
Guidelines for schoolbag carriage: An appraisal of safe load limits for schoolbag weight and duration of carriage
Abstract
BACKGROUND:
There is no global agreement on a schoolbag weight limit and little assessment of its utility. The duration of carriage is another factor yet there is no previous systematic assessment of the utility of cut-off values for it in identifying schoolbag-related discomfort.
OBJECTIVES:
The objectives were to establish if there was a threshold for musculoskeletal discomfort based on (i) percentage bodyweight (% BW) of the schoolbag; (ii) duration of carriage; or (iii) combined % BW and duration.
METHODS:
Using data from 462 primary school children, a novel experimental approach was used to explore the utility of conventional schoolbag weight limit guidelines and duration of carriage. A receiver operating characteristic (ROC) curve was constructed to examine the predictive performance of schoolbag weight and duration of carriage.
RESULTS:
The mean schoolbag weight (4.8±1.43 kg) represented a mean 12.4±4.18% BW. Only 30.7% of the sample carried schoolbags that were≤10% BW. The majority (76%) carried schoolbags to school for≤10 minutes. No % BW, duration of carriage or mechanical burden criterion provided a threshold cut-off point for accurately predicting schoolbag-related discomfort.
CONCLUSIONS:
Guidelines for safe schoolbag carriage that are based on mechanical factors alone could not be upheld. The association between duration of carriage and back discomfort warrants further investigation.
1Introduction
Schoolbag weight is the main factor that has been analyzed in an effort to develop guidelines for the safe carriage of schoolbags [1–6]. However, there is no global agreement on the cut-off point for a schoolbag weight limit. The current guideline in Europe and Australia is that children can carry a schoolbag that weighs up to 10% of their own bodyweight [7–11]. In the United States, the American Occupational Therapy Association recommends 10% bodyweight as the upper limit [12], the American Physical Therapy Association recommends 10–15% bodyweight [13] and the American Academy of Pediatrics recommends 10–20% bodyweight [14]. Despite these guidelines, there is inconsistent evidence for their use [5, 15–18] and little assessment of their utility.
The motivation for the development of schoolbag weight guidelines has been a proposed link between the bag weight and musculoskeletal discomfort. However, the relationship between schoolbag weight and musculoskeletal discomfort is not always clear as it has been found that the percent bodyweight (% BW) carried was both associated [5, 19] and not associated [20, 21] with musculoskeletal discomfort. Previous studies are mostly cross-sectional [10, 20, 21, 25, 29] and therefore have not been able to establish a dose–response relationship between schoolbag carriage and musculoskeletal discomfort. Additionally, they have not evaluated the discriminative ability of the proposed schoolbag weight cut-off values for identifying children with schoolbag-related discomfort. A recent study of the dose-response relationship between schoolbag weight and schoolbag-related discomfort concluded that the weight limit guidelines should be reviewed [22]. Additionally the focus of earlier studies has primarily been on back pain, but evidence indicates that schoolbag-related shoulder pain may be a greater problem than back pain[4, 19, 22].
The length of time that a child spends carrying a schoolbag has had scant attention, and it is not a specified factor in the guidance on schoolbag carriage. Although the duration of carriage has been reported [1, 4, 20, 23–28], the systematic assessment of the utility of cut-off values for duration of carriage in identifying schoolbag-related discomfort has not been undertaken.
Schoolbag weight and duration of carriage have been investigated within the same studies, but independent of each other [1, 4, 24, 26–28]. However fundamental biomechanical principles of load and energy consumption suggest that schoolbag weight, and the exposure to that weight, should be investigated in combination with each other in order to acquire a measure of the mechanical burden that results from carrying a schoolbag. Different loads carried for a fixed [29] or pre-determined [30] length of time have been examined, and the issue has been discussed in general terms [25, 31]. However the effects of schoolbag carriage that simultaneously take these two variables into account, as they increase incrementally, have not been investigated.
Based on a gap found within the evidence literature the aim of this study therefore was to explore the concept of a maximum safe limit for schoolbag weight and duration of schoolbag carriage. The objectives were to establish if there was a threshold beyond which musculoskeletal discomfort was significantly increased that could be based on (i) % BW of a schoolbag; or (ii) duration of carriage; or (iii) the combined % BW and duration i.e. the combined mechanical burden effect of carrying a schoolbag.
2Method
2.1Research design
A quasi-experimental pretest-posttest design was used to determine the prevalence of schoolbag-related musculoskeletal discomfort. A cross-sectional study design was used to establish the child and schoolbag weight, and the duration of carriage. A subset of the data collected as part of the study reported in [22] provided a suitable dataset for assessing the appropriateness of the different weight limit guidelines. The utility of current conventional discrete schoolbag weight limits, and schoolbag weight expressed as a continuous variable, were explored. A novel experimental approach was used to investigate the combined concurrent effects of schoolbag weight and duration of carriage. The dependent variable of interest was the effect of sub and supra-threshold load (10% , 15% , 20% BW) on schoolbag-related back and shoulder discomfort. The frequently used thresholds of duration of carriage (5, 10, 20 minutes) were also scrutinized.
2.2Participants
A purposive sample of children in primary school was included. Children in 4th or 5th class (9–11 year olds) who carried only a schoolbag to school on the day of data collection; i.e. they did not carry an additional item, were eligible for inclusion. Children who were unable to stand or who were unable to carry a schoolbag were excluded.
2.3Procedure
School principals were approached by email or telephone to seek permission for the study to be conducted in their school. An information package was sent to the approving principals for distribution to the potential participants. Within this package, written informed consent and assent was sought from each parent/guardian and child respectively. The study was approved by the Faculty of Health Sciences Ethics Committee, Trinity College Dublin.
A brief meeting was held with the participating children to instruct them on how to complete a Body Discomfort Chart (BDC) and Visual Analogue Scale (VAS). They were asked to complete the BDC and VAS before leaving for school the following morning, and to bring the completed forms to school, to give to the researcher at the study venue. Upon arrival at school, the children completed another BDC and VAS. Subsequently their weight and that of their schoolbag were measured. They were also asked about the duration of carriage of their schoolbag to school on the day of the study.
