
Infant–Father Attachment in Infants Born Preterm - A Brief Report
Abstract
This study examines the infant–father attachment in infants born preterm (< 1500 g at birth and/or < 37 weeks gestation) in comparison to full-term infants. The infant–father attachment was assessed using the Strange Situation Procedure at a (corrected) age of 15 months. We found at least half of preterm and full-term infants (50.0% and 56.5% respectively) securely attached to their fathers, and no significant overall difference was observed concerning the distribution of attachment quality comparing the two groups. In light of the fact that preterm infants tend to have numerous neurodevelopmental problems, it is encouraging that significant differences were not found in the distribution of the attachment quality among the groups. Therefore, from the perspective of attachment research, it would be highly beneficial to include fathers in the care of their preterm infants.
Introduction
Infant–caregiver attachment is to be understood as an emotional bond, which infants form with their consistent caregivers. Attachment quality depends on how sensitive the caregiver is to the child’s signals when caring for the child (Bowlby, 1988; Goldberg et al., 1995; van IJzendoorn et al., 1992). Secure, avoidant, and ambivalent attachment qualities are all considered organised strategies employed by children to optimally adapt to their environment (Ainsworth et al., 1978). In contrast, children classified as disorganised exhibit contradictory, inappropriate or stereotypical behaviours when under stress, which is associated with a breakdown of organised attachment behaviours (Main & Solomon, 1990). Attachment disorganisation is a precursor of psychopathological conditions and poor relationships to peers in later childhood (Carlson, 1998; Main & Solomon, 1990; van IJzendoorn et al., 1999; Wolke et al., 2014).
In clinical attachment research the development of attachment quality among preterm infants has been examined for quite some while (Easterbrooks, 1989; Rode et al., 1981). The term “preterm infants” refers to infants born before the 37th week of gestation. Unlike infants born at term, preterm infants are at increased risk of a range of developmental impairments concerning cognition, socio-emotional behaviour and somatic aspects (Gutbrod & Wolke, 2004; Hille et al., 2001; Montagna et al., 2020; Moster et al., 2008; Samara et al., 2008). While some studies found no differences in the infant–mother attachment between infants born preterm and infants born at term (Karabekiroglu et al., 2015; Korja et al., 2012), other studies report significantly more attachment disorganisation (Wolke et al., 2014), or overall to a lesser extent attachment security (Mangelsdorf et al., 1996) in preterm infants. Although fathers have been included in the care of their preterm infants during their stay in hospital on an increasingly broader base for several years now, they have thus far been relegated to a secondary role in attachment research (Deeney et al., 2009; Kißgen & Carlitscheck, 2013; Witting et al., 2016). Investigating infant–father attachment and its contribution to the development of children from high-risk groups may, however, provide valuable insights, just as the secure infant–mother attachment has been found to be a strong protecting factor in child development (Belsky & Fearon, 2002; Rutter, 1990).
So far there have only been three studies investigating the influence of preterm birth on infant–father attachment (Easterbrooks, 1989; Ruiz et al., 2018; Witting et al., 2016). As early as 1989, using the Strange Situation Procedure (SSP) (Ainsworth et al., 1978), Easterbrooks found that preterm birth did not influence infant–father attachment, infant–mother attachment, and temporal stability of attachment (13 and 20 months), nor did it create any difference in the attachment to the mother or the father. Almost three decades later, Witting et al. (2016) conducted case studies with three boys using both the SSP as well as the Attachment Q-Sort (AQS) that generates an overall attachment security score. They observed a generally smaller variety of attachment behaviours of the two preterm boys compared to the boy born at term. The fathers of the preterm infants in particular had difficulties in adequately understanding and responding appropriately to their children’s behaviour and needs. Recently, Ruiz et al. (2018) found significantly higher attachment security scores with the AQS in the group of full-term infants compared to preterm infants (aged between 12 and 36 months). In the same study lower education of fathers, as well as child’s lower development scores and male gender, were associated with lower attachment scores of preterm children.
