
The application of a feasible exercise training program in the office setting
Abstract
BACKGROUND: Previous research support the claim that people who work in offices and sit for a long time are particularly prone to musculoskeletal disorders.
OBJECTIVE: The main objective of this paper is to introduce an exercise training program designed to decrease muscle stiffness and pain that can be performed in the office setting.
METHODS: Forty healthy office workers (age: 28±5.3 years old; body mass: 87.2±10.2 kg; height: 1.79±0.15 m) apart from suffering from any sub-clinical symptoms of muscle and joint stiffness, and who had at least two years of experience in office work were chosen and randomly assigned to either an experimental group (n = 20) or a control group (n = 20). The experimental group performed the exercise training program three times a week for 11 weeks. The Cornell Musculoskeletal Discomfort Questionnaire was used to measure the pain levels in the neck, shoulders, and lower back areas. The Borg CR-10 Scale was used to measure their perceived exertion when doing the exercises, and a goniometer was used to measure the changes in range of motion (ROM) of the neck, hips, knees, and shoulders.
RESULTS: The overall results indicated that the exercise program could significantly (p < 0.05) reduce the neck, shoulders, and lower back pains of the participants in the exercise group while those in the control group showed no improvement in those pains. There were significant (p < 0.05) increases in the ROM of the hips, the neck, both knees and shoulders in the exercise group. Participants showed significant (p = 0.011) decreases in perceived exertion scores after the exercises.
CONCLUSIONS: The exercise training program designed in this study not only can effectively reduce neck, shoulders, and lower back pains, but also can improve the ROM or flexibility of the office workers.
1Introduction
Lower back, neck, and shoulder pains are the most widespread musculoskeletal conditions worldwide that affect approximately 70% to 80% of adults at some point in their lives [1]. In the United States, approximately 1% of the population was chronically disabled as a result of lower back, neck, or shoulder pains [1, 2]. These musculoskeletal issues, which are particularly prevalent in industrialized countries, can result in both personal and socioeconomic consequences [1]. For example, they not only cause a poor quality of life, but also increase the amount of absenteeism from work and the number of long-term disability claims [3]. For those who are affected, some may experience sleep disturbances, chronic fatigue, and nervousness, while many others become victims of prescription medication abuse [4, 5]. The scale of this problem is anticipated to grow with the increase in the aging population and the advancement of industrialization in the developing world [6, 7].
There are a variety of risk factors (e.g., age, race, sex, and marital status) that contribute to lower back, neck, and shoulders pains. However, the most prevalent factor, especially among adolescents, is the extended amount of time spent on sitting [8]. In this regard, a non-pharmacological and practical way to prevent and treat such musculoskeletal disorders among office workers who spend most of their time sitting would be beneficial. To date, most of the research on musculoskeletal disorders has emphasized on ergonomic modification of the working environment, changing diet, or doing physical activity, but there are very few, if any, exercise packages specifically designed for their prevention and treatment.
The nature of office work is sitting and leaning forwards or sideways. Typical office workers have to sit and work for at least 8 hours a day in typing, answering the phone, and writing [9]. In most cases, office chairs are not adjustable in a way that meets the needs of the office workers and as a result, the neck or back of those office workers is not supported properly. Sitting and working for a long time in an improper position leads to the tightness and weakness of the muscles, which can lead to musculoskeletal disorders such as neck, shoulders, and lower back pains as well as anatomical disorders such as lordosis, kyphosis, and scoliosis [10, 11]. These problems can affect their daily mood and the quality of sleep at night, and eventually their work performance and personal life [12, 13]. Many of these workers with pain problems seek help from medical doctors and start using medicines, which can only solve the problems temporary [5, 14].
Physical activity is a necessary component of healthy living and is vital to maintain the musculoskeletal system in proper functioning order. Lack of exercise can cause stiffness and weakness of the joints and muscles. Those individuals who lead a sedentary lifestyle lose not only the strength, but also the flexibility of their muscles – both of which are important to physical fitness and to maintain natural postures [15, 16]. Regular exercise provides nourishment of the spinal discs, soft tissues, and ligaments. When an individual lacks exercise, these tissues become malnourished and begin to degenerate [17]. In addition, sitting in an office chair for long periods of time can cause or worsen the existing pain problems. Leaning forward or slouching in a chair for extended periods can overstretch the spinal ligaments and put undue strain on the intervertebral discs and the surrounding spinal structures [18]. Overtime, incorrect sitting posture and poor workplace ergonomics can contribute to or cause recurrent episodes of back, shoulders, and neck pains [4, 5].
Previous researchers have suggested to perform physical activity to reduce the pains, but a dedicated package of exercise training for this purpose does not exist [1]. For example, Clemes et al. (2014) emphasized the importance of physical activity [19]; however, they did not introduce a protocol for training and their suggestions were not related to the work place. Instead, they suggested performing general exercises outside of working hours, which is impractical as individuals would rather spend the time to work on other matters (e.g., with their families). The purpose of the current paper was to introduce a feasible exercise training program that could be performed in the office setting. The most important features that distinguish this innovative exercise program from all other exercise programs were: (1) it was easy to apply in an office environment, (2) no additional apparatus was needed, (3) all the exercises were easy to learn and perform, and had been recommended by the American College of Sports Medicine (ACSM) [17], and (4) this was the first time that a package of exercises specifically designed for office workers. For the purpose of the study, it was hypothesized that a series of well-planned stretching and resistance training exercises, performed in a particular sequence, can significantly reduce neck, shoulders, and lower back pains. It was also hypothesized that the participants’ ROM would be significantly improved after the 11-week exercise program.