2.4Measures
2.4.1Body Discomfort Chart and Visual Analogue Scale
A self-completed Body Discomfort Chart (BDC) [32] and Visual Analogue Scale (VAS) [33] were used to assess discomfort before and after schoolbag carriage. Body charts have been widely used by ergonomists and clinicians as an assessment tool for pain or discomfort in children [30, 34, 35]. For this study, the point prevalence of discomfort before and after schoolbag carriage was ascertained by asking “Do you have any soreness or pain now?” If discomfort was reported, the child was instructed to ‘draw the sore area on the body chart’. The children were asked to rate their discomfort on the VAS by marking a 10 cm line with anchors of ‘no pain’ and ‘worst pain possible’ at the point that best described the intensity of their pain. The psychometric properties of the VAS have been investigated and the VAS has been demonstrated to have good reliability, validity and sensitivity for the measurement of pain intensity in children aged 8 years and older [36, 37].
2.4.2Child and schoolbag weight
The children were weighed under two conditions in a designated measuring zone using a Tanita HD-352 weighing scales; firstly without any bag, and secondly while carrying their schoolbag. The children were measured in stocking feet and light indoor clothing.
2.4.3Duration of carriage
The duration of carriage was ascertained with a researcher-assisted questionnaire. Training on the interpretation and completion of the questionnaire was provided for the research assistants prior to the commencement of the study.
The children were asked to state the actual length of time that they carried their schoolbag to school on the day of the study (<5, 5–10, 11–20, 21–30, or >30 minutes). The questionnaire contained 27 items, that have been reported earlier [22], but only those items relating to demographic information (n = 4), the child and schoolbag weight (n = 3), the schoolbag characteristics (n = 2) and the duration of carriage (n = 1) are reported here.
2.5Data analysis
Statistical analysis was conducted using Statistical Package for the Social Sciences (SPSS) software version 20.0 (SPSS Inc., Chicago, IL, USA). Descriptive analysis using percentages and means/SD was used for the analysis of schoolbag characteristics. From analysis of before and after schoolbag carriage BDC and VAS data, the onset and magnitude of discomfort attributable to the physical act of carrying a schoolbag could be identified. From this information, the children were classified into groups who ‘had’ or ‘did not have’ schoolbag-related discomfort. A Pearson’s Chi-square test was used to determine if the proportion of children with schoolbag-related discomfort differed across groups with differing thresholds of load (≤10% vs. >10% ; ≤15% vs. >15% ; ≤20% vs. >20% BW) and durations of schoolbag carriage (<5 vs. ≥5; ≤10 vs. >10; ≤20 vs. >20 minutes). In order to estimate the mechanical burden effect of schoolbag carriage on the children, the product of the % BW carried and the duration of carriage to school was calculated, and the term ‘combined mechanical burden (CMBbag)’ was used to denote it. The % BW calculations were based on the actual child and schoolbag weight. The ‘duration of carriage’ component was estimated as the midpoint of the time category that the child had selected on the researcher-assisted questionnaire. For example, if a child selected the ‘5–10 minutes’ category for the duration of carriage, for the purposes of this calculation, the result was calculated as 7.5 minutes. Risk ratios with 95% confidence intervals (95% CI) were calculated to explore the relative risk of the onset of schoolbag-related back or shoulder discomfort under different load (10% , 15% , 20% BW) and duration (5, 10, 20 minutes) exposure conditions, and both sensitivity and specificity were also calculated [38]. An independent t-test was used to compare the mechanical burden of children with and without schoolbag-related discomfort.
A receiver operating characteristic (ROC) curve was constructed to examine the predictive performance of (i) schoolbag load as % bodyweight; (ii) duration of carriage; and (iii) the combined mechanical burden (CMBbag) in identifying children with schoolbag-related discomfort. This graphical plot demonstrated the performance of the cut-off points in terms of sensitivity (i.e. true positive rate) versus 1-specificity (i.e. the false positive rate). The area under the curve (AUC) is a measure of the accuracy of a test or cut-off point. An AUC equal to 1.0 demonstrates that the test or cut-off point is 100% accurate, whereas a test thatcannot discriminate between two conditions has an AUC equal to 0.5. The area under the curve (AUC) was calculated and tested to determine if this was significantly greater than 0.5, the AUC which indicates that the classification system is no better than chance [39]. In the graphical plot a curve that follows the left hand border and the top border of the graph is indicative of a more accurate threshold [39] (as shown in Fig. 1). Calculations of sensitivity and specificity were made to test the validity of using % bodyweight, duration of schoolbag carriage and combined mechanical burden (CMBbag) as a guideline. Statistical significance at p < 0.05 was assumed for all tests.
3Results
The data analysed in this paper was from a discrete subgroup of the original participants in our prior report [22]. Eligibility for inclusion here was limited to children who carried only a schoolbag on the assessment day. The findings therefore are quite distinct from those reported elsewhere [22].
A total of 462 children were included in the analysis of child demographics and schoolbag characteristics. The mean age of the children was 10.6 years±6.9 months, and the sample comprised 53% males and 47% females. The majority (94.6%) had a backpack, 4.5% had a shoulder bag and 0.9% had a schoolbag on wheels. The majority (85%) carried their schoolbag over two shoulders. Not all children completed the BDC and VAS before and after schoolbag carriage therefore fewer children were included in the analysis of schoolbag-related back discomfort (n = 409) and shoulder discomfort (n = 407).
3.1Schoolbag weight
The mean schoolbag weight was 4.7±1.43 kg and this represented a mean % bodyweight of 12.4±4.18% BW. Only 31% had schoolbags that were ≤10% BW. Schoolbag-related back or shoulder discomfort was reported by 15.2% (n = 62) and 29.2% (n = 119) of children respectively. Chi-square analysis demonstrated that there was no significant difference in the proportions of children reporting back or shoulder discomfort according to the relative schoolbag load (≤ or >10% , 15% , 20% BW) as shown in Tables 1 and 2. The method of carriage (2 shoulders/not 2 shoulders) was also not significant for back discomfort (X2 = 0.124, n = 409, df = 1, p = 0.724) or shoulder discomfort (X2 = 0.020, n = 407, df = 1, p = 0.888). Risk Ratio calculations further indicated no significant association between load and discomfort. None of the conventional % BW cut-off points could be used to correctly identify those with schoolbag-related back or shoulder discomfort as no % BW criterion provided a threshold cut-off point with high sensitivity and specificity for predicting schoolbag-related musculoskeletal discomfort (Tables 1 and 2). From the ROC curve analysis it was clear that the ability of % BW of the schoolbag, expressed as a continuous variable, to discriminate between those with and without schoolbag-related back or shoulder discomfort was poor (AUC = 0.522 and 0.520 respectively, p > 0.05) as shown in Figs. 2 and 3. Likewise, in the ROC curve analysis, no % BW criterion provided a threshold cut-off point with both highsensitivity and specificity for predicting schoolbag-related back discomfort or shoulder discomfort.