The nature and degree of involvement of fathers in childrearing changed dramatically over the past 30 years (Cabrera et al., 2018), as well as the care for preterm infants in hospitals, so findings of the study by Easterbrooks can hardly be applied to the situation nowadays. Preterm infants with higher neonatal medical risk are more often found to have a disorganized attachment to their mothers (Cox et al., 2000). Further, Wolke et al. (2014) found that infants’ neurological characteristics were more important for developing infant–mother attachment than caregiver’s sensitivity. It is not clear whether the same is true for infant–father attachment development.
The present study seeks to revisit the following questions: (1) Do preterm infants differ from infants born at term with regard to their infant–father attachment quality? (2) Do preterm infants’ characteristics (birth weight, gestational age, neurobiological risks, and clinical risks) affect the infant–father attachment?
Methods
Participants
Preterm (Department of Neonatology) and full-term infants (Department of Obstetrics) were recruited at the University of Cologne Children's Hospital in Germany over the period of twelve months. Constituting a convenience sample, fathers were invited to participate in the study by the medical staff after the birth of their children. After obtaining oral agreement, study protocols, consent forms and a questionnaire (assessing the demographic characteristics of fathers, among other variables) were mailed to the participants’ home addresses. Exclusion criteria for fathers were drug addiction, history of psychiatric problems, language difficulties, and not living with the infant’s mother. Infants suffering from intraventricular haemorrhage (IVH)>grade 2, periventricular leukomalacia, neuromuscular disease, and severe malformations were not included in this study. Twenty-four preterm infant–father dyads (birth weight below 1500g or gestational period below 37 weeks or both) and 27 full-term infant–father dyads were recruited for participation in the study. There were two twin pairs and one triplet in the preterm and four twin pairs in the full-term group. Only one child from each of these families was randomly selected and included in the analysis, reducing the sample size to 20 preterm and 23 full-term infants. Assessments were conducted at the infants’ (corrected) age of 15 months. The study was conducted complying with the WMA Declaration of Helsinki and the APA ethical standards. Informed consent was obtained from all fathers prior to inclusion in this study.
Measures
Developmental status was assessed with the Bayley Scales of Infant Development (BSID-II) focussing on the Mental Development Index (MDI) and the Psychomotor Development Index (PDI) (Bayley, 1993). Attachment quality was assessed using the Strange Situation Procedure (SSP)(Ainsworth et al., 1978). Both were conducted by two trained psychologists at the Department of Human Sciences at the University of Cologne. Attachment quality was coded by Fabienne Becker-Stoll and Elizabeth A. Carlson, who were trained by L. Alan Sroufe. Coders received no information about the infants or the fathers and analysed all 43 videotapes separately. The inter-rater agreement across the whole sample was 100%. In the preterm subsample, the following risk scores were assessed shortly after birth by medical staff: The Nursery Neurobiologic Risk Score (NBRS) measures the intensity and severity of seven items related to brain cell injuries, e.g., intensity and duration of assisted ventilation, seizures or infection on a 4-point Likert scale (0 = absence of risk, 1, 2, 4), with higher scores indicating higher intensity and severity of symptoms. The sum score, as a measure of neurobiological risk, has previously been shown to be predictive of infants decreased mental and psychomotor development (Brazy et al., 1991).The Clinical Risk Index for Babies (CRIB) uses six items to assess the severity of perinatal illness (birth weight, gestational age, presence of congenital malformation, maximum base excess, minimum and maximum appropriate inspired oxygen concentration in the first 12 hours) and the resulting sum score has proven to be predictive of infant development and mortality. Higher scores indicate greater risk (Manktelow et al., 2009; Rautonen et al., 1994).
Statistical Analysis
Sample characteristics were compared between the preterm and full-term subsamples using t-tests for continuous variables as well as Pearson’s chi-square tests for categorical data. All comparisons were conducted using SPSS V. 26 (IBM SPSS Statistics, IBM Corporation).
Results
There were significant differences in birth weight, gestational age, sex ratio, and Psychomotor Development (PDI) between preterm and full-term born infants. Differences between all other variables listed in Table 1 were not significant.
