
The Effects of Pomegranate Seed Oil on Mild Cognitive Impairment
Abstract
Background:
In recent years, there has been a growing interest, supported by many experimental and clinical studies, about the benefits of pomegranate in preventing various pathologic conditions, including brain neurodegeneration. The pomegranate seed oil (PSO) contains high levels of fatty acids that have antioxidant and anti-inflammatory properties.
Objective:
Due to the lack of clinical trials, the aim of the present study was to investigate the effects of PSO on cognition of people with mild cognitive impairment (MCI).
Methods:
Eighty people with the diagnosis of MCI were randomized forty to take 5 drops of PSO and follow the Mediterranean Diet (MeDi) and forty just followed MeDi. All were examined with an extensive neuropsychological assessment before and after one year of treatment.
Results:
The results showed that the participants who took the PSO had statistically significantly better global cognition (p = 0.004), verbal episodic memory (p = 0.009), and processing and executive functions (p < 0.001) in contrast with the participants who did not take it.
Conclusions:
In conclusion, the PSO can be beneficial for people with MCI as it is helpful for some important cognitive domains. As PSO is a natural product that does not burden the human body, it can be used by people with MCI and be a significant and promising part of holistic approaches for the prevention of dementia.
INTRODUCTION
Mild cognitive impairment
According to DSM-V, mild cognitive impairment (MCI) can be defined as an objective impairment in one or more cognitive functions projected on standardized neuropsychological tests, while maintaining the ability to complete daily activities [1]. MCI patients can also be divided in amnestic MCI with primary memory impairments and non-amnestic MCI with impairment in other cognitive functions except memory. These subtypes are further classified as “single domain” and “multi-domain”, depending on the impaired cognitive functions [2, 3]. The MCI patients can also be divided into early and late stages. Patients in both stages meet the conventional criteria for MCI but early MCI reflects those at an earlier point in the clinical spectrum.
The World Health Organization (WHO) has declared Alzheimer’s disease (AD) as “global health priority” due to the complexity of the disease and the absence of a permanent cure [4]. Currently, there are various theories and hypotheses about the causes and targets for drugs in treating AD. However, even recent approved medications can only slow down the progression of the disease [5]. Although our knowledge of AD has been significantly expanded in recent years, it remains far from a preventive or curative intervention.
Prevention approaches oriented to wellness are becoming more essential toward a high quality of life and healthy longevity. Within this framework, investigating disease prevention through a comprehensive approach is offering valuable conceptual frameworks to bolster evidence-based medicine grounded in clinical research [6]. Since numerous drugs targeting various aspects have proven unsuccessful in finding a treatment, there is now a growing interest in exploring natural products and nutraceutical compounds as potential preventive therapeutic options. Given that AD is a complex disease influenced by multiple factors, nutraceutical compounds have an advantage in offering a multi-target approach by interacting with different molecular sites in the human brain, in contrast to the single-target activity typically exhibited by most drugs utilized for AD treatment (cholinesterase inhibitors, glutaminergic antagonists, and anti-amyloid drugs [7].
Higher adherence to the Mediterranean Diet (MeDi) can reduce the risk of developing MCI and AD, because it is associated with better cognitive status and less depressive symptoms [8, 9]. It can be a protective factor against memory decline and atrophy of the medial temporal lobe. These associations are likely attributed to a reduction in the accumulation of amyloid plaques and tau pathology [10]. Adherence to the MeDi from midlife is proved to have a significant role in metabolic function, cerebrovascular health, AD pathology, and cognitive function [11]. The review by Siervo et al. (2021) highlights two important points: first, maintaining an optimal nutritional status throughout life is crucial for preserving cognitive health, and second, effective dietary and lifestyle interventions for preventing cognitive decline are most effective during specific critical windows. While observational studies suggest that the MeDi may delay cognitive decline, clinical trials have not yet confirmed these findings. Nevertheless, the MeDi is recommended as a protective dietary pattern for cognitive function based on its well-established antioxidant effects [12].
The effects of pomegranate on memory
Pomegranate (Punica granatum L.) is considered as a food rich in polyphenols and it has been widely used in traditional medicine. The antioxidant activity of pomegranate juice has been recognized as being superior in comparison with other fruits [13]. The polyphenols present in pomegranate juice may help in preventing neuronal damage caused by free radicals produced during normal metabolic processes. Previous studies on animals and a clinical trial on middle-aged and older adults suggest that pomegranate juice has the potential to enhance memory. However, the long-term effects of pomegranate juice consumption on cognitive function have not yet been investigated [14].
Siddarth et al. (2020) designed a randomized placebo-controlled trial regarding the effects of pomegranate juice on memory of middle-age and older adults. The results of this study showed that 98 participants who consumed pomegranate juice for 12 months had significantly better verbal memory performance compared to 102 participants who consumed the placebo drink. The study also found that pomegranate juice consumption was associated with increased functional brain activity during memory tasks. The authors suggested that the observed memory-enhancing effects of pomegranate juice may be due to its high levels of polyphenolic compounds, which have been shown to have antioxidant and anti-inflammatory properties that can protect and enhance cognitive function. However, the authors suggest that further studies are needed to confirm these findings [15].
In cellular level, Abu-Taweel et al. (2021) showed that the pomegranate juice reversed AlCl3-induced neurotoxicity and improved learning and memory in female mice proving its potential efficiency against aluminum chloride-induced neurobehavioral and biochemical disorders. Specifically, AlCl3 had significant effects on female mice, impacting body weight, behavioral tasks (shuttle box, T-maze, and Morris water maze), as well as neurotransmitters and oxidative stress parameters. Notably, pomegranate juice, especially at lower concentrations, led to significant improvements in body weight, spatial memory, learning (T-maze, Morris water maze, and shuttle box tasks), and neurotransmitters and oxidative biomarkers in AlCl3-treated female mice [16]. Moreover, Subash et al. (2015) investigated the effects of dietary supplementation with pomegranate juice extract on memory, anxiety, and learning abilities in a mouse model of AD for 15 months. Transgenic AD mice showed significant cognitive and behavioral impairment, including memory and anxiety. Also, another study showed that mice fed a diet containing pomegranate extract exhibited improvement in memory, learning, locomotor function, and reduced anxiety, suggesting that pomegranate supplementation may slow the progression of cognitive decline in AD [17].
