
Evaluation of a large adrenal carcinoma with 3D reconstruction of computed tomography images: A case report and literature review
Abstract
Adrenocortical carcinoma (ACC) is an extremely rare disease caused by a cancerous growth in the adrenal cortex. Although most of adrenal tumors are benign, the functional ACC is malignant resulting in endocrine dysfunction and necessitates surgical removal. Retroperitoneal laparoscope adrenalectomy is often used to perform adrenal gland surgery. Here, we reported a case of huge ACC with the size of 6.8 cm × 5.2 cm. To achieve better surgical outcome, we integrated 3D reconstructed CT images into a dynamic video for preoperative planning and intraoperative guiding to resect the diseased adrenal gland completely without neighbor organ’s injury and surgery complications. Moreover, we reviewed associated applications using 3D reconstructed CT imaging in surgery field. Finally, the evaluation and effect of such technology were discussed to reveal that the 3D dynamic video can help surgeon to make better preoperative assessment so as to give patients better therapy.
1Introduction
With the development of imaging techniques such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI), the detection rates of adrenal masses has remarkably increased [1, 2]. Most adrenal masses are benign tumors, dividing into three types: adrenocortical adenomas or carcinoma within the adrenal cortex, neuroblastoma and pheochromocytomas within the adrenal medulla [3]. In malignant tumors of adrenal glands, adrenocortical carcinoma (ACC) is an exceedingly rare disease caused by a cancerous growth within the cortex. ACC has the estimated incidence of 0.7 cases per million per year in the United States and lead to 0.2% of all cancer deaths [4, 5]. ACC may occur in adults or children with a female to male ratio of 1.5 – 2.5:1 [5, 6]. Many ACCs are asympomatic and nonfunctional as adrenal incidentalomas. However, some ACCs may be “functional”, producing excessive adrenal hormones. This type of malignancy results in endocrine dysfunction by large amounts of cortisol, testosterone, and aldosterone. Because of their deep location in the retroperitoneum, most ACCs are not diagnosed until they grow to a large size. Frequently, ACCs can invade adjacent large vessels, the renal vein as well as the inferior vena cava. If an ACC is found to be functional, the tumor necessitates surgical removal, although chemotherapy, radiation therapy, and hormonal therapy may also be employed to treat ACC depending on various stage of carcinoma [1].
For surgical resection of adrenal benign mass, laparoscopic adrenalectomy is a common surgery regarded as a gold standard [7]. Compared with laparoscopic via abdominal approach, retroperitoneal laparoscope adrenalectomy is extensively operated for less invasiveness and easy postoperative care [8]. However, due to complicated anatomy and the limited space around adrenal glands, laparoscope adrenalectomy from retroperitoneal approach is a challenge for large tumors (>6 cm in diameter) because the tumors might affect the adjacent important organs or tissues such as kidney, liver or spleen, and inferior vena cava [9]. Thus, to achieve better outcome via retroperitoneal laparoscopy in the treatment of a large and deep-located adrenal tumor, it is required more detail information based on the x-ray images to precisely evaluate the size, location, adhesion with the adjacent tissue, blood supply and metastasis of ACC in anatomic before surgery.
In clinic routines, images in 2D patterns are often used to represent 3D tumor tissue in the body, which limits in illustration of the reality of tumor. Recent advances in medical imaging and radiological technology have meaningfully contributed to surgical development in diagnose, prognosis and treatment of disease [10–12]. Three-dimensional (3D) reconstruction image based of CT and MRI has provided more accurate and insight illustration for better evaluation in surgical planning [13]. The 3D reconstructed images provide more detail information about anatomic relationship and morphological features of diseased tissues or tumors [14–16].
In this study, we developed a technology to generate a video originated from 3D reconstructed CT images. The processed videos demonstrated dynamic, stereo and all-round information, which offered an easier and more accurate pattern to develop a surgery strategy, particularly for performing endoscopic or laparoscopic surgery. With the aid of this 3D video, we successfully removed a large (about 7-cm in diameter) ACC tumor by a laparoscopic resection via retroperitonealapproach.
