
Challenging Cases in Urothelial Cancer: Case 32
This is a 62 year old man who was referred to a nephrologist because his serum creatinine was slightly elevated. He never had any voiding complaints and in particular has not had hematuria. He underwent a renal and bladder ultrasound which identified a small mass in the lower portion of the urinary bladder. He then had a CT scan which identified a small filling defect in the bladder (Fig 1).
Fig. 1
CT image of small filling defect at bladder trigone.

He under when a flexible cystoscopy in the office which was normal except for an unusual appearing papillary neoplasm with a long narrow stalk exiting from the urothelial surface for several millimeters with a papillary appearing structure at the distal end. This was a bladder neoplasm but not the typical appearance of a papillary low grade bladder tumor.
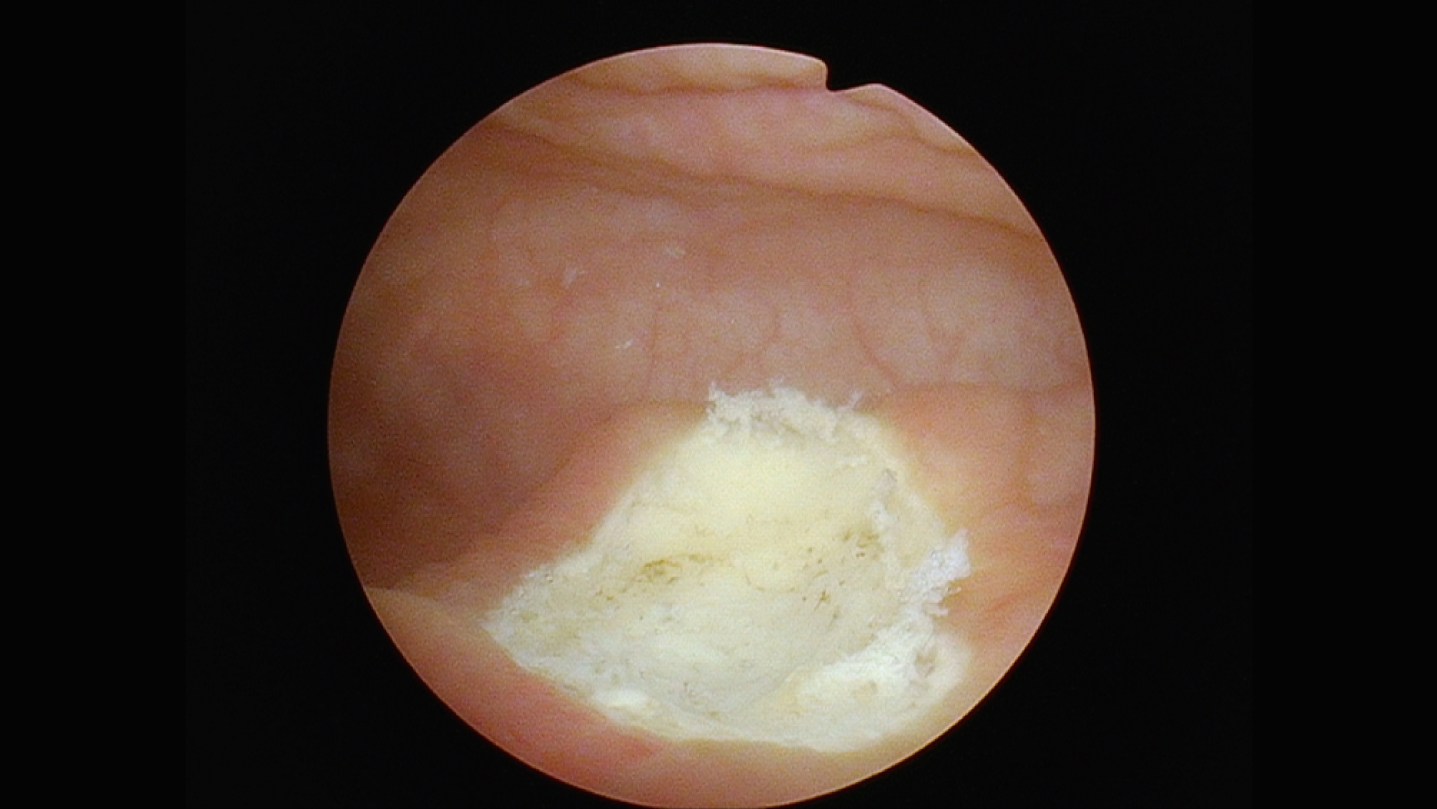
The patient was taken to the operating room for removal of the tumor. Once again, the appearance was exactly as described above (Fig. 2). A cold cup biopsy forceps was used to grasp the base of the stalk and extract the neoplasm intact (Figs. 3-4). The base was cauterized (Fig. 5).