In general, pomegranate juice, known for its abundance of secondary metabolites and natural compounds, has gained attention as a potential alternative to synthetic anti-inflammatory agents. It has demonstrated effectiveness in various chronic inflammatory diseases [18]. In the brain, pomegranate polyphenols can enhance brain neurochemistry by inhibiting NF-κB, a transcription factor involved in the production of pro-inflammatory and toxic molecules [10]. Pomegranate juice also affects the expression of genes related to amyloid precursor protein cleaving, enzymatic activities of cyclooxygenase 2, and caspase enzymes, which collectively reduce neuroinflammation, promote neuronal homeostasis, and alleviate clinical symptoms of the disease leading to reduction of beta-site amyloid precursor protein [19, 20].
Pomegranate seed oil
The pomegranate can be divided into three parts: the leathery exocarp, fleshy mesocarp, and the seeds which include the arils. Approximately 7 to 27% of the seeds are composed of oil which can be extracted with conventional and modern techniques [21]. To begin the process of obtaining pomegranate seed oil (PSO), the seeds are first collected from the fruit juice processing industries. These seeds are then cleaned, dried, and turned into powder before the extraction takes place. It is important to store and preserve the seeds and the extracted oil correctly to prevent the production of mycotoxins and to avoid any negative effects caused by oxidative reactions [22]. The most common extraction method is the cold pressing. Cold-pressed oils are known to possess improved fatty acid composition and physical-chemical characteristics such as low peroxide value, high phenolic content, and an enhanced aroma profile, when compared to data gathered from previous studies [23].
PSO primarily consists of conjugated fatty acids, which make up more than 80% of its composition. Notably, linolenic acids have gathered significant attention due to their functional and therapeutic properties. Linolenic acid, for instance, has seven naturally occurring isomers, including punicic acid, alpha and beta-eleostearic acid, alpha and beta-calendic acid, jacaric acid, and catalpic acid [24]. Furthermore, Białek et al. (2020) utilized the argentometric liquid chromatography method to identify an additional 12 isomers of conjugated linolenic acid in PSO [25]. For this reason, it has been recognized for its antimicrobial, antioxidant, immunomodulatory, anti-carcinogenic, and lipid metabolism regulation properties [26].
The benefits of PSO on memory of experimental animals
The study by Sarkaki et al. (2015) aimed to assess the effects of PSO on avoidance memories in rats with cognitive impairment due to estrogen deficiency. The results showed that PSO administration improved sensorimotor function and memory performance in a dose-dependent manner. These effects were attributed to the phyto-estrogenic and antioxidative actions of PSO, suggesting its therapeutic potential for memory enhancement [27]. The study by Al Sabahi et al. (2017) on rats showed that 3-NP increases free radicals (reactive oxygen species, ROS) and decreases antioxidant levels, while PSO scavenges ROS and enhances antioxidant activities. By restoring cell viability and maintaining antioxidant defense, the oil mitigates vulnerability to oxidative stress. These findings highlight the potential of PSO as a protective agent against neurodegenerative conditions like Huntington’s disease [28].
Moreover, due to its phenolic compounds it has neuroprotective effects. Shrivas et al (2023) tried to create a stable microemulsion using PSO as an adjuvant, specifically for galantamine hydrobromide (GHBr). The microemulsion was characterized for its properties and tested for its protective effects against amyloid-β (Aβ)-induced toxicity in a cell line. The ratio of GHBr and PSO was optimized, and the microemulsion showed positive results in terms of reducing toxicity, exhibiting antioxidant activity, and protecting against cell death caused by Aβ. The study suggests that PSO has the potential to enhance the effectiveness of anti-AD drugs for treating the disease [29]. Besides that, PSO can inhibit enzymes, reduce reactive oxygen species, prevent microglial activation, inhibit hyperphosphorylation of tau protein, maintain synaptic plasticity, exhibit anti-inflammatory activity, and inhibit beta secretase-1 (BACE-1). Although there is a lack of studies on humans, there is strong evidence suggesting that PSO can reduce multiple risk factors associated with AD providing neuroprotection and slowing down the aging process [30].
Aim and hypothesis of the study
Taking into consideration the lack of clinical trials regarding the effects of PSO on memory and other cognitive functions, the primary objective of the present study was to investigate the potential effects of PSO on cognition of people with MCI using an extensive neuropsychological assessment. The first hypothesis of the present study was that the participants who will take PSO and MeDi will have the same or better performance in the neuropsychological tests in comparison with the baseline assessment. The second hypothesis was that the participants who will take PSO plus MeDi will have better performance in the neuropsychological tests than the participants of the control group with only MeDi after one year of treatment.
METHODS
Participants
One hundred (100) Greek native speakers with the diagnosis of MCI participated in the study. The diagnosis of MCI was given by a neurologist according to the criteria of DSM-V after neurological and neuropsychological assessment, evaluation of the MRI and the results of blood tests. However, 20 participants dropped out (Fig. 1) and the analyzed sample consisted of 80 participants, 32 men and 48 women with a mean age of 69.53 (SD = 2.889) years and a mean education of 10.11 (SD = 3.130) years (Table 1). The two groups did not have statistically significant differences in demographics. All the participants followed the same processes, which included clinical examination, laboratory/imaging procedures and neuropsychological assessment. All the laboratory results were evaluated by the neurologist of the Greek Association of Alzheimer’s Disease and Related Disorders (GAADRD). The exclusion criteria were: 1) hearing deficits that could affect the performance of neuropsychological examination, 2) uncorrected visual impairment, 3) inability to comprehend Greek language, 4) currently taking medication or other treatment for dementia, 5) currently taking antipsychotics, 6) having higher score than 6 in Geriatric Depression Scale, and 7) not having the diagnosis of MCI.
