
Photobiomodulation for Alzheimer’s Disease: Translating Basic Research to Clinical Application
Abstract
One of the challenges in translating new therapeutic approaches to the patient bedside lies in bridging the gap between scientists who are conducting basic laboratory research and medical practitioners who are not exposed to highly specialized journals. This review covers the literature on photobiomodulation therapy as a novel approach to prevent and treat Alzheimer’s disease, aiming to bridge that gap by gathering together the terms and technical specifications into a single concise suggestion for a treatment protocol. In light of the predicted doubling in the number of people affected by dementia and Alzheimer’s disease within the next 30 years, a treatment option which has already shown promising results in cell culture studies and animal models, and whose safety has already been proven in humans, must not be left in the dark. This review covers the mechanistic action of photobiomodulation therapy against Alzheimer’s disease at a cellular level. Safe and effective doses have been found in animal models, and the first human case studies have provided reasons to undertake large-scale clinical trials. A brief discussion of the minimally effective and maximum tolerated dose concludes this review, and provides the basis for a successful translation from bench to bedside.
INTRODUCTION
According to the American Alzheimer’s Association, 11% of Americans (aged 65 and older) suffer from Alzheimer’s disease (AD) [1]. There is a similar situation in Austria, where about 100,000 people (6.4% of Austrians aged 65 and older) suffer from AD, and this is predicted to reach 230,000 by the year 2050 [2]. This rise in numbers affected is mainly caused by the overall aging of the population with increased life expectancy, and the generation called “Baby-Boomers” (people born in the 1950s and 1960s) reaching the relevant age [2]. Because it affects such a large number of individuals, AD is becoming a major challenge to the health care system. About one billion Euro per year is spent on AD-care in Austria alone [2, 3], three quarters of which is non-medical expense related to personal assistance in the activities of daily life. Aside from being costly to patients and the state, AD also claims its toll on the quality of life of caregivers. Compared to people who are not affected by AD directly or indirectly, those who care for AD patients have shown weaker immune function, more pro-inflammatory proteins, as well as significantly shorter telomeres [4]. As yet there is no established medical treatment that can cure, prevent, or completely halt the progression of AD. The lack of treatment options is aggravated by the paucity of reliable diagnostic tools that could detect the presence of disease before the onset of symptoms. The pre-symptomatic period of AD may last for decades, but once symptoms start to appear, there is only a short therapeutic window before neurodegeneration renders the affected person completely dependent on external care.
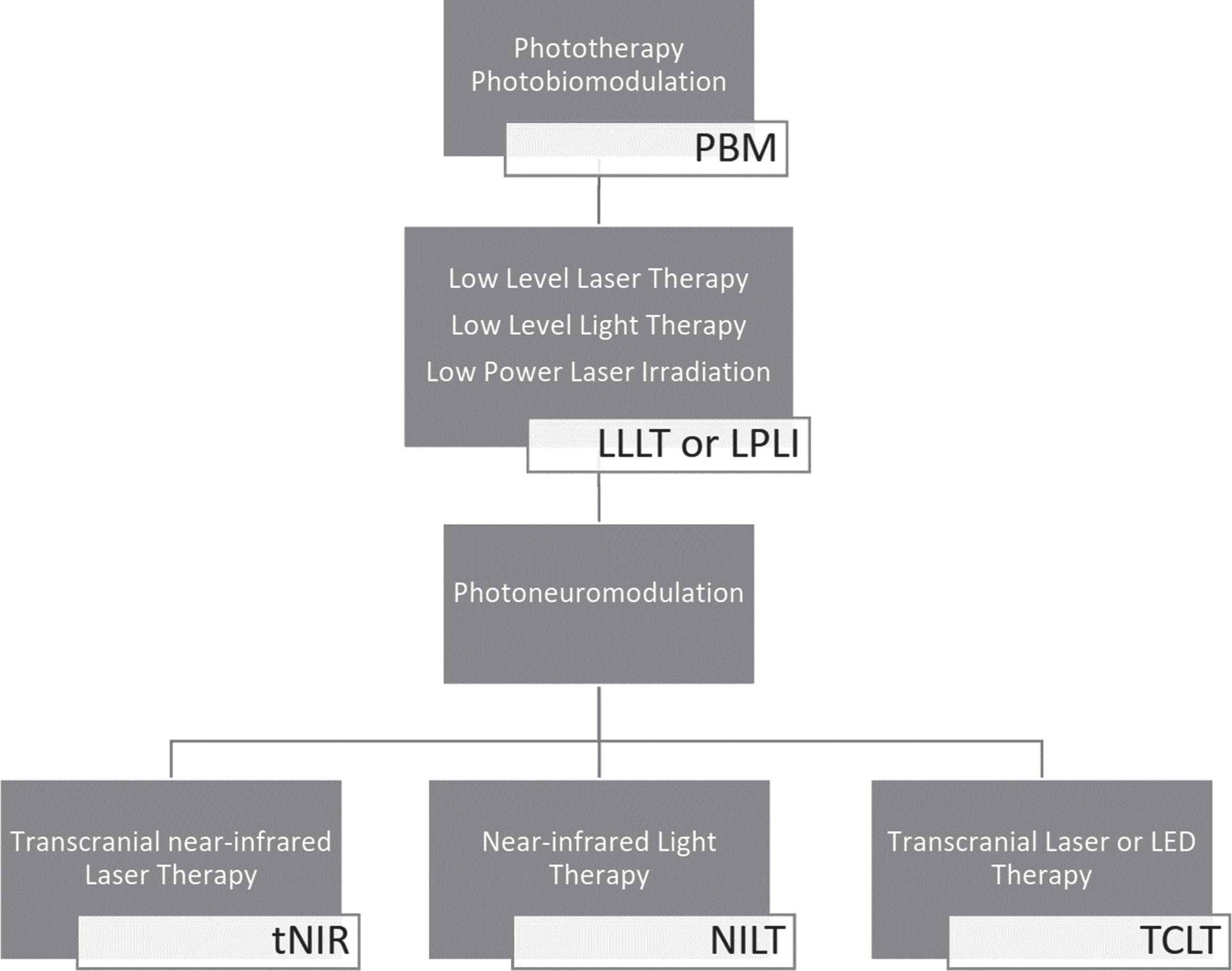
The key to a cure of AD may still lay in the dark, but there is an increasing amount of research being done that suggests that “literal enlightenment” might pave the way as a therapy against AD. Starting off by simply searching for “low level light therapy Alzheimer’s disease” in the PubMed database of the National Center for Biotechnology Information, it quickly becomes obvious that there are many different names for treatments utilizing light. While Kendric C. Smith suggested to use the “simple and correct term, phototherapy” [5], the scientific consensus has recently introduced the term “photobiomodulation therapy” for what used to be called low level laser/light therapy [6, 7]. As the literature also shows, it is possible to apply photobiomodulation to the brain transcranially, for which even more different terms and abbreviations exist. Figure 1 provides an overview of the multiple historic terms describing the same technique that is now grouped under the term photobiomodulation (PBM). Albeit the terminology might be outdated, limiting a literature search to the MeSH terms “Photobiomodulation” and “Alzheimer’s disease” falls a long way short of what can be found when performing a query containing a combination of all search terms from Fig. 1 and identifiers for AD and dementia. The necessity of including outdated and confusing terminology to find more articles concerning PBM for AD in humans [8–13] has motivated us to present this compelling treatment approach against neurodegeneration in a structured and concise matter.