Fig. 2
Fibroepithelial polyp.
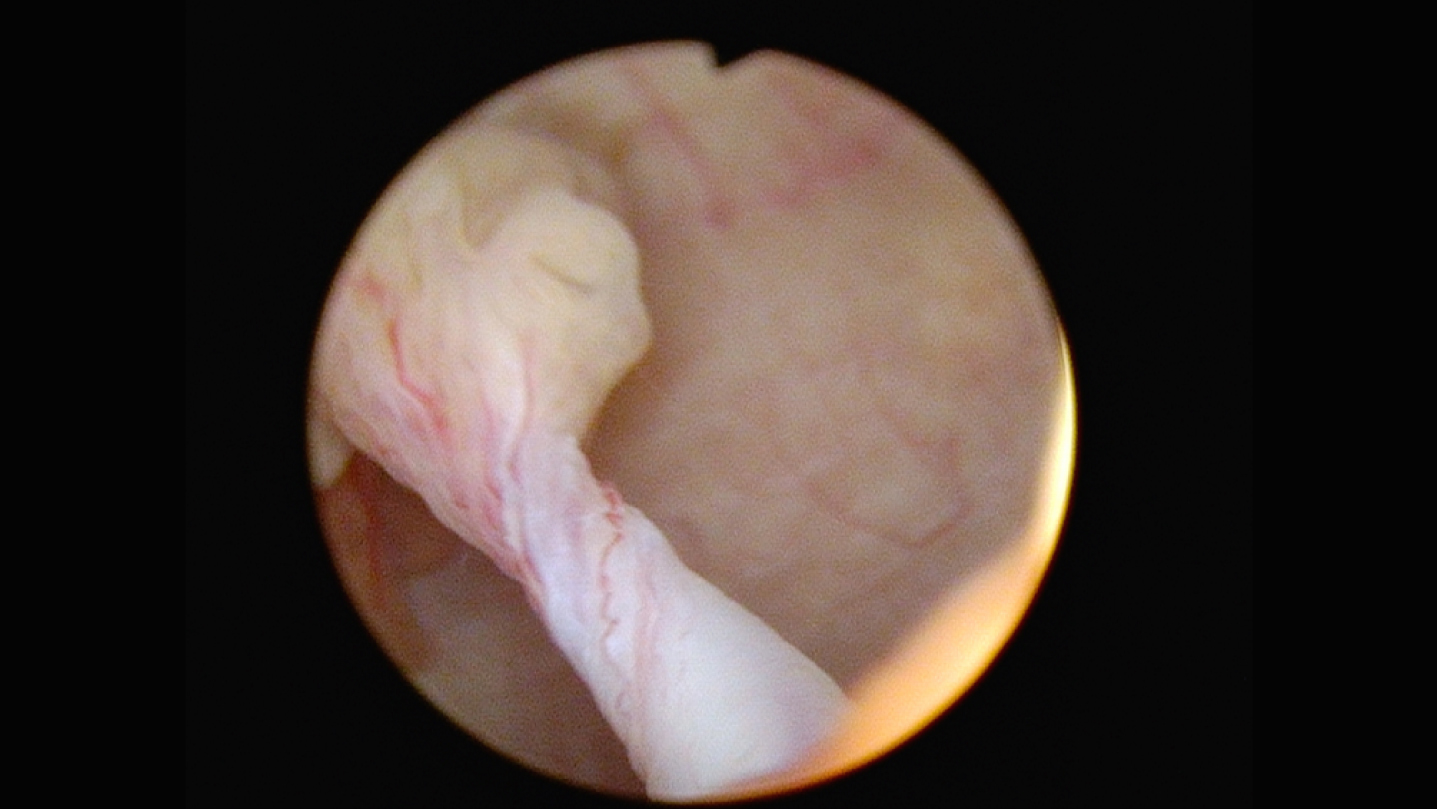
Fig. 3
Tumor grasped at base with forceps.
