
Programme Dementia Prevention (pdp): A Nationwide Program for Personalized Prevention in Luxembourg
Abstract
Background:
With continuously aging societies, an increase in the number of people with cognitive decline is to be expected. Aside from the development of causative treatments, the successful implementation of prevention strategies is of utmost importance to reduce the high societal burden caused by neurodegenerative diseases leading to dementia among which the most common cause is Alzheimer’s disease.
Objective:
The aim of the Luxembourgish “programme dementia prevention (pdp)” is to prevent or at least delay dementia in an at-risk population through personalized multi-domain lifestyle interventions. The current work aims to provide a detailed overview of the methodology and presents initial results regarding the cohort characteristics and the implementation process.
Methods:
In the frame of the pdp, an extensive neuropsychological evaluation and risk factor assessment are conducted for each participant. Based on the results, individualized multi-domain lifestyle interventions are suggested.
Results:
A total number of 450 participants (Mean age = 69.5 years; SD = 10.8) have been screened at different recruitment sites throughout the country, among whom 425 participants (94.4%) met the selection criteria.
Conclusions:
We provide evidence supporting the feasibility of implementing a nationwide dementia prevention program and achieving successful recruitment of the target population by establishing a network of different healthcare providers.
INTRODUCTION
As life expectancy rises and societies continue to age, the public health sector faces increasingly complex challenges pertaining to age-related illnesses. Approximately 50 million people worldwide were living with dementia in 2018 according to the World Alzheimer Report and this number is projected to triple to 152 million by 2050. In 2018, this phenomenon has already incurred significant costs estimated at around 1 trillion US$ in public and private areas and is expected to increase substantially, reaching approximately 2 trillion US$ by 2030 [1]. In Luxembourg, prevalence estimates of 3.8% for dementia and 26.1% for cognitive complaints have been obtained for adults over the age of 64 years [2]. The number of older adults affected by dementia in Luxembourg is expected to increase substantially, as the demographic population aged 65+ is expected to nearly double over the coming decades [3].
During the last two decades, extensive research has been conducted to study risk factors for cognitive decline and dementia. In 2017, the Lancet Dementia Prevention, Intervention and Care Commission presented scientific evidence from observational, epidemiological and interventional studies encouraging an ambitious approach towards dementia prevention [4]. The authors highlighted nine potentially modifiable risk factors believed to reduce the risk of developing dementia by more than one third. First, the level of education has been proven to influence the risk of developing dementia later in life. Furthermore, hypertension, diabetes, physical inactivity, overweight, smoking, hearing loss, as well as depression and social isolation have also been identified as key risk factors. Notably, in 2020, the list expanded to introduce three additional risk factors: excessive alcohol consumption, traumatic brain injury and air pollution. The aforementioned risk factors account for approximatively 40% of dementia cases worldwide [5]. A systematic review conducted by Deckers and colleagues [6] identified a similar set of risk factors, while also including hyperlipidemia. According to these authors, coronary heart disease and renal dysfunction are also to be considered as additional potential risk factors. They also emphasize that the role of diet and cognitive activity needs to be further investigated. Within the frame of our program, we adhere to the aforementioned risk factors, but acknowledge that the list of addressed risk factors is to be adapted and expanded in case of new, emerging scientific findings.
Since studies into single-domain interventions targeting the previously mentioned modifiable risk factors have yielded only mixed results, researchers of the “Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER)” opted to explore multi-domain interventions. Their results imply that cognitive functioning may be maintained or even improved in an older adult at-risk population after having benefited from a combination of cognitive training, exercise, diet counselling, and vascular risk management [7]. To meet the need for multi-domain lifestyle interventions [8], the World-Wide FINGER network was launched in 2017 as the first global network dedicated to multi-domain lifestyle intervention trials for dementia prevention. Its mission is to adapt and harmonize the efforts for dementia prevention across countries [9].
Our program aligns with these efforts aiming to prevent dementia through multi-domain lifestyle interventions. The uniqueness of our program, however, resides in the personalized approach by offering multi-domain interventions tailored to each participant. Although the importance of early dementia prevention is well established, to our knowledge, guidelines for the implementation of such programs into real world health care are missing. The current work aims to bridge this gap by sharing experiences and the methodology proven successful to recruit individuals at risk to a nationwide program for dementia prevention in Luxembourg.
METHODS
Design and aim
The “programme dementia prevention (pdp)” is a nationwide integrated care concept whose aim is to prevent or at least delay dementia in an at-risk cohort by reducing modifiable risk factors through personalized multi-domain interventions. Within the program, we aim to translate research findings related to the prevention of dementia into an applied personalized prevention program. More precisely, the aim of the current work is to describe the design for a successful implementation of a first nationwide integrated care concept for precision prevention. The program was approved by the National Research Ethics Committee (CNER Ref: 201511/01).
Participant selection criteria
To be eligible for enrolment in the program, participants must be at least 18 years old at the time of inclusion and must have the capacity to consent. Other prerequisites to participate in the pdp are a referral letter from the treating physician and an affiliation to the Luxembourgish health care system.
The target population includes participants presenting with a mild cognitive impairment (MCI), which is defined as a syndrome characterized by cognitive decline exceeding what is expected for an individual’s age and educational level but which does not interfere with activities of daily living [10–13]. In the frame of the pdp, MCI is diagnosed if at least one neuropsychological test result is lower than 1.5 standard deviation (SD) below the mean (z-score < –1.5 SD) compared to age-, sex- and education-adjusted normative data, or if at least two test results are located between 1.5 SD and 1 SD below the normative mean (–1.5 SD≤z-scores < –1 SD).
Given that individuals with a subjective cognitive decline (SCD) are at higher risk of developing cognitive impairment in the future [14], we also include those participants to ensure early prevention. SCD is defined by a subjective decline in cognitive capacity compared to a previous level of functioning in the absence of objectified cognitive deficits measured through standardized neuropsychological tests [15]. In the frame of the pdp, the absence of cognitive deficits is established when all neuropsychological test results are located at or above 1 SD below the normative mean (z-scores ≥ – 1 SD) with allowance to have one test result located between 1.5 SD and 1 SD below the normative mean (–1.5 SD ≤ z-score < –1 SD).
Furthermore, participants in a preclinical stage, who are carriers of known mutations in genes related to Alzheimer’s disease, such as mutations in the amyloid precursor protein (APP), presenilin 1 (PS1), or presenilin 2 (PS2) genes, as well as carriers of the risk allele ɛ4 in the APOE gene [16], are also included into the program.
On the other hand, individuals who refuse to sign the informed consent or who are younger than 18 years of age are excluded from participation in the program. Furthermore, individuals who present neither subjective nor objective cognitive impairment are not enrolled. Finally, people with dementia do not qualify for the intervention program. Dementia is characterized by cognitive or behavioral symptoms in at least two domains that represent a deterioration from a previous level of functioning, cannot be explained by delirium or psychiatric disorders, and interfere with the ability to function at work or in usual activities [17].
It should be noted that the categorization regarding the cognitive status is based on the neuropsychological assessment. The close collaboration with referring physicians and the requirement for each participant to provide recent blood analysis and reports from previous examinations enable us to gain insights into potential pre-existing comorbidities. Recommendations from the program to the referring physicians are made for further differential diagnostic procedures to exclude non-neurological causes, which might interfere with the participant’s cognitive performance in case these have not yet beenconducted.