2Methods
2.1Subjects
Forty healthy office workers (age, 28±5.3 years; body mass, 87.2±10.2 kg; height, 1.79±0.15 m) who had worked for at least two years in an office were chosen and randomly assigned to either an experimental group (n = 20) or a control group (n = 20). All subjects worked in the city of Serdang, Malaysia, when the study was conducted in February 2015. Before undergoing a physical examination by a qualified physician, all subjects filled out a health questionnaire, and those who had any chronic medical condition (which could create an unnecessary risk during exercise testing) were excluded from the study. The subjects’ schedule of daily activity was carefully evaluated by a personal trainer, certificated by the ACSM, both two days before the experiment and also during the testing. The testing procedures were performed in accordance with the Helsinki Declaration for the ethical treatment of human participants. This study was approved by the Institutional Review Board of the University Putra Malaysia (FPSK-EXP16-P046). The subjects were given a clear explanation of the objectives of the study as well as the potential risks involved, and a signed consent form was obtained from each subject. Subjects of the experimental group performed a set of exercises for 11 weeks while those in the control group were advised not to alter any of their daily activities or to participate in any type of exercise.
2.2Protocol (package of exercise training)
The exercise training program consisted of 13 different exercises (see Fig. 1) that were specifically designed for office workers. The set of exercises was designed to perform three times a week for 11 consecutive weeks, with each session lasted for approximately 10–15 minutes. Each individual exercise included 10 repetitions (or last for a period of 10–15 s), and the entire set of exercises should be performed three times each day (with a rest of 60–90 s between sets). All the exercises were designed to have slow, controlled, and constant movements. They involved in gradually applying tension to a muscle or muscle groups toward the joint’s range of motion (ROM) until the point of mild discomfort had reached [17]. These training exercises were modified from Mckenzie and William [18] and designed to reduce pains and to increase the flexibility of individuals as well as to be easy to perform in an office environment.
Fig.1
Diagrams and Description of the In-Office Exercise Protocol.
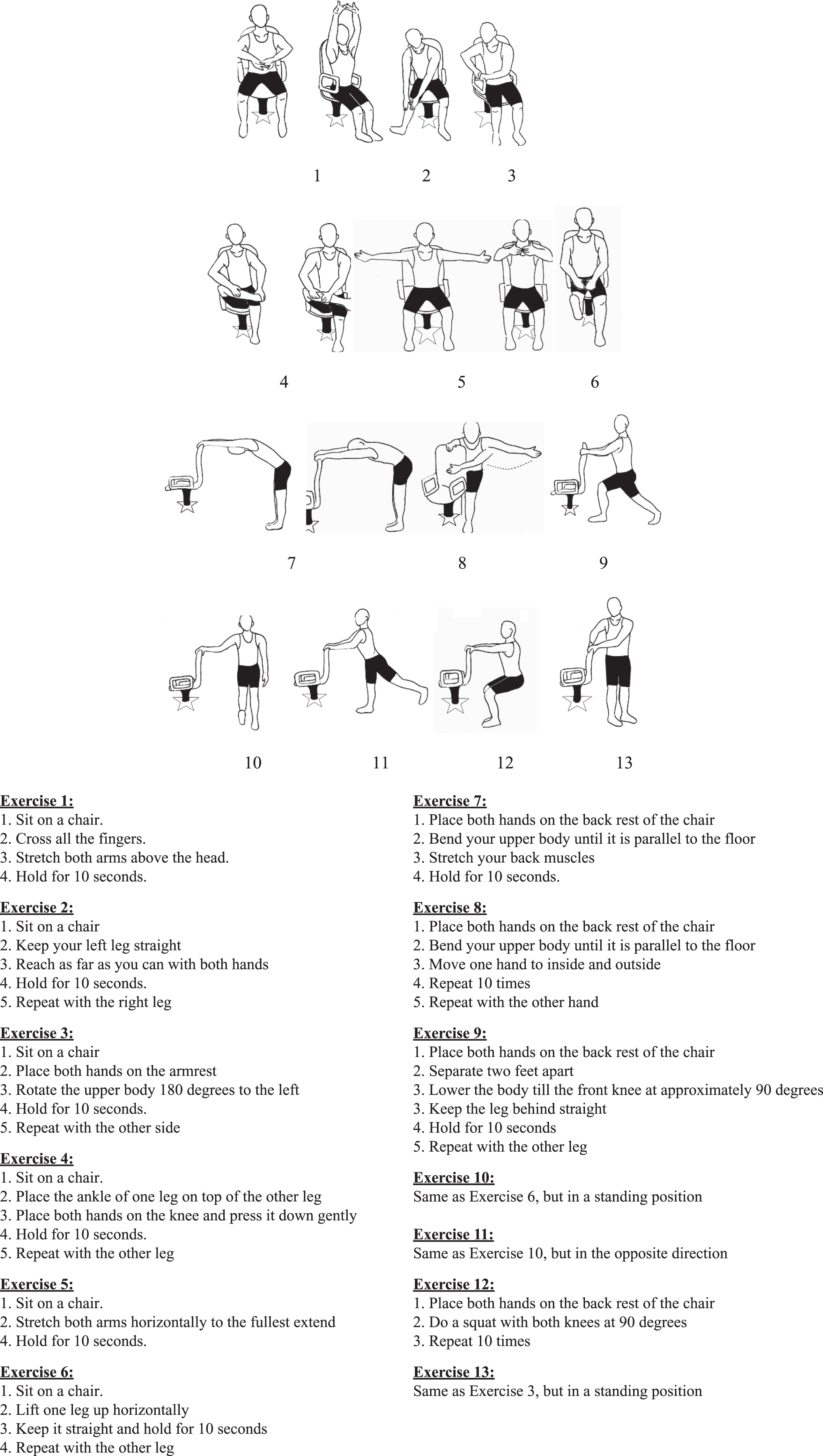
The demonstration of those exercises was recorded by a 15-minute video clip, which was sent to the subjects electronically so that it could be displayed on an electronic device such as a personal computer. The subject spent the first two weeks to learn and practice those exercises. Starting from weeks 3 to 5, the duration of each exercise was 10 s; during weeks 6 to 8, the duration increased to 20 s; and during weeks 9 to 11, the duration raised to 30 s (i.e., no change in the nature of exercises being performed, only the duration). The researchers were made available to the subjects’ working environment to check their progress and adherence to the protocol, and also to answer any questions they mighthave.