Fig. 1
Many terms for the use of light in medical applications can be grouped under the umbrella term of photobiomodulation (PBM). When used against Alzheimer’s disease, photobiomodulation utilizes comparatively low power (low level) near-infrared laser or LED light which can be applied in a transcranial manner for photo-neuro-modulation.
LITERATURE SUMMARY
PBM is defined as the use of monochromatic or quasi-monochromatic light from a low power laser or light emitting diode (LED) source to modify or modulate biological functions. This modulation effect is based on the presence of chromophores in cells and tissues. These chromophores are molecules capable of absorbing light, whose excitation can influence further downstream molecules and biochemical pathways with the potential to exert a therapeutic effect [14]. The optical power output of any light source used for PBM is measured in Watts (W), in combination with a defined working distance this translates to an optical power density measured in W/m² at the point of application. Since only lower power densities are generally used in PBM, the units are usually converted and directly expressed as mW/cm² (1 W/m² corresponds to 0.1 mW/cm²). The total dose of optical energy received during a PBM treatment is measured in Joules (J), i.e., optical power in Watts multiplied by treatment time in seconds. In the literature reviewed for this article, the dose (energy density) is often stated over the treatment area, i.e., as J/cm².
One proposed target receptor molecule in PBM (widely discussed in the literature) is Complex IV (cytochrome c oxidase, CCO) of the mitochondrial respiratory chain. Photons are absorbed by CCO and increase the enzyme activity and thus the activity of the mitochondrial respiratory chain. Following this primary photon absorption event, the increased mitochondrial activity triggers secondary effects by activating pathways, which are involved in energy metabolism, cell homeostasis, and cell survival signaling. The secondary effects of PBM then amplify the primary effects by upregulating the levels of CCO protein itself and thus creating more of the target chromophore for additional PBM [11, 15].
As a treatment for neck pain, arthritis, and for carpal tunnel syndrome, PBM was shown to have an efficacy beyond a mere placebo effect [16], which led to the first low-level light therapy devices for pain relief being approved as medical devices by the U.S. Food and Drug Administration [17]. The power density delivered in PBM is generally too low to cause any concerns about tissue heating or thermal damage [18]. PBM has very few reported side-effects, and in animal studies it appears to be safe even when applied long term [19]. While the long-term data from animal studies can be extrapolated to human lifespans, it should be noted that the effects of long-term use of PBM have yet to be studied in human subjects.
Interest in the use of PBM for neuro-rehabilitation is growing, and it has already shown potential in treating traumatic brain injury, stroke, psychiatric disorders, as well as neurodegenerative disease both in animal models and in some clinical trials and case studies in humans [20–22].
Transcranial photobiomodulation with red to near infra-red light
To make PBM work on the brain, one can take advantage of the optical tissue window which allows wavelengths of light between approximately 650 nm and 1200 nm to travel through skin and skull, i.e., transcranially. The boundaries of the optical tissue window are defined by the strong absorption of hemoglobin and water. The penetration depth of wavelengths within those boundaries was measured for example by Tedford et al., who achieved a maximal penetration depth at a wavelength of 808 nm [23, 24]. Wang and Li evaluated this further and confirmed 810 nm as well as 660 nm to be the best suitable wavelengths for transcranial PBM [25].
In order to deliver light to the brain even deeper, without having to open the skull, Bungart et al. suggest the use of nanoparticles as an alternative light source for PBM [26]. These nanoparticles, termed ‘Bioluminescence Resonance Energy Transfer to Quantum Dots’ (BRET-Qdots), emit light in the near-infrared (NIR) wavelength range when their luciferase enzyme is activated with coelenterazine-h substrate. The reported downside to a nanoparticle treatment is concerns about the toxicity of the heavy metal content of the BRET-Qdots, which are yet to be fully investigated. Considering that blood has been observed to contain circulating cell-free respiratory competent mitochondria [27], and PBM also increases regional blood flow [8, 28, 29], a secondary mechanism might allow the transportation of the beneficial effects of PBM beyond the limits of direct light penetration.
Molecular mechanisms of photobiomodulation and their implications for Alzheimer’s disease
The impact of PBM on cell culture and animal models of AD has been extensively studied. A summary of the progress in each stage of development from basic research to preclinical and clinical Phase I and II trials is presented to form the basis for a treatment protocol.
PBM and AD in vitro
Sommer et al. reported that PBM reduced amyloid-β (Aβ25–35) aggregates in human neuroblastoma cells [30] and Yang et al. observed a reduction in Aβ-induced oxidative stress and inflammatory responses in rat primary cortical astrocytes [31]. Looking further at the implications of PBM on neuro-inflammatory pathways, Song et al. observed the effects of He-Ne laser light (632.8 nm) at doses from 3 J/cm² to 50 J/cm² on central nervous system resident macrophages (microglia) in human neuronal cells [32], and concluded that 20 J/cm² at intervals of 24 h was the optimal dose to attenuate cell death by reducing microglia-mediated neurotoxicity via the tyrosine-protein kinase Src/Syk signaling pathway [30].