Table 1
Infant and Paternal Sample Characteristics
| Preterm | Full-term | Statistical parameter | p | |
| (N = 20) | (N = 23) | |||
| Birth weight (g), M (SD) | 1192.06 (377.07) | 3173.04 (473.67) | 14.221 | .000 |
| Gestational age (weeks), M (SD) | 29.35 (2.08) | 39.35 (1.43) | –18.521 | .000 |
| Sex: female, N (%) | 12 (60) | 5 (21.7) | 6.552 | 0.010 |
| MDI, M (SD) | 104.4 (7.46) | 102 (12.80) | 0.741 | 0.451 |
| PDI, M (SD) | 91.85 (11.95) | 100.3 (13.01) | –2.211 | 0.033 |
| CRIB-Score, M (SD) | 1.94 (2.53) | - | ||
| NBRS, M (SD) | 4.50 (3.47) | - | ||
| Paternal age, M (SD) | 38 (4.30) | 38.55 (6.33) | –0.301 | 0.763 |
| Occupational status: employed, N (%) | 16 (80) | 19 (82.6) | 2.032 | 0.363 |
| Education: university degree, N (%) | 8 (47.1) | 9 (45) | 0.162 | 0.900 |
1T-value; 2Chi-squared value.
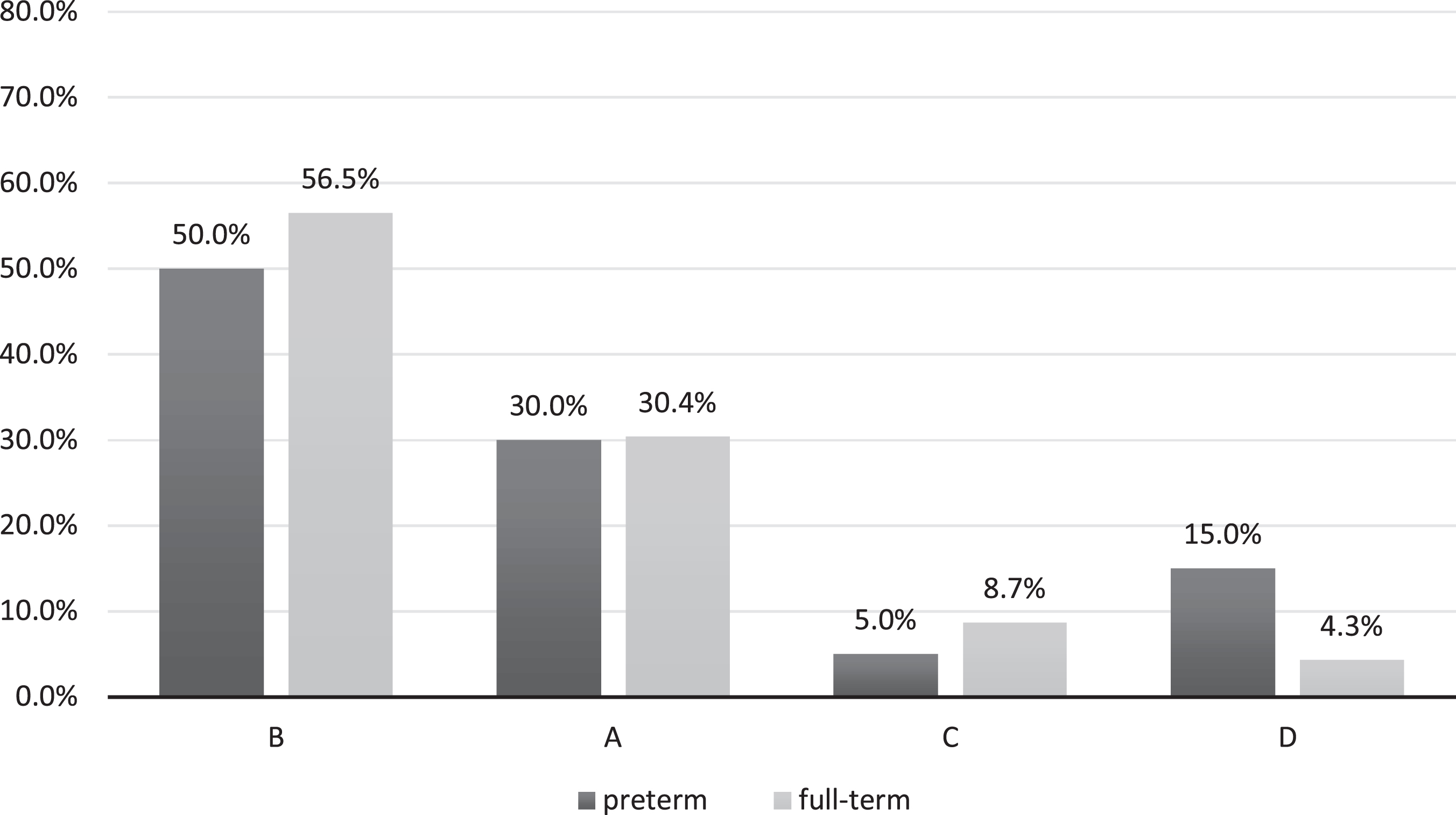
Figure 1 shows the distribution of attachment classifications in our sample. Most infants were securely attached in both groups (preterm = 50.0%; full-term = 56.5%). No significant overall difference was found between preterm and full-term infants (χ² (3, N = 43) = 1.6, p = .659). Comparisons along the primary attachment dimensions secure vs. insecure did not reveal any significant differences either. Within the preterm group, securely attached infants did not differ from insecurely attached infants regarding gestational age (t(18) = –.053, p = .605, d = 0.24) or birth weight (t(15) = –0.36, p = .723, d = 0.18). Although the mean of the NBRS was numerically higher for insecure children, a comparison did not result in a significant difference in the preterm group between secure vs. insecure attachment quality (t(16) = 0.74, p = .472, d = 0.35); the difference of the CRIB-Score was also not significant between secure and insecure children (t(15) = –0.09, p = .932, d = 0.04).
Figure 1
Distribution of attachment classifications in preterm and full-term infants.
Note. B: secure; A: insecure-avoidant; C: insecure-ambivalent; D: disorganised
Discussion
The present study investigated infant–father attachment in infants born preterm using the SSP. The results regarding child development are in line with current state of research. The majority of studies does find differences in cognition between preterm and full-term infants, whereas a considerable amount of studies cannot provide this evidence. For example, Reuner et al. (2015) did not find any significant differences in cognition between preterm and full-term infants. The