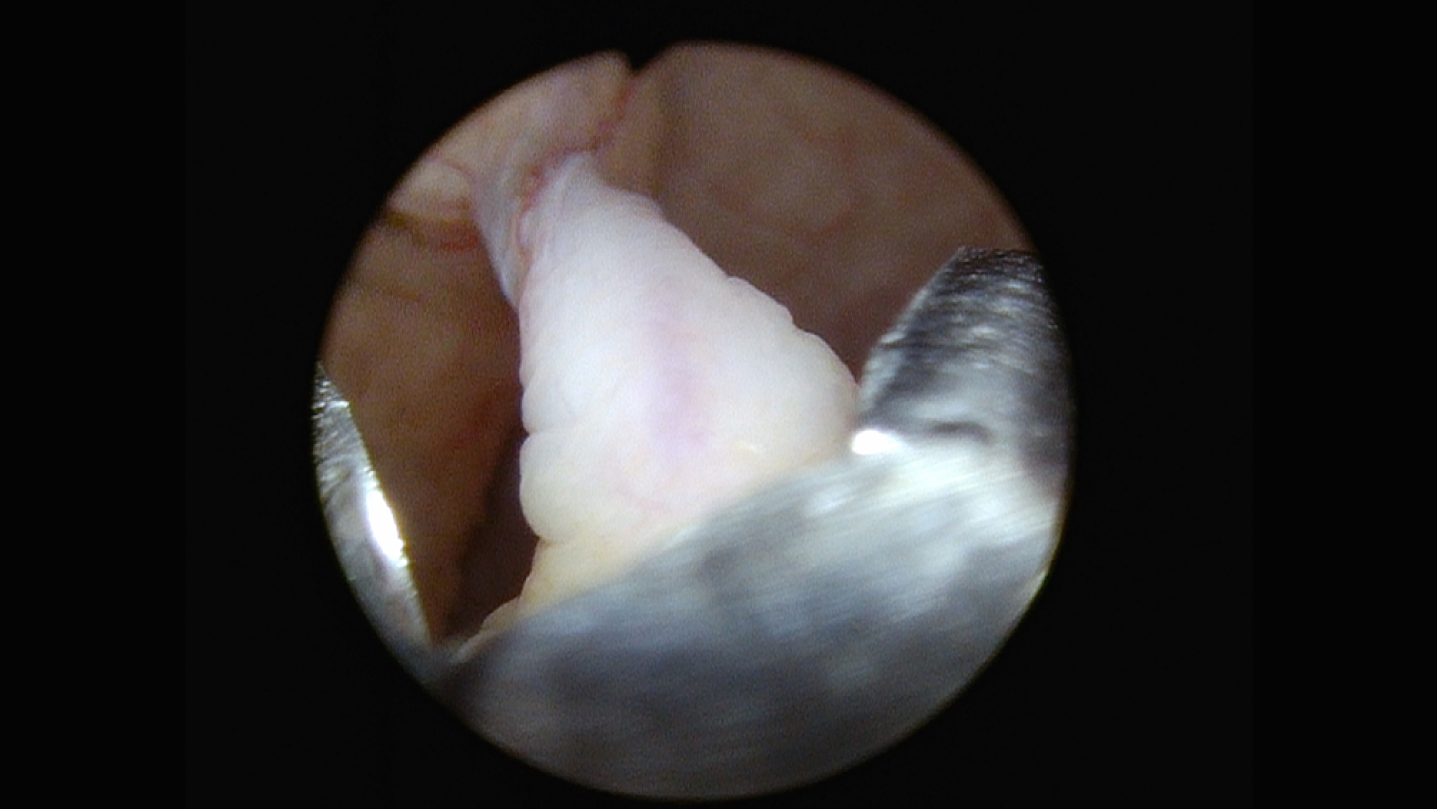
Fig. 4
Specimen intact.

Fig. 5
Base of tumor cauterized.