3.2Duration of carriage
The majority of children (76%) carried their schoolbag for ≤10 minutes on the way to school. There was no significant difference in the prevalence of shoulder discomfort at any of the time intervals studied (Table 2). There was a significantly higher prevalence of schoolbag-related back discomfort in those who carried a schoolbag for ≥5 minutes compared to those who carried it for <5 minutes, however there was no significant difference between those who carried a schoolbag for ≤10 or ≤20 minutes compared to those who carried it for >10 or >20 minutes (Table 1). There was also a greater risk of back discomfort associated with carrying a schoolbag for more than 5 minutes compared to less than 5 minutes (RR = 2.0), however the association did not hold for the longer durations of 10 minutes (RR = 1.07) and 20 minutes (RR = 1.43) as shown in Table 1. In addition, the validity of using duration of carriage as an indicator of schoolbag-related musculoskeletal discomfort could not be upheld as calculations of sensitivity and specificity were low (Tables 1 and 2). Furthermore, the ability of duration of carriage to predict schoolbag-related back or shoulder discomfort was poor as seen in the ROC curve analysis (AUC = 0.57 and 0.49 respectively, p > 0.05), and no threshold of duration of carriage provided a cut-off point with high specificity and sensitivity (Figs. 2 and 3).
3.3Combined mechanical burden
The mean combined mechanical burden while carrying a schoolbag (CMBbag) was 94.5±74.0 kg.mins. The minimum was 10.3 kg.mins and the maximum was 442.7 kg.mins. The children who had schoolbag-related back discomfort had a higher mean CMBbag (108.1±73.93 kg.mins) than those who did not have discomfort (93.4±75.02 kg.mins), but the difference was not statistically significant (t = 1.428, df = 407, p = 0.154). There was also no significant difference in the mean CMBbag (t = 0.001, df = 405, p = 0.999) between those who had schoolbag-related shoulder discomfort (95.3±75.09 kg.mins) and those who did not have discomfort (95.3±74.88 kg.mins). ROC curve analysis showed that the AUC for the combined mechanical burden variable was significantly different from 0.5 with respect to schoolbag-related back discomfort (p = 0.033), but not for shoulder discomfort (p = 0.942) as shown in Figs. 2 and 3. However, neither of these analyses identified cut-off points for CMBbag with high sensitivity and specificity that could be used as a recommended threshold to predict schoolbag-related discomfort.
4Discussion
The current study tested existing guidelines for schoolbag carriage using a novel approach applied to a subset of the dose-response schoolbag carriage data reported in [22]. Similar to previous studies [10, 20, 21, 25, 29] a cross-sectional study design was used for the weight and duration of carriage measurements. However in contrast to previous cross-sectional studies, the prevalence of schoolbag-related musculoskeletal discomfort was established using a quasi-experimental pretest-posttest study design. It was therefore possible in this study to establish the dose-response relationship between schoolbag carriage and musculoskeletal discomfort. The utility of conventional discrete schoolbag weight limits (10, 15, 20% BW) and the weight limit as a continuous variable were examined from different statistical viewpoints. Schoolbag carriage is a global activity that is undertaken by 668 million primary school children [40], therefore the potential impact of the findings is wide-reaching. The findings challenge the suitability of using % bodyweight as a guideline for children’s’ schoolbags and are in keeping with others [5, 20, 41]. Additionally, given the increasing level of obesity in children [42] the calculation of a guideline based on % BW may not be an appropriate approach for individual children because their physical capacity or ability may not correlate with increases in their body weight. In this study, the 10% BW threshold demonstrated a good ability to identify true cases of schoolbag-related back or shoulder discomfort (sensitivity of 0.7–0.72). However, it had poor specificity (0.29) demonstrating a high false positive rate and illustrating its limited ability to be used as a load limit guideline [43]. That is, when the lowestconventional threshold (10% BW) was applied, over 70% of children with schoolbag-related discomfort were correctly identified, but only 29% of those who did not have discomfort were correctly identified. Thus the 10% BW threshold incorrectly classified 71% of those without schoolbag-related discomfort as being in the discomfort group. At the higher thresholds there was poor sensitivity at 15% BW (0.25–0.26) and 20% BW (0.03–0.07). That is, there was little or no ability to correctly identify true cases of children who experienced schoolbag-related discomfort. Furthermore, the probability of discomfort was similar irrespective of the relative schoolbag weight, and there was no evidence of a monotonic relationship between load and risk of back discomfort as the risk ratio (RR) was not higher at each incremental load threshold. These findings are similar to Jones et al. [44] who reported that schoolbag load did not contribute to the risk of developing low back pain in secondary school children. For shoulder discomfort there was a monotonic relationship between load and risk, but the relationship was not linear. The weakness of using % BW as a guideline was further demonstrated in the ROC curve analysis (Figs. 2 and 3) that showed the poor discriminative ability of any load to predict discomfort. In this study the AUC for % BW was close to 0.5 and the curve was close to the 45-degree diagonal of the graph which indicated that no threshold was more accurate at predicting schoolbag-related discomfort than a random guess. Similar analysis has not been undertaken previously, therefore comparisons with other studies could not be made, but these results provide substantial further evidence that relative schoolbag weight alone is not adequate as a guideline.
The duration of schoolbag carrying time was short, and was similar to that reported in the literature on primary school children [4, 26, 27]. Additionally, longer carrying times have been reported in studies that included secondary school children [23–25]. In contrast to others [4, 23–25] the current study did not find a consistent and significant association between duration of carriage and discomfort. It was of interest to note a significant association for carrying time of less than five minutes and back discomfort; however there was no monotonic relationship between duration of carriage and discomfort. An explanation may be that lifting or putting on the schoolbag caused some initial back pain or discomfort and this was reported in the shortest time interval. Although the shortest duration of carriage i.e. <5 minutes, had the highest sensitivity (0.63–0.77) of the three periods of time examined, it had poor specificity (0.37–0.39). Therefore the ‘5 minute’ threshold correctly identified 77% and 63% of children with schoolbag-related back and shoulder discomfort respectively, but incorrectly classified 62% of children without schoolbag-related discomfort as being in the discomfort group. These findings demonstrate that duration of carriage would not be accurate as a guideline for identifying children with schoolbag-related discomfort. Furthermore, the time spent carrying was shown to be a poor indicator of discomfort, as demonstrated by the Area Under the Curve (AUC), but it was close to significance (p = 0.070) for back discomfort as shown in Fig. 2. The different age of the sample population may have contributed to the disparity between this and previous studies of older children [23–25]. It may be the case that duration of carriage is a predictor for schoolbag-related musculoskeletal discomfort in adolescents given that they carry schoolbags for a longer period of time during the day [45]. The discrepancy between this study and another on primary school children [4] could be explained by the difference in type of schoolbag used; very few children in this study used a bag on wheels. The methodological differences between this and previous studies are also likely to account for some discrepancies.