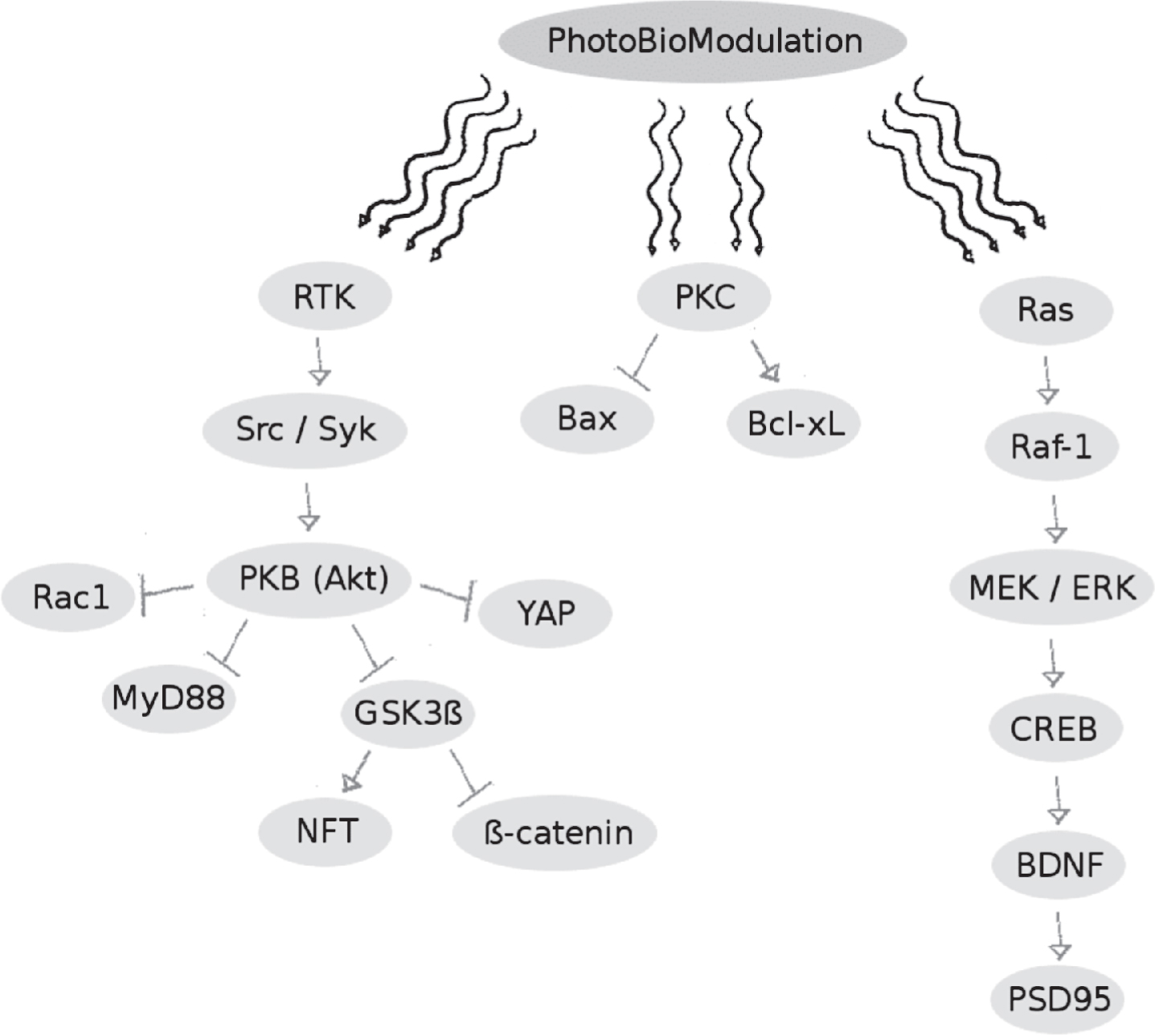
Liang et al. and Zhang et al. both examined the pathways leading to cell apoptosis following the addition of aggregated Aβ25–35 to neuronal-differentiated rat pheochromocytoma (PC12) cells, and observed that treatment with low power light using a He-Ne laser at 623.8 nm demonstrated a positive effect of PBM [33–35]. Zhang et al. specifically reported that protein kinase B was activated by PBM at a dose of 2 J/cm², which in turn promoted a series of anti-apoptotic effects such as inhibiting the translocation of the pro-apoptotic Yes-associated protein from the cytoplasm to the nucleus [35]. PBM using a He-Ne laser also appeared to activate protein kinase C, thereby affecting downstream apoptotic proteins in a dose-dependent manner [34]. Irradiation for 5 to 20 min with a power density of 0.52 mW/cm², corresponding to a delivered dose of 0.156 J/cm² to 0.624 J/cm², decreased levels of the pro-apoptotic Bax and either increased or did not affect levels of the anti-apoptotic Bcl-XL as compared to control cells treated with the toxic amyloid peptide Aβ25–35. This effect was reversed when an irradiation time of 40 min with 0.52 mW/cm² was reached, corresponding to a delivered dose of 1.248 J/cm², which illustrates the biphasic dose dependence of PBM when used to counteract Aβ-induced cell apoptosis. The reports from Liang et al. who used a 632.8 nm He-Ne laser at a dose of 2 J/cm² on neuronal PC12 cells treated with Aβ25–35 showed that PBM had a pro-survival effect by acting on the Akt/GSK3β/β-catenin pathway [33]. Building on the hypothesis that Aβ-induced neurotoxicity and dendrite atrophy may be a consequence of a deficiency of brain-derived neurotropic factor (BDNF), Meng et al. reported that extracellular signal–regulated kinase could be activated with a He-Ne laser at doses from 0.5 J/cm² to 4 J/cm² applied to Aβ25–35-treated human neuronal cells, which upregulated BDNF in a CREB-dependent manner [36]. A summary of the cell signaling effects of PBM in vitro is shown in Fig. 2.
Fig. 2
Summary of the signaling pathways influenced by photobiomodulation, which appear to inhibit Aβ-induced nerve cell apoptosis while simultaneously promoting nerve cell survival. For full names of enzymes/proteins see list of abbreviations at the end of the manuscript.
PBM and AD in vivo
Using a mouse model of AD, Farfara et al. and Oron et al. were able to ameliorate disease progression by stimulating the proliferation of mesenchymal stem cells (MSCs) with PBM [37, 38]. Weekly treatments using PBM at a dose of 1 J/cm² applied to the bone marrow of AD-mice increased the ability of MSCs to phagocytose Aβ-proteins within the brain, which led to improved cognitive function and spatial learning after a total treatment duration of 2 months, compared to a sham-treated control group. This is an interesting observation, albeit outside the scope of this review, since it refers not to the effect of PBM on brain cells directly, but rather on secondary effects through stimulation of MSCs.
