
The Impact of Pregnancy on Myotonic Dystrophy: A Registry-Based Study
Abstract
Background:
The rate of symptom progression during pregnancy in myotonic dystrophy (DM) is not currently known. Further, there is little data regarding the rate of pregnancy complications and neonatal outcomes in DM.
Objective:
This study assesses symptom progression and complication rates during pregnancy in women with DM.
Methods:
DM women completed surveys regarding their prior pregnancies. Participants identified complications during their pregnancies and completed the Myotonic Dystrophy Health Index-Short Form (MDHI-SF) to measure their disease burden and identify the severity of select symptoms six-months prior to, during, and six-months after their first pregnancy.
Results:
152 women with DM reported on 375 pregnancies. Among these pregnancies, there was a 32.5% miscarriage rate. Some complications were common including: pre-term labor (27.8%), pre-eclampsia (10.4%), and peripartum hemorrhage (13.9%). Participants’ perception of their mobility and ability to perform activities, as measured by the MDHI-SF, worsened during pregnancy and did not recover during the post-partum period.
Discussion:
Miscarriage, maternal disease progression during pregnancy, and other pregnancy related complications may occur in DM. Women with DM should be counseled on these potential risks prior to considering pregnancy.
Abbreviations
DM1 | Myotonic dystrophy type 1 |
DM2 | Myotonic dystrophy type 2 MDF Registry |
MDHI | Myotonic Dystrophy Health Index NIH Registry |
SF | Short Form |
INTRODUCTION
The myotonic dystrophies are autosomal dominant, multisystemic disorders due to either a CTG repeat in the DMPK gene (myotonic dystrophy type-1; DM1) [1–3] or a CCTG repeat in the CNBP (ZNF9) gene (myotonic dystrophy type-2; DM2) [4–6]. Both DM1 and DM2 cause muscle weakness, delayed muscle relaxation (myotonia), and early onset cataracts [7, 8]. In addition, both disorders may affect the heart, cognition, and other body systems [9]. Genetic anticipation can lead to expansion in the CTG repeat in DM1. In DM1, genetic anticipation can lead to children with earlier, and more life-altering symptoms than their affected mother. In these cases, mothers with classical or mild DM1 may have children who present with severe symptoms developing in infancy or childhood, known as congenital DM1 or childhood DM1 [8]. In DM2, clinical symptoms associated with the disease do not typically occur until early adulthood or later.
Neuromuscular disease can complicate pregnancy. Maternal weakness, concern over passing a disease to a child, peripartum anesthesia risks, and neonatal complications are common concerns [10]. DM patients are at increased risk of reproductive complications. In prior obstetrical surveys, patients with DM1 had a higher rate of spontaneous abortions, polyhydramnios, ectopic pregnancies, placenta previa, and preterm labor [11]. Pregnant DM2 patients have a higher rate of urinary tract infections and preterm labor [11, 12]. Anecdotally, DM patients often report that their symptoms worsen or begin during pregnancy. In a series of 42 patients with DM2, 21% of women reported developing their initial symptoms during pregnancy [12].
This study builds on prior research by utilizing a large cohort of women with DM to identify the outcomes, complications, and changes in symptoms associated with pregnancy. In addition, this study utilizes the Myotonic Dystrophy Health Index-Short Form (MDHI-SF) to retrospectively estimate the impact pregnancy has on disease burden in DM [9]. Approval for this study was obtained through the local institutional review board and an ethical approval process through both registries.
METHODS
Participants and recruitment
Women with DM between the ages of 18 and 63 were recruited for this study from one of two patient registries: The Myotonic Dystrophy Patient and Family Registry (Myotonic Dystrophy Family Registry; www.myotonicregistry.patientcrossroads.org) and The National Registry of Myotonic Dystrophy and Facioscapulohumeral Muscular Dystrophy Patients and Family Members (National Registry; www.urmc.rochester.edu/neurology/national-registry). Woman under the age of 63 were selected for this study in order to limit participants with a more extensive time period since their last pregnancy. Each qualifying woman from these registries was sent a paper survey to be potentially completed and sent back to the researchers for analysis. In instances were participants were members of both registries; they were instructed to complete the survey only once.