meta-analysis of Kerr-Wilson et al. (2012) documents that 4 out of 27 included studies report no differences in cognitive development between preterm and full-term infants. Evidence regarding the psychomotor development is less ambiguous, as preterm infants persistently get significantly lower scores in these tasks than full-term infants (Evensen et al., 2020; Oudgenoeg-Paz et al., 2017).
Considering the nature of our sample in other aspects, results should be interpreted with caution. Just like Easterbrooks (1989), we found no difference in the distribution of the quality of attachment to fathers between preterm and full-term infants. By contrast, Ruiz et al. (2018) showed that preterm infants have more problems developing a secure attachment to their fathers and that they exhibit significantly lower AQS-values than full-term infants. However, the AQS and the SSP have very different frameworks measuring attachment in different contexts (attachment quality in fearful situations vs. attachment security in everyday life) and might be difficult to compare. To generate a wider understanding of possibly different implications within these frameworks, future studies should use both methodologies with a larger cohort for examining infant–father attachment in preterm infants.
Despite the neurodevelopmental problems and the high levels of stress associated with preterm birth, infants’ characteristics did not affect infant–father attachment. It remains unclear if this finding is due to the father’s or the child’s behaviour or both. Although parental sensitivity does explain the transmission of attachment to a certain degree, the so-called transmission gap still remains (Verhage et al., 2016) and the differences in groups cannot be ascribed to fathers’ lack of differences in behaviour with preterm vs. full-term infants.
However, the effect size of the differences in the NBRS score reached a level that can be considered a small effect (Cohen, 1988) without being statistically significant. This finding could suggest that the differences in neurobiological risk factors might be of statistical significance in a bigger sample and might ultimately affect infant–father attachment differently. However, this conclusion must remain hypothetically by the results of this study.
Nevertheless, our results emphasize the involvement of fathers in the care for preterm infants, as they apparently contribute to the formation of attachment in a way that is comparable to the general population.