Program structure
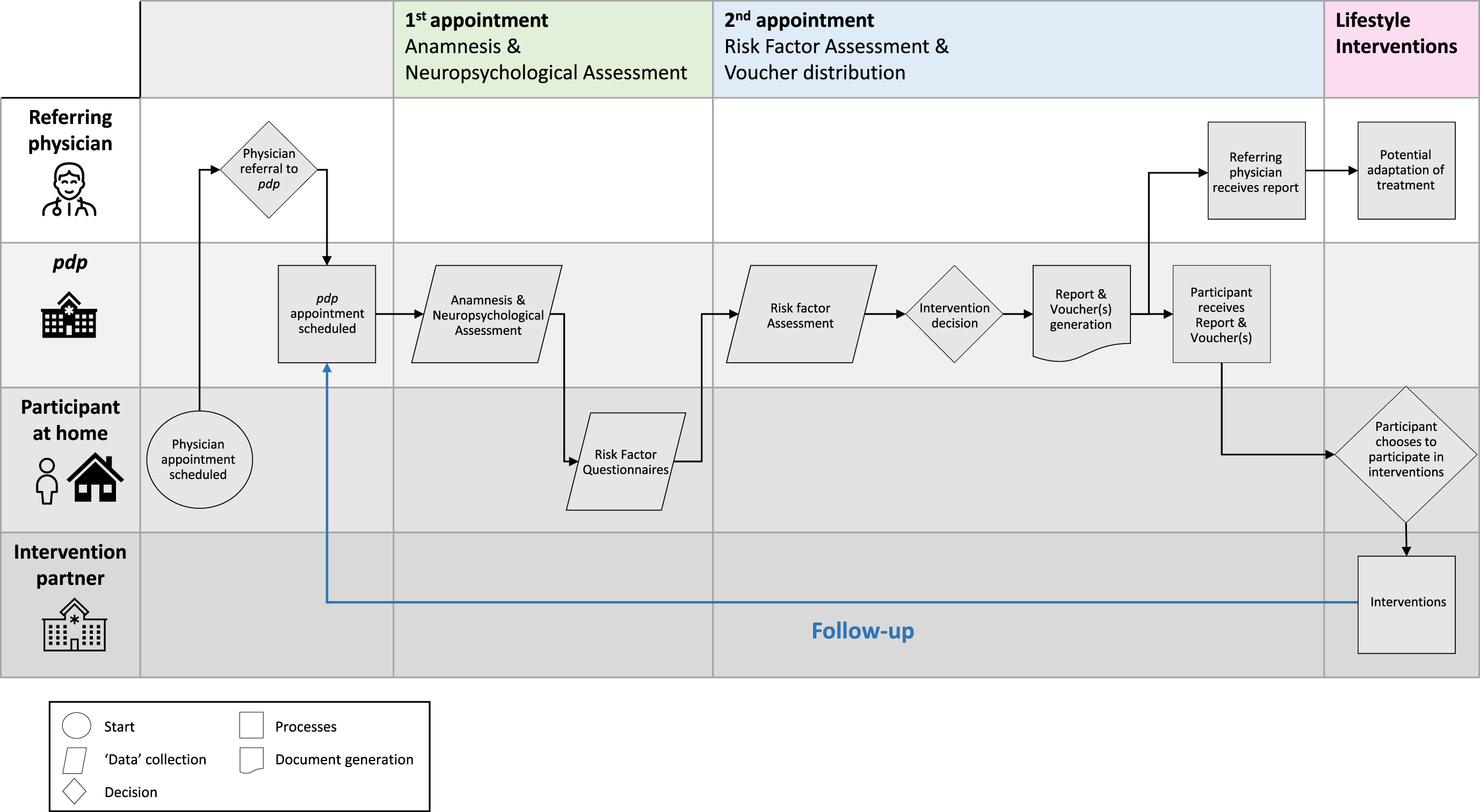
Participation in the program follows a predefined pathway (Fig. 1), which is composed of an initial referral, a neuropsychological assessment and a thorough risk factor profiling. Following these steps, the results of their assessments are communicated, and participants are provided with vouchers giving access to the multi-domain interventions. Finally, regular longitudinal follow-ups are foreseen for participants who meet the inclusion criteria. The different steps are described below in further detail.
Fig. 1
Recruitment pathway of participants in the frame of the pdp.
Referral letter
As previously mentioned, participants must obtain a referral letter from their treating physician. Additionally, participants are encouraged to provide a list of their current medication and preexisting medical history as well as to provide further relevant information from previous medical reports or analyses (e.g., blood analyses, results of brain imaging, cerebrospinal fluid analysis).
Neuropsychological assessment
During the first appointment, an anamnesis is conducted, and participants are invited to undergo an extensive neuropsychological assessment of an approximate duration of two hours, conducted by certified (neuro-) psychologists. The interpretation of results takes into consideration age, sex, and level of education of the participant. The test battery consists of standardized tools designed to evaluate different cognitive functions such as memory, attention, executive functions as well as visuo-spatial abilities and language (Table 1) [18–30].
Table 1
Neuropsychological assessment - Summary of neuropsychological tests and measured cognitive functions [18–28]
| Cognitive functions | Tests / Subtests | |
| Global cognition | Montreal Cognitive Assessment (MoCA) | [18] |
| Mini-Mental State Examination (MMSE) | [19] | |
| Auditory-verbal short-term memory | Digit Span - Forward | [20] |
| Auditory-verbal working memory | Digit Span - Backward | [20] |
| Visuo-spatial short-term memory | Spatial Span - Forward | [21] |
| Visuo-spatial working memory | Spatial Span - Backward | [21] |
| Verbal episodic long-term memory | Rappel libre / rappel indicé à 16 items (RL/RI-16) | [22] |
| Visual episodic long-term memory | Constructional Praxis Recall (CERAD)a | [23] |
| Processing speed | Digit-Symbol-Coding | [20] |
| Visuo-motor speed | Trail Making Test - Part A | [24] |
| Processing speed - Color naming | Stroop Test - Color Naming | [24] |
| Processing speed - Word reading | Stroop Test - Word Reading | [24] |
| Word initiation | Verbal Fluency - Semantic (animals, 2 min) | [24] |
| Verbal Fluency - Phonemic (letter “p”, 2 min) | [24] | |
| Mental flexibility | Trail Making Test - Part B &Part B-A | [24] |
| Inhibitory control | Stroop Test - Interference | [24] |
| Planification | Rey-Osterrieth Complex Figure / | [25, 26] |
| Modified Taylor Complex Figure | [27] | |
| Visuo-constructive capacities | Rey-Osterrieth Complex Figure / | [25, 26] |
| Modified Taylor Complex Figure | [27] | |
| Constructional Praxis (CERAD) | [23] | |
| Visual perception | Figures enchevêtrées (PEGV) | [28] |
| Language - Denomination | Boston Naming Test (CERAD)a | [23] |
CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; PEGV, Protocole d‘évaluation des gnosies visuelles; atests which have replaced former tools (DMS48 [29]; Grémots [30]). The list of tests used in pdp has been adapted in the course of the implementation process and the use of tests may be adapted on a case-by-case basis if needed. This may be the case if the originally intended test cannot be performed due to various restricting factors, such as language, age, or education level or if the use of a complimentary test adds information that could be relevant for the referring physician in the clinical context.