2.3Measurements
Anthropometric characteristics were measured by trained experts with a physician’s beam digital scale (SECA700; Chino, CA, USA). Subjects’ weight was measured (accuracy, ±0.10 kg) when they were barefoot with light clothing, followed by a barefoot measurement of height (accuracy±0.005 m). The Cornell Musculoskeletal Discomfort Questionnaire [3] was used to measure the severity of the pains in the neck, shoulders, and lower back areas. Each subject was asked to fill out the Questionnaire in two occasions: one before the exercise program, and one after the 11-week program. It was filled out by the subjects in the presence of the researcher.
In addition, the ROM in the neck (bending to the right and left), shoulders (abduction and adduction, flexion and extension), hips (flexion and extension), and knees (flexion and extension) were measured using a 12-inch goniometer (Lafayette Instrument Company, USA). This goniometer has a clear plastic construction that permits observation of a joint’s axis of motion and its ROM, marked in 1° increments. The reliability of this instrument was well-established, with an ICC coefficient from 0.785 to 0.978 [20]. The subjects were examined on a table 30 inches high (Winco 8570, SW MED-Source, USA). The Borg CR-10 Scale was used to assess the rating of perceived exertion (RPE) [21, 22] to ensure that the exercise intensity being performed was low-to-moderate. The Borg CR-10 scale scores from 0 to 10 and has been widely used to evaluate exercise intensity in clinical and sporting settings and the reliability (ICC coefficient) of this Scale is between 0.805 and 0.954 for office exercises [20]. The Scale can be self-administered or be recorded by an expert. The scores being recorded depend on the targeted subjects and the type of exercises. As the present participants have a wide range of backgrounds with regard to types of exercise and ability, the RPE should be easy-to-moderate (1–5 on the Borg scale) for these stretching exercises that target the neck (rotation and bending), shoulders (abduction, elevation and flexion), and lower back (bending, rotation, flexion and extension). All measurements were made before the beginning of the exercise package and again at the conclusion of the 11-week program.
2.4Statistical analysis
Descriptive statistics is presented in mean and standard deviation. The distributions of dependent variables in both groups were subjected to normality tests. Since the results were normally distributed, factorial 2 (Exercise) × 2 (Group) mixed design ANOVAs were performed to examine the main effects of exercises (on pains) and between groups as well as their interactions. Two-way repeated measures ANOVAs were utilized to compare the within-subjects factor (pre-test versus post-test) and the between-subjects factor (experimental versus control) of the ROM.