2Case report
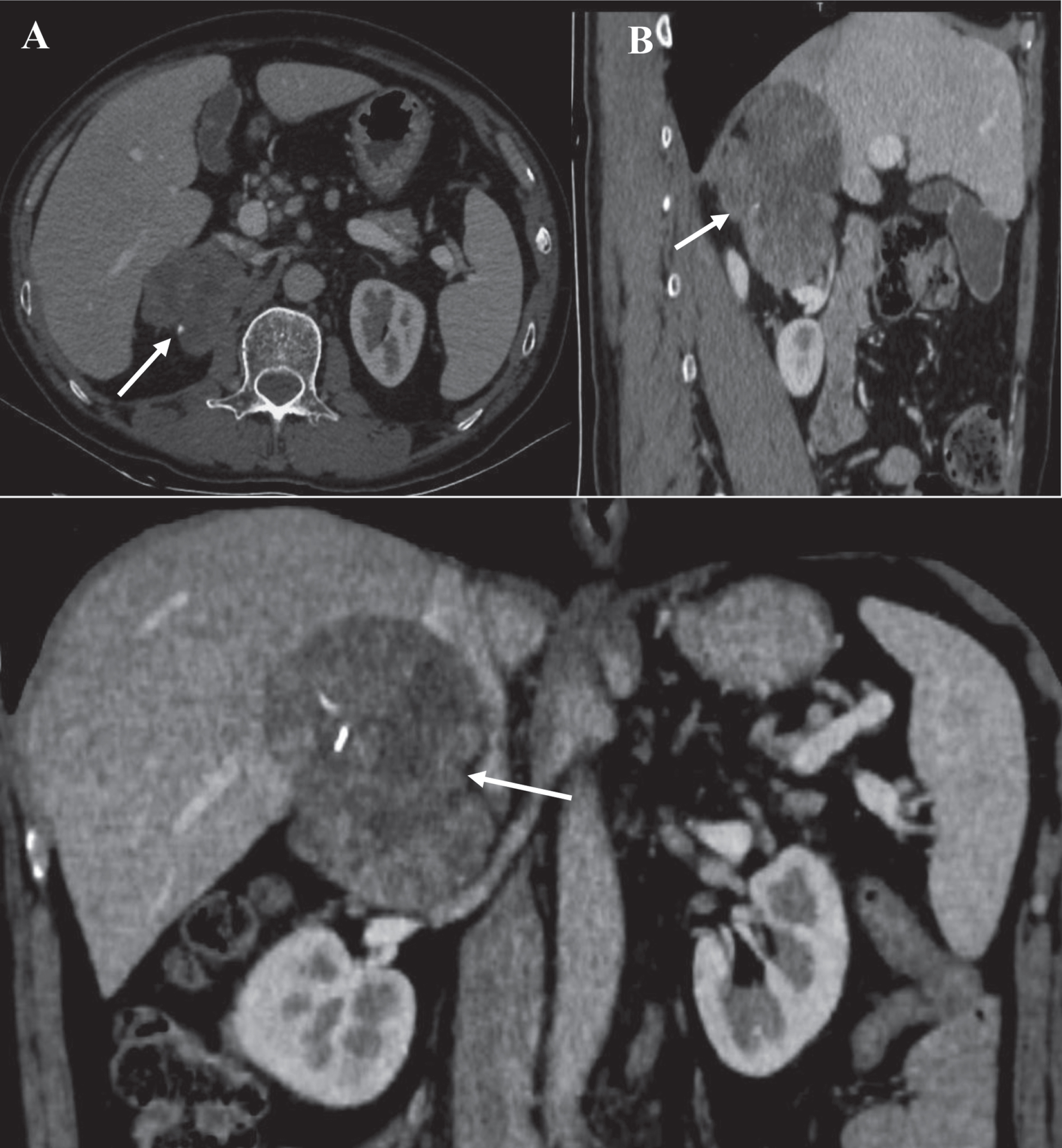
A 55-year-old male patient presented with decline in physical activity and frequent fatigue. On physical examination, his blood pressure was 169/106 mmHg. Laboratory investigations including catecholamines, aldosterone, cortisol, and potassium concentrations in blood or urine revealed 17-hydroxy corticosteroid significantly increased (82.54 μmol/24 h, normal arranging from 8.3 to 27.7 μmol/24 h). Abdominal ultrasound and CT scan indicated a large mass in the right adrenal area. Enhanced CT scan further determined the location (right adrenal), property (neoplastic lesion) and size (6.8 cm ×5.2 cm) of tumor. The CT images were reconstructed into 3D images as a regular pattern (Fig. 1). Further, we integrated all CT data into a 3D adrenal tumor model separated from kidneys, liver, spleen, spine ribs, inferior caval vein and artery by 16.0 Mimics software. The video clearly showed that the isolated tumor was originated from right adrenal gland, which separated from other organs (Fig. 2). After evaluating the surgery risk based on the anatomic relationship among adjacent organs, we made operation planning for retroperitoneal laparoscopic adrenalectomy according to the video. The huge adrenal gland was completely resected with no-injury to liver, right kidney, and other neighboring vessels and tissues (Fig. 3). The operative duration lasted 87-minute and the estimated blood loss was less than 150 ml. No intraoperative and postoperative complications occurred. The pathologic diagnosis was adrenal cortical carcinoma (Fig. 4). Six-month follow-up showed no significant complication associated with surgery.
3Discussion