The results can only be generalized to a limited extent, for example due to a limited sample size and convenient sampling. Moreover, girls were overrepresented in our sample, which may have affected the results, as male gender has been found to be a risk factor in various vulnerable groups, including preterm born infants (Ruiz et al. 2018). Thus, the separate effect of gender on attachment in preterm infants should be investigated in future studies. Additionally, preterm children are more common in families with lower socio-economic status and lower parental education (Whitehead, 2012). Our sample of fathers of children born preterm, however, has a comparable educational background to the sample of fathers of children born term, which possibly accounts for missing differences between the two groups. We recommend further research that accounts for these highlighted limitations.
References
1 | Ainsworth, M. S. , Blehar, M. C. , Waters, E. , & Wall, S. ((1978) ). Patterns of attachment: A psychological study of the strange situation (Vol. xviii). Lawrence Erlbaum. |
2 | Bayley, N. ((1993) ). Bayley Scales of Infant Development: Second edition. Manual. The Psychological Corporation. |
3 | Belsky, J. , & Fearon, R. M. P. ((2002) ). Infant–mother attachment security, contextual risk, and early development: A moderational analysis. Development and Psychopathology, 14: , 293–310. doi: 10.1017/S0954579402002067 |
4 | Bowlby, J. ((1988) ). A secure base: Clinical applications of attachment theory. Routledge. |
5 | Brazy, J. E. , Eckerman, C. O. , Oehler, J. M. , Goldstein, R. F. , & O’Rand, A. M. ((1991) ). Nursery Neurobiologic Risk Score: Important factor in predicting outcome in very low birth weight infants. The Journal of Pediatrics, 118: , 783–792. doi: 10.1016/s0022-3476(05)80047-2 |
6 | Cabrera, N. J. , Volling, B. L. , & Barr, R. ((2018) ). Fathers are parents, too! Widening the lens on parenting for children’s development. Child Development Perspectives, 12: , 152–157. doi: 10.1111/cde12275 |
7 | Carlson, E. A. ((1998) ). A prospective longitudinal study of attachment disorganization/disorientation. Child Development, 69: , 1107–1128. doi: 10.1111/j.1467-8624.1998.tb06163.x |
8 | Cohen, J. ((1988) ). Statistical power analysis for the behavioral sciences (Vol. 2). Routledge. |
9 | Cox, S. M. , Hopkins, J. , & Hans, S. L. ((2000) ). Attachment in preterm infants and their mothers: Neonatal risk status and maternal representations. Infant Mental Health Journal, 21: , 464–480. doi: 10.1002/1097-0355(200011/12)21:6<464::AID-IMHJ5>3.0.CO;2-V |
10 | Deeney, K. , Lohan, M. , Parkes, J. , & Spence, D. ((2009) ). Experiences of fathers of babies in intensive care. Paediatric Nursing, 21: , 45–47. doi: 10.7748/paed2009.02.21.1.45.c6913 |
11 | Easterbrooks, M. A. ((1989) ). Quality of attachment to mother and to father: Effects of perinatal risk status. Child Development, 60: , 825–830. JSTOR. doi: 10.2307/1131023 |
12 | Evensen, K. A. I. , Ustad, T. , Tikanmäki, M. , Haaramo, P. , & Kajantie, E. ((2020) ). Long-term motor outcomes of very preterm and/or very low birth weight individuals without cerebral palsy: A review of the current evidence. Seminars in Fetal and Neonatal Medicine, 25: , 101116–10.1016/j.siny.2020.101116 |
13 | Goldberg, S. , Gotowiec, A. , & Simmons, R. J. ((1995) ). Infant-mother attachment and behavior problems in healthy and chronically ill preschoolers. Development and Psychopathology, 7: , 267–282. doi: 10.1017/S0954579400006490 |
14 | Gutbrod, T. , & Wolke, D. ((2004) ). Attachment formation in very premature infants. In Nöcker-Ribaupierre M. (Ed.), Music therapy for premature and newborn infants (pp. 33-51). Barcelona Publishers. |