Risk factor assessment and additional questionnaires
The second part of the assessment consists of questionnaires and psychometric scales [31–51] with the objective of evaluating the presence of the different risk factors for dementia [4–6] as well as to capture additional outcome variables, such as cognitive, behavioral, social, and psychological aspects (Table 2). The modifiable risk factors assessed by these questionnaires are cardiovascular diseases and high blood pressure, hypercholesterolemia, diabetes, non-Mediterranean diet, obesity, physical inactivity, lack of cognitive activities, depression, social isolation, alcohol and tobacco consumption, renal dysfunction, and hearing loss. To determine and visualize an individual’s potential for improvement in terms of dementia risk reduction, we employ the LIfestyle for BRAin health (LIBRA) index [37], which has been extended in our program to better capture and at least partially quantify individual health-related risk factors. The second in-person appointment is scheduled once the questionnaires, which have been provided during the first appointment and should be filled at home by the participant, have been returned to the pdp.
Table 2
Risk factor assessment and other outcome variables - Summary of scales / questionnaires [31–46]
| Domains | Scales / Questionnaires | |
| Medical aspects | Medication list, Medical history, Medical records (pdp) | |
| Participation | Participation Questionnaire (pdp) | |
| Subjective Cognitive Complaints | Complainer Profile Identification (CPI) | [31] |
| Subjective Cognitive Decline - Informant | Short Form of the Informant Questionnaire on Cognitive Decline in the Elderly (Short IQCODE) | [32] |
| Anamnestic Data | Anamnesis (pdp) | |
| Demographic Data | Demographics (pdp) | |
| Autonomy in Activities of Daily Living | Katz Index of Independence in Activities of Daily Living (ADL) | [33] |
| Lawton Instrumental Activities of Daily Living Scale (IADL) | [34] | |
| Clinical Dementia Rating (CDR) | [35] | |
| Functional Activities Questionnaire (FAQ) | [36] | |
| Risk Factor Assessment | Lifestyle for Brain Health (LIBRA) | [37] |
| Extended Risk Factor Assessment (pdp)a | ||
| Depression | Geriatric Depression Scale (GDS-15)b / Beck Depression Inventory (BDI)b | [38, 39] |
| Social Isolation | Index of social isolation | [40] |
| Loneliness | Three-Item Loneliness Scaleb | [41] |
| Social Support | Social Support Questionnaire (F-SozU, K-14) | [42] |
| Anxiety | Generalized Anxiety Disorder Scale (GAD-7) | [43] |
| Perceived Stress | Perceived Stress Scale (PSS-10) | [44] |
| Apathy | Starkstein Apathy Scale (SAS) | [45] |
| Quality of Life | WHO Quality of Life - BREF (WHOQOL-BREF) | [46] |
(pdp), Questionnaires designed in the frame of pdp tailored to the program’s needs; WHO, World Health Organization; acontains an adapted version of the Alcohol Use Disorders Identification Test (AUDIT) [47]]; bcut-offs for the decision to address these risk factors: GDS-15: ≥6 [48], BDI: ≥10 [49], Three-Item Loneliness Scale: ≥6 [50]. The list of questionnaires used in pdp has been adapted in the course of the implementation process (e.g., previously used questionnaire: Risk Factor Questionnaire (RFQ-U) [51]) and the use of questionnaires may be adapted on a case-by-case basis if needed. This may be the case if the originally intended questionnaire cannot be performed due to various restricting factors, such as language, age, or education level or if the use of a complimentary questionnaire adds information that could be relevant for the referring physician in the clinical context.
Voucher system for personalized multi-domain lifestyle interventions
Based on the results of the neuropsychological assessment as well as the identified risk factors, the (neuro-) psychologist establishes a tailored intervention program for each participant. Participation in pdp is free of charge for the participants, and they receive vouchers that are directly cleared between the healthcare provider and the pdp. To encourage participants to take action and to use the vouchers in a short delay, an expiry date is fixed and clearly indicated on each voucher. Given that activities may start at different time points and that, in some cases, there are longer waiting periods, this date does not represent the date by which the activity should be started or completed, but the date by which the participants must have contacted the voucher partner to express their interest and, if applicable, to be registered on the waiting list.
With respect to the recommended activities, participants can select from a broad range of choices. First of all, participants are offered cognitive training which may take place either in a group- or an individual setting under the guidance of a trained health professional. Recently, this option has been expanded to include paper-pencil training or digital training which the participant can complete at home. The cognitive training targets different cognitive functions such as memory, attention, executive functions, visuo-spatial abilities as well as language. Particularly in the individual sessions as well as in the digital home-based training, the level of difficulty may be adapted to the participant’s needs. In addition, participants are encouraged to engage in physical and/or social activities depending on their risk factors. Participants can choose from a wide range of different options, such as yoga, Nordic walking, aqua-gym, strength training, and Qi Gong. The physical activities offered range from aerobic exercises to strength training or flexibility exercises and can take place either indoors or outdoors. In case of specific physical limitations or post-operative discomfort, the health care specialists may adapt the training to the individual’s specific needs and adjust the difficulty or intensity of the training. For the physical and social activities, care was taken that the range of offered activities is particularly broad, allowing participants to choose activities aligned with their personal interests. Additionally, a dietary consultancy is recommended for participants with an unhealthy diet or facing health issues related to dietary habits. Individual sessions with a dietician offer a distinct advantage as they allow for personalized recommendations tailored to the individual’s unique circumstances taking into account various factors such as the financial situation, lifestyle, dietary regime or pre-existing health conditions. Finally, to improve psychological well-being in case of depression, the participant is encouraged to seek help through psychological health counselling sessions with a certified psychologist, which may serve as an orientation towards other offers in this context. It is important to note that the list of offered activities and voucher partners is constantly being adapted to allow participants to select activities, which best fit their needs.
To measure the adherence to the offered activities and to obtain information regarding the regularity of participation, dates on which the participant has taken part in the activities are tracked by the voucher partners. In case of the paper-pencil training, an exercise journal is provided to the participant where the progress can be recorded. For the digital training, data regarding the level reached and the frequency of the training is available. Finally, some voucher partners provide feedback in form of letters including various information regarding motivation, participation rate or action points.
Communication of results
Results of the neuropsychological testing, the risk factor assessment and recommendations for individualized lifestyle interventions are communicated directly to the participant during the second appointment. Explanations are individually adapted to the participant’s level of understanding and the result discussion is supported by visualization aids. Finally, participants as well as the referring physicians receive a written report of the test results.
Longitudinal follow-up
Finally, longitudinal follow-ups are scheduled in yearly intervals to assess the evolution of cognitive performance, as well as the presence of risk factors over time. To ensure comparability between visits, follow-up visits are structured similar to the baseline visit. Concerning the neuropsychological assessment, emphasis is placed on using parallel versions of the tests, when possible, to avoid learning effects. During the follow-up visit, participants are again offered specific voucher options according to their individual risk profile.
Data storage, scheduling system, and email-encryption
Given that a large amount of sensitive and confidential data is generated in the frame of the program, it is of utmost importance to rely on secure ways to handle and store this data. Hence, to allow secure storage and management of personally identifiable information (PII), a scheduling system, entitled SMASCH (Smart Scheduling System) [52], has been established by the Luxembourg Centre for Systems Biomedicine (LCSB). Aside from storing data, the tool is designed to schedule and manage appointments and generate time-saving letter templates.