3Results
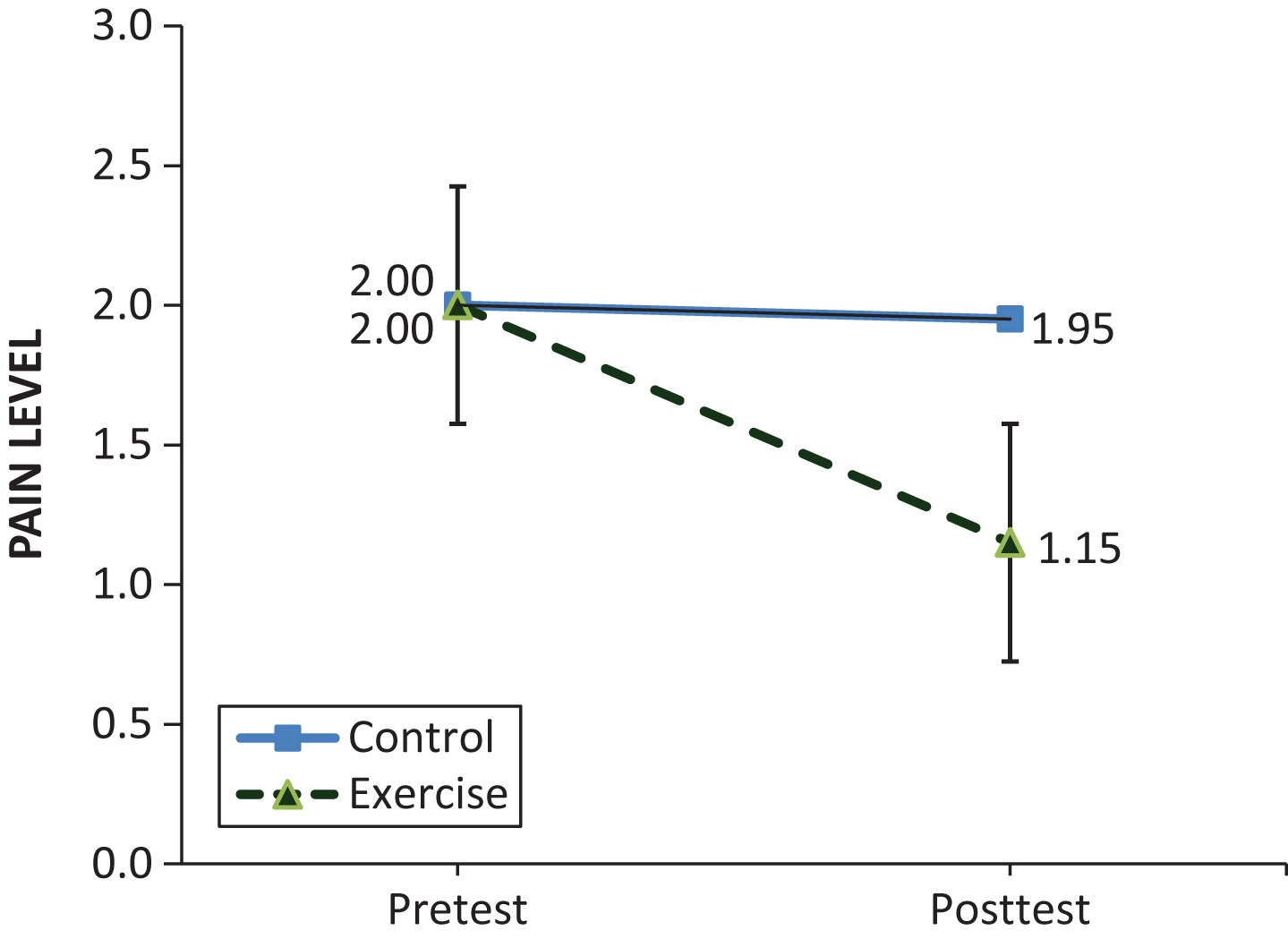
Results of the factorial 2×2 mixed-design ANOVA (Fig. 2) indicated that there was a significant interaction in neck (F1,38 = 6.835, p = 0.013; observed power = 0.722) as well as significant main effects for both Exercise (F1,38 = 4.374, p = 0.043; observed power = 0.531) and Group (F1,38 = 13.380, p = 0.001; observed power = 0.946). For the shoulders (Fig. 3), there was a significant interaction (F1,38 = 50.000, p < 0.001; observed power = 1.000) and a significant main effect for Exercise (F1,38 = 72.000, p < 0.001; observed power = 1.000), but the main effect for Group was not significant (F1,38 = 0.048, p = 0.828; observed power = 0.055). Likewise for the results of the lower back (Fig. 4), where there was a significant interaction (F1,38 = 25.600, p < 0.001; observed power = 0.999) and a significant main effect for Exercise (F1,38 = 32.400, p < 0.001; observed power = 1.000), but the main effect for Group was not significant (F1,38 = 3.713, p = 0.061; observed power = 0.467). The overall results indicated that the exercise program could significantly reduce the neck, shoulders, and lower back pains of the participants in the exercise group, while those in the control group showed no significant improvement in those pains.
Fig.2
Comparisons of Neck Pain Levels Between the Exercise and Control Groups.
