
Quality of Life in Advanced Dementia with Late Onset, Young Onset, and Very Young Onset
Abstract
Background:
Advanced stages of dementia are characterized by severe cognitive and physical impairment. It has not yet been investigated whether persons with young onset dementia (YOD) and late onset dementia (LOD) differ in advanced disease stages.
Objectives:
To compare quality of life (QoL) between persons with advanced YOD and LOD; to explore the determinants of QoL; to investigate whether YOD and LOD differ with regard to symptoms and care.
Methods:
The study was performed in the context of EPYLOGE (IssuEs in Palliative care for persons in advanced and terminal stages of YOD and LOD in Germany). Persons with advanced dementia (PWAD) were assessed and caregivers were interviewed. QoL was measured with the proxy rating Quality of Life in Late Stage Dementia (QUALID) scale.
Results:
93 persons with YOD and 98 with LOD were included. No significant differences in QoL were detected. Determinants of QoL were similar in YOD and LOD. Behavioral and psychological symptoms of dementia (BPSD), suffering and other distressing symptoms were associated with a lower QoL. In YOD but not in LOD antipsychotic treatment was associated with low QoL. The group of persons who were younger than 65 years at the time of the study visit experienced significantly more distressing symptoms than older PWAD.
Conclusion:
Overall, persons with advanced YOD do not appear to be disadvantaged compared to old and oldest PWAD. Special attention, however, must be paid to the group of the very young persons who seem to be particularly vulnerable.
INTRODUCTION
Dementias are life-limiting diseases for which a curative treatment does not exist [1, 2]. Advanced dementia stages are characterized by severe cogni-tive, physical, and functional impairment so that most persons with advanced dementia (PWAD) need 24-hour care [3]. Often PWAD present with neuropsychiatric symptoms, e.g., apathy, depression, or irritability, and sleep disturbances [4]. Dementia-associated medical complications include swallowing disorders, aspiration pneumonia, infections, and dehydration [5]. It is controversial when the palliative phase starts during the disease trajectory. But without any doubt PWAD are subject of palliative care when the aim of treatment is not stabilization of cognitive functio-ning and life prolongation any more, but provision of maximal comfort in order to maximize quality of life [6]. When picturing PWAD in need of palliative care, inevitably old and very old persons appear in front of the inner eye. However, there is a small group of patients with an early disease onset that is still relatively young in advanced dementia stages. Young onset dementia (YOD) (sometimes referred to as early onset dementia or presenile dementia) is usually defined as dementia with an onset of symptoms before an age of 65 years. The prevalence of YOD ranges between 0 to 700 per 100,000 habitants in groups of 25–64 years old with an increasing incidence with age. Similar to late onset dementia (LOD), Alzheimer’s disease (AD) is the major etiology of YOD, followed by vascular dementia and frontotemporal dementia (FTD) [7]. The proportion of FTD is higher in YOD (up to one fourth of cases) than in LOD (about 5%of cases) [7, 8].
A variety of studies has shown that there are sig-nificant differences between YOD and LOD in early disease stages. These differences are not only exp-lained by the younger age of persons with YOD with the subsequent social and socio-economic implications. YOD and LOD also differ with regard to dementia etiology, symptoms, therapy, caregiver burden, and many more [9–15]. However, less attention has been paid to potential differences between YOD and LOD in advanced disease stages. It is unclear whether persons with advanced YOD and LOD differ regarding functional and cognitive impairment, neuropsychiatric and somatic symptoms, or psychotropic drug therapy, wellbeing, and quality of life (QoL). The World Health Organization (WHO) has defined QoL as the individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is affected by physical, psychological, and social wellbeing [16]. QoL has been recognized as an important measure of general wellbeing in dementia [17]. However, QoL measurement in advanced disease stages is problematic since severe cognitive impairment and communication problems hinder reliable self-reports [18]. This might be the reason why only very few studies have investigated QoL in persons with severe dementia using proxy ratings [19, 20]. One study has shown that (within the group of mostly LOD-patients) younger age of the PWAD was correlated with decreased QoL [21]. QoL in advanced YOD has, to the best of our knowledge, so far only been examined in one single study [22]. This is surprising since knowledge about potential differences between YOD and LOD is necessary in order to address special needs of persons with advanced YOD in a setting that is usually designed for LOD and in order to define strategies with the aim to improve QoL.
Therefore, the main aims of our study were to compare QoL between persons with advanced YOD and LOD and to explore the determinants of QoL. As described above, one study has already shown that younger age of the PWAD was correlated with decreased quality of life [21]. Furthermore, our clinical experience was that particularly relatives of PWAD with young onset seemed to seek help. Therefore, our study departed from the hypothesis that QoL is lower in persons with advanced YOD than LOD. In addition, it was investigated whether advanced YOD and LOD differ with regard to symptoms and care.
METHODS
This analysis was performed within the prospective clinical study EPYLOGE (IssuEs in Palliative care for people in advanced and terminal stages of Young-onset and Late-Onset dementia in Germany). The study design of EPYLOGE (ClinicalTrials.gov (NCT03364179)) has already been published [23]. In brief, in the project described below, persons with YOD and LOD in advanced dementia stages, who were cared for at home or in long-term care (LTC) facilities, were prospectively assessed. A standardized interview of the family caregiver was conducted. Additional information was gathered from medical and care files.
The clinical study was approved prior recruitment of participants by the Ethics Committee of the School of Medicine of the Technical University of Munich (18. Aug. 2017; No. 281/17 S). For more details about ethical considerations, data management, quality assurance, and data protection, see [23].
Participants
Dyads of persons with advanced YOD or LOD, who were cared for at home or in LTC, and their family caregivers were recruited. Stratification was used, aiming at the inclusion of 50%YOD and 50%LOD. Inclusion criteria were: 1) “Advanced dementia”, defined as Clinical Dementia Rating (CDR, [24]) global score 2 or 3; 2) An adult family caregiver who was willing to participate; 3) Written informed consent from the family caregiver and the patient’s legal representative. PWAD were identified from previous patients of the Center of Cognitive Disorders at the University Hospital of the Technical University of Munich who had been diagnosed with dementia since 2005.
Assessments
PWAD were visited by a neurologist with psychi-atric and palliative expertise (JH and CR) at their place of living, be it at home or in LTC. A detailed examination of the PWAD was performed, a standardized interview of the family caregiver was con-ducted, and all available medical and care records were studied. Demographic data were collected. So-matic, neurologic, cognitive, and psychiatric symptoms were assessed. Severity of dementia, quality of life, wellbeing/ suffering, psychotropic drug therapy, and non-drug treatments were documented. The assessment tools are summarized in Table 1. To asses QoL, the German version of the Quality of Life in Late Stage Dementia (QUALID) [25] was chosen. The QUALID is a proxy rating of QoL in persons with severe dementia that is composed of 11 items (smiles, appears sad, cries, has a facial expression of discomfort, appears physically uncomfortable, complaints, groans or screams, is irritable or aggressive, enjoys eating, touching or being touched, interacting or being with others, appears emotionally calm and comfortable), rating from one to five, with lower scores representing better QoL. The observation pe-riod is the last seven days before the assessment.