Pseudonymized data are stored in Research Electronic Data Capture (REDCap), an electronic data capture tool, which allows the centralized and highly secured storage of the data [53, 54]. The web-based application has been designed not only to support data capture, but also to share and harmonize data across different sites and institutions. For increased security, REDCap is encrypted, the access to the site is restricted and employs two-factor authentication.
To ensure General Data Protection Regulation (GDPR)-compliant communication with the treating physicians and the voucher partners, a secured email system is used to send encrypted emails.
Implementation strategy
Pdp’s communication strategy aims to raise awareness about the possibilities of dementia prevention and facilitate the recruitment of our target population through various communication channels and outreach activities targeted to medical doctors, allied healthcare professionals, potential future voucher partners, participants, and the general public. Since awareness regarding the potential to reduce the risk of developing dementia seems to remain limited [55], the pdp team regularly participates in outreach events, such as informative events or conferences in the field of neurodegenerative diseases. Furthermore, printed flyers and factsheets are designed to provide additional information on the pdp and modalities of participation as well as relevant information on risk factors and recommendations on how to stay physically and mentally fit. In addition, participants, treating physicians and partners receive regular updates about the program and the latest research findings through newsletters. Due to the linguistic diversity in Luxembourg, communication material is made available in four languages, namely German, French, English and Luxembourgish. Finally, the program has been largely covered in mass media, such as newspapers, radio, and TV. The pdp-website (https://www.pdp.lu/) [56] provides key information about the program for patients and medical professionals and features detailed information on pdp objectives, activities, and associated risk factors.
To accommodate for reduced mobility [57] of the target population and to facilitate access to the program for people living in different regions, pdp offers different regional recruitment hubs geographically spread throughout the country (Fig. 2) [58–60].
Fig. 2
Geographical locations of pdp-recruitment hubs and voucher activities in Luxembourg. A) Map presenting locations of pdp-recruitment hubs and voucher activities. B) Map legend. C) Enlargement of activities/hubs within Luxembourg City. D) Population density map of Luxembourg. From Map of cantons of Luxembourg [political map], by Sémhur [wikigraphist], 2009, Wikimedia Commons [58]; Brinkhoff, T. (2022). City Population. (http://www.citypopulation.de). CC BY 3.0. [59]; Icons by Icons8 (https://icons8.com/) [60].
![Geographical locations of pdp-recruitment hubs and voucher activities in Luxembourg. A) Map presenting locations of pdp-recruitment hubs and voucher activities. B) Map legend. C) Enlargement of activities/hubs within Luxembourg City. D) Population density map of Luxembourg. From Map of cantons of Luxembourg [political map], by Sémhur [wikigraphist], 2009, Wikimedia Commons [58]; Brinkhoff, T. (2022). City Population. (http://www.citypopulation.de). CC BY 3.0. [59]; Icons by Icons8 (https://icons8.com/) [60].](https://content.iospress.com:443/media/jad/2024/97-2/jad-97-2-jad230794/jad-97-jad230794-g002.jpg)
Scientific Advisory Board
To ensure the scientific quality of the program and to monitor the operations along state-of-the-art guidelines and practices of international research on the prevention of dementia, a Scientific Advisory Board (SAB) was implemented at the launch of pdp. The SAB is composed of five internationally renowned researchers and experts in the field of dementia research, care, and prevention, who meet annually and provide a scientific evaluation of the program, allowing for continuous improvement of the program.
RESULTS
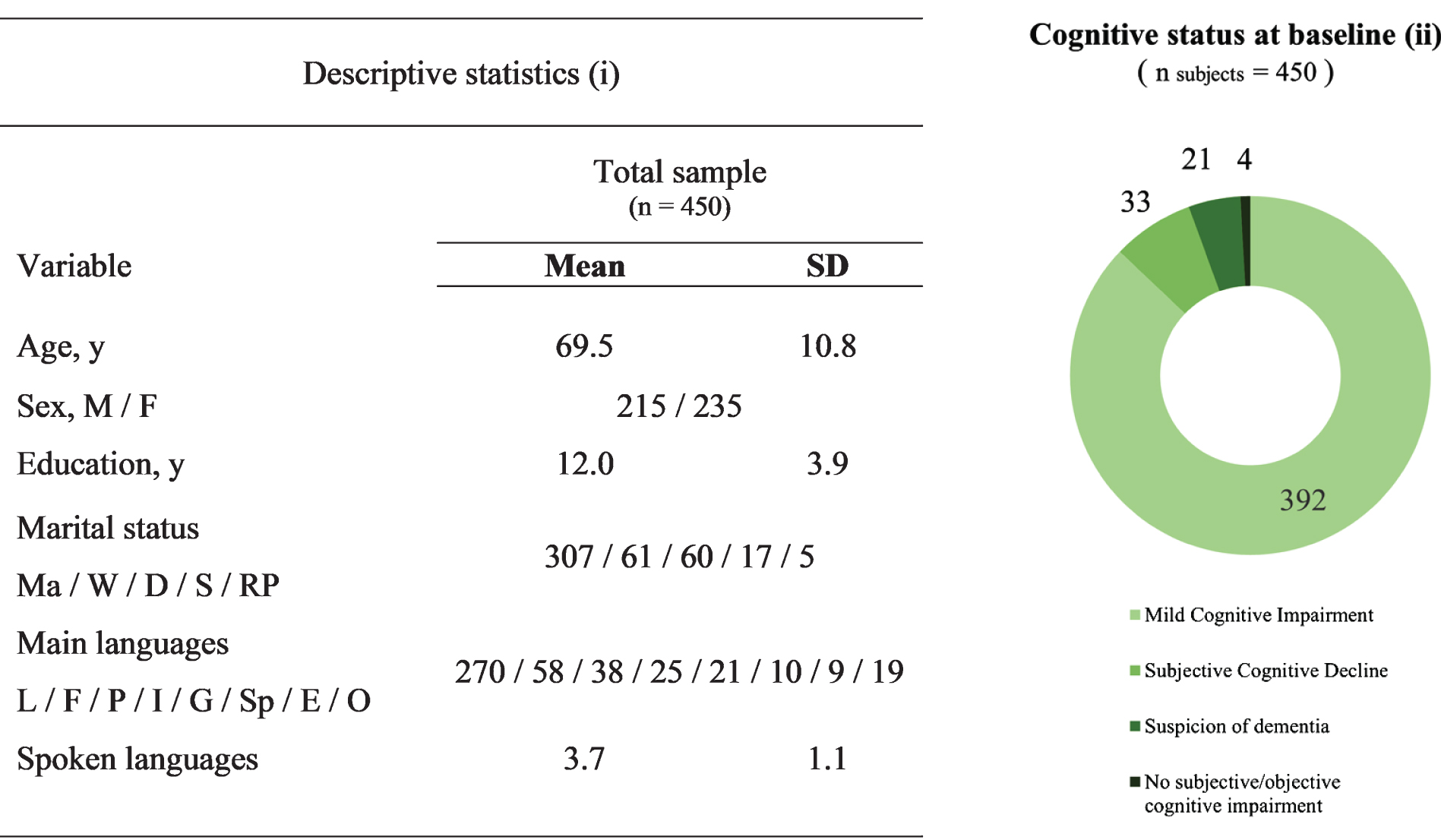
A total number of 450 participants with a mean age of 69.5 years (SD = 10.8 years), ranging from 31 years to 90 years have been recruited since the launch of the program in its current form in February 2018. The cohort consists of 215 male (47.8%) and 235 female (52.2%) participants with a mean number of 12.0 (SD = 3.9) years of education. Regarding the marital status, 307 (68.2%) participants are married, 61 (13.6%) are widowed, 60 (13.3%) are divorced, 17 (3.8%) are single, and 5 (1.1%) live in a registered partnership. With 270 (60.0%) participants indicating Luxembourgish as their native language, this is the most spoken main language, followed by French (n = 58 (12.9%)), Portuguese (n = 38 (8.4%)), Italian (n = 25 (5.6%)), German (n = 21 (4.7%)), Spanish (n = 10 (2.2%)), and English (n = 9 (2.0%)). Finally, 19 (4.2%) participants indicated an “Other” language as their main language. Overall, participants speak a mean number of 3.7 languages (SD = 1.1).