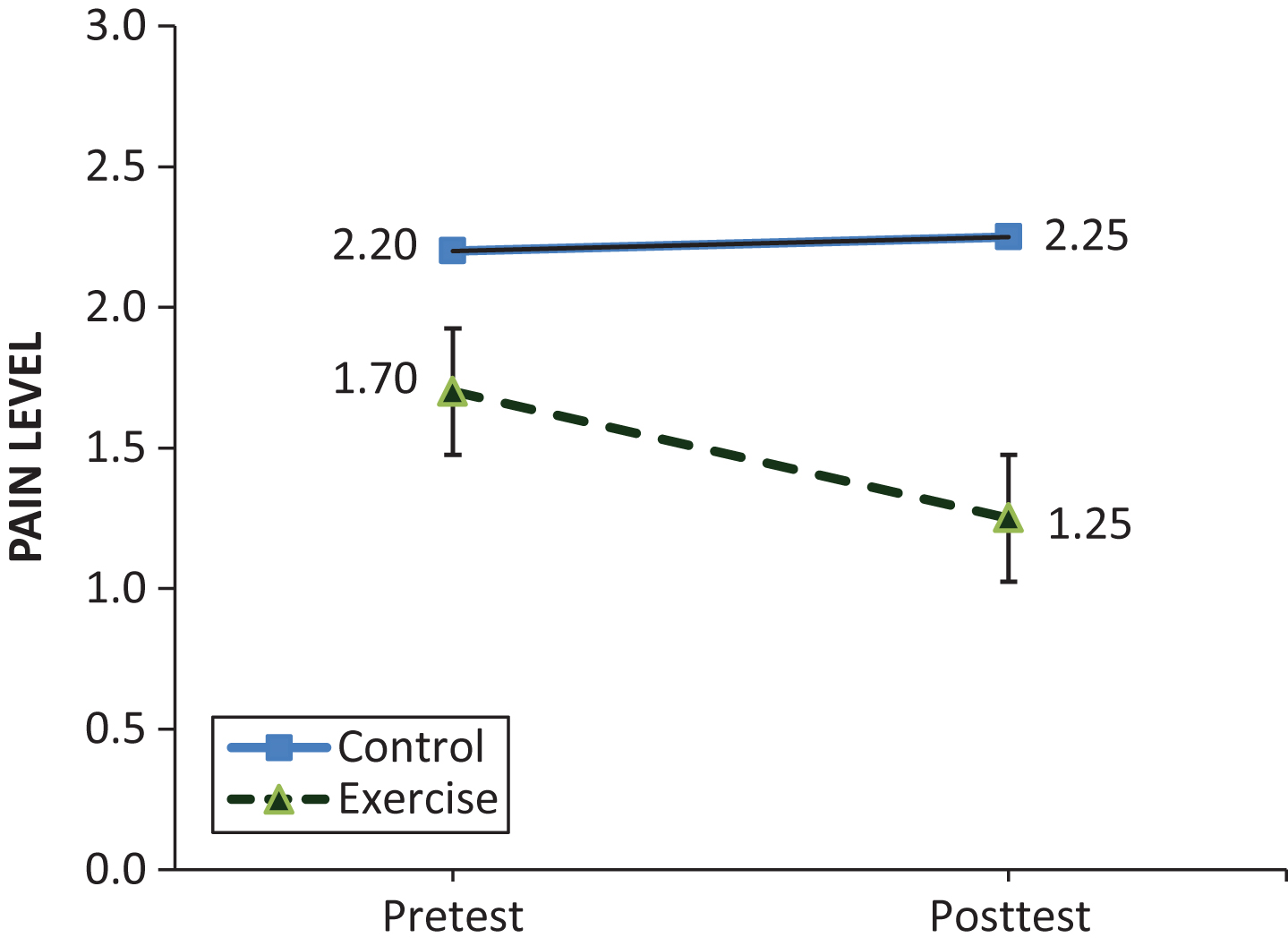
Fig.3
Comparisons of Shoulder Pain Levels Between the Exercise and Control Groups.
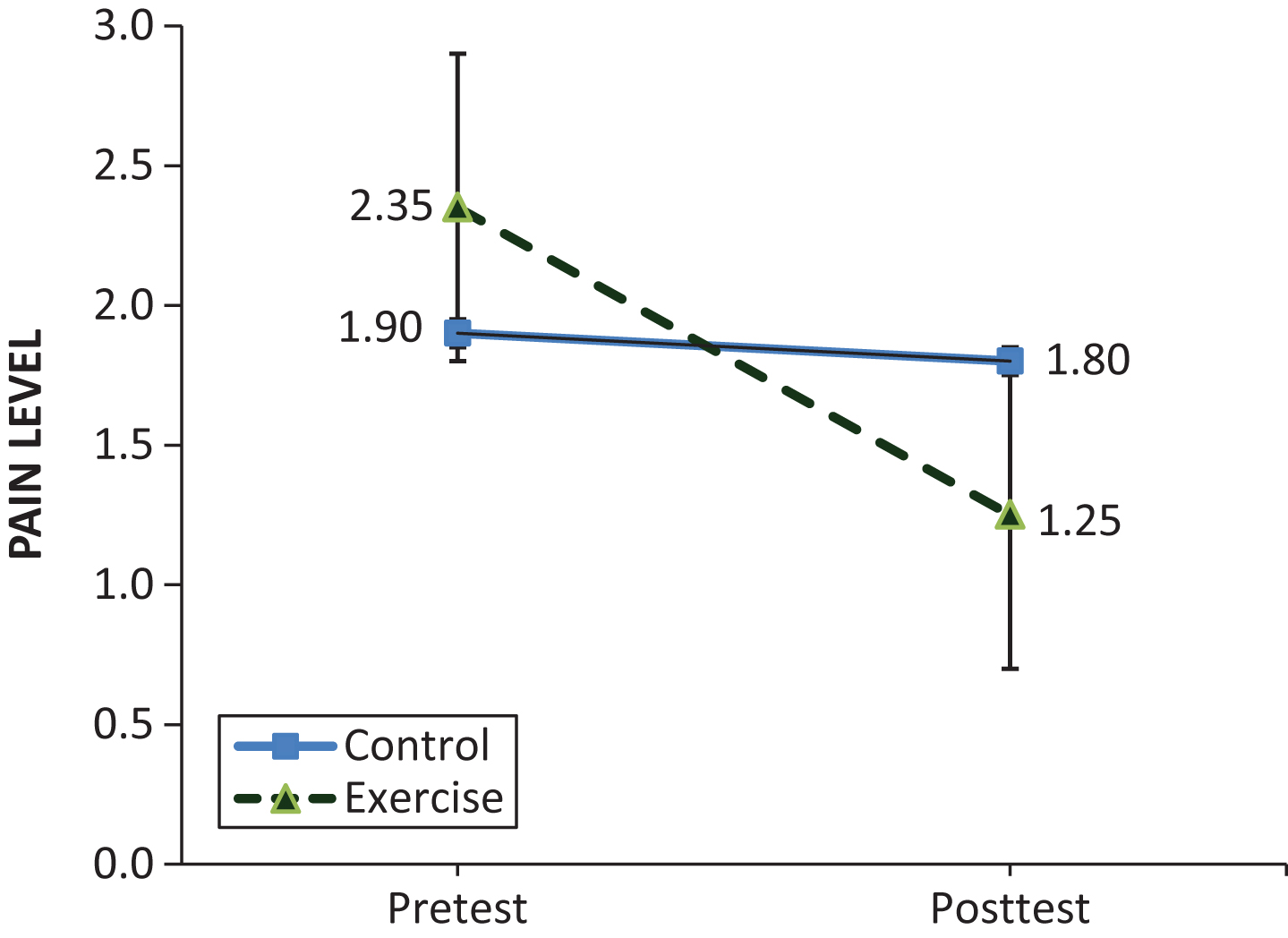
Fig.4
Comparisons of Lower Back Pain Levels Between the Exercise and Control Groups.