To meet the requirement of high quality, safety, and time efficiency, modern CT technique provides a noninvasive approach to obtain a complete cross-sectional X-ray image of entire organs in human body. As laparoscopic surgeries are widely used, it is critical to obtain clear and detail image information about the size, number, location of the tumor lesion and the adhesion status between the tumor and the adjacent organs, vascular distribution and metastasis before surgery. Typically for adrenal surgery, the retroperitoneal space is limited for laparoscopic surgeries [13, 17, 18]. It is a challenge to resect large retroperitoneal neoplasms via retroperitoneal approach [17, 18] because it’s more likely to affect and damage adjacent organs and tissues. In this case, we successfully removed a large adrenal cancer tumor with the aid of dynamic 3D video.
ACC is an extreme rare carcinoma originated from adrenal gland cortex. It is difficult to identify whether the adrenal tumor is benign or malignant before pathological examination. Therefore, the best choice is to resect entire tumor to prevent recurrence and spread of cancer cells. With the aid of 3D reconstruction technology [13], tumor tissue could be precisely evaluated to help make appropriate surgery plan [10]. More applications of 3D reconstruction of CT data have been reported (Table 1) [19–24]. The 3D dynamic videos of target organs can be not only acted as an optimal diagnostic approach for surgery but also be as a better learning tool for residents or medicalstudents.
4Conclusions
The majority of adrenal gland neoplasm is benign, even the malignant neoplasm does not cause serious damage to the adjacent tissue or organs. Thus, the least invasive operation would be best choice for ACC tumor, which helps the wound recover sooner than open surgery. In aid of 3D dynamic video from reconstruction of CT data, laparoscope adrenalectomy is feasible via retroperitoneal approach to resect a large entire adrenal carcinoma.