Regarding the cognitive status at baseline, the current sample is composed of 392 (87.1%) participants presenting with an MCI and 33 (7.3%) subjects with an SCD. In total, 21 (4.7%) participants had to be excluded because of a “suspicion of dementia” and were referred to specialized centers. Finally, 4 (0.9%) participants showed neither subjective nor objective cognitive decline (Fig. 3).
Fig. 3
Demographic data for pdp-participants (n = 450) (i) and Cognitive status at baseline (ii). n, sample size; y, number of years; M, male; F, female; Ma, married; W, widowed; D, divorced; S, single; RP, registered partnership; L, Luxembourgish; F, French; P, Portuguese; I, Italian; G, German; Sp, Spanish; E, English; O, Other.
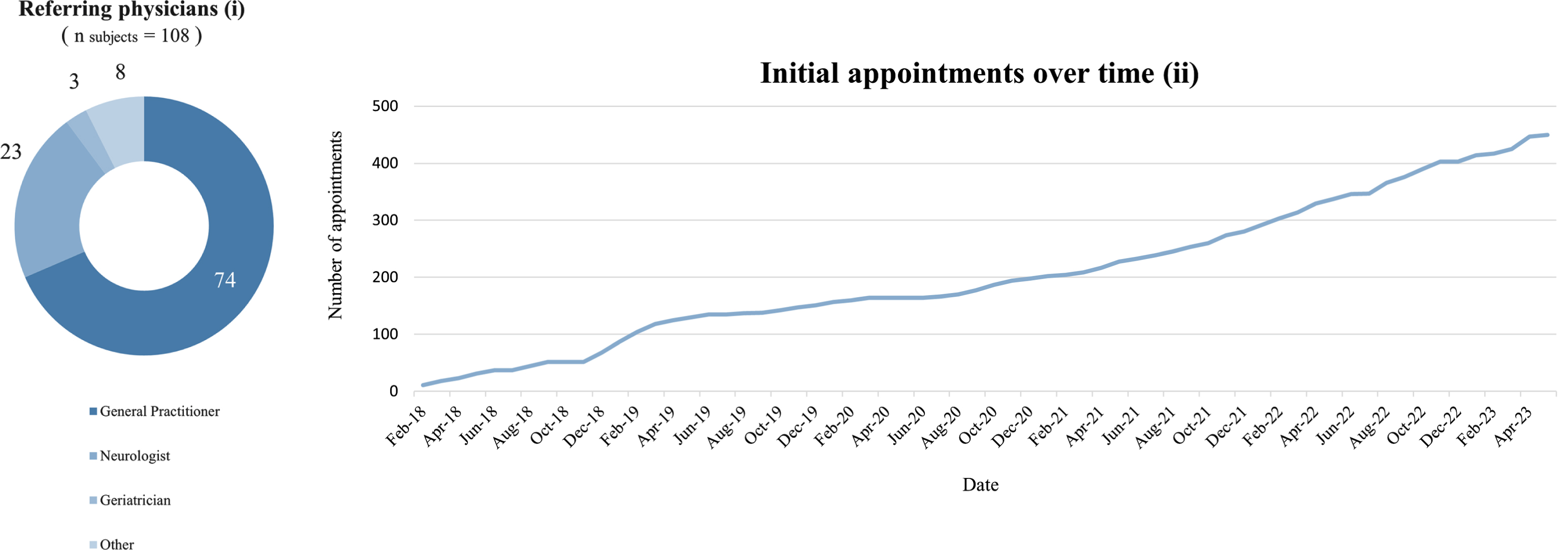
Out of a total number of 108 referring treating physicians, 74 (68.5%) were general practitioners, 23 (21.3%) neurologists, 3 (2.8%) geriatricians, and 8 (7.4%) physicians with other specializations. The referring physicians to the pdp are 74 of 534 (13.9%) general practitioners practicing in Luxembourg, 23 of 41 (56.1%) practicing neurologists and 3 of 13 (23.1%) practicing geriatricians [61]. Continuous referrals by the referring physicians lead to a constantly increasing number of initial in-person appointments (Fig. 4).
Fig. 4
Specialization of referring physicians (i) and cumulative data of initial appointments over time (ii).
In our cohort, the mean interval between the first appointment and the second appointment is 69.9 days (SD = 67.6). Five participants completed the neuropsychological assessment on the same day as the risk factor assessment. Since the launch of the program, a total number of 549 participants have been referred. The difference between this number and the 450 recruited participants mentioned earlier is attributable to the fact that some individuals have initially been referred by the physician but were not or have not yet been recruited into the program. As such, for 38 (38.4%) out of these 99 individuals, appointments have been scheduled to take place in the next three months. Finally, the reasons for non-participation can be multifaceted and may include motivational factors, physical inability, or practical reasons.
As previously mentioned, we offer different regional consultation sites throughout the country to increase access to pdp. 85 (18.9%) of the 450 participants took advantage of this opportunity and were recruited for at least one appointment through additional recruitment hubs (Fig. 2).
11 months after the launch of the program, a survey was conducted to receive feedback from the referring physicians who had at least once referred patients to pdp by that point in time (n = 66) out of which 13 (19.7%) completed the survey. The results indicate that the physicians agree on the importance of an individualized dementia prevention program in Luxembourg and that the continuation of pdp would be highly appreciated in the interest of their patients. Overall, the referring doctors indicated that they were very satisfied with the content of the reports and that the recommendations given were very helpful for their clinical practice. The detailed results of the survey sent to the doctors are available in the Supplementary Material.
DISCUSSION
The “programme dementia prevention (pdp)” is a nationwide integrated care concept whose aim is to prevent or at least delay cognitive decline in a target population at risk for dementia in Luxembourg and whose methodology and first experiences are reported here. The concept is based on research that has shown promising results regarding the effectiveness of multi-domain interventions in this context [7–9]. However, our program expands beyond these studies by translating research findings into an integrated care concept for secondary prevention by taking a personalized approach and offering each participant an individualized set of lifestyle interventions which are tailored to their needs (e.g., temporal availabilities, mobility of the participant, spatial distance between residence and voucher partner, work status, personal interests) in order to improve the adherence to the suggested lifestyle interventions.