Fig. 1
Flow chart presenting randomization and allocation procedure of participants in all groups respectively.
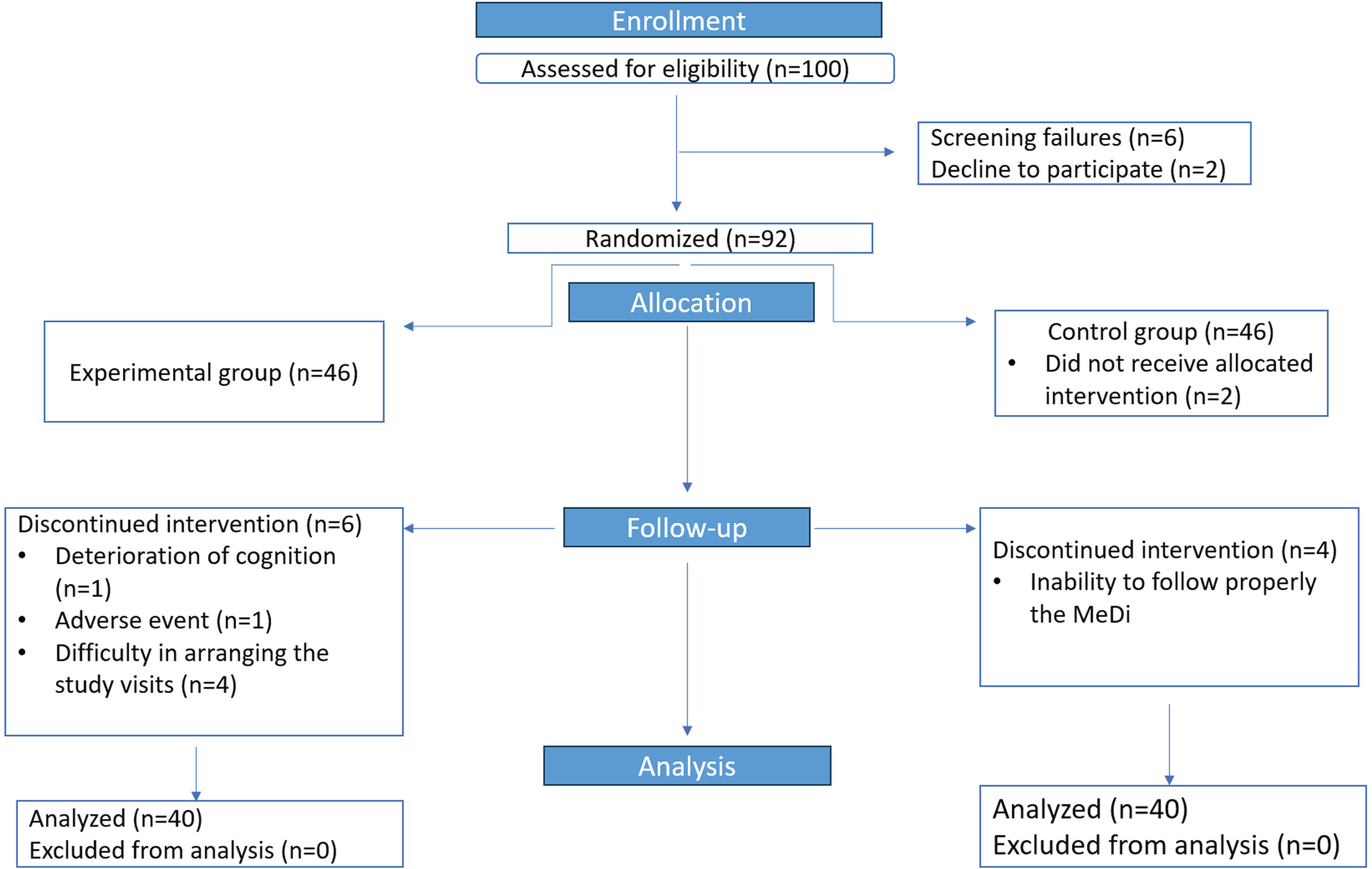
Table 1
Demographics
| Gender | Age | Education | ||||
| % Male | % Female | M | SD | M | SD | |
| Total | 43.8 | 56.3 | 69.53 | 2.899 | 10.11 | 3.130 |
| Experimental Group | 40 | 60 | 69.80 | 3.115 | 10.27 | 3.297 |
| Control Group | 47.5 | 52.5 | 69.30 | 2.672 | 9.93 | 3.025 |
| p | 0.505 | 0.443 | 0.543 | |||
Recruitment
Using ongoing recruitment, participants were recruited from the Day Care Centers “Saint John” and “Saint Helen” of the GAADRD. There were multiple ways of recruitment. After the diagnosis, the participants were informed by the neurologist about the study, and they were asked to participate voluntarily. Moreover, people, who were examined before, were called by phone, and informed about the study. There were, also, posters in the buildings of the Day Care Centers and the people could see the contact details of the investigators and contact them for more information.