Overall, the level of evidence for duration of carriage as a risk factor for schoolbag-related musculoskeletal discomfort is weak. Previous studies assessed the duration of carriage subjectively by questionnaire. In this study the duration of carriage was also estimated by the children on the researcher-assisted questionnaire. However, the researchers attempted to improve the accuracy with a brief discussion to verify the response with each child as they arrived to school. Furthermore, the response was not influenced by recall bias. An objective measure such as a stopwatch would provide more accurate data as it has been demonstrated that adolescents were not accurate in their estimation of schoolbag carrying time [46]. The accuracy of primary school children in estimating carriage time has not yet been explored, and given the findings of this study further investigation is warranted. If an association between objectively-measured duration of carriage and musculoskeletal discomfort was established, the guidance on schoolbag carriage could be developed to include this as a modifiable risk factor.
A novel approach in this study was the calculation and analysis of the combined concurrent effects of schoolbag weight and duration of carriage. Although the CMBbag had the best discriminative ability of the three variables, there was still no identifiable threshold with high sensitivity and specificity for CMBbag that could be used as a predictor of back or shoulder discomfort. The calculation of the CMBbag was based on the objectively collected data for % BW carried by the children, but the duration of carriage was determined subjectively. Further investigation with objective measures of duration of carriage should be considered in future studies.
For an appropriate schoolbag weight limit, it may be a more reasonable alternative to determine limits based on a risk assessment, similar to the approach used in manual handling for adults in the workplace [47]. For manual handling, the person is informed about the assessment of hazards and risks for musculoskeletal injury associated with manual handling [48]. Each person can then assess the risk and alter the modifiable hazards in order to minimise the risk and make the task as safe as possible. A risk assessment typically focuses on four domains: (i) the task, (ii) the individual person who is doing the task, (iii) the load and (iv) the environment [49]. For schoolbag carriage, the four domains would correspond to: (i) putting on/off and carrying the schoolbag, (ii) the child (characteristics, adequate training or knowledge) (iii) the schoolbag (characteristics, weight, frequency, duration, method of carriage and (iv) the environment (home, travel to/from school, school). In the case of primary school children, the parents and teachers could also be informed of the risk assessment of schoolbag carriage and could assist or advise the children. For example, parents could be instructed to assess for the correct fit of a schoolbag for their child, and advised to buy a schoolbag accordingly. Additionally, they could be advised about the optimum utilization of the schoolbag features, such as the shoulder strap length of a backpack. Previous studies that aimed to improve the knowledge and skills of children with regards to schoolbag carriage [50], posture while carrying a schoolbag [51, 52] and lifting in general [53] reported positive outcomes. Similarly, children who participated in back care education programs had significantly better knowledge [50–52] and practical skills [51, 53] after the program than they had before. In contrast, Feingold and Jacobs [54] reported no significant difference in children’s posture following a back care education session. The positive findings of the majority of these studies on back care education are encouraging and could have implications for the role of risk assessment and preventative strategies for schoolbag-related discomfort in children. The growing evidence for the association of psychosocial factors with musculoskeletal discomfort in children [9, 22, 55] must also be acknowledged, and reflected in future studies.
A limitation of the study was the limited age range of the participants. Children in 4th and 5th class in primary school (age 9–11) were included in the study and the findings therefore may not be extrapolated to all schoolchildren. A further limitation was the subjective estimation of the duration of carriage, although measures were used to ensure that the estimation was as accurate as possible.
The findings of this study would imply that there is no merit in recommending guidelines for safe schoolbag carriage that are based on mechanical factors alone. A threshold of % BW, duration of carriage or mechanical burden that could be used as a reliable cut-off point to detect true cases of schoolbag-related discomfort could not be identified. However, the association between duration of carriage and the combined mechanical burden and back discomfort would be worth further investigation.
Although this study would not support specific weight limit guidelines, it does seem reasonable that advice on best practice for schoolbag carriage should be provided to children, parents and teachers. Carrying a well-designed and correctly-fitted backpack over both shoulders has been accepted as the optimum method of carriage in the real-world setting. It is recommended that future research should focus on factors other than schoolbag weight limit guidelines.
Acknowledgments
The authors are grateful to the children who participated in the study and also to their parents, teachers and school principals for their co-operation. We are also grateful to the research assistants who were involved in data collection and entry.