References
[1] | Pantalone KM, Gopan T, Remer EM, Faiman C, Ioachimescu AG, Levin HS, Siperstein A, Berber E, Shepardson LB, Bravo EL and Hamrahian AH, Change in adrenal mass size as a predictor of a malignant tumor, Endocr Pract 16: (4) ((2010) ), 577–587. |
[2] | Lu XB, Wu RP, Huang X and Zhang Y, Noncontrast multidetector-row computed tomography scanning fordetection of radiolucent calculi in acute renal insufficiency caused by bilateral ceftriaxone crystals ureteral obstruction, J X-Ray Sci and Tech 20: (1) ((2012) ), 11–16. |
[3] | Young WF Jr, Clinical practice. The incidentally discovered adrenal mass, N Engl J Med 356: (6) ((2007) ), 601–610. |
[4] | Golden SH, Robinson KA, Saldanha I, Anton B and Ladenson PW, Clinical review: Prevalence and incidence of endocrine and metabolic disorders in the United States: A comprehensive review, J Clin Endocrinol Metab 94: (6) ((2009) ), 1853–1878. |
[5] | Costa R, Carneiro BA, Tavora F, Pai SG, Kaplan JB, Chae YK, Chandra S, Kopp PA and Giles FJ, The challenge of developmental therapeutics for adrenocortical carcinoma, Oncotarget 7: (29) ((2016) ), 46734–46749. |
[6] | Michalkiewicz E, Sandrini R, Figueiredo B, Miranda EC, Caran E, Oliveira-Filho AG, Marques R, Pianovski MA, Lacerda L, Cristofani LM, Jenkins J, Rodriguez-Galindo C and Ribeiro RC, Clinical and outcome characteristics of children with adrenocortical tumors: A report from the International Pediatric Adrenocortical Tumor Registry, J Clin Oncol 22: (5) ((2004) ), 838–845. |
[7] | Carr AA and Wang TS, Minimally Invasive Adrenalectomy, Surg Oncol Clin N Am 25: (1) ((2016) ), 139–152. |
[8] | Zhang X, Lang B, Ouyang JZ, Fu B, Zhang J, Xu K, Wang BJ and Ma X, Retroperitoneoscopic adrenalectomy without previous control of adrenal vein is feasible and safe for pheochromocytoma, Urology 69: (5) ((2007) ), 849–853. |
[9] | Souzaki R, Kinoshita Y, Ieiri S, Kawakubo N, Obata S, Jimbo T, Koga Y, Hashizume M and Taguchi T, Preoperative surgical simulation of laparoscopic adrenalectomy for neuroblastoma using a three-dimensional printed model based on preoperative CT images, J Pediatr Surg 50: (12) ((2015) ), 2112–2115. |
[10] | Bolliger SA, Thali MJ, Ross S, Buck U, Naether S and Vock P, Virtual autopsy using imaging: Bridging radiologic and forensic sciences. A review of the Virtopsy and similar projects, Eur Radiol 18: (2) ((2008) ), 273–282. |