Survey content
Each survey included questions regarding DM type, DNA testing results, age, complications of pregnancy, use of assistive reproductive technology, and pregnancy outcomes associated with each of their pregnancies. To assess for possible congenital myotonic dystrophy, participants were asked if their child had breathing problems, needed a ventilator, needed a feeding tube, had feeding problems, was floppy, or had clubfoot at birth. Questions from the MDHI-SF were included to assess disease burden and symptom severity in the six months prior to the first pregnancy, during the first pregnancy, and in the six months following the first pregnancy. The MDHI-SF is a short form of the Myotonic Dystrophy Health Index (MDHI) [9]. The MDHI is a validated patient-reported outcome measure designed to measure the most relevant symptomatic issues in myotonic dystrophy. The MDHI has been shown to have good test-retest reliability, construct validity, and sensitivity to differentiate between groups of DM patients with different levels of disease severity [9, 13]. The MDHI-SF includes 17 select MDHI questions. These questions represent the 17 most important symptomatic themes in DM1 health and were selected based on their level of relevance to the DM population [13], reliability testing, and individual validity testing [9, 13].
Statistical analysis
The complications and outcomes of pregnancy were summarized descriptively. The first pregnancy was analyzed independently from later pregnancies. Subgroup analysis was performed based on the type of DM, overall number of pregnancies, complications with pregnancy, or having a child with DM. The prevalence of each symptomatic theme in the MDHI-SF was calculated for each time frame (6 months prior to pregnancy, during pregnancy, and 6 months post pregnancy). A chi-square test was utilized to examine the difference between subpopulations. A population impact score for each of the individual items in the MDHI-SF was calculated. As previously described, the population impact score is the prevalence of the symptom in the study population multiplied by the mean impact of the symptom in the participants who experience it (range 0–4) [13]. Comparisons of the prevalence and population impact scores for each individual symptom addressed in the MDHI-SF were determined across time using a pairwise comparison between the score prior to pregnancy and the score after pregnancy. For subpopulation analyses with a small sample size (DM2 analyses), Analysis of Variance was used to compare differences between the score prior to, during, and after pregnancy. All analyses were carried out using the SAS 9.4 software. A P-value of less than 0.05 was considered statistically significant.
RESULTS
From the combined registries, 217 women returned the survey (144 from MDF registry, 73 from national registry) for a 40.0% response rate. 152 (70%) of these women reported that they had been pregnant at least once. The demographic information, number of pregnancies, and abortions/miscarriage rates for both DM1 and DM2 are provided in Table 1.
There were 375 total pregnancies: 290 reported pregnancies from 152 women with DM1 and 70 reported pregnancies from 122 women with DM2. Fifteen pregnancies were reported from DM woman who did not know (n = 5) or did not report (n = 1) what type of myotonic dystrophy they had. A total of 48.9% (49.6% for DM1 and 50% for DM2) of women reported developing some clinical symptoms of DM prior to their first pregnancy, 37.6% (36.3% DM1 and 40.9% DM2) did not have any symptoms prior to their first pregnancy, and 10.6% (12.4 DM1 and 0 for DM2) were unsure.
Assistive reproductive technology (e.g., hormone therapy, in vitro fertilization) was reported during pregnancy in DM. During their first pregnancy, 18.1% (DM1:19.8% , DM2:13.6%) of women used in vitro fertilization, but only 6.9% (DM1:6.9% , DM2:9.1%) of women reported using pre-implantation diagnosis. 34.1% of the pregnancies that used in vitro fertilization resulted in a child with DM. 12.1% of women with DM1 and zero percent of women with DM2 utilized hormone therapy in their first pregnancy.
Of the DM1 initial pregnancies carried to term, 36.2% of the children had a combination of feeding problems, breathing problems, hypotonia, or clubfoot at birth, which may be considered congenital DM1[8].