Procedure
All study participants read the information sheet and signed an informed consent stating that the research group has the permission to use their demographic data, which would be anonymized, such as gender, age, and education, as well as their performance in the neuropsychological tests, for research purposes. After that, they went through an extensive baseline neuropsychological assessment covering a wide range of cognitive functions and blood draw to test the results in blood biomarkers, such as Aβ, tau protein, and phospho-tau protein. The administration of the neuropsychological measurements was conducted individually for each patient in a soundproof room by a trained psychologist and the duration of the assessment was approximately 2 h divided into two different sessions. The participants were randomly allocated either in the experimental group or in the control group. Specifically, the participants of the experimental group took 5 drops of PSO per day and followed the MeDi, whereas the participants of the control group just followed MeDi (Fig. 1). Neuropsychological assessment was conducted after six months and one year of treatment. In the meantime, the participants were asked to fill monthly the MedDiet Score, which is compliance questionnaire [31], and a diary, in which they marked every day that they took PSO, in order to reassure that they follow the MeDi and they regularly take the PSO.
The PSO that was administered to the participants was the PSO Pom Star Rodi Hellas. It is a virgin oil obtained from the pomegranate seeds, with no additives and it is produced with cold pressing. It has been analyzed by the Agrolab RDS and it is accredited with all the necessary certifications. The chemical and physical properties and the fatty acid composition of the product can be found in Table 2.
Table 2
Chemical and physical properties and fatty acid composition of PSO
| Chemical and physical properties | |
| Specific gravity | 0.92–0.96 |
| Moisture and insoluble impurities | Max 0.1% |
| Acid value | Max 7.0 |
| Peroxide value | Max 10.0 |
| Fatty acid composition | |
| Palmitic acid | 2.0% –5.0% |
| Palmitoleic acid | Max 1% |
| Stearic acid | Max 3% |
| Oleic acid | 3.0% –20.0% |
| Linoleic acid | 3.0% –15.0% |
| Punicic acid | 70.0% –85.0% |
| Arachidic acid | Max 1.0% |
| Eicosenoic acid | Max 1.0% |
| Behenic acid | Max 1.0% |
| Erucic acid | Max 1.0% |
| Docosatrienoic acid | 2.0% –5.0% |
| Lignoceric acid | Max 2.0% |
| Other fatty acids | Max 5.0% |
Ethics
All study participants read the information sheet and signed the informed consent during the initial clinical visit, stating that the research group of the GAADRD have the permission to use their demographic data, which would be anonymized, such as gender, age, and education, as well as their performance in the neuropsychological tests, for research purposes.
The study was approved by the Scientific and Ethics Committee of the GAADRD (Scientific Committee Approved Meeting Number: 71/07-10-2021), which follows the new General Data Protection Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regards to the processing of personal data and on the free movement of such data, as well as the principles outlined in the Helsinki Declaration.
Outcome measures
The outcomes were measured with a neuropsychological battery designed to comprehensively evaluate attention, working memory, episodic memory, visuospatial abilities, executive functions, and functionality. The primary efficacy outcomes were the changes in cognition in Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-cog). To assess the global cognition, the Greek versions of Mini-Mental State Examination (MMSE) [32], Montreal Cognitive Assessment (MoCA) [33], and ADAS-cog [34] were used. The Rivermead Behavioral Verbal Learning Test was used for the evaluation of episodic memory [35]. Rey Auditory Verbal Leaning Test (RAVLT) and specifically its immediate and delayed recall was used to assess verbal episodic and working memory [36], whereas the Rey–Osterrieth Complex Figure Test was used for the evaluation of visuospatial episodic memory and executive functions [37]. The Trail Making Test Part B (TMT B) was used to examine visuospatial ability, executive functions, and processing speed [38]. The Functional Cognitive Assessment Scale (FUCAS) was used to assess functionality in daily living [39]. However, this test was used only to support that our patients had no problems in activities of daily living.
Statistics
Data analysis was performed using SPSS version 27.0 for Windows (IBM Corporation, Armonk, NY, USA) statistical software. Using the Kruskal-Wallis test, it was confirmed that there were not statistically significant differences between the two groups regarding age, gender and education. The Shapiro-Wilk test was used to assess the normality assumption for continuous variables. As the focus of the target was to investigate the effects of PSO the two groups were compared using the Mann-Whitney U test for intergroup comparisons and the Wilcoxon Signed Ranks test for intragroup comparisons. p-values less than 0.05 were considered statistically significant. To address the issue of multiple comparisons, Bonferroni correction was applied and the significance level was adjusted to a = 0.05/9. This correction method controls the familywise error rate to reduce the risk of Type I errors. The adjusted p-values obtained after applying the Bonferroni correction were used to determine the statistical significance (p < 0.0056).
RESULTS
Regarding the intragroup comparisons, the Wilcoxon Signed ranks test indicated statistically significant differences in RAVLT immediate recall, TMT B, and ADAS-cog (Table 3). Specifically, in RAVLT the experimental group had statistically significant improvement from the baseline assessment in the mean scores (Z =−4.387, p < 0.001) whereas the control group did not (Z =−1.354, p = 0.250). In the ADAS-cog, the experimental group had statistically better performance from the baseline assessment (Z =−2.887, p = 0.004), whereas the control group did not have any statistically significant change (Z =−0.846, p = 0.398). In TMT, the experimental group had statistically significant improvement from the baseline assessment (Z =−4.064, p < 0.001) and the control group had deterioration in the mean score but not statistically significant (Z =−2.740, p = 0.006). There were not statistically significant differences in the rest of the neuropsychological tests.