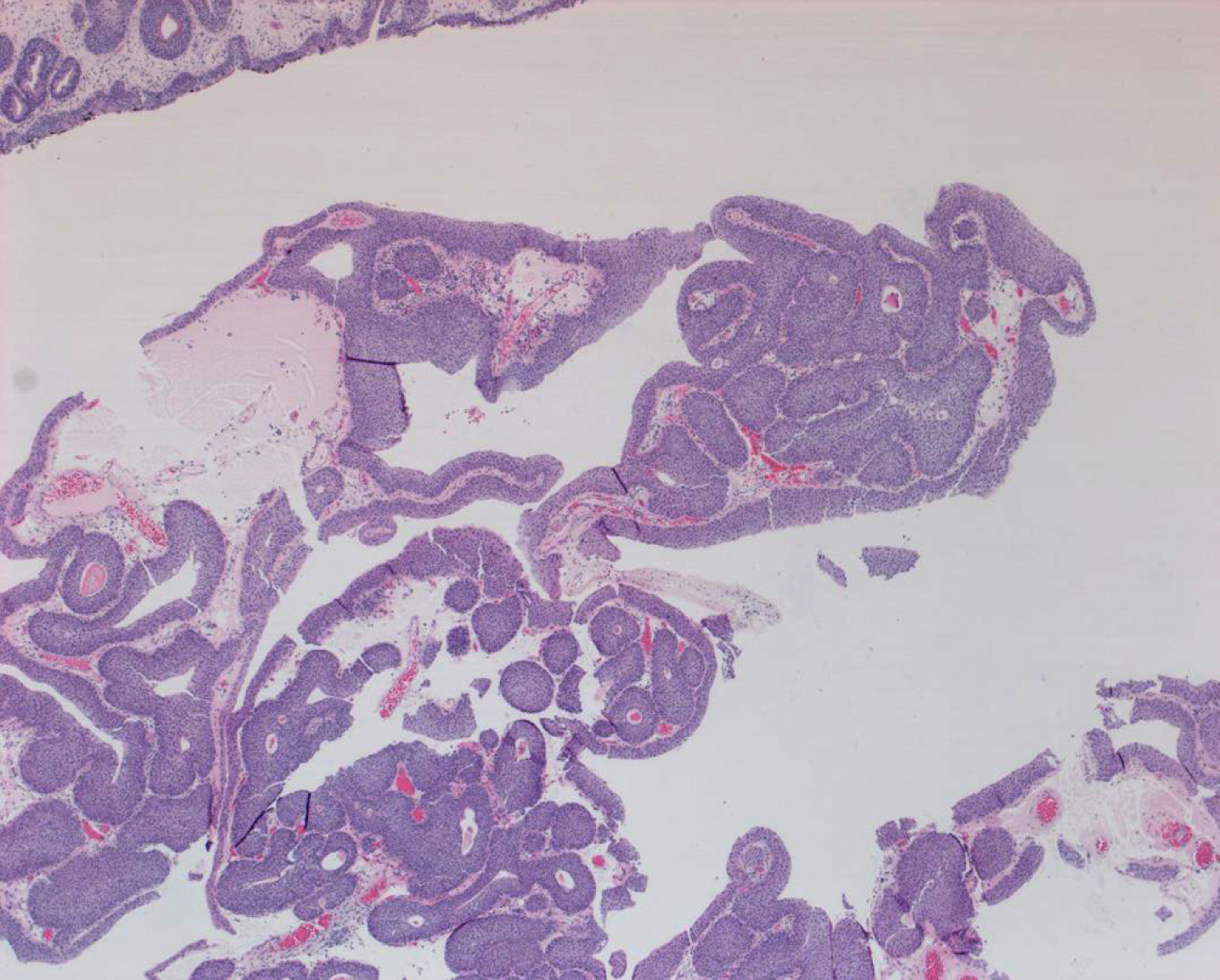
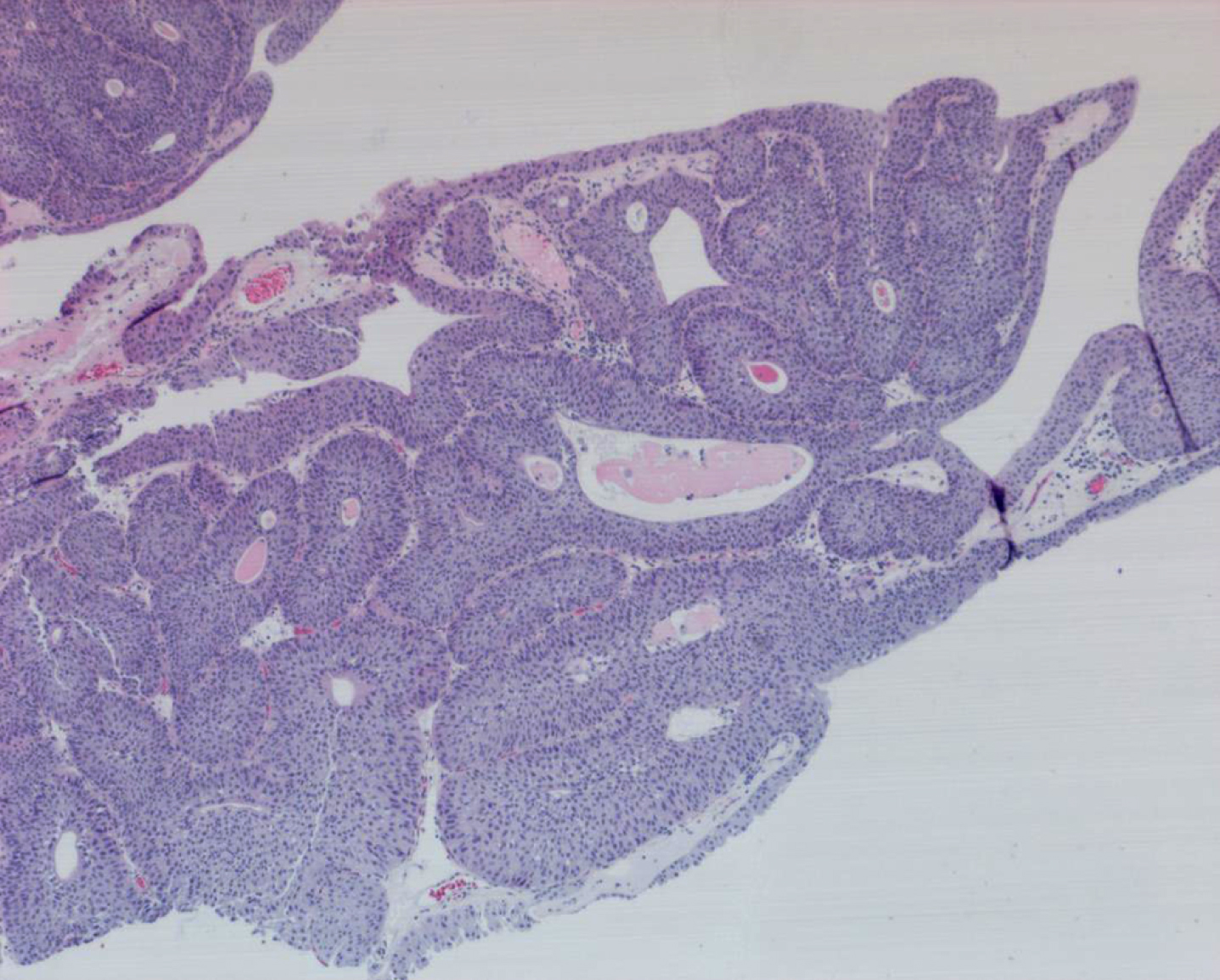
The pathology report indicated that this is a fibroepithelial polyp of the bladder which is a very uncommon benign neoplasm of the urinary tract (Figs. 6-7).
Fig. 6-7
Fibroepithelial polyp with inverted papilloma features. It is benign.
Does the patient require monitoring similar to a patient with a low grade non-invasive papillary bladder tumor (LG Ta)? I asked Michael O’Donnell, MD, and he replied he would perform a cystoscopy at six months and CT imaging of the urinary tract at 12 and 24 months. It is my impression that urinary cytology alone would suffice if any monitoring at all is required.
AUTHOR CONTRIBUTIONS
MSS contributed to the work conception, performance, analysis of data and writing; NAA supplied the histology description and the photos of the pathology.
INFORMED CONSENT
Written informed consent for publication was obtained from the patient.
ETHICAL CONSIDERATIONS
The author has institutional review board approval for reviewing bladder cancer cases for outcome (MHS.2020.026).
CONFLICT OF INTEREST
MSS and NAA have nothing to disclose.