Women with DM experienced a high rate of pregnancy complications (Table 2). During the first pregnancy, 10.4% of women reporting pre-eclampsia and 13.9% of women reporting peripartum hemorrhage. Comparing women with DM1 and DM2, pre-eclampsia was more common in DM2 (13.6% vs 9.5%), while polyhydramnios (25% vs 0.0%) and pre-term labor (31.0% vs 13.6%) were more common in DM1 (Table 2). Polyhydramnios has been specifically associated with congenital DM, which may explain why this is only reported in women with DM1 [14].
Among those DM1 women who had a child with neonatal complications of myotonic dystrophy during the first pregnancy, 49% went on to have a second pregnancy. The outcome of the second pregnancy in these cases resulted in a child with myotonic dystrophy 44% of the time, 33% of these subsequent pregnancies had neonatal complications of myotonic dystrophy.
Women with DM reported that select symptoms progressed during pregnancy. In some cases, these symptoms did not return to baseline six months after pregnancy. When evaluating DM1 participants, the prevalence of mobility limitations (p < 0.001), activity limitations (p = 0.008), pain (p = 0.021), emotional issues (p = 0.041), and myotonia (p = 0.045) increased when comparing results prior to pregnancy with after pregnancy (Fig. 1A). In women with DM1, there was a significant increase in the impact of mobility limitations (p < 0.001), activity limitations (p = 0.001), fatigue (p = 0.043), pain (p = 0.019),emotional issues (p = 0.002) and myotonia (p = 0.039) from pre-pregnancy to after pregnancy (Fig. 1B).
In DM2, women reported that activity limitations (p = 0.044) were more prevalent after pregnancy (Fig. 2A). In DM2, there was a significant increase in the impact of mobility limitations (p = 0.009), activity limitations (p = 0.035), fatigue (p = 0.003), communication difficulties (p = 0.043), and sleep impairment (p = 0.016) after pregnancy (compared to prior to pregnancy) (Fig. 2B).
DISCUSSION
This study highlights the possible complications and outcomes associated with pregnancy in DM. Our DM participants had a higher total miscarriage rate (DM1:32.1% , DM2:37.1%) than the national average of 16.9% [15]. DM rates of preeclampsia (10.4%) and peripartum hemorrhage (13.9%) were also elevated compared to the national rates of 3.4% and 2.9% , respectively [16, 17].
Women with DM were more likely to use reproductive technology (35%) than the national average (12%) [18]. Prior studies have shown that women with DM1 may have diminished ovarian reserve and less favorable outcome with in vitro fertilization, though it is possible for women with DM1 to successfully complete in vitro fertilization [19–21]. While 18.1% of woman used in vitro fertilization during their first pregnancy, only 6.6% used pre-implantation diagnosis. When properly utilized, a combination of in vitro fertilization, genetic testing, and selective implantation can be used to significantly reduce or even prevent the transmission of DM between generations. The low use of pre-implantation diagnosis may have been the result of the mother being unaware of her own diagnosis, personal preference, financial concerns, or a lack of awareness among fertility specialists.
Those participants responding to the survey reported that up to 36.2% of initial DM1 pregnancies carried to term resulted in a child with congenital DM. While this percentage of congenital DM births is higher than previously reported [7], we suspect that this was due in part to a sampling bias and the utilization of only registry participants.
This study identifies a possible risk of disease progression during pregnancy; especially in activity limitation and mobility, fatigue, and pain. In these symptoms, disease burden advanced during pregnancy and did not return to the pre-pregnancy state after 6 months.
The highest reported complication rates were associated with the first DM pregnancy. Similarly, the percentage of mothers with DM1 reporting symptoms associated with congenital DM in their child was reduced in subsequent pregnancies. We suspect that these results reflect the possibility that participants with severe complications during their first pregnancy were more likely than those that had minimal complications to avoid subsequent pregnancies.