Table 3
Mean (M) and standard deviation (SD) of the scores of the neuropsychological assessment at baseline and after 12 months of treatment, and the results of Wilcoxon Signed Ranks test for intragroup comparison
| Baseline Assessment M±SD | Follow-up M±SD | Wilcoxon Signed Ranks Test Z, p | ||
| MMSE | Experimental group | 27.65±1.46 | 27.82±1.01 | Z =−1.011, p = 0.312a |
| Control group | 28.07±1.42 | 27.90±1.057 | Z =−1.006, p = 0.314b | |
| MoCA | Experimental group | 23.23±2.118 | 23.22±1.901 | Z =−0.095, p = 0.924a |
| Control group | 22.95±1.934 | 22.55±1.663 | Z =−1.736, p = 0.083b | |
| RAVLT | Experimental group | 37.85±6.079 | 40.55±5.974 | Z =−4.387, p < 0.001a |
| Control group | 37.95±4.940 | 37.28±5.282 | Z =−1.354, p = 0.250b | |
| RAVLT Recall | Experimental group | 5.00±1.922 | 5.32±1.831 | Z =−1.914, p = 0.056a |
| Control group | 5.05±1.894 | 4.63±1.497 | Z =−2.042, p = 0.041b | |
| ROCFT | Experimental group | 34.275±1.493 | 34.44±1.331 | Z =−0.730, p = 0.466a |
| Control group | 33.663±2.137 | 33.962±1.63 | Z =−1.234, p = 0.217a | |
| ROCFT Recall | Experimental group | 14.55±2.062 | 14.612±2.263 | Z =−0.632, p = 0.528a |
| Control group | 14.407±2.502 | 14.325±2.061 | Z =−0.498, p = 0.619b | |
| ADAS-cog | Experimental group | 15.295±1.694 | 12.110±1.685 | Z =−2.887, p = 0 .004a |
| Control group | 15.362±1.709 | 15.025±1.898 | Z =−0.846, p = 0.398a | |
| TMT B | Experimental group | 209.20±15.667 | 201.60±14.187 | Z =−4.064, p < 0.001a |
| Control group | 204.93±19.965 | 208.32±18.815 | Z =−2.740, p = 0.006b | |
| FUCAS | Experimental group | 42.88±1.381 | 42.65±0.949 | Z =−1.164, p = 0.244a |
| Control group | 42.80±1.344 | 42.88±1.137 | Z =−0.423, p = 0.672b |
aBased on Negative Ranks, bBased on positive Ranks, cThe sum of negative ranks equals the sum of positive ranks. MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; RAVLT, Rey Auditory Verbal Leaning Test; ROCFT, Rey–Osterrieth Complex Figure Test; ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; TMT B, Trail Making Test Part B; FUCAS, Functional Cognitive Assessment Scale.
As far as the intergroup comparisons, there were differences between the two groups proving that the experimental group had improvement in comparison with the control group, but they were not statistically significant. However, the Mann-Whitney U test indicated that the experimental group had significantly better performance in the follow up assessment (MdnDiff = 3.0, U = 273, p < 0.01) in ADAS-cog than the control group (MdnDiff = 0.5). In RAVLT there were statistically significant differences when p < 0.05 (MdnDiff = 3.0, U = 659, 0 = 0.022) but after the Bonferroni correction, it cannot be considered as statistically significant (Table 4).
Table 4
Comparison of the score differences of neuropsychological assessment between the two groups using the Mann-Whitney U test
| Baseline Assessment | Follow-up | |||
| U | p | U | p | |
| MMSE | 657.0 | 0.159 | 764.5 | 0.718 |
| MoCA | 732.5 | 0.510 | 623.5 | 0.084 |
| RAVLT | 659 | 0.173 | 562.5 | 0.022 |
| RAVLT Recall | 763.0 | 0.718 | 635.0 | 0.104 |
| ROCFT | 693.0 | 0.291 | 680.5 | 0.243 |
| ROCFT Recall | 758.5 | 0.688 | 681.0 | 0.249 |
| ADAS-cog | 640.5 | 0.123 | 273 | 0.001 |
| TMT B | 615.5 | 0.076 | 640.0 | 0.123 |
| FUCAS | 778.0 | 0.795 | 727 | 0.402 |
MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; RAVLT, Rey Auditory Verbal Leaning Test; ROCFT, Rey–Osterrieth Complex Figure Test; ADAS-cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; TMT B, Trail Making Test Part B; FUCAS, Functional Cognitive Assessment Scale.
DISCUSSION
As the tools of early detection of AD has been increased and specified, with the discovery of blood and cerebrospinal fluid biomarkers, more precise neuroimaging methods, analysis of electroencephalogram and a variety of neuropsychological tools, it is necessary to find effective ways of prevention. The daily consumption of PSO could be beneficial to this direction due to its antioxidant and anti-inflammatory effects [23]. So, the aim of the present was to identify the effects of PSO on cognition of people with the diagnosis of MCI. To do that a randomized clinical trial was conducted and an extensive neuropsychological assessment before and after one year of treatment was used.
The results of the present study showed that the PSO can improve visuospatial abilities, processing speed and executive functions measured by TMT B, learning and verbal episodic memory measured by RAVLT, and global cognition measured by ADAS-cog which is one of the most widely used psychometric tools in clinical trials [40]. Specifically, the experimental group had statistically significant better performance in the follow up assessment after one year of treatment in the ADAS-cog, TMT B, and RAVLT. However, except for MoCA, there was improvement in the mean score of all the other neuropsychological tests too, but the difference was not statistically significant. On the other hand, the control group not only had worse mean scores in all neuropsychological tests, except FUCAS, in comparison with the baseline assessment. In FUCAS, there were no differences in both baseline and after one year assessment between the two groups, but it was expected because MCI is characterized by cognitive deficits which are not detectable in activities of daily living. Taking into consideration all the above data from the intragroup comparisons, the first hypothesis can be confirmed. Regarding the second hypothesis, the intergroup comparisons showed that even though the two groups did not have statistically significant differences in the baseline assessment, they had statistically significant differences in ADAS-cog performance due to improvement that was marked in the experimental group. As it was mentioned in the study’s design, the analysis of blood biomarkers has been completed and the results will be announced soon with another publication.