Table 1
Tests, interviews, and questionnaires (alphabetic order) used for study purposes
| Name | Reference | Period of observation; type of survey | Interpretation |
| Barthel Index - activities of daily living | [43] | At the visit; Caregiver interview | 10 subitems. Total score 0–100. The higher the better |
| Clinical Dementia Rating Scale (CDR) | [24] | At the visit; Medical opinion based on PWAD assessment and caregiver interview | Global score 0–3. Score 2: moderate dementia; Score 3: severe dementia Sum of boxes: 0 –18. |
| End-of-Life in Dementia Scale: Symptom Management (EOLD-SM) | [44] | Last 90 days; Caregiver interview | The higher the more severe. 9 subitems. Total score 0–45. |
| Global Deterioration Scale (GDS) | [45] | At the visit; Medical opinion based on PWAD assessment and caregiver interview | The higher the better symptom control Score 1 to 7. score 5: moderately severe; score 6: severe; score 7: very severe cognitive decline |
| Mini-Mental State Examination (MMSE) | [46] | At the visit; Cognitive test | Total score 0–30. The higher the less cognitive impairment |
| Mini-Suffering State Examination (MSSE) | [47] | At the visit; Medical opinion based on PWAD assessment and caregiver interview | 10 subitems. Total score 0–10. The higher the more suffering |
| Neuropsychiatric Inventory (NPI) | [48] | Last four weeks; Caregiver interview | 12 subitems. Total score 0–144. The higher the more neuropsychiatric symptoms |
| Pain Assessment in Dementia (PAINAD) | [49] | At the visit; 5-mine observation | 5 subitems. Total score 0–10. The higher the more pain by study physician |
| Quality of Life in Late Stage Dementia (QUALID) | [25] | Last week; Caregiver interview | 11 subitems. Total score 11–55. The higher the lower quality of life. |
Primary outcome and sample size calculation
According to the hypothesis that in advanced dem-entia persons with YOD have a lower QoL than persons with LOD, the total score of the QUALID was chosen as the primary endpoint. Before recruitment sample size calculation for the comparison of persons with YOD and LOD was performed using the primary endpoint QUALID total score. Sample size calculation is described in [23]. At least 86 PWAD per age group were required for the assessments, comprising a total of 172 PWAD.
Statistical methods
SPSS Statistics 25.0 for Windows (Armonk, New York, USA) was used for analyses.
For the QUALID as primary endpoint missing data were imputed. Single missing QUALID values were replaced using the mean observed value for the respective question.
Continuous data were compared between two gr-oups by Student’s t-test or by Mann-Whitney U test, depending on the distribution of variables. Categorical variables were compared by χ2 tests or Fisher exact test. We chose an exploratory approach without Bonferroni correction for multiple testing. For correlation analyses Spearman’s rank correlation coefficient was used. Multiple linear regression analysis was performed in order to adjust for potentially confounding variables (gender, marital status, place of living, dementia etiology, and dementia severity as measured with CDR sum of boxes). The independent variables in parantheses were selected based on existing evidence on, e.g., [26], and clinical experience about determinants of QOL in dementia. The assumptions of linear regression (noncollinearity, linearity, homoscedasticity, normality and independence) were confirmed before regression analysis.
RESULTS
3.1Recruitment
PWAD were included who had been diagnosed with dementia since 2005 at the Center for Cognitive Disorders at the Department of Psychiatry and Psychotherapy at Technical University of Munich. Diagnoses had been made according to the respective diagnostic criteria for Alzheimer’s disease (acc-ording to ICD-10 [27]), frontotemporal dementia (according to Lund-Manchester Criteria, 1994 [28]; Rascovsky-Criteria, 2011 [29]; and Gorno-Tempini-Criteria, 2011 [30]), Lewy Body Disease (according to McKeith-Criteria, 2005 [31]), vascular dementia (according to NINDS-ARIEN criteria [32], and Cre-utzfeldt-Jacob disease (according to Zerr-Criteria, 2009 [33]), that were valid at the time of the examination. 827 family caregivers of patients were phoned. 619 patients had already died or were not eligible for recruitment because they did not meet the inclusion criteria since they were only mildly impaired, according to a rough estimation of dementia severity by a telephone CDR interview of the family caregiver. Seventeen family caregivers refused to participate. Finally, between September 2017 and November 2019 191 PWAD and their family caregivers were recruited for the study. All but seven PWAD lived in Bavaria. 93 (49%) were persons with YOD and 98 (51%) were persons with LOD. Severity of dementia was moderate (CDR global score = 2) in seven cases (4%) and severe (CDR global score = 3) in 184 cases (96%). Demographics and details to dementia etiology, place of living, caregiver, dementia severity, and cognitive impairment are shown in Table 2.
Table 2
Demographic data, dementia etiology, place of living, caregiver, dementia severity, level of care, and cognitive impairment. Mean±standard deviation (minimum –maximum)
| Total sample | YOD | LOD | YOD versus LOD | |
| N = 191 | N = 93; 48.7% | N = 98; 51.3% | p | |
| PWAD age | 74.13±11.134 | 65.39±7.955 | 82.42±6.333 | <0.001* |
| (40 –101) | (40 –82) | (70 –101) | ||
| Sex | Female: 55% | Female: 49.5% | Female: 61.2% | 0.102 |
| Male: 45% | Male: 50.5% | Male: 38.8% | ||
| Marital status | Married/in | Married/in | Married/in | 0.000* |
| partnership: 68.1% | partnership: 83.9% | partnership: 53.1% | ||
| Single: 31.9% | Single: 16.1% | Single: 46.9% | ||
| Place of living | At home: 46.1% | At home: 47.3% | At home: 44.9% | 0.738 |
| LTC§: 53.9% | LTC: 52.7% | LTC: 55.1% | ||
| Dementia etiology | AD: 64.9% | AD: 58.1% | AD: 71.4% | 0.002* |
| FTD: 24.1% | FTD: 35.5% | FTD: 13.3% | ||
| Other: 10.9% | Other: 6.5% | Other: 15.3% | ||
| If home care: family caregiver | Spouse/partner: | Spouse/partner: | Spouse/partner: | <0.001* |
| 62.3% | 76.6% | 46.0% | ||
| Child: 28.8% | Child: 7.6% | Child: 49.0% | ||
| Mother: 1.6% | Mother: 3.2% | Mother: 0.0% | ||
| Other: 6.8% | Other: 8.6% | Other: 5.1% | ||
| GDS total score | 6.59±0.503 | 6.61±0.511 | 6.57±0.497 | 0.504 |
| (5–7) | (5–7) | (6–7) | ||
| Formal level of care | (N = 190) | (N = 92) | (N = 98) | 0.078 |
| 4.28±0.721 | 4.37±0.707 | 4.19±0.727 | ||
| (“Pflegegrad“) | (2–5) | (2–5) | (3–5) | |
| MMSE total score | (N = 173) | (N = 88) | (N = 85) | 0.201 |
| 1.53±3.081 | 1.26±2.961 | 1.81±3.194 | ||
| (0–14) | (0–14) | (0–13) |
AD, Alzheimer’s disease; FTD, frontotemporal dementia; GDS, Global Deterioration Scale; LTC, Long term care; LOD, late onset dementia; MMSE, Mini-Mental Status Examination; YOD, young onset dementia. *difference between YOD und LOD statistically significant. §LTC includes nursing homes and externally assisted dementia residential communities.
3.2Functional impairment
The majority of PWAD was significantly impaired in the basal activities of daily life, measured with the Barthel Index. The mean total score was 26.99±23.697 (min: 0, max: 85). YOD and LOD did not differ significantly in the total score (p = 0.196). Sig-nificant differences were identified in Barthel Index subitems “mobility” (YOD: 8.60±6.969; LOD: 5.97±6.722; p = 0.008) and “stair climbing” (YOD: 3.66±3.980; LOD: 2.24±3.526; p = 0.008). In all other activities of daily life (feeding, bathing, groo-ming, dressing, bowel control, bladder control, toileting, chair transfer) no differences between YOD and LOD were found.
3.3Behavioral and psychological symptoms of dementia
Behavioral and psychological symptoms of dementia (BPSD) were evaluated with the Neuropsychiatric Inventory (NPI). The mean total NPI score was 24.59±17.017. There were large individual differences (min: 0; max: 84 points). The NPI total score did not differ significantly between YOD and LOD. Also, no differences were seen in the NPI subitems delusion, hallucination, aggression, depression, anx-iety, euphoria, sleep disturbances, and change of appetite, neither with regard to the prevalence of sym-ptoms nor to the score (which is the product fre-quency * severity). However, disinhibition was significantly more prevalent in YOD (35.4%) than in LOD (18.9%; p = 0.014) and the frequency * severity score for disinhibition was significantly higher in YOD (1.88±3.286) than in LOD (0.79±2.207; p = 0.007).
3.4Psychotropic drug therapy and pain medication
The proportion of PWAD treated with antipsychotics at the time of the assessment (point pre-valence, as needed medication was not considered) was almost 40%. About 35%received antidepressants. Antidementia drugs were prescribed in 27%of the patients. Seven percent were treated with benzodiazepines. Six percent had opioids, 16%non-opioid pain medication. There were no significant differences between YOD and LOD with regard to the point prevalence of psychotropic drugs or pain medication (Table 3).