Results of the repeated measures ANOVAs for the ROM are presented in Table 1. All the measures of the ROM were found to be significant (p < 0.001). The largest effect size was come from neck bending (i.e., partial eta squared >0.93). Though there were no significant (p > 0.05) differences in the ROM and flexibility between the exercise and control groups at the baseline level, significant (p < 0.05) differences were found between them in all the measuring variables after the 11-week exercise training program (see Table 2). Results of the dependent t-test indicated that there was a significant (p = 0.011) difference in the RPE among subjects of the exercise group before (3.45±1.47) and after (1.50±0.61) the 11-week exercise program. The results showed that as the time doing the exercises (11 weeks) progressed and the musculoskeletal conditions improved, the perceived effort required decreased.
Table 1
Results of Within/Between Repeated Measures ANOVA for the Range of Motion and Flexibility
| Variable | MS | F-ratio | p value | Partial Eta |
| Squared | ||||
| Right Hip Range of Motion | 1767.200 | 148.127 | <0.001 | 0.796 |
| Left Hip Range of Motion | 1584.200 | 128.426 | <0.001 | 0.772 |
| Right Hamstring Flexibility | 1312.200 | 109.398 | <0.001 | 0.742 |
| Left Hamstring Flexibility | 1178.113 | 22.872 | <0.001 | 0.376 |
| Right Shoulder Abduction | 224.450 | 24.772 | <0.001 | 0.395 |
| Left Shoulder Abduction | 231.200 | 29.646 | <0.001 | 0.438 |
| Right Shoulder Flexion | 110.450 | 16.221 | <0.001 | 0.299 |
| Left Shoulder Flexion | 201.613 | 32.072 | <0.001 | 0.458 |
| Right Neck Bending | 768.800 | 524.025 | <0.001 | 0.932 |
| Left Neck Bending | 1369.513 | 612.433 | <0.001 | 0.942 |
Table 2
Pairwise Comparisons (Bonferroni tests) of pre-/post-test Differences Between Groups in the Ranges of Motion and Flexibility
| Range of Motion | Time | Exercise Group Mean±SD | Control Group Mean±SD | P value |
| Right Hip | PRE | 64.75±17.53 | 68.05±11.68 | 0.488 |
| POST | 82.30±13.62 | 66.80±12.16 | 0.001** | |
| Left Hip | PRE | 64.85±17.54 | 67.15±11.68 | 0.628 |
| POST | 82.70±14.06 | 67.20±11.42 | <0.001** | |
| Right Knee | PRE | 152.35±20.86 | 150.30±22.66 | 0.768 |
| POST | 168.95±17.09 | 150.70±23.36 | 0.008** | |
| Left Knee | PRE | 146.60±20.95 | 147.65±24.05 | 0.884 |
| POST | 162.25±18.73 | 147.95±24.03 | 0.043* | |
| Right Shoulder Abduction | PRE | 173.10±6.07 | 172.90±6.66 | 0.921 |
| POST | 179.70±0.47 | 172.80±6.81 | <0.001*** | |
| Left Shoulder Abduction | PRE | 172.70±5.39 | 172.00±5.79 | 0.695 |
| POST | 179.75±0.44 | 172.25±5.36 | <0.001*** | |
| Right Shoulder Flexion | PRE | 174.50±6.33 | 171.05±7.90 | 0.136 |
| POST | 179.15±1.73 | 171.00±7.99 | <0.001*** | |
| Left Shoulder Flexion | PRE | 173.55±5.64 | 171.70±6.63 | 0.348 |
| POST | 179.70±0.73 | 171.50±6.77 | <0.001*** | |
| Right Neck Bending | PRE | 46.15±10.18 | 47.25±8.16 | 0.708 |
| POST | 58.50±9.76 | 47.20±8.10 | <0.001*** | |
| Left Neck Bending | PRE | 45.05±10.07 | 44.95±8.04 | 0.972 |
| POST | 61.55±10.25 | 44.90±8.09 | <0.001*** |
*p < 0.05; **p < 0.01; ***p < 0.001.