The successful implementation critically relied on the establishment of a multidisciplinary network of different healthcare professionals across different domains, pursuing the shared goal of encouraging and supporting individuals to adopt a healthier lifestyle and control for potentially modifiable risk factors. This network consists of various healthcare professionals, ranging from medical doctors to physio- or occupational therapists as well as (neuro-) psychologists. The interventions, which are free of charge for pdp-participants, are delivered by local partners across the country who offer a diversified range of activities. Among these services are, for example, cognitive training, physical and social activities, as well as psychological and dietary counselling. The list of offered activities is constantly being adapted based on the most recent scientific findings and the cohort’s needs to cover the largest possible area and to allow the participants to choose among as broad a range of activities as possible.
Close collaboration with the referring physicians has also proven to be crucial. Within the framework of the pdp, this has been evident through the continuously increasing number of referrals by more than 100 different physicians as well as the positive feedback on a survey among referring physicians during the program’s early stages of implementation. The results of this questionnaire reveal that physicians acknowledge the importance of dementia prevention programs, recognizing the value of the activities offered as part of the program as well as the written report, which is generated for each participant after every visit. Although we consider the response rate of physicians to already be satisfactory, we are actively exploring the possibility of conducting satisfaction surveys for both physicians and participants, to obtain additional feedback with the ultimate goal of further improving the program.
Furthermore, results demonstrate that we were able to reach our target population, comprised of individuals presenting with an SCD or MCI. It is important to note that the few participants who showed a more advanced cognitive decline associated with a loss of autonomy in activities of daily living were not simply excluded from the program but were referred to institutions specialized in the treatment of people with dementia and their relatives. Participants belonging to the target population are invited for follow-up visits with the aim of tracking their evolution in terms of cognitive performance and the presence of risk factors.
Given that a substantial part of the population remains unaware of the possibility that they could potentially influence their risk of developing dementia [55], a major focus of the program is to raise awareness about its objectives and the possibilities of dementia prevention among the general public and other healthcare professionals by engaging in numerous outreach activities, such as informative events and conferences. The development of different printed information material, such as flyers, factsheets, and newsletters, as well as the use of other communication channels, such as mass media (newspaper, TV, and radio) or the pdp-website, have been conducive to this goal and will further be expanded in the future to reach an even broader population including younger individuals to start raising awareness about dementia prevention as early as possible.
Hurdles and barriers to implementation
A first barrier to successfully implementing the program was the fact that older participants often show reduced mobility [57]. To overcome these difficulties, we offer participants the flexibility to choose their preferred location from several recruitment sites available across the country, including the northern and southern regions as well as the center of the country (Fig. 2). Similarly, intervention services were selected to minimize participants’ travel distances. In the meantime, there are also offers, such as cognitive training in a digital form, from which participants can benefit at home at their convenience.
Since a large proportion of our participants encounter cognitive difficulties, it was necessary to adapt some of the processes to the participants’ needs. To streamline administrative steps and reduce the number of missed appointments, participants receive, for example, not only a written confirmation of the appointment including important information regarding their participation but also a reminder by phone a few days prior to the appointment to reduce the number of missed appointments.
Furthermore, when communicating results, care is taken to ensure that explanations are adapted to the participant’s level of understanding and supported with visualization aids, such as the LIBRA index [37] or tables containing a detailed overview of the neuropsychological test results. In all the efforts, it has been shown to be favorable to involve the relatives, particularly in the case of already more pronounced cognitive difficulties.
To improve compliance and facilitate the previously mentioned collaboration with the referring physicians, feedback is provided in form of a written report after every visit, detailing the results of the neuropsychological assessment, identified risk factors and recommendations regarding voucher activities and differential diagnostic options, all which may be conducive to the diagnostic process.
Limitations
The continuous expansion and adaptation to the range of lifestyle interventions offered, which is crucial to improving the quality of the program and increasing participants’ motivation, makes it challenging to compare the effectiveness of the multi-domain interventions. This difficulty arises from the fact that the suggested set of lifestyle interventions varies from participant to participant. In this context, it would be beneficial to have a control group to better measure the effectiveness of the various multi-domain interventions.
Luxembourg’s linguistic context poses another challenge to the program due to the lack of tests and questionnaires available in the three main languages spoken in the country, which are Luxemburgish, French, and German. Moreover, there is a general absence of neuropsychological tests validated in Luxembourgish. For this reason, it was necessary to translate some of the tests and questionnaires. In addition, all written documentation must always be translated into several languages. To account for the multilingual context, it is imperative that team members are multilingual and easily adapt to linguistic variations.
Outlook
Our experiences in the framework of pdp will inform future research in the field of dementia prevention and healthy aging on how to best implement prevention programs based on personalized lifestyle interventions in real-world healthcare. The detailed neuropsychological assessment and the collection of data related to medical, cognitive, psychological, and social aspects gathered through the different questionnaires and psychometric scales result in a deeply phenotyped cohort of individuals at risk for dementia. Thanks to longitudinal follow-ups, it will not only be possible to assess the effectiveness of individualized multi-domain interventions in mitigating risk factors contributing to the onset of dementia, but also to analyze important motivational factors that may influence individuals’ adherence to the suggested lifestyle changes. Qualitative data analysis has the potential to help to shed light on these last aspects. Ultimately, the pdp provides an ideal basis for future precision medicine approaches by already covering the aspects “personalized” and“prevention”.
Since modifiable risk factors appear to play a role not only in late life, but already in middle life and early life [4, 5], we seek to expand our efforts in terms of dementia prevention beyond participants with first cognitive complaints to a younger target population. To further raise awareness about the possibilities of dementia prevention in the general population and to meet the need for early education about dementia and its risk factors, we foresee employing digital tools, such as an application available via mobile (smartphone) and web browser.
Finally, our experience in implementing a nationwide integrated care network for personalized prevention has yielded valuable insights into hurdles and barriers that need to be overcome during the implementation process and may contribute to guidelines for rolling out similar concepts in other countries or regions.
ACKNOWLEDGMENTS
We would like to thank all participants as well as their families who have put their trust in us for their commitment to the program. Furthermore, we would like to thank the Luxembourgish Ministry of Health for initiating and continuously supporting the pdp. We are also very thankful to the Centre Hospitalier de Luxembourg (CHL) for their pivotal role in the implementation of this integrated care program for prevention and the strong commitment of CHL staff to our program, which was instrumental in the advancement and success of pdp. Moreover, we would like to thank all partners offering lifestyle interventions within our program, without whom the success of pdp would not be possible, especially the colleagues of “ZithaAktiv” from the “Hôpitaux Robert Schuman”, the “Centre Hospitalier du Nord (CHdN)”, the “Association Nationale des Diététiciens du Luxembourg (ANDL)”, the different “Club Seniors” belonging to “help asbl” and the “Club Senior Schwaarze Wee”, as well as the “Lëtzebuerger Verein fir Gediechtnistraining asbl”. Furthermore, we would like to thank the referring physicians as well as the accompanying services for people with dementia and their relatives, such as the “Info-Zenter Demenz” and the “Association Luxembourg Alzheimer (ALA)” in Luxembourg. Additionally, we are grateful to be able to offer pdp-consultations in the premises of the different “Maison Médicales” in Luxembourg City, Belval and Ettelbruck as well as the “Hôpitaux Robert Schuman - Clinique Ste Marie”. We thank the communication team members Lucie Debroux and Miriam Fougeras as well for the translations of the communication material. We would like to thank Claudia Vila Verde, Cindy Amado Ferrao, Joy Wolff, Kendra Domingues De Sousa, Nathalie Vanpeteghem and especially Linda Hansen for their valuable support. We also would like to thank the members of the “National Centre for Excellence in Research on Parkinson’s disease (NCER-PD)” - Consortium for the close collaboration.
pdp is part of and supported by the “EU-FINGERS” (https://eufingers.com/) and the “World Wide FINGERS” network.