Table 3
Prevalence of psychotropic drug treatment and pain medication (point prevalence at the day of the study assessment)
| Total sample | YOD | LOD | YOD versus LOD p | |
| Antipsychotic | 39.3% | 40.9% | 37.8% | 0.660 |
| Antidepressant | 34.6% | 39.8% | 29.6% | 0.139 |
| Antidementia drug | 26.7% | 26.9% | 26.5% | 0.956 |
| Benzodiazepine | 7.3% | 9.7% | 5.1% | 0.225 |
| Z-Substances | 3.1% | 2.2% | 4.1% | 0.444 |
| Other sedatives and sleep medication* | 1.6% | 3.2% | 0.0% | 0.073 |
| Opioids | 6.3% | 6.5% | 6.1% | 0.925 |
| Non-opioid pain medication | 15.7% | 14.0% | 17.3% | 0.523 |
LOD, late onset dementia; YOD, young onset dementia; Z-Substances, zopiclone and zolpidem. *Cannabidiol, modified-release melatonine.
3.5Pain, suffering, and end-of-life symptoms
Mean scores of the Mini-Suffering State Examination (MSSE), of the Pain Assessment in Dementia (PAINAD), and of the End of Life in Dementia scale–Symptom Management (EOLD-SM) are sh-own in Table 4. There were some individuals with high levels of suffering, pain and end of life symptoms. There were no significant differences between YOD and LOD in the total scores of the respective scales as displayed in Table 4.
Table 4
End-of-life symptoms: pain and suffering in YOD and LOD Mean±standard deviation (Minimum –Maximum)
| Total sample | YOD | LOD | YOD versus LOD p | |
| EOLD-SM total score | (N = 191) 33.07±7.547 (10–45) | (N = 93) 33.15±7.396 (10–45) | (N = 98) 32.99±7.725 (12–45) | 0.973 |
| PAINAD total score | (N = 190) 1.49±1.790 (0–9) | (N = 93) 1.51±1.730 (0–7) | (N = 97) 1.47±1.855 (0–9) | 0.606 |
| MSSE total score | (N = 191) 2.28±1.643 (0–7) | (N = 93) 2.16±1.617 (0–7) | (N = 98) 2.40±1.667 (0–7) | 0.340 |
PAINAD, Pain Assessment in Dementia; EOLD-SM, End of life in dementia scale: Symptom-Management; LOD, late onset dementia; MSSE, Mini-Suffering State Examination; YOD, young onset dementia.
3.6Quality of life
The mean score of the QUALID, that was used to measure QoL was 21.60±6.390; median 20.7. QUALID total scores of YOD (21.60±6.390; min: 11; max: 40) and LOD (22.16±6.375; min: 12; max: 44) did not differ significantly (p = 0.153) as shown in Fig. 1. In two QUALID items (Question A: PWAD smiles and Question H; PWAD enjoys eating) LOD-patients scored higher (reflecting a worse condition) than YOD-patient (Table 5).
Fig. 1
Quality of life in late stage dementia (QUALID) total scores in YOD and LOD. LOD, late onset dementia; QUALID, Quality of life in late stage dementia; YOD, young onset dementia.
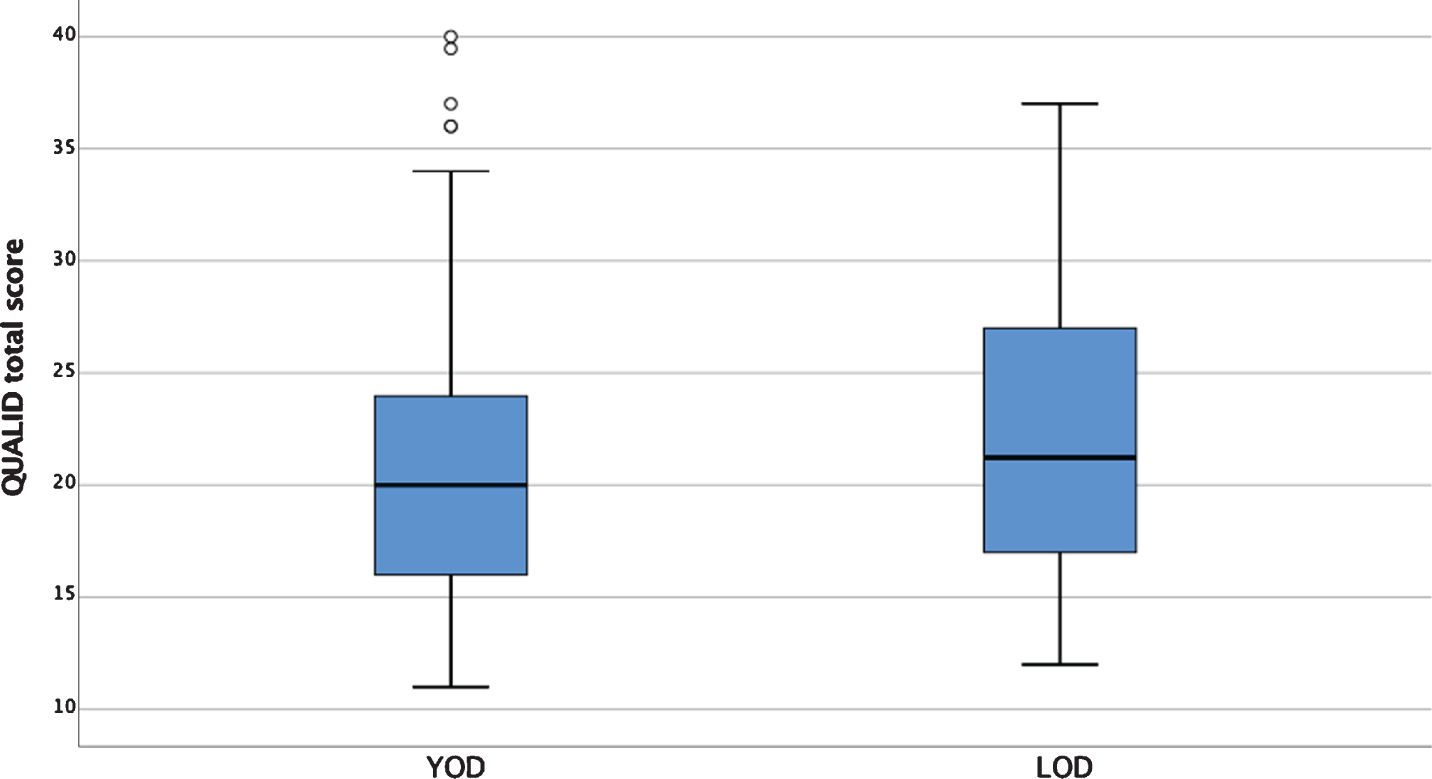
Table 5
Quality of life in late stage dementia (QUALID) in YOD and LOD
| YOD | LOD | YOD versus LOD p | |
| QUALID total score | (N = 93) 21.02±6.389 (11 –40) | (N = 97) 22.16±6.375 (12 –44) | 0.153 |
| QUALID question A: PWAD smiles | (N = 93) 2.67±1.611 (1 –5) | (N = 98) 3.17±1.472 (1 –5) | 0.025* |
| QUALID question H: PWAD enjoys eating | (N = 93) 1.72±1.288 (1 –5) | (N = 98) 2.20±1.573 (1 –5) | 0.035* |
LOD, late onset dementia; PWAD, Person with advanced dementia; QUALID, Quality of life in late stage dementia; YOD, young onset dementia.
A multiple linear regression analysis showed that the QUALID total score still did not differ between YOD and LOD after adjusting for confounding variables: gender, marital status, place of living, dementia etiology, CDR sum of boxes (p = 0.409).