Purushothuman et al. used two transgenic mouse models of AD, engineered to either develop neurofibrillary tangles or Aβ plaques, and treated them for a total of 20 times over the course of four weeks with LED light at 670 nm, delivering a dose of 4 J/cm² per treatment, and provided histochemical evidence of a beneficial effect [39]. Neurofibrillary tangles, hyperphosphorylated tau protein, and oxidative stress markers were reduced to near wild-type levels, and the PBM treatment also reduced the number and size of the Aβ plaques.
De Taboada et al. used a GaAIAs diode laser with a wavelength of 808 nm±10 nm to deliver increasing doses, ranging from 4.8 J/cm² (1.2 J/cm² at the cortical surface) to 48 J/cm² (12 J/cm² at cortical surface), three times per week for a total duration of six months to transgenic mice engineered to develop Aβ plaques [40]. Their results showed an attenuation of amyloid development and improved cognitive function, leading to the conclusion that early and regular administration of PBM has the potential to halt progression from mild cognitive impairment to AD.
Applications of transcranial photobiomodulation to human subjects supporting its therapeutic value for neurological use
In an opinion article by Gonzalez-Lima and Barrett [18], the authors summarized how the development of PBM has evolved over the last 40 years to a point where it is beginning to be used for cognitive-enhancement applications. They conducted a placebo-controlled study focusing on the beneficial cognitive and emotional effects in healthy human volunteers of either sex, age ranging from 18 to 35 years to test this hypothesis. Two weeks after a single therapy session a significant improvement in cognitive tests was observed [41]. These beneficial effects were reflected in improvements in reaction time in a sustained-attention psychomotor vigilance task, in a delayed match-to-sample memory task, and a self-reported Positive and Negative Affect Schedule. Blanco et al. then used the Wisconsin Card Sorting Task in a placebo controlled study on healthy human participants, directly after receiving the PBM treatment to assess the effects of transcranial infrared laser stimulation on executive function [42]. Here, laser light at a wavelength of 1064 nm and power density of 250 mW/cm² was applied to two locations on the right portion of the forehead for a total of 4 min per site. The total supplied dose in this study again corresponded to those stated above, 60 J/cm² per site, and the treatment group performed significantly better than the control group in the Wisconsin Card Sorting Task.
Schiffer et al. reported the beneficial effects of transcranial PBM on anxiety and depression in a study in which PBM was applied using an LED array with peak wavelength at 810 nm and an energy density of 250 mW/cm² [43]. They calculated that from the supplied dose of 60 J/cm² at the scalp, an effective 2.1 J/cm² (3.7%) reached the dura of the brain. Positive effects of a single treatment session (compared to pre-treatment levels) were observed two weeks after PBM, which waned by the time of a further assessment after four weeks.
Chan et al. observed improved frontal cognitive function in older human volunteers (≥60 years) after a single session of PBM [44]. The device used in their study consisted of three LED cluster heads with a mix of 633 nm and 870 nm diodes and a power density of 44.4 mW/cm². Applied for 7.5 min, the devices delivered a dose of 20 J/cm² at the scalp and study participants showed improved reaction time, measured by a modified Eriksen flanker test, and improved mental flexibility, measured by a category fluency test.
Improved cognitive function was also observed by Naeser et al. in case studies where transcranial PBM was used after traumatic brain injury [45, 46], and after left hemisphere stroke, in patients with chronic aphasia [47]. The devices in these studies by Naeser et al. consisted of LED cluster heads, with a mix of 633 nm and 870 nm diodes similar to those used by Chan et al., but with a power density of 22.2 mW/cm². Each treatment site on the scalp received a dose primarily at 13 or 26 J/cm² at each LED cluster placement on the head during a treatment series lasting six weeks (3× per week). The post-PBM testing for the traumatic brain injury participants performed at 1 week, 1 month, and 2 months after the final, 18th treatment with the LED cluster heads, showed significant improvements in cognitive function, as measured by the Stroop Test (executive function), and the California Verbal Learning Test-II (verbal memory). The post-PBM testing for the chronic stroke patients with aphasia showed significant improvements in naming when optimal LED cluster scalp placements (ipsilesional, left hemisphere, and two midline nodes of the default mode network) and 26 J/cm² were used.
As stated by Hashmi et al. in their article about the role of PBM in neurorehabilitation [20], transcranial PBM with low level red to NIR light had already been used on human subjects with moderate AD before the year 2010, although no peer reviewed publications existed as of then. This is slowly changing, with new devices being developed and more individuals being treated in pilot trials, confirming improvements in the Alzheimer’s Disease Assessment Scale-cognitive and enhanced Neuropsychiatric Inventory scores, as well as an increase in regional cerebral blood flow and increased connectivity of the default mode network [29,48–53].
Minimum effective and maximum tolerated dose
When red to NIR monochromatic or quasi-monochromatic light is absorbed by cytochrome oxidase in neuronal mitochondria, the photons increase the proton gradient of the mitochondrial membrane and thus modulate ATP production. The effective dose of PBM appears to follow the principle of hormesis, meaning that low doses are stimulatory while higher doses are less effective or even counterproductive. The minimum effective and maximum tolerated dose has been experimentally evaluated in vitro and in vivo, the translation of these results to transcranial application in humans is supported by results from studies on tissue optical properties and the penetration depth of red and NIR light in the intermediate tissue overlying the brain.
Hormesis
The hormetic effect (or biphasic dose response) of PBM was shown by Gonzalez-Lima and Barrett in a study in rats, where 660 nm LED arrays with a power density of 9 mW/cm² showed the highest increase in cytochrome oxidase activity at a dose of 10.9 J/cm² (13.6% increase), slightly less at the higher dose of 21.6 J/cm² (10.3% increased activity) and finally only a non-significant increase (3%) at the highest dose of 32.9 J/cm² [18]. Using fluorescence-quenching to measure oxygen concentration in the cortex allowing estimates of neuronal oxygen consumption, Rojas et al. reported a 5% increase in oxygen consumption at 1 J/cm² and a 16% increase at a dose of 5 J/cm² when using PBM with 660 nm and a power density of 9 mW/cm² in rats [54].