FUNDING
The program is supported by the Luxembourgish Ministry of Health.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding authors.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-230794.
REFERENCES
[1] | Patterson C ((2018) ) World Alzheimer Report 2018. The state of the art of dementia research: New frontiers. Alzheimer’s Disease International, London. |
[2] | Perquin M , Diederich N , Pastore J , Lair M-L , Stranges S , Vaillant M , MemoVie Group ((2015) ) Prevalence of dementiaand cognitive complaints in the context of high cognitive reserve: A population-based study. PLoS One 10: , e0138818. |
[3] | European Commission. Directorate General for Employment SA, Inclusion (2021) Long-Term Care Report: Trends, Challenges and Opportunities in an Ageing Society. Volume II, Country Profiles. Publications Office Luxembourg. |
[4] | Livingston G , Sommerlad A , Orgeta V , Costafreda SG , Huntley J , Ames D , Ballard C , Banerjee S , Burns A , Cohen-Mansfield J , Cooper C, Fox N, Gitlin LN, Howard R, Kales HC, Larson EB, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbaek G, Teri L, Mukadam N ((2017) ) Dementia prevention, intervention, and care. Lancet 390: , 2673–2734. |
[5] | Livingston G , Huntley J , Sommerlad A , Ames D , Ballard C , Banerjee S , Brayne C , Burns A , Cohen-Mansfield J , Cooper C , Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbaek G, Teri L, Mukadam N ((2020) ) Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396: , 413–446. |
[6] | Deckers K , van Boxtel MP , Schiepers OJ , de Vugt M , Muñoz Sánchez JL , Anstey KJ , Brayne C , Dartigues JF , Engedal K , Kivipelto M , Ritchie K, Starr JM, Yaffe K, Irving K, Verhey FR, Köhler S ((2015) ) Target risk factors for dementia prevention: A systematic review and Delphiconsensus study on the evidence from observational studies. Int J Geriatr Psychiatry 30: , 234–246. |
[7] | Ngandu T , Lehtisalo J , Solomon A , Levälahti E , Ahtiluoto S , Antikainen R , Bäckman L , Hänninen T , Jula A , Laatikainen T , Lindström J, Mangialasche F, Paajanen T, Pajala S, Peltonen M, Rauramaa R, Stigdotter-Neely A, Strandberg T, Tuomilehto J, Soininen H, Kivipelto M ((2015) ) A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 385: , 2255–2263. |
[8] | Kivipelto M , Mangialasche F , Ngandu T ((2018) ) Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat Rev Neurol 14: , 653–666. |
[9] | Kivipelto M , Mangialasche F , Snyder HM , Allegri R , Andrieu S , Arai H , Baker L , Belleville S , Brodaty H , Brucki SM , et al. ((2020) ) World-Wide FINGERS Network: A global approach to risk reduction and prevention of dementia. Alzheimers Dement 16: , 1078–1094. |
[10] | Petersen RC , Smith GE , Waring SC , Ivnik RJ , Tangalos EG , Kokmen E ((1999) ) Mild cognitive impairment: Clinical characterization and outcome. Arch Neurol 56: , 303–308. |
[11] | Petersen RC ((2004) ) Mild cognitive impairment as a diagnostic entity. J Intern Med 256: , 183–194. |
[12] | Petersen RC , Caracciolo B , Brayne C , Gauthier S , Jelic V , Fratiglioni L ((2014) ) Mild cognitive impairment: A concept in evolution. J Intern Med 275: , 214–228. |
[13] | Gauthier S , Reisberg B , Zaudig M , Petersen RC , Ritchie K , Broich K , Belleville S , Brodaty H , Bennett D , Chertkow H , Cummings JL, de Leon M, Feldman H, Ganguli M, Hampel H, Scheltens P, Tierney MC, Whitehouse P, Winblad B ((2006) ) Mild cognitive impairment. Lancet 367: , 1262–1270. |
[14] | Slot RE , Sikkes SA , Berkhof J , Brodaty H , Buckley R , Cavedo E , Dardiotis E , Guillo-Benarous F , Hampel H , Kochan NA , Lista S, Luck T, Maruff P, Molinuevo JL, Kornhuber J, Reisberg B, Riedel-Heller SG, Risacher SL, Roehr S, Sachdev PS, Scarmeas N, Scheltens P, Shulman MB, Saykin AJ, Verfaillie SC, Visser PJ, Vos SJ, Wagner M, Wolfsgruber S, Jessen F, van der Flier WM ((2019) ) Subjective cognitive decline and rates of incident Alzheimer’s disease and non–Alzheimer’s disease dementia. Alzheimers Dement 15: , 465–476. |
[15] | Jessen F , Amariglio RE , Buckley RF , van der Flier WM , Han Y , Molinuevo JL , Rabin L , Rentz DM , Rodriguez-Gomez O , Saykin AJ , Sikkes SA, Smart CM, Wolfsgruber S, Wagner M ((2020) ) The characterisation of subjective cognitive decline. Lancet Neurol 19: , 271–278. |
[16] | St George-Hyslop PH ((2000) ) Molecular genetics of Alzheimer’s disease. Biol Psychiatry 47: , 183–199. |
[17] | McKhann GM , Knopman DS , Chertkow H , Hyman BT , Jack CR Jr , Kawas CH , Klunk WE , Koroshetz WJ , Manly JJ , Mayeux R , Mohs RC, Morris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH ((2011) ) The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 263–269. |
[18] | Nasreddine ZS , Phillips NA , Bédirian V , Charbonneau S , Whitehead V , Collin I , Cummings JL , Chertkow H ((2005) ) The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am GeriatrSoc 53: , 695–699. |
[19] | Folstein MF , Folstein SE , McHugh PR ((1975) ) “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[20] | Wechsler D ((1997) ) WAIS-III, Wechsler adult intelligence scale: Administration and scoring manual. Psychological Corporation, New York, NY. |
[21] | Wechsler D ((1997) ) Psychological Corporation. WMS-III: Wechsler memory scale administration and scoring manual. |
[22] | Van der Linden M , Coyette F , Poitrenaud J , Kalafat M , Calicis F , Wyns C , Adam S ((2004) ) II. L’épreuve derappel libre/rappel indicé à 16 items (RL/RI-16). In L’Evaluation des troubles de la mémoire, Van der Linden M, ed. Solal, Marseille. |
[23] | Morris JC , Heyman A , Mohs RC , Hughes J , van Belle G , Fillenbaum G , Mellits E , Clark C ((1989) ) The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 39: , 1159–1165. |
[24] | Godefroy O ((2008) ) Fonctions exécutives et pathologies neurologiques et psychiatriques: Évaluation enpratique clinique, Groupe de Boeck. |
[25] | Rey A ((1941) ) L’examen psychologique dans les cas d’encephalopathie traumatique. Arch Psychol 28: , 286–340. |