References
[1] | Whittfield JK , Legg SJ , Hedderley DI . The weight and use of schoolbags in New Zealand secondary schools. Ergonomics. (2001) ;44: (9):819–824. |
[2] | Forjuoh SN , Lane BL , Schuchmann JA . Percentage of body weight carried by students in their school backpacks. Am J Phys Med Rehabil. (2003) ;82: (4):261–266. |
[3] | Bauer DH , Freivalds A . Backpack load limit recommendation for middle school students based on physiological and psychophysical measurements. WORK. (2009) ;32: (3):339–350. |
[4] | Dianat I , Javadivala Z , Asghari-Jafarabadi M , Asl Hashemi A , Haslegrave CM . The use of schoolbags and musculoskeletal symptoms among primary school children: Are the recommended weight limits adequate? Ergonomics. (2013) ;56: (1):79–89. |
[5] | Dockrell S , Simms C , Blake C . Schoolbag weight limit: Can it be defined? J Sch Health. (2013) ;83: (5):368–377. |
[6] | Dianat I , Sorkhi N , Pourhossein A , Alipour A , Asghari-Jafarabadi M . Neck, shoulder and low back pain in secondary schoolchildren in relation to schoolbag carriage: Should the recommended weight limits be gender-specific? Appl Ergon. (2014) ;45: (3):437–442. |
[7] | Voll HJ , Klimt F . Strain in children caused by carrying schoolbags. Offentliche Gesundheitswesen. (1977) ;39: (7):369–378. |
[8] | Cottalorda J , Rahmani A , Diop M , Gautheron V , Ebermeyer E , Belli A . Influence of school bag carrying on gait kinetics. J Pediatr Orthop B. (2003) ;12: (6):357–364. |
[9] | van Gent C , Dols JJ , De Rover CM , Hira Sing RA , De Vet HC . The weight of schoolbags and the occurrence of neck, shoulder, and back pain in young adolescents. Spine (Phila Pa 1976). (2003) ;28: (9):916–921. |
[10] | Skaggs DL , Early SD , D’Ambra P , Tolo VT , Kay RM . Back pain and backpacks in school children. J Pediatr Ortho. (2006) ;26: (3):358–363. |
[11] | Education Queensland; 2014. [cited 2014 Oct 08]. Available from: http://education.qld.gov.au/health/pdfs/healthsafe. |
[12] | American Occupational Therapy Association; 2014 [cited 2014 Apr 25]. Available from: http://www.aota.org. |
[13] | American Physical Therapy Association; 2014 [cited 2014 Apr 25]. Available from: http://www.apta.org. |
[14] | American Academy of Pediatrics; 2014 [cited 2014 Apr 25]. Available from: https://www.aaorg. |
[15] | Mackenzie WG , Sampath JS , Kruse RW , Sheir-Neiss GJ . Backpacks in children. Clin Orthop Rel Res. (2003) ;409: :78–84. |
[16] | Brackley HM , Stevenson JM . Are children’s backpack weight limits enough? A critical review of the relevant literature. Spine (Phila Pa. (2004) ;29: (19):2184–2190. |
[17] | Cardon G , Balague F . Backpacks and spinal disorders in school children. Eura Medicophys. (2004) ;40: (1):15–20. |
[18] | Lindstrom-Hazel D . The backpack problem is evident but the solution is less obvious. WORK. (2009) ;32: (3):329–338. |
[19] | Moore MJ , White GL , Moore DL . Association of relative backpack weight with reported pain, pain sites, medical utilization, and lost school time in children and adolescents. J Sch Health. (2007) ;77: (5):232–239. |
[20] | Negrini S , Carabalona R . Backpacks on! Schoolchildren’s perceptions of load, associations with back pain and factors determining the load. Spine (Phila Pa 1976). (2002) ;27: (2):187–195. |
[21] | Korovessis P , Koureas G , Zacharatos S , Papazisis Z . Backpacks, back pain, sagittal spinal curves and trunk alignment in adolescents: A logistic and multinomial logistic analysis. Spine (Phila Pa 1976). (2005) ;30: (2):247–255. |
[22] | Dockrell S , Simms C , Blake C . Schoolbag carriage and schoolbag-realted musculoskeletal discomfort among primary school children. Appl Ergon. (2015) ;51: :281–290. |
[23] | Grimmer K , Williams M . Gender-age environmental associates of adolescent low back pain. Appl Ergon. (2000) ;31: (4):343–360. |
[24] | Chiang HY , Jacobs K , Orsmond G . Gender-age environmental associates of middle school students’ low back pain. WORK. (2006) ;26: (2):197–206. |
[25] | Talbott NR , Bhattacharya A , Davis KG , Shukla R , Levin L . School backpacks: It’s more than just a weight problem. WORK. (2009) ;34: (4):481–494. |
[26] | Kellis E , Emmanouilidou M . The effects of age and gender on the weight and use of schoolbags. Pediatr Phys Ther. (2010) ;22: (1):17–25. |
[27] | Adeyemi AJ , Rohani JM , Abdul Rani M . Back pain arising from schoolbag usage among primary schoolchildren. Int J Ind Ergonom. (2014) ;44: (4):590–600. |
[28] | Mwaka ES , Munabi IG , Buwembo W , Kukkiriza J , Ochieng J . Musculoskeletal pain and school bag use: A cross-sectional study among Ugandan pupils. BMC Res Notes. (2014) ;7: (1):222. |