3.7Determinants of quality of life
Regarding sociodemographic characteristics, there were no differences of the QUALID total score (Table 6). Gender, marital status, dementia etiology, and place of living were not associated with QoL measured with the QUALID, neither in YOD nor in LOD. However, persons with YOD who were treated with antipsychotics had a significantly worse QoL than those without antipsychotic treatment (p = 0.007). In the LOD group no significant association between antipsychotic treatment and quality of life was observed.In both age groups, YOD and LOD, the QUALID total scores correlated weakly with the PAINAD scale and moderately with NPI, EOLD-SM, and MSSE (Table 7). QUALID total scores did not correlate significantly with age, CDR sum of boxes, MMSE, and Barthel-Index.
Table 6
Comparison of quality of life in late stage dementia (QUALID) total scores in YOD and LOD with regard to sociodemographics and antipsychotic drug treatment
| YOD | LOD | |||||||
| N | QUALID mean±SD | p | Difference in means (95%confidence interval) | N | QUALID mean±SD | p | Difference in means (95%confidence interval) | |
| Gender | ||||||||
| Women | 46 | 21.446±6.344 | 0.525 | 0.85 (–1.79 to 3.49) | 59 | 22.503±6.818 | 0.499 | 0.87 (–1.67 to 3.41) |
| Men | 47 | 20.599±6.473 | 38 | 21.635±5.665 | ||||
| Married/ partnership | ||||||||
| yes | 78 | 20.756±6.368 | 0.388 | 1.62 (–5.46 to 2.21) | 51 | 21.253±6.077 | 0.142 | 1.92 (–4.49 to 0.65) |
| no | 15 | 22.379±6.542 | 46 | 23.171±6.609 | ||||
| Dementia etiology | ||||||||
| AD | 54 | 20.724±6.605 | 0.606 | 0.74 (–3.62 to 2.12) | 69 | 21.877±6.446 | 0.606 | 0.97 (–4.84 to 2.91) |
| FTD | 33 | 21.471±6.472 | 13 | 22.844±6.022 | ||||
| Place of living | ||||||||
| Home care | 44 | 21.015±6.981 | 0.996 | 0.01 (–2.68 to 2.67) | 43 | 21.794±6.033 | 0.61 | 0.66 (–3.23 to 1.91) |
| Long term care | 49 | 21.021±5.880 | 54 | 22.456±6.676 | ||||
| Antipsychotic treatment | ||||||||
| yes | 38 | 23.345±4.764 | 0.007* | 3.94 (–6.74 to –1.13) | 37 | 23.103±7.635 | 0.295 | 1.52 (–4.40 to 1.36) |
| no | 55 | 19.410±7.678 | 60 | 21.583±5.446 | ||||
*statistically significant. AD, Alzheimer’s disease; FTD, frontotemporal dementia; LOD, late onset dementia; QUALID, Quality of life in late stage dementia; SD, standard deviation; YOD, young onset dementia.
Table 7
Correlation between Quality of life in late stage dementia (QUALID) total scores in YOD and LOD, PWAD age and measures of dementia severity, cognition, functional abilities, neuropsychiatric and other symptoms
| QUALID YOD | QUALID LOD | |||
| N | Spearman’s rho | N | Spearman’s rho | |
| Patient age | 93 | –0.163 | 97 | 0.032 |
| CDR sum of boxes | 93 | 0.011 | 97 | 0.093 |
| MMSE | 88 | –0.030 | 94 | –0.122 |
| Barthel-Index | 93 | 0.093 | 97 | –0.068 |
| NPI | 93 | 0.424** | 97 | 0.464** |
| EOLD-SM | 93 | –0.409** | 97 | –0.460** |
| PAINAD | 93 | 0.220* | 97 | 0.253* |
| MSSE | 93 | 0.574** | 97 | 0.396** |
*Correlation is significant at the 0.01 level (two-tailed). **Correlation is significant at the 0.05 level (two-tailed). CDR, Clinical Dementia Rating scale; EOLD-SM, End of life in dementia: Symptom-Management; LOD, late onset dementia; MMSE, Mini-Mental State Examination; MSSE, Mini-Suffering State Examination; NPI, Neuropsychiatric Inventory; PAINAD, Pain Assessment in Dementia; QUALID, Quality of life in late stage dementia; YOD, young onset dementia.
3.8Quality of life: individual differences
The majority, 62.4%of YOD-caregivers and 65.3%of LOD-caregivers, estimated that “The person with advanced dementia appears calm and com-fortable most time of the day” (QUALID Question K). On the contrary, 5.4%of YOD-caregivers and 10.2%of LOD-caregivers stated that: “The person with advanced dementia appears calm and comfortable rarely or never.” From Fig. 1, the large individual differences of the QUALID total scores, ranging from 11 (best possible QoL) to 44 points (poor QoL), are obvious. Several PWAD were reported to have a very low QoL with high QUALID scores.
Table 8 gives an overview about neuropsychiatric symptoms, pain, drug and non-drug therapy, and (palliative) care of the 18 PWAD with the worst (defined as >30 points) QUALID total scores. Half of the PWAD were YOD. 67%were female. 56%lived in LTC. NPI scores show that symptoms that required treatment, particularly delusion, hallucinations, aggression, anxiety and pain, obviously did not response to the treatment provided or were not treated sufficiently. Only very few PWAD got specific or unspecific non-drug treatment. In two PWAD care was exclusively provided by the family caregivers. In only six PWAD regular doctor visits were provided. Palliative expertise was involved in five PWAD.
Table 8
PWAD with the worst quality of life, defined as a Quality of Life in Late Stage Dementia (QUALID) total score >30
| Age, Gender, Dementia, Place of living | QUALID total score | NPI Delu-sion | NPI Halluci-nation | NPI Agi-tation | NPI Depre-ssion | NPI Anx-iety | NPI Eup-horia | NPI Apathy | NPI Disin-hibition | NPI Irri-tability | NPI Motor behanvior | NPI Sleep disturbances | NPI Appetite | NPI total score | PAINAD total score | Psychotropic drug (without prn drugs. daily dose) | Non-drug therapy* | (Palliative) Care |
| Female 83, LOD AD LTC | 31 | 0 | 0 | 6 | 4 | 0 | 0 | 8 | 8 | 2 | 4 | 0 | 0 | 32 | 0 | Fentanyl td 25μg every 3 days Venlafaxine 75 mg | none | Regular doctor’s visits |
| Female 70, YOD AD LTC | 31.42 | 0 | 0 | 3 | 4 | 2 | 0 | 8 | 0 | 3 | 8 | 0 | 0 | 28 | 1 | Melperone 75 mg Mirtazapine 30 mg Valproate 600 mg Risperidone 1.5 mg | none | Regular doctor’s visits; palliative care nurse |
| Female 58, YOD AD LTC | 31.49 | na | na | 12 | 12 | 12 | 0 | 12 | 0 | 0 | 0 | 4 | na | 52 | 7 | Ciatyl 15 mg Novaminsulfone 1 g Tilidine/Naloxone 400/32 mg | none | Regular doctor’s visits; SAPV prn |
| Female 59, YOD AD LTC | 32 | 6 | 2 | 6 | 6 | 6 | 0 | 0 | 6 | 6 | 4 | 6 | 12 | 60 | 1 | Sertralin 100 mg Quetiapin 200 mg Quetiapin ret. 150 mg Brivaracetam 100 mg | none | Regular doctor’s visits |
| Female 90, LOD VaD LTC VaD LTC | 32 | na | na | 0 | 4 | 0 | 0 | 12 | 4 | 0 | 4 | 0 | 12 | 36 | 0 | none | none | Regular doctor’s visits |
| Female 88, LOD AD LTC | 33 | 0 | 0 | 3 | 2 | 0 | 4 | 8 | 0 | 4 | 0 | 6 | 0 | 27 | 1 | Lorazepam 1 mg Risperidone 1 mg | none | Regular doctor’s visits |