[11] | Sakamoto T, Roles of universal three-dimensional image analysis devices that assist surgical operations, J Hepatobiliary Pancreat Sci 21: (4) ((2014) ), 230–234. |
[12] | Zhang Y, Tong Z and Zhang Y, X-ray Computed Tomography and Sonography Features of Continuous Splenogonadal Fusion, J X-Ray Sci and Tech 21: (2) ((2013) ), 303–308. |
[13] | Mitterberger M, Pinggera GM, Peschel R, Bartsch G, Pallwein L and Frauscher F, The use of three-dimensional computed tomography for assessing patients before laparoscopicadrenal-sparing surgery, BJU Int 98: (5) ((2006) ), 1068–1073. |
[14] | Kim JW, Shin SS, Heo SH, Lim HS, Lim NY, Park YK, Jeong YY and Kang HK, The role of three-dimensional multidetector CT gastrography in the preoperative imaging of stomach cancer: Emphasis on detection and localization of the tumor, Korean J Radiol 16: (1) ((2015) ), 80–89. |
[15] | Yang C, Zhang Y, Zhang Y, Fan Y and Deng F, Three-dimensional quantification of orthodontic root resorption with time-lapsed imaging of micro-computed tomography in a rodent model, J X-ray Sci Technol 23: (5) ((2015) ), 617–626. |
[16] | Metzler P, Geiger EJ, Alcon A, Ma X and Steinbacher DM, Three-dimensional virtual surgery accuracy for free fibula mandibular reconstruction: Planned versus actual results, J Oral Maxillofac Surg 72: (12) ((2014) ), 2601–2612. |
[17] | Conzo G, Tartaglia E, Gambardella C, Esposito D, Sciascia V, Mauriello C, Nunziata A, Siciliano G, Izzo G, Cavallo F, Thomas G, Musella M and Santini L, Minimally invasive approach for adrenal lesions: Systematic review of laparoscopic versusretroperitoneoscopic adrenalectomy and assessment of risk factors for complications, Int J Surg 18: (S1) ((2016) ), S118–S123. |
[18] | Zhang X, Lang B, Ouyang JZ, Fu B, Zhang J, Xu K, Wang BJ and Ma X, Retroperitoneoscopic adrenalectomy without previous control of adrenal vein is feasible and safe for pheochromocytoma, Urology 69: (5) ((2007) ), 849–853. |
[19] | You B, Cheng Y, Zhang J, Song Q, Dai C, Heng X and Fei C, Application of contrast-enhanced T1-weighted MRI-based 3D reconstruction of the dural tail sign in meningioma resection, J Neurosurg 125: (1) ((2016) ), 46–52. |
