wkly Re (2020) ;69: :1641–7. |
[3] | Gale C , Quigley MA , Placzek A , Knight M , Ladhani S , Draper ES , et al., Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: A prospective national cohort study using active surveillance, Lancet Child Adolesc Health (2021) ;5: :113–21. |
[4] | Shanes ED , Mithal LB , Otero S , Azad HA , Miller ES , Goldstein JA , Placental pathology in COVID-19, Am J Clin Pathol (2020) ;154: :23–32. |
[5] | Schoenmakers S , Snijder P , Verdijk RM , Kuiken T , Kamphuis SSM , Koopman LP , et al., Severe acute respiratory syndrome coronavirus 2 placental infection and inflammation leading to fetal distress and neonatal multi-organ failure in an asymptomatic woman, J Pediatr Infect Dis Soc (2021) ;10: :556–61. |
[6] | Shende P , Gaikwad P , Gandhewar M , Ukey P , Bhide A , Patel V , et al., Persistence of SARS-CoV-2 in the first trimester placenta leading to transplacental transmission and fetal demise from an asymptomatic mother, Hum Reprod (2021) ;36: :899–906. |
[7] | Stonoga ETS , de Almeida Lanzoni L , Rebutini PZ , Permegiani de Oliveira AL , Chiste JA , Fugaca CA , et al., Intrauterine transmission of SARS-CoV-2, Emerg Infect Dis (2021) ;27: :638–41. |
[8] | Schwartz DA , Baldewijns M , Benachi A , Bugatti M , Collins RRJ , De Luca D , et al., Chronic histiocytic intervillositis with trophoblast necrosis is a risk factor associated with placental infection from coronavirus disease (COVID-19) and intrauterine maternal-fetal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission in live-born and stillborn infants, Arch Pathol Lab Med (2021) ;145: :517–28. |
[9] | DeSilva M , Haapala J , Vazquez-Benitez G , Vesco KK , Daley MF , Getahun D , et al. Evaluation of acute adverse events after Covid-19 vaccination during pregnancy. N Engl J Med. (2022) ;387: :187–189. |
[10] | Lipkind HS , Vazquez-Benitez G , DeSilva M , Vesco KK , Ackerman-Banks C , Zhu J , et al., Receipt of COVID-19 vaccine during pregnancy and preterm or small-for-gestational-age at birth - eight integrated health care organizations, United States, December 15, -July 22, MMWR Morb Mortal Wkly Re (2022) ;71: :26–30. |
[11] | Razzaghi H , Meghani M , Pingali C , Crane B , Naleway A , Weintraub E , et al., COVID-19 Vaccination coverage among pregnant women during pregnancy - eight integrated health care organizations, United States, December 14, -May 8, MMWR Morb Mortal Wkly Re (2021) ;70: :895–9. |
[12] | Halasa NB , Olson SM , Staat MA , Newhams MM , Price AM , Pannaraj PS , et al., Maternal vaccination and risk of hospitalization for Covid-19 among infants. N Engl J Med. (2022) ;387: :109–119. |