There are limitations to this study. First, the response rate was relatively low. This is particularly of concern in the interpretation of the responses from DM2 patients, where the number of participants was lower than in DM1. Second, participants were limited to those woman involved in one of the two major United States DM Registries. Results from this study do not include input from DM women outside of these two registries nor does it evaluate cases involving paternal transmission of DM. Though participants were instructed not to, they may have completed the survey in both registries, should they have been members of both. Thirdly, there was no control group, so a similar change in the MDHI-SF can not be compared to those women who were not pregnant. Lastly, this study was retrospective. Participants provided information, which may have been prone to recall bias or potentially DM-associated cognitive dysfunction. Ideally, the reporting of symptoms, complications, and outcomes, including the use of the MDHI-SF, should be performed in a prospective fashion. It is also not known when the mother’s in our study were diagnosed. It is certainly possible that a mother’s knowledge of her own diagnosis of DM1 prior, during, or after her pregnancy played a role in how she retrospectively viewed her symptoms during these time periods. Future prospective studies of pregnancy in DM should beconsidered.
Overall, this study uses patient insight to highlight the risks, complications, and disease progression associated with DM pregnancy. Results from this study provide data regarding possible symptom progression during the course of a DM pregnancy and identifies divergent patterns of symptom progression related to pregnancy in both DM1 and DM2. The information from this research may be utilized by DM patients and family members seeking to better understand the risks and outcomes associated with pregnancy in DM.
ACKNOWLEDGMENTS
This research is supported by the Myotonic Dystrophy Foundation and the Goldberg Nathan Myotonic Dystrophy Type-2 Endowment. The authors thank Jerry Bounsanga from the University of Utah for assistance with data analysis.
REFERENCES
1 | Fu YH, Pizzuti A, Fenwick RGJr, King J, Rajnarayan S, Dunne PW, Dubel J, Nasser GA, Ashizawa T, de Jong P (1992) An unstable triplet repeat in a gene related to myotonic muscular dystrophy Science 255: 5049 1256 1258 |
2 | Mahadevan M, Tsilfidis C, Sabourin L, Shutler G, Amemiya C, Jansen G, Neville C, Narang M, Barcelo J, O’Hoy K (1992) Myotonic dystrophy mutation: An unstable CTG repeat in the 3’ untranslated region of the gene Science 255: 5049 1253 1255 |
3 | Brook JD, McCurrach ME, Harley HG, Buckler AJ, Church D, Aburatani H, Hunter K, Stanton VP, Thirion JP, Hudson T (1992) Molecular basis of myotonic dystrophy: Expansion of a trinucleotide (CTG) repeat at the 3’ end of a transcript encoding a protein kinase family member Cell 68: 4 799 808 |
4 | Bachinski LL, Udd B, Meola G, Sansone V, Bassez G, Eymard B, Thornton CA, Moxley RT, Harper PS, Rogers MT (2003) Confirmation of the type 2 myotonic dystrophy (CCTG)n expansion mutation in patients with proximal myotonic myopathy/proximal myotonic dystrophy of different European origins: A single shared haplotype indicates an ancestral founder effect American Journal of Human Genetics 73: 4 835 848 |
5 | Liquori CL, Ricker K, Moseley ML, Jacobsen JF, Kress W, Naylor SL, Day JW, Ranum LP (2001) Myotonic dystrophy type 2 caused by a CCTG expansion in intron 1 of ZNF9 Science 293: 5531 864 867 |
6 | Ranum LP, Rasmussen PF, Benzow KA, Koob MD, Day JW (1998) Genetic mapping of a second myotonic dystrophy locus Nature Genetics 19: 2 196 198 |