As far as there are no studies on the effects of PSO on patients, the data of the present study can only be compared with the data of studies that used pomegranate juice. The most important advantage of PSO is that it cannot only maintain the cognitive level but also it can improve cognition in people with MCI. Siddarth et al. (2020) performed a 12-month randomized clinical trial on the effects of pomegranate juice on memory of middle-aged and older adults who were healthy or had the diagnosis of MCI. They found that people who took pomegranate juice (236 ml/day) had not statistically significant differences after twelve months, whereas the participants who took the placebo had statistically significant decline in visual memory measured by the Brief Visuospatial Memory Test-Revised (p = 0.002) [15].
Bookheimer et al. (2013) administered 8 ounces pomegranate juice to 15 middle-aged and older adults with self-reported memory complaints but without the diagnosis of MCI for four weeks and they compared them with 13 participants who took placebo. Besides neuropsychological tools, they used functional MRI during cognitive tasks and peripheral biomarkers before and after intervention. The results showed that pomegranate juice can improve verbal memory using the Buschke Selective Reminding Test (p = 0.017) and can increase the neural activity during verbal and visual memory tasks, trolox-equivalent antioxidant capacity, and urolithin A-glucuronide in comparison with the control group [41].
The positive effects could be explained by its high content in punicic acid, the primary active compound found in PSO, is an omega-5 isomer of conjugated α-linoleic acid. It has strong antioxidant and anti-inflammatory properties, which contribute to its beneficial effects against a wide range of diseases. Punicic acid reduces oxidative damage and inflammation by increasing the expression of peroxisome proliferator-activated receptors. Furthermore, it can reduce beta-amyloid deposits and the hyperphosphorylation of tau proteins by enhancing GLUT4 protein expression and inhibiting calpain activation [42].
While we have no clinical trials with PSO we have to say that data confirm previous trials on laboratory animals. Specifically, Akbarian et al. (2022), using the Morris water maze and passive avoidance tasks, proved that PSO could effectively ameliorate memory and learning impairments induced by scopolamine in rats via the improvement of the cholinergic system function, the reduction of oxidative stress, and the modulation of inflammatory cytokines [43]. It was demonstrated that pomegranate juice and seed extracts exhibited antioxidant activity that was 2 to 3 times higher than that of green tea or red wine using four different in vitro testing methods. The extracts of pomegranate showed the ability to scavenge free radicals, reduce oxidative stress in macrophages, and decrease lipid peroxidation in animals. Pomegranate displayed the most potent antioxidant activity, regardless of the concentration of phenolics. Further research on rats and mice revealed that by-product extracts derived from the entire pomegranate fruit reduced oxidative stress by 19% in peritoneal macrophages, decreased cellular lipid peroxide content by 42%, and increased reduced glutathione levels by 53% [44].
In conclusion, because of the absence of clinical trials regarding the effects of PSO on cognition of patients with MCI or other cognitive disorders, the aim of the present study was to identify the potential benefits of PSO in MCI. After one year of treatment, it is proved that the PSO can be beneficial for people with MCI improving different domains of cognition. So, the innovation of the present study is that these results can expand the research in this field and encourage the use of PSO in holistic approaches that can be helpful even in the stage of MCI and lead to prevention of dementia.
A limitation of the present study is the number of the participants. However, similar approaches have examined the potential benefits of the natural compounds for even fewer participants. Another limitation was that the control group did not take a placebo but followed MeDi, which is also useful in prevention of AD. However, while there is no approved treatment for MCI, we strongly believe that not allocating MCI people in any interventional program is unethical since it constitutes a preclinical stage of dementia and if we deploy interventions, we may forestall the progression of the disease. Therefore, the MeDi is a prevention method useful for people with MCI and at the same time offers a more controlled baseline for both groups. If we had the opportunity to use placebo, perhaps our results could be even better. Our final suggestion is to go on with further research by conducting a multi-centered study with more participants from different cities or even different countries and with a placebo group.
CREDIT AUTHOR STATEMENT
Athanasios Chatzikostopoulos (Formal analysis; Project administration; Writing – original draft); Moses Gialaouzidis (Data curation); Anna Koutoupa (Investigation; Resources); Magda Tsolaki (Conceptualization; Supervision; Writing – review & editing).
ACKNOWLEDGMENTS
We would like to warmly thank the company Pomstar Rodi Hellas, for providing PSO free of charge.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data available upon duly justified request.