15 | Hille, E. T. , den Ouden, A. L. , Saigal, S. , Wolke, D. , Lambert, M. , Whitaker, A. , (...) & Paneth, N. ((2001) ). Behavioural problems in children who weigh 1000 g or less at birth in four countries. The Lancet, 357: , 1641–1643. doi: 10.1016/S0140-6736(00)04818-2 |
16 | Karabekiroglu, K. , Akman, I. , Kuscu Orhan, S. , Kuscu, K. , Altuncu, E. , Karabekiroglu, A. , & Yuce, M. ((2015) ). Mother-child interactions of preterm toddlers. Noro Psikiyatri Arsivi, 52: , 157–162. doi: 10.5152/npa.2015.7343 |
17 | Kerr-Wilson, C. O. , Mackay, D. F. , Smith, G. C. S. , & Pell, J. P. ((2012) ). Meta-analysis of the association between preterm delivery and intelligence. Journal of Public Health, 34: , 209–216. doi: 10.1093/pubmed/fdr024 |
18 | Kißgen, R. , & Carlitscheck, J. ((2013) ). Väter in der Neonatologie [Fathers in neonatology]. In J. Reichert & M. Rüdiger (Hrsg.), Psychologie in der Neonatologie. Psychologischsozialmedizinische Versorgung von Familien Frühgeborener (S. 60-70). Hogrefe. |
19 | Korja, R. , Latva, R. , & Lehtonen, L. ((2012) ). The effects of preterm birth on mother-infant interaction and attachment during the infant’s first two years: Preterm birth and mother-infant relationshi. Acta Obstetricia et Gynecologica Scandinavica, 91: , 164–173. doi: 10.1111/j.1600-0412.2011.01304.x. |
20 | Main, M. , & Solomon, J. ((1990) ). Procedures for identifying infants as disorganized/disoriented during the Ainsworth Strange Situation. In M. T. Greenberg, D. Cicchetti, & E. M. Cummings (Eds.), Attachment in the preschool years: Theory, research, and intervention (pp. 121-160). University of Chicago Press. |
21 | Mangelsdorf, S. C. , Plunkett, J. W. , Dedrick, C. F. , Berlin, M. , Meisels, S. J. , McHale, J. L. , & Dichtellmiller, M. ((1996) ). Attachment security in very low birth weight infants. Developmental Psychology, 32: , 914–920. doi: 10.1037/0012-1649.32.5.914 |
22 | Manktelow, B. , Draper, E. , & Field, D. ((2009) ). Predicting neonatal mortality among very preterm infants: A comparison of three versions of the CRIB score. Archives of Disease in Childhood: Fetal and Neonatal Edition, 95: , F9–F13. doi: 10.1136/adc.2008.148015 |
23 | Montagna, A. , Karolis, V. , Batalle, D. , Counsell, S. , Rutherford, M. , Arulkumaran, S. , (...) & Nosarti, C. ((2020) ). ADHD symptoms and their neurodevelopmental correlates in children born very preterm. PLOS ONE, 15: ((3)), e0224343. doi: 10.1371/journal.pone.0224343 |
24 | Moster, D. , Lie, R. T. , & Markestad, T. ((2008) ). Long-term medical and social consequences of preterm birth. New England Journal of Medicine, 359: , 262–273. doi: 10.1056/NEJMoa0706475 |
25 | Oudgenoeg-Paz, O. , Mulder, H. , Jongmans, M. J. , van der Ham, I. J. M. , & Van der Stigchel, S. ((2017) ). The link between motor and cognitive development in children born preterm and/or with low birth weight: A review of current evidence. Neuroscience & Biobehavioral Reviews, 80: , 382–393. doi: 10.1016/j.neubiorev.2017.06.009 |
26 | Rautonen, J. , Mäkelä, A. , Boyd, H. , Apajasalo, M. , & Pohjavuon, M. ((1994) ). CRIB and SNAP: Assessing the risk of death for preterm neonates. The Lancet, 343: , 1272–1273. doi: 10.1016/S0140-6736(94)92158-X |
27 | Reuner, G. , Weinschenk, A. , Pauen, S. , & Pietz, J. ((2015) ). Cognitive development in 7- to 24-month-old extremely/very-to-moderately/late preterm and full-term born infants: The mediating role of focused attention. Child Neuropsychology, 21: , 314–330. doi: 10.1080/09297049.2014.899571 |
28 | Rode, S. S. , Chang, P.-N. , Fisch, R. O. , & Sroufe, L. A. ((1981) ). Attachment patterns of infants separated at birth. Developmental Psychology, 17: , 188–191. doi: 10.1037/0012-1649.17.2.188 |