7 | Harper P (2001) Myotonic Dystrophy 3rd ed London W.B. Saunders |
8 | Johnson NE, Heatwole CR (2012) Myotonic dystrophy: From bench to bedside Seminars in Neurology 32: 3 246 254 |
9 | Heatwole C, Bode R, Johnson N, Dekdebrun J, Dilek N, Heatwole M, Hilbert JE, Luebbe E, Martens W, McDermott MP (2014) Myotonic Dystrophy Health Index: Initial evaluation of a disease-specific outcome measure Muscle & Nerve 49: 6 906 914 |
10 | Hopkins AN, Alshaeri T, Akst SA, Berger JS (2014) Neurologic disease with pregnancy and considerations for the obstetric anesthesiologist Semin Perinatol 38: 6 359 369 |
11 | Awater C, Zerres K, Rudnik-Schoneborn S (2012) Pregnancy course and outcome in women with hereditary neuromuscular disorders: Comparison of obstetric risks in 178 patients European Journal of Obstetrics, Gynecology, and Reproductive Biology 162: 2 153 159 |
12 | Rudnik-Schoneborn S, Schneider-Gold C, Raabe U, Kress W, Zerres K, Schoser BG (2006) Outcome and effect of pregnancy in myotonic dystrophy type 2 Neurology 66: 4 579 580 |
13 | Heatwole C, Bode R, Johnson N, Quinn C, Martens W, McDermott MP, Rothrock N, Thornton C, Vickrey B, Victorson D (2012) Patient-reported impact of symptoms in myotonic dystrophy type 1 (PRISM-1) Neurology 79: 4 348 357 |
14 | Zaki M, Boyd PA, Impey L, Roberts A, Chamberlain P (2007) Congenital myotonic dystrophy: Prenatal ultrasound findings and pregnancy outcome Ultrasound in obstetrics & gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology 29: 3 284 288 |
15 | Ventura SJ, Curtin SC, Abma JC, Henshaw SK (2012) Estimated pregnancy rates and rates of pregnancy outcomes for the United States, -National vital statistics reports: From the centers for disease control and prevention, National Center for Health Statistics, National Vital Statistics System 60: 7 1 21 |
16 | Ananth CV, Keyes KM, Wapner RJ (2013) Pre-eclampsia rates in the United States, 1980-2010: Age-period-cohort analysis BMJ 347: f6564 |
17 | Callaghan WM, Kuklina EV, Berg CJ (2010) Trends in postpartum hemorrhage: United States, -American Journal of Obstetrics and Gynecology 353 e 202: 4 351 356 |
18 | Centers for Disease Control and Prevention, American Society for Reproductive Medicine, Society for Assisted Reproductive Technology. 2011 Assisted Reproductive Technology Fertility Clinic Success Rates Report. Atlanta (GA): US Dept of Health and Human Services; 2013 |
19 | Srebnik N, Margalioth EJ, Rabinowitz R, Varshaver I, Altarescu G, Renbaum P, Levi-Lahad E, Weintraub A, Eldar-Geva T (2014) Ovarian reserve and PGD treatment outcome in women with myotonic dystrophy Reproductive Biomedicine Online 29: 1 94 101 |
20 | Dechanet C, Castelli C, Reyftmann L, Coubes C, Hamamah S, Hedon B, Dechaud H, Anahory T (2010) Myotonic dystrophy type 1 and PGD: Ovarian stimulation response and correlation analysis between ovarian reserve and genotype Reproductive Biomedicine Online 20: 5 610 618 |
21 | Verpoest W, De Rademaeker M, Sermon K, De Rycke M, Seneca S, Papanikolaou E, Spits C, Van Landuyt L, Van der Elst J, Haentjens P (2008) Real and expected delivery rates of patients with myotonic dystrophy undergoing intracytoplasmic sperm injection and preimplantation genetic diagnosis Human Reproduction 23: 7 1654 1660 |
Figures and Tables
Fig.1
Symptomatic Impact of Pregnancy in Women with Myotonic Dystrophy Type-1. A. The prevalence of MDHI themes for women with myotonic dystrophy type-1. B. The impact score for MDHI themes for women with myotonic dystrophy type-1. Themes were compared between the 6 months prior to the first pregnancy and 6 months after the first pregnancy. ( *) indicates a p-value<0.05.