REFERENCES
[1] | American Psychiatric Association, Washington American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders, 5th ed., American Psychiatric Association, Washington, DC, USA. |
[2] | Vermunt L , Sikkes SA , Van Den Hout A , Handels R , Bos I , Van Der Flier WM. , Kern S , Ousset PJ , Marruf P , Skoog I , Verhey F , Freund-Levi Y , Tsolaki M , Wallin A , Rikkert MO , Soininen H , Spiru L , Zetterberg H , Blennow K , Sheltens P , Coley N ((2019) ) Duration of preclinical, prodromal, and dementia stages of Alzheimer’s disease in relation to age, sex, and APOE genotype. Alzheimers Dement 15: , 888–898. |
[3] | Winblad B , Palmer K , Kivipelto M , Jelic V , Fratiglioni L , Wahlund LO , Nordberg A , Bäckman L , Albert M , Almkvist O , Arai H , Basun H. , Blennow K. , De Leon M , DeCarli C , Erkinjuntti T , Giacobini C , Graff C , Hardy J , Jack C , Jorm A , Ritchie K , Van Duijn C , Visser P , Petersen RC ((2004) ) Mild cognitive impairment–beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J Intern Med 256: , 240–246. |
[4] | Wortmann M ((2012) ) Dementia: A global health priority-highlights from an ADI and World Health Organization report. Alzheimers Res Ther 4: , 1–3. |
[5] | Downer B , Al Snih S , Chou LN , Kuo YF , Raji M , Markides KS , Ottenbacher KJ ((2021) ) Changes in health care use by Mexican American Medicare beneficiaries before and after a diagnosis of dementia. J Gerontol A 76: , 534–542. |
[6] | Guzman-Martinez L , Calfío C , Farias GA , Vilches C , Prieto R , Maccioni RB ((2021) ) New frontiers in the prevention, diagnosis, and treatment of Alzheimer’s disease. J Alzheimers Dis 82: , S51–S63. |
[7] | Calfio C , Gonzalez A , Singh SK , Rojo LE , Maccioni RB ((2020) ) The emerging role of nutraceuticals and phytochemicals in the prevention and treatment of Alzheimer’s disease. J Alzheimers Dis 77: , 33–51. |
[8] | García-Casares N , Gallego Fuentes P , Barbancho MÁ , López-Gigosos R , García-Rodríguez A , Gutierrez-Bedmar M ((2021) ) Alzheimer’s disease, mild cognitive impairment and Mediterranean diet. A systematic review and dose-response meta-analysis. J Clin Med 10: , 4642. |
[9] | Mantzorou M , Vadikolias K , Pavlidou E , Tryfonos C , Vasios G , Serdari A , Giaginis C. ((2021) ) Mediterranean diet adherence is associated with better cognitive status and less depressive symptoms in a Greek elderly population. Aging Clin Exp Res 33: , 1033–1040. |
[10] | Ballarini T , van Lent DM , Brunner J , Schröder A , Wolfsgruber S , Altenstein S , Brosseron F , Buerger K , Dechent P , Dobisch L , Duzel E , Ertl-Wagner B , Fliessbach K , Freiesleben S , Frommann I , Glanz W , Hauser D , Haynes JD , Heneka MT , Janowitz D , Kilimann I , Laske C , Maier F , Danielle C , Munk M , Perneczky R , Peters O , Priller J , Ramirez A , Rauchmann BS , Roy N , Scheffler K , Schneider A , Spottke A , Spruth EJ , Teipel S , Vukovich R , Wiltfang J , Jenssen F , Wagner M ((2021) ) Mediterranean diet, Alzheimer disease biomarkers, and brain atrophy in old age. Neurol 96: , 2920–2932. |
[11] | Hoscheidt S , Sanderlin AH , Baker LD , Jung Y , Lockhart S , Kellar D , Whitlow C , Hanson A , Friedman S , Register T , Leverenz J , Craft S ((2022) ) Mediterranean and Western diet effects on Alzheimer’s disease biomarkers, cerebral perfusion, and cognition in mid-life: A randomized trial. Alzheimers Dement 18: , 457–468. |
[12] | Siervo M , Shannon OM , Llewellyn DJ , Stephan BC , Fontana L ((2021) ) Mediterranean diet and cognitive function: From methodology to mechanisms of action. Free Radic Biol Med 176: , 105–117. |
[13] | Tastan Ö , Baysal T (2018) Adulteration analysis of pomegranate juice. In Frontiers in Drug Safety, Adulteration Analysis of Some Foods and Drugs, pp. 91-100. |
[14] | Fahmy H , Hegazi N , El-Shamy S , Farag MA ((2020) ) Pomegranate juice as a functional food: A comprehensive review of its polyphenols, therapeutic merits, and recent patents. Food Funct 11: , 5768–5781. |
[15] | Siddarth P , Li Z , Miller KJ , Ercoli L M , Merril D , Henning SM , Heber D , Small GW ((2020) ) Randomized placebo-controlled study of the memory effects of pomegranate juice in middle-aged and older adults. Am J Clin Nutr 111: , 170–177. |
[16] | Abu-Taweel GM , Al-Mutary MG ((2021) ) Pomegranate juice reverses AlCl3-Induced neurotoxicity and improves learningand memory in female mice. Environ Res 199: , 111270. |
[17] | Subash S , Braidy N , Essa MM , Zayana AB , Ragini V , Al-Adawi S , AlAsmi A , Guillemin GJ ((2015) ) Long-term (15 mo) dietarysupplementation with pomegranates from Oman attenuates cognitive andbehavioral deficits in a transgenic mice model of Alzheimer’sdisease. Nutrition 31: , 223–229. |
[18] | Mehdi A , Lamiae B , Samira B , Ramchoun M , Abdelouahed K , Tamas F , Hicham B ((2022) ) Pomegranate (Punica granatum L.) attenuates neuroinflammation involved in neurodegenerative diseases. Foods 11: , 2570. |
[19] | Kim YE , Hwang CJ , Lee HP , Kim CS , Son DJ , Ham YW , Hellstrom M , Han SB , Kim HS , Park EK , Hong JT ((2017) ) Inhibitory effect of punicalagin on lipopolysaccharide-induced neuroinflammation, oxidative stress and memory impairment via inhibition of nuclear factor-kappaB. Neuropharmacology 117: , 21–32. |
[20] | Velagapudi R , Baco G , Khela S , Okorji U , Olajide O ((2016) ) Pomegranate inhibits neuroinflammation and amyloidogenesis in IL-1β-stimulated SK-N-SH cells. Eur J Nutr 55: , 1653–1660. |
[21] | Ghorbanzadeh R , Rezaei K ((2017) ) Optimization of an aqueous extraction process for pomegranate seed oil. J Am Oil Chem Soc 94: , 1491–1501. |