4Discussion
The purpose of the current study was to introduce a feasible exercise training program that could be utilized in the office setting. The results supported both the hypotheses that a series of stretching and resistance training exercises, performed in a particular sequence, could significantly reduce neck, shoulders, and lower back pains as well as the ROM of the participants after the 11-week exercise program. The absence of physical activity among office workers is the most important reason for their musculoskeletal disorders, especially in the neck, shoulders, and lower back areas. Since the main cause of these pains is related to the stiffness and weakness of muscles, those stretching and strengthen exercises introduced in this study are effective in reducing office workers’ muscle pains. The results of the current study are consistent with previous research. For example, the study of bus drivers by Tamrin et al. concluded that sitting for long periods of time was the major cause of musculoskeletal disorders [5]. Similarly, Cho et al. (2012) indicated that the working style and the absence of physical activity were the most important factors responsible for neck, shoulders and lower back pains [23]. Tunwattanapong et al. assessed 96 office workers with neck and shoulders pains and concluded that a four-week stretching program could decrease the pains in the neck and shoulders significantly. They explained the reason behind such decrease in pains was related to the effect of stretching on proprioception [24].
The main goal of the exercise program in this study is to reduce pains in the neck, shoulders, and lower back. However, the participants can gain additional benefits from the program by improving their ROM. The results showed that the most significant improvements in the ROM were found in the hips and neck. This is probably the set of training exercises is more effective in these two areas rather than the shoulders. The results showed that the left shoulders and neck muscles have made more improvement in the ROM than those muscles on the right side. As most of the subjects mainly used the right side of their body, the increased muscle tightness can be related to the less active muscles on the left side and the big muscles. The results of this study are confirmed by other researchers that people tend to use one side of their body rather than both sides equally [25], and the big muscles are mostly affected by exercise training or any sport treatment [26]. The findings of the current study are also comparable with those found by Miyamoto et al., who measured the effect of Pilates exercise (stretching based) on 43 individuals with low back pain. The results of their 6-week intervention showed that this type of exercise was effective in increasing the flexibility of the hips and back muscles while decreasing their functional disability [27].
Considering the results from the Borg CR-10 Scale, all scores of the participants were significantly decreased after the intervention program. It seems that as the office workers do mostly bending and flexion movements during their office hours, this type of exercise training is effective on their muscles. Jakobsen et al. (2014) showed that the Borg CR-10 scale was a useful and valid instrument to measure RPE among workers, and they also mentioned that the effect of strength training on RPE was greater than the effects of flexibility or stretching exercises [22].
Though Thorp et al. (2012) asserted that standing for a long time was the major cause of lower back and shoulder pains among office workers [28], the exercise program developed in this study can also be applied to workers in a standing working environment. Though the design of the exercise protocol is for in-office setting, the program can also be considered as a non-pharmacological treatment for neck, shoulders, and lower back pain among office workers both during and outside working hours [29] since the protocol covers most large muscles, such as multifidus, that support the vertebral column. Nevertheless, one limitation of this study is that the diet of the participants was not considered nor controlled since Blackford et al. (2013) expressed that the control for the diet as well as performing exercise training had a significant effect on physical health [29]. Further study should include this variable and examining workers in different working conditions (e.g., sitting and standing).
5Conclusion
The exercise training program designed in this study is an effective tool that can be used as a treatment or prevention of musculoskeletal disorders such as neck, shoulders, and lower back pains. One important feature about the exercise program is that it can be performed by office workers in their office, not beyond their working hours (which is not practical). Another benefit of the excise program is to improve the ROM or flexibility of the office workers. Limited ROM can lead to pain, injury, and poor overall performance (e.g., full muscular potential). The flexibility components of the exercise program in this study can facilitate the office workers to obtain better postural control and decreased stress. As a result, this would lower the amount of absenteeism and increase the productivity of the office workers.
Conflict of interest
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
There was no grant or funding for this research and it was done by the personal budget of researchers.
Acknowledgments
Special great thanks to Pro. David Pyne for reviewing the manuscript in spite of his busy schedule. We also thank Faculty of Medicine and Health Sciences, University Putra Malaysia for their support.