[29] | Kistner F , Fiebert I , Roach K , Moore J . Postural compensations and subjective complaints due to backpack loads and wear time in schoolchildren. Pediatr Phys Ther. (2013) ;25: (1):15–24. |
[30] | Mackie HW , Legg SJ . Postural and subjective responses to realistic schoolbag carriage. Ergonomics. (2008) ;51: (2):217–231. |
[31] | Haselgrove C , Straker L , Smith A , O’Sullivan P , Perry M , Sloan N . Perceived school bag load, duration of carraige, and method of transport to school are associated with spinal pain in adolescents. Aust J Physiother. (2008) ;54: (3):193–200. |
[32] | Corlett EN , Bishop RP . A technique for assessing postural discomfort. Ergonomics. (1976) ;19: (2):175–182. |
[33] | Huskisson EC . Measurement of pain. J Rheumatol. (1982) ;9: (5):768–769. |
[34] | Whittfield JK , Legg SJ , Hedderley DI . Schoolbag weight and musculoskeletal symptoms in New Zealand secondary schools. Appl Ergon. (2005) ;36: (2):193–198. |
[35] | Birnie K , Chambers C , Fernandez C , Forgeron P , Latimer M , McGrath P , Cummings E , Finley A . Hospitalized children continue to report undertreated and preventable pain. Pain Res Manag. (2014) ;19: (4):198–204. |
[36] | Stinson JN , Kavanagh T , Yamada J , Gill N , Stevens B . Systematic review of the psychometric properties, interpretability and feasibility of self-report pain intensity measures for use in clinical trials in children and adolescents. Pain. (2006) ;125: (1-2):143–157. |
[37] | Champion G , Goodenough B , von Baeyer C , Thomas W . Measurement of pain by self report. In: Measurement of pain in infants and children. In: Finley G, McGrath P, editors. Progress in Pain Research and Management. IASP press (1998) ;10: :123–160. |
[38] | Confidence interval analysis software. University of Southampton; 2014 [cited 2014 Feb 02]. Available from: www.som.soton.ac.uk/cia/. |
[39] | Metz C . Basic principles of ROC analysis. Semin Nucl Med. (1978) ;8: (4):283–298. |
[40] | Huebler H . International education statistics. 2014 [cited 2014 Nov 25]. Available from: http://blogspot.ie/2008/03/global-population-of-primary-school-age.html. |
[41] | Watson KD , Papageorgiou AC , Jones GT , Taylor S , Symmons DP , Silman AJ , Macfarlane GJ . Low back pain in schoolchildren: The role of mechanical and psychosocial factors. Arch Dis Child. (2003) ;88: (1):12–17. |
[42] | Shultz SP , Anner J , Hills AP . Paediatric obesity, physical activity and the musculoskeletal system. Obes Rev. (2009) ;10: (5):576–582. |
[43] | Parikh R , Mathai A , Parikh S , Sekhar G , Thomas R . Understanding and using sensitivity, specificity and predictive values. Indian J Opthalmol. (2008) ;56: (1):45–50. |
[44] | Jones GT , Watson KD , Silman AJ , Symmons DPM , Macfarlane GJ . Predictors of low back pain in British schoolchildren: A population-based prospective cohort study. Pediatrics. (2003) ;111: (4):822–828. |
[45] | Mackie HW , Legg SJ , Beadle J . Development of activity monitoring for determining load carriage patterns in school students. WORK. (2004) ;22: (3):231–237. |
[46] | Mackie HW , Legg SJ . Measurement of the temporal patterns of school bag carriage using activity monitoring and structured interview. Ergonomics. (2007) ;50: (10):1668–1679. |
[47] | Johnson C . Manual handling risk management. In: Smith J, editor. The guide to the handling of people: A systems approach. Middlesex: Backcare; (2011) . |
[48] | Health and Safety Authority. Dublin: 2014 [cited 2014 Dec 12]. Available from: http://www.hsa.ie/eng/Topics/Hazards. |
[49] | Safety Health and Welfare at Work Regulations. Schedule 3. Dublin: Government publications; (2007) . |
[50] | Goodgold SA , Nielsen D . Effectiveness of a school-based backpack health promotion program: Backpack Intelligence. WORK. (2003) ;21: (2):113–123. |
[51] | Mendez FJ , Gomez-Conesa A . Postural hygiene program to prevent low back pain. Spine. (2001) ;26: (11):1280–1286. |
[52] | Cardon GM , De Clercq DL , De Bourdeaudhuij IM . Back education efficacy in elementary schoolchildren: A 1-year follow-up study. Spine (Phila Pa 1976). (2002) ;27: (3):299–305. |
[53] | Sheldon MR . Lifting instruction to children in an elementary school. J Orthop Sports Phys Ther. (1994) ;19: (2):105–110. |
[54] | Feingold AJ , Jacobs K . The effect of education on backpack wearing and posture in a middle school population. WORK. (2002) ;18: (3):287–294. |
[55] | Trevelyn FC , Legg SJ . Risk factors associated with back pain in New Zealand school children. Ergonomics. (2011) ;54: (3):257–262. |
Figures and Tables
Fig.1
Comparison of ROC curves with different degrees of accuracy.
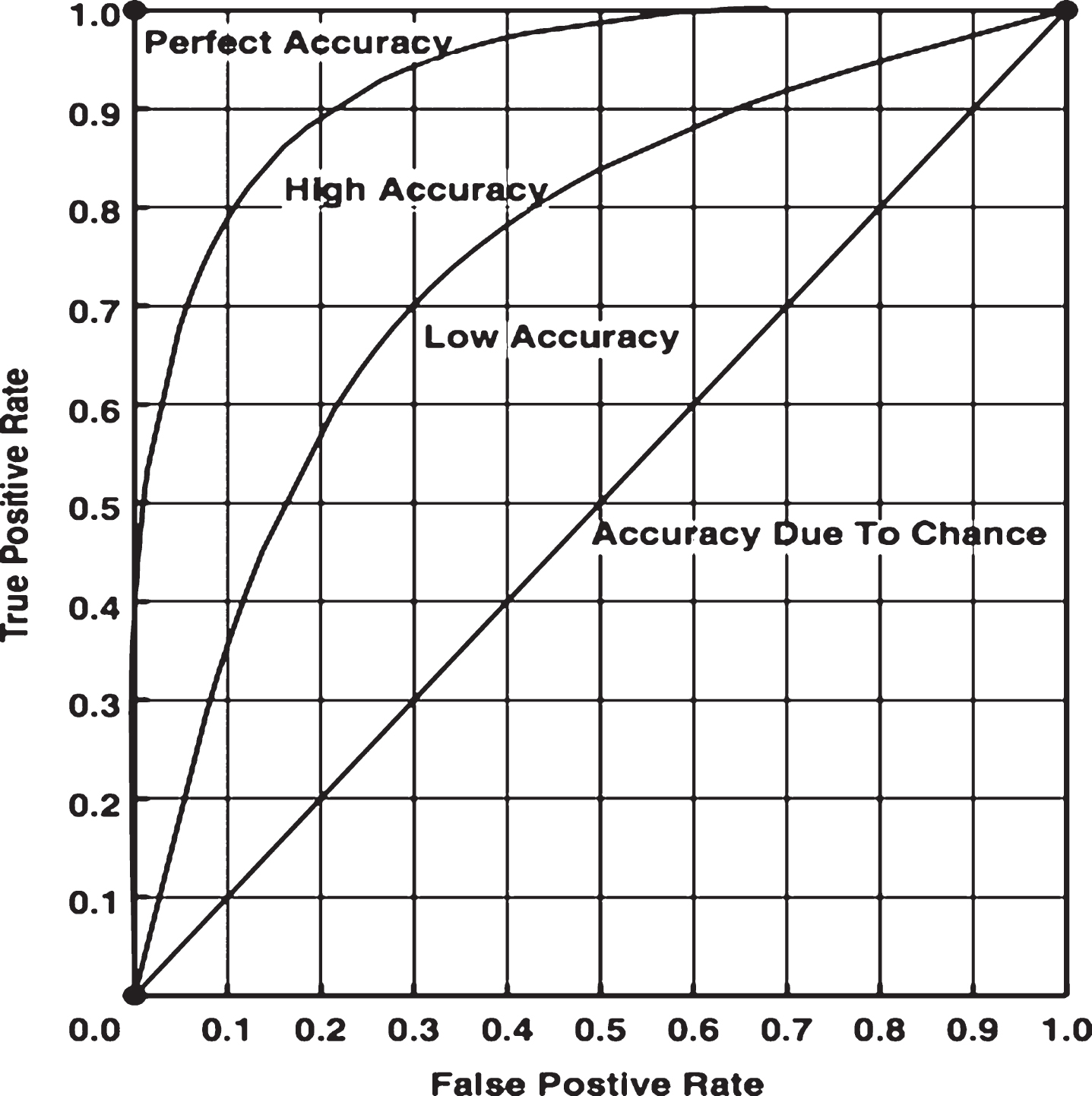
Fig.2
ROC Curve analysis of the discrimination of mechanical burden variables for schoolbag-related back discomfort.