| Female 98, LOD | 33 | 0 | 0 | 0 | 4 | 0 | 0 | 12 | 0 | 0 | 0 | 0 | 12 | 28 | 1 | none | none | Regular doctor’s visits; dementia companion |
| Male 90, LOD AD HC | 33 | na | 0 | 12 | na | 12 | 0 | 12 | 3 | 12 | 8 | 12 | 0 | 71 | 2 | Aripiprazole 7.5 mg Pipamperone 40 mg Valproate 600 mg | none | Regular doctor’s visits; palliative care nurse |
| Male 73, YOD FTD HC | 34 | 12 | 4 | 12 | 4 | 3 | 9 | 0 | 12 | 12 | 12 | 4 | 0 | 84 | 4 | Mirtazapine 7.5 mg | none | Regular doctor’s visits |
| Female 87, LOD AD HC | 35 | 0 | 0 | 9 | 12 | 3 | 0 | 12 | 2 | 4 | 2 | 12 | 0 | 56 | 6 | Memantine 30 mg Risperidone 1 mg Promethazine 12.5 mg | none | Regular doctor’s visits; ambulatory nursing service |
| Male 42, YOD FTD ssHC | 36 | 0 | 0 | 0 | 0 | 2 | 0 | 8 | 4 | 8 | 0 | 0 | 22 | 4 | Risperidone 7 mg Prothipendyle 200 mg | none | Dementia companion | |
| Male 68, YOD AD HC | 36 | 0 | 0 | 12 | 4 | 0 | 0 | 12 | 0 | 8 | 12 | 12 | 0 | 60 | 1 | Risperidone 1 mg Donepezil 10 mg | none | Regular doctor’s visits, dementia companion |
| Female 79, LOD AD LTC | 36.27 | 0 | na | 0 | 12 | na | 0 | 12 | 0 | 0 | 0 | 0 | 4 | 28 | 1 | none | Speech therapy 1/week | Regular doctor’s visits palliative care service; palliative care nurse; support through hospice association |
| Female 69, YOD AD HC | 37 | 12 | 12 | 0 | 0 | 4 | 0 | 12 | 0 | 0 | 12 | 0 | 0 | 52 | 4 | Quetiapine 125 mg Aripiprazole 25 mg | none | none |
| Male 80, LOD FTD HC | 37 | 12 | 0 | 0 | 12 | 12 | 0 | 12 | 0 | 8 | 8 | 12 | 0 | 76 | 6 | Quetiapine 75 mg | none | none |
| Female 41, YOD AD HC | 39.46 | na | na | 0 | 12 | 12 | 0 | na | na | na | na | 0 | na | 24 | 6 | Haloperidole 3 mg Trazodone 50 mg Valproate 1200 mg Lorazepam 2 mg | none | Regular doctor’s visits; ambulatory nursing service |
| Male 61, YOD LTC FTD | 40 | 0 | 4 | 12 | 12 | 8 | 0 | 12 | 0 | 12 | 12 | 0 | na | 72 | 5 | Valproate 1800 mg Valproate ret. 600 mg CiatylZ acuphase i.m. 50 mg once | none | Regular doctor’s visits palliative care nurse; support through hospice association dementia companion |
| Female 82, LOD AD LTC | 44 | 12 | 0 | 0 | 12 | 12 | 0 | 6 | 1 | 12 | 12 | 0 | 12 | 79 | 5 | Pipamperone 40 mg Mirtazapine 30 mg Lorazepam 0.5 mg | none | Regular doctor’s visits |
AD, Alzheimer’s dementia; g, gram; i.m., intramuscular; FTD, frontotemporal dementia; HC, home care; LOD, late onset dementia; LTC, long term care; mg, milligram; na, not assessable; NPI, Neuropsychiatric Inventory; PAINAD, Pain Assessment in Dementia; prn, as needed; QUALID, Quality of Life in Late Stage Dementia; ret., retard; SAPV, special ambulatory palliative care; td, transdermal; VaD, vascular dementia; YOD, young onset dementia. *Non-drug therapy included individualized speech therapy, physiotherapy, occupational therapy, aroma therapy, respiratory therapy, other therapies. Routine group therapies offered in LTC were not considered.
3.9Quality of life of very young persons with YOD
Four out of nine persons suffering from YOD with the worst QoL (Table 8) were PWAD with a very young age at the time of the assessment (41, 42, 59, and 61 years old). This prompted us to perform a post-hoc analysis of QoL of very young persons with YOD in detail. We defined the group of persons with “very young YOD” (VYYOD) as persons with dementia who were younger than 65 years at the time of the EPYLOGE-visit (N = 38). Persons with VYYOD had a mean age of 58.08 years±6.135 (min: 40; max: 64), the 153 not-VYYOD persons of 78.11±8.089; min: 65; max: 101).Persons with VYYOD were male in 39.5 %and female in 60.5%(not-VYYOD: 45.8%male, 54.2%female; p = 0.486). 52.6%of the VYYOD persons lived at home and 47.4%in LTC (not-VYYOD: 44.4%at home, 55.6%LTC; p = 0.365). There was a significant difference between VYYOD and not-VYYOD regarding the etiology of dementia: 55.3%of the persons with VYYOD had a diagnosis of AD, 44.7%of FTD, and 0%other dementia. In the not-VYYOD group, 67.3%suffered from AD, 19.0%from FTD, and 13.7%from other dementias (p = 0.008).The subgroup analysis showed, as displayed in Table 9, that the QUALID item “sadness” was more frequent and “emotional calm and contentment” less frequent in VYYOD. The QUALID total score, however, did not differ significantly between VYYOD (22.56±7.112) and not-VYYOD 21.36±6.200, p =0.418). Furthermore, persons with VYYOD experienced significantly more symptoms (measured with the EOLD-SM total score) and suffering (measured with the MSSE total score) than the older PWAD. In particular “agitation”, “fear”, and “lack of calm” as well as “malnutrition” were more frequent in VYYOD than in not-VYYOD. There were no other significant differences in subitems of EOLD-SM and MSSE, as well as total scores and subitems of PAINAD.
Table 9
Significant differences between VYYOD (age <65 years at the visit) and not-VYYOD (>65 years) with regard to symptoms, suffering and quality of life. Mean±standard deviation (minimum –maximum)
| All PWAD (VYYOD + not -VYYOD) | VYYOD (PWAD < 65 y) | Not-VYYOD (PWAD >65 y) | VYYOD versus not-VYYOD p | |
| QUALID question B: sad | (N = 191) | (N = 38) | (N = 153) | 0.035* |
| 2.27±1.598 | 2.75±1.666 | 2.15±1.563 | ||
| (1 –5) | (1 –5) | (1 –5) | ||
| QUALID question K: calm and comfortable | (N = 191) | (N = 38) | (N = 153) | 0.009* |
| 1.78±1.267 | 2.12±1.236 | 1.69±1.264 | ||
| (1 –5) | (1 –5) | (1 –5) | ||
| EOLD-SM total score | (N = 191) | (N = 38) | (N = 153) | 0.017* |
| 33.07±7.547 | 30.68±6.897 | 33.66±7.606 | ||
| (10 –45) | (10 –43) | (11 –45) | ||
| EOLD-SM agitation | (N = 191) | (N = 38) | (N = 153) | 0.044* |
| 3.51±2.000 | 2.92±2.186 | 3.65±1.931 | ||
| (0 –5) | (0 –5) | (0 –5) | ||
| EOLD-SM fear | (N = 191) | (N = 38) | (N = 153) | 0.036* |
| 3.76±2.001 | 3.18±2.24 | 3.90±1.919 | ||
| (0 –5) | (0 –5) | (0 –5) | ||
| EOLD-SM lack of calmness | (N = 191) | (N = 38) | (N = 153) | 0.012* |
| 4.17±1.730 | 3.55±2.177 | 4.32±1.571 | ||
| (0 –5) | (0 –5) | (0 –5) | ||
| MSSE total score | (N = 191) | (N = 38) | (N = 153) | 0.047* |
| 2.28±1.643 | 2.82±1.843 | 2.15±1.568 | ||
| (0 –7) | (0 –7) | (0 –7) | ||
| MSSE malnutrition | (N = 191) | (N = 38) | (N = 153) | 0.031* |
| 0.13±0.338 | 0.24±0.431 | 0.10±0.307 | ||
| (0–1) | (0–1) | (0–1) |
EOLD-SM, End of life in dementia: Symptom-Management; MSSE, Mini-Suffering Sate Examination; QUALID, Quality of life in late stage dementia; VYYOD, very young onset dementia. *statistically significant difference between VYYOD and not-VYYOD.