[20] | He YB, Bai L, Aji T, Jiang Y, Zhao JM, Zhang JH, Shao YM, Liu WY and Wen H, Application of 3D reconstruction for surgical treatment of hepatic alveolar echinococcosis, World J Gastroenterol 21: (35) ((2015) ), 10200–10207. |
[21] | Wang WH, Deng JY, Li M, Zhu J and Xu B, Preoperative three-dimensional reconstruction in vascularized fibular flap transfer, J Craniomaxillofac Surg 40: (7) ((2012) ), 599–603. |
[22] | Zeng N, Tao H, Fang C, Fan Y, Xiang N, Yang J, Zhu W, Liu J, Guan T, Fang C and Xiang F, Individualized preoperative planning using three-dimensional modeling for Bismuth and Corlette type III hilar cholangiocarcinoma, World J Surg Oncol 14: (1) ((2016) ), 44–. |
[23] | Su L, Dong Q, Zhang H, Zhou X, Chen Y, Hao X and Li X, Clinical application of a three-dimensional imaging technique in infants and young children with complex liver tumors, Pediatr Surg Int 32: (4) ((2016) ), 387–395. |
[24] | Wen J, Hou X, Chu X, Xue X and Xue Z, Application of three dimensional reconstruction technique in selection of incision of thoracicsurgical operation with robot, Int J Clin Exp Med 8: (10) ((2015) ), 17818–17823. eCollection 2015. |
Figures and Tables
Fig.1
A larger tumor in right adrenal gland. Enhanced CT images submitted to doctor in regular pattern. (A) axial plane; (B) sagittal plane; (C) coronal plane. Arrow: ACC.
A dynamic video based on 3D reconstruction of CT images. (1) a large mass in the right adrenal gland (yellow); (2) right kidney (brown); (3) inferior caval vein (dark orange).
Fig.3
Gross view of completely-resected adrenal carcinoma. The tumor was entirely covered by the capsular and minimal tissue adhesion and the tumor size was 6.8 cm ×5.2 cm.
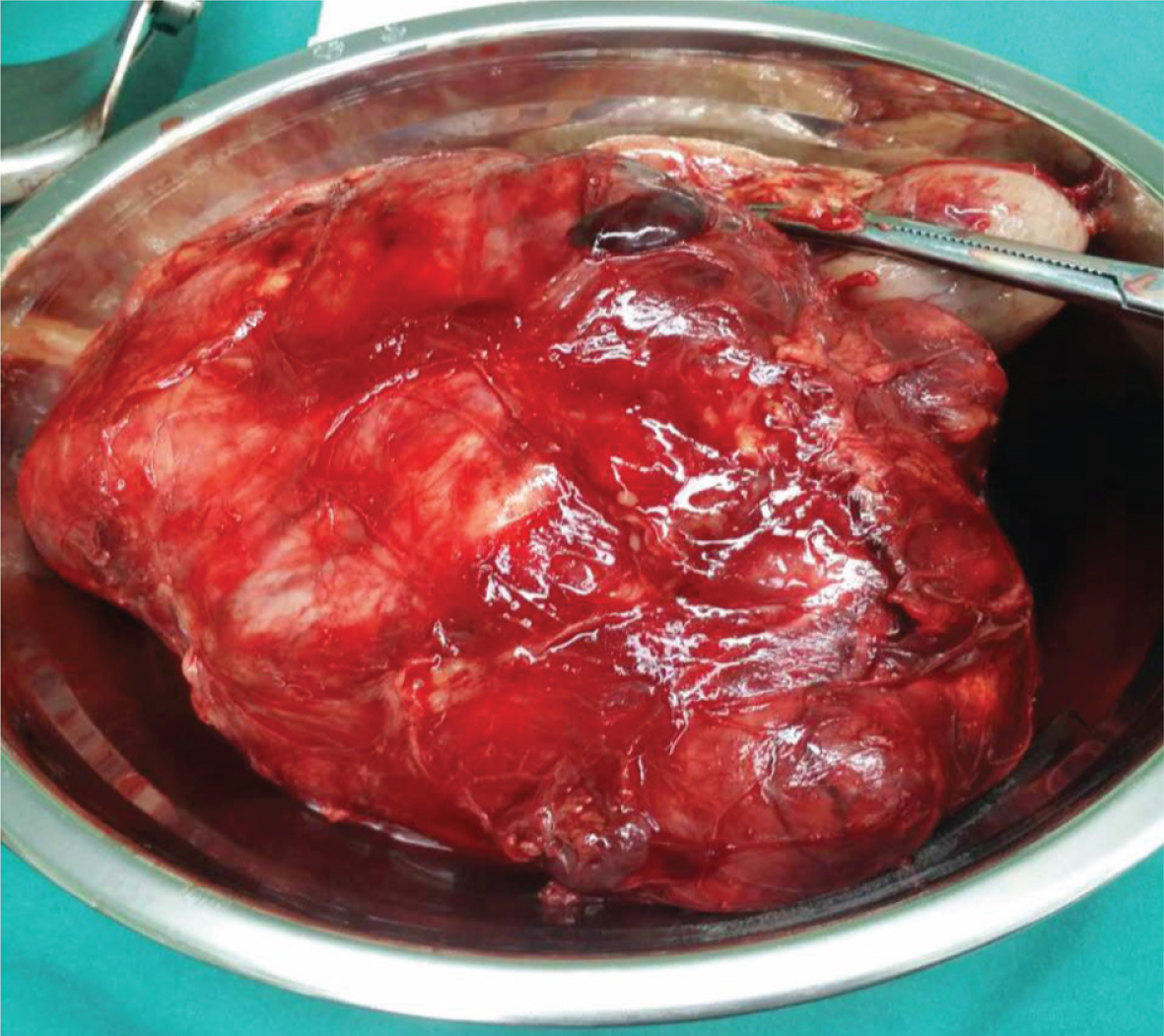
Fig.4
The pathological result of the large adrenal gland tumor. The carcinoma is mainly constituted by eosinophils in adrenal cortex. The carcinoma cells are separated by wide fibrous band, accompanied by calcification and necrosis. (H.E. staining) ×40.
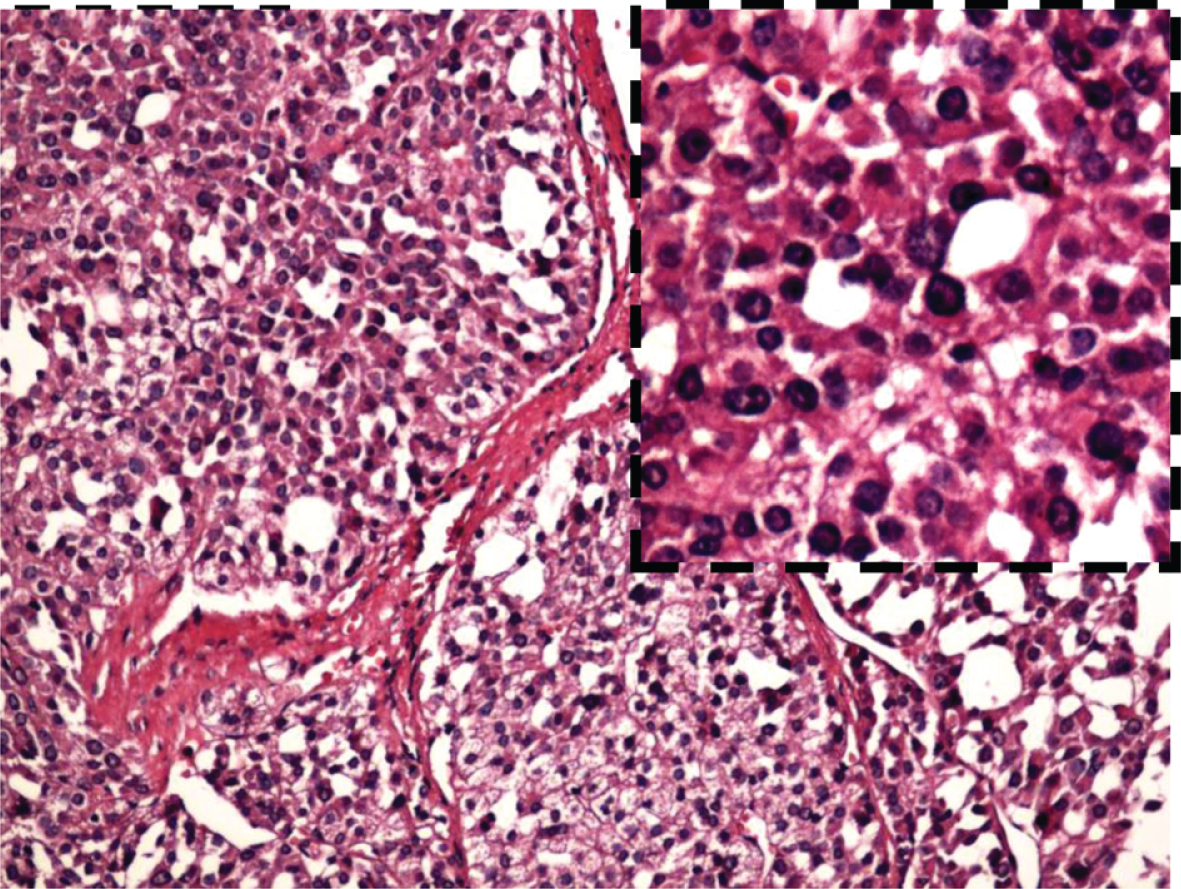
Table 1
Reported application of 3D reconstruction imaging technology in surgery
| Disease | Treatment | Objects of comparison | Studies performed | Important findings | Ref. |