[22] | Paul A , Radhakrishnan M ((2020) ) Pomegranate seed oil in food industry: Extraction, characterization, and applications. Trends Food Sci Technol 105: , 273–283. |
[23] | Khoddami A , Man YBC , Roberts TH ((2014) ) Physico-chemical properties and fatty acid profile of seed oils from pomegranate (Punica granatum L.) extracted by cold pressing. Eur J Lipid Sci Technol 116: , 553–562. |
[24] | Paul D , Dey TK , Chakraborty A , Dhar P (2018) Promising functional lipids for therapeutic applications. In Role of Materials Science in Food Bioengineering, Grumezescu A, Holban A, eds. Academic Press, pp. 413-449. |
[25] | Białek A , Białek M , Lepionka T , Tober E , Czauderna M ((2021) ) The quality determination of selected commercial online purchased edible pomegranate seed oils with new argentometric liquid chromatography method. J Diet Suppl 18: , 351–371. |
[26] | Boroushaki MT , Mollazadeh H , Afshari AR ((2016) ) Pomegranate seed oil: A comprehensive review on its therapeutic effects. Int J Pharm Sci Rev Res 7: , 430–442. |
[27] | Sarkaki A , Farbood Y , Hashemi S , Rad MR ((2015) ) Pomegranate seed hydroalcoholic extract improves memory deficits in ovariectomized rats with permanent cerebral hypoperfusion/ischemia. Avicenna J Phytomed 5: , 43–55. |
[28] | Al-Sabahi BN , Fatope MO , Essa MM , Subash S , Al-Busafi SN , Al-Kusaibi FS , Manivasagam T ((2017) ) Pomegranate seed oil: Effect on 3-nitropropionic acid-induced neurotoxicity in PC12 cells and elucidation of unsaturated fatty acids composition. Nutr Neurosci 20: , 40–48. |
[29] | Shrivas M , Khunt D , Shrivas M , Misra M ((2023) ) Studies on pomegranate seed oil enriched galantamine hydrobromide microemulsion: Formulation, antioxidant and neuroprotective potential. }. Pharm Dev Technol 28: , 1–28. |
[30] | George N , AbuKhader M , Al Balushi K , Al Sabahi B , Khan SA ((2022) ) An insight into the neuroprotective effects and molecular targets of pomegranate (Punica granatum) against Alzheimer’s disease. Nutr Neurosci 26: , 1–22. |
[31] | Panagiotakos DB , Pitsavos C , Arvaniti F , Stefanadis C ((2007) ) Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev Med 44: , 335–340. |
[32] | Fountoulakis KN , Tsolaki M , Chantzi H , Kazis A ((2000) ) Mini mental state examination (MMSE): A validation study in Greece. Am J Alzheimers Dis Other Demen 15: , 342–345. |
[33] | Poptsi E , Moraitou D , Eleftheriou M , Kounti-Zafeiropoulou F , Papasozomenou C , Agogiatou C , Bakoglidou E , Batsila G , Liapi D , Markou N , Nikolaidou E , Ouzouni F , Soumpourou A , Vasiloglou M , Tsolaki M ((2019) ) Normative data for the Montreal Cognitive Assessment in Greek older adults with subjective cognitive decline, mild cognitive impairment and dementia. J Geriatr Psychiatry Neurol 32: , 265–274. |
[34] | Tsolaki M , Fountoulakis K , Nakopoulou E , Kazis A , Mohs RC ((1997) ) Alzheimer’s Disease Assessment Scale: The validation of the scale in Greece in elderly demented patients and normal subjects. Dement Geriatr Cogn Disord 8: , 273–280. |
[35] | Efklides A , Yiultsi E , Kangellidou T , Kounti F , Dina F , Tsolaki M ((2002) ) Wechsler Memory Scale, Rivermead Behavioral Memory Test, and Everyday Memory Questionnaire in healthy adults and Alzheimer’s patients. Eur J Psychol Assess 18: , 63–77. |
[36] | Messinis L , Tsakona I , Malefaki S , Papathanasopoulos P ((2007) ) Normative data and discriminant validity of Rey’s Verbal Learning Test for the Greek adult population. Arch Clin Neuropsychol 22: , 739–752. |
[37] | Tsatali M , Emmanouel A , Gialaouzidis M , Avdikou K , Stefanatos C , Diamantidou A , Kouroundi E , Messini C , Tsolaki M ((2022) ) Rey complex figure test (RCFT): Norms for the Greek older adult population. Appl Neuropsychol Adult 29: , 958–966. |
[38] | Zalonis I , Kararizou E , Triantafyllou NI , Kapaki E , Papageorgiou S , Sgouropoulos P , Vassilopoulos D ((2008) ) A normative study of the trail making test A and B in Greek adults. Clin Neuropsychol 22: , 842–850. |
[39] | Kounti F , Tsolaki M , Kiosseoglou G ((2006) ) Functional cognitive assessment scale (FUCAS): A new scale to assess executive cognitive function in daily life activities in patients with dementia and mild cognitive impairment. Hum Psychopharmacol 21: , 305–311. |
[40] | Cano SJ , Posner HB , Moline ML , Hurt SW , Swartz J , Hsu T , Hobart JC ((2010) ) The ADAS-cog in Alzheimer’s disease clinical trials: Psychometric evaluation of the sum and its parts. J Neurol Neurosurg Psychiatry 81: , 1363–1368. |
[41] | Bookheimer SY , Renner BA , Ekstrom A , Li Z , Henning SM , Brown JA , Jones M , Moody T , Small GW ((2013) ) Pomegranate juice augments memory and FMRI activity in middle-aged and older adults with mild memory complaints. J Evid Based Complementary Altern Med 2013: , 1–14. |
[42] | Guerra-Vázquez CM , Martínez-Ávila M , Guajardo-Flores D , Antunes-Ricardo M ((2022) ) Punicic acid and its role in the preventionof neurological disorders: A review. Foods 11: , 252. |
[43] | Akbarian M , Mirzavi F , Amirahmadi S , Hosseini M , Alipour M , Feizi H , Rajabian A ((2022) ) Amelioration of oxidative stress, cholinergic dysfunction, and neuroinflammation in scopolamine-induced amnesic rats fed with pomegranate seed. Inflammopharmacology 30: , 1021–1035. |
[44] | Jacob J , Rajiv P , Gopalan R , Lakshmanaperumalsamy P ((2019) ) An overview of phytochemical and pharmacological potentials of Punica granatum L. Pharmacogn J 11: , 1167–1171. |