Pulsing
Aside from wavelength and dose, the question of whether a light source used for PBM should emit continuous wave or pulsed light, has led to investigations of different pulse structures. Upon reviewing nine studies which directly compared continuous wave with pulse wave light, Hashmi et al. summarized that six of these nine studies found pulsed light to be more effective than continuous wave [55]. In an effort to find optimal parameters for PBM in wound healing, Barolet et al. studied various pulsing patterns and also found pulsing to be more beneficial in comparison to continuous wave illumination [56]. For PBM to the brain, finding the optimal pulsing parameters benefits from the fact that neural oscillations measured by electroencephalography recordings have been linked to different mental processes. Memory processes are most closely related to oscillations with theta and gamma frequencies (6 Hz and 40 Hz, respectively), while attention seems closely associated with alpha and gamma oscillations (10 Hz and 40 Hz, respectively) [57]. So, in an analogous manner to how the brain can be modulated with acoustical frequencies (10 Hz or 40 Hz) using binaural auditory beats [58], pulsed light at alpha or gamma frequencies elicited a positive effect on the brain in mouse models of AD [59, 60].
Transmission
Tedford et al. quantitatively analyzed the amount of light that reached the brain using human cadaver heads, which they sectioned in such way that all of the intermediate tissues were kept intact and the optical energy was measured “in situ” within the brain [23]. Results showed an exponential increase in fluence rate with a linear decrease in distance between measurement probe and light source. An absorption coefficient for each of the measured wavelengths was also provided which could be used to calculate the dose supplied to any point inside the brain using Equation (1):
(1)
Lychagov et al. studied the NIR transmittance of the human skull and demonstrated that 0.5% to 5% of the emitted light from a 1 W laser with a wavelength of 810 nm was transmitted transcranially, confirming the exponential relationship between the thickness of skin and bone and light transmission in the NIR-range [61].
Comparing the transmission of red light at 633 nm to that of NIR light at 830 nm in a human cadaveric model, Jagdeo et al. observed that 830 nm had better transmittance compared to 633 nm, and that occipital delivery allowed the highest amount of energy to enter the brain, as shown in Table 1 [62]. Bungart et al. investigated different wavelengths for transcranial PBM and concluded that a combination of 660 nm and 810 nm provided superior penetration compared to a combination of 980 nm and 1064 nm [25].
Table 1
Excerpted from the results published in [62]
| Control (Air only, at a distance of 10 mm) | Beneath skin and skull | |||
| temporal | frontal | occipital | ||
| 830 nm | 33.3 mW/cm² | 0.3 mW/cm² | 0.71 mW/cm² | 3.9 mW/cm² |
| 100% | 0.9% | 2.1% | 11.7% | |
| 633 nm | 67.5 mW/cm² | <0.001 mW/cm² | 0.37 mW/cm² | 0.44 mW/cm² |
| 100% | 0.0% | 0.5% | 0.7% | |
Once the light penetrates through the skull, the further depth of penetration is limited by the optical properties of brain tissue. Table 2 shows some results from Stolik et al.’s ex vivo, post mortem measurements of the penetration depths of red and NIR light directly in brain tissue (without extracranial application), suggesting that light with longer wavelengths will penetrate deeper into the tissue [63].
Table 2
Excerpted from the results published in [63]
| Wavelength | 632.8 nm | 675 nm | 780 nm | 835 nm |
| Penetration Depth [mm±standard error] n = 10 | 0.92±0.08 | 1.38±0.13 | 2.17±0.16 | 2.52±0.19 |
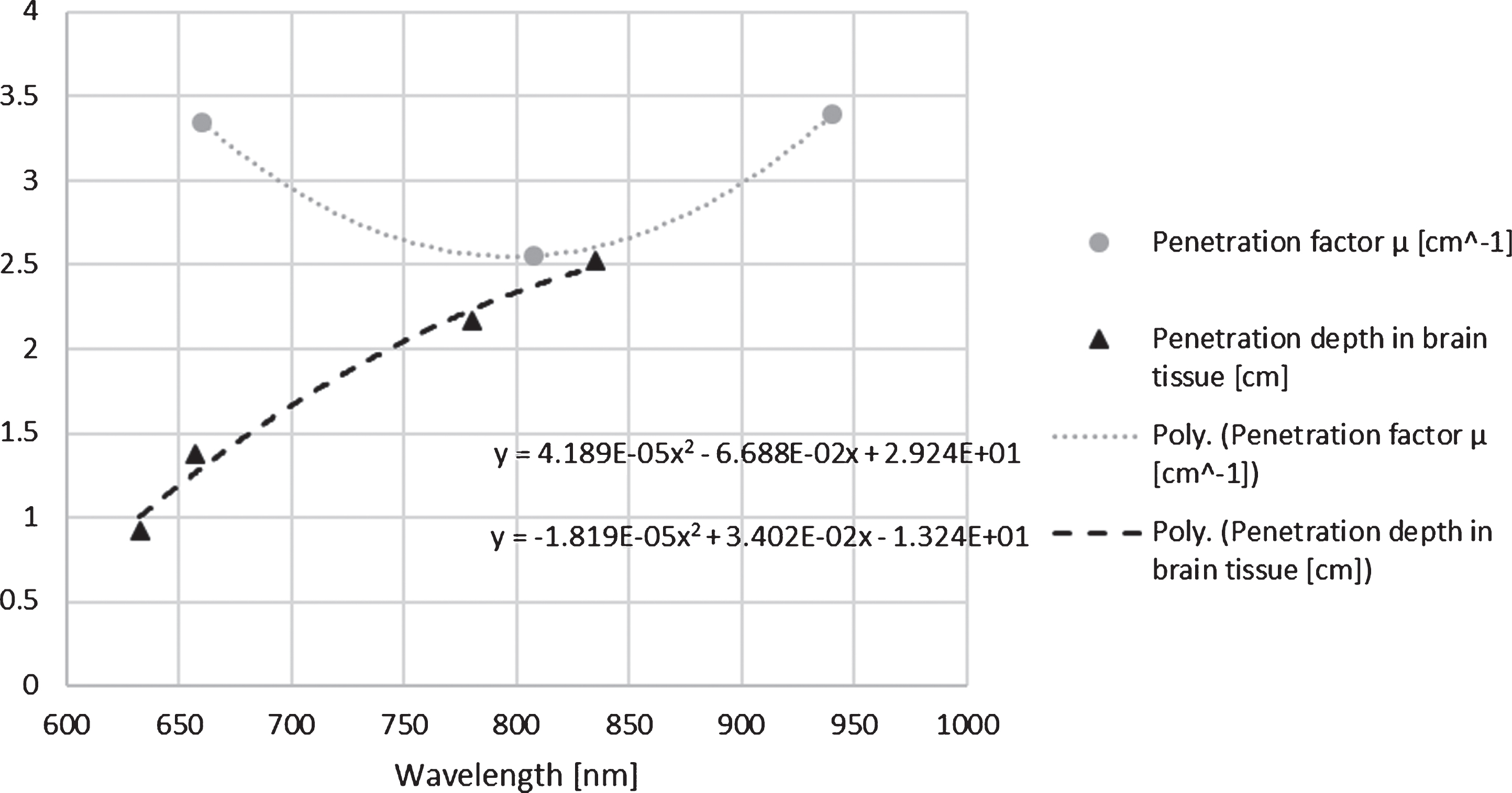
To investigate which wavelength within the tissue optical window will penetrate the deepest and deliver the highest dose, the values for the tissue absorption coefficients as well as the penetration depth were extracted from [23 and 63] and extrapolated by use of polynomial trend lines as shown in Fig. 3. While Fig. 3 suggests that a wavelength between 700 nm and 830 nm is likely to have the most effective and also the deepest delivery of light energy to areas inside the brain, an article by Wu et al. claimed that illumination with 730 nm appeared to be ineffective when used for traumatic brain injury in mice [64]. They reasoned that the CCO absorption spectrum has a minimum at 730 nm and they suggested to use a mix of 665 nm and 810 nm instead, seeing as CCO has two distinct absorption bands at these wavelengths.