| Meningioma | Meningioma resection | T1W MR images v.s. 3D reconstruction images | The vertical and anteroposterior diameters of dural tail sign on the contrast-enhanced T1W MR images and 3D reconstruction images were compared for surgical design | 3D reconstruction can intuitively and accurately reveal the size and shape of dural tail sign in meningioma resection | 19 |
| Hepatic alveolar echinococcosis | Hepatectomy | 3D reconstruction v.s. conventional imaging methods | Outcomes of hepatectomy were compared between the two groups of preoperative assessments, 3D reconstruction plus “virtual” 3D liver resection and conventional imaging methods | 3D reconstruction provides comprehensive and precise anatomical information for the liver with improving the chance of success and reducing the risk | 20 |
| Maxillomandibular tumours | Block resection with vascularized fibular flap transfer | - | The original data of preoperative CTA were retrospectively analysed and applied to the reconstruction of the lower limb | Preoperative 3D reconstruction plays an important role in vascularized fibular flap transfer for lower limb vascular assessment | 21 |
| Type III hilar cholangiocarcinoma | Preoperative surgery simulation | patients undergoing preoperative planning v.s. those who did not | Preoperative simulation and subsequent surgery were performed based on 3D reconstructed CT images. The clinical, surgical and pathological characteristics were compared | 3D assessment improved operative planning for the treatment of hilar cholangiocarcinoma. | 22 |
| Complex liver tumors in infants and young children | Hepatectomy | Three-dimensional (3D) imaging v.s. two-dimensional (2D) computed tomography | The clinical outcomes were analyzed and compared between the two groups (2D and 3D reconstruction) | 3D visualization technology can improve surgical controllability, accuracy, and safety for precise hepatectomy in infants and young children undergoing complex liver tumors | 23 |
| Thoracic mass | Thoracic surgical operation | - | The chest CT images were three-dimensional reconstructed to predetermine the location of incision prior to surgery. The operation time, set up time and work time were evaluated | 3D reconstruction can show the location of tumor, help in planning of appropriate incisions and define anatomical relationships | 24 |