DISCUSSION
QoL in YOD and LOD
The main aim of our study that included PWAD living at home and in LTC was to find out if QoL is worse in PWAD with YOD as compared to LOD. Against our assumption there were no differences between YOD and LOD with regard to QoL as measured with the QUALID scale. Furthermore, no differences were detected with regard to suffering, pain, and end-of-life symptoms.
Unexpectedly, we identified the group of persons who were 65 years and younger at the time of the study visit as a particular subgroup of YOD. Compared to the PWAD who were older than 65 years at the time of the study visit, these persons with VYYOD experienced more suffering, measured with the MSSE, were less calm, less content, and had more symptoms that negatively affected well-being.
Our findings suggest that the group of patients with advanced YOD is not disadvantaged overall in a care system geared to old and very old persons. However, special attention must be paid to the small but particular group of people with VYYOD. These very young PWAD are in danger to experience a low QoL. Therefore, QoL must regularly be assessed in this group so that symptoms can be recognized early and treated sufficiently.
The functional status differed slightly between YOD and LOD. Functional impairment was severe in almost all patients included in the study. However, the Barthel index showed that persons with YOD were more mobile than persons with LOD. This means that PWAD with YOD must have the opportunity to take walks and exercise.
On average, BPSD, as measured with the NPI, were mild to moderate in YOD and LOD. The NPI does not offer cut-offs or a grading system. In our view, an NPI mean score of about 25 points (the maximum value 144 corresponds to most severe BPSD) indicates that BPSD were not very pronounced in most patients. Except for “disinhibition”, which was significantly more prevalent in YOD than in LOD, we did not observe differences in the NPI items between YOD and LOD. Disinhibition is a core clinical feature of FTD [29] and includes, for example, impulsive behavior, tactlessness, or sexual disinhibition. It is a so called “challenging” behavior that is often particularly stressful for the caregivers [34] but also for family members [35], and presumably for the nursing home residents who live together with the disinhibited PWAD. Furthermore, it is likely very time-consuming to supervise a disinhibited and mobile PWAD.
Apart from functional impairment and BPSD, an important difference between YOD and LOD was the family constellation. The vast majority of PWAD with YOD was married. This means that most PWAD with YOD had a relatively young, (cognitively) fit partner who was able to take the role as primary caretaker when the patient lived at home. LOD patients living at home were cared for in 50%by the (usually same age) partner and in 50%by (adult) children. For both young partners of YOD patients and adult children of LOD patients, care efforts may be difficult to reconcile with the many obligations in the middle age. However, one may speculate that caring for a young partner with dementia places a greater psychological burden than caring for an elderly parent—even more if there are still children living with the couple. On the other hand, elderly spouses of people with LOD, themselves suffering from physical or cognitive impairment, might be overburdened by the care situation. Therefore, when providing counselling and support for family caregivers, it is important to consider the relationship of the primary caregiver with the PWAD and to give individualized advice accordingly.
In our study QoL appeared to be mildly impaired overall. The QUALID mean score was 21.6 and the median 20.7, similar to results from a UK study of institutionalized PWAD [20]. The QUALID does not offer a grading system or cut-off scores. A score of 11 reflects the best possible QoL, the maximum score is 55, reflecting worst QoL. A mean score of 21.6 most possibly reflects an overall mild impairment of QoL. Most caregivers, that is 62%in YOD and 65%in LOD, estimated that “The person with advanced dementia appears calm and comfortable most time of the day”. We conclude that QoL was relatively good in the majority of PWAD in our study, despite severe cognitive and communicative impairment, dependency, and loss of autonomy. Our study findings are in line with the results of other studies that have found that severity of cognitive impairment and dementia is not necessarily associated with lower QoL [21, 36].
Similar to other studies [37], we did not find clear associations between QoL and socio-demographic variables including age, gender, and marital status. Also, dementia etiology and place of living were not associated with QoL. The latter is a particularly important finding. Our practical experience is that many families are reluctant to entrust the PWAD to an LTC facility because they fear that the PWAD’s QoL is worse in LTC than at home. Our results, however, indicate, that QoL is not associated with the place of living which might be a basis for counselling. We identified pain, BPSD, end-of-life symptoms, and suffering as determinants for QoL in YOD as well as in LOD. This is not very surprising since the QUALID questions include these dimensions. Various studies have already reported that BPSD are negatively associated with QoL in PWAD, e.g., [38, 39]. Appelhof et al. identified agitation/aggression, depression, and apathy as determinants of QoL in persons with dementia. [22] In their multi-center study of patients with YOD, Milenaar et al. found depression to be a determinant of low QoL [26].
The point prevalence of antipsychotics did not differ between YOD and LOD and was quite high with almost 40%. A remarkable finding of our study was that persons with YOD who were treated with antipsychotics had a significantly worse QoL than those without antipsychotic treatment. This association was not observed in LOD. Other studies have already described a negative effect of psychotropic drug use on QoL [22, 38]. Our study is the first to describe an association between antipsychotic drug treatment and lower QoL, particularly in the group of persons with advanced YOD. It can be assumed that PWAD who have no or only mild BPSD, and therefore a higher QoL, are not treated with antipsychotics and vice versa: exactly the patients with moderate and severe BPSD, and therefore a lower QoL, are treated with antipsychotics. Thus, the reason for the low QoL remains unclear. Is it a consequence of the BPSD? Is it caused by the antipsychotic treatment? Or is it a combination of both? In any case, the clear association between antipsychotic drug treatment and low QoL raises the question of the efficacy of antipsychotics, particularly in YOD. Antipsychotics might be less effective in YOD than in LOD or the doses might be too low. Or perhaps doses are too high and persons with YOD are particularly sensitive to side effects as it has been shown for FTD, which is more frequent in YOD than in LOD, before [40]. It cannot be excluded that the antipsychotic treatment itself has a negative effect on QoL. Side effects on cognition and vigilance are well known [41] but there may be other side effects, like irritability, that have not yet been recorded in a standardized way in the small group of persons with advanced YOD.
Further research on indications, dosage, effects, and side effects of antipsychotic and other psychotro-pic drugs is needed in persons with advanced YOD.
In our study, we identified several patients—both with YOD and LOD, both living at home and in LTC—with high QUALID scores and therefore a low QoL. Most PWAD with low QoL had high NPI scores, indicating that they had frequent and severe BPSD. Some patients appeared to suffer from pain. A closer look into the treatment and care of these PWAD with low QoL showed that in most cases treatment and care appeared to be insufficient. NPI scores showed that symptoms requiring treatment, particularly delusion, hallucinations, aggression, anxiety, and pain, were obviously not or insufficiently treated or did not response to the treatment provided. Only very few patients received non-drug therapy (other than standard group therapy in LTC). Our study design did not allow to examine the reasons for this. We assume that symptoms were not recognized, misattributed, or considered as “normal” signs of dementia by caregivers. Especially for PWAD who lived at home, an experienced neurologist or (geronto-)psychiatrist mi-ght not have been available for treatment. Knowledge about non-drug approaches might have been insufficient.
These cases show the need for a timely recognition of burdening symptoms. This can be achieved by a thorough education of family caregivers and regular, careful assessments by professionals. Particularly family caregivers at home must be encouraged and educated where to seek help if the PWAD suffers from pain or BPSD. Health care professionals must be experienced in the management of challenging behavior. Family and professional caregivers should be informed about non-drug strategies.
Some limitations of our study need to be considered. A selection bias was caused by the recruitment strategy. Patients were identified from previous pat-ients of a memory clinic at a University Hospital. Since the memory clinic is a competence center for FTD, persons with FTD were overrepresented in the patient sample. Furthermore, patients who have alr-eady visited a tertiary care center most likely have another background than the majority of patients who had not. Patient education and counselling might be more intensive at a university-based memory clinic than elsewhere and ongoing counselling throughout the disease course might have resulted in better care. Furthermore, almost all patients lived in Bavaria so that a generalization of results to Germany or even be-yond German borders is limited. Since almost all PWAD were Caucasian, the study lacks ethnic diversity.