Fig. 3
Using literature reports on the transmittance of near infrared light through the scalp and skull, as well as the penetration depth inside the brain, mathematical trends were established in order to provide meaningful values for wavelengths that are not covered in the literature.
Energy density and dose
Summing up the available body of research on PBM to the brain, the application time should be long enough to achieve a dose in the minimum effective range between 5–10 J/cm² at the level of the cortex, therefore, considering the exponential energy decrease during transcranial application, energy densities between 25–60 J/cm² applied to the human scalp are suggested. With 250 mW/cm² continuous wave light, this corresponds to a 4 min treatment, using a 100 mW/cm² continuous wave light would increase the treatment time to 10 min. Pulsing with alpha or gamma frequency might add additional benefit to PBM against AD, and a 50% duty cycle would necessitate a doubling of the treatment time to achieve the same dose as with continuous wave light.
CONCLUSION
When comparing the specifications of PBM devices used in the available literature, especially wavelength and power density, a range of options have already been tested. It can be summarized that the optical window for deep tissue penetration suggests the best results at wavelengths in the far red and NIR range, e.g., at 660 nm and 810 nm. The irradiation intensity of a suitable device for photobiomodulation therapy for AD needs to permit delivery of a dose of up to 60 J/cm² to the scalp within a reasonable period of time while providing a power density below the risk of thermal damage (<250 mW/cm2). The survey of the available literature in this review supports the assumption that PBM with the correct parameters could be useful in the fight against AD. Study protocols suitable for large placebo-controlled studies are now available and we should be able to get significant results with representative statistical power within a year. The time to act is now—lest we forget.
ACKNOWLEDGMENTS
We thank Andreas Drauschke from the University of Applied Sciences FH Technikum Vienna for his valuable scientific input. This study was supported by FFG Basisprogramm grant #853128. Michael R. Hamblin was supported by US NIH Grants R01AI050875 and R21AI121700.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-1210r2).
REFERENCES
[1] | Alzheimer’s Association ((2014) ) 2014 Alzheimer’s disease facts and figures. Alzheimers Dement 10: , e47–92. |
[2] | Sütterlin S , Hoßmann I , Klingholz R ((2011) ) Demenz-Report: Wie sich die Regionen in Deutschland, Österreich und der Schweiz auf die Alterung der Gesellschaft vorbereiten können, Berlin-Institut für Bevölkerung und Entwicklung, Berlin. |
[3] | Dal-Bianco P ((2010) ) DFP Literaturstudium: M. Alzheimer- State of the Art. In ÖÄZ Österreichische Gesellschaft für Neurologie, pp. 40-53. |
[4] | Turkington C , Mitchell DR ((2010) ) The encyclopedia of Alzheimer’s disease. Facts On File, New York. |
[5] | Smith KC ((2005) ) Laser (and LED) therapy is phototherapy. Photomed Laser Ther 23: , 78–80. |
[6] | Arany PR ((2012) ) Photobiomodulation: Poised from the fringes. Photomed Laser Surg 30: , 507–509. |
[7] | Anders JJ , Lanzafame RJ , Arany PR ((2015) ) Low-level light/laser therapy versus photobiomodulation therapy. Photomed Laser Surg 33: , 183–184. |
[8] | de la Torre JC ((2017) ) Treating cognitive impairment with transcranial low level laser therapy. J Photochem Photobiol B 168: , 149–155. |
[9] | de la Torre JC ((2016) ) Cerebral perfusion enhancing interventions: A new strategy for the prevention of Alzheimer dementia. Brain Pathol 26: , 618–631. |
[10] | Santana-Blank L , Rodríguez-Santana E , Santana-Rodríguez KE , Reyes H ((2016) ) “Quantum leap” in photobiomodulation therapy ushers in a new generation of light-based treatments for cancer and other complex diseases: Perspective and mini-review. Photomed Laser Surg 34: , 93–101. |
[11] | Gonzalez-Lima F , Barksdale BR , Rojas JC ((2014) ) Mitochondrial respiration as a target for neuroprotection and cognitive enhancement. Biochem Pharmacol 88: , 584–593. |
[12] | Lapchak PA ((2012) ) Transcranial near-infrared laser therapy applied to promote clinical recovery in acute and chronic neurodegenerative diseases. Expert Rev Med Devices 9: , 71–83. |
[13] | Berman MH , Nichols TW ((2019) ) Treatment of neurodegeneration: Integrating photobiomodulation and neurofeedback in Alzheimer’s dementia and Parkinson’s: A review. Photobiomodul Photomed Laser Surg 37: , 623–634. |
[14] | Rojas JC , Gonzalez-Lima F ((2013) ) Neurological and psychological applications of transcranial lasers and LEDs. Biochem Pharmacol 86: , 447–457. |
[15] | Hayworth CR , Rojas JC , Padilla E , Holmes GM , Sheridan EC , Gonzalez-Lima F ((2010) ) In vivo low-level light therapy increases cytochrome oxidase in skeletal muscle. Photochem Photobiol 86: , 673–680. |
[16] | Naeser MA ((2006) ) Photobiomodulation of pain in carpal tunnel syndrome: Review of seven laser therapy studies. Photomed Laser Ther 24: , 101–110. |