29 | Ruiz, N. , Piskernik, B. , Witting, A. , Fuiko, R. , & Ahnert, L. ((2018) ). Parent-child attachment in children born preterm and at term: A multigroup analysis. PLOS ONE, 13: ((8)), e0202972. doi: 10.1371/journal.pone.0202972 |
30 | Rutter, M. ((1990) ).. Resilience, competence, and coping. In J. Rolf, A. Masten S., D. Cicchetti, K. Nüchterlein H., & S. Weintraub (Eds.), Risk and protective factors in the development of psychopathology (pp. 181-214). Cambridge University Press. |
31 | Samara, M. , Marlow, N. , Wolke, D. , for the EPICure Study Group ((2008) ). Pervasive behavior problems at 6 years of age in a total-population sample of children born at< = 25 weeks of gestation. Pediatrics, 122: , 562–573. doi: 10.1542/peds.2007-3231 |
32 | van IJzendoorn, M. H. , Goldberg, S. , Kroonenberg, P. M. , & Frenkel, O. J. ((1992) ). The relative effects of maternal and child problems on the quality of attachment: A meta-analysis of attachment in clinical samples. Child Development, 63: , 840–858. doi: 10.2307/1131237 |
33 | Van Ijzendoorn, M. H. , Schuengel, C. , & Bakermans-Kranenburg, M. J. ((1999) ). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11: , 225–250. doi: 10.1017/S0954579499002035 |
34 | Verhage, M. L. , Schuengel, C. , Madigan, S. , Fearon, R. M. P. , Oosterman, M. , Cassibba, R. (...) & van IJzendoorn, M. H. ((2016) ). Narrowing the transmission gap: A synthesis of three decades of research on intergenerational transmission of attachment. Psychological Bulletin, 142: , 337–366. doi: 10.1037/bul0000038 |
35 | Whitehead, N. S. ((2012) ). The relationship of socioeconomic status to preterm contractions and preterm delivery. Maternal and Child Health Journal, 16: , 1645–1656. doi: 10.1007/s10995-012-0948-4 |
36 | Witting, A. , Ruiz, N. , & Ahnert, L. ((2016) ). Variations in early attachment mechanisms contribute to attachment quality: Case studies including babies born preterm. International Journal of Developmental Science, 10: , 89–97. doi: 10.3233/DEV-16194 |
37 | Wolke, D. , Eryigit-Madzwamuse, S. , & Gutbrod, T. ((2014) ). Very preterm/very low birthweight infants’ attachment: Infant and maternal characteristics. Archives of Disease in Childhood - Fetal and Neonatal Edition, 99: , F70–F75. doi: 10.1136/archdischild-2013-303788 |
Bio Sketches
Ruediger Kissgen, Ph.D., Professor of Developmental Science and Special Education, Department of Educational Science and Psychology, University of Siegen, Germany. Research topics: clinical attachment research (e. g. ADHD, preterm children), child development in the preschool years.
Sebastian Franke, Ph.D., psychologist and staff member at the chair of Developmental Science and Special Education, Department of Educational Science and Psychology, University of Siegen, Germany. Research topics: attachment research (e. g. ADHD, preschool years), statistics.
Nino Jorjadze, psychologist and staff member at the chair of Developmental Science and Special Education, Department of Educational Science and Psychology, University of Siegen, Germany. Research topics: attachment research (e. g. foster children, institutional care).
Bernhard Roth, M.D., Professor emeritus, former Head of Department of Neonatology, University of Cologne Children's Hospital, Germany. Research topics: paediatric intensive care, development of preterm children, ethics in neonatology.
Angela Kribs, M.D., Assistant Professor, Head of Department of Neonatology, University of Cologne Children's Hospital, Germany. Research topics: paediatric intensive care, development of preterm children, breastfeeding, avoidance of mechanical ventilation.