Another limitation of the study was the use of proxy reports to investigate symptoms and QoL since severe cognitive impairment impeded the use of self-reports. It is well known that proxies estimate QoL of PWAD worse than persons with dementia themselves [42]. Dementia in a very young age might be considered even more dramatic and disastrous by proxy-raters than LOD so that a rater’s bias possibly influences the results. Furthermore, it is very difficult to assess symptoms and wellbeing of PWAD by observation. For example, delusions can hardly be diagnosed when the communicative abilities do not allow the PWAD to talk. What might be interpreted as “calm” by one proxy might be interpreted as “apa-thetic” by another. Agitation might be a motor restlessness or non-verbal expression of fear or pain. Finally, it is still not clear—and will possibly never be clear—what a good QoL in PWAD means since we are unable to ask the patients. We assume that QoL is high when patients appear calm and “content”, do not seem to be sad and are positively engaged with their environment. But we only conclude from observations and do not know—a concern that is often risen by family caregivers—how/if patients really feel.
Strengths of our study were the large patient sample, particularly in the group of YOD, the prospective study design, and a minimized inter-rater variability due to the use of only two investigators who were trained with regard to study assessments prior to study start. It was the first study to investigate persons with YOD in advanced disease stages and to compare YOD with LOD. Thus, a comparison was possible in order to find out whether patients with advanced YOD might be underserved in the care system that is geared to older patients. The study provided important insights into the QoL of PWAD living at home or in LTC and its determinants and the study results enabled us to suggest strategies that might be effective to enhance QoL.
ACKNOWLEDGMENTS
We would like to thank all persons with dementia and their families as well as the nursing staff and LTC administrators and all others for their invaluable contribution to this study.
The study was supported by the German Federal Ministry of Education and Research (project # 01GY1705).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-1302r2).
REFERENCES
[1] | Boersma F , Van Den Brink W , Deeg DJ , Eefsting JA , Van Tilburg W ((1999) ) Survival in a population-based cohort of dementia patients: Predictors and causes of mortality. Int J Geriatr Psychiatry 14: , 748–753. |
[2] | Arvanitakis Z , Shah RC , Bennett DA ((2019) ) Diagnosis and management of dementia: Review. JAMA 322: , 1589–1599. |
[3] | Reisberg B ((1988) ) Functional Assessment Staging (FAST). Psychopharmacol Bull 24: , 653–659. |
[4] | Wetzels R , Zuidema S , Jansen I , Verhey F , Koopmans R ((2010) ) Course of neuropsychiatric symptoms in residents with dementia in long-term care institutions: A systematic review. Int Psychogeriatr 22: , 1040–1053. |
[5] | Riedl L , Bertok M , Hartmann J , Fischer J , Rossmeier C , Dinkel A , Ortner M , Diehl-Schmid J ((2020) ) Development and testing of an informative guide about palliative care for family caregivers of people with advanced dementia. BMC Palliat Care 19: , 30. |
[6] | van der Steen JT , Radbruch L , Hertogh CM , de Boer ME , Hughes JC , Larkin P , Francke AL , Junger S , Gove D , Firth P , Koopmans RT , Volicer L ((2014) ) White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat Med 28: , 197–209. |
[7] | Vieira RT , Caixeta L , Machado S , Silva AC , Nardi AE , Arias-Carrion O , Carta MG ((2013) ) Epidemiology of early-onset dementia: A review of the literature. Clin Pract Epidemiol Ment Health 9: , 88–95. |
[8] | Harvey RJ , Skelton-Robinson M , Rossor MN ((2003) ) The prevalence and causes of dementia in people under the age of 65 years. J Neurol Neurosurg Psychiatry 74: , 1206–1209. |
[9] | Baptista MAT , Santos RL , Kimura N , Marinho V , Simões JP , Laks J , Johannenssen A , Barca ML , Engedal K , Dourado MCN ((2019) ) Differences in awareness of disease between young-onset and late-onset dementia. Alzheimer Dis Assoc Disord 33: , 129–135. |
[10] | Appelhof B , Bakker C , Van Duinen-van Den IJCL , Zwijsen SA , Smalbrugge M , Verhey FRJ , de Vugt ME , Zuidema SU , Koopmans R ((2019) ) Differences in neuropsychiatric symptoms between nursing home residents with young-onset dementia and late-onset dementia. Aging Ment Health 23: , 581–586. |
[11] | Bakker C , de Vugt ME , van Vliet D , Verhey FR , Pijnenburg YA , Vernooij-Dassen MJ , Koopmans RT ((2013) ) Predictors of the time to institutionalization in young- versus late-onset dementia: Results from the Needs in Young Onset Dementia (NeedYD) study. J Am Med Dir Assoc 14: , 248–253. |
[12] | Millenaar JK , de Vugt ME , Bakker C , van Vliet D , Pijnenburg YA , Koopmans RT , Verhey FR ((2016) ) The impact of young onset dementia on informal caregivers compared with late onset dementia: Results from the NeedYD Study. Am J Geriatr Psychiatry 24: , 467–474. |
[13] | Giebel C , Eastham C , Cannon J , Wilson J , Wilson J , Pearson A ((2020) ) Evaluating a young-onset dementia service from two sides of the coin: Staff and service user perspectives. BMC Health Serv Res 20: , 187. |
[14] | Grønning H , Rahmani A , Gyllenborg J , Dessau RB , Høgh P ((2012) ) Does Alzheimer’s disease with early onset progress faster than with late onset? A case-control study of clinical progression and cerebrospinal fluid biomarkers. Dement Geriatr Cogn Disord 33: , 111–117. |
[15] | Wattmo C , Wallin Å K ((2017) ) Early- versus late-onset Alzheimer’s disease in clinical practice: Cognitive and global outcomes over 3 years. Alzheimers Res Ther 9: , 70. |
[16] | The WHOQOL Group ((1995) ) The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc Sci Med 41: , 1403–1409. |
[17] | Ettema TP , Dröes RM , de Lange J , Mellenbergh GJ , Ribbe MW ((2005) ) A review of quality of life instruments used in dementia. Qual Life Res 14: , 675–686. |
[18] | Logsdon RG , Gibbons LE , McCurry SM , Teri L ((2002) ) Assessing quality of life in older adults with cognitive impairment. Psychosom Med 64: , 510–519. |
[19] | Castro-Monteiro E , Alhayek-Aí M , Diaz-Redondo A , Ayala A , Rodriguez-Blazquez C , Rojo-Perez F , Martinez-Martin P , Forjaz MJ ((2016) ) Quality of life of institutionalized older adults by dementia severity. Int Psychogeriatr 28: , 83–92. |
[20] | Clare L , Quinn C , Hoare Z , Whitaker R , Woods RT ((2014) ) Care staff and family member perspectives on quality of life in people with very severe dementia in long-term care: A cross-sectional study. Health Qual Life Outcomes 12: , 175. |
[21] | Banerjee S , Smith SC , Lamping DL , Harwood RH , Foley B , Smith P , Murray J , Prince M , Levin E , Mann A , Knapp M ((2006) ) Quality of life in dementia: More than just cognition. An analysis of associations with quality of life in dementia. J Neurol Neurosurg Psychiatry 77: , 146–148. |
[22] | Appelhof B , Bakker C , Van Duinen-van den Ijssel JCL , Zwijsen SA , Smalbrugge M , Verhey FRJ , de Vugt ME , Zuidema SU , Koopmans R ((2017) ) The determinants of quality of life of nursing home residents with young-onset dementia and the differences between dementia subtypes. Dement Geriatr Cogn Disord 43: , 320–329. |