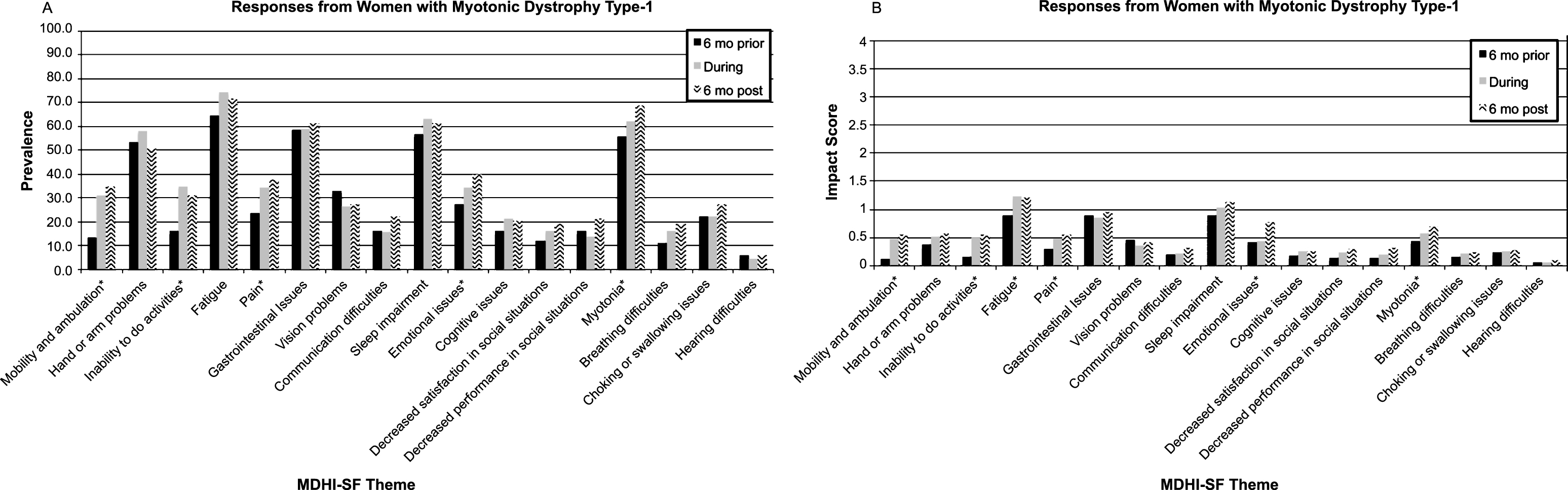
Fig.2
Symptomatic Impact of Pregnancy in Women with Myotonic Dystrophy Type-2. A. The prevalence of MDHI themes for women with myotonic dystrophy type-2. B. The impact score for MDHI themes for women with myotonic dystrophy type-2. Themes were measured 6 months prior to the first pregnancy, during the first pregnancy, and 6 months after the first pregnancy. ( *) indicates a p-value<0.05.
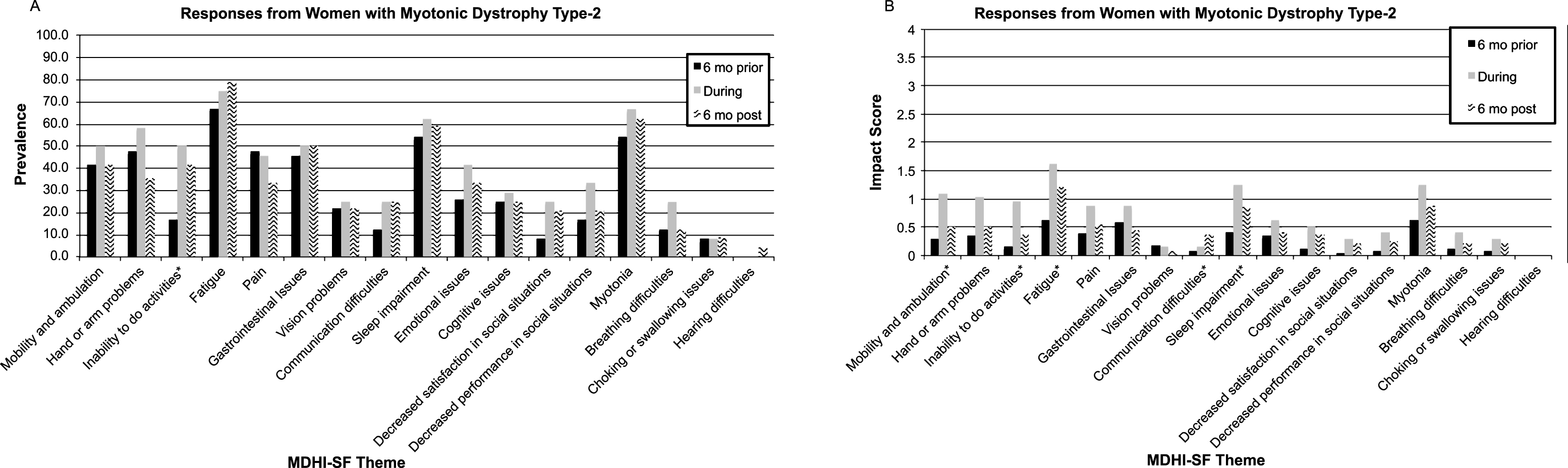
Table 1
Demographics of respondents at time Of survey
| Type1 (n = 122) | Type2 (n = 24) | |
| Mean Maternal Age at Time of Survey | 38.0 (SD 6.5) | 42.0 (SD 8.1) |
| Mean Duration of DM | 14.8 (SD 9.8) | 14.6 (SD 9.8) |
| Ethnicity | Caucasian 95.1%, | Caucasian 100%, |
| Asian 0.8%, | Hispanic 4.2% | |
| Hispanic 9.0%, | ||
| Other 4.1% | ||
| Mean CTG/CCTG length (SD) | 357 (222.5) | 9964 (7299.0) |
| Number of pregnancies | 290 | 70 |
| Pregnancies greater than 20 weeks | 200 | 58 |
| Abortions/Miscarriages | 93 | 26 |
| Abortion/Miscarriage rate | 32.1% | 37.1% |
Table 2
Pregnancy, complications, and outcomes
| 1st pregnancy (DM1; n = 116) | 1st pregnancy (DM2; n = 22) | 2nd and later1 (DM1 n = 66) | 2nd and later1 (DM2 n = 22) | |