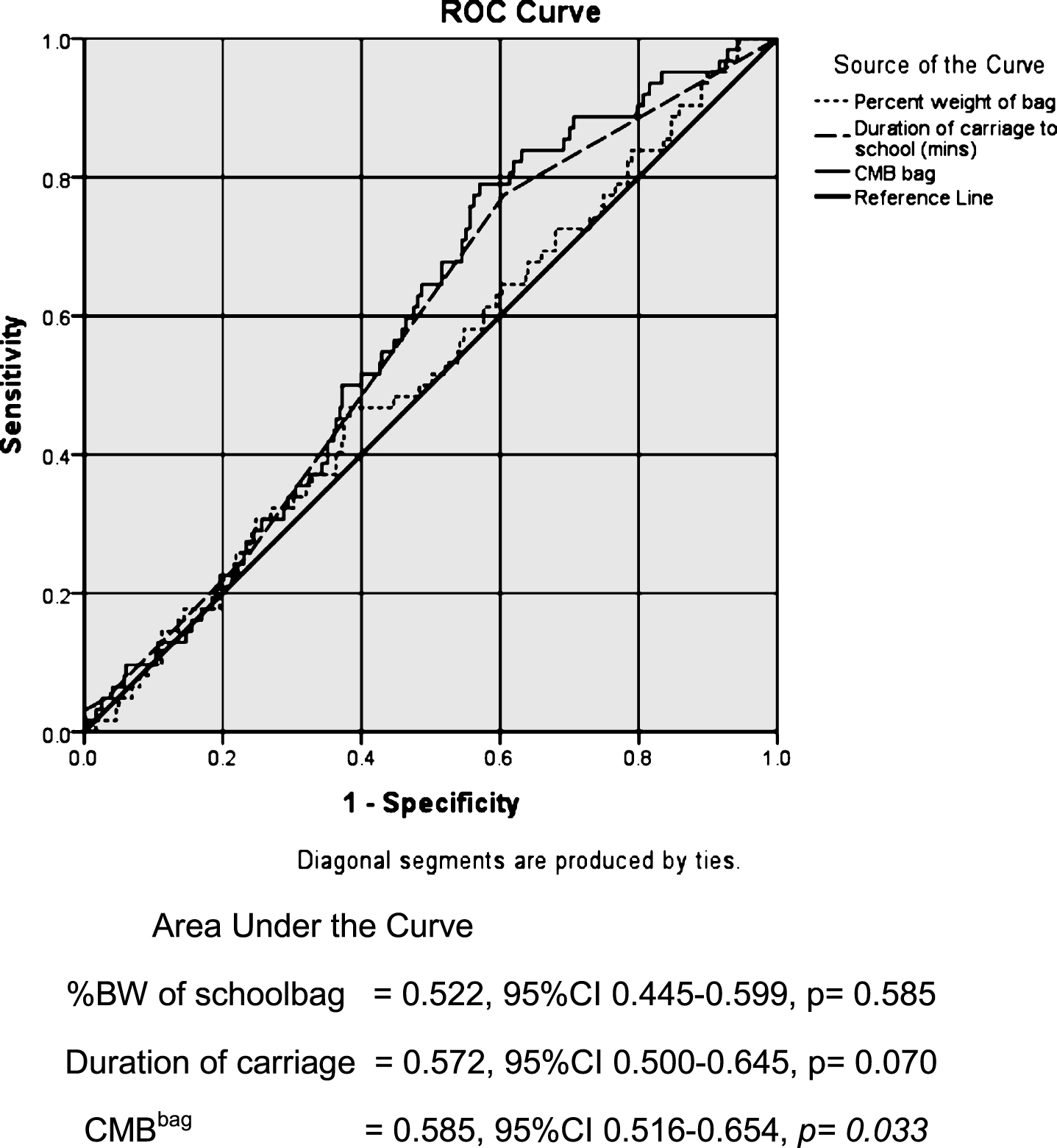
Fig.3
ROC Curve analysis of the discrimination of mechanical burden variables for schoolbag-related shoulder discomfort.
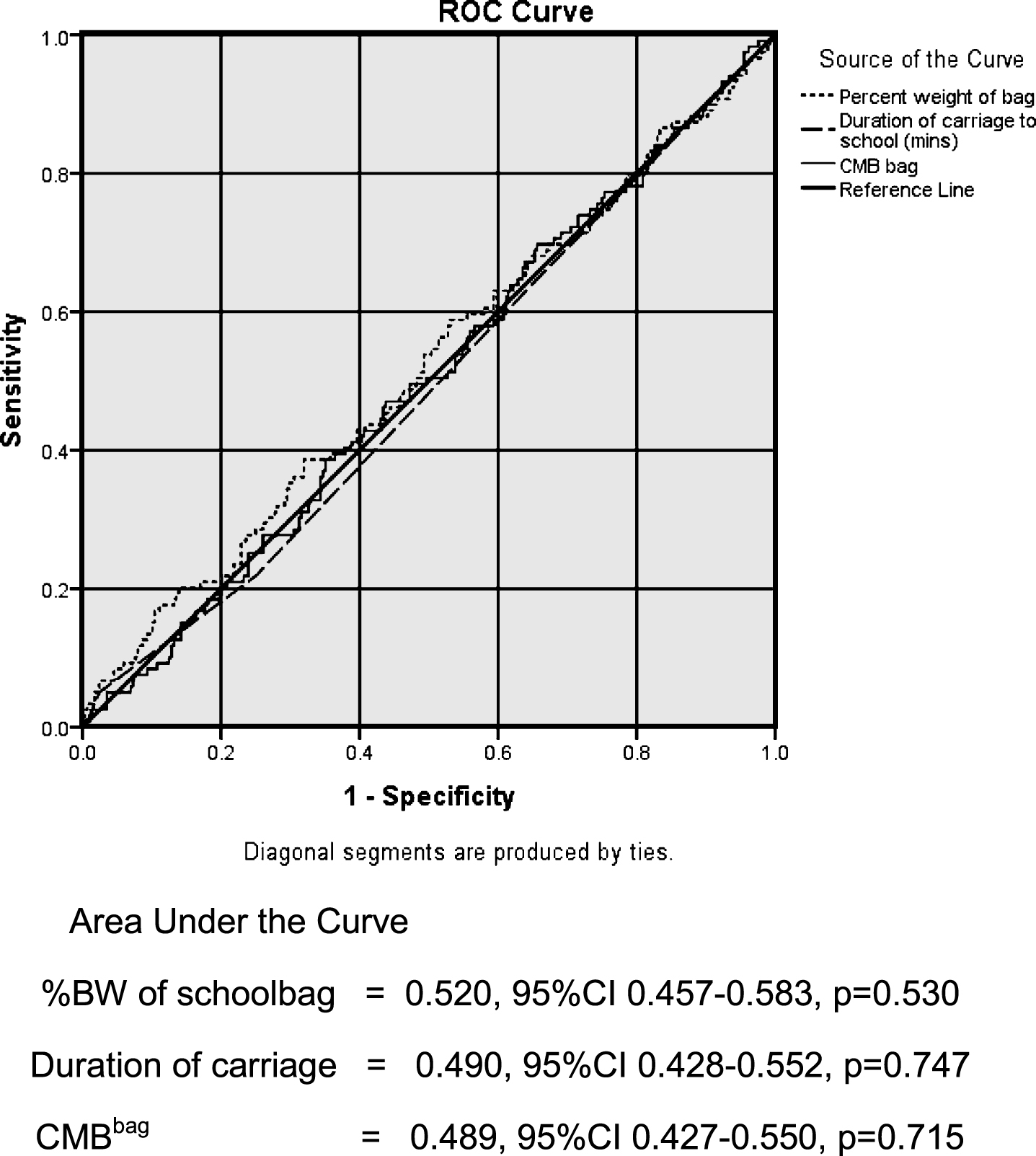
Table 1
Frequency of back discomfort at different schoolbag weight levels and duration of carriage
| n = 409 | Schoolbag-related back discomfort | |||||
| Yes n (%) | No n (%) | Chi-square | Risk Ratio | Sensitivity | Specificity | |
| (95% CI) | (95% CI) | (95% CI) | ||||
| Schoolbag weight | ||||||
| ≤10% BW | 17(14.0) | 104(86.0) | ||||
| 121(29.6) | 0.164, df1, p = 0.685 | 1.11 (0.664–1.863) | 0.72 (0.676–0.763) | 0.29 (0.246–0.334) | ||
| >10% BW | 45(15.6) | 243(84.4) | ||||
| 288(70.4) | ||||||
| ≤15% BW | 46(14.8) | 265(85.2) | ||||
| 311(76.0) | 0.137, df1, p = 0.712 | 1.11 (0.658–1.859) | 0.26 (0.217–0.302) | 0.76 (0.719–0.801) | ||
| >15% BW | 16(16.3) | 82(83.7) | ||||
| 98(24.0) | ||||||
| ≤20% BW | 60(15.4) | 330(84.6) | 0.332, df1, p = 0.564 | 0.68 (0.181–2.591) | 0.03 (0.013–0.046) | 0.95 (0.928–0.971) |
| 390(95.3) | ||||||
| >20% BW | 2(10.5) | 17(89.5) | ||||
| 19(4.7) | ||||||
| Duration of carriage | ||||||
| <5 mins | 14(9.3) | 136(90.7) | 6.251, df1, p = 0.012 | 2.0 (1.134–3.477) | 0.77 (0.729–0.811) | 0.39 (0.343–0.437) |
| 150(36.7) | ||||||
| ≥5 mins | 48(18.5) | 211(81.5) | ||||
| 259(63.3) | ||||||
| ≤10 mins | 46(14.9) | 263(85.1) | ||||
| 309(75.6) | 0.073, df1, p = 0.787 | 1.07 (0.638–1.812) | 0.25 (0.208–0.292) | 0.76 (0.719–0.801) | ||
| >10 mins | 16(16.0) | 84(84.0) | ||||
| 100(24.4) | ||||||
| ≤20 mins | 59(14.9) | 336(85.1) | ||||
| 395(96.6) | 0.443, df1, p = 0.455* | 1.43 (0.512–4.019) | 0.05 (0.029–0.071) | 0.96 (0.941–0.979) | ||