[17] | Fulop AM , Dhimmer S , Deluca JR , Johanson DD , Lenz RV , Patel KB , Douris PC , Enwemeka CS ((2010) ) A meta-analysis of the efficacy of laser phototherapy on pain relief. Clin J Pain 26: , 729–736. |
[18] | Gonzalez-Lima F , Barrett DW ((2014) ) Augmentation of cognitive brain functions with transcranial lasers. Front Syst Neurosci 8: , 36. |
[19] | McCarthy TJ , De Taboada L , Hildebrandt PK , Ziemer EL , Richieri SP , Streeter J ((2010) ) Long-term safety of single and multiple infrared transcranial laser treatments in Sprague-Dawley rats. Photomed Laser Surg 28: , 663–667. |
[20] | Hashmi JT , Huang Y-Y , Osmani BZ , Sharma SK , Naeser MA , Hamblin MR ((2010) ) Role of low-level laser therapy in neurorehabilitation. PM R 2: , S292–S305. |
[21] | Naeser MA , Hamblin MR ((2011) ) Potential for transcranial laser or LED therapy to treat stroke, traumatic brain injury, and neurodegenerative disease. Photomed Laser Surg 29: , 443–446. |
[22] | Chang J , Ren Y , Wang R , Li C , Wang Y , Ping Chu X ((2018) ) Transcranial low-level laser therapy for depression and Alzheimer’s disease. Neuropsychiatry (London) 8: , 477–483. |
[23] | Tedford CE , DeLapp S , Jacques S , Anders J ((2015) ) Quantitative analysis of transcranial and intraparenchymal light penetration in human cadaver brain tissue. Lasers Surg Med 47: , 312–322. |
[24] | Tedford CE , DeLapp S , Jacques S , Anders J ((2015) ) Re: “Quantitative analysis of transcranial and intraparenchymal light penetration in human cadaver brain tissue” Lasers in Surgery and Medicine, 2015;47(4):312-322. Lasers Surg Med 47: , 466–466. |
[25] | Wang P , Li T ((2018) ) Which wavelength is optimal for transcranial low-level laser stimulation? J Biophotonics 12: , e201800173. |
[26] | Bungart BL , Dong L , Sobek D , Sun GY , Yao G , Lee JC-M ((2014) ) Nanoparticle-emitted light attenuates amyloid-β-induced superoxide and inflammation in astrocytes. Nanomedicine 10: , 15–17. |
[27] | Al Amir Dache Z , Otandault A , Tanos R , Pastor B , Meddeb R , Sanchez C , Arena G , Lasorsa L , Bennett A , Grange T , El Messaoudi S , Mazard T , Prevostel C , Thierry AR ((2020) ) Blood contains circulating cell-free respiratory competent mitochondria. FASEB J 34: , 3616–3630. |
[28] | Salgado ASI , Zângaro RA , Parreira RB , Kerppers II ((2015) ) The effects of transcranial LED therapy (TCLT) on cerebral blood flow in the elderly women. Lasers Med Sci 30: , 339–346. |
[29] | Chao LL ((2019) ) Effects of home photobiomodulation treatments on cognitive and behavioral function, cerebral perfusion, and resting-state functional connectivity in patients with dementia: A pilot trial. Photobiomodul Photomed Laser Surg 37: , 133–141. |
[30] | Sommer AP , Bieschke J , Friedrich RP , Zhu D , Wanker EE , Fecht HJ , Mereles D , Hunstein W ((2012) ) 670 nm laser light and EGCG complementarily reduce amyloid-β aggregates in human neuroblastoma cells: Basis for treatment of Alzheimer’s disease? Photomed Laser Surg 30: , 54–60. |
[31] | Yang X , Askarova S , Sheng W , Chen JK , Sun AY , Sun GY , Yao G , Lee JC-M ((2010) ) Low energy laser light (632.8nm) suppresses amyloid-β peptide-induced oxidative and inflammatory responses in astrocytes. Neuroscience 171: , 859–868. |
[32] | Song S , Zhou F , Chen WR ((2012) ) Low-level laser therapy regulates microglial function through Src-mediated signaling pathways: Implications for neurodegenerative diseases. J Neuroinflammation 9: , 1–17. |
[33] | Liang J , Liu L , Xing D ((2012) ) Photobiomodulation by low-power laser irradiation attenuates Aβ-induced cell apoptosis through the Akt/GSK3β/β-catenin pathway. Free Radic Biol Med 53: , 1459–1467. |
[34] | Zhang L , Xing D , Zhu D , Chen Q ((2008) ) Low-power laser irradiation inhibiting Aβ25-35-induced PC12 cell apoptosis via PKC activation. Cell Physiol Biochem 22: , 215–222. |
[35] | Zhang H , Wu S , Xing D ((2012) ) Inhibition of Aβ25-35-induced cell apoptosis by Low-power-laser-irradiation (LPLI) through promoting Akt-dependent YAP cytoplasmic translocation. Cell Signal 24: , 224–232. |
[36] | Meng C , He Z , Xing D ((2013) ) Low-level laser therapy rescues dendrite atrophy via upregulating BDNF expression: Implications for Alzheimer’s disease. J Neurosci 33: , 13505–13517. |
[37] | Farfara D , Tuby H , Trudler D , Doron-Mandel E , Maltz L , Vassar RJ , Frenkel D , Oron U ((2015) ) Low-level laser therapy ameliorates disease progression in a mouse model of Alzheimer’s disease. J Mol Neurosci 55: , 430–436. |
[38] | Oron A , Oron U ((2016) ) Low-level laser therapy to the bone marrow ameliorates neurodegenerative disease progression in a mouse model of Alzheimer’s disease: A minireview. Photomed Laser Surg 34: , 627–630. |
[39] | Purushothuman S , Johnstone DM , Nandasena C , Mitrofanis J , Stone J ((2014) ) Photobiomodulation with near infrared light mitigates Alzheimer’s disease-related pathology in cerebral cortex-evidence from two transgenic mouse models. Alzheimers Res Ther 6: , 2. |
[40] | De Taboada L , Yu J , El-Amouri S , Gattoni-Celli S , Richieri S , McCarthy T , Streeter J , Kindy MS ((2011) ) Transcranial laser therapy attenuates amyloid-β peptide neuropathology in amyloid-β protein precursor transgenic mice. J Alzheimers Dis 23: , 521–535. |