References
[1] | Coggon D , Ntani G , Palmer KT , Felli VE , Harari R , Barrero LH , et al. Disabling musculoskeletal pain in working populations: Is it the job, the person, or the culture? PAIN® (2013) ;154: :856–63. |
[2] | Helmick CG , Felson DT , Lawrence RC , Gabriel S , Hirsch R , Kwoh CK , et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum (2008) ;58: :15–25. |
[3] | Shariat A , Tamrin B , Arumugam M , Ramasamy R . The bahasa melayu version of cornell musculoskeletal discomfort questionnaire (CMDQ): reliability and validity study in Malaysia. Work A J Prev Assesment Rehabil (2016) ;53: :171–8. |
[4] | Mody GM , Brooks PM . Improving musculoskeletal health: Global issues. Best Pract Res Clin Rheumatol (2012) ;26: :237–49. |
[5] | Tamrin SBM , Yokoyama K , Aziz N , Maeda S . Association of risk factors with musculoskeletal disorders among male commercial bus drivers in Malaysia. Hum Factors Ergon Manuf Serv Ind (2014) ;24: :369–85. |
[6] | Steves CJ , Bird S , Williams FMK , Spector TD . The microbiome and musculoskeletal conditions of aging: A review of evidence for impact and potential therapeutics. J Bone Miner Res (2016) ;31: :261–9. |
[7] | Leveille SG . Musculoskeletal aging. Curr Opin Rheumatol (2004) ;16: :114–8. |
[8] | Smith CS , Folkard S , Tucker P , Evans MS . Work schedules, health, and safety. Handb Occup Heal Psychol 2nd ed. Washington, DC: Am Psychol Assoc; (2011) . |
[9] | Goossens RHM , Netten MP , Van der Doelen B . An office chair to influence the sitting behavior of office workers. Work (2012) ;41: :2086–8. |
[10] | Mörl F , Bradl I . Lumbar posture and muscular activity while sitting during office work. J Electromyogr Kinesiol (2013) ;23: :362–8. |
[11] | Kim D , Cho M , Park Y , Yang Y . Effect of an exercise program for posture correction on musculoskeletal pain. J Phys Ther Sci (2015) ;27: :1791–4. |
[12] | Gifford R . Environmental psychology matters. Psychology (2014) 65: , 541. |
[13] | Schultz D , Schultz SE . Psychology and work today 10E. Routledge; (2015) . |
[14] | Shariat A , Bahri Mohd Tamrin S , Daneshjoo A , Sadeghi H . The adverse health effects of shift work in relation to risk of illness/disease: A review. Acta Medica Bulg (2015) ;42: :63–72. |
[15] | Jussila L , Paananen M , Näyhä S , Taimela S , Tammelin T , Auvinen J , et al. Psychosocial and lifestyle correlates of musculoskeletal pain patterns in adolescence: A 2-year follow-up study. Eur J Pain (2014) ;18: : 139–46. |
[16] | Teo PS , Abdullah N-F , Chen CK , Aziz ME , Foo LH . High sedentary lifestyle practices has adverse influence on musculoskeletal health in adolescent boys and girls: Findings from a population-based study in Malaysia. Bone Abstracts (2013) ;2: :79. |
[17] | Medicine AC of S. ACSM’s guidelines for exercise testing and prescription. Lippincott Williams & Wilkins; (2013) . |
[18] | Hosseinifar M , Akbari M , Behtash H , Amiri M , Sarrafzadeh J . The effects of stabilization and McKenzie exercises on transverse abdominis and multifidus muscle thickness, pain, and disability: A randomized controlled trial in nonspecific chronic low back pain. J Phys Ther Sci (2013) ;25: :1541–5. |
[19] | Thorp AA , Healy GN , Winkler E , Clark BK , Gardiner PA , Owen N , et al. Prolonged sedentary time and physical activity in workplace and non-work contexts: A cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Act (2012) ;9: :128–36. |
[20] | Shariat A , Tamrin SB , Arumugam M , Danaee M , Ramasamy R . Comparative reliability of different instruments used to measure the severity of musculoskeletal disorders in office workers. Work (2016) ;54: (3):754–58. |
[21] | Capodaglio EM . Comparison between the CR10 Borg’s scale and the VAS (visual analogue scale) during an arm-cranking exercise. J Occup Rehabil (2001) ;11: : 69–74. |
[22] | Jakobsen MD , Sundstrup E , Persson R , Andersen CH , Andersen LL . Is Borg’s perceived exertion scale a useful indicator of muscular and cardiovascular load in blue-collar workers with lifting tasks? A cross-sectional workplace study. Eur J Appl Physiol (2014) ;114: :425–34. |
[23] | Cho C-Y , Hwang Y-S , Cherng R-J . Musculoskeletal symptoms and associated risk factors among office workers with high workload computer use. J Manipulative Physiol Ther (2012) ;35: :534–40. |
[24] | Tunwattanapong P , Kongkasuwan R , Kuptniratsaikul V . The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: A randomized controlled trial. Clin Rehabil (2016) ;30: :64–72. |
[25] | Kepler CK , Bogner EA , Herzog RJ , Huang RC . Anatomy of the psoas muscle and lumbar plexus with respect to the surgical approach for lateral transpsoas interbody fusion. Eur Spine J (2011) ;20: :550–6. |
[26] | Janssens J , Malfroid K , Nyffeler T , Bohlhalter S , Vanbellingen T . Application of LSVT BIG intervention to address gait, balance, bed mobility, and dexterity in people with Parkinson disease: A case series. Phys Ther (2014) ;94: :1014–23. |
[27] | Miyamoto GC , Costa LOP , Galvanin T , Cabral CMN . Efficacy of the addition of modified Pilates exercises to a minimal intervention in patients with chronic low back pain: A randomized controlled trial Phys Ther (2013) ;93: :310–20. |
[28] | Sihawong R , Janwantanakul P , Sitthipornvorakul E , Pensri P . Exercise therapy for office workers with nonspecific neck pain: A systematic review. J Manipulative Physiol Ther (2011) ;34: :62–71. |
[29] | Blackford K , Jancey J , Howat P , Ledger M , Lee AH . Peer Reviewed: Office-Based Physical Activity and Nutrition Intervention: Barriers, Enablers, and Preferred Strategies for Workplace Obesity Prevention, Perth, Western Australia, 2012. Prev Chronic Dis (2013) ;10. |