| >20 mins | ||||||
| 14(3.4) | 3(21.4) | 11(78.6) | ||||
*Fishers Exact Test.
Table 2
Frequency of shoulder discomfort at different schoolbag weight levels and duration of carriage
| n = 407 | Schoolbag-related shoulder discomfort | |||||
| Yes n (%) | No n (%) | Chi-square | Risk Ratio | Sensitivity | Specificity | |
| (95% CI) | (95% CI) | (95% CI) | ||||
| Schoolbag weight | ||||||
| ≤10% BW | 35(29.2) | 85(70.8) | ||||
| 120(29.5) | 0.000, df1, p = 0.984 | 1.0 (0.715–1.389) | 0.70 (0.655–0.744) | 0.29 (0.246–0.334) | ||
| >10% BW | 84(29.3) | 203(70.7) | ||||
| 287(70.5) | ||||||
| ≤15% BW | ||||||
| 310(76.2) | 89(28.7) | 221(71.3) | 0.176, df1, p = 0.675 | 1.07 (0.763–1.522) | 0.25 (0.208–0.292) | 0.77 (0.729–0.811) |
| >15% BW | 30(30.9) | 67(69.1) | ||||
| 97(23.8) | ||||||
| ≤20% BW | 111(28.6) | 277(71.4) | ||||
| 388(95.3) | 1.595, df1, p = 0.207 | 1.47 (0.849–2.552) | 0.07 (0.045–0.095) | 0.96 (0.941–0.979) | ||
| >20% BW | 8(42.1) | 11(57.9) | ||||
| 19(4.7) | ||||||
| Duration of carriage | ||||||
| <5 mins | 44(29.3) | 106(70.7) | ||||
| 150(36.9) | 0.001, df1, p = 0.974 | 1.0 (0.728–1.361) | 0.63 (0.583–0.677) | 0.37 (0.323–0.417) | ||
| ≥5 mins | 75(29.2) | 182(70.8) | ||||
| 257(63.1) | ||||||
| ≤10 mins | 92(29.9) | 216(70.1) | ||||
| 308(75.7) | 0.244, df1, p = 0.621 | 0.91 (0.634–1.314) | 0.23 (0.189–0.271) | 0.75 (0.708–0.792) | ||
| >10 mins | 27(27.3) | 72(72.7) | ||||
| 99(24.3) | ||||||
| ≤20 mins | 113(28.7) | 281(71.3) | ||||
| 394(96.8) | 1.857, df1, p = 0.214* | 1.61 (0.876–2.954) | 0.05 (0.029–0.071) | 0.97 (0.953–0.986) | ||
| >20 mins | 6(46.2) | 7(53.8) | ||||
| 13(3.2) | ||||||
*Fishers Exact Test.