| Maternal Age | 27.8 (SD 5.6) | 27.1 (SD 5.3) | 30.4 (SD 4.6) | 31.5 (SD 4.7) |
| Assistive Technology (%) | ||||
| In-vitro fertilization | 19.8 | 13.6 | 19.7 | 11.8 |
| Hormone therapy | 12.1 | 0 | 6.1 | 5.9 |
| Pre-implantation diagnosis | 6.9 | 9.1 | 7.6 | 5.9 |
| Pre-eclampsia | 9.5 | 13.6 | 6.1 | 0 |
| Low birth weight | 19.0 | 13.6 | 10.6 | 17.7 |
| Polyhydramnios | 25.0 | 0 | 22.7 | 0 |
| Pre-term labor | 31.0 | 13.6 | 21.2 | 23.5 |
| Miscarriage | 2.6 | 4.6 | 6.1 | 5.9 |
| Stillbirth | 2.6 | 4.6 | 0 | 0 |
| Peripartum hemorrhage | 17.2 | 0 | 9.1 | 11.8 |
| Infection | 1.7 | 0 | 4.6 | 0 |
| None | 37.1 | 63.6 | 47.0 | 52.5 |
| Neonatal Outcomes (%) | ||||
| Mean gestational age | 37.2 (SD 3.7) | 37.0 (SD 4.2) | 37.2 (SD 3.7) | 37.3 (SD 4.5) |
| Child has DM | 57.8% yes, | 9.1% yes, | 46.7 yes, | 0 yes, |
| 18.1% unsure | 77.3% unsure | 23.4 unsure | 75 unsure | |
| Breathing problems | 34.5 | 9.1 | 24.2 | 17.7 |
| Needed ventilator | 26.7 | 0 | 24.2 | 5.9 |
| Feeding problems | 37.9 | 13.6 | 25.8 | 0 |
| Needed a feeding tube | 35.3 | 9.1 | 25.8 | 11.8 |
| Hypotonia | 34.5 | 0 | 31.8 | 0 |
| Clubfoot | 15.5 | 4.6 | 12.1 | 0 |
1 2nd, 3rd, 4th, and later pregnancies were combined for analyses.