[26] | Osterrieth PA ((1944) ) Le test de copie d’une figure complexe; contribution a l’etude de la perception et de la memoire. Arch Psychol 30: , 206–356. |
[27] | Taylor LB ((1969) ) Localisation of cerebral lesions by psychological testing: Chapter XIV. Neurosurgery 16: , 269–287. |
[28] | Agniel A , Joanette Y, Doyon B, Duchein C ((1992) ) Protocole Montréal-Toulouse: Évaluation des gnosies visuelles et auditives, L’Ortho éd. |
[29] | Barbeau E , Tramoni E , Joubert S , Mancini J , Ceccaldi M , Poncet M ((2004) ) Evaluation de la mémoire dereconnaissance visuelle: Normalisation d’une nouvelle épreuve en choix forcé (DMS48) et utilité enneuropsychologie clinique. L’évaluation des troubles de la mémoire, pp. 85–101. |
[30] | Bézy C , Renard A , Pariente J ((2016) ) GRÉMOTS: Évaluation du langage dans les pathologiesneurodégénératives, De Boeck supérieur. |
[31] | Lubitz AF , Eid M , Niedeggen M ((2018) ) Complainer Profile Identification (CPI): Properties of a new questionnaire on subjective cognitive complaints. Aging Neuropsychol Cogn 25: , 99–121. |
[32] | Jorm A ((1994) ) A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): Development and cross-validation. Psychol Med 24: , 145–153. |
[33] | Katz S , Ford AB , Moskowitz RW , Jackson BA , Jaffe MW ((1963) ) Studies of illness in the aged. The Index of ADL: A standardized measure of biological and psychosocial function. JAMA 185: , 914–919. |
[34] | Lawton MP , Brody EM ((1969) ) Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 9: , 179–186. |
[35] | Hughes CP , Berg L , Danziger W , Coben LA , Martin RL ((1982) ) A new clinical scale for the staging of dementia. Br J Psychiatry 140: , 566–572. |
[36] | Pfeffer RI , Kurosaki TT , Harrah C Jr , Chance JM , Filos S ((1982) ) Measurement of functional activities in older adults in the community. J Gerontol 37: , 323–329. |
[37] | Schiepers OJ , Köhler S , Deckers K , Irving K , O’Donnell CA , van den Akker M , Verhey FR , Vos SJ , de Vugt ME , van Boxtel MP ((2018) ) Lifestyle for Brain Health (LIBRA): A new model for dementia prevention. Int J Geriatr Psychiatry 33: , 167–175. |
[38] | Sheikh JI , Yesavage JA ((1986) ) Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin Gerontol 5: , 165–173. |
[39] | Beck AT , Ward CH , Mendelson M , Mock J , Erbaugh J ((1961) ) An inventory for measuring depression. Arch Gen Psychiatry 4: , 561–571. |
[40] | Shankar A , McMunn A , Banks J , Steptoe A ((2011) ) Loneliness, social isolation, and behavioral and biological health indicators in older adults. Health Psychol 30: , 377. |
[41] | Hughes ME , Waite LJ , Hawkley LC , Cacioppo JT ((2004) ) A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res Aging 26: , 655–672. |
[42] | Sommer G , Fydrich T ((1991) ) Entwicklung und Überprüfung eines Fragebogens zur sozialen Unterstützung (F-SOZU). Diagnostica 37: , 160–178. |
[43] | Spitzer RL , Kroenke K , Williams JB , Löwe B ((2006) ) A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med 166: , 1092–1097. |
[44] | Cohen S , Kamarck T , Mermelstein R ((1983) ) A global measure of perceived stress. J Health Soc Behav 24: , 385–396. |
[45] | Starkstein SE , Mayberg HS , Preziosi T , Andrezejewski P , Leiguarda R , Robinson R ((1992) ) Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 4: , 134–139. |
[46] | Whoqol-Group ((1998) ) Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med 28: , 551–558. |
[47] | Saunders JB , Aasland OG , Babor TF , De la Fuente JR , Grant M ((1993) ) Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 88: , 791–804. |
[48] | Herrmann N , Mittmann N , Silver IL , Shulman KI , Busto UA , Shear NH , Naranjo CA ((1996) ) A validation study of the Geriatric Depression Scale short form. Int J Geriatr Psychiatry 11: , 457–460. |
[49] | Beck AT , Steer RA , Carbin MG ((1988) ) Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev 8: , 77–100. |
[50] | Steptoe A , Shankar A , Demakakos P , Wardle J ((2013) ) Social isolation, loneliness, and all-cause mortality in oldermen and women. Proc Natl Acad Sci U S A 110: , 5797–5801. |
[51] | U.S. Department of Health and Human Services. National Institute of Neurological Disorders and Stroke, https://www.commondataelements.ninds.nih.gov/report-viewer/23716/Risk%20Factor%20Questionnaire%20, Accessed March 27, 2023. |
[52] | Vega C , Gawron P , Lebioda J , Grouès V , Matyjaszczyk P , Pauly C , Smula E , Krüger R , Schneider R , Satagopam V ((2022) ) Smart Scheduling (SMASCH): Multi-appointment scheduling system for longitudinal clinical research studies. JAMA Open 5: , ooac038. |
[53] | Harris PA , Taylor R , Thielke R , Payne J , Gonzalez N , Conde JG ((2009) ) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42: , 377–381. |
[54] | Harris PA , Taylor R , Minor BL , Elliott V , Fernandez M , O’Neal L , McLeod L , Delacqua G , Delacqua F , Kirby J , Duda SN ((2019) ) The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 95: , 103208. |
[55] | Heger I , Deckers K , van Boxtel M , de Vugt M , Hajema K , Verhey F , Köhler S ((2019) ) Dementia awareness and risk perception in middle-aged and older individuals: Baseline results of the MijnBreincoach survey on the association between lifestyle and brain health. BMC Public Health 19: , 678. |
[56] | Programme Dementia Prevention (pdp), https://www.pdp.lu/en/, Accessed May 11, 2023. |
[57] | Rantakokko M , Mänty M , Rantanen T ((2013) ) Mobility decline in old age. Exerc Sport Sci Rev 41: , 19–25. |
[58] | Sémhur, Map of cantons of Luxembourg [political map], WikimediaCommons, CC-BY-SA 3.0, https://upload.wikimedia.org/wikipedia/commons/b/bb/Cantons_of_Luxembourg_map-blank.svg, Accessed June 18, 2022. |
[59] | Brinkhoff T, City population, CC BY 3.0, http://www.citypopulation.de, Accessed June 18, 2022. |
[60] | Icons8, https://icons8.de/, Accessed June 18, 2022. |
[61] | Statistiques.lu, https://lustat.statec.lu/vis?fs%5B0%5D=Th%C3%A8mes%2C1%7CConditions+sociales%23C%23%7CSant%C3%A9%23C3%23&pg=0&fc=Th%C3%A8mes&df%5Bds%5D=ds-release&df%5Bid%5D=DF_C3114&df%5Bag%5D=LU1&df%5Bvs%5D=1.0&pd=2015%2C2017&dq=.A, Accessed July 14, 2023. |