[41] | Barrett DW , Gonzalez-Lima F ((2013) ) Transcranial infrared laser stimulation produces beneficial cognitive and emotional effects in humans. Neuroscience 230: , 13–23. |
[42] | Blanco NJ , Maddox WT , Gonzalez-Lima F ((2015) ) Improving executive function using transcranial infrared laser stimulation. J Neuropsychol 11: , 14–25. |
[43] | Schiffer F , Johnston AL , Ravichandran C , Polcari A , Teicher MH , Webb RH , Hamblin MR ((2009) ) Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: A pilot study of 10 patients with major depression and anxiety. Behav Brain Funct 5: , 46. |
[44] | Chan AS , Lee TL , Yeung MK , Hamblin MR ((2018) ) Photobiomodulation improves the frontal cognitive function of older adults. Int J Geriatr Psychiatry 34: , 369–377. |
[45] | Naeser MA , Saltmarche A , Krengel MH , Hamblin MR , Knight JA ((2011) ) Improved cognitive function after transcranial, light-emitting diode treatments in chronic, traumatic brain injury: Two case reports. Photomed Laser Surg 29: , 351–358. |
[46] | Naeser MA , Zafonte R , Krengel MH , Martin PI , Frazier J , Hamblin MR , Knight JA , Meehan WP , Baker EH ((2014) ) Significant improvements in cognitive performance post-transcranial, red/near-infrared light-emitting diode treatments in chronic, mild traumatic brain injury: Open-protocol study. J Neurotrauma 31: , 1008–1017. |
[47] | Naeser MA , Ho MD , Martin PI , Hamblin MR , Koo B-B ((2020) ) Increased functional connectivity within intrinsic neural networks in chronic stroke following treatment with red/near-infrared transcranial photobiomodulation: Case series with improved naming in aphasia. Photobiomodul Photomed Laser Surg 38: , 115–131. |
[48] | Saltmarche AE , Naeser MA , Ho KF , Hamblin MR , Lim L ((2017) ) Significant improvement in cognition in mild to moderately severe dementia cases treated with transcranial plus intranasal photobiomodulation: Case series report. Photomed Laser Surg 35: , 432–441. |
[49] | Berman MH , Halper JP , Nichols TW , Jarrett H , Lundy A , Huang JH ((2017) ) Photobiomodulation with near infrared light helmet in a pilot, placebo controlled clinical trial in dementia patients testing memory and cognition. J Neurol Neurosci 8: , 176. |
[50] | Lim L ((2018) ) The growing evidence for photobiomodulation as a promising treatment for Alzheimer’s disease. J Biosci Med 6: , 100–110. |
[51] | Hamblin MR ((2019) ) Photobiomodulation for Alzheimer’s disease: Has the light dawned? Photonics 6: , 77. |
[52] | Chao LL ((2018) ) A pilot clinical trial of transcranial and intranasal photobiomodulation for cognitive and behavioral function, cerebral perfusion, and resting state functional connectivity. Alzheimers Dement 14: , P672–P673. |
[53] | Zomorrodi R , Saltmarche AE , Loheswaran G , Ho KF , Lim L ((2017) ) [P2-043]: Complementary EEG evidence for a significantly improved Alzheimer’s disease case after photobiomodulation treatment. Alzheimers Dement 13: , P621. |
[54] | Rojas JC , Bruchey AK , Gonzalez-Lima F ((2012) ) Low-level light therapy improves cortical metabolic capacity and memory retention. J Alzheimers Dis 32: , 741–752. |
[55] | Hashmi JT , Huang Y-Y , Sharma SK , Kurup DB , De Taboada L , Carroll JD , Hamblin MR ((2010) ) Effect of pulsing in low-level light therapy. Lasers Surg Med 42: , 450–466. |
[56] | Barolet D , Duplay P , Jacomy H , Auclair M ((2010) ) Importance of pulsing illumination parameters in low-level-light therapy. J Biomed Opt 15: , 048005. |
[57] | Ward LM ((2003) ) Synchronous neural oscillations and cognitive processes. Trends Cogn Sci 7: , 553–559. |
[58] | Lane JD , Kasian SJ , Owens JE , Marsh GR ((1998) ) Binaural auditory beats affect vigilance performance and mood. Physiol Behav 63: , 249–252. |
[59] | Iaccarino HF , Singer AC , Martorell AJ , Rudenko A , Gao F , Gillingham TZ , Mathys H , Seo J , Kritskiy O , Abdurrob F , Adaikkan C , Canter RG , Rueda R , Brown EN , Boyden ES , Tsai L-H ((2016) ) Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature 540: , 230–235. |
[60] | Martorell AJ , Paulson AL , Suk H-J , Abdurrob F , Drummond GT , Guan W , Young JZ , Kim DN-W , Kritskiy O , Barker SJ , Mangena V , Prince SM , Brown EN , Chung K , Boyden ES , Singer AC , Tsai L-H ((2019) ) Multi-sensory gamma stimulation ameliorates Alzheimer’s-associated pathology and improves cognition. Cell 177: , 256–271.e22. |
[61] | Lychagov VV , Tuchin VV , Vilensky MA , Reznik BN , Ichim T , De Taboada L ((2006) ) Experimental study of NIR transmittance of the human skull. In Proceedings of SPIE - The International Society for Optical Engineering, art. no. 60850T. doi: 10.1117/12.650116. |
[62] | Jagdeo JR , Adams LE , Brody NI , Siegel DM ((2012) ) Transcranial red and near infrared light transmission in a cadaveric model. PLoS One 7: , e47460. |
[63] | Stolik S , Delgado JA , Perez A , Anasagasti L ((2000) ) Measurement of the penetration depths of red and near infrared light in human “ex vivo” tissues. J Photochem Photobiol B 57: , 90–93. |
[64] | Wu Q , Xuan W , Ando T , Xu T , Huang L , Huang Y-Y , Dai T , Dhital S , Sharma SK , Whalen MJ , Hamblin MR ((2012) ) Low-level laser therapy for closed-head traumatic brain injury in mice: Effect of different wavelengths. Lasers Surg Med 44: , 218–226. |