[23] | Diehl-Schmid J , Hartmann J , Roßmeier C , Riedl L , Förstl H , Egert-Schwender S , Kehl V , Schneider-Schelte H , Jox RJ ((2018) ) IssuEs in Palliative care for people in advanced and terminal stages of Young-onset and Late-Onset dementia in GErmany (EPYLOGE): The study protocol. BMC Psychiatry 18: , 271. |
[24] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[25] | Weiner MF , Martin-Cook K , Svetlik DA , Saine K , Foster B , Fontaine CS ((2000) ) The quality of life in late-stage dementia (QUALID) scale. J Am Med Dir Assoc 1: , 114–116. |
[26] | Millenaar J , Hvidsten L , de Vugt ME , Engedal K , Selbæk G , Wyller TB , Johannessen A , Haugen PK , Bakker C , van Vliet D , Koopmans RT , Verhey FR , Kersten H ((2017) ) Determinants of quality of life in young onset dementia - results from a European multicenter assessment. Aging Ment Health 21: , 24–30. |
[27] | The International Statistical Classification Of Diseases And Related Health Problems, 10th revision, German Modification (ICD-10-GM) (Version 2004). |
[28] | The-Lund-and-Manchester-Groups ((1994) ) Clinical and neuropathological criteria for frontotemporal dementia. J Neurol Neurosurg Psychiatry 57: , 416–418. |
[29] | Rascovsky K , Hodges JR , Knopman D , Mendez MF , Kramer JH , Neuhaus J , van Swieten JC , Seelaar H , Dopper EG , Onyike CU , Hillis AE , Josephs KA , Boeve BF , Kertesz A , Seeley WW , Rankin KP , Johnson JK , Gorno-Tempini ML , Rosen H , Prioleau-Latham CE , Lee A , Kipps CM , Lillo P , Piguet O , Rohrer JD , Rossor MN , Warren JD , Fox NC , Galasko D , Salmon DP , Black SE , Mesulam M , Weintraub S , Dickerson BC , Diehl-Schmid J , Pasquier F , Deramecourt V , Lebert F , Pijnenburg Y , Chow TW , Manes F , Grafman J , Cappa SF , Freedman M , Grossman M , Miller BL ((2011) ) Sensitivity of revised diagnostic criteria for the behavioral variant of frontotemporal dementia. Brain 134: , 2456–2477. |
[30] | Gorno-Tempini ML , Hillis AE , Weintraub S , Kertesz A , Mendez M , Cappa SF , Ogar JM , Rohrer JD , Black S , Boeve BF , Manes F , Dronkers NF , Vandenberghe R , Rascovsky K , Patterson K , Miller BL , Knopman DS , Hodges JR , Mesulam MM , Grossman M ((2011) ) Classification of primary progressive aphasia and its variants. Neurology 76: , 1006–1014. |
[31] | McKeith IG , Dickson DW , Lowe J , Emre M , O’Brien JT , Feldman H , Cummings J , Duda JE , Lippa C , Perry EK , Aarsland D , Arai H , Ballard CG , Boeve B , Burn DJ , Costa D , Del Ser T , Dubois B , Galasko D , Gauthier S , Goetz CG , Gomez-Tortosa E , Halliday G , Hansen LA , Hardy J , Iwatsubo T , Kalaria RN , Kaufer D , Kenny RA , Korczyn A , Kosaka K , Lee VM , Lees A , Litvan I , Londos E , Lopez OL , Minoshima S , Mizuno Y , Molina JA , Mukaetova-Ladinska EB , Pasquier F , Perry RH , Schulz JB , Trojanowski JQ , Yamada M ((2005) ) Diagnosis and management of dementia with Lewy bodies: Third report of the DLB Consortium. Neurology 65: , 1863–1872. |
[32] | Román GC , Tatemichi TK , Erkinjuntti T , Cummings JL , Masdeu JC , Garcia JH , Amaducci L , Orgogozo JM , Brun A , Hofman A , et al. ((1993) ) Vascular dementia: Diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 43: , 250–260. |
[33] | Zerr I , Kallenberg K , Summers DM , Romero C , Taratuto A , Heinemann U , Breithaupt M , Varges D , Meissner B , Ladogana A , Schuur M , Haik S , Collins SJ , Jansen GH , Stokin GB , Pimentel J , Hewer E , Collie D , Smith P , Roberts H , Brandel JP , van Duijn C , Pocchiari M , Begue C , Cras P , Will RG , Sanchez-Juan P ((2009) ) Updated clinical diagnostic criteria for sporadic Creutzfeldt-Jakob disease. Brain 132: , 2659–2668. |
[34] | Zwijsen SA , Kabboord A , Eefsting JA , Hertogh CM , Pot AM , Gerritsen DL , Smalbrugge M ((2014) ) Nurses in distress? An explorative study into the relation between distress and individual neuropsychiatric symptoms of people with dementia in nursing homes. Int J Geriatr Psychiatry 29: , 384–391. |
[35] | Davis JD , Tremont G ((2007) ) Impact of frontal systems behavioral functioning in dementia on caregiver burden. J Neuropsychiatry Clin Neurosci 19: , 43–49. |
[36] | Farina N , King D , Burgon C , Berwald S , Bustard E , Feeney Y , Habibi R , Comas-Herrera A , Knapp M , Banerjee S ((2020) ) Disease severity accounts for minimal variance of quality of life in people with dementia and their carers: Analyses of cross-sectional data from the MODEM study. BMC Geriatr 20: , 232. |
[37] | Banerjee S , Samsi K , Petrie CD , Alvir J , Treglia M , Schwam EM , del Valle M ((2009) ) What do we know about quality of life in dementia? A review of the emerging evidence on the predictive and explanatory value of disease specific measures of health related quality of life in people with dementia. Int J Geriatr Psychiatry 24: , 15–24. |
[38] | Wetzels RB , Zuidema SU , de Jonghe JF , Verhey FR , Koopmans RT ((2010) ) Determinants of quality of life in nursing home residents with dementia. Dement Geriatr Cogn Disord 29: , 189–197. |
[39] | Samus QM , Rosenblatt A , Steele C , Baker A , Harper M , Brandt J , Mayer L , Rabins PV , Lyketsos CG ((2005) ) The association of neuropsychiatric symptoms and environment with quality of life in assisted living residents with dementia. Gerontologist 45 Spec No 1: , 19–26. |
[40] | Pijnenburg Y , Sampson E , Harvey R , Fox N , Rossor M ((2003) ) Vulnerability to neuroleptic side effects in frontotemporal lobar degeneration. Int J Geriatr Psychiatry 18: , 67–72. |
[41] | Vigen CL , Mack WJ , Keefe RS , Sano M , Sultzer DL , Stroup TS , Dagerman KS , Hsiao JK , Lebowitz BD , Lyketsos CG , Tariot PN , Zheng L , Schneider LS ((2011) ) Cognitive effects of atypical antipsychotic medications in patients with Alzheimer’s disease: Outcomes from CATIE-AD. Am J Psychiatry 168: , 831–839. |
[42] | Wu YT , Nelis SM , Quinn C , Martyr A , Jones IR , Victor CR , Knapp M , Henderson C , Hindle JV , Jones RW , Kopelman MD , Morris RG , Pickett JA , Rusted JM , Thom JM , Litherland R , Matthews FE , Clare L ((2020) ) Factors associated with self- and informant ratings of quality of life, well-being and life satisfaction in people with mild-to-moderate dementia: Results from the Improving the experience of Dementia and Enhancing Active Life programme. Age Ageing 49: , 446–452. |
[43] | Mahoney FI , Barthel DW ((1965) ) Functional evaluation: The BARTHEL Index. Md State Med J 14: , 61–65. |
[44] | Volicer L , Hurley AC , Blasi ZV ((2001) ) Scales for evaluation of end-of-life care in dementia. Alzheimer Dis Assoc Disord 15: , 194–200. |
[45] | Reisberg B , Ferris SH , de-Leon M , Crook T ((1982) ) The Global Deterioration Scale for assessment of primary degenerative dementia. Am J Psychiatry 139: , 1136–1139. |
[46] | Folstein MF , Folstein SE , McHugh PR ((1975) ) ‘Mini Mental State’. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[47] | Aminoff BZ ((2014) ) Prognosis of short survival in patients with advanced dementia as diagnosed by Aminoff suffering syndrome. Am J Alzheimers Dis Other Demen 29: , 673–677. |
[48] | Cummings JL , Mega M , Gray K , Rosenberg-Thompson S , Carusi DA , Gornbein J ((1994) ) The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 44: , 2308–3214. |
[49] | Warden V , Hurley AC , Volicer L ((2003) ) Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc 4: , 9–15. |

